Gly389Arg polymorphism of β1-adrenergic receptor is associated with the cardiovascular response to...
8
PHARMACOGENETICS AND GENOMICS Gly389Arg polymorphism of 1 -adrenergic receptor is associated with the cardiovascular response to metoprolol Objectives: Our objectives were to determine whether the Gly389 polymorphism of the 1 -adrenergic recep- tor exhibits reduced responsiveness in vivo and to test the hypothesis that the Gly389Arg polymorphism affects the blood pressure and heart rate response to metoprolol. Methods: 1 -Adrenergic receptor genotype was determined by polymerase chain reaction–restriction fragment length polymorphism assay. Exercise-induced heart rate increases were compared to determine the functional significance in vivo in 8 healthy Chinese men homozygous for Gly389 and 8 homozygous for Arg389. All of the subjects were given 25, 50, or 75 mg of metoprolol every 8 hours; the dosages were given in a random order, and each dosage was given for 1 day. The degree of -blockade was measured as the reduction in resting and exercise heart rates and blood pressures. Plasma metoprolol concentrations were measured by the use of HPLC–fluorescence detection. Results: Exercise led to a workload-dependent increase in heart rate. There were no differences in exercise- induced heart rate increases between Arg389 and Gly389 homozygotes. Oral metoprolol caused significant dose-dependent decreases in both resting and exercise heart rates in both groups. The reductions in the resting heart rate in 3 dosage levels of metoprolol were 6.3% 0.8% versus 4.1% 0.7%, 10.1% 1.0% versus 6.2% 1.1%, and 14.4% 1.4% versus 10.9% 1.3% in homozygous Arg389 subjects and Gly389 subjects, respectively (P .008). We also found differences with respect to the exercise heart rate (8.9% 0.5%, 14.0% 0.9%, and 20.1% 1.5% in Arg389 subjects and 6.6% 0.7%, 11.7% 1.0%, and 16.4% 1.3% in Gly389 subjects; P .017) and systolic pressure (5.9% 0.7%, 9.2% 1.0%, and 11.6% 1.2% in Arg389 subjects and 4.6% 0.5%, 6.0% 0.8%, and 9.9% 0.9% in Gly389 subjects; P .011). However, the difference in the fall in diastolic pressure was not statistically significant (P .442). Conclusions: The Arg389 variant of the 1 -adrenergic receptor was associated with a greater response to metoprolol than that of Gly389 in young, male Chinese subjects. These data suggested that the 1 -adrenergic receptor Gly389Arg polymorphism is of major functional importance in vivo. (Clin Pharmacol Ther 2003; 74:372-9.) Jie Liu, MD, Zhao-Qian Liu, MD, PhD, Zhi-Rong Tan, BS, Xiao-Ping Chen, MS, PhD, Lian-Sheng Wang, MS, Gan Zhou, MD, and Hong-Hao Zhou, MD Changsha, Hunan, China From the Pharmacogenetics Research Institute, Institute of Clinical Pharmacology, Central South University. Supported by the National Science Foundation of China grants No. 30070880 and No. F30130210 and China Medical Board grant No. 01-755. Received for publication Feb 10, 2003; accepted June 20, 2003. Reprint requests: Hong-Hao Zhou, MD, Pharmacogenetics Research Institute, Institute of Clinical Pharmacology, Central South Uni- versity, Changsha, Hunan 410078, China. E-mail: [email protected] Copyright © 2003 by the American Society for Clinical Pharmacol- ogy & Therapeutics. 0009-9236/2003/$30.00 0 doi:10.1067/S0009-9236(03)00224-8 372
Transcript of Gly389Arg polymorphism of β1-adrenergic receptor is associated with the cardiovascular response to...
PHARMACOGENETICS ANDGENOMICS
Gly389Arg polymorphism of �1-adrenergicreceptor is associated with thecardiovascular response to metoprolol
Objectives: Our objectives were to determine whether the Gly389 polymorphism of the �1-adrenergic recep-tor exhibits reduced responsiveness in vivo and to test the hypothesis that the Gly389Arg polymorphismaffects the blood pressure and heart rate response to metoprolol.Methods: �1-Adrenergic receptor genotype was determined by polymerase chain reaction–restriction fragmentlength polymorphism assay. Exercise-induced heart rate increases were compared to determine the functionalsignificance in vivo in 8 healthy Chinese men homozygous for Gly389 and 8 homozygous for Arg389. All ofthe subjects were given 25, 50, or 75 mg of metoprolol every 8 hours; the dosages were given in a randomorder, and each dosage was given for 1 day. The degree of �-blockade was measured as the reduction in restingand exercise heart rates and blood pressures. Plasma metoprolol concentrations were measured by the use ofHPLC–fluorescence detection.Results: Exercise led to a workload-dependent increase in heart rate. There were no differences in exercise-induced heart rate increases between Arg389 and Gly389 homozygotes. Oral metoprolol caused significantdose-dependent decreases in both resting and exercise heart rates in both groups. The reductions in theresting heart rate in 3 dosage levels of metoprolol were 6.3% � 0.8% versus 4.1% � 0.7%, 10.1% � 1.0% versus6.2% � 1.1%, and 14.4% � 1.4% versus 10.9% � 1.3% in homozygous Arg389 subjects and Gly389 subjects,respectively (P � .008). We also found differences with respect to the exercise heart rate (8.9% � 0.5%, 14.0%� 0.9%, and 20.1% � 1.5% in Arg389 subjects and 6.6% � 0.7%, 11.7% � 1.0%, and 16.4% � 1.3% in Gly389subjects; P � .017) and systolic pressure (5.9% � 0.7%, 9.2% � 1.0%, and 11.6% � 1.2% in Arg389 subjectsand 4.6% � 0.5%, 6.0% � 0.8%, and 9.9% � 0.9% in Gly389 subjects; P � .011). However, the difference inthe fall in diastolic pressure was not statistically significant (P � .442).Conclusions: The Arg389 variant of the �1-adrenergic receptor was associated with a greater response tometoprolol than that of Gly389 in young, male Chinese subjects. These data suggested that the �1-adrenergicreceptor Gly389Arg polymorphism is of major functional importance in vivo. (Clin Pharmacol Ther 2003;74:372-9.)
