GUIDELINES FOR TREATMENT OF INFECTIONS IN...
13
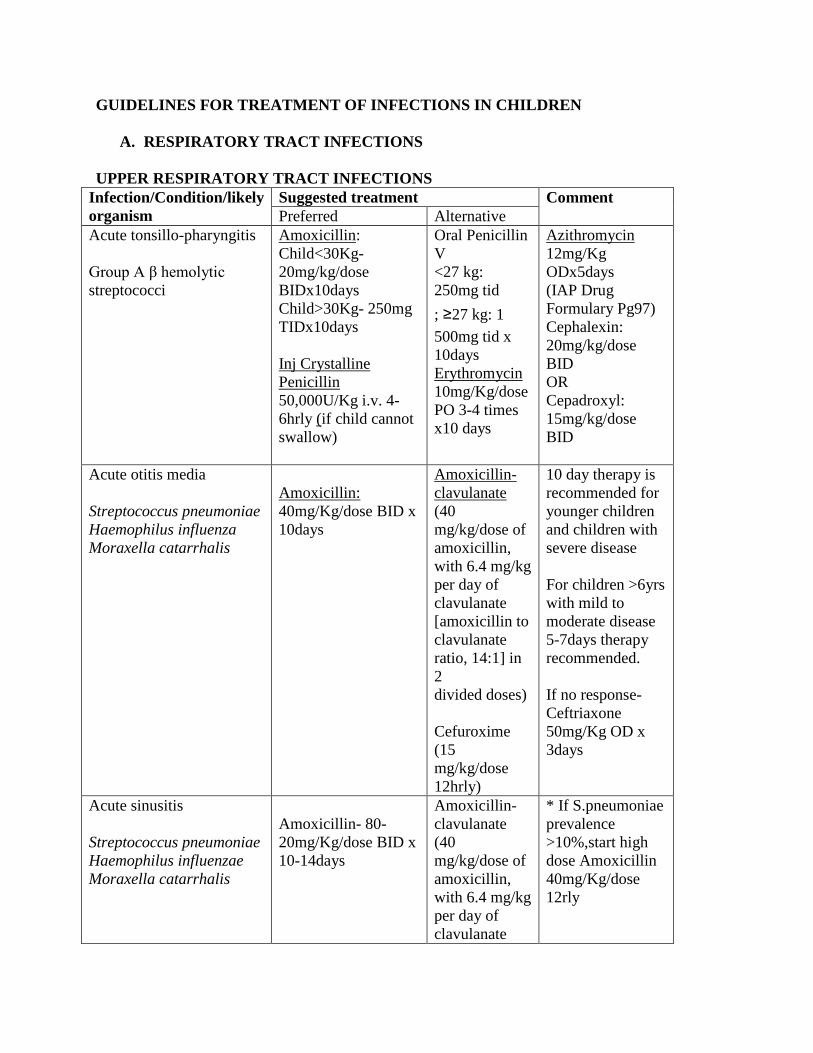
GUIDELINES FOR TREATMENT OF INFECTIONS IN CHILDREN A. RESPIRATORY TRACT INFECTIONS UPPER RESPIRATORY TRACT INFECTIONS Infection/Condition/likely organism Suggested treatment Comment Preferred Alternative Acute tonsillo-pharyngitis Group A β hemolytic streptococci Amoxicillin: Child<30Kg- 20mg/kg/dose BIDx10days Child>30Kg- 250mg TIDx10days Inj Crystalline Penicillin 50,000U/Kg i.v. 4- 6hrly (if child cannot swallow) Oral Penicillin V <27 kg: 250mg tid ; ≥27 kg: 1 500mg tid x 10days Erythromycin 10mg/Kg/dose PO 3-4 times x10 days Azithromycin 12mg/Kg ODx5days (IAP Drug Formulary Pg97) Cephalexin: 20mg/kg/dose BID OR Cepadroxyl: 15mg/kg/dose BID Acute otitis media Streptococcus pneumoniae Haemophilus influenza Moraxella catarrhalis Amoxicillin: 40mg/Kg/dose BID x 10days Amoxicillin- clavulanate (40 mg/kg/dose of amoxicillin, with 6.4 mg/kg per day of clavulanate [amoxicillin to clavulanate ratio, 14:1] in 2 divided doses) Cefuroxime (15 mg/kg/dose 12hrly) 10 day therapy is recommended for younger children and children with severe disease For children >6yrs with mild to moderate disease 5-7days therapy recommended. If no response- Ceftriaxone 50mg/Kg OD x 3days Acute sinusitis Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis Amoxicillin- 80- 20mg/Kg/dose BID x 10-14days Amoxicillin- clavulanate (40 mg/kg/dose of amoxicillin, with 6.4 mg/kg per day of clavulanate * If S.pneumoniae prevalence >10%,start high dose Amoxicillin 40mg/Kg/dose 12rly
Transcript of GUIDELINES FOR TREATMENT OF INFECTIONS IN...
GUIDELINES FOR TREATMENT OF INFECTIONS IN CHILDREN
A. RESPIRATORY TRACT INFECTIONS
UPPER RESPIRATORY TRACT INFECTIONS
Infection/Condition/likely
organism
Suggested treatment Comment
Preferred Alternative
Acute tonsillo-pharyngitis
Group A β hemolytic
streptococci
Amoxicillin:
Child<30Kg-
20mg/kg/dose
BIDx10days
Child>30Kg- 250mg
TIDx10days
Inj Crystalline
Penicillin
50,000U/Kg i.v. 4-
6hrly (if child cannot
swallow)
Oral Penicillin
V
<27 kg:
250mg tid
; ≥27 kg: 1
500mg tid x
10days
Erythromycin
10mg/Kg/dose
PO 3-4 times
x10 days
Azithromycin
12mg/Kg
ODx5days
(IAP Drug
Formulary Pg97)
Cephalexin:
20mg/kg/dose
BID
OR
Cepadroxyl:
15mg/kg/dose
BID
Acute otitis media
Streptococcus pneumoniae
Haemophilus influenza
Moraxella catarrhalis
Amoxicillin:
40mg/Kg/dose BID x
10days
Amoxicillin-
clavulanate
(40
mg/kg/dose of
amoxicillin,
with 6.4 mg/kg
per day of
clavulanate
[amoxicillin to
clavulanate
ratio, 14:1] in
2
divided doses)
Cefuroxime
(15
mg/kg/dose
12hrly)
10 day therapy is
recommended for
younger children
and children with
severe disease
For children >6yrs
with mild to
moderate disease
5-7days therapy
recommended.
