Headache Update - Continuing Medical Education - … H. Ahn, MD PhD Departments of Neurology and...
55
Andrew H. Ahn, MD PhD Departments of Neurology and Anatomy University of California San Francisco Advances in Internal Medicine May 21, 2009 Headache Update
Transcript of Headache Update - Continuing Medical Education - … H. Ahn, MD PhD Departments of Neurology and...

Andrew H. Ahn, MD PhDDepartments of Neurology and Anatomy
University of California San Francisco
Advances in Internal MedicineMay 21, 2009
Headache Update

Overview
Migraine as systems neurobiology
Φ Clinical features
Φ Neurobiological mechanisms
Mechanisms of triptan action
Φ Triptan receptors in PNS and CNS
Φ Modulation of pain circuits
The near future of headache care
Φ CGRP receptor antagonists

France 400 BCNeolithic c. 7000 BC
Case study* (HIPAA compliant)

France 400 BCNeolithic c. 7000 BC
Case study* (HIPAA compliant)
* Headache is not an FDA-approved indication for trephanation

Why Migraine Matters
Migraine is a common disabling disorderYearly prevalence 36 million people (US 2005)18 % of women6 % of men19% of veterans of conflicts in Iraq and Afghanistan
Migraine has a high social cost$31 billion lost productivity
Migraine complicationsPain and disabilityOverdose and dependenceCo-morbid with other pain and medical disordersCo-morbid psychiatric disease

Migraine: A multi-system disorder
∴ Episodic, lasting hours to days
∴ PainModerate to severeUnilateralPulsating, throbbingAggravation with routine activityAllodynia
∴ Neurologic featuresAuraPhotophobia PhonophobiaNausea, vomitingVertigo Slurred speech, somnolence
Based on the Headache Classification Committee of the International Headache Society, 2nd Ed. Cephalalgia 2004

Theories of migraine: an overview
Cortical spreading depressionThe “vascular hypothesis”Central sensitizationBrainstem dysfunctionMigraine geneticsNeurochemical circuits

Environment
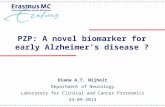
Theories of migraine: a theoretical framework
Neurogenicinflammation
Cortical hyperexcitability
Brainstem dysfunction
Trigeminal excitation(CGRP, glutamate) HEADACHE
+
+
Genetic predisposition
Initiation
Generation/perpetuation
Adapted from Pietrobon Neuroscientist. 2005
Centralsensitization
Peripheralsensitization
+
+

K.S. Lashley, 1941
Theories of migraine: a cortical disorder?

K.S. Lashley, 1941
Theories of migraine: a cortical disorder?

K.S. Lashley, 1941
Theories of migraine: a cortical disorder?

K.S. Lashley, 1941
Theories of migraine: a cortical disorder?

K.S. Lashley, 1941
Theories of migraine: a cortical disorder?

A.A.P. Leao, 1944 Neuronal correlate of aura?
1234567
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

A.A.P. Leao, 1944
stimulus1234567
Neuronal correlate of aura?
Theories of migraine: cortical spreading depression

Woods et al, 1994
Perfusion disturbances in a spontaneous migraine
spreading oligemia

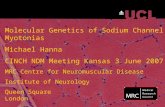
Graham and Wolff, 1938
BP systolic
BP diastolic
TA pulsations
headache
minutes0 10 20 30 40 50 60
Theories of migraine: the vascular hypothesis

FHM: Familial Hemiplegic Migraine
Disorder Gene ProteinFHM-I CACNA1A P/Q Ca2+ channel
FHM-II ATP1A2 Na+/K+-ATPase
FHM-III SCN1A Na+ channel
Theories of migraine: ion channel dysfunction

Substance P and CGRP are “pain” neurotransmitters
Theories of migraine: neuoromodulation

Venous CGRP may be a biomarker of headache
CGRP is a mediator of peripheral inflammation and painEdvinsson and Uddman Brain Res Rev 2005
- no change from before headache.↑ significant increase in neuropeptide level.
VIP Substance P CGRPMigraine without aura - - ↑
Migraine with aura - - ↑
Trigeminal neuralgia - - ↑
Cluster headache ↑ - ↑
Chronic paroxysmal headache
↑ - ↑

CGRP antagonists abort migraine attacks*
BIBN4096 BS reduces migraine pain* Not FDA approved for any clinical application
Olesen et al, NEJM 2004

Analgesics: ASA, APAP, ibuprofen, indomethacin
Opiates: morphine, codeine, meperidine
Phenothiazines: chlorpromazine
Acetazolamide
Ergots: ergotamine, DHE-45
Serotonin (5-HT) sub-selective agonists (triptans):5HT1B, 5HT1D, 5HT1F receptorssuma nara almo ele frova riza zolmi
Theories of migraine: follow the triptans

Triptans activate receptors at multiple sites
5HT = serotonin receptor subtypesGoadsby NEJM 2002

5HT1D Substance P
Bergerot Eur J Neurosci 2006
5HT1D receptors on “pain responsive” afferents
Ahn, unpublished

The classical pain pathway
From Fields Nature Rev Neurosci, 2004
Somatosensory cortex
Insular cortex
Thalamus
Anterolateral tract
Tissue injury

Functional imaging of pain
A distributed representation of painApkarian et al Eur J Pain 2005

Ascending and descending pain pathways
Opiates modulate both afferent and efferent responses to painAdapted from Fields Nature Rev Neurosci, 2004

Potential areas of triptan pain modulationAdapted from Fields Nature Rev Neurosci, 2004
Triptan actions on modulatory pathways

5HT1D receptor terminals within the central nucleus of the amygdala
5HT1D AChE
BLA
CeA
Ahn et al, in preparation