Jie Liu, MD, Zhao-Qian Liu, MD, PhD, Zhi-Rong Tan, BS, Xiao-Ping Chen, MS,PhD, Lian-Sheng Wang, MS, Gan Zhou, MD, and Hong-Hao Zhou, MD Changsha,Hunan, China
From the Pharmacogenetics Research Institute, Institute of ClinicalPharmacology, Central South University.
Supported by the National Science Foundation of China grants No.30070880 and No. F30130210 and China Medical Board grant No.01-755.
Received for publication Feb 10, 2003; accepted June 20, 2003.Reprint requests: Hong-Hao Zhou, MD, Pharmacogenetics Research
Institute, Institute of Clinical Pharmacology, Central South Uni-versity, Changsha, Hunan 410078, China.
E-mail: [email protected] © 2003 by the American Society for Clinical Pharmacol-
ogy & Therapeutics.0009-9236/2003/$30.00 � 0doi:10.1067/S0009-9236(03)00224-8
372

In recent years, there has been increasing interest inthe genetic factors that may influence the dispositionand response to drugs. In addition to genetic polymor-phisms of drug-metabolizing enzymes, there are manydrug receptors that have been emphasized.1 It could beanticipated that a gene defect might be associated witha dysfunction in the receptor protein and subsequentlywith a decreased response to drugs.
�-Adrenergic receptor blockers are the most widelyused agents in the treatment of congestive heart failureand hypertension.2-5 There is a considerable interindi-vidual and interethnic variability in the response to�-adrenergic receptor antagonists.6-8 Changes in theheart rate or blood pressure after administration of�-blockers, even highly �1-selective ones, vary widelyamong healthy or hypertensive subjects.6-8 This is ex-plained partly by differences in pharmacokinetics.Some agents, such as metoprolol and timolol, are me-tabolized by polymorphic cytochrome P450 enzymes,leading to a marked interindividual variability in theplasma concentration.9 In addition, age, smoking, co-administration of other drugs, and underlying diseaseshave all been shown to affect the disposition of�-blockers.10-13 Nevertheless, even allowing for thesefactors, considerable variability remains. In the case ofthe �2-adrenergic receptor, common gene variants havebeen described as affecting both the behavior of thereceptor and the clinical response to �2-agonists.14,15
This has prompted several groups to screen the �1-adrenergic receptor gene for similar functional variantsthat might affect the receptor behavior. Recent studieshave shown that �1-adrenergic receptors are polymor-phic. Podlowski et al16 identified 7 different singlenucleotide polymorphisms, each leading to an aminoacid exchange in the code region of the human �1-adrenergic receptor gene. Two of these polymorphismswere thought to be of functional importance invitro.17,18 One of these was located in the amino ter-minus: An A3G exchange at 145 base pairs (A145G)results in an amino acid substitution of Ser by Gly atresidue 49 (Ser49Gly).19-21 A previous study confirmedthat the amino acid 49 polymorphism of the �1-adrenergic receptor gene affected agonist-promotedtrafficking, with the Gly49 polymorphic receptor hav-ing enhanced agonist-promoted down-regulation.17 An-other single nucleotide polymorphism is 1165G3C,which causes a nonconservative amino acid substitu-tion at residue 389 from Gly to Arg(Gly389Arg).18,20-22 It occurs within a highly con-served motif at the C terminus of the receptor. An invitro study that used site-directed mutagenesis and re-combinant expression in Chinese hamster fibroblasts
confirms that the substitution markedly alters theG-protein coupling of �1-adrenergic receptor, with theArg389 receptor form having nearly 2-fold greaterbasal and 3-fold greater agonist-mediated adenylyl cy-clase activities.18 This dramatic difference suggests thatthe genetic variation of the �1-adrenergic receptor genemay be the basis for interindividual differences inpathophysiologic characteristics or in the response totherapeutic �-adrenergic receptor agonists and antago-nists in cardiovascular and other diseases. Several stud-ies have confirmed the in vivo cardiovascular conse-quence of �1-adrenergic receptor polymorphisms.Sofowora et al23 found that the Arg389 genotype had amarked effect on resting hemodynamic response toatenolol; another study confirmed that �1-adrenergicreceptor haplotypes with respect to codon 49 and codon389 polymorphisms were an important determinant ofthe antihypertensive response to metoprolol.24 In thisstudy, in 16 healthy volunteers who were homozygousfor either the Gly389 or the Arg389 polymorphism, wedetermined exercise-induced increases in the heart rate,which are known to be mediated solely by cardiac�1-adrenergic receptor stimulation. We also assessedthe functional significance of the Gly389Arg �1-adrenergic receptor polymorphism by comparing car-diovascular responses to metoprolol in the 2 groups ofvolunteers.
METHODSSubjects. The study protocol was approved by the
Ethics Committee of Xiangya School of Medicine,Central South University, Hunan, China. One hundredtwenty-three unrelated male volunteers aged 18 to 21years were recruited after providing written informedconsent. After genotype detection, 8 subjects homozy-gous for Gly389 and 8 homozygous for Arg389 wereselected for measuring �1-adrenergic receptor sensitiv-ity and the �1-blockade effect of metoprolol. The se-lected subjects were all homozygous Ser49 to excludethe potential effect of this polymorphic site. All werestudents at Xiangya School of Medicine, Central SouthUniversity. They were of average physical fitness, andnone exercised regularly. Normal health was estab-lished by medical history, routine laboratory tests,physical examination, and electrocardiography. All ofthe subjects were nonsmokers, were drug-free for atleast 2 weeks before entry into the study, and hadabstained from coffee and alcohol for a week before thestudy.
