Interstitial F 2 -Isoprostane 8-Iso-PGF 2α ...
10
Interstitial F 2 -Isoprostane 8-Iso-PGF 2a As a Biomarker of Oxidative Stress after Severe Human Traumatic Brain Injury Fredrik Clausen, 1 Niklas Marklund, 1 Anders Lewe ´ n, 1 Per Enblad, 1 Samar Basu, 2,3 and Lars Hillered 1 Abstract Oxidative stress is a major contributor to the secondary injury process after experimental traumatic brain injury (TBI). The importance of oxidative stress in the pathobiology of human TBI is largely unknown. The F 2 -isoprostane 8-iso-prostaglandin F 2a (8-iso-PGF 2a ), synthesized in vivo through non-enzymatic free radical cat- alyzed peroxidation of arachidonic acid, is a widely used biomarker of oxidative stress in multiple disease states, including TBI and cerebral ischemia/reperfusion. Our hypothesis is that harvesting of biomarkers directly in the injured brain by cerebral microdialysis (MD) is advantageous because of its high spatial and temporal resolution compared to blood or cerebrospinal fluid sampling. The aim of this study was to test the feasibility of measuring 8-iso-PGF 2a in MD, ventricular cerebrospinal fluid (vCSF), and plasma samples collected from patients with severe TBI, and to compare the MD signals with MD-glycerol, implicated as a biomarker of oxidative stress, as well as MD-glutamate, a biomarker of excitotoxicity. Six patients (4 men, 2 women) were included in the study, three of whom had a focal/mixed TBI, and three a diffuse axonal injury (DAI). Following the bedside analysis of routine MD biomarkers (glucose, lactate:pyruvate ratio, glycerol, and glutamate), two 12-h MD samples per day were used to analyze 8-iso-PGF 2a from 24h up to 8 days post-injury. The interstitial levels of 8-iso-PGF 2a were markedly higher than the levels obtained from plasma and vCSF ( p < 0.05), supporting our hypothesis. The MD-8-iso-PGF 2a levels correlated strongly ( p < 0.05) with MD-glycerol and MD-glutamate, which are widely used biomarkers of membrane phospholipid degradation/oxidative stress and excitotoxicity, respectively. This study demonstrates the feasibility of analyzing 8-iso-PGF 2a in MD samples from the human brain. Our results support a close rela- tionship between oxidative stress and excitotoxicity following human TBI. MD-8-iso-PGF 2a in combination with MD-glycerol may be useful biomarkers of oxidative stress in the neurointensive care setting. Key words: biomarkers; microdialysis; oxidative stress; traumatic brain injury Introduction T raumatic brain injury (TBI) is a major global public health problem and the leading cause of mortality and disability in young adults. TBI is a major health issue also in the growing elderly population due to an increasing number of falls. Currently, there are no specific neuroprotective pharmacological treatment options available for TBI patients. Numerous experimental reports suggest that a prominent secondary injury mechanism after TBI is the increased pro- duction of reactive oxygen/nitrogen species (ROS/RNS), overwhelming the endogenous defense systems and leading to oxidative stress and secondary cell damage (Hall et al., 2010; Lewen et al., 2000). ROS/RNS can be defined as an oxygen/nitrogen species with one or more unpaired electrons (Freeman and Crapo, 1982), including the superoxide (O 2 c - ), hydroxyl radical (OHc) and nitric oxide (NOc). Superoxide (O 2 c - ) is generated via normal cell metabolism (Zalba et al., 2007), and this physiological ROS production is effectively balanced by the endogenous scavenger systems, including mitochondrial manganese superoxide dismutase (Mn-SOD), intra- and ex- tracellular copper/zinc superoxide dismutase (Cu/Zn-SOD), catalase, and glutathione (Halliwell, 2006). 1 Departments of Neuroscience and Neurosurgery, and 2 Department of Public Health and Caring Sciences, Oxidative Stress and Inflammation, Uppsala University, Uppsala University Hospital, Uppsala, Sweden. 3 Laboratorie de Biochimie, Biologie Mole ´culaire et Nutrition, Faculte ´ de Pharmacie, Universite ´ d’Auvergne, Clermont-Ferrand, France. JOURNAL OF NEUROTRAUMA 29:766–775 (March 20, 2012) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2011.1754 766
Transcript of Interstitial F 2 -Isoprostane 8-Iso-PGF 2α ...

Interstitial F2-Isoprostane 8-Iso-PGF2a As a Biomarkerof Oxidative Stress after Severe Human
Traumatic Brain Injury
Fredrik Clausen,1 Niklas Marklund,1 Anders Lewen,1 Per Enblad,1 Samar Basu,2,3 and Lars Hillered1
Abstract
Oxidative stress is a major contributor to the secondary injury process after experimental traumatic braininjury (TBI). The importance of oxidative stress in the pathobiology of human TBI is largely unknown. TheF2-isoprostane 8-iso-prostaglandin F2a (8-iso-PGF2a), synthesized in vivo through non-enzymatic free radical cat-alyzed peroxidation of arachidonic acid, is a widely used biomarker of oxidative stress in multiple disease states,including TBI and cerebral ischemia/reperfusion. Our hypothesis is that harvesting of biomarkers directly in theinjured brain by cerebral microdialysis (MD) is advantageous because of its high spatial and temporal resolutioncompared to blood or cerebrospinal fluid sampling. The aim of this study was to test the feasibility of measuring8-iso-PGF2a in MD, ventricular cerebrospinal fluid (vCSF), and plasma samples collected from patients with severeTBI, and to compare the MD signals with MD-glycerol, implicated as a biomarker of oxidative stress, as well asMD-glutamate, a biomarker of excitotoxicity. Six patients (4 men, 2 women) were included in the study, three ofwhom had a focal/mixed TBI, and three a diffuse axonal injury (DAI). Following the bedside analysis of routineMD biomarkers (glucose, lactate:pyruvate ratio, glycerol, and glutamate), two 12-h MD samples per day were usedto analyze 8-iso-PGF2a from 24 h up to 8 days post-injury. The interstitial levels of 8-iso-PGF2a were markedlyhigher than the levels obtained from plasma and vCSF ( p < 0.05), supporting our hypothesis. The MD-8-iso-PGF2a
levels correlated strongly ( p < 0.05) with MD-glycerol and MD-glutamate, which are widely used biomarkers ofmembrane phospholipid degradation/oxidative stress and excitotoxicity, respectively. This study demonstratesthe feasibility of analyzing 8-iso-PGF2a in MD samples from the human brain. Our results support a close rela-tionship between oxidative stress and excitotoxicity following human TBI. MD-8-iso-PGF2a in combination withMD-glycerol may be useful biomarkers of oxidative stress in the neurointensive care setting.
Key words: biomarkers; microdialysis; oxidative stress; traumatic brain injury
Introduction
Traumatic brain injury (TBI) is a major global publichealth problem and the leading cause of mortality and
disability in young adults. TBI is a major health issue also inthe growing elderly population due to an increasing numberof falls. Currently, there are no specific neuroprotectivepharmacological treatment options available for TBI patients.Numerous experimental reports suggest that a prominentsecondary injury mechanism after TBI is the increased pro-duction of reactive oxygen/nitrogen species (ROS/RNS),overwhelming the endogenous defense systems and leading
to oxidative stress and secondary cell damage (Hall et al.,2010; Lewen et al., 2000).
ROS/RNS can be defined as an oxygen/nitrogen specieswith one or more unpaired electrons (Freeman and Crapo,1982), including the superoxide (O2c - ), hydroxyl radical(OHc) and nitric oxide (NOc). Superoxide (O2c - ) is generatedvia normal cell metabolism (Zalba et al., 2007), and thisphysiological ROS production is effectively balanced by theendogenous scavenger systems, including mitochondrialmanganese superoxide dismutase (Mn-SOD), intra- and ex-tracellular copper/zinc superoxide dismutase (Cu/Zn-SOD),catalase, and glutathione (Halliwell, 2006).
