gada ECG pattern and not Brugada syndrome.
21
Transcript of gada ECG pattern and not Brugada syndrome.


ly members, inducibility of ventricular arrhythmiasduring programmed electrical stimulation, syncope,or nocturnal agonal respiration, or a mutation com-patible with the syndrome.14,15 Patients displaying thecharacteristic type-1 ECG without further clinical cri-teria should be described as having an idiopathic Bru-gada ECG pattern and not Brugada syndrome.14
The Brugada syndrome is a channelopathy thatcauses dysfunction of a cardiac channel participating inthe action potential. The electrical dysfunction favorsthe development of arrhythmias. The electrical disorder
is primary, that is, without concomitant underlyingstructural heart disease responsible for the arrhythmiccomplications. Brugada syndrome is thought to be re-sponsible for 4-12% of all SCD and for 20-50% of SCDin subjects without structural cardiopathy.15,16 Its preva-lence has been estimated to be 5/10,000 inhabitants, al-though this rate should be viewed with caution becausemany patients present concealed forms of the disease,thus making it likely that the real prevalence is higher.There exist also ethnic and geographical differences.15
For example, while in a Japanese study a type-1 ECG
Figure 1. Scientific publications on Brugada syndrome from its first description to date. Articles foundin the PubMed database using the search keywords “Right bundle branch block AND ST segment ele-vation AND sudden death” OR “Brugada syndrome”. Light areas indicate review articles.
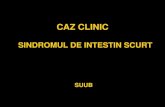
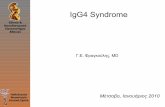
Figure 2. Three different ECG patterns in right precordial leads frequently observed in pa-tients with Brugada syndrome: A) type-1, otherwise called “coved-type” ECG pattern, inwhich a descendent ST-segment elevation is followed by negative T waves; B) type-2 or sad-dleback pattern, an ST-segment elevation followed by positive or biphasic T waves; C) type-3,either a coved-type or a saddleback morphology with ST-segment elevation <1 mm (see textfor more detailed description). A type-1 ECG pattern is required to establish the definite diag-nosis of Brugada syndrome.

pattern was observed in 12/10,000 inhabitants,17 the fewavailable data on North American and European popu-lations point to a much lower prevalence.18,19 SoutheastAsian cultures have long recognized the so-called sud-den unexplained death syndrome (SUDS), also namedBangungot (in the Philippines), Pokkuri (in Japan) orLai Tai (in Thailand), today known to be phenotypical-ly, genetically and functionally the same disorder as theBrugada syndrome.20 SUDS is considered to be ende-mic in these countries and the leading cause of naturaldeath in males younger than 50.16
Genetics of the Brugada syndrome
Inheritance in Brugada syndrome occurs as an autoso-mal dominant trait.15 In up to 60% of patients the dis-ease can be sporadic, that is, absent in parents and oth-er relatives.21 The first mutation related to the syndro-me was described by our group in 1998 and was identi-fied in the SCN5A gene that encodes the ·-subunit ofthe cardiac sodium channel.9 To date, more than 100other different mutations associated with the syndromehave been found.12,13,20,22-25 Functional studies per-formed with expression systems have demonstrated aloss of function of the sodium-channel current (INa),which can occur through different mechanisms (Figure3): a decrease in the number of sodium channels due toa failure in expression (Figure 3A); or qualitative dys-function of the sodium channel due to impaired kinet-ics (a shift in the voltage- and time-dependence activa-
Table 1. Diagnostic criteria of the Brugada syndrome.15
Appearance of a type-1 ST-segment elevation (coved-type) ≥2 mm in more than one right precordial lead (V1–V3):� either spontaneously� or after sodium-blocker exposure
AND
One of the following:detnemucoDnoitallirbif ralucirtnev detnemucoD �
ralucirtnevaidracyhcat ralucirtnev cihpromylop )gnitanimret fleS( �
saimhtyhrrademmargorp htiw saimhtyhrra ralucirtnev fo ytilibicudnI �electrical stimulation
ylimaFsraey 54 erofeb htaed neddus fo yrotsih ylimaF �yrotsihsrebmem ylimaf ni GCE epyt-devoc a fo ecneserP �
� Syncope Arrhythmia-related
smotpmysnoitaripser lanoga lanrutcoN �
Other factor(s) that might account for the ECG abnormality should be ruled out.
{{{
tion, inactivation or reactivation, an entry into an inter-mediate state of inactivation, or an accelerated inactiva-tion) (Figure 3B).9,12,13,20,22-25
Mutations in the SCN5A gene are currently found inonly 18% to 30% of patients with Brugada syndrome.15
In a study by Schulze-Bahr et al, the incidence of SCN5Amutations varied widely according to whether the pa-tients were familial or sporadic cases of Brugada syn-drome. While SCN5A mutations were present in 38% offamilial forms of the disease, the authors could not iden-tify any SCN5A mutation among the 27 sporadic cases(p=0.001).26 The low incidence of SCN5A mutationsidentified in both familial and sporadic Brugada patientssuggests a genetic heterogeneity of the disease.
A different locus on chromosome 3 (3p22-p24), notlinked to SCN5A, was identified by positional cloningin a large family with Brugada syndrome in 2002.27 Thegene involved has been very recently described: glyc-erol-3-phosphate dehydrogenase 1-like (GPD-1L),which seems to affect the trafficking of the cardiac sodi-um channel to the cell surface.28 The mutation respon-sible (A280V) reduces inward sodium currents by
~50% and SCN5A cell surface by ~31%.28
It is not only mutations leading to a loss of functionin the sodium channel (either through SCN5A or GPD-1L) that can cause Brugada syndrome: loss-of-functionmutations in the cardiac calcium channel CACNA1c(Cav1.2) and its �-subunit CACNB2b can also be re-sponsible for a syndrome overlapping short-QT and theBrugada ECG pattern.29 These findings open new lines

of research, where the concept of Brugada syndrome asa pure sodium channelopathy gives way to the conceptof the syndrome as an ionic imbalance between the in-ward and outward currents during phase 1 of the actionpotential.
Polymorphisms have recently acquired more im-portance in the explanation of certain phenotypes ofgenetic diseases. In the SCN5A locus, the commonH558R polymorphism has been shown to restore (atleast partially) the sodium current impaired by other si-
multaneous mutations causing either cardiac conduc-tion disturbances (T512I)30 or Brugada syndrome(R282H).31 Thus, this polymorphism seems to give riseto less severe phenotypes by reducing the effects ofnearby mutations. Our data on the H558R polymor-phism among 75 genotyped Brugada patients haveshown that those carrying the AA genotype have alonger QRS complex duration in lead II (p=0.017),higher J-point elevation in lead V2 (p=0.013), higher“aVR sign” (p=0.005) and a trend towards more symp-
II II
II
II IV
V0661IV0661ITW
-120 -8 -4 40 80
80mV
120m
-1
-2
-3
-4
-7
Na (nA)
WTG1319V
50 m
Nor
mal
ized
I Na
Nor
mal
ized
I Na
Nor
mal
ized
I Na
0.
0.
0.
0.
0.
1.
-8 -6 -4 -2 20
0.
0.
0.
0.
0.
1.
20 40 60 80 120.
0.
0.
0.
0.
1.
-140 -120 -100 -8 -6 -4 10
500 ms-35 mV
-120 m
-160 m
-20 mV
1000 m-120 m
-20 mV
WTG1319V
80mV
-120mV50 m
V (mV)
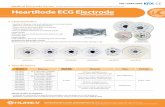
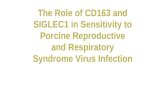
Figure 3. Examples of two different mutations in SCN5A leading to a loss of function of the sodium (Na) channel. A) Mutation I1660V,producing a trafficking defect of the Na channel, and thus a decrease of Na channels present in the sarcolema. Mutant and wild-type (WT)Na channels have been expressed in TSA201 cells and tagged with GFP. A-I) WT channels are present both in the center and the periph-ery of the cell, suggesting that WT channels are manufactured in the cell center and trafficked to the cell membrane. A-II) The fluores-cence distribution of I1660V channels is essentially localized in intracellular organelles, which suggests that mutant channels are manufac-tured but remain trapped within the cell. A-III) Rescue of the mutant channels by incubation at room temperature. (Modified from refer-ence 25 with permission.) B) Mutation G1319V, which modifies the kinetics of the sodium channel. Functional studies performed in HEK-293 cells. B-I) Maximal peak current amplitudes are similar in WT and mutant cells, indicating that the number of functional channels issimilar for WT and mutants. B-II) Voltage-dependence of activation, showing a small depolarizing shift in mutant channels compared toWT channels, with no change in slopes. B-III) Voltage-dependence of steady-state inactivation, reflecting enhanced inactivation in mutantchannels compared to WT. B-IV) Recovery from inactivation, which is markedly slowed in G1319V channels. (Modified from reference 24with permission.)
A
B