Genotyping procedures for �1-adrenergic recep-tor. Genomic deoxyribonucleic acid (DNA) was ex-tracted from peripheral lymphocytes with phenol-
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 4 Liu et al 373

chloroform followed by ethanol precipitation.25
Genotyping analysis was conducted by the polymerasechain reaction–restriction fragment length polymor-phism (PCR-RFLP) assay. The PCR of the �1-adrenergic receptor gene was performed as describedpreviously with minor modification.20 Because thecomplementary DNA sequence of the human �1-adrenergic receptor gene was GC-rich, a commercialadvantage GC-rich genomic PCR buffer (TaKaRa Bio-tech, Dalian, China) was used to obtain more legiblebands in electrophoresis. For the Ser49Gly locus, weused the primer pair as follows: the sense primer P1(5'-CCGGGCTTCTGGGGTGTTCC-3') and the anti-sense primer P2 (5'-GGCGAGGTGATGGCGAGGTAGC-3'). The final 25 �L of PCR mixture contained5.25 �L of PCR-grade water, 12.5 �L of 2� PCRbuffer (Mg��), 4 �L of deoxyribonucleoside triphos-phates (2.5 �mol/L each), 1.5 �L of primer (10 �mol/Leach), 0.25 �L of Taq DNA polymerase (5 U/�L;TaKaRa Biotech), and 1.5 �L of genomic DNA sam-ple. Temperature cycling proceeded as follows: initialdenaturation for 1 minute at 94°C, followed by 30cycles of 30 seconds at 94°C, 1 minute at 62°C, 1minute at 72°C, and a terminal extension for 7 minutesat 72°C. The Gly389Arg polymorphic locus was am-plified by the use of the sense primer P3 (5'-CATCATGGGCGTCTTCACGC-3') and the antisenseprimer P4 (5'-TGGGCTTCGAGTTCACCTGC-3').The reaction system and amplification conditions weresimilar to those of the A145G locus, except that thedenaturation temperature was 60°C. The amplifiedDNA fragments including the Ser49Gly or Gly389Argpolymorphic site were separately digested withEcoO109I (TaKaRa Biotech) or BcgI (England Bio-labs, Beverly, Mass) at 37°C for 8 hours. The differentpatterns of the digested fragments were visualized onethidium bromide–stained 2% agarose gel.
Protocol. The volunteers and investigators wereblinded with regard to genotype in this study. The heartrate and blood pressure were measured by an automaticblood pressure monitor with Intellisense (Omron, To-kyo, Japan), which allows the detection of alterations inthe heart rate by �1 beat/min and in the blood pressureby �1 mm Hg. All experiments were performed in aquiet, air-conditioned room and with an almost identi-cal time schedule. Our study was carried out in 4 days;on 1 day, subjects received no drug and there were 3additional study days for each level of metoprolol, witha 1-week interval between study days. The subjectsfasted for at least 3 hours before bicycle exercise.Before metoprolol treatment, the baseline heart ratewas measured after 30 minutes of supine rest. The
subjects then did exercise using an ergometrics bicycle(Ergoline GmbH, Windhagen, Germany) at increasingworkloads of 25, 50, and 75 W, each load for 3 minutes.The heart rate was measured and recorded at the last 10seconds of each load level to evaluate �1-adrenergicreceptor sensitivity. The effect of genotypes on thecardiovascular response to metoprolol was assessedafter metoprolol (AstraZeneca Pharmaceutical Com-pany, Ltd, Wuxi, China) treatment by measuring theresting heart rate, exercise heart rate (measured duringthe last 10 seconds of 9 minutes of exercise), and bloodpressure. Each subject underwent treatment for 1 daywith each dosage level of metoprolol (ie, 25, 50, or 75mg every 8 hours). The order of administration wasrandomized according to a random-number table. Threehours after the last dose of metoprolol at each dosagelevel, the heart rate and blood pressure were measured.At the same time, a blood sample (6 mL) was drawnfrom the vein for the measurement of metoprolol con-centration. The subjects then performed treadmill exer-cise at increasing workloads of 25, 50, and 75 W, eachload for 3 minutes, with a total of 9 minutes of exercise.In the last 10 seconds, the heart rate and blood pressurewere measured.
Plasma metoprolol concentration measured by theuse of HPLC fluorescence detection. Fifty microliters(50 ng/mL) of propranolol (Sigma Chemical Co, StLouis, Mo) was added to a 1-mL plasma sample as theinternal standard for assaying metoprolol, both ofwhich were extracted with dichloromethane. The ali-quot of the organic layer, after being shaken vigorouslyfor 3 minutes and centrifuged for 10 minutes (3500rpm), was transferred to another glass tube and evapo-rated to dryness under a gentle stream of nitrogen at37°C. Residues were reconstituted by 50 �L of theHPLC mobile phase. The HPLC was performed on a5-�m Zorbax C8 column (4.6 mm � 250 mm internaldiameter; Agilent Technologies, Inc, Palo Alto, Calif)at the excitation wavelength of 230 nm and the emis-sion wavelength of 310 nm at 29.5°C of column tem-perature. The mobile phase was a mixture of methanol/water/glacial acetic acid/triethylamine (70:30:0.12:0.03[vol/vol]) at a flow rate of 1.0 mL/min. The retentiontimes of metoprolol and the internal standard were6.984 and 5.411 minutes. The intra-assay and interas-say coefficients of variation for metoprolol were 3.7%and 4.0%, respectively.
Statistical analysis. Data analysis was performedwith SPSS (version 10.0 for Windows; SPSS Inc, Chi-cago, Ill). The independent t test was used to comparethe metoprolol concentrations of 2 groups. Pearsoncorrelation analysis was used to test the relationship
CLINICAL PHARMACOLOGY & THERAPEUTICS374 Liu et al OCTOBER 2003
between the plasma metoprolol concentration and car-diovascular response. An unpaired Student t test wasused to compare demographic and resting hemody-namic data. The blood pressure and heart rate (exercise-induced increases or treatment-related decreases) werecompared by use of the general liner model option ofSPSS to provide repeated-measures ANOVA,Gly389Arg genotype was used as a factor, and themetoprolol concentration and body mass index wereused as covariates. Linear regression for metoprololconcentration to response was compared by t test and Ftest. All values are reported as mean � SEM in thefigures and text, unless stated otherwise. A 2-tailedvalue of P � .05 was considered statisticallysignificant.