1Departments of Neuroscience and Neurosurgery, and 2Department of Public Health and Caring Sciences, Oxidative Stress andInflammation, Uppsala University, Uppsala University Hospital, Uppsala, Sweden.
3Laboratorie de Biochimie, Biologie Moleculaire et Nutrition, Faculte de Pharmacie, Universite d’Auvergne, Clermont-Ferrand, France.
JOURNAL OF NEUROTRAUMA 29:766–775 (March 20, 2012)ª Mary Ann Liebert, Inc.DOI: 10.1089/neu.2011.1754
766

Following acute brain injury including TBI and ischemicstroke, numerous mechanisms including intracellular Ca2 +
overload, inhibition of the mitochondrial respiratory chain,release of arachidonic acid from membrane phospholipids,and accumulation of hypoxanthine lead to the overproduc-tion of superoxide (Bayir and Kagan, 2008; Fiskum et al.,1999). Superoxide is not considered harmful, but may readilyreact with nitric oxide (NOc) to form peroxynitrite (ONOO - )or dismutate to hydrogen peroxide, which reacts with iron toform hydroxyl radicals (OHc), with the capacity to damagecells by lipid peroxidation, protein oxidation, and DNAdamage.
Isoprostanes are synthesized in vivo mainly via non-enzymatic, free radical-catalyzed peroxidation of arachidonicacid (Morrow et al., 1990). One of the most studied isopro-stanes, 8-iso-prostaglandin F2a (8-iso-PGF2a; molecular weight454.5 Da), is overproduced in diverse disorders such as ath-erosclerosis, rheumatoid arthritis, hypertension, and Alzhei-mer’s disease, all of which are associated with oxidative stress(Basu, 2008; Morrow et al., 1992). 8-iso-PGF2a measured inblood or cerebrospinal fluid (CSF) has been implicated asa useful marker of oxidative stress in cerebral ischemia/reperfusion in a porcine cardiac arrest model and in cardiacarrest patients (Basu et al., 2000; Wiklund et al., 2005), as well asin CSF of human pediatric and adult TBI patients (Bayir et al.,2002,2004).
Oxidative stress following TBI is thought to be closelyassociated with excitotoxicity (i.e., glutamate-mediated in-tracellular accumulation of Ca2 + ), leading to membranephospholipid degradation and the formation of arachidonicacid (for references see Hillered et al., 2005). Another endproduct of this phospholipid degradation process is glycerol(Clausen et al., 2005; Hillered et al., 2005; Marklund et al.,1997; Nguyen et al., 2007), which has also been implicated as abiomarker of oxidative stress (Clausen et al., 2005; Lewen andHillered, 1998; Merenda et al., 2008). Another potentiallyimportant link between oxidative stress and excitotoxicity isthe microglial antiporter system Xc
2 (Sato et al., 2002), whichreleases cytotoxic levels of glutamate into the interstitialcompartment to replenish intracellular cystine to maintain theglutathione system, which is challenged by oxidative stress(Qin et al., 2006).
Microdialysis (MD) is the only bedside monitoring tool thatcan evaluate, hour-by hour, the focal neurochemistry of theinjured human brain, and is being used as a clinically relevantmonitoring method in neurointensive care units (neuro-ICUs)worldwide (Goodman and Robertson, 2009; Hillered et al.,2006; Tisdall and Smith, 2006). Our basic hypothesis is thatharvesting of biomarkers directly in the injured brain tissueprovides chemical signals with a better temporal and spatialresolution, and also avoids biomarker degradation, comparedto conventional CSF or blood sampling methods (Liu et al.,2010; Marklund et al., 2009). Although other techniques suchas gas chromatography/mass spectrometry (GC/MS), liquidchromatography/mass spectrometry (LC-MS), and enzymeimmunoassay (EIA) have been used to measure isoprostanesin a variety of compartments (Basu, 2008), we chose toquantify 8-iso-PGF2a in the MD samples with a radioimmu-noassay (RIA) previously developed and characterizedwithin the group (Basu, 1998).
The aims of the present study were to: (1) explore the fea-sibility of measuring 8-iso-PGF2a in cerebral MD samples from
neuro-ICU patients with severe TBI, (2) to compare 8-iso-PGF2a
levels in the cerebral interstitial compartment (MD) with vCSFand blood, and (3) to study the relationship between MD-8-iso-PGF2a and MD-glycerol as well as MD-glutamate, widely usedbiomarkers of membrane phospholipid degradation/oxidativestress and excitotoxicity, respectively.
Methods
All research procedures described herein were approvedby the Regional Ethical Review Board at Uppsala Universityand informed consent was obtained from the patient’s closestrelative.
Patients
Six patients with severe TBI arriving to the Uppsala Uni-versity Hospital Neuro-ICU with a motor component of theGlasgow Coma Scale (GCS, Teasdale and Jennett, 1974) of 3–5,corresponding to a Reaction Level Scale (RLS) score of 3–6(Stalhammar et al., 1988) were included in the present study(Table 1). All patients were mechanically ventilated and fol-lowing admission to our unit, an intracranial pressure (ICP)monitoring device was inserted, and evacuation of significantmass lesions was immediately performed when needed. Threepatients were classified as a focal/mixed TBI, and three pa-tients a diffuse axonal injury (DAI), according to CT criteria(Marshall et al., 1992). All patients were treated in the neuro-ICU using an ICP-guided protocol with mild hyperventilation(partial carbon dioxide pressure [Paco2] 30–35 mm Hg; 4.0–4.5 kPa), head elevation (30�), and careful volume expansion toobtain normovolemia (Elf et al., 2002). The neurological con-dition of each patient was regularly assessed, up to six timesdaily, using the neurological wake-up test (Skoglund et al.,2009). Outcome was assessed at 6 months post-injury using theextended Glasgow Outcome Scale (eGOS; Jennett et al., 1981).
Microdialysis and bedside biomarkers in the neuro-ICU
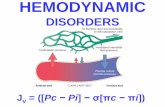
Intracerebral MD was initiated, in conjunction with theinsertion of an ICP monitoring device, through MD cathetersinserted via a burr hole (n = 5), 1–2 cm anterior to the coronalsuture, or in the pericontusional tissue following craniectomyfor the removal of a mass lesion (n = 1). In all patients care wastaken to insert the MD catheter obliquely into the cortex usinga non-traumatic technique to achieve a position with themajor part of the membrane surface within the gray matter.This was confirmed by evaluating the CT scans of each pa-tient. Theoretically this positioning should enable the MDcatheter tip to follow the movements of the brain withoutfurther tissue damage. Figure 1 shows the MD probe and ICPmonitor probe in patient 2. We used CMA-71 MD catheterswith a membrane length of 10 mm and a 100-kDa nominalmolecular weight cut-off polyarylethersulfone (PAES) mem-brane (CMA Microdialysis, Stockholm, Sweden). The outflowhydrostatic pressure of the perfusion system was set at thezero mid-cranial reference level by taping the collecting vialsat the bandage on the patient’s head to avoid additional hy-drostatic effects on fluid recovery of the catheter (Hillmanet al., 2005). Perfusion of the catheters was performed usingartificial CSF (Perfusion Fluid CNS; CMA Microdialysis),containing 147 mM NaCl, 2.7 mM KCl, 1.2 mM CaCl2, and0.85 mM MgCl2, at a rate of 0.3 lL/min using a CMA106
ISOPROSTANE AS A BIOMARKER FOR OXIDATIVE STRESS 767

Ta
bl
e1.