If no response-
Ceftriaxone
50mg/Kg OD x
3days
Acute sinusitis
Streptococcus pneumoniae
Haemophilus influenzae
Moraxella catarrhalis
Amoxicillin- 80-
20mg/Kg/dose BID x
10-14days
Amoxicillin-
clavulanate
(40
mg/kg/dose of
amoxicillin,
with 6.4 mg/kg
per day of
clavulanate
* If S.pneumoniae
prevalence
>10%,start high
dose Amoxicillin
40mg/Kg/dose
12rly
[amoxicillin to
clavulanate
ratio, 14:1] in
2
divided doses)
Cefuroxime
(15
mg/kg/dose
12hrly x 10-
14days
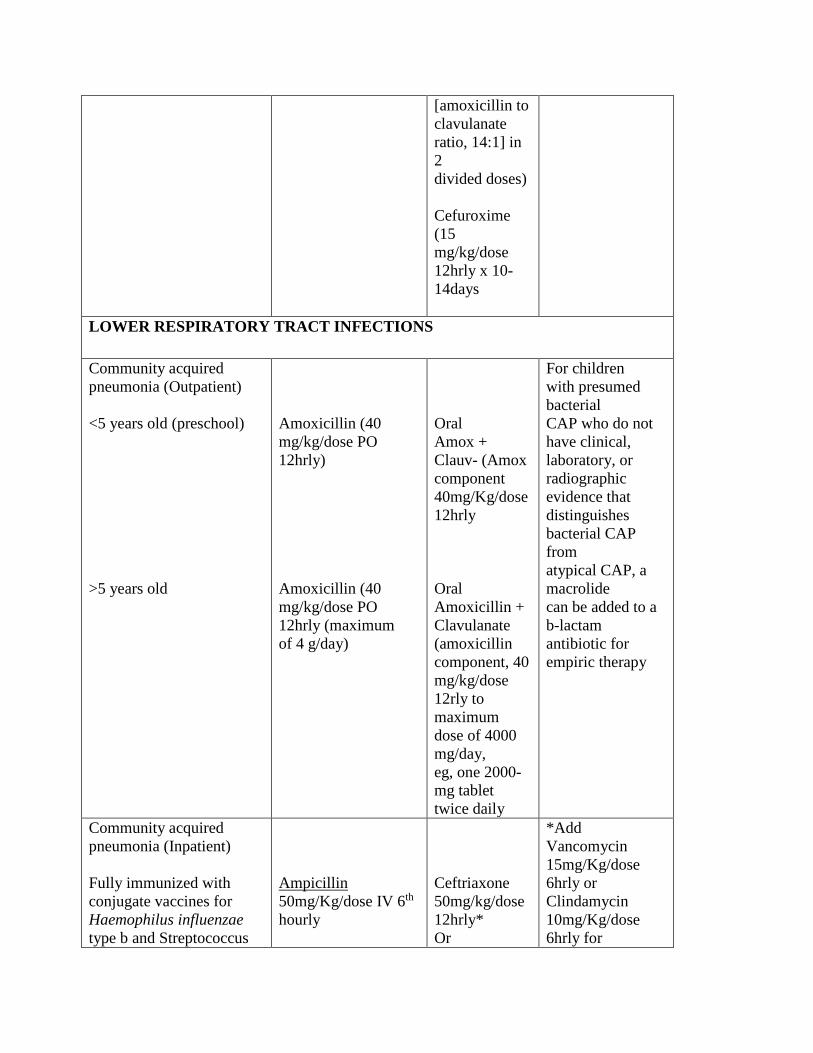
LOWER RESPIRATORY TRACT INFECTIONS
Community acquired
pneumonia (Outpatient)
<5 years old (preschool)
>5 years old
Amoxicillin (40
mg/kg/dose PO
12hrly)
Amoxicillin (40
mg/kg/dose PO
12hrly (maximum
of 4 g/day)
Oral
Amox +
Clauv- (Amox
component
40mg/Kg/dose
12hrly
Oral
Amoxicillin +
Clavulanate
(amoxicillin
component, 40
mg/kg/dose
12rly to
maximum
dose of 4000
mg/day,
eg, one 2000-
mg tablet
twice daily
For children
with presumed
bacterial
CAP who do not
have clinical,
laboratory, or
radiographic
evidence that
distinguishes
bacterial CAP
from
atypical CAP, a
macrolide
can be added to a
b-lactam
antibiotic for
empiric therapy
Community acquired
pneumonia (Inpatient)
Fully immunized with
conjugate vaccines for
Haemophilus influenzae
type b and Streptococcus
Ampicillin
50mg/Kg/dose IV 6th
hourly
Ceftriaxone
50mg/kg/dose
12hrly*
Or
*Add
Vancomycin
15mg/Kg/dose
6hrly or
Clindamycin
10mg/Kg/dose
6hrly for
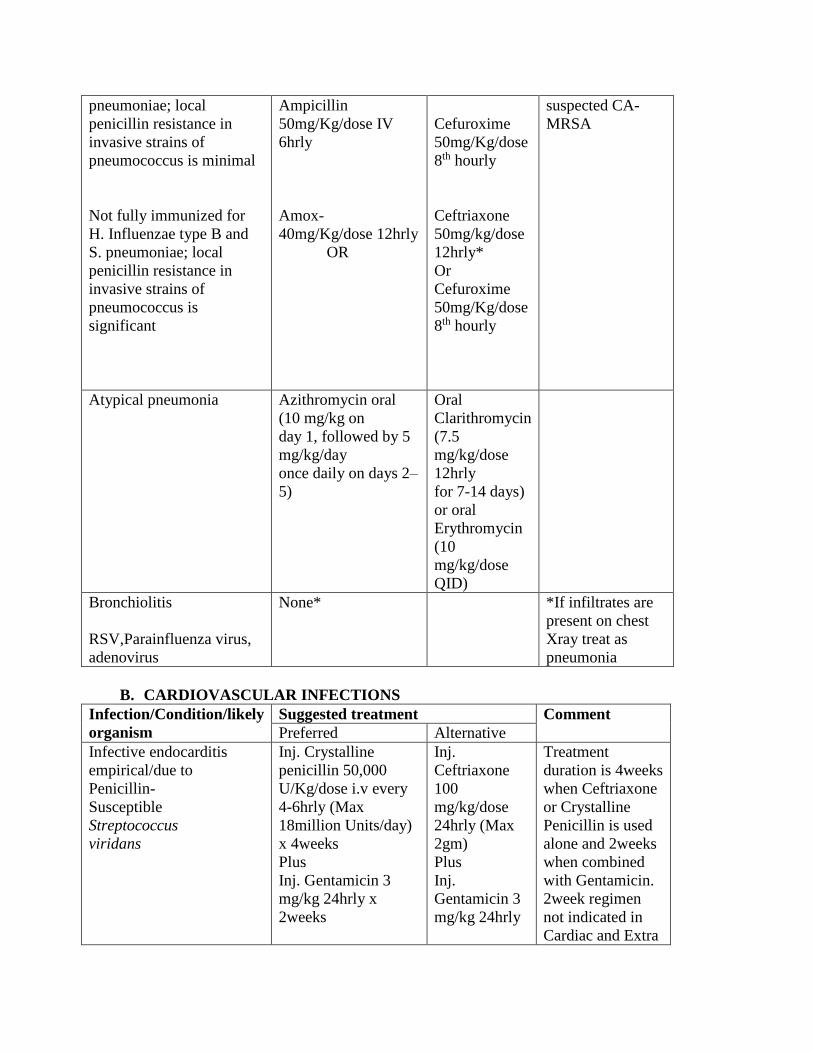
pneumoniae; local
penicillin resistance in
invasive strains of
pneumococcus is minimal
Not fully immunized for
H. Influenzae type B and
S. pneumoniae; local
penicillin resistance in
invasive strains of
pneumococcus is
significant
Ampicillin
50mg/Kg/dose IV
6hrly
Amox-
40mg/Kg/dose 12hrly
OR
Cefuroxime
50mg/Kg/dose
8th hourly
Ceftriaxone
50mg/kg/dose
12hrly*
Or
Cefuroxime
50mg/Kg/dose
8th hourly
suspected CA-
MRSA
Atypical pneumonia Azithromycin oral
(10 mg/kg on
day 1, followed by 5
mg/kg/day
once daily on days 2–
5)
Oral
Clarithromycin
(7.5
mg/kg/dose
12hrly
for 7-14 days)
or oral
Erythromycin
(10
mg/kg/dose
QID)
Bronchiolitis
RSV,Parainfluenza virus,
adenovirus
None* *If infiltrates are
present on chest
Xray treat as
pneumonia
B. CARDIOVASCULAR INFECTIONS
Infection/Condition/likely
organism
Suggested treatment Comment
Preferred Alternative
Infective endocarditis
empirical/due to
Penicillin-
Susceptible
Streptococcus
viridans
Inj. Crystalline
penicillin 50,000
U/Kg/dose i.v every
4-6hrly (Max
18million Units/day)
x 4weeks
Plus
Inj. Gentamicin 3
mg/kg 24hrly x
2weeks
Inj.
