Honorarium from ASTRA ZENECAstatic.livemedia.gr/kebe/documents/al15432_us63... · PEGASUS-TIMI 54:...
73
Conflict of interest Honorarium from ASTRA ZENECA
Transcript of Honorarium from ASTRA ZENECAstatic.livemedia.gr/kebe/documents/al15432_us63... · PEGASUS-TIMI 54:...

Conflict of interest
Honorarium from ASTRA ZENECA

FOR REACTIVE MEDICAL USE ONLY

Mεσογειακή διατροφή
3

FOR REACTIVE MEDICAL USE ONLY

FOR REACTIVE MEDICAL USE ONLY
ΑΠ
ΣΤΟΧΟΙ ΑΝΤΙΥΠΕΡΤΑΣΙΚΗΣ ΑΓΩΓΗΣ
Διαβητικοί ασθενείςJNC VII: 2003
<140/90mmHg
<130/80mmHg
ΣΑΠ<140mmHg ΔΑΠ<90mmHg
AHA/ACC/ASH Scientific Statement Circulation 2015

EUROASPIRE IV n:8000(2012-13) Eur J Prev Cardiology 2015 in press
Kάπνισµα 16% Καθόλου Φυσική άσκηση 60% Παχύσαρκοι 38% κεντρική παχυσαρκία (>102, ή > 88 cm 60% ΑΠ >140/90 mm 43% LDL >1.8 80% Διαβήτη 27%

EUROASPIRE IV(2012-13) Eur J Prev Cardiology 2015 in press
Αντιαιµοπεταλιακά 94% Β αποκλειστές 82.6% ACE/ARB 75% Στατίνες 86%
Rehabilitation center: 51% συµβουλεύτηκαν

• 65 ετών
• Εµφραγµα Μυοκαρδίου 3 χρόνια πριν – Κλειστή RCA,
– Αγγειοπλαστική, DES
– LVEF 48% (reassessed 1 year ago)
• Οικογενειακό ιστορικό (πατέρας 52)
• Δυσλιπιδαιµία υπο atorvastatin 20 mg
Γιωρίκας
Copyright © 2014

Medications initiated 3 years ago at time of post MI evaluation:
Aspirin 325 mg daily 81-162 mg daily Clopidogrel 75 mg daily
Carvedilol 12.5 mg twice daily
Enalapril 10 mg daily
Statin
Medications
Copyright © 2014

FOR REACTIVE MEDICAL USE ONLY

Repeat Revascularization after DES
11

12
BMJ 2015;350;1618

FOR REACTIVE MEDICAL USE ONLY
<5 χρόνια median 2
PCI 23%, CABG 20%

FOR REACTIVE MEDICAL USE ONLY

PEGASUS-TIMI 54: Major Exclusion Criteria
• Planned use of a P2Y12 receptor antagonist, dipyridamole, cilostazol, or anticoagulant therapy during the study period
• Bleeding disorder, history of ischaemic stroke or intracranial bleeding, central nervous system tumour or intracranial vascular abnormality
• Gastrointestinal bleeding within the previous 6 months or major surgery within the previous 30 days
• High risk of bradycardic events
• Severe hepatic or renal disease
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 15

PEGASUS-TIMI 54: Baseline CharacteristicsCharacteristic Ticagrelor 90 mg bid
N=7050; n (%)Ticagrelor 60 mg bid
N=7045; n (%)Placebo
N=7067; n (%)Demographics Age – year, mean (SD) 65.4 (8.4) 65.2 (8.4) 65.4 (8.3) Female 1682 (23.9) 1661 (23.6) 1717 (24.3) Caucasian* 6126 (86.9) 6077 (86.3) 6124 (86.7) Weight – kg, mean (SD) 82.0 (16.7) 82.0 (17.0) 81.8 (16.6)Clinical characteristics Hypertension 5462 (77.5) 5461 (77.5) 5484 (77.6) Hypercholesterolaemia 5410 (76.7) 5380 (76.4) 5451 (77.1) Current smoker 1187 (16.8) 1206 (17.1) 1143 (16.2) Diabetes mellitus 2241 (31.8) 2308 (32.8) 2257 (31.9) Multivessel coronary disease – n/total n (%) 4155/7049 (58.9) 4190/7042 (59.5) 4213/7067 (59.6) History of PCI** – n/total n (%) 5852/7049 (83.0) 5879/7044 (83.5) 5837/7066 (82.6) >1 prior MI 1143 (16.2) 1168 (16.6) 1188 (16.8) Peripheral artery disease 371 (5.3) 368 (5.2) 404 (5.7) Creatinine clearance <60 mL/min – n/total n (%) 1653/6958 (23.8) 1547/6955 (22.2) 1649/6985 (23.6)Qualifying event†
Years from MI – median (IQR) 1.7 (1.2–2.3) 1.7 (1.2–2.3) 1.7 (1.2–2.3) STEMI 3763/7043 (53.4) 3757/7035 (53.4) 3809/7057 (54.0) NSTEMI 2898/7043 (41.1) 2842/7035 (40.4) 2843/7057 (40.3) MI type unknown 382/7043 (5.4) 436/7035 (6.2) 405/7057 (5.7)Medication at enrolment ASA (any dose) 7039 (99.8) 7036 (99.9) 7057 (99.9) Statin 6526 (92.6) 6495 (92.2) 6583 (93.2) Beta-blocker 5812 (82.4) 5796 (82.3) 5878 (83.2) ACEI or ARB 5702 (80.9) 5631 (79.9) 5697 (80.6)
*Self-reported; **96.5% of PCIs involved stenting; †Patients for whom it could not be verified that they had had a myocardial infarction were excluded from the denominator as well as from the calculation for the median years since the myocardial infarction All P values for comparisons are >0.05; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; SD, standard deviation
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 16

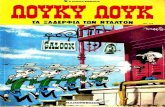
PEGASUS-TIMI 54: Primary Endpoint
17CI, confidence interval; HR, hazard ratio
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
No. at risk Placebo 90 mg bid 60 mg bid
7067 7050 7045
6979 6973 6969
6892 6899 6905
6823 6827 6842
6761 6769 6784
6681 6719 6733
6508 6550 6557
6236 6272 6270
5876 5921 5904
5157 5243 5222
4343 4401 4424
3360 3368 3392
2028 2038 2055
Even
t rat
e (%
)
Months from randomisation
Ticagrelor 60 mg vs placebo HR 0.84 (95% CI 0.74–0.95) P=0.004
Ticagrelor 90 mg vs placebo HR 0.85 (95% CI 0.75–0.96) P=0.008
9.04% Placebo
7.85% 90 mg bid
7.77% 60 mg bid
Placebo Ticagrelor 90 mg bid Ticagrelor 60 mg bid
0 3 6 9 12 15 18 21 24 27 30 33 360
1
2
3
4
5
6
7
8
9
10

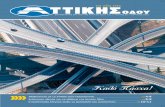
PEGASUS-TIMI 54: Bleeding
0
1.25
2.5
3.75
5
TIMI major bleeding Fatal bleeding or ICH Fatal bleeding
Ticagrelor 90 mg bidTicagrelor 60 mg bidPlacebo
18
3-ye
ar K
M e
vent
rate
2.62.3
1.11.3 1.2
0.40.6 0.7 0.6 0.6 0.6 0.5
0.1 0.3 0.3
Rates are presented as 3-year Kaplan-Meier estimates P<0.026 indicates statistical significance
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
P<0.001
P<0.001P=NS P=NS P=NS