toms (p=0.067) than AG or GG carriers. Thus, thiscommon variant H558R seems to be a genetic modula-tor of Brugada syndrome among carriers of an SCN5Amutation, in whom the presence of the less common al-lele G makes Brugada syndrome less severe.
Cellular and ionic mechanisms
Experimental studies have elucidated the cellular andmolecular basis for the two clinical diagnostic criteria ofthe Brugada syndrome: the particular ECG morpholo-gy (ST-segment elevation in right precordial leads) andthe susceptibility to VF and SCD.
Figure 4 shows the normal ventricular myocyte ac-tion potential and the major ionic currents involved in
the phases. Sodium loss-of-function conditions, themost commonly encountered disorder in SCN5A muta-tions related to Brugada syndrome, create an imbal-ance between outward and inward positive currentsduring phase 1, favoring repolarization and the appear-ance of a particular notch in the action potential medi-ated by the transient outward potassium current (Ito)(dashed line). Under normal conditions,32 some degreeof phase-1 notch of the action potential is present in theepicardium (particularly in the right ventricle), but theaugmented notch present in Brugada patients gives riseto a transmural voltage gradient between epicardiumand endocardium, resulting in the characteristic ST-segment elevation on the ECG (Figure 5).16 This hy-pothesis has been confirmed by experimental studies
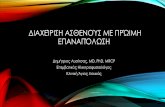
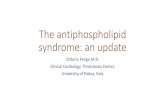
Figure 4. Ventricular myocyte action potential and main underlying ionic currents.The shaded area highlights phase 1, mostly determined by the balance between in-ward sodium and calcium currents (INa and ICa), and transient outward potassiumcurrents (Ito). When positive inward currents are impaired with respect to positiveoutward currents (*), the cell achieves a greater degree of repolarization and the nor-mal dome of the action potential is lost, leading to the development of a particularnotch at the end of phase 1 (dashed line). This is the basis of sodium loss-of-functionchannelopathies such as the Brugada syndrome.

with arterially perfused canine wedge preparations,11
and also by human studies with recordings of monopha-sic action potentials from the epicardium and endo-cardium of the right ventricular outflow tract.33
Ventricular arrhythmias in Brugada syndrome canalso be explained by the imbalance between outwardand inward positive currents during phase 1 of the ac-tion potential. The mechanism involves phase-2 reen-try, which is illustrated in Figure 6. When the notch issuch that phase 1 reaches approximately -30 mV, an all-or-none repolarization leads to a complete loss of theaction potential dome. The heterogeneity of the loss ofthe dome among different sites within the epicardiumand between the epicardium and the endocardium re-sults in epicardial and transmural dispersion of repolar-ization (Figure 6A). This substrate facilitates the de-velopment of premature beats, by means of conductionof the action potential dome from the sites where it ismaintained to the sites where it is lost (Figure 6B).11,16
Studies using high resolution optical mapping in arteri-ally perfused canine right ventricular preparations con-firm the presence of a gradient between dome-loss re-gions and dome-restoration regions in the epicardium,and a subsequent development of a reentrant pathwaythat rotates in the epicardium and gradually involvesthe transmural myocardium (Figure 6C).34
Understanding that the imbalance between in-ward and outward ionic currents in phase 1 is the patho-logical substrate for the Brugada syndrome (Figure 4)has helped the development of experimental models of
Figure 5. Proposed mechanism that underlies ST-segment elevation in Brugada syndrome. The accentuatednotch present in epicardium but not in endocardium gives rise to transmural voltage gradient and J point ele-vation (Brugada saddleback). Further accentuation of the notch may be accompanied by a prolongation of theaction potential in epicardium, which becomes longer than in endocardium, thus leading to the development ofnegative T waves in addition to the ST-segment elevation (Brugada coved-type). (Modified from reference 16with permission.)
the disease, and allows us to explain the effects of cer-tain modulators and certain particularities of the syn-drome. This view also provides very valuable informa-tion for the development of possible therapeutic ap-proaches. In this regard, experimental models of thesyndrome have been developed using the intact wallof arterially perfused canine heart preparations, byadding the potassium opener pinacidil, or a combina-tion of a sodium blocker (flecainide) and acetylcho-line.11 These interventions create a relative predomi-nance of outward positive currents at the end of phase1, and thus accentuate the notch. Recently, the com-bined sodium- and calcium-blocker effect of terfena-dine has been shown to be more effective than sodiuminhibitors alone in precipitating the Brugada syndromein experimental models.35 Even a combination of terfe-nadine and pilsicainide (another sodium blocker) hasbeen used to create phase-2 reentry.34
Modulators of autonomic tone seem to play a rolein the Brugada syndrome through a direct effect onionic currents, since acetylcholine has been shown todecrease calcium currents (ICa) whereas �-adrener-gic agonists increase them.36 Consistent with thesefindings, patients with Brugada syndrome have beenshown to have an increase in ST-segment elevationafter vagal maneuvers, and to attenuate the ECG sig-nature after exposure to �-adrenergic agents.37 Thus,interventions that decrease inward positive currents(such as sodium or calcium blockers) increase ST-seg-ment elevation and could thus be harmful to patients

with Brugada syndrome�although they could never-theless be useful for unmasking concealed forms ofthe disease.38 In contrast, Ito blockers, such as quini-dine, could be a good therapeutic option for reducingthe notch at the end of phase 1.39 Constitutional dif-ferences in the density of ionic currents may also pro-vide an explanation for some of the characteristics ofthe syndrome. Examples supplied by experimental
models are the greater density of Ito currents in rightventricular compared to left ventricular epicardium,40
and also the greater Ito density in male versus femaleright ventricle.41 These findings give a possible expla-nation why Brugada syndrome is a disease mainly ofthe right ventricle and why its phenotypic manifesta-tion is more frequent and severe in male than in femalepatients.
Figure 6. Proposed mechanism that underlies ventricular arrhythmias in Brugada syndrome. A) With a further shift in the balance of cur-rents at the end of phase 1, all-or-none repolarization occurs and leads to a complete loss of the action potential dome (silver figure). Thearrhythmogenic substrate is thought to develop when the loss of dome appears at some epicardial sites but not at others, creating bothtransmural dispersion of repolarization (TDR) and epicardial dispersion of repolarization (EDR) (blue arrows). At this point, a prematureimpulse or extrasystole can induce a reentrant arrhythmia. B) Simultaneous transmembrane action potentials at two epicardial si tes andone endocardial site, together with a transmural electrocardiogram recorded from a canine arterially perfused right ventricular wedgepreparation. The administration of terfenadine (5 �M), a potent sodium and calcium blocker, accentuates the epicardial action potentialnotch (dashed arrow). When combined with continued pacing at basic cycle length 400 ms, all-or-none repolarization occurs heteroge-neously at the end of phase 1, creating local EDR and TDR (solid arrow). Propagation from the site where the dome is maintained (epi-cardial site 1) to the site where it is lost (epicardial site 2) results in development of a premature beat induced by phase 2 re-entry, trigger-ing spontaneous polymorphic ventricular tachycardia. (Modified from reference 34 with permission.) C) High-resolution optical mappingsystem with transmembrane action potentials from 256 sites simultaneously (epicardial and endocardial surface) of an arterially perfusedcanine right-ventricular wedge preparation. Recording at the beginning of a polymorphic ventricular tachycardia. Propagation by phase-2reentry occurs from red areas (where the dome is maintained) towards blue areas (where the dome is lost). The initial re-entrant pathwaymainly rotates in the epicardium and gradually involves the transmural myocardium, precipitating non-sustained polymorphic ventriculartachycardia. (Modified from reference 34 with permission.)
A
C
B

