“In vitro” azathioprine-induced changes in peripheral T cell apoptosis and IFN-γ production...
10
“In vitro” azathioprine-induced changes in peripheral T cell apoptosis and IFN- production γ associate with drug response in patients with Crohn's Disease Andrea Cossu a , c , Livia Biancone b , Marta Ascolani b , Francesco Pallone b , Monica Boirivant c , ⁎ a Department of Clinical Sciences, Policlinico Umberto I, University “La Sapienza”, Roma, Italy b GI Unit, Department of Internal Medicine, University “Tor Vergata”, Roma, Italy c Immune-mediated Diseases Section, Department of Infectious, Parasitic and Immune-mediated Diseases, Istituto Superiore di Sanità, Roma, Italy Received 4 April 2012; received in revised form 11 June 2012; accepted 26 June 2012 KEYWORDS Crohn's Disease; Azathioprine; Apoptosis; IFN-γ Abstract Background and aim: The use of the highly effective thiopurines as early therapeutic option in Crohn's Disease (CD) may be discouraged by the long time interval required to obtain clinical efficacy as also by their potential side effects. The development of non‐invasive markers of responsiveness to thiopurines represents a major attempt in the clinical management of CD patients. Azathioprine is able to induce apoptosis of T cells. We studied the effect of thiopurines on “in vitro” T cell apoptosis, IFN-γ and IL-10 production in a group of CD patients with known response to a previous treatment with AZA. Methods: Heparinized blood samples were drawn from 25 CD patients showing or not a previous responsiveness to a conventional azathioprine treatment (n = 17 and n = 8, respectively). CD4 + T cells were stimulated “in vitro” with aCD3/28 mAbs in the presence or absence of azathioprine, 6-mercaptopurine or 6-thioguanine. Apoptosis was assessed using Annexin V staining, and IFN-γ and IL-10 production in cell culture supernatants was evaluated by ELISA. Results: Apoptosis stimulation index (% of apoptotic cells in the presence of thiopurine/% of apoptotic cells in the absence of thiopurine) and IFN-γ stimulation index (IFN-γ production in the presence of thiopurine/IFN-γ production in the absence of thiopurine) were, respectively, significantly lower and higher in non‐responder when compared to responder patients. No variation was observed in IL-10 production. ⁎ Corresponding author. Tel.: + 39 0649902976; fax: + 39 06 49902931. E-mail addresses: [email protected] (A. Cossu), [email protected] (L. Biancone), [email protected] (M. Ascolani), [email protected] (F. Pallone), [email protected] (M. Boirivant). 1873-9946/$ - see front matter © 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.crohns.2012.06.020 Available online at www.sciencedirect.com Journal of Crohn's and Colitis (2013) 7, 441–450
Transcript of “In vitro” azathioprine-induced changes in peripheral T cell apoptosis and IFN-γ production...

Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Journal of Crohn's and Colitis (2013) 7, 441–450
“In vitro” azathioprine-induced changesin peripheral T cell apoptosis and IFN-production
γassociate with drug response
in patients with Crohn's Disease
Andrea Cossu a, c, Livia Biancone b, Marta Ascolani b,Francesco Pallone b, Monica Boirivant c,⁎
a Department of Clinical Sciences, Policlinico Umberto I, University “La Sapienza”, Roma, Italyb GI Unit, Department of Internal Medicine, University “Tor Vergata”, Roma, Italyc Immune-mediated Diseases Section, Department of Infectious, Parasitic and Immune-mediated Diseases,Istituto Superiore di Sanità, Roma, Italy
Received 4 April 2012; received in revised form 11 June 2012; accepted 26 June 2012
⁎ Corresponding author. Tel.: +39 06E-mail addresses: andrea.cossu3@t
[email protected] (F. Pallone)
1873-9946/$ - see front matter © 2012doi:10.1016/j.crohns.2012.06.020
KEYWORDSCrohn's Disease;Azathioprine;Apoptosis;IFN-γ
Abstract
Background and aim: The use of the highly effective thiopurines as early therapeutic optionin Crohn's Disease (CD) may be discouraged by the long time interval required to obtain clinicalefficacy as also by their potential side effects. The development of non‐invasive markers ofresponsiveness to thiopurines represents a major attempt in the clinical management of CD
patients. Azathioprine is able to induce apoptosis of T cells. We studied the effect of thiopurineson “in vitro” T cell apoptosis, IFN-γ and IL-10 production in a group of CD patients with knownresponse to a previous treatment with AZA.Methods: Heparinized blood samples were drawn from 25 CD patients showing or not a previousresponsiveness to a conventional azathioprine treatment (n=17 and n=8, respectively). CD4+ Tcells were stimulated “in vitro” with aCD3/28 mAbs in the presence or absence of azathioprine,6-mercaptopurine or 6-thioguanine. Apoptosis was assessed using Annexin V staining, and IFN-γand IL-10 production in cell culture supernatants was evaluated by ELISA.Results: Apoptosis stimulation index (% of apoptotic cells in the presence of thiopurine/% ofapoptotic cells in the absence of thiopurine) and IFN-γ stimulation index (IFN-γ production inthe presence of thiopurine/IFN-γ production in the absence of thiopurine) were, respectively,significantly lower and higher in non‐responder when compared to responder patients. No variationwas observed in IL-10 production.49902976; fax: +39 06 49902931.in.it (A. Cossu), [email protected] (L. Biancone), [email protected] (M. Ascolani),, [email protected] (M. Boirivant).
