Does Extinction distribution determine the offspring distribution in Simple Branching?

How Does TGF-� Mediate Tubulointerstitial Fibrosis?
Leslie Gewin, MD,*,† and Roy Zent, MD, PhD†,‡,§,�
Summary: Tubulointerstitial fibrosis mediates the development of end-stage renal disease from renal injuries ofall etiologies and is considered an important predictor of renal survival. Transforming growth factor-� (TGF-�) isone of the most important growth factors that promotes tubulointerstitial fibrosis, but the mechanisms whereby thisoccurs are not well defined. This is because TGF-� has pleiotropic effects that depend on the target cell type. Thisreview discusses how TGF-� signaling in each of the relevant cell types (eg, tubular epithelium, fibroblasts) maycontribute to tubulointerstitial fibrosis progression and suggests ways in which future research can improve ourunderstanding of TGF-�–mediated tubulointerstitial fibrosis.Semin Nephrol 32:228-235 Published by Elsevier Inc.Keywords: TGF-�, tubulointerstitial fibrosis, extracellular matrix, chronic kidney disease
btr
iT
pftpa
dmni
ir
csocoTutd
Renal fibrosis, characterized by the accumulationof extracellular matrix (ECM), is the final com-mon pathway whereby all renal injuries lead to
end-stage renal disease. Although fibrosis in the kidneycan occur as either tubulointerstitial fibrosis or glomeru-losclerosis, injury to both the tubulointerstitial and glo-merular compartments ultimately results in tubulointer-stitial fibrosis. Exactly how glomerular injury causestubulointerstitial fibrosis is poorly understood, but it iswell established that the best predictor of renal survivalfrom kidney disease of any etiology is tubulointerstitialfibrosis. Fibrosis in the renal tubulointerstitium, similarto fibrosis in all organs, results from increased ECMsynthesis, reduced degradation, or a combination of both.Dysregulation of this equilibrium can occur during tissuerepair as a result of persistent inflammation, increasedreactive oxygen species (ROS) production, changes inprotease levels, as well as altered cell-ECM interactions.These cellular events are regulated at the molecular level
*Department of Research, Veterans Affairs Hospital, Tennessee ValleyHealthcare System, Nashville, TN.
†Division of Nephrology, Department of Medicine, Vanderbilt MedicalCenter, Nashville, TN.
‡Department of Medicine, Veterans Affairs Hospital, Tennessee ValleyHealthcare System, Nashville, TN.
§Cell and Developmental Biology, Vanderbilt Medical Center, Nash-ville, TN.
�Cancer Biology, Vanderbilt Medical Center, Nashville, TN.Financial support: Supported in part by a Veterans Affairs Career
Development Award, Biomedical Laboratory Research and Devel-opment (L.G.); the Vanderbilt Physician Scientist DevelopmentAward (L.G.); National Institutes of Health grants DK065123,DK075594, DK65123, and DK083187 (all to R.Z.); an AHA estab-lished investigator award (R.Z.); a Merit Award from the Depart-ment of Veterans Affairs (R.Z.); and the George O’Brien CenterGrant (R.Z.).
Conflict of interest statement: none.Address reprint requests to Leslie Gewin, Vanderbilt University Med-
ical Center, Room C3210 MCN, 1161 21st Ave. S., Nashville, TN37232-2372. E-mail: [email protected]
0270-9295/ - see front matterPublished by Elsevier Inc.
http://dx.doi.org/10.1016/j.semnephrol.2012.04.001228
y numerous proteins including growth factors. One ofhe most important growth factors that plays a role inenal fibrosis is transforming growth factor-� (TGF-�).
TGF-� has 3 mammalian isoforms (TGF-�1, -�2, and-�3) that are a part of the TGF-� superfamily, which alsoncludes the bone morphogenic proteins and activins.GF-� is secreted in a latent form as a result of nonco-
valent binding to the latency-associated peptide (LAP),and is anchored to the ECM by latent TGF-� bindingroteins (Fig. 1).1 To become active, TGF-� is releasedrom the LAP by numerous mechanisms, including pro-eolytic cleavage (eg, matrix metalloproteinases [MMPs],lasmin), ROS, heat, or through conformational changes induced by thrombospondin and certain integrins.2
Once activated, TGF-� ligands bind to the TGF-� type IIreceptor (T�RII), which phosphorylates the TGF-� typeI receptor, leading to activation of multiple intracellularsignaling pathways.3,4 Canonical TGF-� signaling is me-iated by the Smads, but other downstream proteins (eg,itogen-activated protein kinase, TGF-beta activated ki-
ase) can modulate Smad signaling and exert Smad-ndependent effects.5,6 These complex signaling path-
ways allow TGF-� to regulate multiple cellular eventsnvolved in tissue development, immune function, woundepair, and cancer biology.
