Full Inferior Vena Cava Agenesis Causing Acute Abdominal ... · Absence of the entire inferior vena...
8
Reprinted from VASCULAR SURGERY Vol. 27, Νο. 2 March 1993 Copyright © 1993 Printed in U.S.A. Αll Rights Reserved Full Inferior Vena Cava Agenesis Causing Acute Abdominal Symptoms: Case Report and Literature Review Anastasios Chr. Liatas, M.D. Soterios Dendrinos, M.D. Socrates Koundourakis, M.D. and Theodore Liakakos, M.D. ATHENS, GREECE Abstrαct Absence of the entire inferior vena cava caused acute abdominal symptoms, and the patient, a twenty-year-old man, was operated on οη an emergency ba- sis. Subsequent ascending venography, abdominal computed tomographic scan, intraarterial digital subtraction angiography, and intraosseous phlebography revealed full inferior vena cava and iliac venous system agenesis, up to and above the level of the hepatic veins, venous return from the lower limbs and the abdominal viscera being through a series of multiple collateral channels and the azygos-hemiazygos system. Introduction The fol1owing developmental anomalies of the inferior vena cava (lVC), which arises from various segments, have been distinguished: (1) left-sided position (0.5% ), (2) duplication (3%), (3) anomalous insertion into the left atrium, (4) agenesis, and (5) stenosis and occlu- sion. 1,2 “Absent IVC” designates a well-defined abnormality with absence of the prerenal (supra- renal) segment of the IVC. 3-6 Various abnormalities of the postrenal (infrarenal) IVC have been reported, but absence of the postrenal segment is indeed very uncommon. 4,6 “Ful1 IVC agenesis,” an extremely rare condition, may be compatible with normal adolescence, 6 and such a congenital abnormality has never to our knowledge caused acute abdominal symptoms. Case Report Α twenty-year-old white man was admitted owing to gradual1y deteriorating constipation, left abdomen pain, pyrexia (38.5°C), and prostration. On examination he was lying stil1 on the From the 2nd Department of General Surgery, Athens General Hospita1, Athens, Greece 155 Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ" A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"
Transcript of Full Inferior Vena Cava Agenesis Causing Acute Abdominal ... · Absence of the entire inferior vena...

Reprinted from VASCULAR SURGERY Vol. 27, Νο. 2 March 1993 Copyright © 1993 Printed in U.S.A.
Αll Rights Reserved
Full Inferior Vena Cava Agenesis Causing Acute Abdominal Symptoms: Case Report and Literature Review
Anastasios Chr. Liatas, M.D. Soterios Dendrinos, M.D. Socrates Koundourakis, M.D.
and Theodore Liakakos, M.D.
ATHENS, GREECE
Abstrαct
Absence of the entire inferior vena cava caused acute abdominal symptoms, and the patient, a twenty-year-old man, was operated on οη an emergency ba- sis. Subsequent ascending venography, abdominal computed tomographic scan, intraarterial digital subtraction angiography, and intraosseous phlebography revealed full inferior vena cava and iliac venous system agenesis, up to and above the level of the hepatic veins, venous return from the lower limbs and the abdominal viscera being through a series of multiple collateral channels and the azygos-hemiazygos system.
Introduction
The fol1owing developmental anomalies of the inferior vena cava (lVC), which arises from various segments, have been distinguished: (1) left-sided position (0.5% ), (2) duplication (3%), (3) anomalous insertion into the left atrium, (4) agenesis, and (5) stenosis and occlu- sion. 1,2 “Absent IVC” designates a well-defined abnormality with absence of the prerenal (supra-renal) segment of the IVC.3-6 Various abnormalities of the postrenal (infrarenal) IVC have been reported, but absence of the postrenal segment is indeed very uncommon.4,6 “Ful1 IVC agenesis,” an extremely rare condition, may be compatible with normal adolescence,6 and such a congenital abnormality has never to our knowledge caused acute abdominal symptoms.
Case Report
Α twenty-year-old white man was admitted owing to gradual1y deteriorating constipation, left abdomen pain, pyrexia (38.5°C), and prostration. On examination he was lying stil1 on the
From the 2nd Department of General Surgery, Athens General Hospita1, Athens, Greece
155
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