European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.

442 A. Cossu et al.
Conclusions: Evaluation of apoptosis and IFN-γ stimulation index of peripheral CD4+ T cell may beuseful for a proper selection of CD patients candidate to thiopurine treatment.© 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.
1. Introduction
Azathioprine (AZA) and mercaptopurine (MP) are establishedimmunomodulatory drugs successfully used in inflammatorybowel disease (IBD).1 Induction of remission in active CD byusing AZA requires a long period of time (from 3 to 6 months),since the response rate increases after 17 weeks.2 Indepen-dent studies indeed support that treatment with thiopurinesfor ≤17 weeks does not induce a statistically significantbenefit for inducing remission in active CD.3 These drugs havea proven steroid-sparing effect2 and efficacy in perianal CD.4
Thiopurines also showed more efficacy than placebo formaintaining remission in CD.5 More recently, AZA and MPshowed to be more effective than placebo6 or mesalazine7 inpreventing both clinical and endoscopic postoperative recur-rence in CD. However, in both studies thiopurine use wasassociated with a higher rate of adverse events leading todrug withdrawal.6,7 Up to 20% of IBD patients treated withthiopurines indeed discontinue treatment due to potentiallysevere adverse events related to either dose-dependent phar-macologically induced events or dose-independent, hypersen-sitivity reactions.8 Therefore, although AZA and MP showproven efficacy in IBD, the relatively long term treatmentrequired to obtain a full pharmacological effect together withrelatively frequent adverse reactions, reduces their use asan early therapeutic option. The possibility to predict theirefficacy in each single patient might encourage a moreaggressive strategy with an early use of these immunomodu-latory drugs in subgroups of patients with a more aggressiveIBD course.9,10 The monitoring of 6-thioguanine nucleotide(6-TGN) and 6-methylmercaptopurine (6-MMP) metaboliteshas been proposed for the evaluation of clinical efficacy.11
However, a relatively low sensitivity in predicting clinicalresponse has been shown in a meta-analysis12 and a recentprospective multicenter study including steroid-resistant/dependent IBD patients did not support that assessing 6-TGNlevel may predict treatment outcome.13 Recently, it has beendemonstrated that the immunosuppressive effects of AZA arerelated to its ability to induce apoptosis of T cells14 which, inCD, is defective.15 Consequently, more recently, the evalua-tion of 6-thioguanosine triphosphate levels directly responsi-ble for the proapoptotic effect, as well as of its precursor,6-thioguanoside diphosphate, has been proposed for predict-ing AZA responsiveness in IBD patients.16 However, the mon-itoring ofmetabolites implies the assumption of the drug for anadequate length of time and, therefore, the exposure to therisk of potential adverse effects.
Aim of the present study was to analyse the “in vitro”thiopurine-induced effects on peripheral T cell apoptosisand IFN-γ production in a group of CD patients with knownresponse to a previous treatment with AZA. For this purpose,the effect of thiopurines on “in vitro” T cell apoptosis andIFN-γ production was investigated and results analyzedaccording to previous clinical response to these drugs.
2. Methods
2.1. Patients
In a retrospective study, clinical records of all CD patientswith a previous treatment with AZA and under regular followup at the tertiary IBD referral center of the University of TorVergata of Rome (Italy) were reviewed. Clinical details ofeach patient were prospectively recorded in clinical recordsat each visit. Inclusion criteria included: 1) Diagnosis ofCD according to current guidelines17; 2) Age N18 years; 3)Regular follow up at the time of the study; 4) Previoustreatment with AZA at a standard dosage (2–2.5 mg/kg)according to clinical indication based on current guide-lines.17 Exclusion criteria include: 1) No reliable data onclinical response to AZA; 2) AZA treatment b6 months. AZAresponsiveness was defined as steroid-free clinical remission(CDAI b150) and/or at least 50% fistula closure for at least1 month.
