Diagnosing Diabetes Mellitus in Adults: Type 1, LADA, Type 2 ...
Upload
shashikiran-umakanthCategory
view
684download
0
GLP-1 and Diabetes
Dr. Shashikiran UmakanthProf & Head, MedicineDr. TMA Pai Hospital, UdupiMMMC, Manipal University

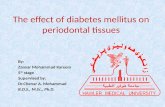
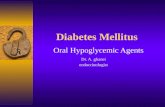
Microvascular changes
Macrovascular changes
Kendall DM, et al. Am J Med 2009;122:S37-S50.Kendall DM, et al. Am J Manag Care 2001;7(suppl):S327-S343.
Rel
ativ
e C
hang
es
β-cell failure
Years-10 -5 0 5 10 15 20 25 30
Insulin resistance
Insulin level
0
50100
150200
250
-15
b-cell function
Onsetdiabetes
Glu
cose
(m
g/dL
)Diabetesdiagnosis
50100150200250300350
Fasting glucose
Prediabetes (Obesity, IFG, IGT)
Postmeal Glucose
-10 -5 0 5 10 15 20 25 30-15Years
Natural history of type 2 diabetes

Case
A 58-year-old gentleman, Mr Kumar, a building contractor with
Type 2 diabetes Hypertension Obesity Recurrent balanoposthitis

Mr Kumar
He is on treatment with Metformin 1000mg 1-0-1 Enalapril 10mg 1-0-0 Rosuvastatin 0-0-1 Vitamin supplements
Complains of Nocturia Discomfort while passing
urine Abdominal bloating - “gas”
Has very irregular eating habits

Examination Gen exam - normal
except abd obesity Eyes - normal CVS & RS - normal Abdomen - normal Nervous system -
absent ankle reflexes
Pulse - 80/min, regularBP 130/80Weight - 84 kgBMI - 30.8
Mr Kumar

Investigations FBS - 150 PPBS - 265 HbA1c - 8.7% Creatinine - 1.2 Potassium - 4.1 LFT - normal
Lipid profile Cholesterol - 230 Triglycerides - 215 HDL - 32 LDL - 155
Urine 8 WBCs/HPF
Mr Kumar

Kumar doesn’t want to take an injection. Which antidiabetic would you add to metformin?
1. Sulfonylurea2. Pioglitazone3. DPP-4 inhibitor4. Voglibose5. SGLT-2 inhibitor6. Bromocriptine
Mr Kumar


In patients with type 2 diabetes and inadequate glycaemic control on metformin monotherapy, the addition of sitagliptin or glimepiride led to similar improvement in glycaemic control after 30 weeks.
Sitagliptin was generally well tolerated. Compared to treatment with glimepiride, treatment with sitagliptin was associated with a lower risk of hypoglycaemia and with weight loss versus weight gain

Treatment with metformin plus vildagliptin compared with metformin plus sulphonylurea is expected to result in a lower incidence of diabetes-related adverse events and to be a cost-effective treatment strategy.

Started on Vildagliptin 50mg 1-0-1 Rosuvastatin 20mg 0-0-1 Metformin and Enalapril continued
Balanoposthitis treated
Mr Kumar - Progress

Glucagon-like peptide 1 (GLP-1)

GLP-1
An incretin (hormone that increases insulin secretion in response to a meal)
30-amino acid peptide secreted in response to the oral ingestion of nutrients by intestinal L cells
GLP-1 receptors (GLP-1R) are located in islet cells, central nervous system, and other organs
GLP-1 is metabolized by the enzyme dipeptidyl peptidase-4 (DPP-4)

Seru
m In
sulin
Time (min)
Incretin Effect*
*
**
* *
*
Oral Glucose
Intravenous Glucose(Isoglycemic)
60 120 1800
Adapted from Circulation. 2011; 124: 2285-2289First described in New Interpretation of Oral Glucose Tolerance. Lancet. 1964 Jul 4;2(7349):20-1.
A phenomenon whereby a glucose load delivered orally produces a much greater insulin secretion than the same glucose load administered intravenously