RESULTSGenotype result. All of the subjects could be geno-
typed unambiguously for Gly389Arg and Ser49Glypolymorphisms of the �1-adrenergic receptor. Wefound that in the 123 volunteers the allele frequenciesof Gly49 and Arg389 were 13.2% and 75.6% (data notshown), respectively. The frequencies of the polymor-phisms are similar to those in various whitepopulations,16,18-22 but the frequency of the Gly389variant is significantly lower than that shown in a blackpopulation.21,24
Baseline characteristics of subjects. The baselinecharacteristics of the 2 genotype groups are summa-rized in Table I. The age, height, weight, and body massindex did not differ between the subjects with theGly389 polymorphism and those with the Arg389 poly-morphism. Basal values for the heart rate were 72.6 �1.9 beats/min among Arg389 homozygotes and 68.0 �1.6 beats/min among Gly389 homozygotes (P � .084).
The systolic blood pressure and diastolic blood pressurewere not statistically different between the 2 groups.
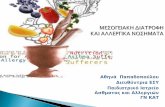
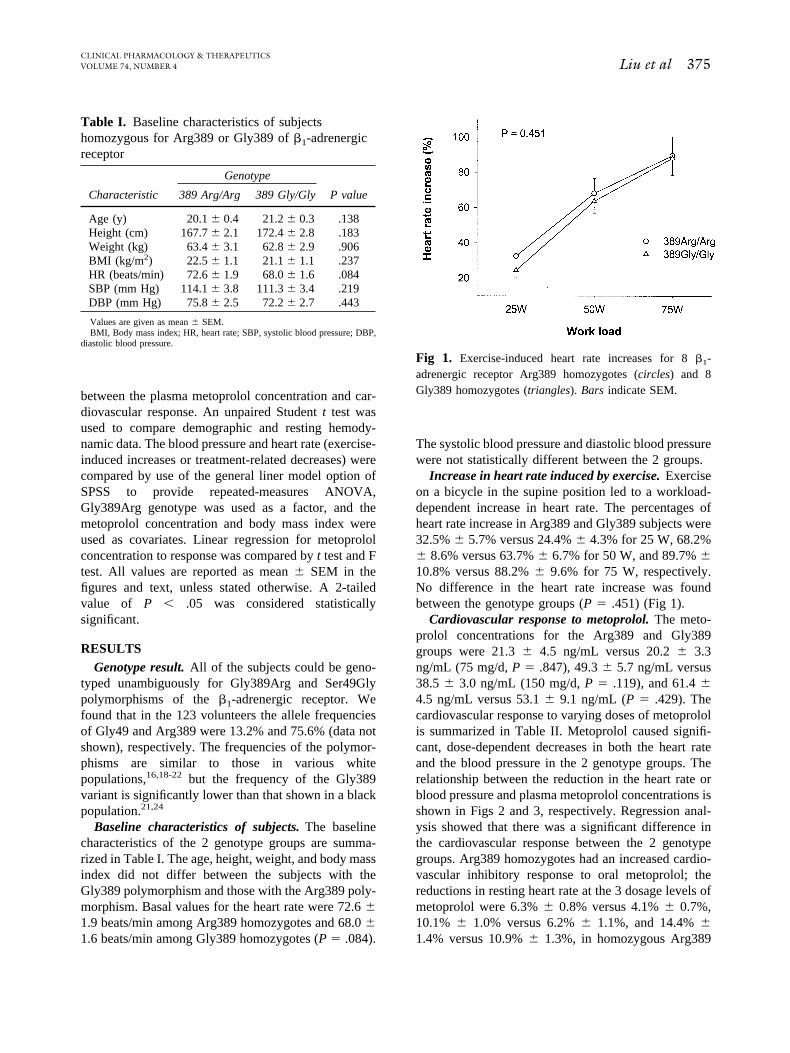
Increase in heart rate induced by exercise. Exerciseon a bicycle in the supine position led to a workload-dependent increase in heart rate. The percentages ofheart rate increase in Arg389 and Gly389 subjects were32.5% � 5.7% versus 24.4% � 4.3% for 25 W, 68.2%� 8.6% versus 63.7% � 6.7% for 50 W, and 89.7% �10.8% versus 88.2% � 9.6% for 75 W, respectively.No difference in the heart rate increase was foundbetween the genotype groups (P � .451) (Fig 1).
Cardiovascular response to metoprolol. The meto-prolol concentrations for the Arg389 and Gly389groups were 21.3 � 4.5 ng/mL versus 20.2 � 3.3ng/mL (75 mg/d, P � .847), 49.3 � 5.7 ng/mL versus38.5 � 3.0 ng/mL (150 mg/d, P � .119), and 61.4 �4.5 ng/mL versus 53.1 � 9.1 ng/mL (P � .429). Thecardiovascular response to varying doses of metoprololis summarized in Table II. Metoprolol caused signifi-cant, dose-dependent decreases in both the heart rateand the blood pressure in the 2 genotype groups. Therelationship between the reduction in the heart rate orblood pressure and plasma metoprolol concentrations isshown in Figs 2 and 3, respectively. Regression anal-ysis showed that there was a significant difference inthe cardiovascular response between the 2 genotypegroups. Arg389 homozygotes had an increased cardio-vascular inhibitory response to oral metoprolol; thereductions in resting heart rate at the 3 dosage levels ofmetoprolol were 6.3% � 0.8% versus 4.1% � 0.7%,10.1% � 1.0% versus 6.2% � 1.1%, and 14.4% �1.4% versus 10.9% � 1.3%, in homozygous Arg389
Table I. Baseline characteristics of subjectshomozygous for Arg389 or Gly389 of �1-adrenergicreceptor
Characteristic
Genotype
P value389 Arg/Arg 389 Gly/Gly
Age (y) 20.1 � 0.4 21.2 � 0.3 .138Height (cm) 167.7 � 2.1 172.4 � 2.8 .183Weight (kg) 63.4 � 3.1 62.8 � 2.9 .906BMI (kg/m2) 22.5 � 1.1 21.1 � 1.1 .237HR (beats/min) 72.6 � 1.9 68.0 � 1.6 .084SBP (mm Hg) 114.1 � 3.8 111.3 � 3.4 .219DBP (mm Hg) 75.8 � 2.5 72.2 � 2.7 .443
Values are given as mean � SEM.BMI, Body mass index; HR, heart rate; SBP, systolic blood pressure; DBP,
diastolic blood pressure.
