Five year outcome of lentiviral gene therapy for human beta-thalassemia, lessons and prospects
28
Five year outcome of lentiviral gene therapy for human beta- thalassemia, lessons and prospects Cyprus TIF 2012 - P. Leboulch
description
Five year outcome of lentiviral gene therapy for human beta-thalassemia, lessons and prospects. Cyprus TIF 2012 - P. Leboulch. - PowerPoint PPT Presentation
Transcript of Five year outcome of lentiviral gene therapy for human beta-thalassemia, lessons and prospects

Five year outcome of lentiviral gene
therapy for human beta-thalassemia,
lessons and prospects
Cyprus TIF 2012 - P. Leboulch

The only curative treatment for the β-thalassemia currently is allogeneic hematopoietic transplantation, although fewer than 25% patients have an HLA-matched related donor, and those who do still face the risks of engraftment failure and Graft-Versus-Host Disease (GVHD)
Ex vivo gene therapy by transfer of a therapeutic β-globin gene into the patient’s own hematopoietic stem cells (HSCs) would alleviate both donor shortage and GVHD.
It is however especially challenging and a paradigm of gene therapy with no intrinsic in vivo advantage for corrected HSCs.


HS2 HS3 HS4
human -globin gene
3’ enhancer
III p
ppt
RRE
cPPT/FLAP 644bp 845bp 1153bp
III
266bp
2 x cHS4Insulator cores
2 x cHS4Insulator cores
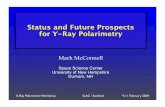
Lentiviral vector design with marked β-globin gene
SIN + Insulator(Δ 1 core in ≈ 50%)
SIN + Insulator(Δ 1 core in ≈ 50%) A-T87Q
Why A-T87 marking / mutation?•Provides anti-sickling properties (Leboulch and coll. Science 2001)•In-vivo biomarker for detection therapeutic globin by HPLC

Overview of the clinical protocol
Testingand Release
While Frozen
Maximize% Transduced
HSCs
Vector+
Cytokines
Bone Marrowor PB Harvest
MaximizeMyeloablation
WithoutImmunosuppression
Bone MarrowConditioning
Busulfex
IV InfusionTransduced Cells
(≈ 4x106 CD34+/Kg)(Spontaneous Homing)
CD34+ cells
(2x108 unsorted BM cells/Kgkept for rescue)

Phase I/II clinical trial: Initial focus on severe E/0-thalassemia
In Thailand alone, ~ 3,000 new cases born each year.~ 4% of the 350 million Southern China population carry a E- or a 0- allele.High prevalence among US immigrants.
High worldwide prevalence
Transfusion dependency, iron chelation therapy and often splenectomy.Candidates for allogenic transplant when HLA-matched sibling donor.
Mean spontaneous Hb levels separated by > 2 g/dl.
Severe in ~ 50% cases (similar to 0 Thalassemia major)
Narrow differential Hb levels between severe and well tolerated cases

Transplantation 5 years ago at age 19 on June 7, 2007
Transfusion dependent since age 3 (> 225 ml RBCs /kg/year for Hb > 10 g/dl).
Spontaneous Hb levels as low as 4.5 g/dl.
Major hepato-splenomegaly (splenectomy at age 6) and growth retardation.
Failure of Hydroxyurea therapy (between ages 5 and 17).
Desferoxamine (5 days/week) since age 8, and oral Exjade since age 18 (although nausea). No liver fibrosis. Moderate iron overload by liver MRI (561 mol/g).
Only child. No related, genoidentical HLA-matched donor. Match strict inclusion and exclusion criteria.
18 year old male with severe E/0-thalassemia (major) and no HPFH or α mutation.
Pre-transplant clinical history of the first gene therapy patient without injection of backup cells

CD15 (neutrophils)CD19 (lymphocytes B)CD45-CD71+ (erythroblasts)CD3+ (lymphocytes T)
Whole blood
CD14 (monocytes)
0.000.020.040.060.080.100.120.140.160.180.20
0 10 20 30 40 50 60Months post-transplantation
Vect
or c
opy
/ cel
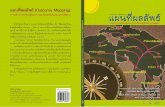
lVector copy numbers per circulating cell subsets
(up to 5 years post-transplantation)

