Expression of αvβ6 integrin and collagen fibre in oral squamous cell carcinoma: association with...
10
Expression of avb6 integrin and collagen fibre in oral squamous cell carcinoma: association with clinical outcomes and prognostic implications Hai-Xia Li 1 , Jin-Hua Zheng 1 , Hai-Xia Fan 1 , Hui-Ping Li 1 , Zhong-Xiuzi Gao 1 , Dong Chen 2 1 Department of Anatomy, Basic Medical Science College, Harbin Medical University, Harbin, China; 2 Harbin Medical University Stomatological Hospital, Harbin Medical University, Harbin, China BACKGROUND: This study aims to investigate the expression and significance of the avb6 integrin, collagen fibres and matrix metalloproteinases (MMP)-3 in oral squamous cell carcinoma (OSCC) and to analyse the possible regulatory relationships between avb6, collagen fibres and MMP-3. MATERIALS AND METHODS: A series of 80 patients (mean age 56.4 years) diagnosed with OSCC were enrolled. Associations between avb6, MMP-3, collagen fibre expression levels and clinicopathological parame- ters were evaluated using the Fisher exact test. Survival analysis was performed with Kaplan–Meier curves. Spear- man rank correlation was used to analyse interactions between avb6, MMP-3 and collagen fibres. RESULTS: avb6 and MMP-3 were strongly expressed in human OSCC, especially at the peripheral borders of invasive tumour islands, and collagen fibres were gener- ally disrupted and degraded in the same areas. The expression intensity of avb6 was associated with the differentiation state of cells. b6 mRNA was expressed in almost all cancer cells. In carcinomas, avb6 and MMP-3 expression were correlated with the distribution of collagen fibres. CONCLUSIONS: Tumour cells highly expressing avb6 have a strong capability for invasion and migration, due to concomitant protease production and the destruction and remodelling of collagen fibres. Increased avb6 inte- grin and MMP-3 expression and collagen fibre changes in human OSCCs are related to unfavourable clinical prog- nostic factors and decreased survival. J Oral Pathol Med (2013) Keywords: collagen fibre; MMP-3; oral squamous cell carcinoma; prognosis; avb6 integrin Introduction Oral squamous cell carcinoma (OSCC) is the most common head and neck cancer and the eighth most common cancer worldwide (1), accounting for over 300 000 new cancer cases worldwide every year (2). It is characterized by an aggressive growth pattern, a high degree of local invasive- ness and cervical lymph node metastasis (3). Although its pathogenesis and management has been extensively researched, the 5-years survival rate for OSCC patients has not improved in the last 25 years and remains at 50% (1). Currently, OSCC prognosis depends mainly on the site where the primary tumour arises, tumour size, neck node status and presence of distant metastases. However, the biological behaviour of OSCC is characterized by signif- icant heterogeneity, and tumours of the same clinical stage often differ in clinical course and treatment response. Thus, identification of key factors affecting invasion and metastasis, establishment of new diagnostic/prognostic models and adoption of new therapeutic strategies are of paramount importance. The interaction between cancerous epithelial cells and stromal cells destroys basement membranes, the first barriers to tissue invasion and then promotes tumour cell invasion and migration (4, 5). As another major component of extracellular matrix (ECM), collagen fibres play an important role in ECM destruction and remodelling. Changes in collagen morphology and content are regulated by matrix metalloproteinases (MMPs) – another key factor in epithelial tumour growth and invasion (6, 7). Integrins are a family of heterodimeric cell surface receptors that mediate cell adhesion. Integrins interact with ECM and transmit signals to the nucleus through a complex pathway that regulates cytokine expression, thus affecting cell movement, proliferation, differentiation, survival and tumour cell invasion and metastasis (8, 9). As an epithe- lium-restricted integrin, avb6 integrin is detected in wound healing, inflammation and diverse epithelial malignancies (9–11). Ramos et al. (12, 13) have shown that avb6 increases the invasive ability of OSCC in vitro and in vivo by upregulating MMP-3. In addition, avb6 regulates Correspondence: Jin-Hua Zheng, PhD, Department of Anatomy, Basic Medical Science College of Harbin Medical University, 194 Xuefu-Road, Harbin 150081, China. Tel: +86 451 86674508, Fax: +86 451 86674001, E-mail: [email protected] Accepted for publication December 6, 2012 doi: 10.1111/jop.12044 J Oral Pathol Med © 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd wileyonlinelibrary.com/journal/jop
Transcript of Expression of αvβ6 integrin and collagen fibre in oral squamous cell carcinoma: association with...

Expression of avb6 integrin and collagen fibre in oralsquamous cell carcinoma: association with clinicaloutcomes and prognostic implications
Hai-Xia Li1, Jin-Hua Zheng1, Hai-Xia Fan1, Hui-Ping Li1, Zhong-Xiuzi Gao1, Dong Chen2
1Department of Anatomy, Basic Medical Science College, Harbin Medical University, Harbin, China; 2Harbin Medical UniversityStomatological Hospital, Harbin Medical University, Harbin, China
BACKGROUND: This study aims to investigate the
expression and significance of the avb6 integrin, collagen
fibres and matrix metalloproteinases (MMP)-3 in oral
squamous cell carcinoma (OSCC) and to analyse the
possible regulatory relationships between avb6, collagenfibres and MMP-3.
MATERIALS AND METHODS: A series of 80 patients
(mean age 56.4 years) diagnosed with OSCC were
enrolled. Associations between avb6, MMP-3, collagen
fibre expression levels and clinicopathological parame-
ters were evaluated using the Fisher exact test. Survival
analysis was performed with Kaplan–Meier curves. Spear-
man rank correlation was used to analyse interactions
between avb6, MMP-3 and collagen fibres.