-50
-40
-30
-20
-10
0
10
20
30
40
50
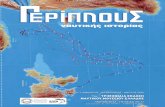
PEGASUS-TIMI 54: Estimates of First Efficacy and Bleeding Events Prevented and Caused
Rates are annualised from 3-year Kaplan-Meier event rates in the intention-to-treat population
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print]
Ticagrelor 90 mg bid
Ticagrelor 60 mg bid
CV death, MI or stroke
TIMI major bleeding
Num
ber o
f eve
nts
per 1
0,00
0 pa
tient
s in
itiat
ed o
n tre
atm
ent f
or 1
yea
r
-40 -42
41
31
19

PEGASUS-TIMI 54: Summary
• The PEGASUS-TIMI 54 study demonstrated that the addition of ticagrelor 60 mg bid or 90 mg bid to low-dose ASA in patients 1–3 years after a MI significantly reduced the risk of the primary endpoint of CV death, MI or stroke
• A directionally consistent effect was observed on all components of the primary endpoint, including CV death
• The benefit of ticagrelor was consistent among major clinical subgroups and by region and continued to accrue over time with a median of 33 months of follow-up
• The rate of the primary safety endpoint of TIMI major bleeding was higher with both doses of ticagrelor compared with placebo
• The rate of fatal bleeding or non-fatal intracranial haemorrhage was low (<1% at 3 years) and did not differ between treatment arms
• Dyspnoea was more frequent with both doses of ticagrelor; however, the majority of episodes with either dose were characterised as either mild (58.1%) or moderate (36.9%) in severity
20Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

PEGASUS-TIMI 54: Conclusions
• Patients who have had a MI remain at heightened risk for ischaemic events over the long term1–3
• PEGASUS-TIMI 54 is the first prospective, randomised controlled clinical trial appropriately powered to demonstrate the benefit of long-term DAPT in patients with prior MI4
• Coupled with the established benefit of ticagrelor in the setting of ACS, these data support consideration of long-term antiplatelet therapy with ticagrelor plus low-dose ASA, in appropriately selected patients with prior MI4
1. Bhatt DL et al. JAMA 2010;304:1350–1357 2. Fox KA et al. Eur Heart J 2010;31:2755–2764 3. Jernberg T et al. Eur Heart J 2015; pii: ehu505. [Epub ahead of print] 4. Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 21

…seeking the optimal balance
Efficacy To reduce intravascular thrombosis
Safety Less bleedings with increased risk of bleeding

FOR REACTIVE MEDICAL USE ONLY
Αν σε ρωτήσει ο γέρος µου πέστου πως πήγα για rehabilitation

Τι φάρµακα πρέπει να παίρνει ο Γιωρίκας;
24
Ασπιρίνη Στατίνη Και ? Τικαγρελόρη

FOR REACTIVE MEDICAL USE ONLY

FOR REACTIVE MEDICAL USE ONLY

FOR REACTIVE MEDICAL USE ONLY

Μεσογειακή Δίαιτα:Φρούτα, λαχανικά, όσπρια ,προϊόντα ολικης αλεσης, Λαδι. παξιµάδι, µαργαρινη και οχι βούτυρο και αλλα λίπη,Ψαρι µικροτερη κατανάλωση
κόκκινου κρέατος

PEGASUS-TIMI 54
A randomised, double-blind, placebo-controlled, parallel-group, multinational trial to assess the prevention of thrombotic events with ticagrelor compared with placebo on a background of acetylsalicylic acid therapy in patients with
a history of myocardial infarction
George Giannakoulas Academic Lecturer in Cardiology
Aristotle University of Thessaloniki

Reminder of the Current EU Indication
• Ticagrelor, co-administered with ASA, is indicated for the prevention of atherothrombotic events in adult patients with ACS (unstable angina, NSTEMI or STEMI), including patients managed medically, and those who are managed with PCI or CABG
• Ticagrelor is only indicated in patients with ACS for up to 1 year of treatment
30
ACS, acute coronary syndromes; ASA, acetylsalicylic acid; CABG, coronary artery bypass grafting; NSTEMI, non-ST elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST elevation myocardial infarction
BRILIQUE™ [Summary of Product Characteristics]. Södertälje, Sweden: AstraZeneca;2013

Table of Contents Background/Study Design 1. Study Rationale 2. Study Organisation 3. Steering Committee 4. Study Design 5. Inclusion Criteria 6. Major Exclusion Criteria 7. Randomisation and Ticagrelor Dosing 8. Concomitant Therapies 9. Modified Study Treatment Scenario 10. Patients Undergoing Procedures 11. Efficacy Endpoints 12. Primary Safety Endpoint 13. Other Safety Endpoints 14. Statistical Methodology 15. Statistical Considerations
Results 1. Study Patients and Study Drug 2. Global Enrolment 3. Baseline Characteristics 4. Follow-up 5. CONSORT Diagram 6. Primary Endpoint 7. Efficacy Endpoints 8. Primary Endpoint by Subgroup 9. Safety Endpoints 10. Bleeding 11. Primary Safety Endpoint by Subgroup 12. Analyses of Net Clinical Benefit 13. Estimates of First Efficacy and Bleeding Events
Prevented and Caused 14. NNT/NNH 15. Dyspnoea 16. Other Safety Endpoints 17. Adverse Events 18. Non-CV Deaths 19. Summary 20. Conclusions 31
NB: In SLIDESHOW view, click on the heading to go that section within the slide deck; on any slide,
click on the PEGASUS-TIMI 54 icon in the right-corner to return to this contents page

PEGASUS-TIMI 54: Rationale (1)• Patients who have suffered a MI are at heightened risk of recurrent
ischaemic events1–3 – The recent APOLLO-HELICON registry highlighted that 1 in 5 patients who remain
event free 1 year post-MI will go on to suffer another MI, a stroke, or die from CV causes in the subsequent 3 years3
– These data suggest that patients with a history of MI may derive particular benefit from intensive secondary prevention strategies
• The role of P2Y12 receptor antagonists in long-term secondary prevention after MI has not been established
• Both US and European ACS practice guidelines currently recommend treatment with a P2Y12 receptor antagonist for up to 1 year after MI4–7
CV, cardiovascular; MI, myocardial infarction 1. Bhatt DL et al. JAMA 2010;304:1350–1357 2. Fox KA et al. Eur Heart J 2010;31:2755–27643. Jernberg T et al. Eur Heart J 2015; pii: ehu505 [Epub ahead of print]4. Amsterdam EA et al. Circulation 2014;130:2354–23945. Hamm CW et al. Eur Heart J 2011;32:2999–30546. O'Gara PT et al. Circulation 2013;127:e362–425 7. Steg PG et al. Eur Heart J 2012;33:2569–2619 32