2.2. Blood sampling
Heparinized peripheral blood samples (20 cm3) were obtainedfrom 25 compliant CD patients during a scheduled follow upvisit. At the time of blood collection, the clinical characteristicsof patients (CD localization, disease activity, drug treatments,and time interval from the last thiopurine treatment) wererecorded. Blood samples were processed according to thereported protocol below. Investigators were blind to thepatients' clinical data during all the experimental procedure.
Peripheral blood mononuclear cells (PBMC) were isolatedusing Ficoll–Paque (Pharmacia Biotech, Uppsala, Sweden)density gradient. Purified CD4+ T cells were obtained fromPBMC by immunomagnetic negative selection using CD4+ Tcell isolation Kit II (Miltenyi Biotec, Auburn, CA, USA). Theresulting (unbound) CD4+ T cell population contained greaterthan 96% CD4+ cells as assessed by flow cytometric analysis.
2.3. Cell cultures
CD4+ T cells (1×106) were resuspended in 1 ml of completemedium (RPMI 1640 supplemented with 2 mM L-glutamine,100 U/ml of penicillin, 50 μg/ml of streptomycin, 25 μg/mlof gentamycin and 10% heat-inactivated FCS) and culturedfor 4–5 days in 24-well plates in a humidified 5% CO2
incubator in the presence of recombinant IL-2 (20 U/ml;Roche Diagnostic, Indianapolis, IN, USA). Cells were culturedeither in the absence of any stimulus or in the presence ofplate-bound anti-CD3 Ab (0.04 μg/ml; BD Biosciences Phar-mingen, San Diego, CA, USA) and soluble anti-CD28 (1 μg/ml;BD Biosciences Pharmingen), in the presence or absence ofAZA, 6-mercaptopurine (6-MP) or 6-thioguanine (6-TG) (allfrom Sigma-Aldrich) used at 5 μM concentration, for 4–5 days.

443T cells and azathioprine response
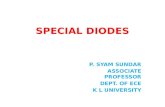
In few experiments, in additional cultures, cells were in-cubated with AZA 10 μM. At the end of the culture period,supernatants were collected and stored at −20 °C for furtheranalysis and cells were collected for apoptosis evaluation.Apoptosis was assessed using Annexin V staining (BD Bio-sciences Pharmingen, San Diego, CA, USA), analyzed byFACScan cytofluorimeter and expressed as % of early apoptoticcells (Annexin V positive cells)+ late apoptotic cells (Annexin Vpositive/PI positive cells) (Fig. 1). The degree of apoptosisinduction was expressed as apoptosis stimulation index usingthe following formula: % apoptotic cells cultured in thepresence of AZA/% of apoptotic cells cultured in the absenceof AZA.
2.4. Cytokine measurement
The amount of IFN-γ and IL-10 in cell culture supernatantswas measured by ELISA using commercially available kits (BDBiosciences Pharmingen, San Diego, California, USA) follow-ing the manufacturer's instructions. The variation of IFN-γ andIL-10 production was expressed as IFN-γ or IL-10 stimulationindex using the following formula: cytokine production byCD4+ T cells cultured in the presence of AZA/cytokine pro-duction by CD4+ T cells cultured in the absence of AZA.
2.5. Statistical analysis
Mann–Whitney and Wilcoxon tests were used as appropriate.Results were analyzed in relation to clinical responsivenessto a previous treatment with AZA.
3. Results
3.1. Patients
Clinical characteristics of the 25 CD patients consideredin the analysis, including indication and responsivenessto AZA treatment are summarized in Table 1. All patientshad a previous treatment with AZA (2 mg/kg) for at least
Figure 1 Flow cytometry dot plot of a representative responder CDof plate-bound anti-CD3 Ab and soluble anti-CD28 in the presencecollected for apoptosis evaluation. Apoptosis was assessed usingexpressed as % of early apoptotic cells (Annexin V positive cells)+ la
6 months. Adverse events requiring drug discontinuationafter N6 months were observed in 3/25 (12%) patients (2lymphopenia, 1 Epstein–Barr virus hepatitis). AZA respon-siveness was observed in 17 out of 25 (68%) patients.
3.2. Apoptosis evaluation
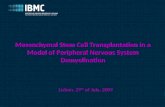
In initial experiments, we evaluated the apoptosis inducedby AZA, MP and 6TG on unstimulated and aCD3/CD28stimulated CD4+ T cells. As expected,14 unstimulated cellsco-incubated with the drugs showed level of apoptosiscomparable to that observed in unstimulated untreatedcells. Furthermore, no difference was observed among AZA,MP and 6TG. Differently, AZA was able to increase the % ofapoptotic cells detectable in CD4+ T cells stimulated withaCD3/28 mAb and the apoptosis induction by AZA, MP and6TG was comparable (Fig. 2).