De
mo
gr
ap
hic
sa
nd
In
ju
ry
Ch
ar
ac
te
rist
ic
s
Pat
ien
tn
o.1
23
45
6
Gro
up
Fo
cal
Dif
fuse
Dif
fuse
Fo
cal
Fo
cal
Dif
fuse
Ag
e/g
end
er15
/F
19/
M25
/M
62/
M32
/M
67/
FC
ause
of
inju
ryM
VA
Fal
lF
all
Fal
lF
all
Fal
lA
sso
ciat
edin
juri
es/
con
dit
ion
sS
ku
llfx
,cl
avic
ula
rfx
Sk
ull
fx,
alco
ho
lP
neu
mo
thx
,sk
ull
/fa
cial
fx,
Th
fxA
lco
ho
l.sk
ull
fxaR
up
ture
dan
eury
sm,
seiz
ure
sF
all
GM
S/
RL
So
nar
riv
al4/
IV4/
IV5/
III
5/II
I3/
VI
4/V
Pu
pil
so
nar
riv
alB
ilat
no
rmal
Bil
atn
orm
alB
ilat
no
rmal
Bil
atn
orm
alB
ilat
no
n-r
esp
on
siv
eB
ilat
no
rmal
Pen
tob
arb
ital
No
Yes
Yes
No
No
No
MD
loca
tio
nR
FR
FL
FR
F-c
rtR
FR
FM
Dd
ura
tio
n(h
)20
–129
16–9
921
–59
30–1
9115
–142
25–8
4L
eng
tho
fst
ay(d
ays)
816
1611
257
GM
S/
RL
So
nd
epar
ture
6/I
6/I
6/I
6/II
3/V
I6/
IIeG
OS
3m
on
ths
67
53
N/
A4
Mar
shal
lcl
assi
fica
tio
nE
ML
DI2
DI2
EM
LE
ML
DI2
Les
ion
typ
e/h
emat
om
av
olu
me
(cm
3)
ED
H/
44C
cx/
9C
cx,
ED
H/
11.5
Ccx
/63
SD
H/
52tS
AH
/N
A
tSA
HB
il.
Sy
l+
+L
Sy
l+
Bci
st,
+B
cist
,cx
++
+N
o.
of
CT
scan
s4
76
64
2M
idli
ne
shif
t(m
m)
43
28.
510
0IV
H-
--
--
+B
asal
cist
ern
s2
11
22
0M
ass
lesi
on
loca
tio
nB
FB
FN
F,
LT
BF
LF
PN
A
aT
his
pat
ien
tfe
llan
dsu
stai
ned
ase
ver
eT
BI
du
eto
aru
ptu
red
aneu
rysm
.C
om
pu
ted
tom
og
rap
hy
(CT
)ch
arac
teri
stic
su
sin
gth
ew
ors
tC
Tsc
and
uri
ng
the
neu
ro-I
CU
stay
(Ser
vad
eiet
al.,
2000
)ac
cord
ing
toth
eM
arsh
all
clas
sifi
cati
on
(Mar
shal
let
al.,
1992
).+
,++
,an
d++
+is
ase
miq
uan
tita
tiv
esc
ale
ind
icat
ing
the
deg
ree
of
sub
arac
hn
oid
blo
od
;R
F-c
rt,
rig
ht
fro
nta
l,in
sert
edv
iacr
anio
tom
y;
cx,
con
tusi
on
;G
MS
,m
oto
rco
mp
on
ent
of
the
Gla
sgo
wC
om
aS
cale
;RL
S,R
eact
ion
Lev
elS
cale
;eG
OS
,ex
ten
ded
Gla
sgo
wO
utc
om
eS
cale
;M,m
ale;
F,f
emal
e;M
VA
,mo
tor
veh
icle
acci
den
t;R
F,r
igh
tfr
on
tal;
LF
,lef
tfr
on
tal;
N/
A,d
ata
mis
sin
g;f
x,fr
actu
re;P
neu
mo
thx
,p
neu
mo
tho
rax
;T
h,
Th
ora
cic;
tSA
H,
trau
mat
icsu
bar
ach
no
idh
emo
rrh
age;
IVH
,in
trav
entr
icu
lar
hem
orr
hag
e;D
I2,
dif
fuse
inju
ry2;
BF
,b
ifro
nta
l;S
DH
,su
bd
ura
lh
emat
om
a;E
ML
,ev
acu
ated
mas
sle
sio
n;
ED
H,
epid
ura
lh
emat
om
a;C
cx,
cort
ical
con
tusi
on
;B
il.
Sy
l,b
ilat
eral
Sy
lvia
nfi
ssu
re;
LS
yl,
left
Sy
lvia
nfi
ssu
re;
Bci
st,
bas
alci
ster
ns;
MD
,m
icro
dia
lysi
s;N
A,
no
tap
pli
cab
le;
0,n
orm
al;
1,co
mp
ress
edy
etv
isib
le;
2,co
mp
ress
ed;
BF
,b
ifro
nta
l;L
T,
left
tem
po
ral;
LF
P,
left
fro
nto
par
ieta
l;T
BI,
trau
mat
icb
rain
inju
ry.
768

microinjection pump (CMA Microdialysis). The rationale forusing this perfusion fluid was the data from Hutchinson andassociates (Hutchinson et al., 2005), showing similar in vivoextraction efficiency for small molecules with the CMA-71compared with the CMA-70 (20-kDa cutoff ) catheter. Atleast 2 h passed after insertion of the probe and the start ofsampling, to allow for normalization of changes due toprobe insertion. MD samples (approximately 18 lL) wereobtained hourly and analyzed bedside for glucose, lactate,pyruvate, and urea, with an enzymatic colorimetric tech-nique on a CMA 600 Microdialysis Analyser (CMA Micro-dialysis). The lactate/pyruvate (L/P) ratio was calculated.Urea was monitored to control the probe performance(Ronne-Engstrom et al., 2001). After bedside analysis, theremaining samples were stored on ice for up to 12 h in theneuro-ICU, and then at -20�C for up to 7 days, pendinganalysis of glutamate and glycerol on a CMA 600. The re-maining samples were stored at - 70�C until further ana-lyzed for isoprostane.
The CMA 600 Analyser was automatically calibrated whenstarted, as well as every sixth hour, using standard calibrationsolutions from the manufacturer (CMA Microdialysis). Qualitycontrols at two different concentrations for each substancewere performed every weekday. Imprecision values for be-tween-assay coefficient of variation was < 10% for all analytes.
Blood, ventricular cerebrospinal fluid,and urine sampling
Arterial plasma (heparin), vCSF, and urine samples werecollected simultaneously on a daily basis following morning
rounds, normally between 11 am and 2 pm. Occasionally, theintracranial situation did not permit vCSF sampling from theventricular drain. All samples were centrifuged and trans-ferred to a new test tube. All samples (1- to 2-mL fractions)were stored immediately upon work-up at -70�C to mini-mize isoprostane degradation until they were analyzed for 8-iso-PGF2a.
Radioimmunoassay of 8-iso-PGF2a
MD, plasma, CSF, and urine samples were analyzed for 8-iso-PGF2a by an RIA as previously described (Basu, 1998). Toachieve a sample size sufficient for the analysis of 8-iso-PGF2a
the microdialysate samples from 12 consecutive hours werepooled. The cross-reactivities of the 8-iso-PGF2a antibody with15-keto-13,14-dihydro-8-iso-PGF2a, 8-iso-PGF2a, PGF2a, 15-keto-PGF2a, 15-keto-13,14-dihydro-PGF2a, TXB2, 11b-PGF2a,9b-PGF2a, and 8-iso-PGF3a, were 1.7, 9.8, 1.1, 0.01, 0.01, 0.1,0.03, 1.8 and 0.6%, respectively. The detection limit was23 pmol/L (8 pg/mL).