5HT1D receptor terminals within the central nucleus of the amygdala
5HT1D receptorSERT - 5HT vesicular transporter
Ahn et al, in preparation

5HT1D receptor terminals within the central nucleus of the amygdala
5HT1D receptor CGRP
Ahn et al, in preparation

CGRP
5HT1B
5HT1
D
5HT1F

5HT1D receptors in the rat thalamus after ICV colchicine
5-HT1D receptor CGRP
5-HT1D receptor in SPF and SPFFCAhn et al, in preparation

The central amygdala in pain processing
∴ Affective and nociceptive circuits through CeASpino-parabrachio-amygdaloid pathwayMulti-modal connections to lateral (LA) and basolateral (BLA)CGRP: nociceptive and enteroceptive input
∴ Amygdala plays a central role in nociceptive processingEmotional learning - Fear conditioning“Nociceptive amygdala” in arthritic painConditioned place aversion
∴ Modulation of mood and anxiety

CGRP receptor antagonists in amygdala reduce pain-evoked responses
Pain alters synaptic plasticity in CeA at post-synaptic sites blocked by CGRP antagonistsHan et al, J Neurosci 2005

Headache Treatment Horizon
υ CGRP receptor antagonists
υ Occipital nerve stimulation

Why Headache Treatment Fails
υ Diagnosis is incomplete or incorrect
υ Important exacerbating factors were missed
υ Pharmacotherapy is inadequate
υ Non-pharmacologic interventions are
inadequate
υ Other factors: co-morbidity, unrealistic
expectations, psychiatric disease
Lipton, Silberstein, Saper, Bigal, Goadsby. Neurology Apr 8;60(7):1064-70 (2003)

Re-evaluation of the diagnosis I
Lipton, Silberstein, Saper, Bigal, Goadsby. Neurology Apr 8;60(7):1064-70 (2003)
ν Secondary Headache Disordersυ Giant Cell Arteritisυ Carotid dissectionυ High- and low-pressure headachesυ Chronic sphenoid sinusitisυ Nasopharyngeal carcinomaυ Chronic infection (Lyme, HIV)υ Metabolic disorders (hepatic, renal,
endocrine)υ Mediastinal process (angina, lesion, SVC)υ Ocular disturbancesυ Dental, mandibular joint pain

Re-evaluation of the diagnosis II
Lipton, Silberstein, Saper, Bigal, Goadsby. Neurology Apr 8;60(7):1064-70 (2003)
ν Primary Headache Disorders υ Medication Overuse Headacheυ Chronic Tension Type Headacheυ Cluster-migraine disorder
ν Primary Headache Disorders (rare)υ Hemicrania continua (indomethacin)υ Paroxysmal hemicrania (short, frequent,
indomethacin)υ Hypnic headache (elderly, <30min, Li, mel, caff,
verap)υ New daily persistent headache

What is a Chronic Daily Headache?
ν The International Classification of Headache Disorders, second edition (2003)
υ Greater than 15 headache days per month

Medication Overuse Headache
υ The most common cause of chronic migrainous headache
υ Mixed migraine-like and tension-type-like headache
υ Associated with overuse of migraine drugs or analgesics
υ Highest risk in 3 or more treatment days per week
υ Applies to ergotamines, triptans, analgesics, opioids, combination medications

Exacerbating factors in CDH
Lipton, Silberstein, Saper, Bigal, Goadsby. Neurology Apr 8;60(7):1064-70 (2003)
υ Medication overuse headache (rebound)
υ Chronic cervical strain
υ Caffeine overuse
υ Other medications (NTG, retin-A)
υ Over-the-counter preparations (Valerian, Vit A, D)
υ Dietary, hormonal, psychosocial triggers
υ Visual correction / ocular disorder
υ Sleep apnea / poor sleep hygiene
υ High BMI

Migraine Prophylaxis
ν Medicationsυ Tricyclics, beta-blockersυ Ca-channel blockers (verapamil)υ Anticonvulsantsυ Adjustments to hormone therapy
ν Behavior modificationsυ Diet, hydration, caffeine/alcohol useυ Exercise, sleep hygiene, altitude
changesν Physical Therapy
υ Chronic cervical strain, posture trainingν Biofeedback and relaxationν Alternative/Integrative medicine

Medical Migraine Prophylaxis
ν Patient ready for a daily medication?
ν Starting medical prophylaxis depends on the level of disabilityυ Severity - interruption of critical activitiesυ Frequency - greater than 3 times per week
ν Start at low doses, increase slowly
ν Maintain a diary / journal of headaches
ν Reproductive considerations

Physical Treatments for Headache
Biondi, Headache: The Journal of Head and Face Pain 45 (6), 738-746 (2005)
ν Migraine: PT most effective when combined with:υ Exerciseυ Relaxation trainingυ Thermal biofeedback
ν Tension-type headache:υ physical therapy >> massage, acupuncture
ν Chiropractic manipulationυ Trend toward benefit, but data is weakυ Probably TTH > Migraineυ Probably not harmful (excl: high velocity neck manip)

UCSF - PT Health and Wellness Program
PT Health and Wellness [email protected]://www.ptrehab.medschool.ucsf.edu/WellnessCenter/
Spine HealthRepetitive Strain InjuryWater Fit Stress Control and Relaxation






![Introduction Abstract - Neurology...medulla oblongata were dissected [27] and were stored in RNA later solution for RNA isolation. Whole brain (n = 5 per group) weighing 80-90mg) and](https://static.fdocument.org/doc/165x107/5f7aaac355c0bb44193d6438/introduction-abstract-neurology-medulla-oblongata-were-dissected-27-and.jpg)