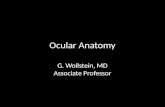
Fig. 3A shows the % of apoptosis observable afterstimulation with aCD3/aCD28 alone or in the presence ofAZA in CD patients according to AZA responsiveness. The % ofapoptosis after aCD3/aCD28 stimulation was not differentbetween responder (R) patients and non‐responder patients(NR) [R: 18.8% (8.1–38.8); NR: 19.07% (15.6–58.3) median(range) p=0.39 by Mann–Whitney test]. R patients showed asignificant increase in the % of apoptotic cells after aCD3/aCD28 stimulation in the presence of AZA. Comparableresults were obtained with aCD3/28 stimulation in thepresence of MP and 6TG (data not shown).
In order to quantify the ability of AZA to increase theapoptosis observable after aCD3/aCD28 stimulation, weconveyed the data as apoptosis stimulation index. As shownin Fig. 3B, NR patients showed a significant reduced ap-optosis stimulation index when compared to R patients [NR:1.21 (0.90–1.65); R: 1.75 (1.20–2.65) median (range) p=0.002 by Mann–Whitney test]. In 2 NR patients, apoptosiswas evaluated after incubation of lymphocytes with AZA10 μM also. In both cases, the % of apoptosis observed wasnot different from the one observed in cultures containingAZA 5 μM (data not shown). It is interesting to note that inthe NR group we observed the highest values of apoptosis
patient. Peripheral CD4+ T cells were cultured in the presenceor absence of AZA. At the end of 5 days cultured cells were
Annexin V staining, analyzed by FACScan cytofluorimeter andte apoptotic cells (Annexin V positive/PI positive cells).

Table 1 Clinical characteristics of patients with Crohn'sDisease.
Responderpatients(n=17)
Non‐responderpatients(n=8)
p
M/F 10/7 1/7Age (y) 0.03Mean±SD 39±12 52±15Range 16–65 33–71
Disease duration (y) 0.12Mean±SD 15±8 22±11Range 3–29 7–36
Indication for AZA treatmentFistulizing disease(including perianal disease)
2 1 (1)
Steroid-dependence 13 4Steroid dependence andfistulae (perianal disease)
2 (1) 3 (2)
CD localization at time ofAZA treatment(post-operative recurrence)Small bowel 10 (6) 4 (3)Small and large bowel 7 4Concomitant perianaldisease
1 4
CD localization at time ofblood collection(post-operative recurrence)Small bowel 12 (7) 6 (5)Small and large bowel 5 2Concomitant perianaldisease
1 2
CD activity at time of bloodcollectionActive (CDAI N150) 1 4Remission (CDAI ≤150) 16 4
Treatment at time ofblood collectionAZA 5 a 2Mesalazine 12 4Prednisone 1Budesonide 4 2Infliximab b 2 3Adalimumab b 1
Duration of AZA treatment attime of blood collection (mo)Mean±SD 22±18 7±1Range 4–42 6–8
Time interval from the lastAZA treatment and bloodcollection (mo)Mean±SD 26±26 41±35Range 2–84 3–96
In brackets: patients with recurrence or fistulae.
a Responder patients not assuming AZA at time of bloodcollection discontinued the drug due to: stable remission(n=6); low compliance (n=3); adverse events (n=3).b Maintenance treatment.
Figure 2 Azathioprine and its metabolites induce apoptosis inaCD3/28 stimulated T cells. CD4+ T cells were isolated fromperipheral blood of 3 healthy volunteers cultured in thepresence of IL-2 and stimulated or not with antibodies to CD3and CD28 in the presence or absence of azathioprine, 6-MP and6TG. T cell apoptosis was assessed by FACS analysis after 5 daysof cell culture. Columns indicate mean±SE.
444 A. Cossu et al.
and apoptosis stimulation index (apoptosis aCD3/28: 58.29%;aCD3/28 AZA: 96.15%; apoptosis stimulation index: 1.65)in a patient whom indication for AZA treatment includedboth a steroid-dependent CD and recto-vaginal fistula.This patient was classified as NR due to the persistence ofthe recto-vaginal fistula. The 3 responder patients whodeveloped severe side effects using AZA, when tested forapoptosis showed widely distributed apoptosis stimulationindex: 1.87, 1.2 and 2.6
3.3. Cytokine production
We next evaluated the amount of IFN-γ in the supernatantsof cell cultures utilized for apoptosis evaluation. The IFN‐γproduction after aCD3/28 stimulation was not differentbetween R and NR patients [R: 13,200 pg/ml (227–358,000);NR: 874 pg/ml (79–1,000,000) median (range) p=0.30 byMann–Whitney test]. As shown in Fig. 3C, R patients showeda significant decrease in IFN-γ production after aCD3/aCD28stimulation in the presence of AZA and a significant re-duction of the IFN-γ stimulation index when compared to NRpatients [R: 0.18 (0.003–0.48); NR: 0.76 (0.47–1.26) median(range) p=0.0001 by Mann–Whitney test] (Fig. 3D). The 3responder patients who developed severe side effects usingAZA showed the following IFN-γ stimulation index: 0.3, 0.18and 0.003. To investigate whether the effect on IFN-γproduction was the result of a generalized immunosuppres-sive activity of thiopurines we measured IL-10 levels inthe same cell culture supernatants. As shown in Fig. 3E andF, IL-10 production was not affected by incubation withazathioprine.