RESULTS: avb6 and MMP-3 were strongly expressed in
human OSCC, especially at the peripheral borders of
invasive tumour islands, and collagen fibres were gener-
ally disrupted and degraded in the same areas. The
expression intensity of avb6 was associated with the
differentiation state of cells. b6 mRNA was expressed in
almost all cancer cells. In carcinomas, avb6 and MMP-3
expression were correlated with the distribution of
collagen fibres.
CONCLUSIONS: Tumour cells highly expressing avb6have a strong capability for invasion and migration, due
to concomitant protease production and the destruction
and remodelling of collagen fibres. Increased avb6 inte-
grin and MMP-3 expression and collagen fibre changes in
human OSCCs are related to unfavourable clinical prog-
nostic factors and decreased survival.
J Oral Pathol Med (2013)
Keywords: collagen fibre; MMP-3; oral squamous cell carcinoma;
prognosis; avb6 integrin
Introduction
Oral squamous cell carcinoma (OSCC) is the most commonhead and neck cancer and the eighth most common cancerworldwide (1), accounting for over 300 000 new cancercases worldwide every year (2). It is characterized by anaggressive growth pattern, a high degree of local invasive-ness and cervical lymph node metastasis (3). Although itspathogenesis and management has been extensivelyresearched, the 5-years survival rate for OSCC patientshas not improved in the last 25 years and remains at 50%(1). Currently, OSCC prognosis depends mainly on the sitewhere the primary tumour arises, tumour size, neck nodestatus and presence of distant metastases. However, thebiological behaviour of OSCC is characterized by signif-icant heterogeneity, and tumours of the same clinicalstage often differ in clinical course and treatment response.Thus, identification of key factors affecting invasion andmetastasis, establishment of new diagnostic/prognosticmodels and adoption of new therapeutic strategies are ofparamount importance.The interaction between cancerous epithelial cells and
stromal cells destroys basement membranes, the firstbarriers to tissue invasion and then promotes tumour cellinvasion and migration (4, 5). As another major componentof extracellular matrix (ECM), collagen fibres play animportant role in ECM destruction and remodelling.Changes in collagen morphology and content are regulatedby matrix metalloproteinases (MMPs) – another key factorin epithelial tumour growth and invasion (6, 7).Integrins are a family of heterodimeric cell surface
receptors that mediate cell adhesion. Integrins interact withECM and transmit signals to the nucleus through a complexpathway that regulates cytokine expression, thus affectingcell movement, proliferation, differentiation, survival andtumour cell invasion and metastasis (8, 9). As an epithe-lium-restricted integrin, avb6 integrin is detected in woundhealing, inflammation and diverse epithelial malignancies(9–11). Ramos et al. (12, 13) have shown that avb6increases the invasive ability of OSCC in vitro and in vivoby upregulating MMP-3. In addition, avb6 regulates
Correspondence: Jin-Hua Zheng, PhD, Department of Anatomy, BasicMedical Science College of Harbin Medical University, 194 Xuefu-Road,Harbin 150081, China. Tel: +86 451 86674508, Fax: +86 451 86674001,E-mail: [email protected] for publication December 6, 2012
doi: 10.1111/jop.12044
J Oral Pathol Med
© 2013 John Wiley & Sons A/S. Published by Blackwell Publishing Ltd
wileyonlinelibrary.com/journal/jop

expression of MMP-1, MMP-2, MMP-9 and MMP-13 inOSCC cells (14, 15). The avb6 integrin may have multipleregulatory functions in oncogenesis (9). Studies have shownavb6 to be involved in fibrosis. Inhibition of integrin avb6prevents radiation-induced lung fibrosis (16), and oralsubmucous fibrosis has been recognized as a potentiallymalignant oral disorder (16, 17). Our previous studiesshowed that during 7,12-dimethylbenz(a)anthracene-induced carcinogenesis in the tongues of hamsters, themorphology and content of collagen fibres in the laminapropria underwent significant changes that were closelyassociated with MMP-1 expression (18).
Stromelysin-type MMP-3s have a broad range of sub-strates. They cannot directly degrade type I and II collagens,but they activate MMP-1 and other family members toparticipate in the degradation of collagen fibres (19).Because MMP-1 is the main protease involved in degrada-tion of type I, II and III collagens, the level of MMP-3 canindirectly reflect collagen degradation. MMP-3 can alsodegrade fibronectin, which is an important ligand of avb6integrin (9), and it is thus directly related to avb6 integrin.
Therefore, we speculated that there is a regulatoryrelationship between the expression of avb6, MMP-3 andcollagen fibres, and this relationship may be involved inchanging the microenvironment of OSCC and then promotetumour invasion. In this study, we collected clinical tissuesamples of oral cancer to investigate the expression of avb6,collagen fibres and MMP-3 in tumour microenvironments,and analyse the expression correlation between them, withthe aim of better understanding the biological significanceof avb6 and MMP-3 in the invasion process of OSCC.
Materials and methodsPatientsThis study is based on a retrospective cohort of 80 patientssuffering from primary OSCC who underwent resections ofprimary tumours and radical or selective ipsi- or bilateralneck dissections between January 2000 and December 2004at the Harbin Medical University Stomatological Hospital,Harbin, Heilongjiang, China. All patients gave informedconsent, and the study was approved by the Research EthicsCommittee of Harbin Medical University, Harbin. Histo-logical sections were stained with haematoxylin and eosinfor diagnostic purposes. The main clinical characteristics ofthe 80 patients selected for this study are detailed inTable 1. All patients were followed up for 5 years from thetime of surgery. The minimum patient follow-up time was5 months, median follow-up time was 60 months andmedian survival time was 58 months. All patients wereclassified into stages according to the 1997 UICC TNMClassification of Malignant Tumours (20).