156
Vascular Surgery
March, 1993 bed, he was apprehensive, his color was normal, his breath was diaphragmatic (25/min), and his pulse rate was 100/min. His lower extremities were large but not edematous (no pitting edema). He stated that at times his lower extremities would become even larger, especially following vigorous exercise, since childhood. Νο varicose veins, caput medusae, or distended abdominal wall veins were seen, but on inspection the abdomen was slightly prominent in the left iliac fossa. His medical history was unremarkable.
His bowel sounds were diminished, his abdomen was tender and rigid especially on the left side, and rebound tenderness could be elicited. On rectal examination a palpable, soft, tender mass was felt. Hematologic and biochemical reports, urinalysis, chest x-ray, abdominal x-ray, and ECG were within normal reference ranges. An abdominal computed tomographic (CT) scan before and after injection of contrast material disclosed: (1) a collection of fluid in the left prerenal and left retroperitoneal space, (2) a mass having a tube-like appearance beginning just below the left renal vein and extending to the level of the left iliac crest, (3) numerous rounded masses in the pelvis and abdomen quite apart from the opacified bowel, (4) dilatation and significant lateral displacement of the left ureter, and (5) displacement of the urinary bladder to the right and cephalad. During the thirty-six-hour investigation in the hospital the patient fainted twice when he attempted to stay upright.
With the possible diagnosis of an abscess and under combination chemotherapy, the patient was operated on on an emergency basis. Upon entrance to the peritoneal cavity through a midline incision, about 200 mL of blood was found, the sigmoid colon was displaced medially, and the retroperitoneal space was bulging anteriorly, having the appearance of a large, black, grape-like structure and giving the impression of having bled recently. On palpation this struc- ture was soft, but some regions were solid. An attempt to sever the retroperitoneum caused remarkable hemorrhage. Following laborious hemostasis a tube drain was left in place and the abdomen was closed. The next day the patient was feverish (39°C) but stable, and so intraven- ous pyelography (IVP) was performed, which disclosed obstruction of the left ureter at the level of its lower third (Fig. 1).
On the second postoperative day the patient developed extensive edema of both lower extremities extending to the level of the lower abdomen, and he remained pyrexial (39o C). Phlebothrombosis of both lower extremities was confirmed by duplex ultrasonography, and the patient was placed on full-dose heparin regardless of having been operated on recently and the coexistent spontaneous retroperitoneal hemorrhage.
Οn the third postoperative day the patient continued to be feverish and prostrated, and it was decided to have him reexplored in order to relieve the lower third obstruction of the left ureter, for it was thought that this was the most possible cause of his pyrexia. At that time percutaneous renal pelvis drainage was judged to be unsuitable for the patient. Just before reoperation there was heparin reversal with protamine sulfate, and all bleeding parameters were normal. Heparin was reinstituted immediately after operation. During reoperation the left ureter was mobilized and made free of the constricting venules, a stent was placed in it because it had had to be repaired during mobilization, and there was considerable blood loss.
Two days later the temperature returned to normal and the antibiotics were discontinued on the seventh postoperative day, but anticoagulant therapy continued with warfarin. The first signs of improvement of the deep phlebothrombosis were seen on the sixth postoperative day,
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

Liatas ‒ Total Inferior Vena Cava Agenesis
157
and on the twentieth day the patient’s lower extremities had returned to their usual size. The patient was discharged on a warfarin regimen in good condition on the thirtieth postop-
eratiνe day, and bilateral ascending venography (Fig. 2), intraosseous venography (Fig. 3), intraarterial digital subtraction angiography (DSA), a new abdominal CT scan (Fig. 4), and IVP (Fig. 5a, 5b) were scheduled.
These investigations proνed that the patient has total agenesis of his inferior vena caνa (IVC) and iliac venous system, up to and above the leνel of the hepatic νeins, venous return from the lower limbs and the abdominal viscera being through a series of multiple collateral channels and the azygos-hemiazygos system.
Three months later he deνeloped extensiveνe venous collaterals on the lateral aspects of his lower abdomen, especially on the left side (left superficial lower epigastric vein and thora- coepigastric vein). The medial and lateral saphenous νeins on both sides were dilated. These new clinical findings were compatible with those already known from the ascending phlebo- gram of his lower extremities (Fig. 2).
Six months later the patient complained of lower back pain on exertion (quick walking on uphill ground) ceasing three to fiνe minutes following rest. This has been ascribed to venous blood pooling in the retroperitoneal collaterals during exercise due both to still obstructed channels and inadequate superficia1 abdominal wall collaterals. The patient has been instructed to reduce the magnitude of exertion, and his problem has now been solνed.
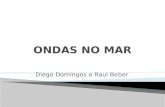
FIG. 2. Bilateral ascending phlebogram of the lower ex-tremities showing occlusion of both saphenous veins in the groin and bilateral total occlusion of both popliteal and fe- moral veins. (Only the left side is presented)
FIG. 1. Intravenous pyelography disclosed complete ob- struction of the left ureter at the junction of its middle and lower third.
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