The levels of 8-iso-PGF2a in urine samples were used as amethodological control to verify a reasonable urinary outputcompared to published reference data (Basu, 2008), since toour knowledge there are no published reference data for 8-iso-PGF2a in MD samples from the human brain. Therefore,only the average urinary level of the patient group is pre-sented in the text, while the primary interest was focused onthe MD, vCSF, and blood levels in the illustrations.
Statistical methods
Statistical analyses were made using Statistica� software(StatSoft, Tulsa, OK). The hourly measurements of lactate, py-ruvate, glutamate, glucose, and glycerol were averaged for the12 h corresponding to the pooled sample used for 8-iso-PGF2a
analysis. Medians of 8-iso-PGF2a and the routine biomarkersfrom each patient were subjected to weighted non-parametriccorrelation analysis (Spearman Rank correlation), for whichthe weight was determined by the number of samples fromeach patient. Samples from vCSF, plasma, and urine werematched to the corresponding pooled MD samples so thatthe 12-h MD sampling period started at least 3 h before snapsample collection. Data were analyzed statistically usingnon-parametric tests (Kruskal-Wallis analysis of variance[ANOVA], followed by Mann-Whitney U tests). All MD dataare presented as dialysate concentrations without correctionfor in vivo recovery.
Results
Patients
The mean age of the patients was 37 – 22 years (range 15–67years), and there were four male and two female patients. Theclinical and radiological characteristics for each patient areshown in Table 1.
Microdialysis and bedside biomarkers in the neuro-ICU
Microdialysis was started at a mean of 19.5 – 3.6 h afterinjury, and the average duration of sampling was 97 – 45 h.The critical values considered in this study were glucose<1.0 mmol/L; L/P ratio > 40; lactate > 3.8 mmol/L; pyruvate<120lmol/L; glutamate > 15 lmol/L; and glycerol > 100 lmol/
FIG. 1. A computed tomography (CT) scan image frompatient 2 confirming the location of the microdialysis (MD)catheter. Arrow A points to the intracranial pressure moni-tor, and arrow B at the MD catheter.
ISOPROSTANE AS A BIOMARKER FOR OXIDATIVE STRESS 769

L, based on published data and our own experience (Reinstrupet al., 2000; Schulz et al., 2000). Five out of six patients hadconsistently high lactate concentrations during the moni-toring period (patients 2–6). Two of the six patients hadglutamate concentrations within the normal range (patients1 and 4). Three patients (patients 3, 5, and 6) had initiallyhigh concentrations of glutamate, which abated over time,and one patient initially had a normal concentration of gluta-mate, which was then markedly increased at *50 h post-TBI(patient 2). Three patients (patients 4, 5, and 6) had initially highconcentrations of glycerol ( >100lmol/L), that normalizedover time, two had initially normal concentrations that in-creased over time to markedly elevated levels ( >100 lmol/L;patients 2 and 3), and one had normal concentrationsthroughout the monitoring period (patient 1).
8-iso-PGF2a concentrations in interstitial fluid,CSF, plasma, and urine
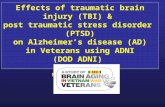
In the plasma and vCSF, 8-iso-PGF2a levels were low,reaching 134.6 – 56 pmol/L and 135.2 – 69 pmol/L, respec-tively (Fig. 2). In the urine, 8-iso-PGF2a levels reached701 – 280 pmol/L (not shown) when corrected for creatinine(Sjogren et al., 2005). The level of 8-iso-PGF2a was significantlyhigher in the MD samples (1057 – 326 pmol/L) compared toCSF and plasma ( p < 0.05; Fig. 2). The MD 8-iso-PGF2a levelsdecreased over time in three patients. Two patients showedhigh concentrations throughout the sample collection( > 1500 pmol/L), and one patient had a concentration con-sistently at approximately 800 pmol/L (Fig. 3).
Relations among 8-iso-PGF2a
and other MD biomarkers
We found strong, statistically significant correlationsbetween the levels of MD-8-iso-PGF2a and MD-glycerol(r = 0.830, p < 0.05), as well as MD-glutamate (r = 0.626,p < 0.05; Table 2). The calculated factors of dependency (r2;0.69 and 0.39, respectively) suggest that about 70% of the MD-glycerol signal and 40% of the MD-glutamate signal is relatedto oxidative stress, based on the assumption that 8-iso-PGF2a
is a specific marker for oxidative stress (Awad et al., 1993;Basu, 2008; Morrow et al., 1992). Furthermore, MD-8-iso-PGF2a correlated negatively with MD-L/P ratio (r = –0.554;p < 0.05). There was a weak correlation between MD-8-iso-PGF2a and MD-lactate and MD-pyruvate levels (r = 0.41;p < 0.05), and no correlation with MD-glucose (Table 2).
8-iso-PGF2a levels and focal versus diffuse brain injury
Patients with a focal TBI had lower MD-8-iso-PGF2a levels(mean 1019 – 160 pmol/L) than the levels observed in patientswith diffuse brain injury (mean 1776 – 1012 pmol/L). How-ever, due to the difference in the number of observations, andthe variance in patients with diffuse axonal injury, this did notreach statistical significance.
Illustrative cases
Patient 2, diffuse brain injury. This 19-year-old male pa-tient fell 2.5 m and suffered a TBI. Initially the patient was RLS4 (GCS 6–7), and a CT scan showed minimal bifrontal con-tusions, traumatic subarachnoid hemorrhage, cerebral swell-
ing, and signs of a diffuse brain injury. The patient receivedintraparenchymal ICP monitoring, and initially the ICP wasslightly elevated at *20 mm Hg, which responded to hyper-ventilation. At *28 h post-injury, the patient self-extubatedand was immediately re-intubated. ICP gradually normalizedand hyperventilation was discontinued at *56 h post-injury.The patient was GMS 5 and was extubated at *80 h post-injury. However, at approximately 6 days post-injury, thepatient became more confused, and a CT scan showed in-creased swelling, and the patient was again intubated andhigh-dose pentobarbital treatment was needed to control theelevated ICP. At the end of the stay in the neuro-ICU, thepatient was again extubated, and had GCS score 13–14 andRLS score 1–2. The patient made an uneventful recovery withan eGOS score of 7 at long-term follow-up. This patient had apeak in the 8-iso-PGF2a levels of more than 5000 pmol/L(Fig. 4A), which decreased when hyperventilation was dis-continued. The same pattern was observed for MD-gluta-mate, which also reached very high levels at the early stage.MD-glycerol levels gradually increased in a delayed fashionduring the monitoring period, reaching a high concentration( > 100 lmol/L) 88 h after injury (Fig. 4A). The L/P ratio didnot reveal signs of ongoing ischemia (data not shown).
Patient 4, focal brain injury. This patient fell backwards,struck his head, and was initially unconscious. In the emer-gency department at the primary hospital, he had GMS scoreof 5 (RLS 3), and had left-sided weakness. Following intuba-tion, a CT scan showed a frontal right epidural hematoma,bifrontal contusions, and a skull fracture. Initially the patientwas stable, but at *30 h post-TBI, the right pupil dilated and aCT scan showed marked progress of the right-sided frontalcontusion that was immediately evacuated and intra-parenchymal ICP monitoring and a pericontusional MDprobe was inserted via the right-sided craniotomy. After thecontusion hematoma was evacuated, ICP was within thenormal range, and the patient had an uneventful clinicalcourse during the neuro-ICU stay. He was subsequently
Plasma CSF MD0
200
400
600
800
1000
1200
1400
1600
1800
2000
pm
ol/L
Median 25%-75% Non-outlier range
*
FIG. 2. Concentrations of 8-iso-PGF2a in different compart-ments, presented as the median value, quartiles, and non-outlier range. The microdialysis (MD) samples showed sig-nificantly higher concentrations of 8-iso-PGF2a (marked withan asterisk; p < 0.05) than plasma and cerebrospinal fluid(CSF; 8-iso-PGF2a, F2-isoprostane 8-iso-prostaglandin F2a).