Clinical manifestations of the Brugada syndrome
Patients with Brugada syndrome may remain asymp-tomatic. However, syncope or cardiac arrest, as a con-sequence of an arrhythmic complication such as poly-morphic VT or VF, occur in up to 42% of diagnosedindividuals during their lifetime (before or after thediagnosis).42-45 This rate may overestimate the realprevalence of symptoms among Brugada patients,given that most asymptomatic patients remain under-diagnosed. But on the other hand, many sudden de-aths in young individuals remain unexplained. Theage of symptom occurrence (especially cardiac arrest)is around the fourth decade of life in all published series(Figure 7),42-46 though there is no definite explanationfor this observation thus far. Previous syncope may bepresent in up to 23% of patients who present withcardiac arrest,43 but most cardiac arrests occur as firstmanifestation of the disease.
Up to 20% of patients with Brugada syndromemay suffer from supraventricular arrhythmias,47 andmay complain of palpitations and/or dizziness. An in-creased atrial vulnerability to both spontaneous and in-duced atrial fibrillation has been reported in patientswith Brugada syndrome.48 The electrophysiologic ba-sis seems to be abnormal slow atrial conduction.48
Whether atrial vulnerability is correlated with an in-
creased susceptibility to ventricular arrhythmias is notknown. Other symptoms, such as neurally mediatedsyncope, have also recently been associated with theBrugada syndrome, but their implication for prognosishas not yet been established.49,50
Ventricular arrhythmias and SCD in Brugada syn-drome typically occur at rest, especially during night-time or sleep. In a study by Matsuo et al, 26 out of 30episodes of VF documented in ICD recordings of Bru-gada patients appeared during sleep, suggesting thatvagal activity may play an important role in the ar-rhythmogenesis of Brugada syndrome.51 Indeed, re-cent data on the cardiac autonomic nervous system, as-sessed by positron emission tomography, confirm thatBrugada patients display a certain degree of sympa-thetic autonomic dysfunction, with increased presynap-tic norepinephrine recycling and thus a decrease in theconcentration of norepinephrine at the synaptic cleft;this imbalance facilitates arrhythmogenicity by decreas-ing intracellular levels of cyclic adenosine monophos-phate.52,53
Gender differences
It is currently accepted that the clinical phenotype ofthe Brugada syndrome is 8-10 times more prevalent inmale than in female patients.16,54 Consequently, in the
Figure 7. Incidence of spontaneous ventricular fibrillation (VF) or sudden cardiac death (SCD) dur-ing the lifetime of patients with Brugada syndrome. Data from 370 updated patients of the interna-tional registry. SCD or VF occurred in 120 (32.4%) patients. Presented in the Congreso de las Enfer-medades Cardiovasculares de la Sociedad Española de Cardiologia 2007.46

main clinical studies published thus far 71-77% of pa-tients are male and appear to be generally more symp-tomatic as compared to the female population.42-45 Be-cause specific clinical data on the gender distinctionare, however, lacking, we recently conducted a studythat aimed to analyze gender differences in a large pop-ulation of patients with Brugada syndrome, prospec-tively enrolled in the Hospital Clinic of Barcelona andin UZ Brussel (article in press). The study population(n=384) included 272 males (70.8%) and 112 females(29.2%). General demographic characteristics weresimilar in males and females (mean age 45.8 years), butat diagnosis males presented more frequently withsymptoms (syncope in 18%, previous aborted SCD in6%) than females (14% and 1%, respectively, p=0.04).Males also had higher rates of spontaneous type-1 ECG(47% versus 23%, p=0.0001) and inducibility of VFduring the electrophysiologic study (32% versus 12%,p=0.0001) (Figure 8).
In a recent meta-analysis pooling data from 30studies and including more than 1500 patients, malegender appeared as an independent predictor of car-diac events, defined as SCD, syncope or internal defib-rillator shock, with a risk ratio (RR) of 3.47 (95% confi-dence interval [CI] 1.58 – 7.63) as compared to fe-males.55
Two main hypotheses have been proposed for thegender distinction, perhaps interacting with each other:the sex-related intrinsic differences in ionic currentsand the hormonal influence. Di Diego and coworkers
elegantly demonstrated that Ito density quantified bywhole-cell patch-clamp techniques was significantlygreater in the male than in the female right ventricularepicardia of arterially perfused canine heart prepara-tions,41 thus explaining the deeper notch in phase 1 ofthe action potential in males as compared to females(Figure 10).41 The administration of terfenadine (anNa-Ca blocker) in this model induced transmural andepicardial dispersion of repolarization, thus leading toST-segment elevation and providing a basis for phase-2reentry and VF.41 Both phenomena were observedmainly in male samples, due to their deeper phase-1magnitude at baseline.
The role of sex hormones is not established, al-though some data exist to suggest they might also play arole in the phenotypic manifestations of Brugada syn-drome. Regression of the typical ECG features hasbeen reported in castrated men,56 and levels of testos-terone seem to be higher in Brugada male patients ascompared to controls.57 Some experimental studiespoint out that hormones could modify the ionic mem-brane currents,58,59 but their effect on human currentsis still unclear. In accordance with the hormonal hy-pothesis, the few available data existing thus far of Bru-gada syndrome in children have not shown a differencein phenotypic presentation between boys and girls.60
Children
Although 3 of the 8 patients reported in the first de-
Figure 8. Differences in symptoms, baseline ECGand inducibility of arrhythmias in patients withBrugada syndrome according to gender. Malesare more symptomatic, display a more pathologi-cal ECG at baseline and present more inducibili-ty of ventricular fibrillation (VF) than females.

scription of the disease were within pediatric ages, littleinformation has become available on the clinical presen-tation and prognosis of Brugada syndrome in childhood.Probst et al recently provided data from a multicenterstudy that included 30 Brugada patients aged less than16 years (mean 8 ± 5 years).60 More than half (n=17)had been diagnosed during family screening, but symp-toms were present in 11 patients (1 aborted SCD and 10
syncope). Interestingly, 10 of the 11 symptomatic pa-tients displayed spontaneous type-1 ECG, and in 5 ofthem symptoms were precipitated by fever. Five patientsreceived an ICD and four were treated with hydroquini-dine. During a mean follow-up period of 37 ± 23months, 3 patients (10% of the population) experiencedSCD (n=1) or appropriate shock by ICD (n=2). Impor-tantly, all 3 patients had presented with syncope at the
Figure 9. Kaplan-Meier analysis of cardiacevents�sudden cardiac death or document-ed ventricular fibrillation�during followup, in relation to gender.
Figure 10. Sex-based differences in Ito currents and transmembrane action potentials in a model of arterially per-fused wedge preparations. A) Ito density is significantly greater in male versus female right ventricular (RV) epi-cardia, with no differences in the left ventricle (LV). B) Consequently, male samples present greater phase-1 mag-nitude than females. (Modified from reference 41 with permission.)

time of diagnosis and displayed spontaneous type-1ECG. The 4 patients under quinidine remained asymp-tomatic during 28 ± 24 months of follow up.60
Our results from a larger series of 58 pediatric pa-tients with Brugada syndrome are along the same li-nes. In our population (mean age 11.8 ± 4 years), 22patients (38%) were symptomatic (11 with previoussyncope and 11 with aborted SCD), while 36 had beendiagnosed during family screening. Spontaneoustype-1 ECG was present in 18 patients (31%), and theelectrophysiologic study (EPS), performed in 31 pa-tients, induced VF in 7 of them. An ICD was implant-ed in 14 patients. Cardiac events occurred in 6 patients(2 SCD and 4 appropriate ICD shocks) during a meanfollow-up of 48.8 ± 48 months. Cardiac events occurredmore frequently among patients with spontaneous type-1 ECG and among those with inducible VF during theEPS, but in our series symptoms at diagnosis were thestrongest variable for predicting events during followup (Figure 11).61
Though small, these studies suggest that:� The Brugada syndrome can manifest during child-
hood.� Symptoms may appear particularly during febrile
episodes.� Symptomatic patients, especially if they present
spontaneous type-1 ECG, may be at high risk of car-diac events over a relatively short period of follow up(48 months).
� Patients at risk can be protected by an ICD, althoughquinidine could be an option in certain patients, par-ticularly the youngest.
ECG and modulating factors
As mentioned above, three types of repolarization ab-normalities have been described (Figure 2), but onlythe coved-type ST-segment elevation (type-1 ECG pat-tern) is diagnostic of the syndrome. However, it is im-portant to underline that the ECG typically fluctuatesover time in Brugada patients, and thus can changefrom type-1 to type-2 or type-3, or even be transientlynormal. The prevalence of spontaneous ECG fluctua-tions has been recently assessed in a study by Veltmannet al, including 310 ECGs from 43 patients followed for17.7 months.62 Among 15 patients with an initial diag-nostic ECG, 14 revealed at least one non-diagnosticECG in a median time of 12 days, while 8 out of 28 pa-tients with a non-diagnostic ECG developed a type-1ECG pattern in a median time of 16 days.62 On the ba-sis of these results, it seems that repeated ECG record-ings may be mandatory in patients with the syndromeand, on the other hand, that the role of the baselineECG as a risk marker should be better specified (seerisk stratification).62,63
It is worth noting that a number of factors can ac-count for an ECG abnormality that may closely re-semble the Brugada ECG (Table 2). Importantly,some of them are conditions different than the syn-drome and should be carefully excluded during thedifferential diagnosis, while others may induce ST-segment elevation, probably when an underlying ge-netic predisposition is present.
Modulating factors play a major role in the dynam-ic nature of the ECG and also may be responsible for
Figure 11. Kaplan Meier estimates ofcardiac events�sudden cardiac death(SCD) or documented ventricular fib-rillation (VF)�in children, in relationto symptoms. Note that symptomaticpatients were also more likely to have atype-1 ECG and inducible ventricularfibrillation during EPS.61