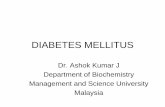
Numerous functions of GLP-1
Stomach: Helps regulate
gastric emptying
Promotes satiety and reduces appetite
Liver: Glucagon reduces
hepatic glucose outputBeta cells:Enhances glucose-dependent
insulin secretion
Alpha cells: Glucose-dependent
postprandialglucagon secretion
Data from Flint A, et al. J Clin Invest 1998;101:515-520. Data from Larsson H, et al. Acta Physiol Scand 1997;160:413-422.Data from Nauck MA, et al. Diabetologia 1996;39:1546-1553. Data from Drucker DJ. Diabetes 1998;47:159-169.
GLP-1: Secreted upon the ingestion of food

GLP-1 preserves human islet cell morphology and function in cultured islets in vitro
Day 1
Day 3
Day 5
Control GLP-1 treated Farilla et al. Endocrinology. 2003 Dec;144(12):5149-58

Comparison of incretins
YesYesPromotes insulin biosynthesis
NoYesReduces food intake
NoYesDecreased secretion in T2DM
YesYesKnockout mice (result in IGT)
YesYesStimulates beta-cell mass/growth
NoYesSlows gastric emptying
NoYesInhibits glucagon secretion postprandially
Site of ProductionGIP
K-cells(Duodenum and Jejunum)
GLP-1L-cells
(Ileum and Colon)

Microvascular changes
Macrovascular changes
Kendall DM, et al. Am J Med 2009;122:S37-S50.Kendall DM, et al. Am J Manag Care 2001;7(suppl):S327-S343.
Rel
ativ
e C
hang
es
β-cell failure
Years-10 -5 0 5 10 15 20 25 30
Insulin resistance
Insulin level
0
50100
150200
250
-15
b-cell function
Onsetdiabetes
Glu
cose
(m
g/dL
)Diabetesdiagnosis
50100150200250300350
Fasting glucose
Prediabetes (Obesity, IFG, IGT)
Postmeal Glucose
-10 -5 0 5 10 15 20 25 30-15Years
Natural history of type 2 diabetes
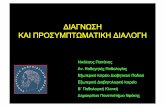
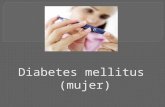
Incretin effect

Incretin effect is blunted in type 2 diabetesIn
sulin
(mU
/L)
Time (min)
Healthy Subjects
Insu
lin (m
U/L
)Time (min)
Type 2 Diabetes
N = 22; Mean (SE); *P0.05 Data from Nauck M, et al. Diabetologia 1986;29:46-52.
0
20
40
60
80
0 60 120 1800
20
40
60
80
0 60 120 180
Intravenous (IV) GlucoseOral Glucose
Reduced Incretin EffectIncretin Effect
*
**
*
*
**
***

GLP-1 has a short half-life - 2 min
Glu Gly Thr Phe Thr Ser Asp
Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Ile Ala Trp Leu Val Lys Gly Arg Gly
Val
Ser
Glu
Phe
Lys
DPP-4
His Ala
7
37
9

Therapeutic potential of GLP-1HOW DO WE LEVERAGE IT?

HbA1c Goals unmet in most
AACE/ACE recommended target (<6.5%)
ADA recommended target (<7%)
1. Data from Saydah SH, et al. JAMA 2004; 291:335-342.2. Calculated from Koro CE, et al. Diabetes Care 2004; 27:17-20. 3. Data from ADA. Diabetes Care 2003; 26(suppl 1):S33-S50.4. Data from ACE. Endocrine Practice 2002.
8.0
9.5
HbA1c (%)
6.0
8.5
10.0
6.5
5.5
9.0
7.0
7.5
37.2% have A1C >8%
20.2% have A1C >9%
12.4% have A1C >10%
64.2% of patients with type 2 diabetes have A1C 7%

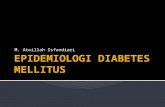
Contribution of PPBS to HbA1c%
Con
trib
utio
n
HbA1c Range (%)
0
20
40
60
80
100
FPG (Fasting Plasma Glucose)PPG (Postprandial Plasma Glucose)
>10.2
70%
30%
9.3-10.2
60%
40%
8.5-9.2
55%
45%
7.3-8.4
50%
50%
<7.3
30%
70%
Data from Monnier L, et al. Diabetes Care 2003; 26:881-885.