A large body of evidence suggests that TGF-� plays aritical role in the pathogenesis of tubulointerstitial fibro-is. The best direct evidence for these effects is thatverexpression of TGF-�1 by renal tubular epithelialells resulted in tubulointerstitial fibrosis in the absencef any injury,7 and, conversely, a blocking antibody toGF-� ameliorated interstitial matrix accumulation afternilateral ureteral obstruction (UUO), a model of severeubulointerstitial fibrosis.8 Despite this compelling evi-ence that TGF-� promotes tubulointerstitial fibrosis, the
mechanism whereby it does so remains unclear. This ispartly owing to the complexity of tubulointerstitial fibro-sis progression, which involves many different cell types:interstitial fibroblasts produce matrix components, in-
flammatory cells generate profibrotic growth factors, andSeminars in Nephrology, Vol 32, No 3, May 2012, pp 228-235

TGF-� and tubulointerstitial fibrosis 229
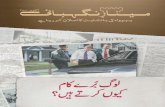
Figure 1. The effects of TGF-� vary depending on target cell type. TGF-� ligands are secreted as mature homodimers noncovalently boundto the LAP. This latent complex is anchored to the ECM by LTBP, and the mature TGF-� homodimer must be separated from the LAP tobecome active and bind to the TGF-� type II receptor. TGF-� has pleiotropic effects that vary depending on the target cell type. Shown arethe different cellular responses to TGF-� by various cell types involved in tubulointerstitial fibrosis (tubular epithelium, renal fibroblast,macrophage, and endothelium). Many of these cellular responses were determined by in vitro studies, and validation of these effects in vivo
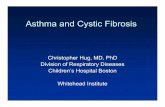
has yet to be confirmed. Abbreviations: CTGF, connective tissue growth factor; LTBP, latent TGF-� binding protein; PAI-1, plasminogenactivator inhibitor-1.Figure 2. Proposed cellular interactions that lead to TGF-�–mediated tubulointerstitial fibrosis. Various forms of injury (eg, mechanical stretch,hypoxia) target the renal tubular epithelium, leading to production of inflammatory cytokines such as monocyte chemoattractant protein-1(MCP-1), which recruits macrophages. The infiltrating macrophages are potent sources of TGF-� that can signal on neighboring epithelial cellsor renal fibroblasts. TGF-� from either macrophages or injured tubular epithelium stimulates fibroblasts to produce matrix components such ascollagen I and fibronectin. The increased TGF-� production by injured epithelium can signal in an autocrine fashion, leading to further TGF-�
production, de-differentiation, and possibly increased collagen IV production. Tubular injury also may increase integrin �v�6 expression andactivation of latent TGF-�.
o
rcT
R
trtiatektbtT
si
tttn
230 L. Gewin and R. Zent
tubular epithelial cells are often the initial target of injury(Fig. 2). The lack of a clearly defined mechanismwhereby TGF-� promotes fibrosis is due to the fact thatTGF-� receptors are expressed ubiquitously and TGF-�has pleiotropic effects that are cell type–specific and varyin different forms of injury. In addition to these factors,the role of TGF-� in renal injury has been studied pri-marily by modulating TGF-� activity through systemicapproaches. This strategy only reveals the aggregate re-sponse of the kidney to TGF-� and does not elucidate themechanism whereby TGF-� increases tubulointerstitialfibrosis. In this review, we outline what is known aboutthe specific effects of TGF-� signaling on the response toinjury by each cell type involved in tubulointerstitialfibrosis (Fig. 1) to define some of the important questionsthat future research should address.
TGF-� SIGNALING AND RENAL FIBROBLASTS
The fibroblast, considered the primary cell responsiblefor matrix synthesis, is thought to be the main mediatorof the profibrotic effects of TGF-�. This perception isbased on several in vitro studies showing increased fi-broblast proliferation and matrix production in responseto TGF-�. Specifically, TGF-� induces a morphologictransformation of human subcutaneous fibroblasts intomyofibroblasts, potent matrix-producing cells, by in-creasing expression of �-smooth muscle actin (�-SMA).9
TGF-� also stimulates fibroblast transcription of collagenI and fibronectin, important components of tubulointer-stitial fibrosis.10,11 In addition, TGF-� signaling in fibro-blasts promotes matrix accumulation by suppressing itsdegradation through down-regulation of certain MMPsand increased expression of tissue inhibitor of MMP.12,13
There are several reasons why validation of these invitro findings with in vivo studies is critical. First, not allfibroblasts respond equally to TGF-�. Thus, studies ondermal fibroblasts may not necessarily predict cellularbehavior of renal fibroblasts. Furthermore, althoughmany early in vitro studies were performed on renalfibroblasts (NRK-49F cell line), heterogeneic responsesto TGF-� by subclones of NRK-49F cells have beenreported.14 Perhaps this is because NRK-49F cells are amixture of cortical and medullary fibroblasts that havemorphologic and perhaps functional differences. Second,the response of cells to TGF-� is determined by the dose;for example, TGF-� can stimulate matrix production inrenal cortical fibroblasts at one dose (0.2 ng/mL) butsuppress collagen secretion at higher amounts (1 ng/mL).15 Whether the concentration of active TGF-� in theinjured renal tubulointerstitium results in fibroblast sup-pression or stimulation of ECM is unclear and an impor-tant reason why in vivo studies are necessary. Finally, theactions of TGF-� are not just cell-specific but also de-pendent on the surrounding microenvironment and canbe modulated by other growth factors and cytokines.16
Because the cell culture milieu is quite different from that d
f the injured kidney, the fibroblast’s response to TGF-�in vitro may poorly predict its actions after injury in vivo.
The intracellular signaling pathways whereby TGF-�mediates its profibrotic effects on renal fibroblasts arealso not well delineated. Both p21-activated kinase-2 andc-Abl kinases have been shown to mediate the prolifer-ative effects of TGF-� on renal fibroblasts but do nothave this effect on other renal cell types such as mesan-gial cells.17 The signaling pathways whereby TGF-�stimulates matrix production have been investigated inmesangial cells,18-20 but have not yet been defined inenal fibroblasts. This is an important area of study be-ause one potentially could identify fibroblast-specificGF-� signaling pathways that could be safer and more
specific pharmaceutical targets.
TGF-� SIGNALING ANDENAL TUBULAR EPITHELIAL CELLS
The renal tubular epithelium is often the cellular target ofinjury, and there is also increasing literature supportingits role as an effector of tubulointerstitial fibrosis. In-creased expression of TGF-� and its receptors have beenshown in the damaged epithelium in multiple models ofglomerular and renal tubular injury.21-23 These includehe following: (1) the UUO injury model, the classicodent model of renal tubulointerstitial fibrosis in whichhe collecting duct epithelium is directly injured by thencreased intraluminal pressure from obstruction; (2) di-betic models of injury resulting in proteinuria thatargets the proximal tubule epithelium as an importantxtraglomerular site of injury; (3) models of acuteidney injury using toxins or ischemia/reperfusion thatarget the proximal tubule because of its high meta-olic requirements and unique vascular supply. Inhese settings of injured renal tubules, epithelialGF-� signaling is thought to promote tubulointersti-
tial fibrosis by affecting tubular cell integrity andincreasing ECM production by both tubular epithelialcells and neighboring fibroblasts.