PEGASUS-TIMI 54: Rationale (2)• Ticagrelor is a potent, reversibly binding, direct-acting agent P2Y12 receptor
antagonist that has low inter-individual variability1
• Ticagrelor also increases endogenous adenosine levels via inhibition of the equilibrative nucleoside transporter-12
• When added to ASA for up to 1 year after an ACS event, ticagrelor 90 mg bid reduced the rate of major adverse CV events, including CV death, as compared with clopidogrel 75 mg once daily, with an accrual of benefit over time3
• Building on these observations, the PEGASUS-TIMI 54 trial was designed to test the hypothesis that long-term therapy with ticagrelor added to low-dose ASA will reduce the risk of major adverse CV events in high-risk patients with a history of MI
331. Husted S et al. Eur Heart J 2006;27:1038–1047 2. Cattaneo M et al. J Am Coll Cardiol 2014;63:2503–2509 3. Wallentin L et al. N Engl J Med 2009;361:1045–1057

PEGASUS-TIMI 54: Study Organisation
34
TIMI Study Group Eugene Braunwald (Chair) Marc S Sabatine (Principal Investigator) Marc P Bonaca (Co-Principal Investigator) Stephen D Wiviott (CEC Chair) Suzanne Morin & Polly Fish (Operations) Sabina Murphy & Kelly Im (Statistics)
Executive Committee Eugene Braunwald (Chair) Marc S Sabatine Deepak L Bhatt Marc Cohen Ph Gabriel Steg Robert Storey
Sponsor: AstraZeneca Peter Held Eva Jensen Per Johanson Ann Maxe Ahlbom Barbro Boberg Olof Bengtsson
Independent Data Monitoring Committee Jeffrey L Anderson (Chair) Terje R Pedersen Freek WA Verheugt Harvey D White David L DeMets

PEGASUS-TIMI 54: Steering Committee
35
Argentina Germany RussiaR Diaz / E Paolasso C Hamm M RudaAustralia Hungary S. AfricaP Aylward R Kiss A DalbyBelgium Italy S. KoreaF Van der Werf D Ardissino K SeungBrazil Japan SlovakiaJ Nicolau S Goto G KamenskyBulgaria The Netherlands SpainA Goudev T Oude Ophuis J Lopez-SendonCanada Norway SwedenP Theroux F Kontny M DellborgChile Peru TurkeyR Corbalan F Medina S GuneriChina Philippines UK D Hu MT Abola R StoreyColombia Poland UkraineD Isaza A Budaj A ParkhomenkoCzech Republic Romania USAJ Spinar D Dimulescu Bonaca / Bhatt / CohenFranceG Montalescot / PG Steg

PEGASUS-TIMI 54: Study Design
Patients aged ≥50 years with a history of spontaneous MI 1–3 years prior to enrolment AND at least one additional atherothrombosis risk factor*
(N=21,162)
Ticagrelor 60 mg bid + ASA 75–150 mg/day
Minimum of 12 months’ follow up: Every 4 months in Year 1,
then semi-annually
Primary efficacy endpoint: CV death, MI or stroke Primary safety endpoint: TIMI-defined major bleeding
Placebo + ASA 75–150 mg/day
Ticagrelor 90 mg bid + ASA 75–150 mg/day
*Age ≥65 years, diabetes mellitus, second prior MI, multivessel CAD or chronic non-end stage renal disease bid, twice daily; CAD, coronary artery disease; TIMI, Thrombolysis in Myocardial Infarction
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 36

• Eligible patients were randomly assigned in a 1:1:1 ratio within each site to receive ticagrelor 90 mg bid, ticagrelor 60 mg bid, or placebo bid
– Randomisation was performed using a central computerised telephone or web-based system and allocation was double-blinded
• Two doses of ticagrelor were selected to study to the balance between ischaemic and bleeding risk in the chronic setting
– A lower intensity of antiplatelet therapy may be required than in the acute setting – Ticagrelor 90 mg bid
• The dose used in the PLATO study and is indicated for up to 12 months of treatment in ACS patients
– Ticagrelor 60 mg bid • Selected from PK/PD modelling suggesting that this dose will provide a lower level of platelet inhibition
than ticagrelor 90 mg bid, but greater mean platelet inhibition and less variability than clopidogrel 75 mg qd
• No ticagrelor loading dose was administered
PD, pharmacodynamics; PK, pharmacokinetics; qd, once daily
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
PEGASUS-TIMI 54: Randomisation and Ticagrelor Dosing
37

PEGASUS-TIMI 54: Concomitant Therapies
• All patients were recommended to be on standard secondary prevention therapy, including ASA at a dose of 75–150 mg daily – ASA dose was consistent with recommendations for secondary
prevention and with approved dosing labels for ticagrelor
• Additional antithrombotic therapy was prohibited
– Patients must have stopped study treatment for the duration of treatment with any other antithrombotic therapy
– Exception: Modified study treatment protocol
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 38

• A modified study treatment option (blinded double-dummy ticagrelor or clopidogrel) was provided to investigators for use if a patient developed an indication for P2Y12 receptor blockade and the investigator’s treatment choice would have been clopidogrel
– Patients originally randomised to either ticagrelor dose received • Ticagrelor 180 mg loading dose • Ticagrelor 90 mg bid maintenance dose
– Patients originally randomised to placebo received • Clopidogrel loading dose at the discretion of the treating physician • Recommended clopidogrel 75 mg qd maintenance dose
• The modified study treatment was administered for a period determined by the treating physician, after which the patient returned to their original randomised therapy
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
PEGASUS-TIMI 54: Modified Study Treatment Scenario (1)
39

PEGASUS-TIMI 54: Modified Study Treatment Scenario (2)
*LD at the discretion of the treating physician ADP, adenosine diphosphate; LD, loading dose
Bonaca MP et al. Am Heart J 2014;167:437–444
Ticagrelor 60 mg bid PlaceboTicagrelor 90 mg bid
Ticagrelor 90 mg bid Clopidogrel 75 mg qd
Indication for ADP receptor blockade
Ticagrelor 180 mg LD Clopidogrel LD*
40

PEGASUS-TIMI 54: Patients Undergoing Procedures
• Patients undergoing elective major non-CV procedures stopped study treatment 5 days before the procedure
– Treatment was resumed when deemed appropriate by the treating physician
– Periprocedural management of ASA was at the discretion of the treating physician
• Management of study treatment in the context of minor surgery or invasive procedures was at the discretion of the treating physician
Bonaca MP et al. Am Heart J 2014;167:437–444 41

PEGASUS-TIMI 54: Efficacy Endpoints
• Primary endpoint – Composite of CV death, MI or stroke
• Secondary endpoints – CV death – All-cause death
• Other prespecified exploratory endpoints – Composite of coronary heart disease death, MI or stroke – Individual components of the composite endpoints – Urgent coronary revascularisation – Hospitalisation for unstable angina – Transient ischaemic attack – Analyses of net clinical benefit
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] Data on file: ATLAS approval ID 691,431.011 42

PEGASUS-TIMI 54: Primary Safety Endpoint
• The primary safety endpoint was TIMI major bleeding, defined as
– Fatal bleeding (a bleeding event that directly led to death within 7 days)
– Any intracranial bleeding
OR
– Other TIMI major bleeding
• Clinically overt signs of haemorrhage associated with a drop in haemoglobin of ≥5 g/dL (when haemoglobin was not available, a fall in haematocrit of ≥15%)
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] Data on file: ATLAS approval ID 697,114.011 43