Incretin based therapies

GLP-1 infusion restores glucose homeostasis in type 2 diabetes
0
2
4
6
8
10
12
14
16
00:00 04:00 08:00 12:00 16:00
SnackLunchBreakfast
Gluc
ose
(mm
ol/L
)
Time of day
Type 2 diabetes: Saline (n=8) Type 2 diabetes: Exogenous GLP-1 (n=7) Healthy subjects (n=6)
20:00
Continuous GLP-1 infusion

DPP-4
GLP-1
GLP-1R
Synthetic GLP-1R Agonists
DPP-4 inhibitors

Incretin based therapies
GLP-1 Analogueso Exenatideo Liraglutideo Lixisenatideo Albiglutideo Dulaglutide
DPP-4 Inhibitorso Sitagliptino Vildagliptino Saxagliptin o Linagliptino Anagliptino Teneligliptino Alogliptino Trelagliptino Omarigliptin
GLP-1 secretion is reduced in type 2 diabetes
Natural GLP-1 is rapidly degraded by DPP-4
Parenteral, potent Oral, less potent

Exendin-4
Gila monster: a species of venomous lizard; Mexico
Eats only 4 times a year When fasting, it shuts down the
pancreas, stopping insulin When its time to eat, it restarts
pancreas with exendin-4 in its saliva -
a GLP-1R agonist
Exenatide is a synthetic version of exendin-4

DPP-4 Inhibitors (Gliptins)

Saxagliptin
VildagliptinSitagliptin
Linagliptin
Incretin Based Therapies: DPP-4 Inhibitors
DPP-4 Inhibitorso Sitagliptino Vildagliptino Saxagliptin o Linagliptino Anagliptino Teneligliptino Alogliptino Trelagliptino Omarigliptin
Teneligliptin

Sitagliptin 100 mg once/day 79% eliminated
unchanged by the kidney
Slight increased risk of pancreatitis (?)
25-50mg/day in renal failure
in HbA1c vs Placebo = -0.65%
Placebo (n=224)Sitagliptin 100 mg (n=453)
Add-on to Metformin Study
7.0
7.2
7.4
7.6
7.8
8.0
8.2
0 6 12 18 24Time (weeks)
(%)
(P<0.001)
in HbA1c vs Placebo = -0.70%
Add-on to Pioglitazone Study
Placebo (n=174)Sitagliptin 100 mg (n=163)
7.0
7.2
7.4
7.6
7.8
8.0
8.2
0 6 12 18 24Time (weeks)
HbA
1c (%
)
(P<0.001)
HbA
1c
Charbonnel B et al Diabetes Care. 2006;29:2638-2643Rosenstock J et al. Clin Ther. 2006;28:1556-1568

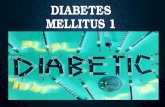
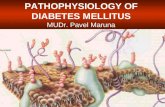
Vildagliptin
125
175
225
275
Glucose(mg/dl)
60
80
100
120
–30 0 30 60 90 120
Time (min)
Glucagon(pmol/l)
PlaceboVildagliptin
50mg twice/day 79% eliminated
unchanged by the kidney
Slight increased risk of skin lesions (?)
2
6
10
14
GLP-1(pmol/l)