Increased Epithelial Cell Death
TGF-� signaling can impair renal tubule cell integrityleading to tubular atrophy, a hallmark of tubulointerstitialfibrosis, by inducing either epithelial apoptosis or au-tophagy. TGF-�, a strong promoter of epithelial apopto-is, has been shown to induce renal tubule cell apoptosisn vitro.24 Furthermore, the protective effects of a TGF-
�–blocking antibody (clone 1D11) on the response toUUO partially were attributed to reduced tubular apopto-sis in vivo.8 Recently, TGF-� was shown to cause tubulardestruction because overexpression of TGF-�1 in renalubules in vivo led to autophagy and tubular degenera-ion.7 One of the problems with this elegant model is thathe levels of TGF-�1 in these mice were very high (�200g/mL), and likely were much higher than those pro-
uced by most chronic disease states.
ttcpi
bTeg
EcipTc
o
et
lioangs
TGF-� and tubulointerstitial fibrosis 231
In tubulointerstitial fibrosis, there is concurrent tubularatrophy that raises the question: does epithelial apoptosiscause increased matrix accumulation? In the pulmonaryliterature, the increased apoptosis induced in the lungs ofTGF-�1–overexpressing mice was mediated by the earlygrowth response gene-1, and inhibiting early growth re-sponse gene-1 not only rescued the mice from TGF-�–dependent apoptosis but also reduced fibrosis, establish-ing a link between the two.25 A similar connectionbetween TGF-�–dependent apoptosis and fibrosis hasnot yet been proven in the kidney. A putative mechanismwhereby apoptosis leads to fibrosis is through the phago-cytosis of apoptotic cells by macrophages.26 This stimu-lates the production of TGF-�, which may induce matrixproduction by surrounding fibroblasts. The tubular atro-phy induced by epithelial TGF-� signaling contributes tothe injury and impaired renal function observed in tubu-lointerstitial fibrosis even if a causal relationship withECM production has not yet been established.
Altered Production of ECM
TGF-� facilitates the de-differentiation of injured renalepithelial cells into more mesenchymal-like cells, and itis possible that this process results in increased ECMsynthesis. During this phenotypic change, tubular cellslose epithelial markers such as E cadherin and zonulaoccludens-1, express mesenchymal-like proteins such as�-SMA and vimentin, and undergo cytoskeletal altera-tions resulting in dissolution of tight junctions and adap-tation of a more migratory structure.27 Numerous mech-anisms are responsible for this change in phenotype.TGF-� mediated the loss of E cadherin in renal epithelialcells in vitro through induction of integrin-linked kinasein a Smad-dependent fashion.28 TGF-� also induced theexpression of �-SMA in renal epithelial cells throughpathways involving �-catenin as well as the guanosinetriphosphatase Rho.29,30 TGF-� can induce all of thesemorphologic changes in renal tubular epithelial cells aswell as increase the expression of collagens I and IV, andfibronectin in vitro, suggesting that the alteration in phe-notype may cause the increased matrix production.31,32
Alternatively, it is possible that these are two independenteffects induced by TGF-� and there is no causal relation-ship. TGF-� also may stimulate the de-differentiation ofinjured epithelial cells in vivo because Smad3 null epithelialcells had better preservation of epithelial markers afterUUO.33 Whether these de-differentiated tubular epithelialcells in vivo actually migrate through the tubular basementmembrane and populate the interstitium as matrix-produc-ing fibroblasts is controversial.34,35 Even if these mesenchy-mal-like epithelial cells never become bona fide interstitialfibroblasts, they still may contribute to peritubular fibrosis.Further research is necessary to determine how much auto-crine ECM production occurs in response to renal tubularTGF-� signaling in vivo.
TGF-� signaling in injured tubular epithelium also
may promote tubulointerstitial fibrosis by increasingECM production of neighboring fibroblasts. TGF-� au-oinduces its own production in a feedforward processhat depends on the coordinated actions of Smad3, extra-ellular signal-regulated kinase (ERK) and p38 in renalroximal tubules.36,37 Therefore, injury to tubules resultsn increased epithelial synthesis of TGF-�, which can
signal on nearby fibroblasts. Such paracrine signalinglikely accounts for the proliferating fibroblasts and inter-stitial matrix accumulation observed in mice overex-pressing TGF-�1 in renal tubules.7
Epithelial TGF-� signaling also can increase the ex-pression of other profibrotic growth factors such as con-nective tissue growth factor, which has been shown tostimulate matrix production by increasing transcriptionof collagen I in both renal proximal tubules and fibro-blasts in vitro. Plasminogen activator inhibitor-1 is an-other protein downstream of TGF-� with clear profi-rotic actions in the kidney.38,39 Also, in nonrenal cells,GF-� signaling has been shown to modify the actions ofpidermal growth factor–receptor ligands, hepatocyterowth factor, and insulin-like growth factor.16,40,41 Fu-
ture research is required to define how TGF-� signalingalters these growth factors’ actions in the injured renaltubulointerstitium.