Ceftriaxone
100
mg/kg/dose
24hrly (Max
2gm)
Plus
Inj.
Gentamicin 3
mg/kg 24hrly
Treatment
duration is 4weeks
when Ceftriaxone
or Crystalline
Penicillin is used
alone and 2weeks
when combined
with Gentamicin.
2week regimen
not indicated in
Cardiac and Extra
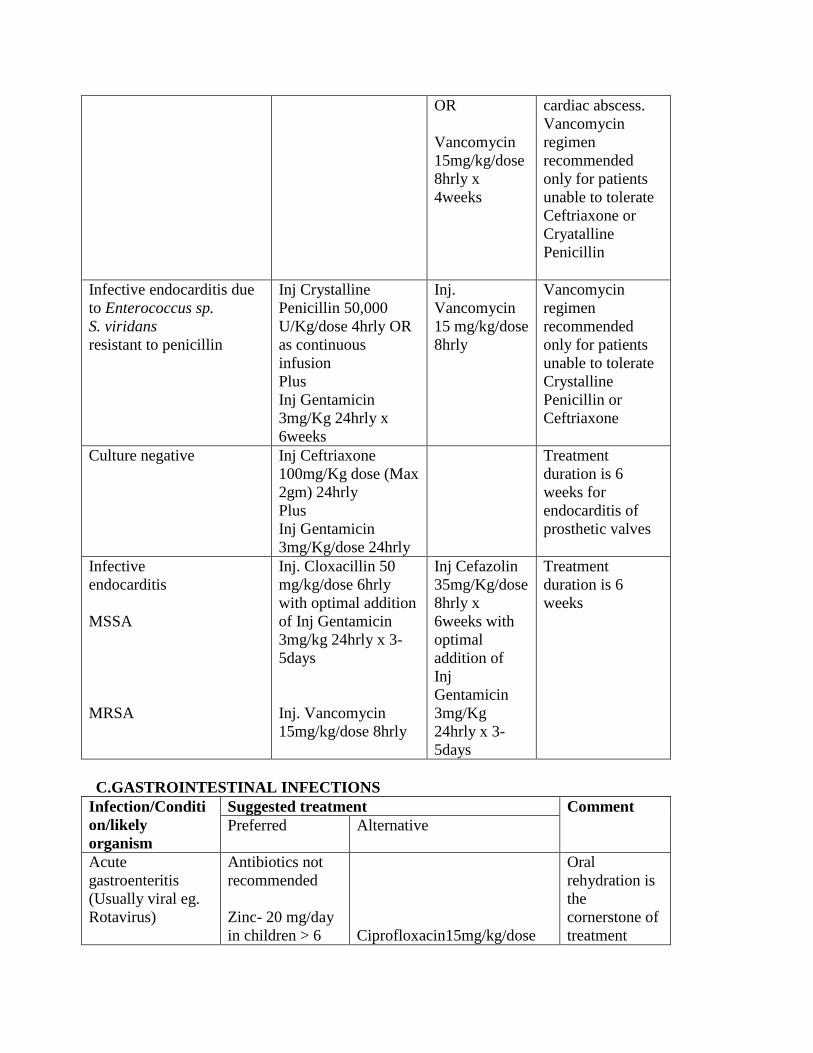
OR
Vancomycin
15mg/kg/dose
8hrly x
4weeks
cardiac abscess.
Vancomycin
regimen
recommended
only for patients
unable to tolerate
Ceftriaxone or
Cryatalline
Penicillin
Infective endocarditis due
to Enterococcus sp.
S. viridans
resistant to penicillin
Inj Crystalline
Penicillin 50,000
U/Kg/dose 4hrly OR
as continuous
infusion
Plus
Inj Gentamicin
3mg/Kg 24hrly x
6weeks
Inj.
Vancomycin
15 mg/kg/dose
8hrly
Vancomycin
regimen
recommended
only for patients
unable to tolerate
Crystalline
Penicillin or
Ceftriaxone
Culture negative
Inj Ceftriaxone
100mg/Kg dose (Max
2gm) 24hrly
Plus
Inj Gentamicin
3mg/Kg/dose 24hrly
Treatment
duration is 6
weeks for
endocarditis of
prosthetic valves
Infective
endocarditis
MSSA
MRSA
Inj. Cloxacillin 50
mg/kg/dose 6hrly
with optimal addition
of Inj Gentamicin
3mg/kg 24hrly x 3-
5days
Inj. Vancomycin
15mg/kg/dose 8hrly
Inj Cefazolin
35mg/Kg/dose
8hrly x
6weeks with
optimal
addition of
Inj
Gentamicin
3mg/Kg
24hrly x 3-
5days
Treatment
duration is 6
weeks
C.GASTROINTESTINAL INFECTIONS
Infection/Conditi
on/likely
organism
Suggested treatment Comment
Preferred Alternative
Acute
gastroenteritis
(Usually viral eg.