HbA1c /weight : FAS, hypoglycemia : safety set, insulin : randomized set .*P < 0.001.
.Diabetes Obes Metab. 2013 Mar;15(3):252-7. doi: 10.1111/dom.12020. Epub 2012 Nov 1. Kothny W1, Foley J, Kozlovski P, Shao Q, Gallwitz B, Lukashevich V.
8.80
Vildagliptin 50 mg bidPlacebo Between-treatment difference
Weight Change from BL to EP
227 221N =
Hypoglycemic Events
-1.0
-0.8
-0.6
-0.4
-0.2
0.0 -0.05
-0.72
Mea
n ch
ange
(SE)
in H
bA1c
, %
BL = 8.84N = 215221
HbA1c Change from BL to EP
*
BL = 78.878.1N = 215222
Mea
n ch
ange
(SE)
in
bod
y w
eigh
t, kg
Vildagliptin add-on with insulin

Saxagliptin
Adjusted mean change in HbA1c from baseline to wk 24
Adjusted mean change in HbA1c frombaseline versus placebo
* *
*
*
#
Saxagliptin + TZDs
Saxagliptin + Metformin
2.5-5 mg once/day Primarily
eliminated by the kidney
Most potent DPP-4i Increased risk of
heart failure
N Engl J Med 2013; 369:1317-1326

Linagliptin 5 mg/day Entero-hepatic
excretion, 84.7% eliminated in feces
No dosage adjustment in renal disease
This 24-week, double-blind, placebo-controlled study randomized 791 individuals with T2 DM that were drug naïve with an A1c> 7.5% and <11% or that were using one oral antidiabetic drug (metformin) with an A1c >7.0 and <10.5%.

Teneligliptin
Changes in a plasma glucose and b serum insulin levels in response to the oral glucose tolerance test before and after 12 weeks of teneligliptin administration. Data are expressed as mean ± standard error (SE). *p < 0.05, **p < 0.01, before vs. after 12 weeks of teneligliptin administration. 12W 12 weeks
20 mg/day Improves early
phase insulin secretion too
Slight increase in free fatty acid levels
No dosage adjustment in renal disease
Ito R et al. Drugs R D (2015) 15:245–251

Limitations with some therapies with type 2 diabetes & renal impairment
GLP-1 receptor agonists
Metformin
Sulfonylurea
Pioglitazone
DPP-4 inhibitors
Insulin
Acarbose
SGLT-2 inhibitors
Renal functionNormal Mild RI Moderate Severe Terminal
GFR (mL/min) >90 60–90 <60 <30 <15

DPP-4 inhibitors in renal failure
Sitagliptin1
DPP-4 inhibitors
100 mg o.d. 50 mg o.d. 25 mg o.d.
Saxagliptin2
5 mg o.d.Linagliptin4
Vildagliptin5 50 mg o.d.50 mg b.i.d.
CreatinineClearance (mL/min) 30
Mild RI Moderate RI Severe RI
50
2.5 or 5 mg o.d. 2.5 mg o.d.
1. Available at: http://www.merck.com/product/usa/pi_circulars/j/januvia/januvia_pi.pdf; 2. Available at: http://www1.astrazeneca-us.com/pi/pi_onglyza.pdf#page=1;3. Available at: http://general.takedapharm.com/content/file.aspx?FileTypeCode=NESINAPI&cacheRandomizer=7236cffb-eb6c-4b0a-ac79-26810425c89e;
4. Available at: http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBase=renetnt&folderPath=/Prescribing+Information/PIs/Tradjenta/Tradjenta.pdf;5. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000771/WC500020327.pdf

GLP-1 Receptor Agonists

GLP1 receptor agonists
Short acting Exenatide Lixisenatide
Lower PPBS levels By delaying of gastric emptying Stimulation of insulin secretion
Long acting Albiglutide Dulaglutide Exenatide QW Liraglutide
Lower blood glucose levels Stimulation of insulin secretion Reduction of glucagon levels

Comparison of short 7 long-acting GLP-1R agonistsShort Acting GLP-1RA Long Acting GLP-1RA
Compounds ExenatideLixisenatide
Albiglutide, DulaglutideExenatide-QW, Liraglutide
Half-life 2-5 hr 12h - many days
HbA1c reduction Modest Strong
FBS reduction Modest Strong
PPBS reduction Strong Modest
Glucagon secretion Yes Yes
Gastric emptying Delayed No effect
Blood pressure Reduction Reduction
Heart rate No effect Modest increase (2-5bpm)
Weight reduction 1-5 kg 2-5 kg
Nausea 20-50%, slow attenuation 20-40%, quick attenuation
Route of administration Subcutaneous Subcutaneous