Epithelial Activation of TGF-�
Renal tubular epithelium also plays an important role inTGF-� activation. Abundant TGF-� is sequestered in itsLAP-bound latent form anchored to the matrix, so acti-vation is a critical rate-limiting step in controlling TGF-�signaling.1 The �v integrins are important in vivo acti-vators of TGF-�.42 In particular, integrin �v�6 has beenshown to mediate TGF-�–dependent tubulointerstitialfibrosis after UUO injury.43 The expression of integrin�v�6 is restricted to epithelial cells where it binds theLAP of TGF-�1 and TGF-�3, which are tethered to the
CM. For integrin �v�6 to induce the conformationalhange necessary to activate TGF-�, there must be anntact actin cytoskeleton as well as integrin activation,resumably causing traction on the matrix via binding toGF-�/LAP.44,45 Furthermore, latent TGF-� must be an-hored to the ECM through one of the latent TGF-�
binding proteins for integrin �v�6-mediated activation toccur.46 As such, integrin �v�6’s interaction with latent
TGF-� that is anchored to the ECM may be one way forpithelial cells to transmit mechanical stress and/or cy-oskeletal changes to the surrounding matrix.47 The cel-
lular stress from UUO-induced stretch imposed on col-lecting duct epithelial cells may activate integrin �v�6,eading to TGF-� activation. This mechanical strain fromncreased intraluminal pressure may not be limited tobstructive nephropathy. Reduction in nephron number,s occurs in the 5/6 nephrectomy model or chronic kid-ey disease, has been shown to increase single-nephronlomerular filtration rate, and, consequently, induce fluidhear stress to the tubules.48 This intratubular shear stress
can activate TGF-� independent of proteinuria or hyper-

a
t
T
pspr
t
232 L. Gewin and R. Zent
tension.49 Therefore, changes in intratubular fluid pres-sure caused by declining renal function may promoteTGF-�–mediated tubulointerstitial fibrosis through ef-fects on tubular epithelium.50
As discussed earlier, injured renal tubular epitheliumhas been shown to contribute to TGF-�–dependent tu-bulointerstitial fibrosis by inducing apoptosis/autophagy,increasing TGF-� and other growth factor production,and through augmented TGF-� activation. Paradoxically,when our group injured mice lacking TGF-� signaling inthe collecting duct tubular epithelium, the conditionalknockout mice sustained greater fibrosis and injury.51
These results suggest that, although excessive TGF-�signaling is deleterious, some TGF-� signaling is neces-sary for maintenance of the normal epithelial structure.Consistent with this, reduced epithelial TGF-� activity inlung epithelia resulted in emphysematous changes,52 anddominant-negative T�RII expression in the exocrine pan-creas perturbed epithelial homeostasis.53
TGF-� SIGNALING AND INFLAMMATORY CELLS
Inflammation plays an important role in the pathophysi-ology of tubulointerstitial fibrosis.54 Most renal injurieshave some component of an inflammatory infiltrate com-posed of T cells, macrophages, and neutrophils, withvarying distribution based on the nature of injury. Inchronic renal injury, the macrophage is the predominantimmune cell and although it exerts beneficial effects byphagocytosis of cellular debris and apoptotic cells, mac-rophages also are associated with worsened tubulointer-stitial injury.55 The detrimental actions of macrophagesmay be mediated, in part, by augmenting TGF-� activity.Macrophages directly increase TGF-� activity by bothproducing large amounts of TGF-� as well as generatingROS, which activate latent TGF-�. Also, macrophages
Table 1. TGF-� Modulates the Immune Response
TGF-� as Proinflammatory
TGF-�1 increased inflammatory cytokine (MCP-1, IL-8) production by proximal tubule cells invitro
Qi et al61
Smad3�/� mice had attenuated macrophageinfiltration after UUO
Sato et al3
Smad3�/� mice had less interleukin-6 after acutekidney injury
Nath et al7
ALK5 inhibitor targeted to proximal tubule reducedinflammation after UUO
Prakash et
NOTE. TGF-� has been described as a proinflammatory and anti-icell and microenvironment. This table shows seemingly contrahave immunosuppressive effects on immune cells but proinflamby Cao et al,74 in which only macrophages ex vivo were treateinflammation, likely as a result of altered signaling in inflammatoto how their models differentially affected the activity of SmaOverexpressing latent TGF-�1 as well as deleting Smad4 both athe inflammatory effects.74,77
produce inflammatory cytokines such as IL-6, which
lters TGF-�–receptor trafficking, leading to heightenedsignaling.56
Not only do inflammatory cells modulate TGF-� ac-ivity, but TGF-� affects immune responses as evidenced
by the early death of TGF-�1 null mice from overwhelm-ing inflammation.57 Although this finding implies that
GF-� has an immunosuppressive effect, the preciseeffect of TGF-� on immune responses is complicated andlikely depends on the cellular milieu (Table 1). Theeffects of TGF-� on monocytes/macrophages vary, de-ending on cellular differentiation: this growth factortimulates monocyte migration and adhesion but sup-resses inflammatory cytokine production by tissue mac-ophages (Fig. 3).58 The effect of TGF-� signaling on
inflammation also may vary, depending on the cell typein which signaling is altered: TGF-� signaling in mac-rophages may decrease the production of proinflamma-tory growth factors and cytokines whereas TGF-� sig-naling within injured epithelium likely heightens theinflammatory response.59,60 For example, Smad3-defi-cient mice have attenuated macrophage infiltration afterinjury by UUO,33 suggesting that TGF-� may promoteinflammation in injured kidneys. One possible explana-tion for this increased macrophage infiltration is thatTGF-� can stimulate monocyte chemoattractant pro-ein-1 expression in renal proximal tubules.61 Thus, it is
likely that TGF-� signaling in injured tubular epitheliumresults in increased macrophage infiltration that, if pro-longed, can lead to synthesis of growth factors such asTGF-�, which stimulates neighboring fibroblasts to pro-duce matrix components (Figs. 2 and 3).