the ST-segment elevation in genetically predisposed pa-tients (Table 2). Autonomic balance, hormones, meta-bolic factors and pharmacological agents, by means ofspecific effects on transmembrane ionic currents (Fig-ure 4), are not only thought to modulate the ECG mor-phology, but also explain the development of ventricu-lar arrhythmias under certain conditions. Indeed, bra-dycardia and vagal tone may contribute to ST-segmentelevation and arrhythmia initiation by decreasing calci-um currents.11 This explains the greater ST-segment el-evation recorded in vagal situations,37,64-66 and the noto-rious incidence of cardiac arrhythmias and SCD at nightin patients with Brugada syndrome.51 The role of hor-mones (especially sex hormones) as a modulating factoris less understood, but it is suspected in view of the find-ings of some experimental studies and the male pre-dominance with regard to the clinical manifestations ofthe syndrome.16,56,57,67
Temperature may be an important modulator insome patients with Brugada syndrome. Premature inac-tivation of the sodium channel has been shown to be ac-centuated at higher temperatures in some SCN5A mu-tations, suggesting that febrile states may unmask cer-tain Brugada patients or temporarily increase the riskof arrhythmias.10 Several case reports where fever pre-cipitated the syndrome or an arrhythmic complicationhave been published recently.68,69 It seems that fevercould be a particularly important trigger factor amongthe pediatric population.60
Numerous studies have analyzed the ECG of the
Brugada syndrome, aiming to identify new electrocar-diographic hallmarks or risk markers. Pitzalis and co-workers described a prolongation of the corrected QTinterval (QTc) in right, but not in left precordial leadsafter administration of flecainide in patients withBrugada syndrome and a non-diagnostic baselineECG.70 Subsequently, other groups have correlated aQTc ≥460 ms in V2 with the occurrence of life-threat-ening arrhythmias.71 More recently, the aVR sign (an Rwave ≥3 mm or an R/q ratio ≥0.75 in lead aVR) has al-so been defined as a risk marker of cardiac events inBrugada syndrome; the prominent R wave possibly re-flects right ventricular conduction delay and subse-quently more electrical heterogeneity.72 Studies with12-lead ECGs and signal-averaged ECGs show thatdaily fluctuations of ST-segment elevation are moreprominent in symptomatic than in asymptomatic pa-tients, with a strong dependence on heart rate and vagalactivity.64,65 T-wave alternans in Brugada syndrome hasalso been reported after administration of sodiumchannel blockers, and is thought to be associated withan increased risk of developing VF, since it may reflectincreased transmural dispersion of repolarisation.73 Arecent study, conducted in 77 Brugada patients under-going a pharmacological test, has confirmed that theoccurrence of T-wave alternans after the sodium-block-er exposure identifies a subgroup of patients with a high-er risk of spontaneous VF (52.9% vs. 8.3%, p<0.001).74
Cardiac conduction disturbances may be presentin patients with Brugada syndrome. Both phenotypes
Table 2. ECG abnormalities that can lead to ST-segment elevation in V1-V3.
?noitisopsiderp citeneGsisongaid laitnereffiD
aimelakrepyH -kcolb hcnarb eldnub thgir lacipytA -aimeclacrepyH -VR fo yllaicepse ,noitcrafni laidracoym etucA -
noitacixotni lohocla/eniacoC -sitidracirepoym/sitidracirep etucA - :htiw tnemtaerT -muidracirepomeH -
:sgurd cimhtyhrraitnA .Imsilobme yranomluP -)AI ssalc ,CI ssalc( srekcolb lennahc aN �msyruena citroa gnitcessiD -
srekcolb lennahc aC �sredrosid metsys suovren cimonotua dna lartneC -srekcolb-B � yhportsyd ralucsum ennehcuD -
:sgurd lanignaitnA .IIaixata hcierdeirF -srekcolb lennahc aC �yhportrepyh VL -
setartiN �yhtapoymoidrac VR cinegomhtyhrrA -:sgurd ciportohcysP .IIItcart wolftuo VR fo noisserpmoc lacinahceM -
stnasserpeditna cilcycirT �romut lanitsaideM �� Pectus excavatum � Tetracyclic antidepressants
senizaihtonehP �noisrevoidrac lacirtcele retfA -srotibihni ekatpuer ninotores evitceleS �setelhta ni yllaicepse ,noitaziraloper ylraE -
muihtiL �aimrehtopyH -
LV – left ventricle; RV – right ventricle.

(Brugada syndrome and cardiac conduction disor-ders) can be explained by a reduction of the sodiumcurrent, and have been described within the same fami-ly carrying a mutation on the SCN5A gene.75 Conse-quently, conduction parameters (specifically PQ inter-val, QRS duration and HV interval) seem to be longeramong patients with Brugada syndrome who areSCN5A genetic carriers (and do have a mutation in thesodium channel) as compared to non-SCN5A geneticcarriers, in whom the underlying mechanism or muta-tion is not identified.76 These differences have recentlybeen shown to accentuate progressively during followup.77 We recently identified some conduction parame-ters, such as QRS complex duration, as prognostic indi-cators in Brugada syndrome. In a population of 200Brugada patients, of whom 66 (33%) were sympto-matic, QRS complex duration in V2 was 115 ± 26 ms insymptomatic and 104 ± 19 ms in asymptomatic pa-tients, this difference being statistically significant(p<0.001). The optimized cut-off point of V2 QRS ≥120 ms gave an odds ratio (OR) of 2.5 (95% CI: 1.4-4.6,p=0.003) for being symptomatic.78
Diagnostic tools: drug challenge
The ECG of Brugada syndrome is dynamic and thusthe characteristic ECG hallmark may be concealed. Adrug challenge with sodium channel blockers, which“increase” the sodium channel dysfunction, is a usefultool for the diagnosis.38 Ajmaline, flecainide, procaina-mide, pilsicainide, disopyramide and propafenone havebeen used,15 although the specific diagnostic value foreach of them has not yet been systematically analyzed.The recommended dose regimens for the most com-monly used drugs are listed in Table 3. Brugada syn-drome is diagnosed if a coved-type (type-1 ECG pat-tern) appears after the sodium channel blocker is ad-ministered. The pharmacological test should be moni-tored with a continuous ECG recording and should beterminated when: 1) the diagnostic test is positive; 2)premature ventricular beats or other arrhythmias devel-op; 3) QRS widens to ≥130% of baseline.
Current data indicate that ajmaline is probably thebest available drug for unmasking the Brugada syn-drome. In a study with 147 individuals from 4 large fam-ilies with identified SCN5A mutations, ajmaline had asensitivity of 80%, a specificity of 94.4%, a positive pre-dictive value of 93.3% and a negative predictive valueof 82.9% for the diagnosis of Brugada syndrome.79 Pen-etrance of the disease phenotype increased from 32.7%to 78.6% with the use of the sodium channel blocker.79
Table 3. Drugs used to unmask Brugada syndrome.15
Drug Dosage Administration
Ajmaline 1 mg/kg over 5 min IVFlecainide 2 mg/kg over 10 min IV
OPgm 004Procainamide 10 mg/kg over 10 min IVPilsicainide 1 mg/kg over 10 min IV
IV – intravenous; PO – per os.Modified from reference 15 with permission.
These results are considerably higher than those obtain-ed for flecainide in another study with 110 genotypedpatients, in whom the sensitivity, the specificity, the pos-itive and the negative predictive values for the diagnosiswere 77%, 80%, 96% and 36%, respectively.80 It is im-portant to note that the low negative predictive valueshould be taken into account when using flecainide, es-pecially during genetic screening. In fact, Priori et alhave reported from their series that, among 115 geneti-cally affected individuals, a type-1 ECG (spontaneousor induced by flecainide) was lacking in 29 patients(25%).81 This is a major concern, because it suggeststhat even experts are not capable of correctly reading a12-lead ECG or correctly controlling or being willing tocontrol the position of the ECG leads during the test.
Ajmaline and flecainide were compared in a studyinvolving 22 patients with confirmed Brugada syn-drome, who underwent both ajmaline and flecainidetests. While the test was positive in 22 of 22 patients fol-lowing ajmaline administration, only 15 patients show-ed a positive response to flecainide.82 Also, the increaseof the ST-segment elevation after the test was largerwith ajmaline than with flecainide (Figure 12). Whole-cell patch clamp experiments revealed that flecainidereduced Ito to a greater extent than ajmaline, thus ex-plaining its lower diagnostic accuracy.82
Placement of the right precordial leads in an upperposition (2nd or 3rd intercostal spaces) can increase thesensitivity of the ECG in detecting the Brugada pheno-type.83,84 Recent data demonstrate that the presence ofa type-1 ECG pattern recorded at higher intercostalspaces, even when the standard ECG is normal, canidentify a subgroup of patients that behaves similarly interms of prognosis to those with spontaneous type-1ECG pattern in standard leads (Figure 13).85 There-fore, the diagnosis of Brugada syndrome seems to beimproved by recording at upper intercostals spaces; thisstrategy allows the identification of a subset of patientsat risk who would otherwise have been underdiagnosed.