Immunohistochemical stainingImmunochemistry for avb6 and MMP-3 was performedusing 8-lm, OCT-embedded serial sections of tumourblocks. Immunohistochemical staining was performed byusing the universal two-step method. Briefly, the sectionswere first fixed with acetone. Endogenous peroxidaseactivity was blocked by immersion of slides in 3% hydrogenperoxide. To block non-specific antigens, 1% bovine serum
albumin was applied for 15 min. The mixtures were thenincubated with a monoclonal antibody against avb6 integrin(E7P6; Millipore, Billerica, MA, USA) or MMP-3(BA1272; Wuhan Boster Bio-engineering Ltd Co., Wuhan,China) overnight in a humidified chamber maintained at4°C. Subsequently, they were incubated with the corre-sponding non-biotinylated secondary antibody (PV6002;Zhongshan Goldenbridge Biotechnology, Beijing, China)for 30 min at 37°C. The antibody reaction was visualized byusing diaminobenzidine (DAB) chromogen (ZhongshanGoldenbridge Biotechnology). Then, all the slides werecounterstained with haematoxylin. An isotype IgG1 andPBS were substituted for the primary antibody as a negativecontrol, and F6 cell lines (avb6) and human breast cancertissue (MMP-3) were used as positive controls.
Masson’s trichrome stainingFormalin-fixed, paraffin-embedded tissues were sectioned,deparaffinised and rehydrated. Masson’s trichrome staining(21) was used to observe deposited collagen fibres. Theextent of collagen fibres was assessed per area of staining.
Table 1 Clinical features in 80 patients with oral squamous cellcarcinoma
Characteristics Number of cases (%) (n = 80)
Age (years; mean: 56.4; range: 35–76)<55 37 (46)� 55 43 (54)
GenderMale 59 (74)Female 21 (26)Primary sitesTongue 48 (60)Lip 11 (14)Floor of mouth 21 (26)TT1 39 (49)T2 32 (40)T3 1 (1)T4 8 (10)NN0 23 (29)N1 35 (43)N2 22 (27)N2a 3 (4)N2b 4 (5)N2c 15 (18)Clinical stageI 20 (25)II 3 (4)III 30 (37)IV 27 (34)Tumour differentiationWell 48 (60)Moderate 28 (35)Poor 4 (5)Initial therapySurgery alone 29 (36)Surgery/chemotherapy combined 51 (64)RecurrenceNo 58 (73)Yes 22 (27)Clinical status at the end of follow–up periodLive 39 (49)Dead 36 (45)Lost 5 (6)
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
2

In situ hybridizationIn situ hybridization was performed according to themanufacturers’ protocols (MK3270-h; Wuhan Boster Bio-engineering Ltd Co.). For human integrin b6 target gene, thefollowing mRNA sequences were used: (i) 5′-TTCCAACACC AAAAG AAATG CTCTC ACATG AAAGT-3′;(ii) 5′-TATGG AAACA TTTAT GGGCC TTATT GCCAGTGTGA-3′; and (iii) 5′-AATGT AACTT ATAAA CACAGGGAAA AACAA AAGGT-3′. Frozen slides were fixed inbuffered 4% paraformaldehyde solution and washed; pepsindigestion was used to expose mRNA nucleic acid frag-ments. Each section was covered with 20 ll of hybridiza-tion buffer (containing integrin b6 oligonucleotide probes)at 42°C. Slides were washed for 30 min at room temper-ature (RT). Biotinylated mouse anti-digoxin was thenadded. After 2-h incubation at RT, slides were washedand one droplet of streptavidin-biotin complex-peroxidaserat IgM was added to each slide and incubated for 30 min at37°C. Slides were then incubated in DAB. For controlstains, DIG-conjugated sense oligos were used instead ofhybridization buffer.
Immunofluorescence stainingImmunofluorescence staining for avb6 and MMP-3 wasperformed using OCT-embedded serial sections of tumourblocks according to the manufacturers’ protocols. Sectionswere incubated with a monoclonal antibody mouse againstavb6 integrin (Millipore) or rabbit against MMP-3 (WuhanBoster Bio-engineering Ltd Co.) in an azide-free mediumovernight at 4°C. They were then incubated with fluor-conjugated donkey anti-rabbit IgG and fluor-conjugateddonkey anti-mouse IgG (Invitrogen, Carlsbad, CA, USA)for 1 h. Fluorescence was observed under a fluorescencemicroscope (Olympus BX51, Tokyo, Japan) equipped withFlash Point software (Olympus).
Computer-aided morphological analysisImage Pro Plus 6.0 (Media Cybernetics Inc., Rockville,MD, USA) was used to calculate the intensity and extent ofdetected molecules and the ratio of Masson’s trichromestaining area to the total area of the image in tumour tissueand normal mucosa. Five microscopic fields in OSCCtissues (original magnification 9200) were randomlyselected and their images were cropped. The integral opticaldensity in stained cells and the Masson’s trichrome stainingper unit area in tumour tissue were then calculated by imageanalysis. Results were expressed as mean � SD per tissueexamined (Data S1).
Statistical analysisSPSS 15.0 (IBM Corporation, Armonk, NY, USA) wasused for statistical analysis. Differences between meanvalues of two sets were assessed using the SNK-q test.Associations among avb6 protein, MMP-3 protein and b6mRNA expression, collagen fibre staining area and clinico-pathological parameters were evaluated using the Fisherexact test. Survival analysis was performed with the Kaplan–Meier curve and log-rank test, while univariate andmultivariate analysis of overall survival (OS) was performedaccording to Cox proportional hazards models. Spearmanrank correlation was used to analyse interactions among
avb6 protein, MMP-3 protein and collagen fibre stainingarea. All tests were two-sided; significance was set atP = 0.05.
ResultsPatient prognosisOf the 80 OSCC patients included in the study, 41 (51%)patients were alive and well at the end of the follow-upperiod, 36 (45%) had died of disease and three (4%) werealive with disease. OS probability for the whole group was52.85%. We analysed the effect of clinicopathologicalparameters on patients’ prognoses and found that onlylymph node metastasis was statistically significant (Table 2).