PEGASUS-TIMI 54: Other Safety Endpoints
• Other safety endpoints were – ICH
– Fatal bleeding
– TIMI minor bleeding
– Bleeding requiring transfusion
– Bleeding leading to study drug discontinuation
ICH, intracranial haemorrhage
Bonaca MP et al. Am Heart J 2014;167:437–444 Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 44

PEGASUS-TIMI 54: Statistical Methodology
• The primary efficacy analysis was conducted on an intention-to-treat basis, with each of the two doses individually compared to placebo, as a time to event analysis from randomisation to the first occurrence of any element of the primary composite endpoint
• Analysis of secondary endpoints proceeded in a hierarchical fashion starting with CV death and then all-cause death; additional endpoints were evaluated on an exploratory basis
• An exploratory analysis of both doses combined compared with placebo was also pre-specified
• Safety analyses included all randomised patients who received at least one dose of study drug and for whom post-dose data were available
• Safety was analysed as on-treatment, including all events occurring after the first dose and within 7 days after the last dose of study drug
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 45

PEGASUS-TIMI 54: Statistical Considerations
• To control the overall type I error, alpha was apportioned to each ticagrelor dose–placebo comparison and a Haybittle-Peto approach was employed to take into account an interim analysis of efficacy that was performed by the Independent Data Monitoring Committee
• Consequently a significance level of 0.026 was deemed to be indicative of statistical significance for the final analyses
• Event probabilities are expressed as Kaplan-Meier estimates of cumulative incidence at 36 months
– The median duration of follow up was 33 months (IQR 28–37), resulting in 56,004 patient-years of follow-up
• Hazard ratios and 95% confidence intervals were generated using a Cox proportional hazards model and all reported P values are two-sided
IQR, interquartile range
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 46

PEGASUS-TIMI 54: Study Patients and Study Drug
• In total, 21,162 patients were randomised between October 2010 and May 2013, from 1161 sites in 31 countries
• 20,942 patients (99.0%) received at least one dose of study drug
• The median time from the qualifying MI was 1.7 years
• 53.6% of the qualifying events were ST-elevation MIs
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 47

PEGASUS-TIMI 54: Global Enrolment
48
Randomized 10/2010 – 5/2013: 31 countries; 1161 sites; 21,162 patients
Poland: 1399Sweden: 507
Canada: 1306
United States:2601
UK: 647The Netherlands: 1560
Belgium: 431
Germany: 924France: 333
Spain: 535
Czech Rep: 870
Italy: 392
South Africa: 473
Australia: 327
Japan: 903Hungary: 831Bulgaria: 447
China: 383
S Korea: 506
Philippines: 250
Colombia: 528
Chile: 322
Argentina: 499
Brazil: 864Peru: 245
Romania: 404
Slovakia: 475
Russia: 1061Ukraine: 623
Turkey: 180
Norway: 336
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print]

PEGASUS-TIMI 54: Follow-up
IQR, interquartile range
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
Randomised 21,162 patients
Ticagrelor 60 mg bid (N=7045)
Follow-up median 33 months (IQR 28–37) Range 14–48 months
Placebo (N=7067)
Ticagrelor 90 mg bid (N=7050)
49
Premature permanent drug discontinuation n=2233 (32%) n=1999 (29%) n=1496 (21%)
Withdrew consent n=52 (0.7%) n=50 (0.7%) n=52 (0.7%)
Lost to follow-up n=3 (<0.1%) n=6 (<0.1%) n=1 (<0.1%)
Ascertainment for primary endpoint was complete for 99.2% of potential patient–years of follow-up

*Patients who prematurely discontinued study drug were followed for all safety and efficacy endpoints through to the end of the trial. The majority of premature discontinuations in the ticagrelor arms were because of adverse events **Includes patients who died after the Common Study End Date †No contact after the Common Study End Date or not listed in a death registry Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print]
Included in primary efficacy analysis (n=7067) Included in primary safety analysis (n=6996) • Excluded because never received study drug
(n=71)
Randomised to placebo (n=7067) • Received at least 1 dose (n=6996, 99%) • Never received a dose (n=71)
Premature permanent drug discontinuation* (n=1496, 21%) • Due to adverse event (n=784) • Due to patient decision (n=590) • Due to protocol issues (n=61) • Other (n=61)
Died during follow-up** (n=331, 4.7%) Withdrew consent (n=52, 0.7%) • Vital status known (n=47) • Not listed as dead in registry (n=4) • Vital status not searched (n=1) Lost to follow-up† (n=1, <0.1%)
Randomised to ticagrelor 90 mg bid (n=7050) • Received at least 1 dose (n=6988, 99%) • Never received a dose (n=62)
Randomised to ticagrelor 60 mg bid (n=7045) • Received at least 1 dose (n=6958, 99%) • Never received a dose (n=87)
Premature permanent drug discontinuation* (n=2233, 32%) • Due to adverse event (n=1434) • Due to patient decision (n=689) • Due to protocol issues (n=67) • Other (n=43)
Premature permanent drug discontinuation* (n=1999, 29%) • Due to adverse event (n=1257) • Due to patient decision (n=635) • Due to protocol issues (n=61) • Other (n=46)
Died during follow-up** (n=334, 4.7%) Withdrew consent (n=52, 0.7%) • Vital status known (n=48) • Not listed as dead in registry (n=3) • Vital status not searched (n=1) Lost to follow-up† (n=3, <0.1%)
Died during follow-up** (n=297, 4.2%) Withdrew consent (n=50, 0.7%) • Vital status known (n=46) • Not listed as dead in registry (n=2) • Vital status not searched (n=2) Lost to follow-up† (n=6, <0.1%)
Included in primary efficacy analysis (n=7050) Included in primary safety analysis (n=6988) • Excluded because never received study drug
(n=62)
Included in primary efficacy analysis (n=7045) Included in primary safety analysis (n=6958) • Excluded because never received study drug
(n=87)
Randomised(n=21,162)
PEGASUS-TIMI 54: CONSORT Diagram
50

PEGASUS-TIMI 54: Primary Endpoint
51CI, confidence interval; HR, hazard ratio
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
No. at risk Placebo 90 mg bid 60 mg bid
7067 7050 7045
6979 6973 6969
6892 6899 6905
6823 6827 6842
6761 6769 6784
6681 6719 6733
6508 6550 6557
6236 6272 6270
5876 5921 5904
5157 5243 5222
4343 4401 4424
3360 3368 3392
2028 2038 2055
Even
t rat
e (%
)
Months from randomisation
Ticagrelor 60 mg vs placebo HR 0.84 (95% CI 0.74–0.95) P=0.004
Ticagrelor 90 mg vs placebo HR 0.85 (95% CI 0.75–0.96) P=0.008
9.04% Placebo
7.85% 90 mg bid
7.77% 60 mg bid
Placebo Ticagrelor 90 mg bid Ticagrelor 60 mg bid
0 3 6 9 12 15 18 21 24 27 30 33 360
1
2
3
4
5
6
7
8
9
10