LentiglobinTreatment
Published Sept 2010
Transfused Blood
Conversion to transfusion independence for 4.4 years(5.4 years post-transplantation)
Transplantation on June 7, 2007Last RBC transfusion on June 6, 2008

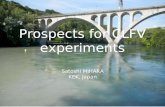
Conversion to transfusion independence (II)
0 10 20 30 40 50 600
2
4
6
8
10
12
HbA
HbAT87Q
HbFHbE
Hem
oglo
bin
(g/d
L)
Months post-transplantation
Last transfusion > 4.4 years ago
≈ 3.5 g/dL vector-encoded AT87Q-globin
Hb totale
Phlebotomies (200 ml each)

Partial correction of dyseythropoiesisand red blood cell maturation/lifespan
Red
blo
od c
ells
(x10
6 /µL)
Ret
icul
ocyt
es(x
105 /µ
L)
Blo
od e
ryth
robl
asts
(x
103 /µ
L)
Months post-transplantation Months post-transplantation
5101520253035
1,01,52,02,53,03,54,0
1,01,52,02,53,03,54,0
10 20 30 40 50 6010 20 30 40 50 60

1000
1500
2000
2500
3000
3500
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Ferr
itin
(µg/
L)Phlebotomies
Months post-transplantation
Partial decrease in plasma ferritin levels

Sustained amelioration of the thalassemic phenotype
Complete MCH correction (28.4 pg)(Average MCH for βE/β0-Thal patients = 19 pg)
Calculated expression βAT87Q > 70% endogenous βA-globin on a per gene basis
Calculated increased RBC lifespan > 8.5-fold
Decreased circulating erythroblasts > 3-fold (> 9-fold for vector+ cells)
Significant decrease (> 2-fold) in plasma ferritin levels
Excellent clinical status (full time job)

Integration site (IS) analysis by LM-PCR and DNA pyrosequencing(whole nucleated blood cells and purified sub-populations)
Low total number of different IS (< 300)In actively transcribed regions, similar to generic HIV vector
24 IS both myeloid and lymphoid
Months post-transplantation (whole nucleated blood cells)
020406080
100%
3 5 9 13 16 18 19 20 24
HMGA2FBXL11TBC1D5PILRBMKLN1IRAK1ZZEF1RFX3NUP98ATXN10EPB41L2EIF1PHF16SAE1GNA12POLA2
Relative dominance of IS at the HMGA2 locus(dominance relative to other IS, but > 80 % cells remain untransduced)
HMGA2

Aberrant splicing of the third intron and polyadenylation within the globin lentiviral vector
ATG51516 51517
TAGGlobin-LV
E1 E2 E3 E4 E5
Let-7 miRNAs
Intron 3 (~ 113 kb)Deletion of 1 copy insulator core
Sequencing of the main HMGA2 transcript:Aberrant splicing within the vector insulator + polyadenylationERYTHROID-SPECIFIC EXPRESSION +++++

Cell type distribution of HMGA2 IS (3 months post-transplant)
CFU-GM colonies ~ 7 % positive(~ 67% of vector+)
BFU-E colonies ~ 15 % positive(~ 78% of vector+)
Lymphocytes (thorough search) ~ undetectable(fresh sorted CD3 / CD19 or
lectin expanded)
LTC-IC (7 weeks) ~ 6 % positive(~ 50% of vector+)

First evidence in humans for long-term hematopoietic lineage bias (myleoid vs. lymphoid vs. totipotent)
Further evidence is accumulating in mice …• By limited dilution transplant analyses from C. Eaves lab (e.g., Cell Stem Cell 2012;10:273-83).
• By barcoded transplant analysis from P. Leboulch lab (submitted).
• CD86- marks myeloid restriction from W. Kincade lab (Blood 2012;119:4889-97).