770 CLAUSEN ET AL.

extubated, and had GMS and RLS scores of 6 and 2, respec-tively, prior to departure from our unit. At long-term follow-up, he had an eGOS score of 3. In this patient, MD-glutamatelevels were consistently low (Fig. 4B). In contrast, initial MD-glycerol levels were markedly elevated, and then graduallysubsided (Fig. 3B). The MD-8-iso-PGF2a levels were initiallyabove 1500 pmol/L, decreasing to under 1000 pmol/L 2 daysafter injury, after which there was a slow increase over thenext 2 days (Fig. 4B).
Discussion
In this study we evaluated the feasibility of measuringinterstitial levels of 8-iso-PGF2a, a widely used biomarker foroxidative stress, using intracerebral MD in neuro-ICU pa-tients with severe TBI. We also measured and compared 8-iso-PGF2a levels in other compartments, including vCSF andplasma. Finally, we studied the relations between MD-8-isoPGF2a levels and MD-glycerol, as well as MD-glutamate,
widely used biomarkers of membrane phospholipid degra-dation/oxidative stress and excitotoxicity, respectively. Ourmain findings were that 8-iso-PGF2a can be measured in MDsamples, and that the levels of MD-8-iso-PGF2a were distinctlyhigher than in vCSF and blood, supporting our basic hy-pothesis of the usefulness of harvesting biomarkers directlyin the injured brain tissue. Importantly, there was a strongrelation between MD-8-iso-PGF2a, MD-glycerol, and MD-glutamate levels, supporting the link between oxidative stress,membrane phospholipid degradation, and excitotoxicity, aspreviously suggested in the experimental TBI setting (Lewenet al., 2000; Schulz et al., 1995).
Following TBI, the secondary injury process markedly ex-acerbates, up to several times, the size of the primary lesion.Experimental evidence clearly demonstrates the importantrole of oxidative stress (Hall, 1993; Kontos and Wei, 1986;Marklund et al., 2001a; Shohami et al., 1997) following TBI,and inhibition of ROS has consistently been shown to atten-uate the histological and behavioral deficits (Clausen et al.,
Table 2. Spearman-Rank Order Correlation Coefficients for the MD Biomarkers
Glucose Lactate Pyruvate L/P-ratio MD-isoprostane Glutamate Glycerol
Glucose 1.000000 0.600331 0.600331 - 0.283323 0.097334 - 0.220500 0.181649Lactate 0.600331 1.000000 1.000000 0.167183 0.409382 20.345319 0.226700Puryvate 0.600331 1.000000 1.000000 0.167183 0.409382 20.345319 0.226700L/P-ratio - 0.283323 0.167183 0.167183 1.000000 -0.553627 20.663567 20.495350MD-isoprostane 0.097334 0.409382 0.409382 20.553627 1.000000 0.626369 0.830130Glutamate - 0.220500 20.345319 - 0.345319 20.663567 0.626369 1.000000 0.712751Glycerol 0.181649 0.226700 0.226700 20.495350 0.830130 0.712751 1.000000
Bold values are statistically significant ( p < 0.05; n = 45), weighted for the number of samples per patient. The strongest correlation wasfound between MD-8-iso-PGF2a and glycerol (r = 0.83; p < 0.05), followed by MD-8-iso-PGF2a and glutamate (r = 0.63, p < 0.05).
L/P, lactate/pyruvate ratio; MD, microdialysis; 8-iso-PGF2a, F2-isoprostane 8-iso-prostaglandin F2a.
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Sample
0
1000
2000
3000
4000
5000
6000
7000
MD
-8-i
so-P
GF
2a (
pM
)
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
FIG. 3. Individual concentrations of 8-iso-PGF2a in brain interstitial fluid using intracerebral microdialysis (MD; patients 1,4, and 5 with focal TBI; patients 2, 3, and 6 with diffuse axonal injury; 8-iso-PGF2a, F2-isoprostane 8-iso-prostaglandin F2a; TBI,traumatic brain injury).
ISOPROSTANE AS A BIOMARKER FOR OXIDATIVE STRESS 771

2008; Hall et al., 2010; Marklund et al., 2001b). Following ex-perimental TBI (Roof et al., 1997; Tyurin et al., 2000), andglobal cerebral ischemia (Idris et al., 2005), in animal models,early F2-isoprostane levels were markedly increased. Al-though F2-isoprostane in CSF has been shown to correlatewith clinical neurological outcomes in a small study of pa-tients with severe TBI (Wagner et al., 2004), bedside tools formonitoring ROS activity in human TBI are lacking, and havehampered our understanding of the role of oxidant activity inhumans. Since F2-isoprostanes are stable and extremely sen-sitive and robust markers of secondary oxidant injury (Awadet al., 1993), they could be useful target markers for oxidativestress following human TBI, as suggested in studies of vCSFin pediatric and adult TBI patients (Bayir et al., 2002, 2004).
In the present report, we found that the interstitial (MD)levels of 8-iso-PGF2a were markedly (five- to sixfold) higherthan in vCSF and plasma, supporting our basic hypothesisabout the advantage of sampling with MD directly in injuredbrain tissue, thus improving spatial and temporal resolutionof the biomarker. Notably, a significantly higher level of 8-iso-PGF2a in the MD samples compared to the other com-partments was found, even though no correction for in vivorecovery (currently unknown) was done, suggesting that the8-iso-PGF2a levels obtained by MD may be markedly under-estimated. The 8-iso-PGF2a levels in plasma samples were inline with those found in previous reports using a pig model ofcardiac arrest and the same analytical method for measuringfree 8-iso-PGF2a (Wiklund et al., 2005). These levels are notdirectly comparable with the studies of Bayir and associates(Bayir et al., 2002, 2004), who used a different assay to mea-sure the total amount of 8-iso-PGF2a. The concentrations of8-iso-PGF2a in the normal, uninjured human brain are stillunknown.
In the validation part of the study, we found a strong cor-relation between MD-8-iso-PGF2a and MD-glycerol. MD-glycerol is a widely used biomarker in the neuro-ICU setting,and can readily be measured at the bedside using commer-cially available MD analyzers. MD-glycerol is generallythought to reflect cell membrane phospholipid (PL) degra-dation following brain injury, leading to an accumulation ofarachidonic acid (AA) and other free fatty acids (for referencessee Hillered et al., 2005). Since AA is an important substratefor ROS production that may trigger additional membrane
degradation, MD-glycerol has also been implicated as a bio-marker of oxidative stress (Clausen et al., 2005; Lewenand Hillered, 1998). The strong correlation between MD-8-iso-PGF2a and MD-glycerol in this study supports the close rela-tionship between membrane PL degradation and oxidativestress in the human brain following TBI. The finding thatabout 70% of the MD-glycerol signal is related to oxidativestress (as indicated by the factor of dependency and the as-sumption that 8-iso-PGF2a is a specific marker for oxidativestress) supports the experimental TBI studies implicatingMD-glycerol as a biomarker of oxidative stress (Lewen andHillered, 1998; Merenda et al., 2008). Taken together, ourresults suggest that MD-8-iso-PGF2a, together with MD-glycerol, may prove to be clinically useful as markers ofoxidative stress, once a bedside analytical method for 8-iso-PGF2a becomes available.