Fig 1. Exercise-induced heart rate increases for 8 �1-adrenergic receptor Arg389 homozygotes (circles) and 8Gly389 homozygotes (triangles). Bars indicate SEM.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 4 Liu et al 375
subjects and Gly389 subjects, respectively (P � .008).We also found differences between the Gly389 andArg389 groups with respect to the exercise heart rate (P� .017) and systolic pressure (P � .011). All of thedoses of metoprolol caused a significant decrease in thediastolic pressure; however, the difference was not sta-tistically significant between the 2 groups (P � .442).
DISCUSSIONGenetic differences may greatly alter the response of
individuals to a number of drugs. Such differences mayarise from genetically conditioned deficiencies in drugmetabolism or in receptor sensitivity. This study inves-tigated the potential effects of the �1-adrenergic recep-tor Gly389Arg polymorphism on the sensitivity of thisreceptor and the cardiovascular response to metoprolol.
The �1-adrenergic receptor is the predominant sub-type expressed in the human heart and plays an impor-tant role in the physiologic and pathophysiologic reg-ulation of the cardiovascular system.26 A number ofstudies have made it clear that signaling through thisreceptor subtype is important for both cardiac chronot-ropism and cardiac inotropism.26 It is generally ac-cepted that the dynamic exercise-induced increase inthe heart rate is mediated by cardiac �1-adrenergicreceptor stimulation, because it is antagonized by �1-adrenergic receptor blockers, such as bisoprolol oratenolol, but not by �2-adrenergic receptor blockers.27
On the basis of these findings, we adopted the exercise-induced heart rate as an index for evaluating the sen-sitivity of �1-adrenergic receptor. Previous studiesdemonstrated a significantly higher resting heart rate,diastolic pressure, and double product among personshomozygous for the Arg389 genotype than amongthose with other codon 389 genotypes.28 Our resultsshowed that basal values for the heart rate were 72.6 �
19 beats/min among the Arg389 homozygotes and 68.0� 1.6 beats/min among the Gly389 homozygotes. Thisstudy failed to find a significant effect of the 389 locuson resting heart rate (P � .084), which may be due tothe fact that the gene effect of this polymorphism mayhave been significant but was so small that the samplesize (n � 8 for 2 genotypes) used in our study did notallow detection.
We found no difference in exercise-induced heartrate increase between subjects who were homozygousfor the 389Arg allele and those homozygous for the389Gly allele. This finding, in agreement with the ob-servations by other authors, demonstrated no evidenceof an association between this polymorphism and heartrate responses to exercise; despite this 2 studies did notsubclassify their subjects with respect to the Ser49Glypolymorphism of the �1-adrenergic receptor; this poly-morphism had significant effects on the receptor func-tion and resting heart rate.17,29,30
It has long been known by cardiologists who haveused �-blockers in patients with heart failure or hyper-tension that there are responders and nonresponders tothis therapy.31,32 Many attempts have been made toidentify responders, but the association with differentmarkers is only slight. Our data showed that the sub-jects with the Arg389 genotype had an exaggeratedresponse of the heart rate and systolic blood pressure tometoprolol. Because plasma metoprolol concentrationsdid not show significant differences between the 2groups, we can infer from our results that the altereddose-response relationship reflected a difference in theresponse to similar concentrations. Furthermore, ourstudy indicated that there were differences in the re-duction of resting heart rate, exercise heart rate, andsystolic blood pressure between the 2 genotypes inresponse to each metoprolol concentration, with
Table II. Cardiovascular responses to varying dosages of metoprolol in subjects with different �1-adrenergicreceptor genotypes
Metoprololdosage (mg)
� Resting HR(beats/min)
� RestingHR (%)
� Exercise HR(beats/min)
� ExerciseHR (%)
� SBP(mm Hg)
� SBP(%)
� DBP(mm Hg)
� DBP(%)
389Arg75 4.5 � 0.7 6.3 � 0.8 6.5 � 0.8 8.9 � 0.5 6.7 � 1.0 5.9 � 0.7 5.1 � 0.9 6.3 � 0.6150 7.1 � 0.9 10.1 � 1.0 12.0 � 1.2 14.0 � 0.9 10.1 � 0.9 9.2 � 1.0 6.6 � 1.0 10.2 � 1.2225 10.4 � 1.4 14.4 � 1.4 17.5 � 1.9 20.1 � 1.5 12.3 � 0.9 11.6 � 1.2 9.3 � 1.0 13.2 � 1.5
389Gly75 3.1 � 0.7 4.1 � 0.7 4.2 � 0.5 6.6 � 0.7 6.5 � 1.1 4.6 � 0.5 3.8 � 0.7 5.3 � 0.5150 4.9 � 1.0 6.2 � 1.1 9.5 � 0.9 11.7 � 1.0 8.6 � 1.1 6.0 � 0.8 5.4 � 0.9 9.1 � 1.1225 6.5 � 1.2 10.9 � 1.3 13.3 � 1.1 16.4 � 1.3 10.8 � 1.1 9.9 � 0.9 7.9 � 7.7 12.9 � 1.4
P value .006 .008 .027 .017 .021 .011 .178 .442
� Exercise HR was calculated as the difference in HR at last 10 seconds of total 9-minute exercise, with and without metoprolol. P values were of repeat measureddate ANOVA between genotypes, with plasma metoprolol as a covariate.
CLINICAL PHARMACOLOGY & THERAPEUTICS376 Liu et al OCTOBER 2003
Arg389 homozygous subjects having a larger decreasein heart rate and systolic blood pressure. Our resultssuggested that the Gly389Arg polymorphism of the�1-adrenergic receptor would appear to represent a
useful predictor in deciding which subjects are mostlikely to benefit from the administration of a �1-adrenergic receptor antagonist. These results may ex-plain some variability in the response to �-blockers.