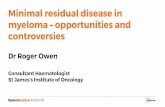
Expression of avb6 in human tissue specimensNormal epithelium generally displayed negative or weakstaining for avb6 in the basal cell layer (Fig. 1A);expression in the cytoplasm was associated with membranesof dysplastic epithelium basal cell layers (Fig. 1B). A widerange of staining patterns was observed in the 80 OSCCsamples. Cells at the peripheral borders of tumours demon-strated stronger avb6 immunoreactivity compared with cellsat the centre of tumour nests and cords (Fig. 1C). Further-more, small nests or individually infiltrating tumour cellsbordering the stroma demonstrated stronger avb6 immuno-reactivity compared with large, massive nests and cords oftumour cells (Fig. 1D).We assessed staining intensity and the proportion of cells
expressing avb6 using computer-aided morphological anal-ysis (Table 2). Table 3 summarizes the relationshipbetween integrin avb6 expression and clinicopathologicalfeatures of the 80 OSCC cancer patients. avb6 expression intumours did not significantly vary with sex, age, tumour size(T) or tumour recurrence (P > 0.05), but avb6 expressionwas significantly correlated with tumour location, differen-tiation and nodal status (P < 0.001). The survival time ofpatients with strong avb6 expression was significantlyshorter than that of patients with weak avb6 expression(Fig. 2A). Multivariate analysis using the Cox regressionmodel indicated that amb6 may reflect poor prognosis inpatients with OSCC (P = 0.085, RR = 3.68; Table 4).
Assessment of b6 mRNA expressionb6mRNA was detectable in all OSCC samples, and stronglyexpressed in 69 (86%) cases. Strong expression of b6mRNAwas observed in the neoplastic epithelial islands and diffuselyin tumour cells in adjoining connective tissue (Fig. 1E). Cellsat the periphery of small tumour islands and tumourconnective tissue demonstrated stronger b6 mRNA expres-sion. Expression of b6mRNAwas not detected in normal oralmucosa (Fig. 1F), but was detectable in the basal cell layers ofdysplastic epithelium (Fig. 1G). Non-cancerous cells scat-tered in the lamina propria and tumour connective tissuedisplayed positive staining for b6 mRNA (Fig. 1H).
Assessment of collagen matrix using Masson’s trichromestainingIn the lamina propria of normal tissue, collagen fibres wereinterwoven into a network; extensive fibre cross-linking wasclearly evidenced by thinning bundles, wavy appearance
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
3

and loose arrangement. Thinning collagen fibre bundlessurrounded vessels like a ring (Fig. 3A).
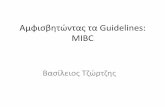
With different degrees of pathological differentiation, themorphology and distribution of collagen fibres demon-strated significant change. Many vessels demonstratedblockage (Fig. 3B). Collagen fibres in well-differentiatedtumour stroma appeared as dense bundles and werearranged in a disorderly manner, with some areas of theconnective tissue appearing like thick, long ribbons andshowing masses of collagen deposition (Fig. 3C). Collagenfibre structures surrounded cancer nests with stratumcircularity and were arranged in an orderly manner,encasing cancer nests, layer upon layer, and forming
membrane-like structures, but their collagen fibre contentwas less than that seen in the lamina propria. However,intense collagen staining was also observed around cancernests in individual sections. Compared with vessels in thelamina propria, collagen fibres around vessels of tumourislands were clearly decreased.Collagen fibre content was significantly decreased in
moderately differentiated OSCC tissues. Irregular laminae ofcollagen fibres surrounded the nests, and the margin betweenthe collagen fibres in and around the cancer nests was unclear.At the peripheral borders of invasive tumour islands, collagenfibres became thinner, disrupted and lighter stained (Fig. 3D)– even degraded in some specimens. Interestingly, collagenfibres surrounding vessels were obviously decreased, and thenumber of open vessels was increased (Fig. 3E). Muscleatrophy had increased in most cases.Poorly differentiated OSCC demonstrated very low
collagen fibre content; in tumours, the fibres became thinand short, with reduced cross-linking and an irregular wavyappearance (Fig. 3F). However, the membrane-like struc-ture fractured, collapsed or even completely disappeared inmost cases. No obvious fibres were found around vessels.The number of vessels in the lamina propria increased,while the collagen fibres surrounding the vessels weredisrupted and arranged in a disorderly manner. Because ofthe invasion of extended collagen fibres and cancer tissue,muscle atrophy was observed to a greater extent in thesubmucosal area.We assessed the extent of collagen fibres per unit area in
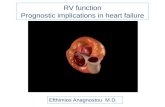
different tissues using computer-aided morphological anal-ysis (Fig. 3G,H). Table 3 summarizes the relationshipbetween collagen fibre expression and clinicopathologicalfeatures of the 80 OSCC cancer patients. Collagen contentwas negatively correlated with patient survival; the 5-yearOS of patients with large, moderate or small amounts ofcollagen fibre was 80%, 46.09% and 34.72%, respectively,showing a statistically significant trend (P < 0.01; Table 2),and the OS time of patients with high collagen fibreexpression was significantly longer than that of patients withlow collagen fibre expression (Fig. 2B).