Rotavirus)
Antibiotics not
recommended
Zinc- 20 mg/day
in children > 6
Ciprofloxacin15mg/kg/dose
Oral
rehydration is
the
cornerstone of
treatment
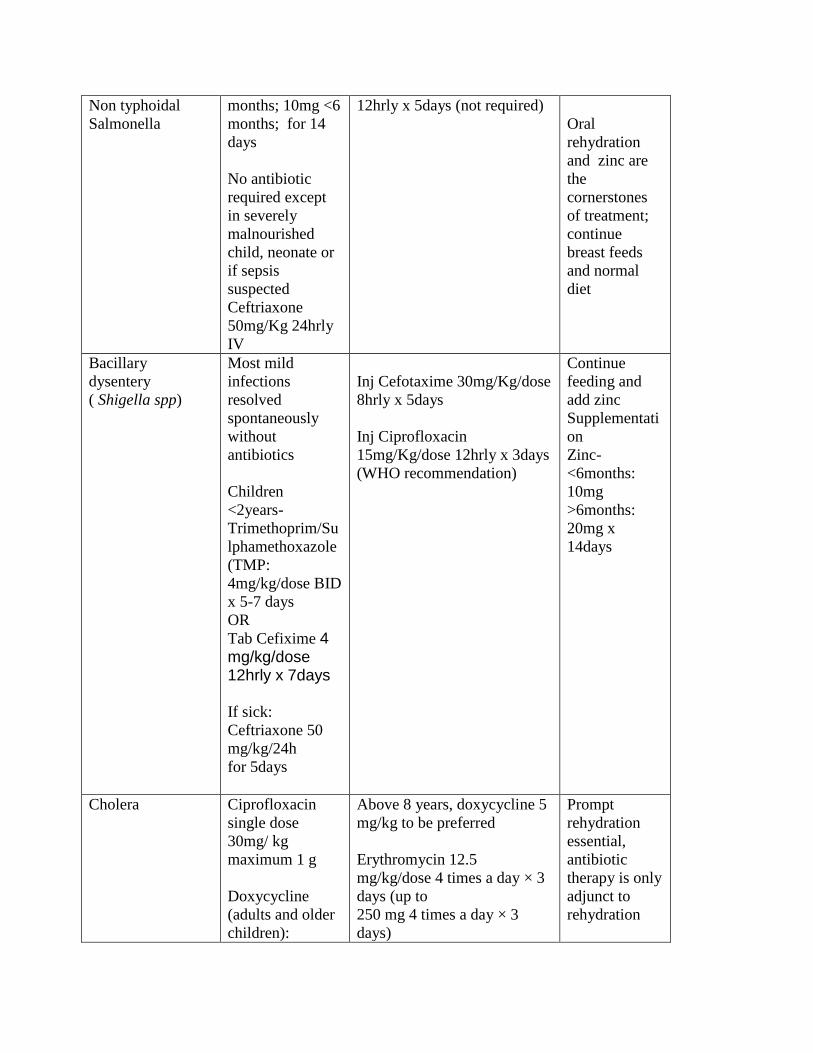
Non typhoidal
Salmonella
months; 10mg <6
months; for 14
days
No antibiotic
required except
in severely
malnourished
child, neonate or
if sepsis
suspected
Ceftriaxone
50mg/Kg 24hrly
IV
12hrly x 5days (not required)
Oral
rehydration
and zinc are
the
cornerstones
of treatment;
continue
breast feeds
and normal
diet
Bacillary
dysentery
( Shigella spp)
Most mild
infections
resolved
spontaneously
without
antibiotics
Children
<2years-
Trimethoprim/Su
lphamethoxazole
(TMP:
4mg/kg/dose BID
x 5-7 days
OR
Tab Cefixime 4 mg/kg/dose 12hrly x 7days
If sick:
Ceftriaxone 50
mg/kg/24h
for 5days
Inj Cefotaxime 30mg/Kg/dose
8hrly x 5days
Inj Ciprofloxacin
15mg/Kg/dose 12hrly x 3days
(WHO recommendation)
Continue
feeding and
add zinc
Supplementati
on
Zinc-
<6months:
10mg
>6months:
20mg x
14days
Cholera Ciprofloxacin
single dose
30mg/ kg
maximum 1 g
Doxycycline
(adults and older
children):
Above 8 years, doxycycline 5
mg/kg to be preferred
Erythromycin 12.5
mg/kg/dose 4 times a day × 3
days (up to
250 mg 4 times a day × 3
days)
Prompt
rehydration
essential,
antibiotic
therapy is only
adjunct to
rehydration
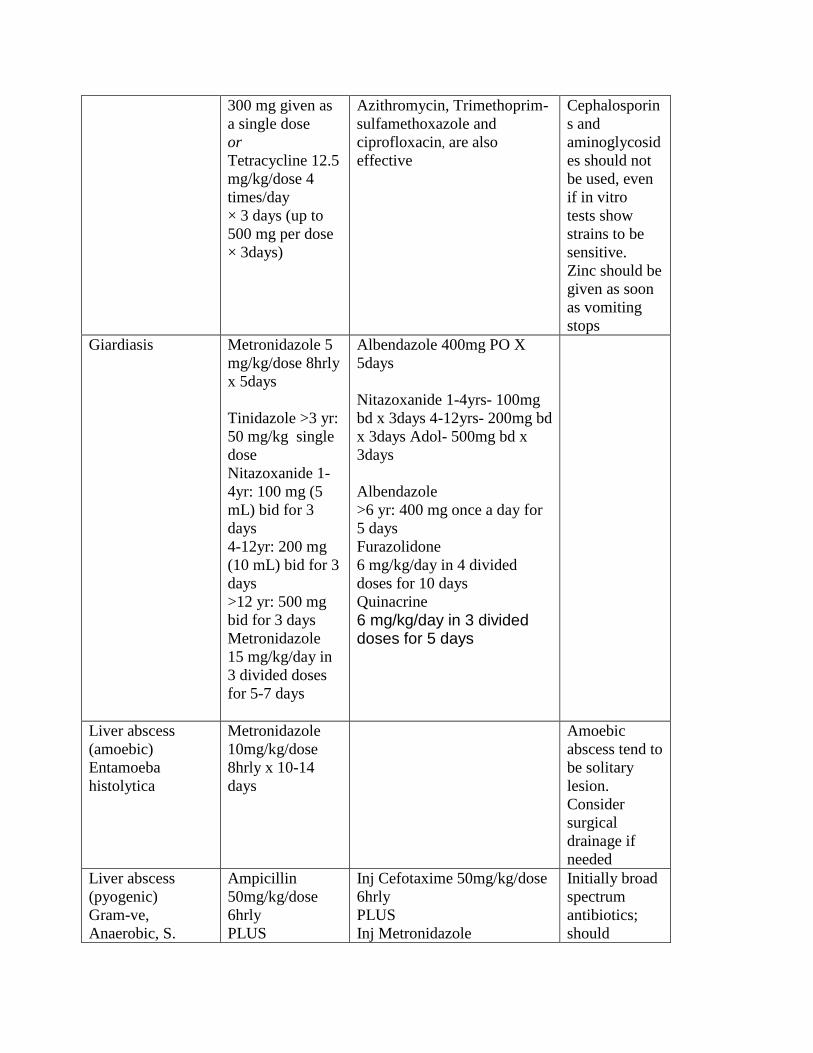
300 mg given as
a single dose
or
Tetracycline 12.5
mg/kg/dose 4
times/day
× 3 days (up to
500 mg per dose
× 3days)
Azithromycin, Trimethoprim-
sulfamethoxazole and
ciprofloxacin, are also
effective
Cephalosporin
s and
aminoglycosid
es should not
be used, even
if in vitro
tests show
strains to be
sensitive.
Zinc should be
given as soon
as vomiting
stops
Giardiasis Metronidazole 5
mg/kg/dose 8hrly
x 5days
Tinidazole >3 yr:
50 mg/kg single
dose
Nitazoxanide 1-
4yr: 100 mg (5
mL) bid for 3
days
4-12yr: 200 mg
(10 mL) bid for 3
days
>12 yr: 500 mg
bid for 3 days
Metronidazole
15 mg/kg/day in
3 divided doses
for 5-7 days
Albendazole 400mg PO X
5days
Nitazoxanide 1-4yrs- 100mg
bd x 3days 4-12yrs- 200mg bd
x 3days Adol- 500mg bd x
3days
Albendazole
>6 yr: 400 mg once a day for
5 days
Furazolidone
6 mg/kg/day in 4 divided
doses for 10 days
Quinacrine
6 mg/kg/day in 3 divided doses for 5 days
Liver abscess
(amoebic)
Entamoeba
histolytica
Metronidazole
10mg/kg/dose
8hrly x 10-14
days
Amoebic
abscess tend to
be solitary
lesion.