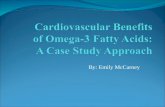
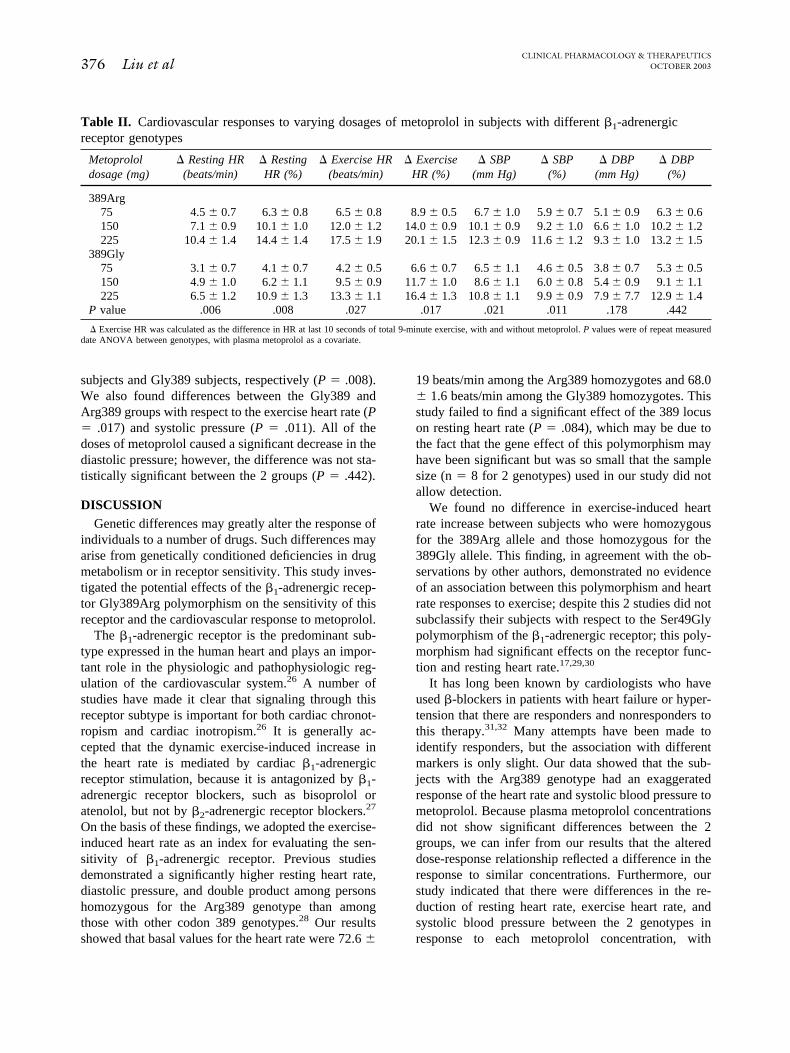
Fig 2. Relationship between resting heart rate reduction (A) or exercise heart rate reduction (B) andplasma metoprolol concentrations for 8 volunteers homozygous for Arg389 (circles) and 8 volun-teers homozygous for Gly389 (triangles) of �1-adrenergic receptor polymorphism. Solid linerepresents regression line for Arg389, and broken line represents regression line for Gly389. Thedecrease in resting heart rate (P � .001) and in exercise heart rate (P � .027) was significantlydifferent between genotypes.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 4 Liu et al 377
For example, decreased sensitivity to �-blockers inblack patients could be explained in part by the higherfrequency of the Gly389 allele.29,33
Our study failed to find a significant effect of theGly389Arg polymorphism on the reduction in diastolicpressure response to metoprolol. The likely reason wasthat the diastolic pressure was not as predominantlyregulated by the �1-adrenergic receptor as heart rateand systolic pressure. In addition, systolic pressure wasmainly mediated by heart rate and cardiac output,which are attributed to the functions of �1-adrenergicreceptors, whereas the diastolic blood pressure ismainly determined by peripheral vascular resistance.
We only studied healthy, young, male Chinese sub-jects. Therefore we do not know whether the resultscould be extended to other populations (eg, older pop-ulations, women, and patients with hypertension). Inaddition, our study was not designed to test the long-term effects of metoprolol, so the longer-duration ef-fects of genetic polymorphisms on cardiovascular re-sponse to metoprolol need to be studied further.
In summary, the Gly389Arg polymorphism of the�1-adrenergic receptor was associated with the cardio-vascular response to metoprolol in our homogeneousgroup of young male subjects. These results providedevidence for a major role of the Gly389Arg polymor-phism for the short-term effects of metoprolol.
All authors have no conflict of interest.
References1. Vesell ES. Advances in pharmacogenetics and pharma-
cogenomics. J Clin Pharmacol 2000;40:930-8.2. Ambrosioni E, Bacchelli S, Esposti DD, Borghi C. Beta-
blockade in hypertension and congestive heart failure.J Cardiovasc Pharmacol 2001;38(Suppl 3):S25-31.
3. Lund-Johansen P, Ohm OJ. Haemodynamic long-termeffects of metoprolol at rest and during exercise in es-sential hypertension. Br J Clin Pharmacol 1977;4:147-51.
4. Falase AO, Salako LA. Beta-adrenoceptor blockers in thetreatment of hypertension. Afr J Med Sci 1979;8:13-8.
5. Clausen N, Damsgaard T, Mellemgaard K. Antihyperten-sive effect of a non-selective (propranolol) and a cardio-selective (metoprolol) beta-adrenoceptor blocking agentat rest and during exercise. Br J Clin Pharmacol 1979;7:379-83.
6. Venter CP, Joubert PH. Ethnic differences in response tobeta 1-adrenoceptor blockade by propranolol. J Cardio-vasc Pharmacol 1984;6:361-4.
7. Venter CP, Joubert PH, Strydom WJ. The relevance ofethnic differences in hemodynamic responses to thehead-up tilt manoeuvre to clinical pharmacological in-vestigations. J Cardiovasc Pharmacol 1985;7:1009-10.