MMP-3Protein expression of MMP-3 was observed in the cyto-plasm of tumour cells and detected in 44 (55%) of 80 cancertissues. MMP-3 expression was mainly observed in diffusetumour cells in adjoining tumour stroma and small tumourislands; immunostaining, in brown granules, was observedin cytoplasm (Fig. 4A). Normal epithelium generallydisplayed negative or weak staining for MMP-3 (Fig. 4B).In dysplastic epithelium, a few stromal fibroblasts alsodemonstrated MMP-3 expression (Fig. 4C).We analysed the relationship between MMP-3 expression
and clinicopathological features (Table 3) and found thatMMP-3 expression was significantly correlated with nodalstatus and tumour recurrence, but not tumour size(P = 0.1749). Expression of MMP-3 was significantlyrelated to patients’ 5-year survival (P < 0.01; Table 2).The survival time of patients with positive MMP-3 expres-sion was significantly shorter than that of patients withnegative MMP-3 expression (Fig. 2C). MMP-3 was inde-pendently associated with poor-prognosis OSCC patients
Table 2 Association of avb6 protein, b6 mRNA, MMP-3 protein,collagen fibre expression and clinicopathological parameters with overall5-year survival
Variable Number(a) Survival number
Overall 5-yearsurvival
% P
avb6 proteinWeak 18 (2) 14 88.15 0.0026Strong 62 (3) 25 42.82b6 mRNAWeak 11 7 63.64 0.5263Strong 69 (5) 32 50.99MMP-3 proteinNegative 36 (3) 26 79.59 <0.0001Positive 44 (2) 13 31.45Collagen fibreSmall 16 (1) 5 34.72 0.0097Moderate 44 (4) 18 46.09Large 20 16 80.00Age<55 37 (2) 16 54.38 0.5091� 55 43 (3) 23 51.77
GenderMale 59 (3) 28 50.61 0.5995Female 21 (2) 11 59.58Primary sitesTongue 48 (2) 26 62.34 0.4098Lip 11 (1) 6 54.86Floor of the mouth 21 (2) 7 43.08TT1/T2 71 (5) 35 53.85 0.2791T3/T4 9 4 44.44Lymph nodePositive 57 (3) 22 81.14 0.0016Negative 23 (2) 17 41.48Tumour differentiationWell 48 (3) 24 57.03 0.8973Moderate 28 (2) 13 46.38Poor 4 2 50.00Initial therapySurgery alone 29 (4) 14 64.72 0.0478Combinedb 51 (1) 25 46.25RecurrenceNo 22 (1) 7 60.05 0.0216Yes 58 (4) 32 33.94
Five-year overall survival analysis of avb6 protein, b6 mRNA, matrixmetalloproteinase (MMP)-3 protein, collagen fibre and well-known prog-nostic parameters calculated by Kaplan–Meier method and log-rank test.Statistically significant associations are italicized; P values were calculatedusing 5-year survival time.aMissing cases.bSurgery and chemotherapy combined.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
4

A B C
D E F
G H I J
Figure 1 The expression of avb6 (A–D) and b6 mRNA (E–H) in oral squamous cell carcinoma. (A) Normal avb6-basal cells. (B) avb6 protein in thecytoplasm associated with basal cell layers of dysplastic epithelium, arrowhead: positive cells. (C) avb6 protein expression at the periphery of cancer nests isstronger than in the nest centres. (D) Small tumour cell nests or individually infiltrating tumour cells show more intense staining than large tumour nests. (E)b6 mRNA expression in tumour cells. (F) Normal b6-mRNA basal cells. (G) b6 mRNA expression in basal cell layers of dysplastic epithelium. (H) b6mRNA expression in non-tumour cells scattered in the lamina propria and connective tissue. (I) Isotype mouse IgG1 (ab81216, Abcam) instead of primaryantibody as control in immunohistochemical; (J) DIG-conjugated sense oligos instead of DIG-conjugated nonsense oligos as a negative control in In situhybridization. Ep, epithelium; Ca, tumour; S, stroma; Lp, lamina propria. Magnification shown in figures.
Table 3 Relationships of avb6 protein, b6 mRNA, MMP-3 protein, collagen fibre expression with patient and tumour characteristics
Factor Patientsa
avb6 intensity(n)
P
b6mRNAexpression (n)
P
MMP-3intensity
(n)
P
Collagen fibre (n)
PWeak Strong Weak Strong Pos Neg Small Mod Large
GenderMale 59 13 46 0.867 8 51 0.934 27 32 0.818 13 32 14 0.728Female 21 5 16 3 18 9 12 3 12 6Age<55 37 11 26 0.151 5 32 0.955 20 17 0.131 6 22 9 0.686� 55 43 7 36 6 37 16 27 10 22 11
Primary sitesTongue 11 5 6 0.026 2 9 0.376 8 3 0.134 2 3 6 0.158Lip 48 12 36 8 40 19 29 9 30 9Floor of mouth 21 1 20 1 20 9 12 5 11 5TT1/T2 71 18 53 0.086 10 61 0.807 34 37 0.175 14 39 18 1.000T3/T4 9 – 9 1 8 2 7 2 5 2Lymph nodeNegative 23 13 10 <0.001 5 18 0.280 21 2 <0.001 1 12 10 0.015Positive 57 5 52 6 51 15 42 15 32 10Differentiation gradeWell 48 17 31 0.003 10 38 0.083 25 23 0.319 5 26 17 0.005Moderate 28 1 27 1 27 10 18 8 17 3Poor 4 – 4 – 4 1 3 3 1 –RecurrenceNo 58 13 45 0.976 10 48 0.273 32 26 0.003 9 31 18 0.071Yes 22 5 17 1 21 4 18 7 13 2
Statistical analysis of staining results of avb6 protein, b6 mRNA, MMP-3 protein and collagen fibre with clinicopathological parameters. Clinicopathologicalparameters were evaluated using Fisher exact tests. Statistically significant P values are italicized.aIncidentally missing cases are marked in Table 2.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
5

using multivariate analysis with the Cox regression model(P = 0.006, RR = 3.39; Table 4).
Association of collagen staining results with integrin avb6and MMP-3Morphologically, both avb6 protein and b6 mRNA dem-onstrated strong staining at the peripheral borders ofinvasive tumour islands. However, collagen fibres weregenerally disrupted and degraded (Fig. 3E), and strongexpression of MMP-3 was diffusely observed in tumourcells in adjoining tumour stroma (Fig. 4A). To explore theirrelationships, we analysed the correlations among collagenfibre per unit area, MMP-3 and avb6 expression (Table 5).
Colocalization of the expression avb6 and MMP-3For further study of the relationships between avb6 andMMP-3 expression, we proceeded with double immunoflu-orescence (Fig. 5). We found avb6 and MMP-3 expressionin the same cells at the peripheral borders of invasivetumour islands (Fig. 5A,B), although they did not exactlycolocalize (Fig. 5C). However, collagen fibres weredisrupted and degraded at the peripheral borders of invasivetumour islands (Fig. 5D).