PEGASUS-TIMI 54: Efficacy Endpoints
*Indicates nominal P value; P<0.026 indicates statistical significance
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 52
Ticagrelor better Placebo better
0.4 0.6 0.8 1 1.25 1.67
Primary (CV death, MI or stroke)
CV death
MI
Stroke
Endpoint3-year KM event
rates (%)HR (95% CI) P valueTicagrelor Placebo
7.85 9.04 0.85 (0.75–0.96) 0.008 7.77 9.04 0.84 (0.74–0.95) 0.004 7.81 9.04 0.84 (0.76–0.94) 0.001
2.94 3.39 0.87 (0.71–1.06) 0.15 2.86 3.39 0.83 (0.68–1.01) 0.07 2.90 3.39 0.85 (0.71–1.00) 0.06
4.40 5.25 0.81 (0.69–0.95) 0.01* 4.53 5.25 0.84 (0.72–0.98) 0.03* 4.47 5.25 0.83 (0.72–0.95) 0.005*
1.61 1.94 0.82 (0.63–1.07) 0.14* 1.47 1.94 0.75 (0.57–0.98) 0.03* 1.54 1.94 0.78 (0.62–0.98) 0.03*
Ticagrelor 90 mg bid Ticagrelor 60 mg bid Ticagrelor pooled

EndpointTicagrelor 90 mg bid
N=7050; n (%)
Ticagrelor 60 mg bid
N=7045; n (%)Placebo
N=7067; n (%)
Ticagrelor 90 mg bid vs
placebo HR (95% CI)
Ticagrelor 60 mg bid vs
placebo HR (95% CI)
Primary endpoint
CV death, MI or stroke 493 (7.85) 487 (7.77) 578 (9.04) 0.85 (0.75–0.96)
P=0.0080.84 (0.74–0.95)
P=0.004Secondary endpoints
CV death 182 (2.94) 174 (2.86) 210 (3.39) 0.87 (0.71–1.06) P=0.15
0.83 (0.68–1.01) P=0.07
Death from any cause 326 (5.15) 289 (4.69) 326 (5.16) 1.00 (0.86–1.16)
P=0.99*0.89 (0.76–1.04)
P=0.14*Other efficacy endpoints
MI 275 (4.40) 285 (4.53) 338 (5.25) 0.81 (0.69–0.95) P=0.01*
0.84 (0.72–0.98) P=0.03*
All stroke 100 (1.61) 91 (1.47) 122 (1.94) 0.82 (0.63–1.07) P=0.14*
0.75 (0.57–0.98) P=0.03*
Ischaemic stroke 88 (1.41) 78 (1.28) 103 (1.65) 0.85 (0.64–1.14) P=0.28*
0.76 (0.56–1.02) P=0.06*
PEGASUS-TIMI 54: Efficacy Endpoints
*Indicates nominal P value; P<0.026 indicates statistical significance Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 53

EndpointTicagrelor 90 mg bid
N=7050; n (%)
Ticagrelor 60 mg bid
N=7045; n (%)Placebo
N=7067; n (%)
Ticagrelor 90 mg bid vs
placebo HR (95% CI)
Ticagrelor 60 mg bid vs
placebo HR (95% CI)
Other efficacy endpointsCoronary heart disease death 97 (1.53) 106 (1.72) 132 (2.08) 0.73 (0.56–0.95)
P=0.02*0.80 (0.62–1.04)
P=0.09*
Coronary heart disease death, MI, or stroke
438 (6.99) 445 (7.09) 535 (8.33) 0.82 (0.72–0.93) P=0.002*
0.83 (0.73–0.94) P=0.003*
CV death or MI 424 (6.79) 422 (6.77) 497 (7.81) 0.85 (0.75–0.97) P=0.01*
0.85 (0.74–0.96) P=0.01*
Coronary heart disease death or MI 350 (5.59) 360 (5.75) 429 (6.68) 0.81 (0.71–0.94)
P=0.004*0.84 (0.73–0.96)
P=0.01*
Hospitalisation for unstable angina 33 (0.50) 39 (0.61) 37 (0.57) 0.89 (0.56–1.43)
P=0.63*1.05 (0.67–1.65)
P=0.82*
Urgent coronary revascularisation for unstable angina
74 (1.16) 62 (0.95) 76 (1.13) 0.97 (0.71–1.34) P=0.87*
0.82 (0.58–1.14) P=0.24*
Transient ischaemic attack 17 (0.27) 17 (0.27) 17 (0.29) 1.00 (0.51–1.96)
P=1.00*1.00 (0.51–1.96)
P=1.00*
PEGASUS-TIMI 54: Efficacy Endpoints
*Indicates nominal P value; P<0.026 indicates statistical significance Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 54

All patients 21,162 7.85 7.77 9.04 0.85 (0.75–0.96)
0.84 (0.74–0.95)
Age at randomisation 0.09 0.50
<75 years 18,079 6.77 7.23 8.27 0.80 (0.70–0.92)
0.86 (0.75–0.98)
≥75 years 3083 13.94 11.02 13.50 1.02 (0.80–1.30)
0.77 (0.59–1.01)
Sex 0.21 0.12
Female 5060 6.67 9.03 9.15 0.74 (0.57–0.95)
0.98 (0.78–1.24)
Male 16,102 8.23 7.37 8.99 0.89 (0.77–1.02)
0.79 (0.69–0.91)
Qualifying MI 0.32 0.67
NSTEMI 8583 9.53 9.32 10.14 0.92 (0.77–1.09)
0.89 (0.74–1.06)
STEMI 11,329 6.52 6.43 7.83 0.81 (0.68–0.97)
0.81 (0.68–0.97)
Unknown 1223 7.78 9.46 12.34 0.65 (0.41–1.03)
0.74 (0.48–1.13)
Time from qualifying MI 0.58 0.09
<2 years 12,980 8.15 7.79 9.74 0.83 (0.71–0.96)
0.77 (0.66–0.90)
≥2 years 8155 7.33 7.76 7.94 0.89 (0.73–1.08)
0.96 (0.79–1.17)
History of diabetes 0.97 0.96
Diabetes 6806 10.14 10.00 11.60 0.85 (0.71–1.03)
0.83 (0.69–1.00)
No diabetes 14,355 6.77 6.68 7.83 0.85 (0.73–0.99)
0.84 (0.72–0.98)
PEGASUS-TIMI 54: Primary Endpoint* by Subgroup (1)
*Composite of CV death, MI or strokeKM, Kaplan-Meier
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
Subgroup Patients Ticagrelor 90 mg 3-year KM (%)
Ticagrelor 60 mg 3-year KM (%)
Placebo 3-year KM
(%)
HR (95% CI) ticagrelor
90 mg bid vs placebo
HR (95% CI)
Interaction P value
HR (95% CI) ticagrelor 60
mg bid vs placebo
HR (95% CI)
Interaction P value
Ticagrelor 90 mg better Ticagrelor 60 mg betterPlacebo better Placebo better0.4 0.5 0.85 1 1.5 2.0 2.50.4 0.5 0.85 1 1.5 2.0 2.5
55