Prognosis and risk stratification
Prognosis and risk stratification are probably the mostcontroversial issues in Brugada syndrome. The mainclinical studies arising from the largest databases differas regards the risk of SCD or VF in the population with
Brugada syndrome, and particularly with respect todefining the specific risk markers influencing prognosis.
In our most recently updated population withBrugada syndrome, drawn from the international reg-istry, the percentage of patients who experiencedSCD or VF during their lifetime was 25% (178 out of
Figure 12. Ajmaline versus flecainide in the diagnosis of Brugada syndrome. A) Flecainide failed in 7 of 22 cases (32%) that were un-masked by ajmaline. B) Change in maximal ST-segment elevation before (pre) and after (post) intravenous ajmaline (ajm) and flecainide(flec) administration. C) Example of greater ST-segment elevation in the same patient with ajmaline than with flecainide. (Modified fromreference 82 with permission.)
Figure 13. Kaplan-Meier analysis of cardiacevents�sudden cardiac death or documentedventricular fibrillation�during follow up inpatients with spontaneous type-1 ECG patternin standard leads (dashed line), patients withspontaneous type-1 ECG recorded only at ahigher intercostal space (solid line), and pa-tients with type-1 ECG pattern at standardand/or higher intercostal spaces after receivinga sodium channel blocker (dotted line). Nosignificant difference was observed in the fre-quency of cardiac events between the first twogroups. (Modified from reference 85 with per-mission.)
A B
C

724 patients). The mean age at cardiac events was 42± 15 years. Such a high rate of events might have beeninfluenced by a baseline high-risk population recordedin the international registry. Our reported annual rateof events has decreased from the first patients includ-ed in the registry5 to the most recent published se-ries.42,44,86 The change probably reflects the inherentbias during the first years following the description of anovel disease, when particularly severe forms of the dis-ease were those mostly diagnosed.
Several clinical variables have been demonstratedto predict a worse outcome in patients with Brugadasyndrome. In all the analyses of our series over time,the presence of symptoms before diagnosis, a sponta-neous type-1 ECG at baseline, the inducibility of ven-tricular arrhythmias during the EPS, and male genderhave consistently been shown to be related to the oc-currence of cardiac events during follow-up.5,42,44,86
Little controversy exists as to the value of a previ-ous cardiac arrest as a risk marker for future events.Our data show that up to 62% of patients who recoverfrom an aborted SCD are at risk of a new arrhythmicevent within the following 54 months.42 Thus, these pa-tients should be protected with an ICD irrespective ofthe presence or absence of other risk factors (indicationclass I).15 Because there is not such a general agree-ment on the best approach to patients who have never
Figure 14. Kaplan Meier analysis of arrhythmic events�sudden cardiac death or documented ventricular fibrillation (VF)�during followup, in relation to symptoms and inducibility of VF during EPS. (Modified from reference 44 with permission.)
developed ventricular fibrillation, we conducted aprospective study that included 547 individuals withBrugada syndrome and no previous cardiac arrest.44,86
Of these (mean age 41 ± 45 years, 408 males), 124 hadpresented syncope (22.7%), while 423 (77.3%) wereasymptomatic and had been diagnosed during routineECG or family screening. The baseline ECG showed atype-1 ECG pattern spontaneously in 391 patients(71.5%), and after sodium blocker challenge in 156(28.5%). During a mean follow up of 24 ± 32 months,45 individuals (8.2%) developed a first cardiac event(documented VF or SCD).44 By univariate analysis, aprevious history of syncope (HR 2.79, 95% CI 1.5-5.1,p=0.002), a spontaneous type-1 ECG (HR 7.69, 95%CI 1.9-33.3, p=0.0001), male gender (HR 5.26, 95% CI1.6-16.6, p=0.001) and inducibility of ventricular ar-rhythmias during EPS (HR 8.33, 95% CI 2.8-25,p=0.0001) were significantly related to VF or SCD dur-ing follow up. Multivariate analysis identified previoussyncope and inducibility of VF as the only independentrisk factors for the occurrence of events during followup (Figure 14).44 Logistic regression analysis allowedthe definition of eight different categories of risk.Asymptomatic patients with a normal ECG at baselineand no inducible VF during EPS represent the lowestrisk population, whereas patients with syncope, sponta-neous type-1 ECG and VF inducibility during EPS

had the worst outcome (Figure 15). Further analysisindicated that the EPS was particularly useful in pre-dicting cardiac events among asymptomatic patientswith no family history of SCD (“fortuitous cases”,n=167).86 Indeed, 11 out of 167 patients (6%) pre-sented VF during follow up, and the only indepen-dent predictor was inducibility during EPS, while thelack of an EPS was shown to be predictive of effectiveSCD (p=0.002).86
Other groups agree that previous symptoms and aspontaneous type-1 ECG are risk factors, althoughthey have found a much lower incidence of arrhyth-mic events for the whole population (6.5% in 34 ± 44months of follow up in Priori’s work and 4.2% in 40 ±50 months of follow-up in Eckardt’s).43,45 The worseoutcome in our series may possibly reflect a more se-verely ill baseline population.45 The other large reg-istries also agree that VF inducibility during EPS isgreatest among patients with previous SCD or syn-cope,43,45 but have failed to demonstrate the value ofthe EPS in predicting outcome. There could be sever-al reasons for this discrepancy:86 1) the use of multi-ple testing centers with non-standardized stimulationprotocols; 2) the inclusion of patients with type-2 and
type-3 ST-segment elevation (and not type-1) in someseries, suggesting that they may contain individualswho do not have the syndrome; 3) the lack of eventsduring follow up in the other registries. The lattermight change when data from longer follow-up peri-ods are available, since events can only increase dur-ing follow up and thus so does the positive predictivevalue.86 Because this issue is a source of ongoing con-troversy, we are currently performing a new prospec-tive study to determine the role of EPS in the riskstratification of Brugada syndrome.
Male gender has consistently shown a trend to pre-sent more arrhythmic events in all the studies, and haseven been defined as an independent predictor for aworse outcome in a recent meta-analysis.55 A very re-cent study by our group indicates that males with Bru-gada syndrome display a higher-risk profile than fe-males, and thus have a worse prognosis during followup. Multiple ECG parameters have been assessed inthe search for new risk markers, of which a prolongedQTc in right precordial leads, the aVR sign, the pres-ence of T-wave alternans and probably a wide QRScomplex seem to be the most important. Interestingly, apositive family history of SCD or the presence of an
Figure 15. Probability of events in follow up by logistic regression, according to symptoms, inducibility of ventric-ular arrhythmias during EPS, and baseline ECG. Data from reference 44.

SCN5A mutation have not been proven to be riskmarkers in any of the large studies conducted thusfar.42-45,55
Treatment
ICD
The ICD is the only proven effective treatment forBrugada syndrome. On the basis of available clinicaland basic science data, a II consensus conference washeld in September 2003 focused on risk stratificationschemes and approaches to therapy.15 The recom-mendations for ICD implantation stated by this con-sensus are summarized in Figure 16. Briefly, sympto-matic patients should always receive an ICD. An EPScould be performed in these patients to better assess
Figure 16. Indications for ICD implantation in patients with Brugada syndrome. Class I designation indicates clear evidence that the proce-dure or treatment is useful or effective; Class II, conflicting evidence about usefulness or efficacy; Class IIa, weight of evidence in favor ofusefulness or efficacy; Class IIb, usefulness or efficacy less well established.
the sensitivity and specificity of the test in predictingoutcome, and also for the study of supraventriculararrhythmias. Asymptomatic patients may benefitfrom EPS for risk stratification: an ICD should be im-planted in those with inducible VF who have a spon-taneous type-1 ECG at baseline or a sodium blocker-induced ECG with a positive family history of SCD.Finally, asymptomatic patients who have no familyhistory of SCD and who develop a type 1 ECG onlyafter sodium blockade should be closely followed up,though there is neither sufficient evidence for theusefulness of the EPS nor a direct indication forICD.15
From the two main retrospective studies conductedon patients with Brugada syndrome who have receiveda primary prophylactic ICD, it can be concluded thatthe ICD is an effective therapy for patients at risk,87,88