Discussion
In the process of tumour invasion, the involvement ofMMPs in ECM degradation is accompanied by altered
expression of many cell-adhesion molecules by transformedcells. Although epithelial cells may express a variety ofcell-adhesion molecules, integrins are the most importantECM receptors and are known to play major roles in tumourinvasion and progression (9, 22).A consistent observation, confirmed by our own results,
is that avb6 is undetectable in normal oral tissues, butupregulated in many carcinomas (12, 23–29). We found thatavb6 expression levels differed in tumour cells at the edgesof tumours, which may indicate different differentiationstates of the cells. Cells at the peripheral borders of tumourswith strong avb6 expression were poorly differentiated,with strong invasion and migration abilities.b6 mRNA expression has been reported in epithelial cells
and cancer cells (10, 11). We detected b6 mRNA expressionin almost all cancer cells, including avb6� cells. A possibleexplanation for this observation is that b6 mRNA is onlytranscribed and translated into avb6 protein under certaincircumstances, such as cancer and wound healing, and thisspecific condition maintains cells in a state of excesshyperplasia.Many types of malignant tumours express MMP-3
protein at levels significantly higher than correspondingpericarcinoma or normal tissues (30–34). Studies havedemonstrated that avb6 can upregulate MMP-3 expressionin OSCC (13, 35), We detected strong avb6 and MMP-3expression at the peripheral borders of invasive tumours,which suggests that these cells have strong invasion andmigration abilities. As a possible mechanism, increasedavb6 expression may promote cancer cell adhesion to theECM, and feedback information then increases MMP-3levels (35). Elucidating the precise relationships andregulatory mechanisms between avb6 and MMP-3 requiresfurther study.In many tissues, the presence of fibrotic lesions signif-
icantly increases the risk of cancer, including lung, liver andbreast (36–38). In the past few years, oral submucousfibrosis has been accepted as a pre-malignant disease (17,39). Sumeth Perera et al. (17) demonstrated that collagen inthe lamina propria increased and extended up to theunderlying muscle layers as oral submucous fibrosis
Table 4 Relationship between avb6 intensity and overall survival in oralsquamous cell carcinoma
v2 P‐value RR 95% CI
avb6 proteinStrong 2.9584 0.085 3.68 0.83–16.22MMP-3 proteinPositive 7.7041 0.006 3.39 1.43–8.03
Only variables with P < 0.10 in the univariate analysis (Table 2) wereincluded in the multivariate model. Data were analysed using a multivariateCox model.RR, relative risk; CI, confidence interval.
A B C
Figure 2 Kaplan–Meier overall survival (OS) curves for 80 patients with oral squamous cell carcinoma (log-rank test). (A) Patients with intense avb6staining patterns had significantly worse OS compared with those with weak avb6 protein staining patterns. (B) Patients with high (n = 20) or moderate(n = 44) amounts of collagen fibre had significantly worse OS compared with those with low collagen fibre (n = 16). (C) Patients with matrixmetalloproteinase (MMP)-3+ biopsies had significantly worse OS compared with those with MMP-3� biopsies.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
6

progressed in an animal model. We observed that duringcarcinogenesis, collagen fibre thickened in the laminapropria, and its synthesis increased. This change may bedue to the response of fibres to stimulation by surroundingcells, such as myofibroblasts, increasing the number ofcollagen fibres to resist invasive cells, thus playing a role in
suppressing the generation and progression of tumours.However, as tumour malignancy increases, collagen fibreswere shown to decrease and loosen in the tumour stroma.This phenomenon indicates that increased invasiveness isassociated with morphological and content changes tocollagen fibre in ECM (40).
A B
C D
E F
G H
Figure 3 Collagen fibre changes in different tissues with Masson’s trichrome staining. (A) Normal oral mucosa. (B) Dysplastic epithelium. (C) Well-differentiated squamous cell carcinoma; arrowhead indicates thick fibre bundles. (D–E) Moderately differentiated squamous cell carcinoma; asterisk indicatesopening vessels. (F) Poorly differentiated squamous cell carcinoma. Ep, epithelium; Lp, lamina propria; Ca, cancer nest; M, muscle. Magnification shown infigures. (G–H) The staining area of collagen fibre in the lamina propria (G) and stroma (H) around invading epithelial islet of oral squamous cell carcinoma.N, normal oral mucosa; DY, dysplastic epithelium; CA, carcinoma in situ; W, well differentiated; M, moderately differentiated; P, Poorly differentiated.Values are means � SEM. *Statistically significant difference.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
7

Collagen fibre in poorly differentiated tissues wasfractured and misshapen, especially at the peripheral bordersof invasive tumours, and collagen fibre structures surround-ing vessels gradually disappeared. Collagen fibre formationwas very dense in well-differentiated cells. These observa-tions represent an apparent paradox with tumour invasive-ness. However, collagen fibres have been shown to affectrelocation of invading cells in two opposing ways: provid-ing support for invasive cells, and producing barriers toinvasion (7). This evidence supports our results. Interest-ingly, positive expression of MMP-3 was observed in thesamples with high-density collagen.
Possibly, excess ECM stimulates expression of matrix-degrading enzymes (41, 42), which then contribute totumour invasion. We speculated that increased MMP-3expression was associated with stimulation and increase incollagen fibres. Expression of MMP-3 in the mammaryglands and lungs of transgenic mice has been shown toinduce fibrosis (43); however, MMP activity is probablynecessary to remove excess collagen structures present infibrosis (44). The role and mechanisms of MMP-3 incollagen formation and degradation require further study.