MD-glutamate is widely used as a marker of excitotoxicity inthe neuro-ICU setting, and can be readily analyzed at thebedside with MD analyzers. We found a significant correlationbetween MD-8-iso-PGF2a and MD-glutamate in this study.This correlation probably reflects the well-known causal rela-tionship between the intracellular accumulation of Ca2 +
caused by glutamate receptor overactivation, leading to phos-pholipase activation, and membrane phospholipase degrada-tion, as revealed by numerous experimental TBI studies (forreferences see Hillered et al., 2005). To our knowledge, this isthe first direct demonstration of this relationship in the humanbrain following TBI. Our finding that about 40% of the MD-glutamate signal is related to oxidative stress (as indicated bythe factor of dependency and the assumption that 8-iso-PGF2a
is a specific marker for oxidative stress) is intriguing, and mayreflect another potentially important link between oxidativestress and excitotoxicity via the microglial antiporter systemXc
2 (Sato et al., 2002), releasing cytotoxic levels of glutamateinto the interstitial compartment to replenish intracellularcystine to maintain the glutathione system when challenged byoxidative stress (Qin et al., 2006).
Although there were marked inter-individual differencesin 8-iso-PGF2a levels, there was a difference between patientswith focal and diffuse brain injury, although this was notstatistically significant. We observed that 8-iso-PGF2a levelsappeared to be lower in focal compared to diffuse TBI, war-ranting further study.
28 40 52 64 76 88
Time after injury (h)
0
20
40
60
80
100
120
140
160
180
200
220
240
260
MD
-Glu
tam
ate
and
MD
-Gly
cero
l (µ
M)
0
1000
2000
3000
4000
5000
6000
7000
MD
-8-i
so-P
GF
2a (
pM
)
Isoprostane Glutamate Glycerol
Patient 2 Patient 4A B
32 44 56 68 80 92 104 106 118
Time after injury (h)
-200
20406080
100120140160180200220240260
MD
-Glu
tam
ate
and
MD
-Gly
cero
l (µ
M)
0
200
400
600
800
1000
1200
1400
1600
1800
2000
MD
-iso
-8-P
GF
2a (
pM
)
Isoprostane Glutamate Glycerol
FIG. 4. Illustrative cases. (A) Glutamate, glycerol, and 8-iso-PGF2a concentrations in brain interstitial fluid using micro-dialysis (MD) from patient 2, who had a predominantly diffuse TBI. (B) Glutamate, glycerol, and 8-iso-PGF2a concentrationsin brain interstitial fluid using MD from patient 4, who had a predominantly focal TBI (8-iso-PGF2a, F2-isoprostane 8-iso-prostaglandin F2a; TBI, traumatic brain injury).
772 CLAUSEN ET AL.

Methodological considerations and limitations
Admittedly, since this is a small feasibility study includingonly six patients, the results need to be confirmed in a largerseries of patients. However, despite the small number of pa-tients, our findings are novel, significant, and important in thecontext of translation of our knowledge of secondary injurymechanisms in animal models of TBI to human patients in theneuro-ICU setting.
Similarly to other clinical TBI studies, we were unable topresent any data from non-injured controls for comparisonbecause of the invasiveness of the methodology. In futurestudies, reference data may be obtained from patients withinfratentorial conditions requiring invasive ICP monitoring.
We plan to perform in vivo recovery experiments in theneuro-ICU employing the extrapolation-to-no-flow ratemethod ( Jacobson et al., 1985).
There has been some controversy regarding the specificityof 8-iso-PGF2a as a marker of oxidative stress because ofpossible enzymatic production of 8-iso-PGF2a by cycloox-ygenase (COX). This was based on data from Pratico andassociates, who found that in vitro COX inhibition of humanplatelets reduced the amount of 8-iso-PGF2a in culture media(Pratico et al., 1995). However, this has been refuted in severalother in vivo studies (Bachi et al., 1997; Belton et al., 2000;Pratico et al., 1998).
Even though the sensitivity of the assay is good on low pg/mL levels (the detection limit was 8 pg/mL; Basu, 1998), ourinitial pilot experiments showed that we needed to pool MDsamples to obtain the volume needed to analyze 8-iso-PGF2a.This is because of the routine measurement of other MD bio-markers (glucose, lactate, pyruvate, glutamate, glycerol, andurea), leaving a small remaining hourly sample for the iso-prostane assay. We therefore decided on a feasibility studydesign with pooling of 12 hourly MD fractions to be on the safeside (allowing for repeated analyses if needed), resulting inpoor temporal resolution. An optimized study design allowsfor quantification of 8-iso-PGF2a in MD fluid with a temporalresolution of 2 h in our follow-up study, which we believe isrelevant for this biomarker in the neurointensive care setting.
The implantation of an MD probe/catheter causes a briefrise in metabolite levels, including glutamate and lactate.However, our own and other studies have shown that thiseffect dissipates after less than an hour (Hillered et al., 1990;Nilsson et al., 1990; Sumbria et al., 2010), suggesting that itshould have no impact on our data with MD sampling com-mencing ‡ 2 h following implantation.
The data shed light on the interpretation of MD biomarkerscurrently used extensively in neuro-ICU settings around theworld. The data supporting MD-glycerol as a useful marker ofoxidative stress appear particularly intriguing. Thus, MD-8-iso-PGF2a and MD-glycerol in combination may prove to beuseful as biomarkers of oxidative stress in the neuro-ICUsetting, both as monitoring tools and as surrogate end-pointsin neuroprotective drug development.
Conclusions
This study demonstrates the feasibility of analyzing 8-iso-PGF2a in MD samples from the human brain following TBI.The highest concentrations of 8-iso-PGF2a were found in MDsamples, compared to vCSF and blood, suggesting that theinterstitial compartment is the preferred site for harvesting
this biomarker. Our results support a close relationship be-tween excitotoxicity and oxidative stress following humanTBI, and that MD-8-iso-PGF2a in combination with MD-glycerol may be useful biomarkers of oxidative stress in theneuro-ICU setting.
Acknowledgments
The authors would like to thank Mrs. Inger Stahl-Myllyahoand Eva Sejby for analyzing the samples, and Dr. Lars Ber-glund for statistical consultation.
This study was supported by the Swedish Research Coun-cil, the Swedish Brain Foundation, Uppsala University Hos-pital, the Selander Foundation, and the Ahlen Foundation.
Author Disclosure Statement
No competing financial interests exist.
References
Awad, J.A., Morrow, J.D., Takahashi, K., and Roberts, L.J.,2nd (1993). Identification of non-cyclooxygenase-derivedprostanoid (F2-isoprostane) metabolites in human urine andplasma. J. Biol. Chem. 268, 4161–4169.
Bachi, A., Brambilla, R., Fanelli, R., Bianchi, R., Zuccato, E.,and Chiabrando, C. (1997). Reduction of urinary 8-epi-prostaglandin F2 alpha during cyclo-oxygenase inhibition inrats but not in man. Br. J. Pharmacol. 121, 1770–1774.
Basu, S. (2008). F2-isoprostanes in human health and diseases:from molecular mechanisms to clinical implications. Antioxid.Redox. Signal 1, 1405–1434.
Basu, S., Nozari, A., Liu, X.L., Rubertsson, S., and Wiklund, L.(2000). Development of a novel biomarker of free radicaldamage in reperfusion injury after cardiac arrest. FEBS Lett.470, 1–6.
Basu, S. (1998). Radioimmunoassay of 8-iso-prostaglandinF2alpha: an index for oxidative injury via free radical cata-lysed lipid peroxidation. Prostaglandins Leukot. Essent. FattyAcids 58, 319–325.
Bayir, H., and Kagan, V.E. (2008). Bench-to-bedside review:Mitochondrial injury, oxidative stress and apoptosis—there isnothing more practical than a good theory. Crit. Care. 12, 206.