who can have an annual rate of appropriate shocks ofup to 3.7%.88 It is important to note that this rate is notonly comparable to that of other ICD trials dealing withother cardiac diseases, but also applies to young andotherwise healthy people, whose life expectancy couldbe more than 30 years. Therefore, should this rate re-main constant over time, it seems that most patientswould be likely to experience an appropriate shock dur-ing their lifetime.
However, perhaps just because of this youth factor,a noteworthy rate of inappropriate shocks by the devicehas also been reported. In a study by Saher et al, 45 outof 220 patients (20%) had inappropriate shocks dur-ing follow up.87 In our series the rate was even higher(36%).88 The reasons for inappropriate therapies weremainly sinus tachycardia, supraventricular arrhythmias,T-wave oversensing and lead failure.87,88 On the basis ofthese results, and because ICD therapy is not afford-able worldwide, there is a growing effort to find cheap-er approaches to treating the disease.
Pharmacological options
With the aim of rebalancing the ion channel currentsactive during phase 1 of the action potential, so as toreduce the magnitude of the notch (Figure 4), twomain pharmacological approaches have been assessed(Table 4):
� drugs that decrease outward positive currents, suchas Ito inhibitors;
� drugs that increase inward positive currents (ICa,INa).
Quinidine, a drug with Ito- and IKr-blocking prop-erties, has been the most assessed drug in clinical stud-ies. In a work by Belhassen et al, 25 patients with in-ducible VF were treated with quinidine (1483 ± 240 mgp.o.). After treatment, 22 out of 25 patients (88%) wereno longer inducible during the EPS, and none of the 19patients receiving ongoing medical therapy with oralquinidine developed arrhythmias during the follow up(56 ± 67 months).39 However, 36% of the patients hadtransient side effects that led to drug discontinuation.39
Preliminary data have also proven quinidine to be agood adjunctive therapy in patients with ICD and mul-tiple shocks,89 and an effective treatment for electricalstorm associated with Brugada syndrome.90 More re-cently, quinidine has been proposed as a good alterna-tive to ICD implantation in child patients who have thesyndrome and are at high risk for malignant arrhyth-mias.60 However, large, randomized, controlled clinicaltrials assessing the effectiveness of quinidine (whichshould be addressed in patients who have already re-ceived an ICD) are still lacking.
Beta-adrenergic agents, through an increase in ICacurrents, decrease transmural and epicardial disper-sion of repolarization in experimental models.11 Clin-
Table 4. Pharmacological approach to therapy in the Brugada syndrome.
no devorPnoitcA
Ito blockers:)yrtneer 2-esahp fo noisserppus( sledom latnemirepxe ni evitceffEenidiryponima-4 11
Probable neurotoxicity in humans)yrtneer 2-esahp fo noisserppus( sledom latnemirepxe ni evitceffEenidiniuQ 11
Initial results showing effectiveness in clinical practice:- ↓ inducibility of VF39
- ↓ spontaneous VF in follow-up39,89
- Adjunctive therapy in patients with ICD and multiple shocks89
- Effective in electrical storm90
- A possible option in children60
)yrtneer 2-esahp fo noisserppus( sledom latnemirepxe ni evitceffElimasideT 16
)yrtneer 2-esahp fo noisserppus( sledom latnemirepxe ni evitceffE8110EVA 16
ICa activators:)yrtneer 2-esahp fo noisserppus( sledom latnemirepxe ni evitceffE loneretorposI 11
(�-adrenergic agents) Effective in electrical storm91
FV gnitneverp ni stluser yranimilerp laisrevortnoClozatsoliC 92,93
(phosphodiesterase III inhibitor)
INa openers: Dimethyl Lithospermate B (dmLSB) Effective in experimental models (suppression of phase-2 reentry)16
VF – ventricular fibrillation.

ically, they have proven effectiveness in the treatmentof electrical storm associated with Brugada syn-drome.91 Recently, phosphodiesterase III inhibitorshave appeared as a new appealing option, since theywould increase ICa and decrease Ito. Indeed, cilosta-zol prevented ICD shocks in a patient with recurrentepisodes of VF.92 However, another publication report-ed the failure of such a drug in a patient with multipleICD discharges, despite sustained therapy.93
Dimethyl Lithospermate B (dmLSB), an extractof Danshen, a traditional Chinese herbal remedythat slows the inactivation of INa, has recently beenassessed in experimental models, demonstrating areduction of both epicardial and transmural disper-sion of repolarization and abolishing phase 2 reen-try-induced extrasystoles and VT/VF in 9 out of 9preparations. Clinical data from the use of this agentare not yet available, but the results of experimentalstudies suggest that it could be a new candidate forthe pharmacological treatment of Brugada syndro-me.16
References
1. Brugada P, Brugada J. Right bundle branch block, persistentST segment elevation and sudden cardiac death: a distinctclinical and electrocardiographic syndrome. A multicenter re-port. J Am Coll Cardiol. 1992; 20: 1391-1396.
2. Ferracci A, Fromer M, Schlapfer J, Pruvot E, KappenbergerL. Primary ventricular fibrillation and early recurrence: apro-pos of a case of association of right bundle branch block andpersistent ST segment elevation. Arch Mal Coeur Vaiss.1994; 87: 1359-1362.
3. Proclemer A, Facchin D, Feruglio GA, Nucifora R. Recur-rent ventricular fibrillation, right bundle-branch block andpersistent ST segment elevation in V1-V3: a new arrhythmiasyndrome? A clinical case report. G Ital Cardiol. 1993; 23:1211-1218.
4. Brugada J, Brugada P. Further characterization of the syn-drome of right bundle branch block, ST segment elevation,and sudden cardiac death. J Cardiovasc Electrophysiol. 1997;8: 325-331.
5. Brugada J, Brugada R, Brugada P. Right bundle-branchblock and ST-segment elevation in leads V1 through V3: amarker for sudden death in patients without demonstrablestructural heart disease. Circulation. 1998; 97: 457-460.
6. Alings M, Wilde A. “Brugada” syndrome: clinical data andsuggested pathophysiological mechanism. Circulation. 1999;99: 666-673.
7. Priori SG, Napolitano C, Gasparini M, et al. Clinical and ge-netic heterogeneity of right bundle branch block and ST-seg-ment elevation syndrome: a prospective evaluation of 52 fam-ilies. Circulation. 2000; 102: 2509-2515.
8. Brugada P, Brugada R, Brugada J. Sudden death in patientsand relatives with the syndrome of right bundle branch block,ST segment elevation in the precordial leads V1 to V3 andsudden death. Eur Heart J. 2000; 21: 321-326.
9. Chen Q, Kirsch GE, Zhang D, et al. Genetic basis and molec-ular mechanism for idiopathic ventricular fibrillation. Nature.1998; 392: 293-296.
10. Dumaine R, Towbin JA, Brugada P, et al. Ionic mechanismsresponsible for the electrocardiographic phenotype of theBrugada syndrome are temperature dependent. Circ Res.1999; 85: 803-809.
11. Yan GX, Antzelevitch C. Cellular basis for the Brugada syn-drome and other mechanisms of arrhythmogenesis associatedwith ST-segment elevation. Circulation. 1999; 100: 1660-1666.
12. Rook MB, Bezzina Alshinawi C, Groenewegen WA, et al.Human SCN5A gene mutations alter cardiac sodium channelkinetics and are associated with the Brugada syndrome. Car-diovasc Res. 1999; 44: 507-517.
13. Deschênes I, Baroudi G, Berthet M, et al. Electrophysiologi-cal characterization of SCN5A mutations causing long QT(E1784K) and Brugada (R1512W and R1432G) syndromes.Cardiovasc Res. 2000; 46: 55-65.
14. Wilde AAM, Antzelevitch C, Borggrefe M, et al. Proposeddiagnostic criteria for the Brugada syndrome. Eur Heart J.2002; 23: 1648-1654.
15. Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syn-drome: report of the second consensus conference: endorsedby the Heart Rhythm Society and the European Heart RhythmAssociation. Circulation. 2005; 111: 659-670.
16. Antzelevitch C. Brugada syndrome. Pacing Clin Electrophysi-ol. 2006; 29: 1130-1159.
17. Miyasaka Y, Tsuji H, Yamada K, et al. Prevalence and mor-tality of the Brugada-type electrocardiogram in one city in Ja-pan. J Am Coll Cardiol. 2001; 38: 771-774.
18. Donohue D, Tehrani F, Jamehdor R, Lam C, Movahed MR.The prevalence of Brugada ECG in adult patients in a largeuniversity hospital in the western United States. Am HeartHosp J. 2008; 6: 48-50.
19. Hermida JS, Lemoine JL, Aoun FB, Jarry G, Rey JL, QuiretJC. Prevalence of the Brugada syndrome in an apparentlyhealthy population. Am J Cardiol. 2000; 86: 91-94.
20. Vatta M, Dumaine R, Varghese G, et al. Genetic and biophysi-cal basis of sudden unexplained nocturnal death syndrome(SUNDS), a disease allelic to Brugada syndrome. Hum MolGenet. 2002; 11: 337-345.
21. Schulze-Bahr E, Eckardt L, Paul M, Wichter T, Breithardt G.Molecular genetics of the Brugada syndrome. In: AntzelevitchC, Brugada P, editors. The Brugada Syndrome: from Bench toBedside. 1st ed. Blackwell Publishing; 2005. p. 42-51.
22. Vatta M, Dumaine R, Antzelevitch C, et al. Novel mutationsin domain I of SCN5A cause Brugada syndrome. Mol GenetMetab. 2002; 75: 317-324.
23. Pfahnl AE, Viswanathan PC, Weiss R, et al. A sodium chan-nel pore mutation causing Brugada syndrome. Heart Rhythm.2007; 4: 46-53.
24. Casini S, Tan HL, Bhuiyan ZA, et al. Characterization of anovel SCN5A mutation associated with Brugada syndromereveals involvement of DIIIS4-S5 linker in slow inactivation.Cardiovasc Res. 2007; 76: 418-429.
25. Cordeiro JM, Barajas-Martinez H, Hong K, et al. Compoundheterozygous mutations P336L and I1660V in the human car-diac sodium channel associated with the Brugada syndrome.Circulation. 2006; 114: 2026-2033.
26. Schulze-Bahr E, Eckardt L, Breithardt G, et al. Sodium chan-nel gene (SCN5A) mutations in 44 index patients with Bruga-da syndrome: different incidences in familial and sporadicdisease. Hum Mutat. 2003; 2: 651-652.