Consider
surgical
drainage if
needed
Liver abscess
(pyogenic)
Gram-ve,
Anaerobic, S.
Ampicillin
50mg/kg/dose
6hrly
PLUS
Inj Cefotaxime 50mg/kg/dose
6hrly
PLUS
Inj Metronidazole
Initially broad
spectrum
antibiotics;
should
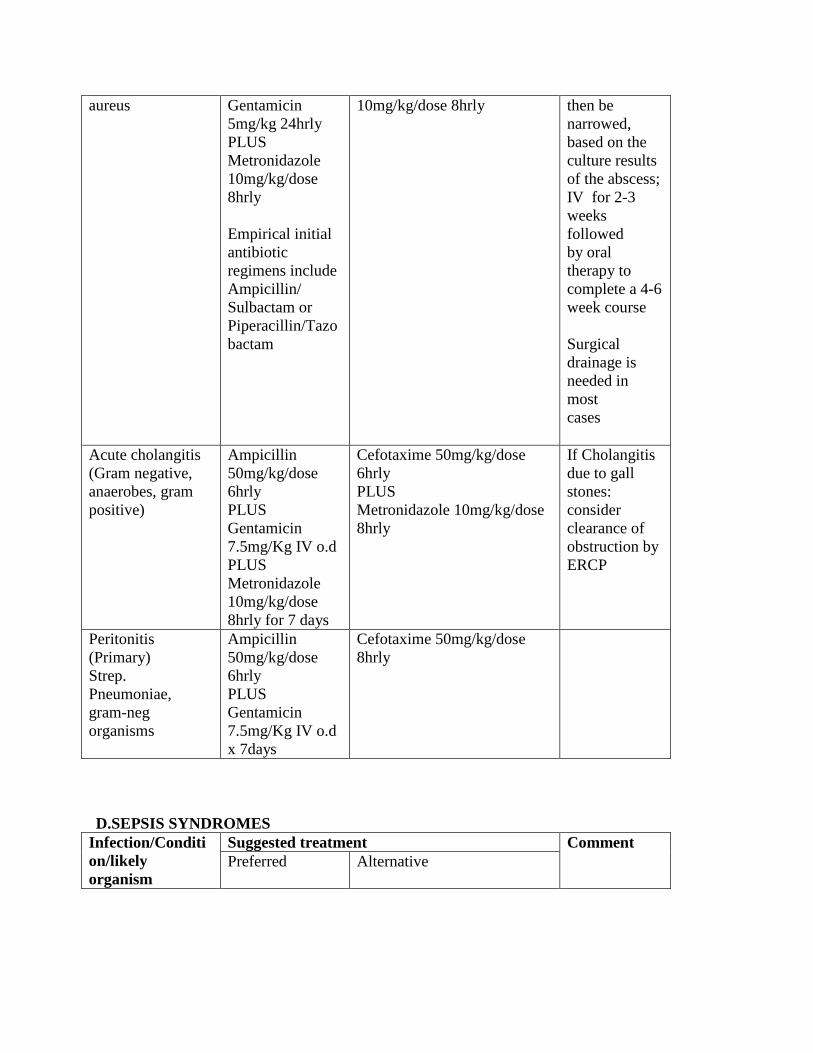
aureus Gentamicin
5mg/kg 24hrly
PLUS
Metronidazole
10mg/kg/dose
8hrly
Empirical initial
antibiotic
regimens include
Ampicillin/
Sulbactam or
Piperacillin/Tazo
bactam
10mg/kg/dose 8hrly then be
narrowed,
based on the
culture results
of the abscess;
IV for 2-3
weeks
followed
by oral
therapy to
complete a 4-6
week course
Surgical
drainage is
needed in
most
cases
Acute cholangitis
(Gram negative,
anaerobes, gram
positive)
Ampicillin
50mg/kg/dose
6hrly
PLUS
Gentamicin
7.5mg/Kg IV o.d
PLUS
Metronidazole
10mg/kg/dose
8hrly for 7 days
Cefotaxime 50mg/kg/dose
6hrly
PLUS
Metronidazole 10mg/kg/dose
8hrly
If Cholangitis
due to gall
stones:
consider
clearance of
obstruction by
ERCP
Peritonitis
(Primary)
Strep.
Pneumoniae,
gram-neg
organisms
Ampicillin
50mg/kg/dose
6hrly
PLUS
Gentamicin
7.5mg/Kg IV o.d
x 7days
Cefotaxime 50mg/kg/dose
8hrly
D.SEPSIS SYNDROMES
Infection/Conditi
on/likely
organism
Suggested treatment Comment
Preferred Alternative
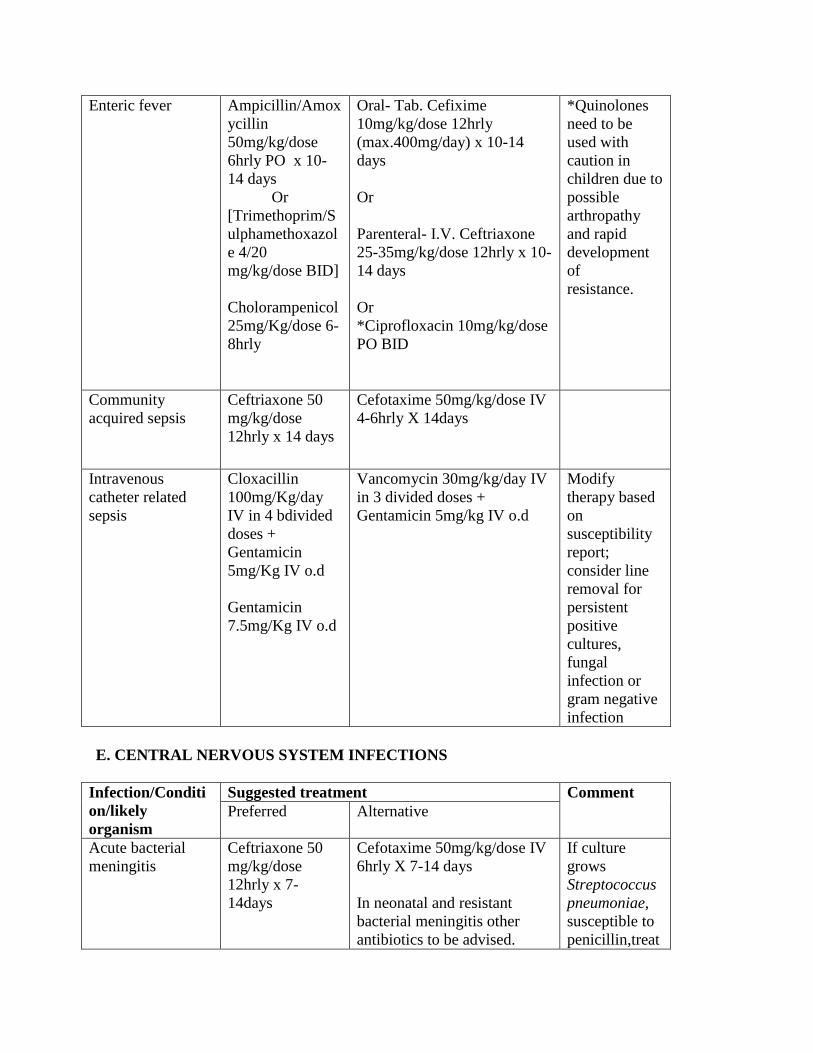
Enteric fever Ampicillin/Amox
ycillin
50mg/kg/dose
6hrly PO x 10-
14 days
Or
[Trimethoprim/S
ulphamethoxazol
e 4/20
mg/kg/dose BID]
Cholorampenicol
25mg/Kg/dose 6-
8hrly
Oral- Tab. Cefixime
10mg/kg/dose 12hrly
(max.400mg/day) x 10-14
days
Or
Parenteral- I.V. Ceftriaxone
25-35mg/kg/dose 12hrly x 10-
14 days
Or
*Ciprofloxacin 10mg/kg/dose
PO BID
*Quinolones
need to be
used with
caution in
children due to
possible
arthropathy
and rapid
development
of
resistance.