All patients 21,162 7.85 7.77 9.04 0.85 (0.75–0.96)
0.84 (0.74–0.95)
ASA dose 0.64 0.80
≤75 mg 4182 7.52 7.73 9.23 0.80 (0.61–1.05)
0.82 (0.63–1.07)
>75 mg 16,950 7.89 7.79 8.93 0.86 (0.75–0.99)
0.85 (0.74–0.97)
History of PCI 0.88 0.72
Prior PCI 17,568 7.20 6.87 8.09 0.86 (0.74–0.98)
0.83 (0.72–0.96)
No prior PCI 3591 10.97 12.06 13.44 0.84 (0.66–1.07)
0.87 (0.69–1.11)
Region 0.99 0.83
North America 3907 9.12 7.79 9.77 0.86 (0.66–1.13)
0.75 (0.57–0.99)
South America 2458 8.60 9.94 9.75 0.83 (0.60–1.16)
0.90 (0.65–1.24)
Europe 12,428 7.64 7.54 8.96 0.85 (0.73–1.00)
0.85 (0.72–0.99)
Asia 2369 6.08 7.11 6.86 0.82 (0.54–1.23)
0.90 (0.60–1.34)
PEGASUS-TIMI 54: Primary Endpoint* by Subgroup (2)
Subgroup Patients Ticagrelor 90 mg 3-year KM (%)
Ticagrelor 60 mg 3-year KM (%)
Placebo 3-year KM
(%)
HR (95% CI) ticagrelor
90 mg bid vs placebo
HR (95% CI)
Interaction P value
HR (95% CI) ticagrelor 60
mg bid vs placebo
HR (95% CI)
Interaction P value
Ticagrelor 90 mg better Ticagrelor 60 mg betterPlacebo better Placebo better0.4 0.5 0.85 1 1.5 2.0 2.50.4 0.5 0.85 1 1.5 2.0 2.5
56*Composite of CV death, MI or stroke
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

All patients 21,162 7.85 7.77 9.04 0.85 (0.75–0.96)
0.84 (0.74–0.95)
Race 0.49 0.12
Caucasian 18,327 8.10 7.61 9.15 0.86 (0.76–0.98)
0.81 (0.71–0.92)
Non-Caucasian 2835 5.88 8.78 8.32 0.75 (0.53–1.08)
1.07 (0.77–1.48)
Weight 0.16 0.18
< Median (81 kg) 10,550 7.66 7.62 9.38 0.78 (0.66–0.92)
0.77 (0.65–0.92)
≥ Median (81 kg) 10,581 7.97 7.89 8.69 0.93 (0.78–1.10)
0.91 (0.77–1.08)
Second prior MI 0.54 0.88
Second MI 3499 14.68 13.65 15.21 0.90 (0.72–1.13)
0.85 (0.68–1.06)
No second MI 17,662 6.53 6.59 7.79 0.83 (0.72–0.96)
0.83 (0.72–0.96)
Multivessel disease 0.79 0.55
Multivessel disease
12,558 8.07 7.80 9.37 0.84 (0.72–0.98)
0.81 (0.70–0.95)
No multivessel disease
8600 7.51 7.69 8.57 0.87 (0.72–1.05)
0.88 (0.72–1.06)
Non-endstage renal dysfunction 0.48 0.54
Renal dysfunction
4849 11.26 11.31 14.00 0.81 (0.66–0.99)
0.81 (0.66–0.99)
No renaldysfunction
16,049 6.81 6.79 7.43 0.88 (0.76–1.03)
0.88 (0.76–1.02)
PEGASUS-TIMI 54: Primary Endpoint* by Subgroup (3)
Subgroup Patients Ticagrelor 90 mg 3-year KM (%)
Ticagrelor 60 mg 3-year KM (%)
Placebo 3-year KM
(%)
HR (95% CI) ticagrelor
90 mg bid vs placebo
HR (95% CI)
Interaction P value
HR (95% CI) ticagrelor 60
mg bid vs placebo
HR (95% CI)
Interaction P value
0.4 0.5 0.85 1 1.5 2.0 2.5 0.4 0.5 0.85 1 1.5 2.0 2.5
Ticagrelor 90 mg better Ticagrelor 60 mg betterPlacebo better Placebo better
57
*Composite of CV death, MI or stroke n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

EndpointTicagrelor 90 mg bid
N=6988; n (%)
Ticagrelor 60 mg bid
N=6958; n (%)
Placebo N=6996; n (%)
Ticagrelor 90 mg bid vs
placebo HR (95% CI)
Ticagrelor 60 mg bid vs
placebo HR (95% CI)
Primary safety endpoint
TIMI major bleeding 127 (2.60) 115 (2.30) 54 (1.06) 2.69 (1.96–3.70)P<0.001
2.32 (1.68–3.21)P<0.001
Secondary safety endpoints
ICH 29 (0.56) 28 (0.61) 23 (0.47) 1.44 (0.83–2.49)P=0.19
1.33 (0.77–2.31)P=0.31
Haemorrhagic stroke 4 (0.07) 8 (0.19) 9 (0.19) 0.51 (0.16–1.64)P=0.26
0.97 (0.37–2.51)P=0.94
Fatal bleeding 6 (0.11) 11 (0.25) 12 (0.26) 0.58 (0.22–1.54) P=0.27
1.00 (0.44–2.27) P=1.00
Fatal bleeding or non-fatal ICH
32 (0.63) 33 (0.71) 30 (0.60) 1.22 (0.74–2.01) P=0.43
1.20 (0.73–1.97) P=0.47
PEGASUS-TIMI 54: Safety Endpoints
Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events P<0.026 indicates statistical significance
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 58

EndpointTicagrelor 90 mg bid
N=6988; n (%)
Ticagrelor 60 mg bid
N=6958; n (%)
Placebo N=6996; n (%)
Ticagrelor 90 mg bid vs
placebo HR (95% CI)
Ticagrelor 60 mg bid vs
placebo HR (95% CI)
Secondary safety endpoints
TIMI minor bleeding 66 (1.31) 55 (1.18) 18 (0.36) 4.15 (2.47–7.00) P<0.001
3.31 (1.94–5.63) P<0.001
Bleeding requiring transfusion
122 (2.43) 105 (2.09) 37 (0.72) 3.75 (2.59–5.42) P<0.001
3.08 (2.12–4.48) P<0.001
Bleeding leading to study drug discontinuation
453 (7.81) 354 (6.15) 86 (1.50) 5.79 (4.60–7.29) P<0.001
4.40 (3.48–5.57) P<0.001
PEGASUS-TIMI 54: Safety Endpoints
59
Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events P<0.026 indicates statistical significance
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

PEGASUS-TIMI 54: Bleeding
0
1.25
2.5
3.75
5
TIMI major bleeding Fatal bleeding or ICH Fatal bleeding
Ticagrelor 90 mg bidTicagrelor 60 mg bidPlacebo
60
3-ye
ar K
M e
vent
rate
2.62.3
1.11.3 1.2
0.40.6 0.7 0.6 0.6 0.6 0.5
0.1 0.3 0.3
Rates are presented as 3-year Kaplan-Meier estimates P<0.026 indicates statistical significance
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]
P<0.001
P<0.001P=NS P=NS P=NS