158
Vascular Surgery
March, 1993
FIG. 3. Intraosseous phlebogram of pelvis and abdomen
showing neither evidence of patent external or common il- iac veins nor of IVC. Very enlarged azygos and hemiazygos veins are seen (These two photographs were joined together for better understanding of the condition).
FIG. 4. Abdominal CT scan at the level of the liver showing vessels in front of the vertebral column represent- ing the aorta (middle) and the azygos and hemiazygos veins (on either side of the aorta) but no IVC.
Discussion
The development of the IVC inνolνes fusion, regression, and establishment of midline anastomoses between parts of three paired fetal venous systems: the two posterior cardinal νeins, the two subcardinal, and two supracardinal νeins.7,8 The changes in the abdominal venous systems that produce the final IVC coνer a long period from day 25 to day 50, mainly between days 29 and 41.5 Depending on the embryonic origin, four parts of the IVC haνe been recognized: (1) hepatic segment, (2) prerenal segment, (3) renal segment and, (4) postrenal
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

Liatas ‒ Total Inferior Vena Cava Agenesis
159
FIG. 5. Α. IVP showing multiple notches on the right ureter due το pressure from the retroperitoneal venous col- laterals. The stent in the left ureter is deviated laterally ow- ing apparently to the same etiology. Β. Excretory cystogram showing bilateral compression of the urinary bladder by the extensive venous collaterals in the pelvis. Many of them are seen laterally to the right aspect of the bladder.
segment.4,9-11 “Absent IVC” normally designates absence of the prerenal segment of the IVC
only, with azygos continuation3-6 being the most common variety of an interrupted IVC. 11 “Full
IVC agenesis" should cover those cases in which all four parts of the IVC and the iliac venous system are absent and blood return is accomplished by one or both of the following pathways: (1) vertebrolumbar pathway (anterior external vertebral plexus, ascending lumbar veins, and azygos and hemiazygos veins), and (2) superficial anterior abdominal wall collaterals. This definition is exemplified by the present case and other ones previously reported.3,6,12-15
The incidence of an absent IVC in the general population is very small, whereas this ranges from 0,6% to 1,3% among patients with malformations of the heart and increases to 20% in situs inversus and to 46% in the asplenia syndrome.4,5,16 These conditions have in common their dependence on a blood supply that is changing from being symmetrical to asymmetrical. Any uncertainty about whether the situs is to be normal or inverted may cause bilateral superior vena cavae or an absent IVC.5
Computed tomography is the investigation of first choice, before cavography, which dem- onstrates the associated venous anomalies (retro-aortic and para-aortic space-occupying struc- tures representing the enlarged collaterals draining the lower half of the body).7,17,21 Exact diagnosis and classification can be made also via intravenous and intraarterial DSA21 and magnetic resonance imaging.22 Most of the reported cases have been recognized as a result of angiocardiography when the advancing catheter via the femoral vein encountered difficulty.4,11
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