TGF-� AND THEMICROVASCULATURE
Capillary degeneration is linked integrally to tubulointer-stitial fibrosis, and endothelial cell drop-out may play a
TGF-� as Anti-Inflammatory
TGF-�1–treated macrophages attenuatedinflammation after adriamycin nephrosis
Cao et al74
Overexpression of latent TGF-�1prevented inflammation in UUO model
Wang et al77
Deletion of Smad4 in renal tubulesenhanced renal inflammation after UUO
Meng et al79
Deletion of T�RII caused increasedinflammation in kidney and other organs
Leveen et al81
matory growth factor, and its specific effect depends on the targety effects of TGF-� in modulating renal inflammation. TGF-� canry effects on renal parenchyma.73 This is consistent with the study
TGF-�. Also, the global deletion of T�RII produced multi-organlls. The conflicting reports of the other studies listed may be owinga known modulator of inflammation and nuclear factor-�B.75,76
red to have dramatic effects on Smad7 activity, which may explain
3
8
al80
nflamdictormatod withry ced7,
ppea
causal role in the progression of fibrosis.62 Loss of post-

tt
cnii
aiiemw
crosi
TGF-� and tubulointerstitial fibrosis 233
glomerular capillaries creates a hypoxic environment thatfurther stimulates fibrosis.63 Exactly how TGF-� signal-ing in the endothelium promotes fibrosis in vivo is un-clear. Endothelial injury can stimulate TGF-� productionas shown in animal models of increased salt intake andsalt-sensitive hypertension in which TGF-� productionwas up-regulated by endothelial cells of renal arteri-oles.64,65 Conversely, TGF-� may have adverse effects onthe renal microvasculature by promoting both endothelialapoptosis and de-differentiation, leading to increased ma-trix production.66,67 TGF-� also may modulate angiogen-esis, a pivotal event in the restoration of healthy renalvasculature after injury. TGF-� signaling on endothelialcells in vitro has been shown to have a net anti-angio-genic effect.68 However, the in vivo effect of TGF-� onangiogenesis is complicated because this growth factorinduces renal proximal tubular expression of both vascu-lar endothelial growth factor-A and thrombospondin-1,which have pro-angiogenic and anti-angiogenic effects,respectively, in vivo.69-71 These findings suggest thatTGF-� signaling on injured epithelium may affect theadjacent vasculature and that divergent effects on angio-genesis may occur. Interestingly, a neutralizing TGF-�antibody protected against the vascular loss that occurred5 weeks after ischemia-reperfusion, implying that TGF-�may mediate chronic microvascular changes that resultfrom acute kidney injury.72 Whether these changes werecaused by TGF-�–mediated anti-angiogenesis or causedby other effects on the endothelium (eg, apoptosis) isunclear. To better define the role of TGF-� in the endo-thelial response to injury, future studies should examineendothelial-specific TGF-� signaling in vivo as well asanalyze the TGF-�–mediated cross-talk between injured
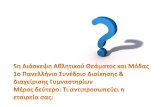
Figure 3. The effects of TGF-� on monocytes/macrophages. TGF-�such as macrophage inflammatory protein-1� (MIP-1�) and monocytof monocytes also are enhanced by TGF-� through up-regulated expTGF-� suppresses activation of macrophages as evidenced by decreproduction of inflammatory cytokines such as IFN-� but increases tinterferon-�; iNOS, inducible nitric oxide synthase; TNF-�, tumor ne
tubular epithelium and the surrounding vasculature.
CONCLUSIONS
TGF-� clearly plays a key role in the progression ofubulointerstitial fibrosis, but the mechanisms wherebyhis occurs remain undefined. Understanding how TGF-�
mediates tubulointerstitial fibrosis is challenging becausemultiple cell types are involved in fibrosis and the re-sponses to TGF-� vary, depending on cell type andellular milieu. Fortunately, the advent of Cre/lox tech-ology allows for selective inhibition of TGF-� signalingn specific compartments of the kidney. This tool willmprove our understanding of cell-autonomous TGF-�
signaling, providing important information regarding theeffects of inhibiting TGF-� activity in targeted cell typesin vivo. Another important direction for future studies iselucidating cell-specific downstream pathways ofTGF-�. These pathways likely mediate the divergenteffects of TGF-�, and defining how these pathways differin epithelial cells and fibroblasts may identify pharma-cologic targets with safer profiles than TGF-�. Also, abetter understanding of how inhibiting TGF-� signalinglters the activity of other growth factors after renalnjury is crucial and could have important therapeuticmplications. As the population with chronic kidney dis-ase continues to expand, a safe and effective way toodulate TGF-�–dependent tubulointerstitial fibrosisould make a huge medical and economic impact.
REFERENCES1. Rifkin DB. Latent transforming growth factor-beta (TGF-beta)
binding proteins: orchestrators of TGF-beta availability. J BiolChem. 2005;280:7409-12.
2. Jenkins G. The role of proteases in transforming growth factor-
motes monocyte migration by increasing chemoattractant cytokinesmoattractant protein-1 (MCP-1). Cell-cell and cell-matrix interactionsn of integrins. In contrast to these stimulatory effects on monocytes,iNOS and TNF-� expression. TGF-� signaling reduces macrophagenthesis of profibrotic factors such as TGF-�. Abbreviations: IFN-�,s factor-�.
proe cheressioasedhe sy
beta activation. Int J Biochem Cell Biol. 2008;40:1068-78.

234 L. Gewin and R. Zent
3. Wrana JL, Attisano L, Carcamo J, Zentella A, Doody J, Laiho M,et al. TGF beta signals through a heteromeric protein kinasereceptor complex. Cell. 1992;71:1003-14.
4. Yamashita H, ten Dijke P, Franzen P, Miyazono K, Heldin CH.Formation of hetero-oligomeric complexes of type I and type IIreceptors for transforming growth factor-beta. J Biol Chem. 1994;269:20172-8.
5. Brown KA, Pietenpol JA, Moses HL. A tale of two proteins:differential roles and regulation of Smad2 and Smad3 in TGF-beta signaling. J Cell Biochem. 2007;101:9-33.
6. Zhang YE. Non-Smad pathways in TGF-beta signaling. Cell Res.2009;19:128-39.
7. Koesters R, Kaissling B, Lehir M, Picard N, Theilig F, GebhardtR, et al. Tubular overexpression of transforming growth factor-beta1 induces autophagy and fibrosis but not mesenchymal tran-sition of renal epithelial cells. Am J Pathol. 2010;177:632-43.
8. Miyajima A, Chen J, Lawrence C, Ledbetter S, Soslow RA, SternJ, et al. Antibody to transforming growth factor-beta amelioratestubular apoptosis in unilateral ureteral obstruction. Kidney Int.2000;58:2301-13.
9. Desmouliere A, Geinoz A, Gabbiani F, Gabbiani G. Transforminggrowth factor-beta 1 induces alpha-smooth muscle actin expres-sion in granulation tissue myofibroblasts and in quiescent andgrowing cultured fibroblasts. J Cell Biol. 1993;122:103-11.