27. Weiss R, Barmada MM, Nguyen T, et al. Clinical and molec-ular heterogeneity in the Brugada syndrome: a novel gene lo-cus on chromosome 3. Circulation. 2002; 105: 707-713.
28. London B, Michalec M, Mehdi H, et al. Mutation in glycerol-3-phosphate dehydrogenase 1 like gene (GPD1-L) decreasescardiac Na+ current and causes inherited arrhythmias. Cir-culation. 2007; 116: 2260-2268.
29. Antzelevitch C, Pollevick GD, Cordeiro JM, et al. Loss-of-func-tion mutations in the cardiac calcium channel underlie a new clini-cal entity characterized by ST-segment elevation, short QT inter-vals, and sudden cardiac death. Circulation. 2007; 115: 442-449.
30. Viswanathan PC, Benson DW, Balser JR. A commonSCN5A polymorphism modulates the biophysical effects ofan SCN5A mutation. J Clin Invest. 2003; 111: 341-346.
31. Poelzing S, Forleo C, Samodell M, et al. SCN5A polymor-phism restores trafficking of a Brugada syndrome mutationon a separate gene. Circulation. 2006; 114: 368-376.
32. Litovsky SH, Antzelevitch C. Transient outward current pro-minent in canine ventricular epicardium but not endocar-dium. Circ Res. 1988; 62: 116-126.
33. Kurita T, Shimizu W, Inagaki M, et al. The electrophysiologicmechanism of ST-segment elevation in Brugada syndrome. JAm Coll Cardiol. 2002; 40: 330-334.
34. Shimizu W, Aiba T, Kamakura S. Mechanisms of disease:current understanding and future challenges in Brugada syn-drome. Nat Clin Pract Cardiovasc Med. 2005; 2: 408-414.
35. Fish J, Antzelevitch C. Role of sodium and calcium channelblock in unmasking the Brugada syndrome. Heart Rhythm.2004; 1: 210-217.
36. Litovsky SH, Antzelevitch C. Differences in the electrophysi-ological response of canine ventricular subendocardium andsubepicardium to acetylcholine and isoproterenol. A directeffect of acetylcholine in ventricular myocardium. Circ Res.1990; 67: 615-627.
37. Miyazaki T, Mitamura H, Miyoshi S, Soejima K, Aizawa Y,Ogawa S. Autonomic and antiarrhythmic drug modulation ofST segment elevation in patients with Brugada syndrome. JAm Coll Cardiol. 1996; 27: 1061-1070.
38. Brugada R, Brugada J, Antzelevitch C, et al. Sodium channelblockers identify risk for sudden death in patients with ST-segment elevation and right bundle branch block but struc-turally normal hearts. Circulation. 2000; 101: 510-515.
39. Belhassen B, Glick A, Viskin S. Efficacy of quinidine in high-risk patients with Brugada syndrome. Circulation. 2004; 110:1731-1737.
40. Di Diego JM, Sun ZQ, Antzelevitch C. I(to) and action po-tential notch are smaller in left vs. right canine ventricularepicardium. Am J Physiol. 1996; 271 (2 Pt 2): H548-H561.
41. Di Diego JM, Cordeiro JM, Goodrow RJ, et al. Ionic and cel-lular basis for the predominance of the Brugada syndromephenotype in males. Circulation. 2002; 106: 2004-2011.
42. Brugada J, Brugada R, Antzelevitch C, Towbin J, Nadema-nee K, Brugada P. Long-term follow-up of individuals withthe electrocardiographic pattern of right bundle-branch blockand ST-segment elevation in precordial leads V1 to V3. Cir-culation. 2002; 105: 73-78.
43. Priori SG, Napolitano C, Gasparini M, et al. Natural historyof Brugada syndrome: insights for risk stratification and man-agement. Circulation. 2002; 105: 1342-1347.
44. Brugada J, Brugada R, Brugada P. Determinants of suddencardiac death in individuals with the electrocardiographic pat-tern of Brugada syndrome and no previous cardiac arrest. Cir-culation. 2003; 108: 3092-3096.
45. Eckardt L, Probst V, Smits JPP, et al. Long-term prognosis ofindividuals with right precordial ST-segment-elevation Bru-gada syndrome. Circulation. 2005; 111: 257-263.
46. Benito B, Arzamendi D, Porres J, et al. Seguimiento a largoplazo de los pacientes con sindrome de Brugada. Estudiomulticentrico de los factores de mal pronostico. Congreso delas Enfermedades Cardiovasculares de la SEC 2007. 2007(abstract).
47. Eckardt L, Kirchhof P, Loh P, et al. Brugada syndrome andsupraventricular tachyarrhythmias: a novel association? JCardiovasc Electrophysiol. 2001; 12: 680-685.
48. Morita H, Kusano-Fukushima K, Nagase S, et al. Atrial fibril-lation and atrial vulnerability in patients with Brugada syn-drome. J Am Coll Cardiol. 2002; 40: 1437-1444.
49. Benito B, Brugada J. Recurrent syncope: an unusual presen-tation of Brugada syndrome. Nat Clin Pract Cardiovasc Med.2006; 3: 573-577.
50. Makita N, Sumitomo N, Watanabe I, Tsutsui H. Novel SCN5Amutation (Q55X) associated with age-dependent expressionof Brugada syndrome presenting as neurally mediated syn-cope. Heart Rhythm. 2007; 4: 516-519.
51. Matsuo K, Kurita T, Inagaki M, et al. The circadian patternof the development of ventricular fibrillation in patients withBrugada syndrome. Eur Heart J. 1999; 20: 465-470.
52. Wichter T, Matheja P, Eckardt L, et al. Cardiac autonomic dys-function in Brugada syndrome. Circulation. 2002; 105: 702-706.
53. Kies P, Wichter T, Schafers M, et al. Abnormal myocardialpresynaptic norepinephrine recycling in patients with Bruga-da syndrome. Circulation. 2004; 110: 3017-3022.
54. Eckardt L. Gender differences in Brugada syndrome. J Car-diovasc Electrophysiol. 2007; 18: 422-424.
55. Gehi A, Duong T, Metz L, Gomes J, Mehta D. Risk stratifi-cation of individuals with the Brugada electrocardiogram: Ameta-analysis. J Cardiovasc Electrophysiol. 2006; 17: 577-583.
56. Matsuo K, Akahoshi M, Seto S, Yan K. Disappearance of theBrugada-type electrocardiogram after surgical castration: arole for testosterone and an explanation for the male prepon-derance. Pacing Clin Electrophysiol. 2003; 26: 1551-1553.
57. Shimizu W, Matsuo K, Kokubo Y, et al. Sex hormone and gen-der difference-role of testosterone on male predominance inBrugada syndrome. J Cardiovasc Electrophysiol. 2007; 18: 415-421.
58. Bai CX, Kurokawa J, Tamagawa M, Nakaya H, Furukawa T.Nontranscriptional regulation of cardiac repolarization cur-rents by testosterone. Circulation. 2005; 112: 1701-1710.
59. Song M, Helguera G, Eghbali M, et al. Remodeling of Kv4.3potassium channel gene expression under the control of sexhormones. J Biol Chem. 2001; 276: 31883-31890.
60. Probst V, Denjoy I, MeregalIi PG, et al. Clinical aspects andprognosis of Brugada syndrome in children. Circulation.2007; 115: 2042-2048.
61. Benito B, Sarkozy A, Berne P, et al. Características clínicas ypronóstico del síndrome de Brugada en la población pediátrica.Congreso de las Enfermedades Cardiovasculares de la SEC2007. 2007 (abstract).
62. Veltmann C, Schimpf R, Echternach C, et al. A prospectivestudy on spontaneous fluctuations between diagnostic andnon-diagnostic ECGs in Brugada syndrome: implications forcorrect phenotyping and risk stratification. Eur Heart J. 2006;27: 2544-2552.
63. Wilde AA. Spontaneous electrocardiographic fluctuations inBrugada syndrome: does it matter? Eur Heart J. 2006; 27:2493-2494.