160 Vascular Surgery
March, 1993 Some cases have been diagnosed accidentally on a posteroanterior chest film by an opacity. in the right tracheobronchial angle corresponding to the very dilated azygos vein.7,17,23,25
In making the differential diagnosis the following conditions should be taken into account: 1. Pathological mediastinal lesions and other vascular anomalies, when the IVC agenesis
presents as a mediastinal abnormality on the chest radiograph, to avoid mediastinos- copy or thoracotomy 6,7
2. Causes of dilatation of the azygos-hemiazygos venous systeml3 3. The syndrome of obstruction of IVC in childhood3 4. Abdominal wall venous collaterals and varicose veins because excision of these veins
would interrupt a vital venous return or at least result in intractable ulcers6 5. Retroperitoneal and para-aortic space-occupying structures13,19 6. Causes of difficulty or prevention of catheterization of the heart from the IVC4,11 7. Other causes of acute abdominal symptoms (although it should be last in the list) 8. Causes of ureteric obstruction 9. Causes of retroperitoneal hemorrhage
10. Causes of lower back pain 11. Causes of Klippel-Trenaunay syndrome26 There are at present no known therapeutic measures for this very rare anomaly.19 Ιn pure
IVC agenesis disclosed accidentally (eg, by chest x-ray),7,18,23-25 those cases revealed during investigation of patients with congenital heart abnormalities,4,11,27 and those in symptomatic patients,6,19 the management should be focused on the prevention of complications, such as thromboses in the distal drainage channels. 19
Οn the other hand, knowledge of this condition is important for surgeons to avoid ligation of the azygos vein in the course of pulmonary or cardiac operation because prevention of the only major route of venous drainage from below the diaphragm may result in death.4,7,28 In complicated cases, eg, hypertension due to a hypoplastic kidney, or ureteric obstruction from constricting venous collaterals as in the present case, surgery is unavoidable. When thrombo- sis occurs,28,29,31 a life-threatening condition for this type of patient, vigorous anticoagulant treatment has to be instituted promptly that will last until sufficient venous return has been reestablished.
We believe that prolonged anticoagulant therapy has no benefits; on the contrary it in- creases the risk of retroperitoneal hemorrhage. When thrombosis and retroperitoneal hemor- rhage occur simultaneously, as in the present case, anticoagulant therapy should not be a contraindication, because hemorrhage is the end result when blood cannot escape forward. Note here a discrepancy between the extent of venous collaterals found on operation and seen by CT scan and those shown by phlebography. It is evident that a large part of the retroperito- neal venous collaterals is not operational. Obviously this is due to previous subclinical throm- boses and subsequent development of new collaterals, which is in accord with the patient’s history of having at times "large legs" since childhood. The clinical course of this case has proved that dilated superficial abdominal wall veins do not appear until a critical number of obstructed deep venous collaterals has been exceeded.
The prognosis of this rare congenital anomaly seems to be directly related to the presence of thrombosis in the retroperitoneal venous collaterals and to any coexistent congenital anoma-
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

Liαtαs ‒ Totαl Inferior Venα Cαvα Agenesis
161 lies (cardiac and vascular defects, situs inversus). In “full IVC agenesis” thrombosis is the major cause of mortality 9,11 and morbidity 6,12,19,29-31 (paresthesias of lower legs and lower back pain on exertion, retroperitonea1 hemorrhage, hypertension, ureteric obstruction, and emo- tional distress due to dilated superficial abdominal wall veins). Apart from this anomaly per se,31 implicating factors favoring thrombosis in this category of patients have been reported such as (1) oral contraceptives and cigarette smoking30; (2) increased intraabdominal pressure (constipation, tumors, pregnancy), and (3) dehydration, marasmus, sepsis, and exertion.9 Therefore, prevention of thrombosis must be our mainstay in helping these patients.
Anastasios C. Liαtαs, Μ. D. 71 Mikrαs Asias Str. 115 27 Athens, Greece
References 1. Buurman R, Buecheler Ε: Die Missbildungen der un-
teren Hohl vene. Fortschr Rontgenstr (ROFO) 125:337-345, 1976.
2. Seib GA: The azygos system of veins in American Whites and American Negroes, including observations on the inferior cava1 venous system. Am J Phys An- thropol 19:39-169, 1934.
3. Alexander ES, Clark RA, Gross ΒΗ, et a1: CT of con-genita1 anomalies of the inferior vena cava. Comput Radiol 6:219-226, 1982.
4. Anderson RC, Adams Ρ Jr, Burke Β: Anomalous infe-rior vena cava with azygos continuation (infrahepatic interruption of the inferior vena cava). J Pediatr 59:370-383, 1961.
5. Campbell Μ, Deuchar DC: Absent inferior vena cava, symmetrical liver, splenic agenesis, and situs inversus, and their embryology. Br Heart J 29:268-275, 1967.
6. Κnudtzon Ι, Gudmundsen ΤΕ, Svane S: Congenita1 ab- sence of the inferior vena cava. Acta Chir Scand 152:541-546, 1986.
7. Beedie RJ, Yeo W, Morcos SK: Congenita1 absence of the intrahepatic segment of the inferior vena cava with azygos continuation presenting as a mediastina1 mass. Postgrad Med J 65:253-255, 1989.
8. Goss CM: The Veins. Ιn: Gray's Anatomy, ed. 29, ed. by Goss CM. Philadelphia: Lea & Febiger, 1973, pp 673-729.
9. Angelman Η, Hall EG, Spencer R: The syndrome of obstruction of inferior vena cava in childhood. Br Med J 3:752-755, 1950.
10. Schmidt GP, Lob Μ: “Fehlen” einer unteren hohlvene bei gleichzeitigem fehlen der linken niere bei einem menschlichen foeten. Anat Anz 137:408-416, 1975.
11. Van Der Horst RL, Hastreiter AR: Congenital inter- ruption of the inferior vena cava. Chest 80:638-640, 1981.
12. Brem AS, O'Shea ΡΑ, Wesselhoeft CA: Absence of the inferior vena cava associated with an atrophic right kidney and hypertension. J Urol 126: 539-541, 1981.
13. Milner LB, Marchan R: Complete absence of the infe- rion vena cava presenting as a paraspinous mass. Tho- rax 35: 798-800, 1980.
14. Mosli ΗΑ, Papoff WJ, Moors DE: Unusua1 clinica1 presentation of a patient with absent inferior vena cava. J Urol 134:969-971, 1985.
15. Swaimann ΚF, Αustrian S, Raiale RB: Congenita1 atre- sia of the inferior vena cava, common iliac veins, and left innominate vein. Am J Dis Child 96:81-86, 1958.
16. Huelheims GH, Mudd JG: Anomalous inferior vena cava. Am J Cardiol 9:945, 1962.
17. Dwight Τ: Absence of the inferior vena cava below the diaphragm. J Anat Physiol 35:7, 1901.
18. Alex JF, Girodet Β, Straaten LV, et al: La continuation azygos la veine cave inferieure agenesique. Rev Fr Ma1 Resp 10:277-284, 1982.
19. Boecken G: Temporaere, belastungsabhangige paraes- thesien bei agenesie der vena cava inferior. Dtsch Med Wochenschr 113: 1879-1881, 1988.
20. Jaschke W, Kempmann G, van Kaick G: Computer to- mographischer nachweis der sogenannten azygos kon- tinuation bei fehlendem hepatischen segment der unte-ren hohlvene. 3 beobachtungen. Fortschr Rönt-genstr (RÖFO) 135:316-320, 1981.
21. Kullnig Ρ, Lammer J, Ranner G, et a1: Agenesie der vena cava inferior. Roentgenblatter 39:350-353, 1986.
22. Rettori R, Laπoque Ρ, Benzimra JC: Identification clinique et paraclinique par les differentes techniques d’imagerie des anomalies congenitales de la veine cave inferieure (a propos de 4 cas). J Ma1 Vasc 14: 191-201, 1989.
23. Dowing DF: Absence of the inferior vena cava. Pe- diatr 12:675-680, 1953.
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"