10. Ignotz RA, Endo T, Massague J. Regulation of fibronectin andtype I collagen mRNA levels by transforming growth factor-beta.J Biol Chem. 1987;262:6443-6.
11. Roberts AB, Sporn MB, Assoian RK, Smith JM, Roche NS, Wake-field LM, et al. Transforming growth factor type beta: rapid inductionof fibrosis and angiogenesis in vivo and stimulation of collagenformation in vitro. Proc Natl Acad Sci U S A. 1986;83:4167-71.
12. Edwards DR, Murphy G, Reynolds JJ, Whitham SE, Docherty AJ,Angel P, et al. Transforming growth factor beta modulates theexpression of collagenase and metalloproteinase inhibitor. EMBOJ. 1987;6:1899-904.
13. Leco KJ, Khokha R, Pavloff N, Hawkes SP, Edwards DR. Tissueinhibitor of metalloproteinases-3 (TIMP-3) is an extracellularmatrix-associated protein with a distinctive pattern of expressionin mouse cells and tissues. J Biol Chem. 1994;269:9352-60.
14. Tang N, Cunningham K, Enger MD. TGF beta elicits oppositeresponses in clonal subpopulations of NRK-49F cells. Exp CellRes. 1991;196:13-9.
15. Alvarez RJ, Sun MJ, Haverty TP, Iozzo RV, Myers JC, NeilsonEG. Biosynthetic and proliferative characteristics of tubulointer-stitial fibroblasts probed with paracrine cytokines. Kidney Int.1992;41:14-23.
16. Uttamsingh S, Bao X, Nguyen KT, Bhanot M, Gong J, Chan JL,et al. Synergistic effect between EGF and TGF-beta1 in inducingoncogenic properties of intestinal epithelial cells. Oncogene.2008;27:2626-34.
17. Wang S, Wilkes MC, Leof EB, Hirschberg R. Imatinib mesylateblocks a non-Smad TGF-beta pathway and reduces renal fibro-genesis in vivo. FASEB J. 2005;19:1-11.
18. Runyan CE, Schnaper HW, Poncelet AC. The phosphatidylino-sitol 3-kinase/Akt pathway enhances Smad3-stimulated mesan-gial cell collagen I expression in response to transforming growthfactor-beta1. J Biol Chem. 2004;279:2632-9.
19. Runyan CE, Schnaper HW, Poncelet AC. Smad3 and PKCdeltamediate TGF-beta1-induced collagen I expression in human mes-angial cells. Am J Physiol Renal Physiol. 2003;285:F413-22.
20. Hayashida T, Poncelet AC, Hubchak SC, Schnaper HW. TGF-beta1 activates MAP kinase in human mesangial cells: a possiblerole in collagen expression. Kidney Int. 1999;56:1710-20.
21. Basile DP, Rovak JM, Martin DR, Hammerman MR. Increased trans-forming growth factor-beta 1 expression in regenerating rat renal tubulesfollowing ischemic injury. Am J Physiol. 1996;270:F500-9.
22. Sutaria PM, Ohebshalom M, McCaffrey TA, Vaughan ED Jr,
Felsen D. Transforming growth factor-beta receptor types I and IIare expressed in renal tubules and are increased after chronicunilateral ureteral obstruction. Life Sci. 1998;62:1965-72.
23. Goumenos DS, Tsakas S, El Nahas AM, Alexandri S, Oldroyd S,Kalliakmani P, et al. Transforming growth factor-beta(1) in thekidney and urine of patients with glomerular disease and protein-uria. Nephrol Dial Transplant. 2002;17:2145-52.
24. Yoshikawa M, Hishikawa K, Idei M, Fujita T. Trichostatin aprevents TGF-beta1-induced apoptosis by inhibiting ERK activa-tion in human renal tubular epithelial cells. Eur J Pharmacol.2010;642:28-36.
25. Lee CG, Cho SJ, Kang MJ, Chapoval SP, Lee PJ, Noble PW, etal. Early growth response gene 1-mediated apoptosis is essentialfor transforming growth factor beta1-induced pulmonary fibrosis.J Exp Med. 2004;200:377-89.
26. Fadok VA, Bratton DL, Konowal A, Freed PW, Westcott JY,Henson PM. Macrophages that have ingested apoptotic cells invitro inhibit proinflammatory cytokine production through auto-crine/paracrine mechanisms involving TGF-beta, PGE2, andPAF. J Clin Invest. 1998;101:890-8.
27. Bottinger EP, Bitzer M. TGF-beta signaling in renal disease. J AmSoc Nephrol. 2002;13:2600-10.
28. Li Y, Yang J, Dai C, Wu C, Liu Y. Role for integrin-linked kinasein mediating tubular epithelial to mesenchymal transition andrenal interstitial fibrogenesis. J Clin Invest. 2003;112:503-16.
29. Masszi A, Fan L, Rosivall L, McCulloch CA, Rotstein OD, MucsiI, et al. Integrity of cell-cell contacts is a critical regulator ofTGF-beta 1-induced epithelial-to-myofibroblast transition: rolefor beta-catenin. Am J Pathol. 2004;165:1955-67.
30. Masszi A, Di Ciano C, Sirokmany G, Arthur WT, Rotstein OD,Wang J, et al. Central role for Rho in TGF-beta1-induced alpha-smooth muscle actin expression during epithelial-mesenchymaltransition. Am J Physiol Renal Physiol. 2003;284:F911-24.
31. Yang J, Liu Y. Dissection of key events in tubular epithelial tomyofibroblast transition and its implications in renal interstitialfibrosis. Am J Pathol. 2001;159:1465-75.
32. Strutz F, Zeisberg M, Ziyadeh FN, Yang CQ, Kalluri R, MullerGA, et al. Role of basic fibroblast growth factor-2 in epithelial-mesenchymal transformation. Kidney Int. 2002;61:1714-28.