8. Zhou HH, Koshakji RP, Silberstein DJ, Wilkinson GR,Wood AJJ. Racial differences in drug response: alteredsensitivity to and clearance of propranolol in men ofChinese descent as compared with American whites.N Engl J Med 1989;320:565-70.
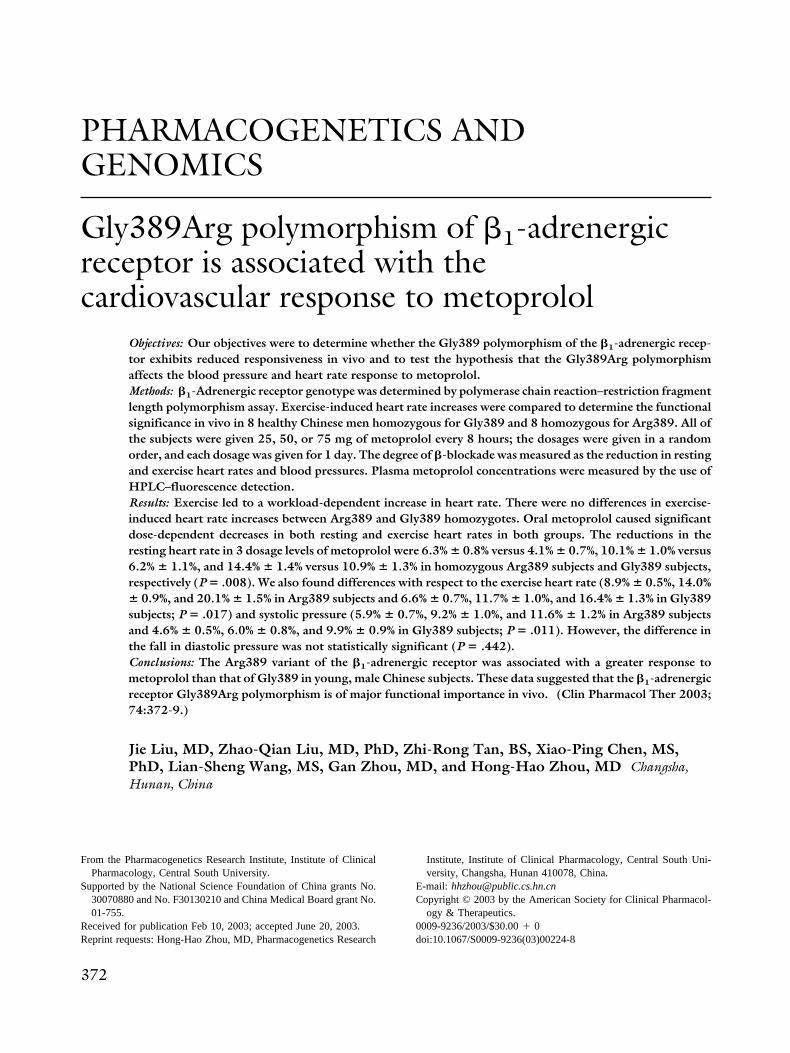
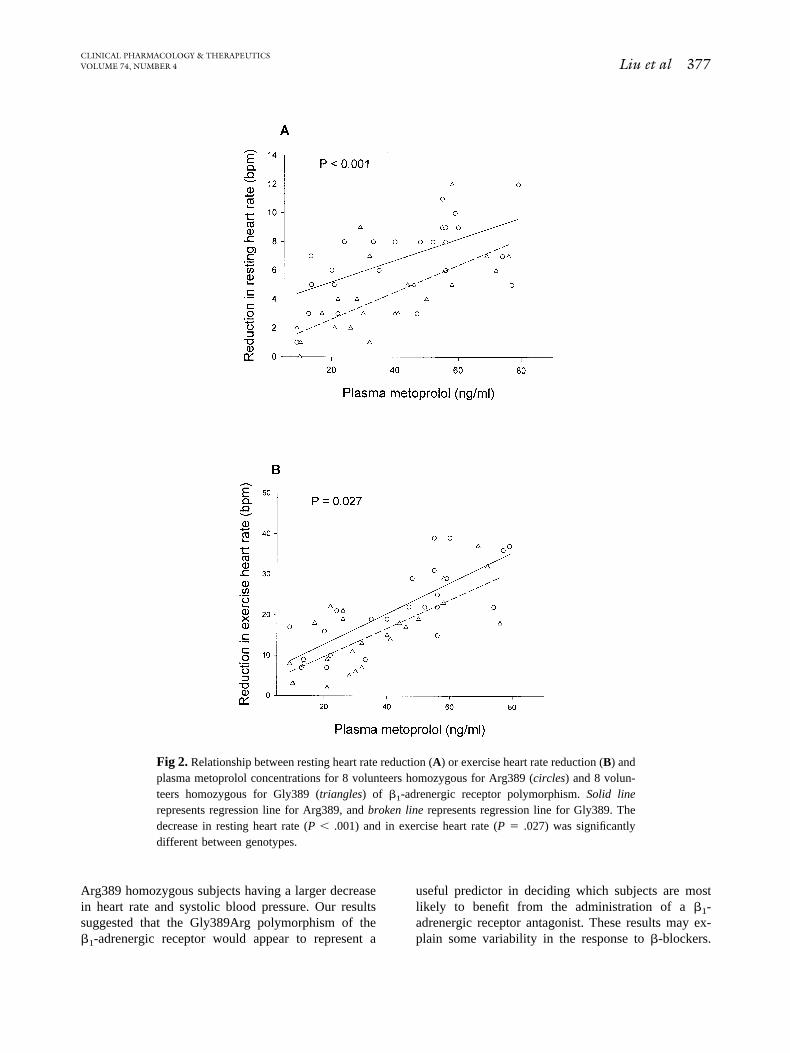
Fig 3. Relationship between systolic blood pressure de-creases (A) or diastolic pressure decreases (B) and plasmametoprolol concentrations for 8 volunteers homozygous forArg389 (circles) and 8 volunteers homozygous for Gly389 (tri-angles) of �1-adrenergic receptor polymorphism. Solid line rep-resents regression line for Arg389, and broken line representsregression line for Gly389. The decrease in systolic blood pres-sure was significantly different between genotypes (P � .013).