Hematopoietic homeostasis is maintained
Normal blood and bone marrow cytology – Normal cytoflurometry analysis
Normal karyotype and high resolution CGH-array chromosomal analysis –No Trisomy 8 with specific probe
Lack of cytokine-independence in CFU-C assays
Normal LTC-IC countsNo preferred engraftment in NSG mice (coll. C. Eaves)
Asymptotic stabilization of the clone relative dominance
No abnormality detected for MPL. JAK2 and TET2
Natural cases of PNH with HMGA2 dysregulation followed for > 19 years

- Lack of detection in mouse studies- Evidence for initial integration bias ?- Evidence for homeostatic in vivo selection ?- General principle seen with other key genes
HMGA2 IS is frequently retrieved by DNA pyrosequencing in vivo after retroviral and lentiviral human CD34+ gene transfer
HMGA2 in X-SCID trial (γ-RV vector)
> 15 cluster IS in HMGA2 (aggregates of patients data):- several in HMGA2 Intron 3- several with tendency to increase with time and then stabilize- 2 with truncated RNA by aberrant splicing Intron 3 into vector
HMGA2 in ALD trial (LV vector)
1 IS in HMGA2 Intron 3 in patient P1:- only in B lymphocytes and 1 time-point
Wiskot Aldrich trial (γ-RV vector)
MGMT glioblastoma trial (γ-RV vector)

The percentage of partially dominant HMGA2 site is decreasing over time in whole nucleated blood cells (qPCR – 5 years post-transplant) …

Integration site (IS) analysis by LM-PCR and DNA pyrosequencing4 and 5 years post-transplantation
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PMS2P1RFX3
ZZEF1HMGA2
SPATS2POLA2
WBC WBC CD45 CD3 CD19 CD15 CD14 Erythro
4 years 5 years post-transplantationIn
sers
ion
site
s (%
of e
ach)
Already the most common after 3 years
38 27 20 10 22 19 23 9Number unique IS

qPCR based kinetics of the four most common ISup to 5 years post-transplantation
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0 10 20 30 40 50 60
Months post-transplantation
Vect
or c
opy
num
ber copies
HMGA2
RFX3
FBXL11
ZZEF1
4 years
ZZEF1 = 1/3 HMGA2
5 years
ZZEF1 = HMGA2

Second E/0-thalassemia (major) gene therapy patient transplanted on November 24, 2011
• 23 year old woman, βE/β0 Thal Major‑
• Transfusion dependent since her 2nd month of life. No HLA matched sibling donor
• The transplantation was uneventful. Engrafted neutrophils by day 20 and had delayed platelet reconstitution (no related complications)
• The patient has returned to full time work
• Peripheral vector copy numbers and therapeutic βAT87Q globin protein in reticulocytes‑ approximately 3-fold greater than in the previous patient at same time-points
• Red blood cell transfusions are now being tapered down to stimulate erythropoiesis and increase βAT87Q globin production‑

PATIENT 1 (specific chain / non- chain)
0
5
10
15
20
0 2 4 6 8
Months post transplant
glob
ins
[%]
87
E
PATIENT 1
0.00.20.40.60.81.01.21.41.6
0 2 4 6 8
Months post transplant
hem
oglo
bins
[g/
dL]
87
E
E
Parallel evolution of therapeutic Hb in the second β-thalassemia patient after lentiviral gene therapy
0
5
10
15
20
0 2 4 6 8
Months post transplant
glob
ins
[%]
87
E
0.00.20.40.60.81.01.21.41.6
0 2 4 6 8
Months post transplant
hem
oglo
bins
[g/d
L]87
E
E
PATIENT 2PATIENT 2 (specific chain / non- chain)

Comparative globin chain analysis by reverse phase HPLC Patient 1 (transfusion independent since 4.5 years ago) and Patient 2