Community
acquired sepsis
Ceftriaxone 50
mg/kg/dose
12hrly x 14 days
Cefotaxime 50mg/kg/dose IV
4-6hrly X 14days
Intravenous
catheter related
sepsis
Cloxacillin
100mg/Kg/day
IV in 4 bdivided
doses +
Gentamicin
5mg/Kg IV o.d
Gentamicin
7.5mg/Kg IV o.d
Vancomycin 30mg/kg/day IV
in 3 divided doses +
Gentamicin 5mg/kg IV o.d
Modify
therapy based
on
susceptibility
report;
consider line
removal for
persistent
positive
cultures,
fungal
infection or
gram negative
infection
E. CENTRAL NERVOUS SYSTEM INFECTIONS
Infection/Conditi
on/likely
organism
Suggested treatment Comment
Preferred Alternative
Acute bacterial
meningitis
Ceftriaxone 50
mg/kg/dose
12hrly x 7-
14days
Cefotaxime 50mg/kg/dose IV
6hrly X 7-14 days
In neonatal and resistant
bacterial meningitis other
antibiotics to be advised.
If culture
grows
Streptococcus
pneumoniae,
susceptible to
penicillin,treat
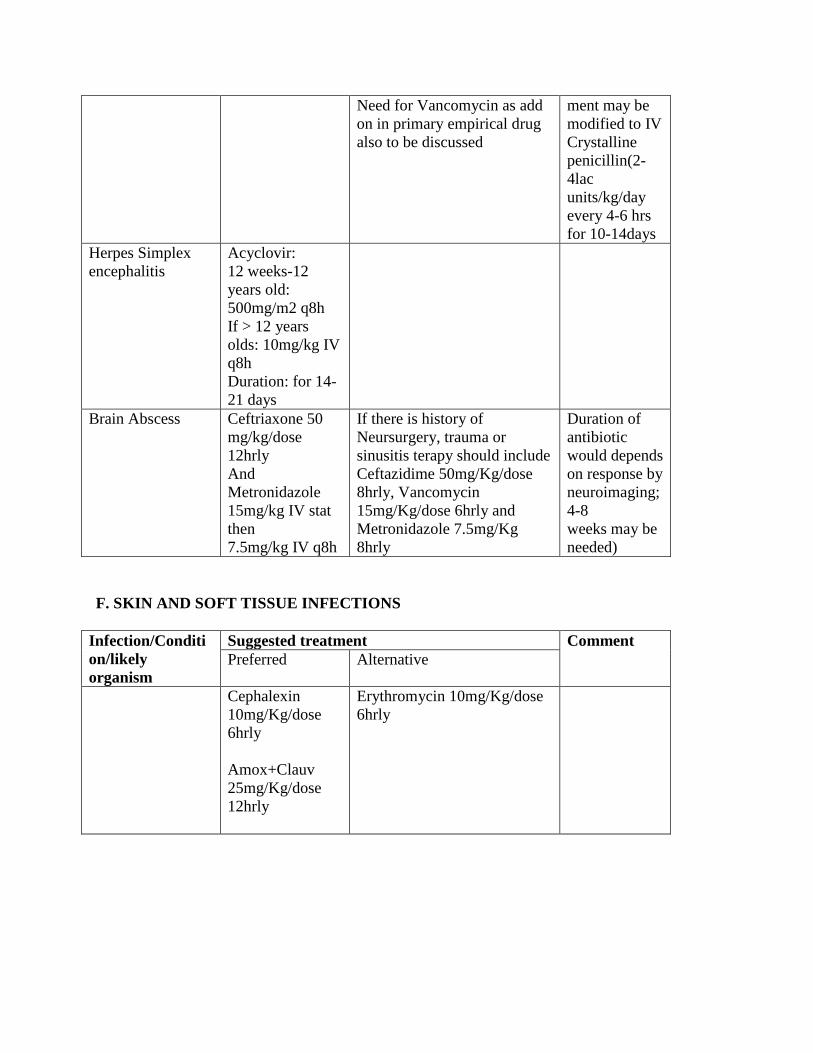
Need for Vancomycin as add
on in primary empirical drug
also to be discussed
ment may be
modified to IV
Crystalline
penicillin(2-
4lac
units/kg/day
every 4-6 hrs
for 10-14days
Herpes Simplex
encephalitis
Acyclovir:
12 weeks-12
years old:
500mg/m2 q8h
If > 12 years
olds: 10mg/kg IV
q8h
Duration: for 14-
21 days
Brain Abscess Ceftriaxone 50
mg/kg/dose
12hrly
And
Metronidazole
15mg/kg IV stat
then
7.5mg/kg IV q8h
If there is history of
Neursurgery, trauma or
sinusitis terapy should include
Ceftazidime 50mg/Kg/dose
8hrly, Vancomycin
15mg/Kg/dose 6hrly and
Metronidazole 7.5mg/Kg
8hrly
Duration of
antibiotic
would depends
on response by
neuroimaging;
4-8
weeks may be
needed)
F. SKIN AND SOFT TISSUE INFECTIONS
Infection/Conditi
on/likely
organism