3.4. Analysis of apoptosis and IFN-γ productionaccording to clinical activity at time of bloodcollection
At time of blood collection, only 1 R patient showed activedisease. In the NR group 4 patients showed active disease.

Figure 3 “In vitro” affect of AZA on peripheral blood CD4+ T lymphocytes in responder or non‐responder patients to AZA treatment(2 mg/kg). Cells, cultured in the presence of IL-2, were stimulated with aCD3/28 mAbs in the presence or in the absence of AZA(see Methods). Panel A: % of apoptotic cells in cell culture of CD4+ T cells in the absence or in the presence of AZA (+AZA);Panel B: apoptosis stimulation index. Panel C: IFN-γ production in cell culture of CD4+ T cells in the absence or in the presenceof AZA (+AZA). Panel D: IFN-γ stimulation index. Panel E: IL-10 production in cell culture of CD4+ T cells in the absence or in thepresence of AZA (+AZA). Panel F: IL-10 stimulation index. R = responder patients, NR = non‐responder patients.
445T cells and azathioprine response
NR patients showing clinical activity did not show differencesin the % of apoptotic cells and IFN-γ production after aCD3/28stimulation when compared to NR patients in clinicalremission [apoptosis: 17.9% (15.6–36.4) vs. 24.3% (18.3–58.3) median (range). IFN-γ production: 112,277 pg/ml(79–1,000,000) vs. 874 pg/ml (600–3051) median (range)]as well as no difference was observable in apoptosis and IFN-γstimulation index [apoptosis stimulation index: 1.17 (0.90–1.46) vs. 1.2 (1.0–1.6); IFN-γ stimulation index: 0.75 (0.5–1.1)vs. 0.96 (0.58–1.26) median (range)].
3.5. Analysis of apoptosis and IFN-γ productionaccording to different treatments at time of bloodcollection
No patient was receiving no medication at time of bloodcollection.
3.5.1. Treatment with azathioprineAt time of blood collection, 5 R patients were assuming AZAalone, while in the NR patients, 2 patients were treated withAZA, one of which was receiving AZA in association withinfliximab for perianal disease. R patients treatedwith AZA didnot show differences in the % of apoptotic cells and IFN-γproduction after aCD3/28 stimulation when compared toR patients not treated with AZA (three patients in this groupwere assuming anti-TNFs andwere excluded from this analysis)[apoptosis: 14.9% (10.8–32.5) vs. 20.2% (13.5–38.8) median(range). IFN-γ production: 40,625 pg/ml (227–225,107) vs.12,668 pg/ml (277–124,000) median (range)] as well as nodifference was observable in apoptosis and IFN-γ stimulationindex (Fig. 4, panel A).
3.5.2. Treatment with 5-ASAAt time of blood collection, 5 R and no NR were treated with5-ASA alone. R patients treated with 5-ASA only did not show

446 A. Cossu et al.
differences in the % of apoptotic cells and IFN-γ productionafter aCD3/28 stimulation, when compared to R patients nottreated with 5-ASA [apoptosis: 26.4% (15.7–38.8) vs. 23.9%(14.9–35.5) median (range)]. IFN-γ production: 6919 pg/ml(277–124,000) vs. 20,000 pg/ml (227–225,100) median(range). No differences were also observed in terms ofapoptosis and IFN-γ stimulation index (Fig. 4, panel B).
3.5.3. Treatment with local and systemic corticosteroidsNo R patient and only 1 NR patient were assumingprednisone at time of blood collection. 4 R and 2 NR patientswere treated with budesonide. R patients treated withbudesonide did not show differences in the % of apoptoticcells and IFN-γ production after aCD3/28 stimulationwhen compared to R patients not treated with budesonide[apoptosis: 17.7 (13.5–26) vs 20.2% (10.8–38.8). median
Figure 4 Apoptosis and IFN-γ stimulation index in R and NR patient
(range). IFN-γ production: 16,600 pg/ml (9335–113,000) vs.12,137 pg/ml (227–225,107) median (range)]. No differencewas also detected in terms of apoptosis and IFN-γ stimula-tion index (Fig. 4, panel C).