64. Extramiana F, Seitz J, Maison-Blanche P, et al. Quantitative as-sessment of ST segment elevation in Brugada patients. HeartRhythm. 2006; 3: 1175-1181.
65. Tatsumi H, Takagi M, Nakagawa E, Yamashita H, Yoshiya-ma M. Risk stratification in patients with Brugada syndrome:analysis of daily fluctuations in 12-lead electrocardiogram(ECG) and signal-averaged electrocardiogram (SAECG). JCardiovasc Electrophysiol. 2006; 17: 705-711.
66. Mizumaki K, Fujiki A, Tsuneda T, et al. Vagal activity modu-lates spontaneous augmentation of ST elevation in the dailylife of patients with Brugada syndrome. J Cardiovasc Electro-physiol. 2004; 15: 667-673.
67. Shimizu W. Gender difference and drug challenge in Bruga-da syndrome. J Cardiovasc Electrophysiol. 2004; 15: 70-71.
68. Gonzalez Rebollo JM, Hernandez MA, Garcia A, Garcia deCA, Mejias A, Moro C. [Recurrent ventricular fibrillation dur-ing a febrile illness in a patient with the Brugada syndrome].Rev Esp Cardiol. 2000; 53: 755-757. Spanish.
69. Porres JM, Brugada J, Urbistondo V, Garcia F, Reviejo K,Marco P. Fever unmasking the Brugada syndrome. PacingClin Electrophysiol. 2002; 25: 1646-1648.
70. Pitzalis MV, Anaclerio M, Iacoviello M, et al. QT-interval pro-longation in right precordial leads: an additional electrocardio-graphic hallmark of Brugada syndrome. J Am Coll Cardiol.2003; 42: 1632-1637.
71. Castro Hevia J, Antzelevitch C, Tornés Bárzaga F, et al. Tpeak-Tend and Tpeak-Tend dispersion as risk factors for ventriculartachycardia/ ventricular fibrillation in patients with the Brugadasyndrome. J Am Coll Cardiol. 2006; 47: 1828-1834.
72. Babai Bigi MA, Aslani A, Shahrzad S. aVR sign as a risk fac-tor for life-threatening arrhythmic events in patients withBrugada syndrome. Heart Rhythm. 2007; 4: 1009-1012.
73. Fish JM, Antzelevitch C. Cellular mechanism and arrhythmo-genic potential of T-wave alternans in the Brugada syndrome.J Cardiovasc Electrophysiol. 2008; 19: 301-308.
74. Tada T, Kusano KF, Nagase S, et al. The relationship betweenthe magnitude of T wave alternans and amplitude of the cor-responding T Wave in patients with Brugada syndrome. JCardiovasc Electrophysiol. 2008; 19: 56-61.
75. Kyndt F, Probst V, Potet F, et al. Novel SCN5A mutation lead-ing either to isolated cardiac conduction defect or Brugada syn-drome in a large French family. Circulation. 2001; 104: 3081-3086.
76. Smits JP, Eckardt L, Probst V, et al. Genotype-phenotype rela-tionship in Brugada syndrome: electrocardiographic featuresdifferentiate SCN5A-related patients from non-SCN5A-relatedpatients. J Am Coll Cardiol. 2002; 40: 350-356.
77. Yokokawa M, Noda T, Okamura H, et al. Comparison oflong-term follow-up of electrocardiographic features in Bru-gada syndrome between the SCN5A-positive probands andthe SCN5A-negative probands. Am J Cardiol. 2007; 100: 649-655.
78. Junttila MJ, Brugada P, Hong K, et al. Differences in 12-leadelectrocardiogram between symptomatic and asymptomaticBrugada syndrome patients. J Cardiovasc Electrophysiol. 2008;19: 380-383.
79. Hong K, Brugada J, Oliva A, et al. Value of electrocardiogra-
phic parameters and ajmaline test in the diagnosis of Brugadasyndrome caused by SCN5A mutations. Circulation. 2004;110: 3023-3027.
80. Meregalli PG, Ruijter JM, Hofman N, Bezzina CR, WildeAA, Tan HL. Diagnostic value of flecainide testing in un-masking SCN5A-related Brugada syndrome. J CardiovascElectrophysiol. 2006; 17: 857-864.
81. Priori SG, Napolitano C. Should patients with an asymptomaticBrugada electrocardiogram undergo pharmacological and elec-trophysiological testing? Circulation. 2005; 112: 279-292.
82. Wolpert C, Echternach C, Veltmann C, et al. Intravenous drugchallenge using flecainide and ajmaline in patients with Bru-gada syndrome. Heart Rhythm. 2005; 2: 254-260.
83. Sangwatanaroj S, Prechawat S, Sunsaneewitayakul B, Sit-thisook S, Tosukhowong P, Tungsanga K. New electrocardio-graphic leads and the procainamide test for the detection ofthe Brugada sign in sudden unexplained death syndrome sur-vivors and their relatives. Eur Heart J. 2001; 22: 2290-2296.
84. Shimizu W, Matsuo K, Takagi M, et al. Body surface distribu-tion and response to drugs of ST segment elevation in Brugadasyndrome: clinical implication of eighty-seven-lead body sur-face potential mapping and its application to twelve-lead elec-trocardiograms. J Cardiovasc Electrophysiol. 2000; 11: 396-404.
85. Miyamoto K, Yokokawa M, Tanaka K, et al. Diagnostic andprognostic value of a type 1 Brugada electrocardiogram athigher (third or second) V1 to V2 recording in men with Bru-gada syndrome. Am J Cardiol. 2007; 99: 53-57.
86. Brugada P, Brugada R, Brugada J, et al. Should patients withan asymptomatic Brugada electrocardiogram undergo phar-macological and electrophysiological testing? Circulation.2005; 112: 279-292.
87. Sacher F, Probst V, Iesaka Y, et al. Outcome after implanta-tion of a cardioverter-defibrillator in patients with Brugadasyndrome: a multicenter study. Circulation. 2006; 114: 2317-2324.
88. Sarkozy A, Boussy T, Kourgiannides G, et al. Long-term fol-low-up of primary prophylactic implantable cardioverter-de-fibrillator therapy in Brugada syndrome. Eur Heart J. 2007;28: 334-344.
89. Hermida JS, Denjoy I, Clerc J, et al. Hydroquinidine therapyin Brugada syndrome. J Am Coll Cardiol. 2004; 43: 1853-1860.
90. Mok NS, Chan NY, Chiu AC. Successful use of quinidine intreatment of electrical storm in Brugada syndrome. Pacing ClinElectrophysiol. 2004; 27 (6 Pt 1): 821-823.
91. Ohgo T, Okamura H, Noda T, et al. Acute and chronic man-agement in patients with Brugada syndrome associated withelectrical storm of ventricular fibrillation. Heart Rhythm. 2007;4: 695-700.
92. Tsuchiya T, Ashikaga K, Honda T, Arita M. Prevention of ven-tricular fibrillation by cilostazol, an oral phosphodiesterase in-hibitor, in a patient with Brugada syndrome. J Cardiovasc Elec-trophysiol. 2002; 13: 698-701.
93. Abud A, Bagattin D, Goyeneche R, Becker C. Failure of cilo-stazol in the prevention of ventricular fibrillation in a patientwith Brugada syndrome. J Cardiovasc Electrophysiol. 2006;17: 210-212.