Integration site (IS) analysis by LM-PCR and DNA pyrosequencingin Patient 2 “MHV” 6 months post-transplantation
CD34
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
lowJAK3*WDHD1ACSL4SPOCK3C19ORF47C4ORF45FBXL11(1)MPRIPTNKS2PFASCARM1CEP290DHX8BST2CIP29*C12ORF64
WBC
lowSIRT3RAB5C*EIF4G3GATAD2BSETD2*CHD6,CHD5*AK090973SAFBNCK1*TNFSF12FLJ45340
VWFHORMAD2NBR1*ARID1A*BC031827PLEKHA3
CD45
lowIQGAP1C6ORF106TXNRD3TAFII105DKFZP686B0790C11ORF49B7ARIH1CEP110*FCHSD2TK1*SAPS3CLN3MAGGUSBL2DHDDSTCF12*
CD3
LHX3GUSBL2IMAA
CD19
lowNIP30NAV3SPOPTBLR1RBM5*RPS6KA1*DNAL1C17ORF26MAP1SMALAT1KIAA0827SUV420H1RAB14FBXL11(2)KIF1BFBXL11(3)
DKFZP434N1217
VAPAGTF2IRD2
CD15
lowNR_002821BTBD11IL6ST*GTF3C2SLC19A2
CD14
lowUNQ747MAP3K3VDPC9ORF86PLEKHA3MIER2CUTL1RHOA*NUP88UBA2,SAE2TXNDC11ATP6V1A
DKFZP434 C2019
Erythro
lowCSNK1G1MEX3CSPATS2PMS2P1HMGA2*PB1CRAMP1LPTRFNHN1ZNF280BSF3A3ZNF318*VPS16JUP
Inse
rtion
site
s (%
of
each
)
218 unique sites

Modified vector BB305 (G. Veres & M. Finer – bluebird bio) for continuation French trial and for US trial
VCN ~ 3• Removal insulator and TAT independent
together with novel purification system
• Higher GMP production titers and >2-3-fold better human CD34+ transduction efficiency
• Greater vector copy number (VCN) per cell(important for β0-thal)
• High βAT87Q globin protein expression even in non-‑thalassemic erythroid cells (e.g., βS/ βS)
• Maintained low genotoxic potential in IVIM assays (coll. C. Baum)
• Vector substitution in French trial planned for next patients
• US trial with new vector filed with RAC (unanimous approval) and with FDA in December

Other University Hospitals of Paris (AP-HP): Saint-Louis, Mondor, CHIC, Tenon, Saint Vincent de PaulEliane Gluckman Françoise Bernaudin Gérard Socié
Hopital Necker (AP-HP), ParisMarina Cavazzana-Calvo (current PI clinical trial) Salima Hacein-Bey Abina
Olivier Hermine Felipe Suarez Antoine RibeilBluebird bio, Inc, Cambridge, MA and bluebird bio - FranceOlivier Negre Gabor Veres Maria DenaroBéatrix Gillet-Legrand Yves Beuzard Kathleen Kirby Robert Kutner Dave Davidson Mitchell Finer
Indiana Vector Production Facility, Indianapolis, INKen Cornetta Scott Cross Chris Ballas
Institute of Emerging Diseases and Innovative Therapies – INSERM U. 962 – University Paris 11Bluebird bio – France and Harvard Medical School, Brigham and Women’s Hospital, Boston, MAEmmanuel Payen Olivier Negre Leila Maouche-ChrétienAlisa Tubsuwan Soumeya Abed Robert PawliukKaren Westerman Resy Cavallesco Julian DownKathy Hehir Philippe Leboulch
University of Pennsylvania School of Medicine, Philadelphia, PAFrederick Bushman Gary Wang Troy Brady
Mahidol University and Ramathibodi Hospital, Bangkok, ThailandAlisa Tubsuwan Suradej Hongeng Suthat Fucharoen
German Cancer Research Center (DKFZ), Heidelberg, GermanyAnnette Deichmann Manfred Schmidt Kristof Von Kalle
Terry Fox Laboratory, University of British Columbia, Vancouver, CanadaMelanie Kardel Alice Cheung Connie Eaves