All patients 20,942 2.60 2.30 1.06 2.69 (1.96–3.70)
2.32 (1.68–3.21)
Age at randomisation 0.70 0.84
<75 years 17,905 2.30 2.05 0.96 2.63 (1.83–3.78)
2.30 (1.60–3.32)
≥75 years 3037 4.81 4.11 1.68 3.06 (1.56–5.99)
2.50 (1.25–4.97)
Sex 0.67 0.79
Female 5003 2.10 2.25 1.06 2.34 (1.16–4.70)
2.51 (1.27–4.98)
Male 15,939 2.75 2.31 1.06 2.78 (1.94–3.97)
2.27 (1.57–3.27)
Qualifying MI 0.49 0.54
NSTEMI 8496 2.43 2.67 1.08 2.58 (1.56–4.26)
2.56 (1.56–4.23)
STEMI 11,216 2.76 2.06 0.95 3.11 (1.99–4.88)
2.42 (1.52–3.84)
Unknown 1207 2.37 2.05 1.46 1.49 (0.45–4.89)
1.26 (0.38–4.12)
Time from qualifying MI 0.07 0.23
<2 years 12,841 2.42 2.36 1.24 2.18 (1.48–3.23)
2.05 (1.38–3.03)
≥2 years 8078 2.89 2.23 0.72 4.15 (2.34–7.36)
3.17 (1.76–5.70)
History of diabetes 0.99 0.79
Diabetes 6735 2.62 2.51 0.98 2.67 (1.52–4.71)
2.47 (1.40–4.35)
No diabetes 14,207 2.59 2.20 1.09 2.70 (1.84–3.97)
2.25 (1.52–3.33)
PEGASUS-TIMI 54: Primary Safety Endpoint* by Subgroup (1)
*TIMI major bleeding
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print]
Subgroup Patients Ticagrelor 90 mg 3-year KM (%)
Ticagrelor 60 mg 3-year KM (%)
Placebo 3-year KM
(%)
HR (95% CI) ticagrelor
90 mg bid vs placebo
HR (95% CI)
Interaction P value
HR (95% CI) ticagrelor 60
mg bid vs placebo
HR (95% CI)
Interaction P value
Ticagrelor 90 mg better Placebo better0.1 0.4 0.75 1 1.25 2.5 10
Ticagrelor 60 mg better Placebo better0.1 0.4 0.75 1 1.25 2.5 10
61

All patients 20,942 2.60 2.30 1.06 2.69 (1.96–3.70)
2.32 (1.68–3.21)
ASA dose 0.52 0.53
≤75 mg 4157 2.41 1.40 0.70 3.35 (1.57–7.14)
1.81 (0.79–4.13)
>75 mg 16,761 2.67 2.55 1.16 2.56 (1.80–3.64)
2.43 (1.71–3.45)
History of PCI 0.68 0.56
Prior PCI 17,379 2.63 2.44 1.06 2.76 (1.95–3.91)
2.42 (1.70–3.44)
No prior PCI 3562 2.47 1.63 1.04 2.31 (1.05–5.11)
1.85 (0.81–4.22)
Region 0.92 0.65
North America 3865 3.10 3.61 1.38 2.33 (1.16–4.65)
2.67 (1.36–5.23)
South America 2439 3.50 1.99 1.09 3.39 (1.44–7.97)
1.60 (0.61–4.21)
Europe 12,305 2.23 1.72 0.88 2.75 (1.76–4.31)
2.09 (1.31–3.32)
Asia 2333 2.97 3.74 1.44 2.37 (1.02–5.50)
3.23 (1.45–7.18)
PEGASUS-TIMI 54: Primary Safety Endpoint* by Subgroup (2)
Subgroup Patients Ticagrelor 90 mg 3-year KM (%)
Ticagrelor 60 mg 3-year KM (%)
Placebo 3-year KM
(%)
HR (95% CI) ticagrelor
90 mg bid vs placebo
HR (95% CI)
Interaction P value
HR (95% CI) ticagrelor 60
mg bid vs placebo
HR (95% CI)
Interaction P value
Ticagrelor 90 mg better Placebo better0.1 0.4 0.75 1 1.25 2.5 10
Ticagrelor 60 mg better Placebo better0.1 0.4 0.75 1 1.25 2.5 10
62*TIMI major bleeding
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print]

All patients 20,942 2.60 2.30 1.06 2.69 (1.96–3.70)
2.32 (1.68–3.21)
Race 0.65 0.14
Caucasian 18,151 2.54 2.09 1.06 2.61 (1.85–3.68)
2.06 (1.44–2.93)
Non-Caucasian 2791 3.01 3.57 1.01 3.22 (1.36–7.60)
4.04 (1.76–9.29)
Weight 0.46 0.23
< Median (81 kg) 10,429 2.84 2.39 1.28 2.43 (1.61–3.67)
1.95 (1.27–2.99)
≥ Median (81 kg) 10,497 2.36 2.21 0.83 3.11 (1.88–5.12)
2.91 (1.76–4.79)
Second prior MI 0.57 0.20
Second MI 3461 2.27 3.17 0.72 3.46 (1.46–8.19)
3.82 (1.65–8.87)
No second MI 17,481 2.67 2.13 1.12 2.58 (1.83–3.64)
2.10 (1.48–2.99)
Multivessel disease 0.96 0.26
Multivessel disease
12,423 2.45 2.58 1.08 2.66 (1.75–4.05)
2.68 (1.77–4.07)
No multivessel disease
8519 2.83 1.91 1.03 2.72 (1.67–4.43)
1.83 (1.09–3.07)
Non-endstage renal dysfunction 0.11 0.99
Renal dysfunction
4788 2.13 2.94 1.34 1.69 (0.89–3.19)
2.29 (1.25–4.19)
No renaldysfunction
15,934 2.74 2.09 0.99 3.05 (2.10–4.43)
2.29 (1.56–3.36)
PEGASUS-TIMI 54: Primary Safety Endpoint* by Subgroup (3)
Subgroup Patients Ticagrelor 90 mg 3-year KM (%)
Ticagrelor 60 mg 3-year KM (%)
Placebo 3-year KM
(%)
HR (95% CI) ticagrelor
90 mg bid vs placebo
HR (95% CI)
Interaction P value
HR (95% CI) ticagrelor 60
mg bid vs placebo
HR (95% CI)
Interaction P value
Ticagrelor 90 mg better Ticagrelor 60 mg betterPlacebo better Placebo better0.1 0.4 0.75 1 1.25 2.5 100.1 0.4 0.75 1 1.25 2.5 10
63*TIMI major bleeding
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print]

PEGASUS-TIMI 54: Numbers needed to treat and numbers needed to harm
64
Ticagrelor 90 mg bid Ticagrelor 60 mg bid
Efficacy endpoint ARR NNT ARR NNT Primary endpoint: CV death, MI or stroke 1.19% 84 1.27% 79
CV death 0.45% 222 0.53% 189
MI 0.85% 118 0.72% 139
Stroke 0.33% 303 0.47% 213
Safety endpoint ARI NNH ARI NNH
Primary safety endpoint: TIMI major bleeding 1.54% 65 1.24% 81
ICH 0.09% 1111 0.14% 714
Fatal bleeding -0.15% N/A -0.01% N/A
ARRs/ARIs based on 3-year KM event rates NNT/NNH calculated as 100/ARR or ARI, as described by Laupacis A N Engl J Med 1988;318:1728–1733 ARR, actual risk reduction; ARI, actual risk increase; NNH, number needed to harm; NNT, number needed to treat
Calculated from Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