Bayir, H., Kagan, V.E., Tyurina, Y.Y., Tyurin, V., Ruppel, R.A.,Adelson, P.D., Graham, S.H., Janesko, K., Clark, R.S., and Ko-chanek, P.M. (2002). Assessment of antioxidant reserves andoxidative stress in cerebrospinal fluid after severe traumaticbrain injury in infants and children. Pediatr. Res. 51, 571–578.
Bayir, H., Marion, D.W., Puccio, A.M., Wisniewski, S.R., Ja-nesko, K.L., Clark, R.S., and Kochanek, P.M. (2004). Markedgender effect on lipid peroxidation after severe traumaticbrain injury in adult patients. J. Neurotrauma. 21, 1–8.
Belton, O., Byrne, D., Kearney, D., Leahy, A., and Fitzgerald, D.J.(2000). Cyclooxygenase-1 and -2-dependent prostacyclinformation in patients with atherosclerosis. Circulation 102,840–845.
Clausen, F., Marklund, N., Lewen, A., and Hillered, L. (2008).The nitrone free radical scavenger NXY-059 is neuroprotectivewhen administered after traumatic brain injury in the rat.J. Neurotrauma 25, 1449–1457.
Clausen, T., Alves, O.L., Reinert, M., Doppenberg, E., Zauner,A., and Bullock, R. (2005). Association between elevated braintissue glycerol levels and poor outcome following severetraumatic brain injury. J. Neurosurg. 103, 233–238.
Elf, K., Nilsson, P., and Enblad, P. (2002). Outcome after trau-matic brain injury improved by an organized secondary insult
ISOPROSTANE AS A BIOMARKER FOR OXIDATIVE STRESS 773

program and standardized neurointensive care. Crit. CareMed. 30, 2129–2134.
Fiskum, G., Murphy, A.N., and Beal, M.F. (1999). Mitochondriain neurodegeneration: acute ischemia and chronic neuro-degenerative diseases. J. Cereb. Blood Flow Metab. 19, 351–369.
Freeman, B.A., and Crapo, J.D. (1982). Biology of disease: freeradicals and tissue injury. Lab. Invest. 47, 412–426.
Goodman, J.C., and Robertson, C.S. (2009). Microdialysis: is itready for prime time? Curr. Opin. Crit. Care. 15, 110–117.
Hall, E.D. (1993). The role of oxygen radicals in traumatic injury:clinical implications. J. Emerg. Med. 11 Suppl. 1, 31–36.
Hall, E.D., Vaishnav, R.A., and Mustafa, A.G. (2010). Anti-oxidant therapies for traumatic brain injury. Neurotherapeutics7, 51–61.
Halliwell, B. (2006). Oxidative stress and neurodegeneration:where are we now? J. Neurochem. 97, 1634–1658.
Hillered, L., Persson, L., Nilsson, P., Ronne-Engstrom, E., andEnblad, P. (2006). Continuous monitoring of cerebral metab-olism in traumatic brain injury: a focus on cerebral micro-dialysis. Curr. Opin. Crit. Care 12, 112–118.
Hillered, L., Persson, L., Ponten, U., and Ungerstedt, U. (1990).Neurometabolic monitoring of the ischaemic human brainusing microdialysis. Acta Neurochir. (Wien.) 102, 91–97.
Hillered, L., Vespa, P.M., and Hovda, D.A. (2005). Translationalneurochemical research in acute human brain injury: thecurrent status and potential future for cerebral microdialysis.J. Neurotrauma 22, 3–41.
Hillman, J., Aneman, O., Anderson, C., Sjogren, F., Saberg, C.,and Mellergard, P. (2005). A microdialysis technique for rou-tine measurement of macromolecules in the injured humanbrain. Neurosurgery. 56, 1264–1268; discussion 1268–1270.
Hutchinson, P.J., O’Connell, M.T., Nortje, J., Smith, P., Al-Rawi,P.G., Gupta, A.K., Menon, D.K., and Pickard, J.D. (2005).Cerebral microdialysis methodology—evaluation of 20 kDaand 100 kDa catheters. Physiol. Meas. 26, 423–428.
Idris, A.H., Roberts, L.J., 2nd, Caruso, L., Showstark, M., Layon,A.J., Becker, L.B., Vanden Hoek, T., and Gabrielli, A. (2005).Oxidant injury occurs rapidly after cardiac arrest, cardiopul-monary resuscitation, and reperfusion. Crit. Care Med. 33,2043–2048.
Jacobson, I., Sandberg, M., and Hamberger, A. (1985). Masstransfer in brain dialysis devices—a new method for theestimation of extracellular amino acids concentration. J. Neu-rosci. Methods 15, 263–268.
Jennett, B., Snoek, J., Bond, M.R., and Brooks, N. (1981). Dis-ability after severe head injury: observations on the use of theGlasgow Outcome Scale. J. Neurol. Neurosurg. Psychiatry 44,285–293.
Kontos, H.A., and Wei, E.P. (1986). Superoxide production inexperimental brain injury. J. Neurosurg. 64, 803–807.
Lewen, A., and Hillered, L. (1998). Involvement of reactiveoxygen species in membrane phospholipid breakdown andenergy perturbation after traumatic brain injury in the rat.J. Neurotrauma 15, 521–530.
Lewen, A., Matz, P., and Chan, P.H. (2000). Free radical path-ways in CNS injury. J. Neurotrauma 17, 871–890.
Liu, M.C., Akinyi, L., Scharf, D., Mo, J., Larner, S.F., Muller, U.,Oli, M.W., Zheng, W., Kobeissy, F., Papa, L., Lu, X.C., Dave,J.R., Tortella, F.C., Hayes, R.L., and Wang, K.K. (2010). Ubi-quitin C-terminal hydrolase-L1 as a biomarker for ischemic andtraumatic brain injury in rats. Eur. J. Neurosci. 31, 722–732.
Marklund, N., Blennow, K., Zetterberg, H., Ronne-Engstrom, E.,Enblad, P., and Hillered, L. (2009). Monitoring of brain inter-
stitial total tau and beta amyloid proteins by microdialysis inpatients with traumatic brain injury. J. Neurosurg. 110, 1227–1237.
Marklund, N., Clausen, F., Lewander, T., and Hillered, L.(2001a). Monitoring of reactive oxygen species productionafter traumatic brain injury in rats with microdialysis and the4-hydroxybenzoic acid trapping method. J. Neurotrauma 18,1217–1227.
Marklund, N., Clausen, F., McIntosh, T.K., and Hillered, L.(2001b). Free radical scavenger posttreatment improves func-tional and morphological outcome after fluid percussion in-jury in the rat. J. Neurotrauma 18, 821–832.
Marklund, N., Salci, K., Lewen, A., and Hillered, L. (1997).Glycerol as a marker for post-traumatic membrane phospho-lipid degradation in rat brain. Neuroreport 8, 1457–1461.
Marshall, L.F., Marshall, S.B., Klauber, M.R., Van Berkum Clark,M., Eisenberg, H., Jane, J.A., Luerssen, T.G., Marmarou, A.,and Foulkes, M.A. (1992). The diagnosis of head injury re-quires a classification based on computed axial tomography.J. Neurotrauma 9 Suppl. 1, S287–S292.
Merenda, A., Gugliotta, M., Holloway, R., Levasseur, J.E.,Alessandri, B., Sun, D., and Bullock, M.R. (2008). Validation ofbrain extracellular glycerol as an indicator of cellular mem-brane damage due to free radical activity after traumatic braininjury. J. Neurotrauma 25, 527–537.
Morrow, J.D., Awad, J.A., Kato, T., Takahashi, K., Badr, K.F.,Roberts, L.J., 2nd, and Burk, R.F. (1992). Formation of novelnon-cyclooxygenase-derived prostanoids (F2-isoprostanes) incarbon tetrachloride hepatotoxicity. An animal model of lipidperoxidation. J. Clin. Invest. 90, 2502–2507.