33. Sato M, Muragaki Y, Saika S, Roberts AB, Ooshima A. Targeteddisruption of TGF-beta1/Smad3 signaling protects against renaltubulointerstitial fibrosis induced by unilateral ureteral obstruc-tion. J Clin Invest. 2003;112:1486-94.
34. Zeisberg M, Duffield JS. Resolved: EMT produces fibroblasts inthe kidney. J Am Soc Nephrol. 2010;21:1247-53.
35. Kriz W, Kaissling B, Le Hir M. Epithelial-mesenchymal transi-tion (EMT) in kidney fibrosis: fact or fantasy? J Clin Invest.2011;121:468-74.
36. Van Obberghen-Schilling E, Roche NS, Flanders KC, Sporn MB,Roberts AB. Transforming growth factor beta 1 positively regu-lates its own expression in normal and transformed cells. J BiolChem. 1988;263:7741-6.
37. Zhang M, Fraser D, Phillips A. ERK, p38, and Smad signalingpathways differentially regulate transforming growth factor-beta1autoinduction in proximal tubular epithelial cells. Am J Pathol.2006;169:1282-93.
38. Krag S, Danielsen CC, Carmeliet P, Nyengaard J, Wogensen L.Plasminogen activator inhibitor-1 gene deficiency attenuatesTGF-beta1-induced kidney disease. Kidney Int. 2005;68:2651-66.
39. Oda T, Jung YO, Kim HS, Cai X, Lopez-Guisa JM, Ikeda Y, etal. PAI-1 deficiency attenuates the fibrogenic response to ureteralobstruction. Kidney Int. 2001;60:587-96.
40. Naim R, Naumann A, Barnes J, Sauter A, Hormann K, Merkel D,et al. Transforming growth factor-beta1-antisense modulates theexpression of hepatocyte growth factor/scatter factor in keloidfibroblast cell culture. Aesthetic Plast Surg. 2008;32:346-52.
41. Gardner S, Alzhanov D, Knollman P, Kuninger D, Rotwein P.TGF-beta inhibits muscle differentiation by blocking autocrinesignaling pathways initiated by IGF-II. Mol Endocrinol. 2011;25:
128-37.
TGF-� and tubulointerstitial fibrosis 235
42. Yang Z, Mu Z, Dabovic B, Jurukovski V, Yu D, Sung J, et al.Absence of integrin-mediated TGFbeta1 activation in vivo reca-pitulates the phenotype of TGFbeta1-null mice. J Cell Biol. 2007;176:787-93.
43. Ma LJ, Yang H, Gaspert A, Carlesso G, Barty MM, Davidson JM,et al. Transforming growth factor-beta-dependent and -indepen-dent pathways of induction of tubulointerstitial fibrosis in be-ta6(-/-) mice. Am J Pathol. 2003;163:1261-73.
44. Jenkins RG, Su X, Su G, Scotton CJ, Camerer E, Laurent GJ, etal. Ligation of protease-activated receptor 1 enhances alpha-(v)beta6 integrin-dependent TGF-beta activation and promotesacute lung injury. J Clin Invest. 2006;116:1606-14.
45. Munger JS, Huang X, Kawakatsu H, Griffiths MJ, Dalton SL, WuJ, et al. The integrin alpha v beta 6 binds and activates latent TGFbeta 1: a mechanism for regulating pulmonary inflammation andfibrosis. Cell. 1999;96:319-28.
46. Annes JP, Chen Y, Munger JS, Rifkin DB. Integrin alphaVbeta6-mediated activation of latent TGF-beta requires the latent TGF-beta binding protein-1. J Cell Biol. 2004;165:723-34.
47. Keski-Oja J, Koli K, von Melchner H. TGF-beta activation bytraction? Trends Cell Biol. 2004;14:657-9.
48. Essig M, Terzi F, Burtin M, Friedlander G. Mechanical strainsinduced by tubular flow affect the phenotype of proximal tubularcells. Am J Physiol Renal Physiol. 2001;281:F751-62.
49. Ying WZ, Sanders PW. Dietary salt modulates renal productionof transforming growth factor-beta in rats. Am J Physiol. 1998;274:F635-41.
50. Rohatgi R, Flores D. Intratubular hydrodynamic forces influencetubulointerstitial fibrosis in the kidney. Curr Opin Nephrol Hy-pertens. 2010;19:65-71.
51. Gewin L, Bulus N, Mernaugh G, Moeckel G, Harris RC, MosesHL, et al. TGF-beta receptor deletion in the renal collectingsystem exacerbates fibrosis. J Am Soc Nephrol. 2010;21:1334-43.
52. Morris DG, Huang X, Kaminski N, Wang Y, Shapiro SD, Dol-ganov G, et al. Loss of integrin alpha(v)beta6-mediated TGF-betaactivation causes Mmp12-dependent emphysema. Nature. 2003;422:169-73.
53. Bottinger EP, Jakubczak JL, Roberts IS, Mumy M, Hemmati P,Bagnall K, et al. Expression of a dominant-negative mutant TGF-beta type II receptor in transgenic mice reveals essential roles forTGF-beta in regulation of growth and differentiation in the exo-crine pancreas. EMBO J. 1997;16:2621-33.
54. Ferenbach D, Kluth DC, Hughes J. Inflammatory cells in renalinjury and repair. Semin Nephrol. 2007;27:250-9.
55. Sean Eardley K, Cockwell P. Macrophages and progressive tu-bulointerstitial disease. Kidney Int. 2005;68:437-55.
56. Zhang XL, Topley N, Ito T, Phillips A. Interleukin-6 regulation oftransforming growth factor (TGF)-beta receptor compartmental-ization and turnover enhances TGF-beta1 signaling. J Biol Chem.2005;280:12239-45.
57. Shull MM, Ormsby I, Kier AB, Pawlowski S, Diebold RJ, Yin M,et al. Targeted disruption of the mouse transforming growthfactor-beta 1 gene results in multifocal inflammatory disease.Nature. 1992;359:693-9.