162
Vascular Surgery
March, 1993 24. Heeler RM, Dorst JP, James ΑΕ Jr, et al: Α useful sign
in the recognition of azygos continuation of the inferior vena cava. Radiol 101:519-522, 1971.
25. Stauffer ΗΜ, Labree Ι, Adams Ρ: The normally situ- ated arch of the azygos vein: Its roentgenologic identi- f i ca t ion and ca the te r iza t ion . Am J Roentgenol 66:353-358, 1951.
26. Servelle Μ, Babillot J: Les ma1formations des veines profondes dans le syndrome de klippel et Trenaunay. Phlebologie 33:31-36, 1980.
27. Hawass ND, Kolawole ΤΜ, Badawi MG: Concomi- tant pulmonary arteriovenous and inferior vena cava ma1formations. Α case report. Eur J Radiol 8: 102-105, 1988.
28. Effler DB, Greer ΑΕ, Sistres EC: Anoma1y of the vena cava inferior. Report of a fata1ity after ligation. JAMA 146:1321-1322,1951.
29. Barack BM: Persistence of the cardinal veins and thrombosis: CT demonstration. J Comp Assoc Tomo- graph 10:327-328, 1986.
30. Leu JA, Leu JH, Pouliadis G: Bein-beckenvenen- thrombose bei agenesie der vena cava inferior. Phlebo- logie und Proktologie 14:119-120, 1985.
31. Manouvrier Ι, Ducloux G, Millaire Α, et a1: L’angene- sie congenitale de la veine cava inferieure. Α propos d’un cas revele par une phlebite ilio-femorale. Apport de l’echographie et de la tomodinsitometrie. J Ma1 Vasc 10:235-239, 1985.
Αναστάσιος Λιάτας MD. F.I.C.A. Διευθυντής Χειρουργός ΕΣΥ Γ.Ν.Α "ΕΥΑΓΓΕΛΙΣΜΟΣ"
A C Liatas MD F.I.C.A. - Consultant Surgeon Athens General Hospital "EVAGELISMOS"





![INDEX [librairie.vetbooks.fr]...INDEX Note: page numbers in italics refer to fi gures, those in bold refer to tables.AB blood group typing 715–17, 1102, 1103 abdominal artery aneurysms](https://static.fdocument.org/doc/165x107/5e6849c121f76b3fda6af5c7/index-index-note-page-numbers-in-italics-refer-to-i-gures-those-in-bold.jpg)