Short acting GLP-1 R agonists
Exenatide S.C twice daily Rapid absorption, peak in ~2
hours Little metabolism in circulation Clearance is glomerular
filtration
Liraglutide S.C once daily Peak in 8-12 hrs Elimination t½ is 12-14 hours Clearance is primarily through
the metabolic pathways of large plasma proteins

Long-acting GLP-1R agonists
Better glycemic control than the short-acting GLP 1 receptor agonists‑ Patients have higher insulin levels in the fasting state (and
presumably during the night) 5–10% of patients discontinue treatment due to nausea & vomiting Diarrhoea in ~10–20% of patients - more with long acting
compounds Few cases of acute pancreatitis have been reported
Meier J. Nat. Rev. Endocrinol. 8, 728–742 (2012);

Precautions with GLP-1 agonists
Avoid in patients with prior history of pancreatitis In rats and mice, GLP-1 agonists were found to
increase medullary thyroid cancer (MTC) Not reported in humans so far Avoid in patients with history/ family history of MTC Avoid in patients with MEN-2 syndrome

Efficacy of GLP-1 Receptor Agonists and DPP-4 Inhibitors

Efficacy of GLP-1 Receptor Agonists and DPP-4 Inhibitors: A meta-analysis
Aroda VR et al. Clin Ther. 2012 Jun;34(6):1247-1258.e22
• 80 RCTs (≥12 weeks’ duration in T2DM)
• Mean baseline HbA1c 7.4% - 10.3% (GLP-1RA studies) and 7.2% - 9.3% (DPP-4 inhibitor studies)
• All incretin-based therapies in the meta-analysis were associated with significant reductions from baseline in HbA1c and FPG.

HbA1c reduced from 8.7 to 7.6 LDL reduced from 155 to 110 Weight has remained same Balanoposthitis resolved Patient is willing to start an injectable if required, as he
wants to lose weight
Mr Kumar - 3 months later

What is the best choice now?1. Add sulfonylurea2. Start long-acting insulin3. Start basal-bolus insulin regimen4. Stop gliptin and start GLP-1R agonist5. Continue gliptin and start GLP-1R agonist
Mr Kumar

Gliptin stopped Liraglutide 0.6mg/day SC started, and gradually
increased to 1.2, then 1.8mg/dayMetformin continuedRosuvastatin increased to 40mg/day
Mr Kumar

HbA1c is 6.9%LDL is 90 mg/dLWeight has reduced by 7 kg
Mr Kumar - 6 months later

Summary

GLP-1
Stomach: Helps regulate gastric
emptying
Promotes satiety and reduces appetite
Liver: Glucagon reduces
hepatic glucose outputBeta cells:Enhances glucose-dependent insulin
secretion
Alpha cells: Glucose-dependent
postprandialglucagon secretion
GLP-1: Secreted upon the ingestion of food
Enhanced understanding of the complicated physiological mechanisms governing postprandial glucose homeostasis

Choice between DPP-4 inhibitors and GLP-1 agonists
Elderly: Consider DPP-4 inhibitors because of moderate effect on lowering blood glucose and neutral effect on caloric intake
Young diabetics, recent onset diabetes, abdominal obesity: consider GLP-1 analogs
Moderate-severe renal failure: DPP-4 inhibitors (in reduced doses) are safe, but GLP-1 analogs are generally contraindicated
Diabetes Care May 2011. 34:Suppl 2; S276-8
Age
Weight
Compliance
Affordability

Thank you

Pathophysiology of Type 2 Diabetes
Insulin Resistance
Relative Insulin Deficiency
Hyperglycemia(Diabetes)
Incretin Defect