58. Letterio JJ, Roberts AB. Regulation of immune responses byTGF-beta. Annu Rev Immunol. 1998;16:137-61.
59. Kitamura M, Suto T, Yokoo T, Shimizu F, Fine LG. Transform-ing growth factor-beta 1 is the predominant paracrine inhibitor ofmacrophage cytokine synthesis produced by glomerular mesan-gial cells. J Immunol. 1996;156:2964-71.
60. Alexandrow MG, Moses HL. Transforming growth factor betaand cell cycle regulation. Cancer Res. 1995;55:1452-7.
61. Qi W, Chen X, Polhill TS, Sumual S, Twigg S, Gilbert RE, et al.TGF-beta1 induces IL-8 and MCP-1 through a connective tissuegrowth factor-independent pathway. Am J Physiol Renal Physiol.2006;290:F703-9.
62. Bohle A, Mackensen-Haen S, Wehrmann M. Significance ofpostglomerular capillaries in the pathogenesis of chronic renal
failure. Kidney Blood Press Res. 1996;19:191-5.63. Kimura K, Iwano M, Higgins DF, Yamaguchi Y, Nakatani K,Harada K, et al. Stable expression of HIF-1alpha in tubularepithelial cells promotes interstitial fibrosis. Am J Physiol RenalPhysiol. 2008;295:F1023-9.
64. Sanders PW. Vascular consequences of dietary salt intake. Am JPhysiol Renal Physiol. 2009;297:F237-43.
65. Jing L, Zhang JZ, Zhao L, Wang YL, Guo FY. High-expressionof transforming growth factor beta1 and phosphorylation of ex-tracellular signal-regulated protein kinase in vascular smoothmuscle cells from aorta and renal arterioles of spontaneous hy-pertension rats. Clin Exp Hypertens. 2007;29:107-17.
66. Rouschop KM, Claessen N, Pals ST, Weening JJ, Florquin S.CD44 disruption prevents degeneration of the capillary networkin obstructive nephropathy via reduction of TGF-beta1-inducedapoptosis. J Am Soc Nephrol. 2006;17:746-53.
67. Zeisberg EM, Potenta SE, Sugimoto H, Zeisberg M, Kalluri R.Fibroblasts in kidney fibrosis emerge via endothelial-to-mesen-chymal transition. J Am Soc Nephrol. 2008;19:2282-7.
68. Pepper MS, Belin D, Montesano R, Orci L, Vassalli JD. Trans-forming growth factor-beta 1 modulates basic fibroblast growthfactor-induced proteolytic and angiogenic properties of endothe-lial cells in vitro. J Cell Biol. 1990;111:743-55.
69. Nakagawa T, Li JH, Garcia G, Mu W, Piek E, Bottinger EP, et al.TGF-beta induces proangiogenic and antiangiogenic factors viaparallel but distinct Smad pathways. Kidney Int. 2004;66:605-13.
70. Kang DH, Anderson S, Kim YG, Mazzalli M, Suga S, JeffersonJA, et al. Impaired angiogenesis in the aging kidney: vascularendothelial growth factor and thrombospondin-1 in renal disease.Am J Kidney Dis. 2001;37:601-11.
71. Kang DH, Hughes J, Mazzali M, Schreiner GF, Johnson RJ. Im-paired angiogenesis in the remnant kidney model: II. Vascular en-dothelial growth factor administration reduces renal fibrosis andstabilizes renal function. J Am Soc Nephrol. 2001;12:1448-57.
72. Spurgeon KR, Donohoe DL, Basile DP. Transforming growthfactor-beta in acute renal failure: receptor expression, effects onproliferation, cellularity, and vascularization after recovery frominjury. Am J Physiol Renal Physiol. 2005;288:F568-77.
73. Saxena V, Lienesch DW, Zhou M, Bommireddy R, Azhar M,Doetschman T, et al. Dual roles of immunoregulatory cytokineTGF-beta in the pathogenesis of autoimmunity-mediated organdamage. J Immunol. 2008;180:1903-12.
74. Cao Q, Wang Y, Zheng D, Sun Y, Lee VW, Zheng G, et al. IL-10/TGF-beta-modified macrophages induce regulatory T cells and protectagainst adriamycin nephrosis. J Am Soc Nephrol. 2010;21:933-42.
75. Ng YY, Hou CC, Wang W, Huang XR, Lan HY. Blockade ofNFkappaB activation and renal inflammation by ultrasound-me-diated gene transfer of Smad7 in rat remnant kidney. Kidney IntSuppl. 2005;94:S83-91.
76. Chen HY, Huang XR, Wang W, Li JH, Heuchel RL, Chung AC,et al. The protective role of Smad7 in diabetic kidney disease:mechanism and therapeutic potential. Diabetes. 2011;60:590-601.
77. Wang W, Huang XR, Li AG, Liu F, Li JH, Truong LD, et al.Signaling mechanism of TGF-beta1 in prevention of renal inflam-mation: role of Smad7. J Am Soc Nephrol. 2005;16:1371-83.
78. Nath KA, Croatt AJ, Warner GM, Grande JP. Genetic deficiencyof Smad3 protects against murine ischemic acute kidney injury.Am J Physiol Renal Physiol. 2011;301:F436-42.
79. Meng X, Huang XR, Xiao J, Chung AC, Qin W, Chen HY, et al.Disruption of Smad4 impairs TGF-beta/Smad3 and Smad7 tran-scriptional regulation during renal inflammation and fibrosis invivo and in vitro. Kidney Int. 2011.
80. Prakash J, de Borst MH, van Loenen-Weemaes AM, Lacombe M,Opdam F, van Goor H, et al. Cell-specific delivery of a transforminggrowth factor-beta type I receptor kinase inhibitor to proximal tubu-lar cells for the treatment of renal fibrosis. Pharm Res. 2008;10:2427-39.
81. Leveen P, Larsson J, Ehinger M, Cilio CM, Sundler M, SjostrandLJ, et al. Induced disruption of the transforming growth factorbeta type II receptor gene in mice causes a lethal inflammatory
disorder that is transplantable. Blood. 2002;100:560-8.