3.5.4. Treatment with anti-TNFs3 R patients were treated with anti-TNFs (infliximab n=2;adalimumab n=1) at time of blood collection. In one ofthem, AZA was discontinued due to leucopenia, whilethe remaining 2 patients showing high responsiveness toAZA leading to a long steroid-free remission, subsequentlydiscontinued AZA and were treated with anti-TNFs due toperianal disease (n=1) or arthralgias (n=1). R patientstreated with anti-TNFs did not show differences in the %of apoptotic cells and IFN-γ production after aCD3/28stimulation when compared to R patients not treated with
s analyzed according to the treatment at time of blood collection.

Figure 4 (continued).
447T cells and azathioprine response
anti-TNFs [apoptosis: 19.5% (8.11–35.5) vs. 19.5% (10.8–38.8)median (range); IFN-γ production: 9435 pg/ml (1526–358,000)vs. 13,200 pg/ml (227–225,107) median (range)]. No differ-ences were also observed in terms of apoptosis and IFN-γstimulation index (Fig. 4, panel D).
Three NR patients were treated with anti-TNFs at timeof blood collection. NR patients treated with anti-TNFs didnot show differences in the % of apoptotic cells and IFN-γproduction after aCD3/28 stimulation when compared to NRpatients not treated with anti-TNFs [apoptosis: 18.3% (16.9–29.3) vs. 19.3% (15.6–58.2) median (range); IFN-γ production:874 pg/ml (600–223,922) vs. 1786 pg/ml (79–1,000,000)median (range)]. No differences were also observed in termsof apoptosis and IFN-γ stimulation index (Fig. 4, panel E). Inorder to further analyze the effect of anti-TNFs on the %apoptosis and IFN-γ production, we compared the values ofapoptosis and IFN-γ stimulation index observed in the 3 R and
NR patients treated with anti-TNFs. Although no differencewas observed in IFN-γ production after aCD3/28 stimulation,the values of IFN-γ stimulation index were substantiallydifferent in the two groups (Fig. 4, panel F), thus indicatingthat the treatment at the time of blood collection did notinfluence the “in vitro” response to AZA.
3.6. Impact of previous treatment with AZA
In the present study, analyzed T cells were isolated fromblood of patients with a documented AZA history to enable aclear definition of responder and non-responder patients.However, in this setting it cannot be excluded that previousin vivo AZA therapy still impacted the behavior of isolated Tcells in cell culture and their in vitro response to stimulationand AZA. In order to address this issue we correlated the

448 A. Cossu et al.
time interval between the last AZA treatment and bloodcollection with the apoptosis and IFN-γ stimulation indexof patients not treated with AZA at time of blood collection.As illustrated in Fig. 5, we did not observe a significantcorrelation between the parameters evaluated.
4. Discussion
In the present study we describe the differential ability ofAZA to induce apoptosis of aCD3/28 stimulated peripheralblood CD4+ T cells in CD patients responsive to AZA whencompared to patients not responsive to a previous AZAtreatment. AZA induced a significantly higher degree ofapoptosis in peripheral blood cells from patients withprevious response to AZA, than in cells from patientsshowing no responsiveness to a previous AZA treatment.The degree of “in vitro” responsiveness did not apparentlycorrelate with the development of severe AZA‐related sideeffects, since the values of apoptosis and IFN-γ stimulationindexes of the 3 patients who discontinued the drug due tosevere side effects were widely distributed. The observeddifferent apoptosis responses to AZA were not related to a
Figure 5 Correlation between the time interval between lastazathioprine treatment and blood collection (AZA free-time)and apoptosis (panel A) and IFN-γ (panel B) stimulation index.
different % of apoptosis observable between the two groupsof patients after aCD3/28 stimulation, thus suggesting anintrinsic difference in terms of responsiveness to AZA. As aconsequence of the differential apoptosis observed betweenresponder and non‐responder patients, we observed agreater reduction of IFN-γ content in cultures from respond-er when compared to non‐responder patients. This differ-ence is even more pronounced than the one observed inapoptosis. In fact, in this case, the overlap of IFN-γ stimulationindex between R and NR patients is less pronounced with only1 R patient showing a value comparable to the values observedin NR patients. Reasons for this discrepancy may be inherentin different sensitivities of the two assays. The effect of AZAon IFN-γ production appears to be selective, since IL-10production is not affected. This finding is in agreement with aprevious report showing a preferential dampening of the Th-1response in peripheral blood of CD patients treated with AZA18
and suggests a selective proapoptotic activity of AZA on IFN-γproducing cells. It is interesting to note that in the NR groupwe observed the highest values of apoptosis and apoptosisstimulation index in a patient treated with AZA for steroid-dependent CD and recto-vaginal fistula. This patient wasclassified as NR due to the persistence of the recto-vaginalfistula. At time of blood collection this patient was in clinicalremission (CDAI b150). Whether the remission of luminalsymptoms after AZA treatment may account for the observedhigh apoptosis stimulation index in this patient can be onlyhypothesized.