We found that avb6 expression was significantlycorrelated with tumour location, differentiation and nodalstatus, which reflect histological invasion and clinical
behaviours. Previous studies have shown that avb6expression is high in patients with poor prognosis, butthe difference is not statistically significant (45, 46). Thisdiscrepancy may be related to the application of differentantibodies, the sample size and the application of differentmethods for data extraction. Collagen fibre content inhuman OSCC tissues significantly correlated with tumourdifferentiation, recurrence and nodal status, which reflectdestruction and remodelling of collagen fibre in thecarcinogenic process. While the relationships betweenMMP-3 expression and clinicopathological features arecontroversial in different tumours (31, 33, 47, 48), wefound MMP-3 expression to be significantly correlatedwith nodal status and tumour recurrence, but not tumoursize (P = 0.1749; Table 3). These results differ from thosereported by Kusukawa et al. (47) concerning stage I and IIsquamous cell carcinoma of the oral cavity, possibly due todifferences in sample size or clinical stage. MMP-3expression and nodal status are significantly related (44,47), implying an important role for MMP-3 in humanOSCC invasion and metastasis.In human OSCC specimens, the effects of avb6 and
MMP-3 expression and collagen fibre distribution onprognosis have not been previously reported. In this study,expression of avb6 and MMP-3 were predictive of a shorter5-year OS rate (Table 2). This study is the first toquantitatively analyse the correlation between collagen fibrecontent and patient prognosis from a morphologicalperspective; the 5-year OS of patients showed a statisticallysignificant trend towards positive association with collagenlevels. Using Cox multivariate analysis, MMP-3 was anindependent prognostic variable for OS. High expression ofamb6 also demonstrated a trend towards being an indepen-dent prognostic factor, but did not reach statistical signif-icance (P = 0.085). However, further research is required toinvestigate this conclusion.
A B C
Figure 4 (A) Expression of matrix metalloproteinase (MMP)-3 protein in tumour cells. (B) MMP-3 was negative or weakly expressed in normal basal cells.(C) Expression of MMP-3 protein in the cytoplasm of basal cells and stromal fibroblasts (arrowhead) in dysplastic epithelium. Ep, epithelium; Ca, tumour; S,stroma. Magnification shown in figures.
Table 5 Correlation between avb6 protein, MMP-3 protein and collagenfibre expression in 80 patients with oral squamous cell carcinoma, asdetermined by Spearman correlation from rank
Item avb6–MMP-3a avb6–collagen MMP-3–collagen
r 0.59833 �0.47163 �0.71401P <0.0001 <0.0001 <0.0001
MMP, matrix metalloproteinases.aA–B means correlation between A and B.
A B C D
Figure 5 Immunofluorescence staining of avb6 and matrix metalloproteinase (MMP)-3 in oral squamous cell carcinoma. (A) shows staining for avb6 ingreen at the peripheral borders of invasive tumour islands. (B) shows the same field staining for MMP-3 in red. (C) reflects the overlay of green and red.MMP-3 was present in the same cells (arrowhead), but did not exactly colocalize with avb6. (D) shows that collagen fibres were disrupted and degraded(arrowhead) at the same sites. Ca, cancer nest.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
8

Spearman correlation from ranks was used to analyseinteractions among avb6, MMP-3 and collagen fibres(Table 5). Our results showed that MMP-3 expressionwas significantly correlated with avb6 expression andcollagen fibre. In addition, we found that avb6 andMMP-3 expression in the same cells at the peripheralborders of invasive tumour islands. Increased avb6upregulates MMP-3 expression in OSCC cells (13, 35),so we believe that avb6 maybe also can regulate MMP-3expression in human OSCC. MMP-3 expression wassignificantly negative correlated with collagen fibre in ourresults; this indicates that MMP-3 is directly or indirectlyinvolved in the degradation of collagen fibre. And, avb6was expressed in the peripheral borders of invasivetumour islands, but collagen fibres were generallydisrupted and degraded at the same sites. So, our resultssupport the speculation that there is a regulation pathwaybetween the expression of avb6, MMP-3 and collagenfibres, and this pathway may be involved in the invasionof the OSCC.
In conclusion, increased avb6 integrin and MMP-3expression and collagen fibre changes in human OSCCsindicate poor prognosis and decreased survival. avb6 andMMP-3 expression were correlated with collagen fibredistribution. Tumour cells with high avb6 expression havestrong invasion and migration abilities, and show concom-itant protease production, and destruction and remodellingof collagen fibre.
References
1. Scully C, Bagan J. Oral squamous cell carcinoma overview.Oral Oncol 2009; 45: 301–8.
2. Lippman SM, Sudbo J, Hong WK. Oral cancer prevention andthe evolution of molecular-targeted drug development. J ClinOncol 2005; 23: 346–56.
3. de Vicente JC, Lequerica-Fernandez P, Santamaria J, FresnoMF. Expression of MMP-7 and MT1-MMP in oral squamouscell carcinoma as predictive indicator for tumor invasion andprognosis. J Oral Pathol Med 2007; 36: 415–24.
4. Rowe RG, Weiss SJ. Navigating ECM barriers at the invasivefront: the cancer cell-stroma interface. Annu Rev Cell Dev Biol2009; 25: 567–95.
5. Hu M, Polyak K. Microenvironmental regulation of cancerdevelopment. Curr Opin Genet Dev 2008; 18: 27–34.
6. Friedl P, Wolf K. Plasticity of cell migration: a multiscaletuning model. J Cell Biol 2010; 188: 11–9.
7. Makareeva E, Han S, Vera JC, et al. Carcinomas contain amatrix metalloproteinase-resistant isoform of type I collagenexerting selective support to invasion. Cancer Res 2010; 70:4366–74.
8. Hynes RO. Integrins: versatility, modulation, and signaling incell adhesion. Cell 1992; 69: 11–25.
9. Thomas GJ, Nystrom ML, Marshall JF. Alphavbeta6 integrinin wound healing and cancer of the oral cavity. J Oral PatholMed 2006; 35: 1–10.