PEGASUS-TIMI 54: Analyses of Net Clinical Benefit
65
Ticagrelor 90 mg bid versus placebo Ticagrelor 60 mg bid versus placebo
Characteristic RRR HR (95%CI) P value RRR HR (95%CI) P value
Net clinical benefit: CV death, MI, stroke, or TIMI major bleeding
0% 1.00 (0.90–1.22)
0.9563 5% 0.95 (0.85–1.06)
0.3412
Irreversible harm: CV death, MI, stroke, ICH and fatal bleeding
12% 0.88 (0.78–0.99)
0.0372 14% 0.86 (0.77–0.97)
0.0160
Rates are annualised from 3-year Kaplan-Meier event rates in the intention-to-treat population RRR, relative risk reduction
*Data on file: ATLAS approval ID 691,431.011

Ticagrelor 90 mg bid
N=6988; n (%)
Ticagrelor 60 mg bid
N=6958; n (%)
Placebo N=6996; n (%)
Ticagrelor 90 mg bid vs
placebo HR (95% CI)
Ticagrelor 60 mg bid vs
placebo HR (95% CI)
Dyspnoea
Adverse event 1205 (18.93) 987 (15.84) 383 (6.38) 3.55 (3.16–3.98) P<0.001
2.81 (2.50–3.17) P<0.001
Leading to study drug discontinuation
430 (6.50) 297 (4.55) 51 (0.79) 8.89 (6.65–11.88) P<0.001
6.06 (4.50–8.15) P<0.001
Serious adverse event 22 (0.41) 23 (0.45) 9 (0.15) 2.68 (1.24–5.83) P=0.01
2.70 (1.25–5.84) P=0.01
PEGASUS-TIMI 54: Dyspnoea
Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 66

PEGASUS-TIMI 54: Dyspnoea
• The majority of patients with dyspnoea AEs had only one episode regardless of treatment group1
• The majority of episodes with ticagrelor were either mild (58%) or moderate (37%) in severity2
• The pattern of dyspnoea AEs, SAEs and discontinuations due to AEs in the ticagrelor groups compared with the placebo group was similar for patients with a medical history of asthma or COPD compared with patients without1
• Patients who had dyspnoea AEs tended to be older and more frequently had dyspnoea, asthma, or COPD at baseline; the characteristics of those patients with dyspnoea AEs were similar between treatment groups1
67
AE, adverse event; COPD, chronic obstructive pulmonary disease; SAEs, serious adverse events
1. Data on file: ATLAS approval ID 691,524.011 2. Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

EndpointTicagrelor 90 mg bid
N=6988; n (%)
Ticagrelor 60 mg bid
N=6958; n (%)Placebo
N=6996; n (%)
Ticagrelor 90 mg bid vs
placebo HR (95% CI)
Ticagrelor 60 mg bid vs
placebo HR (95% CI)
Renal AE* 166 (3.30) 173 (3.43) 161 (2.89) 1.17 (0.94–1.46) P=0.15
1.17 (0.94–1.45) P=0.15
Bradyarrhythmia AE 107 (2.04) 121 (2.32) 106 (1.98) 1.15 (0.88–1.50) P=0.31
1.24 (0.96–1.61) P=0.10
Gout AE** 115 (2.28) 101 (1.97) 74 (1.51) 1.77 (1.32–2.37) P<0.001
1.48 (1.10–2.00) P=0.01
PEGASUS-TIMI 54: Other Safety Endpoints
*The most common renal AEs were; elevations in blood creatinine, acute renal failure, renal failure, renal dysfunction and proteinurea. Event rates were similar across treatment groups **Gout AEs were assessed by the investigator as being predominantly mild to moderate in intensity. The number of gout AEs of severe intensity were balanced across the treatment groups Rates are presented as 3-year Kaplan-Meier estimates n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 68

Adverse events Ticagrelor 90 mg bid N=6988; n (%)
Ticagrelor 60 mg bid N=6958; n (%)
Placebo N=6996; n (%)
Any AE (serious and non-serious)* 5375 (76.9) 5311 (76.3) 4899 (70.0)
Leading to discontinuation of study drug* 1326 (19.0) 1139 (16.4) 621 (8.9)
Most common AEs leading to discontinuation Bleeding** 453 (6.5) 354 (5.1) 86 (1.2)
Dyspnoea 430 (6.2) 297 (4.3) 51 (0.7)
Arrhythmia 78 (1.1) 103 (1.5) 96 (1.4)
Any SAE 1648 (23.6) 1650 (23.7) 1676 (24.0)
Leading to discontinuation of study drug 271 (3.9) 273 (3.9) 231 (3.3)
PEGASUS-TIMI 54: Adverse Events
*Excludes patients who stopped drug because of an efficacy event with no associated bleeding **Bleeding as confirmed by the Clinical Events Committee n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print] 69

Adverse Event Ticagrelor 90 mg bid N=7050; n (%)
Ticagrelor 60 mg bid N=7045; n (%)
Placebo N=7067; n (%)
All-cause death 336 (4.8) 299 (4.2) 336 (4.8)
Non-cardiovascular death 145 (2.1) 117 (1.7) 115 (1.6)
Accident/trauma 6 (0.09) 2 (0.03) 4 (0.06)
Infection/sepsis 31 (0.44) 25 (0.36) 24 (0.34)
Malignancy 77 (1.10) 64 (0.92) 53 (0.76)
Pulmonary failure 10 (0.14) 9 (0.13) 9 (0.13)
Renal failure 2 (0.03) 4 (0.06) 4 (0.06)
Other 19 (0.27) 13 (0.19) 21 (0.30)
PEGASUS-TIMI 54: Non-CV Deaths
Includes deaths occurring after the common study end date (safety window) Data presented as proportions n = number of patients with events, not the number of events
Bonaca MP et al. N Engl J Med 2015, Supplementary Appendix [Epub ahead of print] 70

PEGASUS-TIMI 54: Summary
• The PEGASUS-TIMI 54 study demonstrated that the addition of ticagrelor 60 mg bid or 90 mg bid to low-dose ASA in patients 1–3 years after a MI significantly reduced the risk of the primary endpoint of CV death, MI or stroke
• A directionally consistent effect was observed on all components of the primary endpoint, including CV death
• The benefit of ticagrelor was consistent among major clinical subgroups and by region and continued to accrue over time with a median of 33 months of follow-up
• The rate of the primary safety endpoint of TIMI major bleeding was higher with both doses of ticagrelor compared with placebo
• The rate of fatal bleeding or non-fatal intracranial haemorrhage was low (<1% at 3 years) and did not differ between treatment arms
• Dyspnoea was more frequent with both doses of ticagrelor; however, the majority of episodes with either dose were characterised as either mild (58.1%) or moderate (36.9%) in severity
71Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print]

PEGASUS-TIMI 54: Conclusions
• Patients who have had a MI remain at heightened risk for ischaemic events over the long term1–3
• PEGASUS-TIMI 54 is the first prospective, randomised controlled clinical trial appropriately powered to demonstrate the benefit of long-term DAPT in patients with prior MI4
• Coupled with the established benefit of ticagrelor in the setting of ACS, these data support consideration of long-term antiplatelet therapy with ticagrelor plus low-dose ASA, in appropriately selected patients with prior MI4
1. Bhatt DL et al. JAMA 2010;304:1350–1357 2. Fox KA et al. Eur Heart J 2010;31:2755–2764 3. Jernberg T et al. Eur Heart J 2015; pii: ehu505. [Epub ahead of print] 4. Bonaca MP et al. N Engl J Med 2015 [Epub ahead of print] 72

FOR REACTIVE MEDICAL USE ONLY