Factors that may influence the response to thiopurinesinclude the thiopurine methyltransferase (TPMT) activity,which influences the 6-thioguanine nucleotides (6-TGMP,6-TGDP, and the active 6-TGTP) levels. TPMT activity showswide interindividual differences because of common geneticpolymorphisms. However, a very high TPMT activity, which isassociated with pharmacologic resistance to AZA, has beendescribed in 1% of IBD patients while around 90% presenta normal TPMT activity.19 Moreover, we observed similardifferences in the induction of apoptosis between responderand non‐responder patients when CD4+ T cells werestimulated in the presence of 6-TG which is less affectedby TPMT.20 Therefore, it is unlikely that interindividualdifferences in TPMT activity might account for the differ-ence in apoptosis observed in the present study. In our studypopulation, the frequency of both responsiveness (68%) toAZA and of induction of adverse events (12%) by usingAZA was comparable to those reported in the general CDpopulation,17 thus supporting the reliability of our findings.
Several variables, including CD activity and treatment attime of blood collection might have influenced the “in vitro”response to AZA observed in the present study. However,although a higher number of NR patients at time of bloodcollection showed clinical active disease when compared toresponder patients, we did not find differences in bothapoptosis and IFN-γ stimulation index in NR patients groupedaccording to disease activity. Regarding CD treatment attime of blood collection, we did not find any significanttreatment-related difference in the percentage of apoptosisand in the IFN-γ production after aCD3/28 “in vitro” stimulationof T cells aswell as in the “in vitro” AZA-induced effects (Fig. 3).The small number of patients included in the analysis ofsubgroups however does not allow conclusive statements at thisregard. Present observations suggest that it is unlikely that

449T cells and azathioprine response
treatment at the time of blood collectionmight have influencedthe “in vitro” responses to AZA in our study population.
Finally, the lack of correlation observed in the presentstudy between the length of the interval between last AZAtreatment at blood collection with the apoptosis and IFN-γstimulation index suggests that apoptosis, IFN-γ productionand AZA responsiveness of peripheral T cells in patients withCD are not significantly affected by a previous treatmentwith AZA. This suggestion is reinforced by the comparison ofour apoptosis collective values (NR+R) with the values ofapoptosis observed in peripheral blood CD4+ T cells isolatedfrom IBD patients before AZA therapy and stimulated withanti-CD3/CD28 plus IL-2 in the presence or absence of 6-MPfor 5 days reported in a previous study.14 Our values (CD3/28: 23±2%, aCD3/28+AZA: 37±4%, respectively) are compa-rable to the mean values reported in the above cited studysupporting the suggestion that the apoptosis of peripheralT cells in patients with CD is not significantly affected by aprevious treatment with AZA and that in our study previousAZA treatment did not significantly affect our findings. Inconclusion, we observed a differential “in vitro” thiopurine-apoptotic response of peripheral blood CD4+ T cells isolatedfrom CD patients responder or non‐responder to AZA. Thisfeature seems to be independent from the time intervalbetween AZA treatment and blood sampling, being ratherlinked with an individual trait of the inflammation. Onceconfirmed in a large prospective study, present findings suggestthat the evaluation of apoptosis and/or IFN-γ stimulation indexof peripheral CD4+ T cell after incubation with AZA mightrepresent a parameter useful for a proper selection of CDpatients candidate to thiopurine treatment.
Conflict of interests
The authors declare no conflict of interest.
Acknowledgments
This study was funded in full by the Italian Ministry ofHealth, grant number 8ABF/8.
A.C. is a recipient of a scholarship from the PhD course“Fisiopatologia Chirurgica e Gastroenterologia” University“La Sapienza”. Roma, Italy.
Statement of authorship:AC carried out the “in vitro” studies, data analyses and
performed the statistical analysis. LB participated in thedesign of the study, acquired clinical data and revised themanuscript. MA acquired clinical data and contributed thestatistical analysis. FP critically revised the manuscript forimportant intellectual content. MB conceived the study,participated in its design and coordination and wrote themanuscript. All authors critically discussed the results andrevised the manuscript. All authors read and approved thefinal manuscript.
References
1. Fraser AG, Orchard TR, Jewell DP. The efficacy of azathioprinefor the treatment of inflammatory bowel disease: a 30-yearreview. Gut 2002;50:485–9.
2. Prefontaine E, MacDonald JK, Sutherland LR. Azathioprine or6-mercaptopurine for induction of remission in Crohn's disease.Cochrane Database Syst Rev 2010;6:CD000545.