Suggested treatment Comment
Preferred Alternative
Cephalexin
10mg/Kg/dose
6hrly
Amox+Clauv
25mg/Kg/dose
12hrly
Erythromycin 10mg/Kg/dose
6hrly
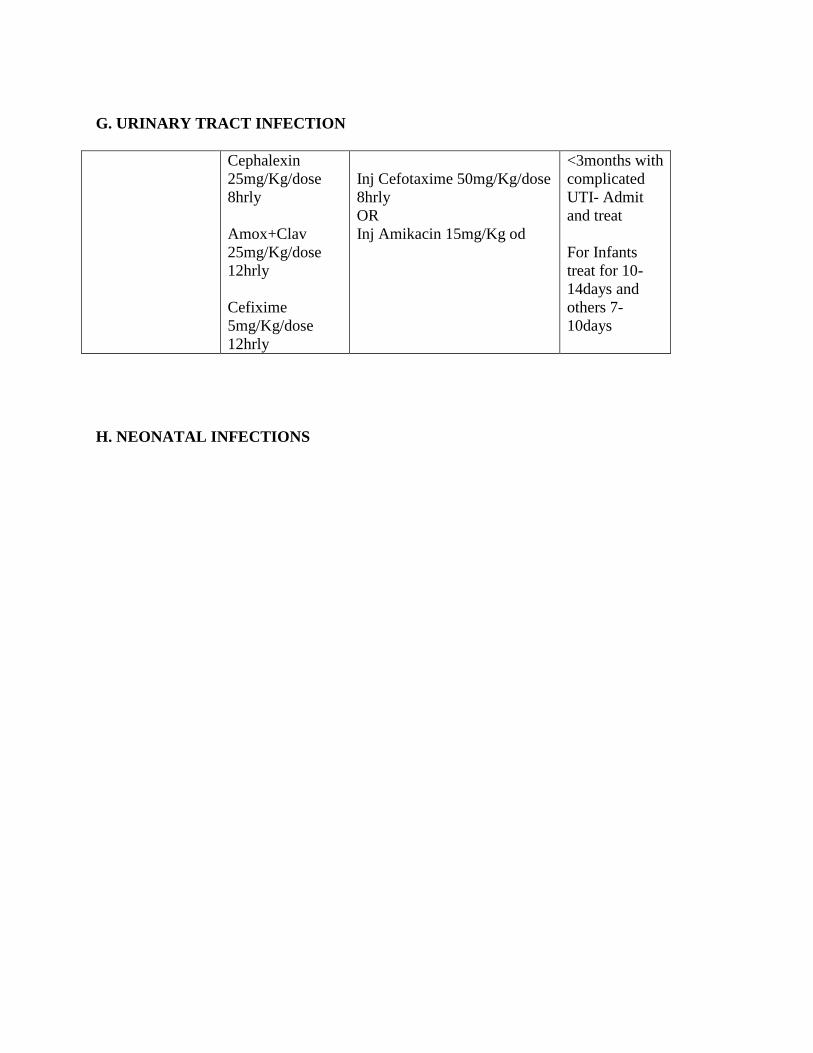
G. URINARY TRACT INFECTION
Cephalexin
25mg/Kg/dose
8hrly
Amox+Clav
25mg/Kg/dose
12hrly
Cefixime
5mg/Kg/dose
12hrly
Inj Cefotaxime 50mg/Kg/dose
8hrly
OR
Inj Amikacin 15mg/Kg od
<3months with
complicated
UTI- Admit
and treat
For Infants
treat for 10-
14days and
others 7-
10days
H. NEONATAL INFECTIONS
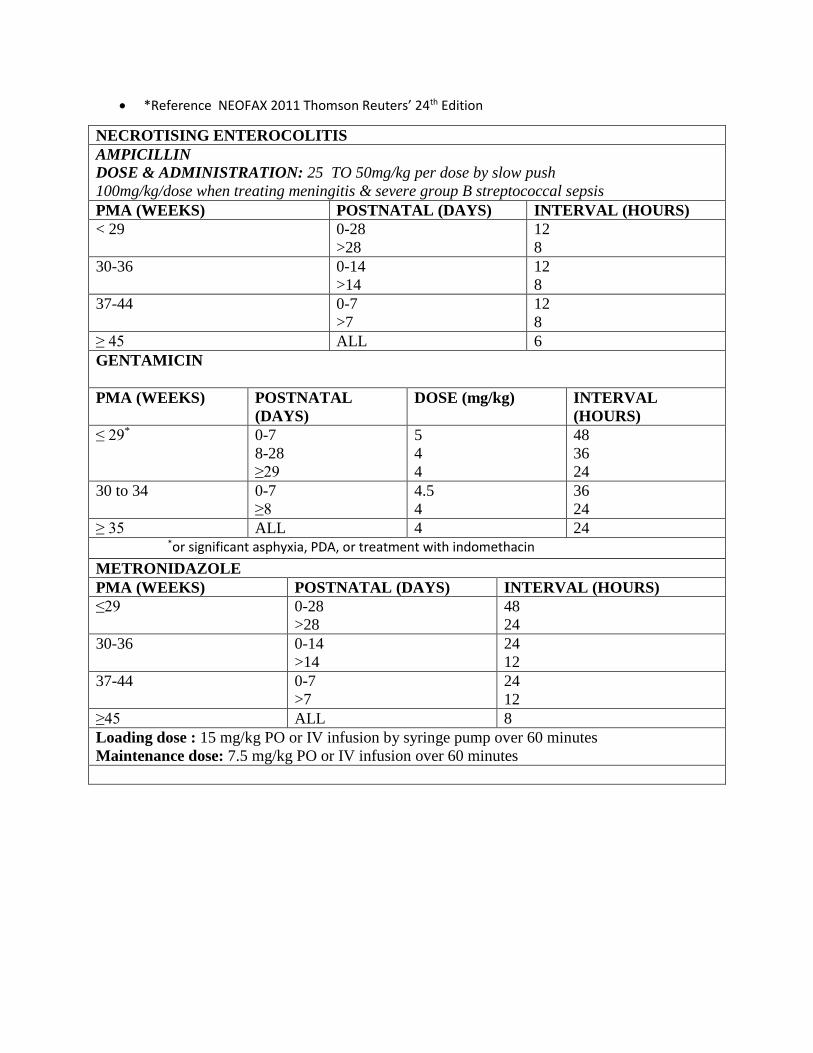
*Reference NEOFAX 2011 Thomson Reuters’ 24th Edition
NECROTISING ENTEROCOLITIS
AMPICILLIN
DOSE & ADMINISTRATION: 25 TO 50mg/kg per dose by slow push
100mg/kg/dose when treating meningitis & severe group B streptococcal sepsis
PMA (WEEKS) POSTNATAL (DAYS) INTERVAL (HOURS)
< 29 0-28
>28
12
8
30-36 0-14
>14
12
8
37-44 0-7
>7
12
8
≥ 45 ALL 6
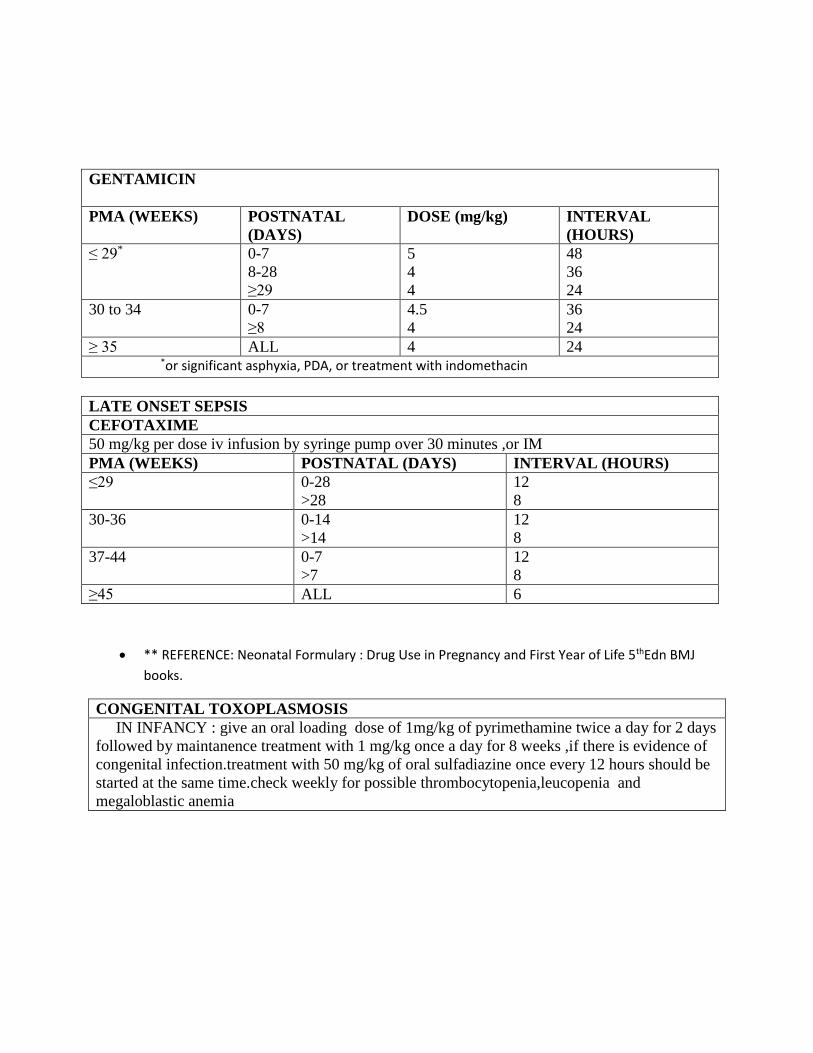
GENTAMICIN
PMA (WEEKS) POSTNATAL
(DAYS)
DOSE (mg/kg) INTERVAL
(HOURS)
≤ 29* 0-7
8-28
≥29
5
4
4
48
36
24
30 to 34 0-7
≥8
4.5
4
36
24
≥ 35 ALL 4 24 *or significant asphyxia, PDA, or treatment with indomethacin
METRONIDAZOLE
PMA (WEEKS) POSTNATAL (DAYS) INTERVAL (HOURS)
≤29 0-28
>28
48
24
30-36 0-14
>14
24
12
37-44 0-7
>7
24
12
≥45 ALL 8
Loading dose : 15 mg/kg PO or IV infusion by syringe pump over 60 minutes
Maintenance dose: 7.5 mg/kg PO or IV infusion over 60 minutes
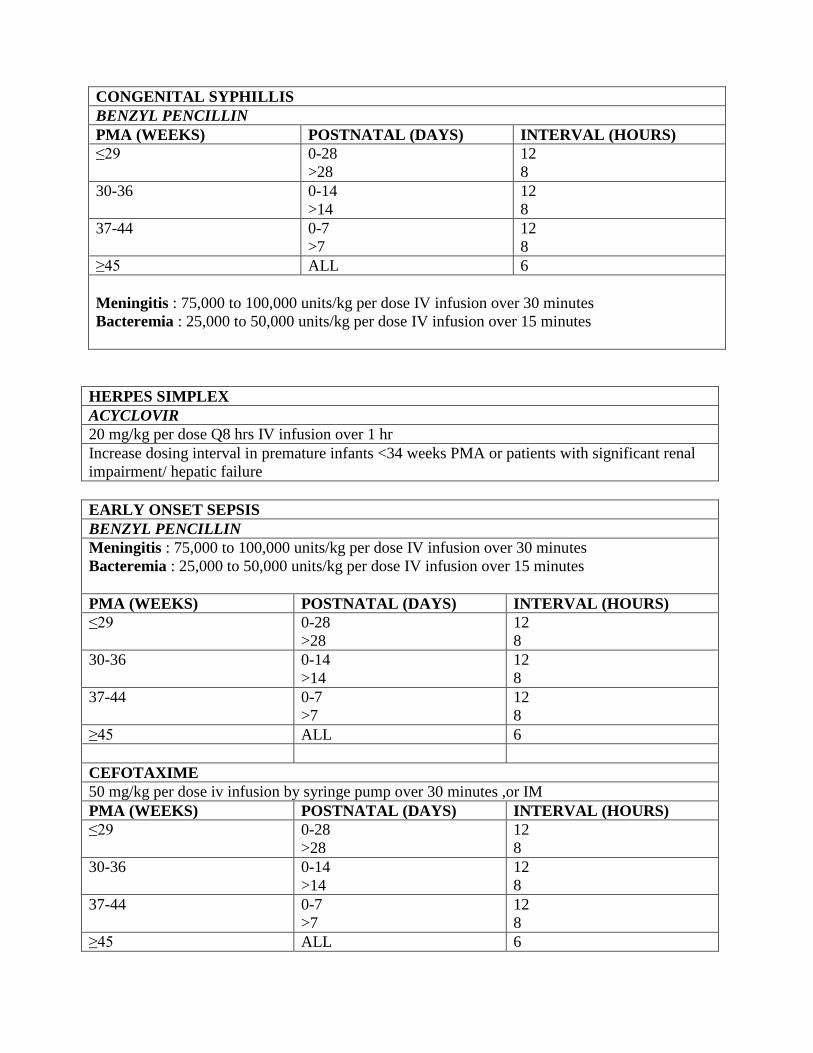
HERPES SIMPLEX
ACYCLOVIR
20 mg/kg per dose Q8 hrs IV infusion over 1 hr
Increase dosing interval in premature infants <34 weeks PMA or patients with significant renal
impairment/ hepatic failure
EARLY ONSET SEPSIS
BENZYL PENCILLIN