Morrow, J.D., Hill, K.E., Burk, R.F., Nammour, T.M., Badr, K.F.,and Roberts, L.J., 2nd (1990). A series of prostaglandin F2-likecompounds are produced in vivo in humans by a non-cyclooxygenase, free radical-catalyzed mechanism. Proc. Natl.Acad. Sci. USA 87, 9383–9387.
Nguyen, N.H., Gonzalez, S.V., and Hassel, B. (2007). Formationof glycerol from glucose in rat brain and cultured brain cells.Augmentation with kainate or ischemia. J. Neurochem. 101,1694–1700.
Nilsson, P., Hillered, L., Ponten, U., and Ungerstedt, U. (1990).Changes in cortical extracellular levels of energy-related me-tabolites and amino acids following concussive brain injury inrats. J. Cereb. Blood Flow Metab. 10, 631–637.
Pratico, D., Barry, O.P., Lawson, J.A., Adiyaman, M., Hwang,S.W., Khanapure, S.P., Iuliano, L., Rokach, J., and FitzGerald,G.A. (1998). IPF2alpha-I: an index of lipid peroxidation inhumans. Proc. Natl. Acad. Sci. USA 95, 3449–3454.
Pratico, D., Lawson, J.A., and FitzGerald, G.A. (1995). Cycloox-ygenase-dependent formation of the isoprostane, 8-epi pros-taglandin F2 alpha. J. Biol. Chem. 270, 9800–9808.
Qin, S., Colin, C., Hinners, I., Gervais, A., Cheret, C., and Mallat,M. (2006). System Xc- and apolipoprotein E expressed bymicroglia have opposite effects on the neurotoxicity of amy-loid-beta peptide 1–40. J. Neurosci. 26, 3345–3356.
Reinstrup, P., Stahl, N., Mellergard, P., Uski, T., Ungerstedt, U.,and Nordstrom, C.H. (2000). Intracerebral microdialysis inclinical practice: baseline values for chemical markers duringwakefulness, anesthesia, and neurosurgery. Neurosurgery 47,701–709; discussion 709–710.
Ronne-Engstrom, E., Cesarini, K.G., Enblad, P., Hesselager, G.,Marklund, N., Nilsson, P., Salci, K., Persson, L., and Hillered,L. (2001). Intracerebral microdialysis in neurointensive care:the use of urea as an endogenous reference compound.J. Neurosurg. 94, 397–402.
774 CLAUSEN ET AL.

Roof, R.L., Hoffman, S.W., and Stein, D.G. (1997). Progesteroneprotects against lipid peroxidation following traumatic braininjury in rats. Mol. Chem. Neuropathol. 31, 1–11.
Sato, H., Tamba, M., Okuno, S., Sato, K., Keino-Masu, K., Masu,M., and Bannai, S. (2002). Distribution of cystine/glutamateexchange transporter, system x(c)-, in the mouse brain.J. Neurosci. 22, 8028–8033.
Schulz, J.B., Henshaw, D.R., Siwek, D., Jenkins, B.G., Ferrante,R.J., Cipolloni, P.B., Kowall, N.W., Rosen, B.R., and Beal, M.F.(1995). Involvement of free radicals in excitotoxicity in vivo.J. Neurochem. 64, 2239–2247.
Schulz, M.K., Wang, L.P., Tange, M., and Bjerre, P. (2000). Cer-ebral microdialysis monitoring: determination of normal andischemic cerebral metabolisms in patients with aneurysmalsubarachnoid hemorrhage. J. Neurosurg. 93, 808–814.
Servadei, F., Murray G.D., Penny, K., Teasdale, G.M., Dearden,M., Iannotti, F., Lapierre, F., Maas, A.J., Karimi, A., Ohman, J.,Persson, L., Stocchetti, N., Trojanowski, T., and Underberg, A.(2000). The value of the ‘‘worst’’ computed tomography scanin clinical studies of moderate and severe head injury. Eur-opean Brain Injury Consortium. Neurosurgery 46, 70–75.
Shohami, E., Beit-Yannai, E., Horowitz, M., and Kohen, R.(1997). Oxidative stress in closed-head injury: brain antioxi-dant capacity as an indicator of functional outcome. J. Cereb.Blood Flow Metab. 17, 1007–1019.
Sjogren, P., Basu, S., Rosell, M., Silveira, A., de Faire, U., Vessby,B., Hamsten, A., Hellenius, M.L., and Fisher, R.M. (2005).Measures of oxidized low-density lipoprotein and oxidativestress are not related and not elevated in otherwise healthymen with the metabolic syndrome. Arterioscler. Thromb.Vasc. Biol. 25, 2580–2586.
Skoglund, K., Enblad, P., and Marklund, N. (2009). Effects of theNeurological Wake-Up Test on intracranial pressure and ce-rebral perfusion pressure in brain-injured patients. Neurocrit.Care 11, 135–142.
Stalhammar, D., Starmark, J.E., Holmgren, E., Eriksson, N.,Nordstrom, C.H., Fedders, O., and Rosander, B. (1988).Assessment of responsiveness in acute cerebral disorders. A
multicentre study on the reaction level scale (RLS 85). ActaNeurochir. (Wien.) 90, 73–80.
Sumbria, R.K., Klein, J., and Bickel, U. (2010). Acute depressionof energy metabolism after microdialysis probe implantationis distinct from ischemia-induced changes in mouse brain.Neurochem Res. 36, 109–116.
Teasdale, G., and Jennett, B. (1974). Assessment of coma andimpaired consciousness. A practical scale. Lancet 2, 81–84.
Tisdall, M.M., and Smith, M. (2006). Cerebral microdialysis: re-search technique or clinical tool. Br. J. Anaesth. 97, 18–25.
Tyurin, V.A., Tyurina, Y.Y., Borisenko, G.G., Sokolova, T.V.,Ritov, V.B., Quinn, P.J., Rose, M., Kochanek, P., Graham,S.H., and Kagan, V.E. (2000). Oxidative stress followingtraumatic brain injury in rats: quantitation of biomarkersand detection of free radical intermediates. J. Neurochem.75, 2178–2189.
Wagner, A.K., Bayir, H., Ren, D., Puccio, A., Zafonte, R.D., andKochanek, P.M. (2004). Relationships between cerebrospinalfluid markers of excitotoxicity, ischemia, and oxidative dam-age after severe TBI: the impact of gender, age, and hypo-thermia. J. Neurotrauma 21, 125–136.
Wiklund, L., Sharma, H.S., and Basu, S. (2005). Circulatory arrestas a model for studies of global ischemic injury and neuro-protection. Ann. NY Acad. Sci. 1053, 205–219.
Zalba, G., Fortuno, A., San Jose, G., Moreno, M.U., Beloqui, O., andDiez, J. (2007). Oxidative stress, endothelial dysfunction andcerebrovascular disease. Cerebrovasc. Dis. 24 Suppl. 1, 24–29.
Address correspondence to:Fredrik Clausen, Ph.D.
Department of NeuroscienceSection of Neurosurgery
Uppsala UniversityEntrance 85, 2nd Floor
Uppsala University Hospital75185 Uppsala, Sweden
E-mail: [email protected]
ISOPROSTANE AS A BIOMARKER FOR OXIDATIVE STRESS 775

![Υψίσυχνος Αερισμός [High Frequency Oscillation (HFO)] · Targets ARDS • Gas Exchange • Lung but also RV PROTECTION . Traumatic Brain Injury (TBI) • Maintain](https://static.fdocument.org/doc/165x107/5e9abd7ece9fb21b0444bac5/f-foe-high-frequency-oscillation-hfo-targets-ards.jpg)