3. Khan KJ, Dubinsky MC, Ford AC, Ullman TA, Talley NJ, Moayyedi P.Efficacy of immunosuppressive therapy for inflammatory boweldisease: a systematic review andmeta-analysis.AmJGastroenterol2011;106:630–42.
4. Rutgeerts P. Review article: treatment of perianal fistulizingCrohn's disease. Aliment Pharmacol Ther 2004;20(Suppl 4):106–10.
5. Prefontaine E, Sutherland LR, MacDonald JK, Cepoiu M.Azathioprine or 6-mercaptopurine for maintenance of remis-sion in Crohn's disease. Cochrane Database Syst Rev 2009;4:CD000067.
6. Peyrin-Biroulet L, Deltenre P, Ardizzone S, D'Haens G, HanauerSB, Herfarth H, et al. Azathioprine and 6-mercaptopurine forthe prevention of postoperative recurrence in Crohn's disease:a meta-analysis. Am J Gastroenterol 2009;104:2089–96.
7. Reinisch W, Angelberger S, Petritsch W, Shonova O, Lukas M,Bar-Meir S, et al. Azathioprine versus mesalazine for preventionof postoperative clinical recurrence in patients with Crohn'sdisease with endoscopic recurrence: efficacy and safety resultsof a randomised, double-blind, double-dummy, multicentretrial. Gut 2010;59:752–9.
8. Present DH, Meltzer SJ, Krumholz MP, Wolke A, Korelitz BI.6-Mercaptopurine in the management of inflammatory boweldisease: short and long-term toxicity. Ann Intern Med 1989;111:641–9.
9. Etchevers MJ, Aceituno M, Sans M. Are we giving azathioprinetoo late? The case for early immunomodulation in inflammatorybowel disease. World J Gastroenterol 2008;14:5512–8.
10. D'Haens G, Baert F, van Assche G, Caenepeel P, Vergauwe P,Tuynman H, et al. Early combined immunosuppression orconventional management in patients with newly diagnosedCrohn's disease: an open randomised trial. Lancet 2008;371:660–7.
11. Wright S, Sanders DS, Lobo AJ, Lennard L. Clinical significanceof azathioprine active metabolite concentrations in inflamma-tory bowel disease. Gut 2004;53:1123–8.
12. Osterman MT, Kundu R, Lichtenstein GR, Lewis JD. Associationof 6-thioguanine nucleotide levels and inflammatory boweldisease activity: a meta-analysis. Gastroenterology 2006;130:1047–53.
13. González-Lama Y, Bermejo F, López-Sanromán A, García-SánchezV, Esteve M, Cabriada JL, et al. Thiopurine methyl-transferaseactivity and azathioprine metabolite concentrations do notpredict clinical outcome in thiopurine-treated inflammatorybowel disease patients. Aliment Pharmacol Ther 2011;34:544–54.
14. Tiede I, Fritz G, Strand S, Poppe D, Dvorsky R, Strand D, et al.CD28-dependent Rac1 activation is the molecular target ofazathioprine in primary human CD4 T lymphocytes. J Clin Invest2003;111:1133–45.
15. Boirivant M, Marini M, Di Felice G, Pronio AM, Montesani C, TersigniR, et al. Lamina propria T cells in Crohn's disease and othergastrointestinal inflammation showdefective CD2 pathway-inducedapoptosis. Gastroenterology 1999;116:557–65.
16. Neurath MF, Kiesslich R, Teichgräber U, Fischer C, Hofmann U,Eichelbaum M, et al. 6-Thioguanosine diphosphate and triphos-phate levels in red blood cells and response to azathioprinetherapy in Crohn's disease. Clin Gastroenterol Hepatol 2005;3:1007–14.
17. Dignass A, Van Assche G, Lindsay JO, Lémann M, Söderholm J,Colombel JF, et al. The second European evidence-basedconsensus on the diagnosis and management of Crohn's disease:current management. J Crohns Colitis 2010;4:28–62.
18. Cuffari C, Li DY, Mahoney J, Barnes Y, Bayless TM. Peripheralblood mononuclear cell DNA 6-thioguanine metabolite levels

450 A. Cossu et al.
correlate with decreased interferon-g production in patientswith Crohn's disease on AZA therapy. Dig Dis Sci 2004;49:133–7.
19. Ansari A, Hassan C, Duley J, Marinaki A, Shobowale-Bakre EM,Seed P, et al. Thiopurine methyltransferase activity and the
use of azathioprine in inflammatory bowel disease. AlimentPharmacol Ther 2002;16:1743–50.
20. Lennard L, Davies HA, Lilleyman JS. Is 6-thioguanine moreappropriate than 6-mercaptopurine for children with acutelymphoblastic leukaemia? Br J Cancer 1993;68:186–90.