Meningitis : 75,000 to 100,000 units/kg per dose IV infusion over 30 minutes
Bacteremia : 25,000 to 50,000 units/kg per dose IV infusion over 15 minutes
PMA (WEEKS) POSTNATAL (DAYS) INTERVAL (HOURS)
≤29 0-28
>28
12
8
30-36 0-14
>14
12
8
37-44 0-7
>7
12
8
≥45 ALL 6
CEFOTAXIME
50 mg/kg per dose iv infusion by syringe pump over 30 minutes ,or IM
PMA (WEEKS) POSTNATAL (DAYS) INTERVAL (HOURS)
≤29 0-28
>28
12
8
30-36 0-14
>14
12
8
37-44 0-7
>7
12
8
≥45 ALL 6
CONGENITAL SYPHILLIS
BENZYL PENCILLIN
PMA (WEEKS) POSTNATAL (DAYS) INTERVAL (HOURS)
≤29 0-28
>28
12
8
30-36 0-14
>14
12
8
37-44 0-7
>7
12
8
≥45 ALL 6
Meningitis : 75,000 to 100,000 units/kg per dose IV infusion over 30 minutes
Bacteremia : 25,000 to 50,000 units/kg per dose IV infusion over 15 minutes
GENTAMICIN
PMA (WEEKS) POSTNATAL
(DAYS)
DOSE (mg/kg) INTERVAL
(HOURS)
≤ 29* 0-7
8-28
≥29
5
4
4
48
36
24
30 to 34 0-7
≥8
4.5
4
36
24
≥ 35 ALL 4 24 *or significant asphyxia, PDA, or treatment with indomethacin
LATE ONSET SEPSIS
CEFOTAXIME
50 mg/kg per dose iv infusion by syringe pump over 30 minutes ,or IM
PMA (WEEKS) POSTNATAL (DAYS) INTERVAL (HOURS)
≤29 0-28
>28
12
8
30-36 0-14
>14
12
8
37-44 0-7
>7
12
8
≥45 ALL 6
** REFERENCE: Neonatal Formulary : Drug Use in Pregnancy and First Year of Life 5thEdn BMJ
books.
CONGENITAL TOXOPLASMOSIS
IN INFANCY : give an oral loading dose of 1mg/kg of pyrimethamine twice a day for 2 days
followed by maintanence treatment with 1 mg/kg once a day for 8 weeks ,if there is evidence of
congenital infection.treatment with 50 mg/kg of oral sulfadiazine once every 12 hours should be
started at the same time.check weekly for possible thrombocytopenia,leucopenia and
megaloblastic anemia