CLINICAL PHARMACOLOGY & THERAPEUTICS378 Liu et al OCTOBER 2003

9. Lennard MS, Silas JH, Freestone S, Ramsay LE, TuckerGT, Woods HF. Oxidation phenotype: a major determi-nant of metoprolol metabolism and response. N EnglJ Med 1982;307:1158-60.
10. Castleden CM, Kaye CM, Parsons RL. The effect of ageon plasma levels of propranolol and practolol in man.Br J Clin Pharmacol 1975;2:303-6.
11. Vestal RE, Wood AJ, Shand DG. Reduced beta-adrenoceptor sensitivity in the elderly. Clin PharmacolTher 1979;26:181-6.
12. Vestal RE, Wood AJ, Branch RA, Shand DG, WilkinsonGR. Effects of age and cigarette smoking on propranololdisposition. Clin Pharmacol Ther 1979;26:8-15.
13. Feely J, Crooks J, Stevenson IH. The influence of age,smoking and hyperthyroidism on plasma propranololsteady state concentration. Br J Clin Pharmacol 1981;12:73-8.
14. Green SA, Turki J, Innis M, Liggett SB. Amino-terminalpolymorphisms of the human �2-adrenergic receptor im-part distinct agonist-promoted regulatory properties. Bio-chemistry 1994;33:9414-9.
15. Martinez FD, Graves P E, Baldini M, Solomon S, Erick-son R. Association between genetic polymorphisms ofthe beta-2-adrenoceptor and response to albuterol in chil-dren with and without a history of wheezing. J ClinInvest 1997;100:3184-8.
16. Podlowski S, Wenzel K, Lutter HP, Muller J, BramlageP, Baumann G, et al. �1-adrenoceptor gene variations: arole in idiopathic dilated cardiomyopathy? J Mol Med2000;78:87-93.
17. Rathz DA, Brown KM, Kramer LA, Liggett SB. Aminoacid 49 polymorphisms of the human �1-adrenergic re-ceptor affect agonist-promoted trafficking. J CardiovascPharmacol 2002;39:155-60.
18. Mason DA, Moore JD, Green SA, Liggett SB. A gain-of-function polymorphism in a G-protein coupling do-main of the human �1-adrenergic receptor. J Biol Chem1999;274:12670-4.
19. Borjesson M, Magnusson Y, Hjalmarson A, AnderssonB. A novel polymorphism in the gene coding for thebeta(1)-adrenergic receptor associated with survival inpatients with heart failure. Eur Heart J 2000;21:1853-8.
20. Maqbool A, Hall AS, Ball SG, Balmforth AJ. Commonpolymorphisms of �1-adrenoceptor: identification andrapid screening assay [letter]. Lancet 1999;353:897.
21. Moore JD, Mason DA, Green SA, Hsu J, Liggett SB.Racial differences in the frequencies of cardiac �1-adrenergic receptor polymorphisms: analysis ofc145A3G and c1165G3C. Hum Mutat 1999;14:271.
22. Tesson F, Charron P, Peuchmaurd M, Nicaud V, Cam-bien F, Tiret L, et al. Characterization of a unique geneticvariant in the �1-adrenoceptor gene and evaluation of itsrole in idiopathic dilated cardiomyopathy. CARDIGENEGroup. J Mol Cell Cardiol 1999;31:1025-32.
23. Sofowora GG, Dishy V, Muszkat M, Xie HG, Kim RB,Harris PA, et al. A common beta1-adrenergic receptorpolymorphism (Arg389Gly) affects blood pressure re-sponse to beta-blockade. Clin Pharmacol Ther 2003;73:366-71.
24. Johnson JA, Zinen I, Puckett BJ, McGorray SP, YarandiHN, Pauly DF. �1-Adrenergic receptor polymorphismsand antihypertensive response to metoprolol. Clin Phar-macol Ther 2003;74:44-52.
25. Sambrook J, Fritsch EF, Maniatis T. Molecular cloning:a laboratory manual. 2nd ed. Cold Spring Harbor (NY):Cold Spring Harbor Laboratory Press; 1989.
26. Johnson M. The beta-adrenoceptor. Am J Respir CritCare Med 1998;158(5 Pt 3):S146-53.
27. Motomura S, Reinhard-Zerkowski H, Daul A, BroddeOE. On the physiologic role of beta-2 adrenoceptors inthe human heart: in vitro and in vivo studies. Am Heart J1990;119(3 Pt 1):608-19.
28. Humma LM, Puckett BJ, Richardson HE, Terra SG,Andrisin TE, Lejeune BL, et al. Effects of �1-adrenoceptor genetic polymorphisms on resting hemody-namics in patients undergoing diagnostic testing for isch-emia. Am J Cardiol 2001;88:1034-7.
29. Xie HG, Dishy V, Sofowara G, Kim RB, Landau R,Smiley RM, et al. Arg389Gly �1-adrenoceptor polymor-phism varies in frequency among different ethnic groupsbut does not alter response in vivo. Pharmacogenetics2001;11:191-7.
30. Buscher R, Belger H, Eilmes K, Tellkamps R, Radke J,Dhein S, et al. In-vivo study do not support a majorfunctional role for the Gly389Arg �1-adrenoceptor poly-morphism in humans. Pharmacogenetics 2001;11:199-205.
31. Krukemyer JJ. Use of beta-adrenergic blocking agents incongestive heart failure. Clin Pharm 1990;9:853-63.
32. De Servi S, Ferrario M, Ghio S, Cioffi P, Angoli L,Bramucci E, et al. Variable response to atrial pacing afterintravenous propranolol in patients with stable exertionalangina. Eur Heart J 1990;11:997-1005.
33. Zhou HH, Wood AJJ. Increased suppression of exercise-induced increase in renin by propranolol in Chinese sub-jects. Clin Pharmacol Ther 1991;50:150-6.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 4 Liu et al 379