10. Breuss JM, Gallo J, Delisser HM, et al. Expression of the beta6 integrin subunit in development, neoplasia and tissue repairsuggests a role in epithelial remodeling. J Cell Sci 1995; 108:2241–51.
11. Breuss JM, Gillett N, Lu L, Sheppard D, Pytela R. Restricteddistribution of integrin beta 6 mRNA in primate epithelialtissues. J Histochem Cytochem 1993; 41: 1521–7.
12. Impola U, Uitto VJ, Hietanen J, et al. Differential expressionof matrilysin-1 (MMP-7), 92 kD gelatinase (MMP-9), andmetalloelastase (MMP-12) in oral verrucous and squamouscell cancer. J Pathol 2004; 202: 14–22.
13. Ramos DM, But M, Regezi J, et al. Expression of integrin beta6 enhances invasive behavior in oral squamous cell carcinoma.Matrix Biol 2002; 21: 297–307.
14. Ylipalosaari M, Thomas GJ, Nystrom M, et al. Alpha v beta 6integrin down-regulates the MMP-13 expression in oral squa-mous cell carcinoma cells. Exp Cell Res 2005; 309: 273–83.
15. Thomas GJ, Lewis MP, Hart IR, Marshall JF, Speight PM.AlphaVbeta6 integrin promotes invasion of squamous carci-noma cells through up-regulation of matrix metalloproteinase-9. Int J Cancer 2001; 92: 641–50.
16. Puthawala K, Hadjiangelis N, Jacoby SC, et al. Inhibition ofintegrin alpha (v) beta6, an activator of latent transforminggrowth factor-beta, prevents radiation-induced lung fibrosis.Am J Respir Crit Care Med 2008; 177: 82–90.
17. Sumeth Perera MW, Gunasinghe D, Perera PA, et al. Devel-opment of an in vivo mouse model to study oral submucousfibrosis. J Oral Pathol Med 2007; 36: 273–80.
18. Peng Z, Yu-Bin D, Miao Y, et al. Changes of the elastic fibersand collagen fibers during the development and progression ofexperimentally induced tongue zarcinoma in hamsters. J SouthMed Univ.2010; 12: 2696–8.
19. Kerkela E, Saarialho-Kere U. Matrix metalloproteinases intumor progression: focus on basal and squamous cell skincancer. Exp Dermatol 2003; 12: 109–25.
20. Sobin LH, Fleming ID. TNM classification of malignanttumors, fifth edition (1997) Union Internationale Contre leCancer and the American Joint Committee on Cancer. Cancer1997; 80: 1803–4.
21. Laitakari J, Stenbeck F. Collagen matrix in development andprogression of experimentally induced respiratory neoplasmsin the hamster. Toxicol Pathol 2001; 29: 514–27.
22. Juliano RL, Varner JA. Adhesion molecules in cancer: the roleof integrins. Curr Opin Cell Biol 1993; 5: 812–8.
23. Hazelbag S, Kenter GG, Gorter A, et al. Overexpression of thealpha v beta 6 integrin in cervical squamous cell carcinoma is aprognostic factor for decreased survival. J Pathol 2007; 212:316–24.
24. Bates RC, Bellovin DI, Brown C, et al. Transcriptionalactivation of integrin beta6 during the epithelial-mesenchymaltransition defines a novel prognostic indicator of aggressivecolon carcinoma. J Clin Invest 2005; 115: 339–47.
25. Patsenker E, Wilkens L, Banz V, et al. The alphavbeta6integrin is a highly specific immunohistochemical marker forcholangiocarcinoma. J Hepatol 2010; 52: 362–9.
26. Ahmed N, Riley C, Rice GE, Quinn MA, Baker MS.avb6Integrin-a marker for the malignant potential ofepithelial ovarian cancer. J Histochem Cytochem.2002; 50:1371–80.
27. Saha A, Ellison D, Thomas GJ, et al. High-resolution in vivoimaging of breast cancer by targeting the pro-invasive integrinalphavbeta6. J Pathol 2010; 222: 52–63.
28. Hecht JL, Dolinski BM, Gardner HA, Violette SM, WeinrebPH. Overexpression of the alphavbeta6 integrin in endometrialcancer. Appl Immunohistochem Mol Morphol 2008; 16: 543–7.
29. Kawashima A, Tsugawa S, Boku A, et al. Expression ofalphav integrin family in gastric carcinomas: increasedalphavbeta6 is associated with lymph node metastasis. PatholRes Pract 2003; 199: 57–64.
30. Nakopoulou L, Gakiopoulou H, Zervas A, et al. MMP-3mRNA and MMP-3 and MMP-1 proteins in bladder cancer: acomparison with clinicopathologic features and survival. ApplImmunohistochem Mol Morphol 2001; 9: 130–7.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
9

31. Duffy MJ, Maguire TM, Hill A, McDermott E, O’Higgins N.Metalloproteinases: role in breast carcinogenesis, invasion andmetastasis. Breast Cancer Res 2000; 2: 252.
32. Arguello-Ramirez J, Perez-Cardenas E, Delgado-Chavez R,Solorza-Luna G, Villa-Trevino S, Arenas-Huertero F. Matrixmetalloproteinases-2, -3, and -9 secreted by explants of benignand malignant lesions of the uterine cervix. Int J GynecolCancer 2004; 14: 333–40.
33. Lim BJ, Jung SS, Choi SY, Lee CS. Expression of metastasis-associated molecules in non-small cell lung cancer and theirprognostic significance. Mol Med Report 2010; 3: 43–9.
34. Mukherjee S, Roth MJ, Dawsey SM, et al. Increased matrixmetalloproteinase activation in esophageal squamous cellcarcinoma. J Transl Med 2010; 8: 91.
35. Dang D, Yang Y, Li X, et al. Matrix metalloproteinases andTGFbeta1 modulate oral tumor cell matrix. Biochem BiophysRes Commun 2004; 316: 937–42.
36. Artinian V, Kvale PA. Cancer and interstitial lung disease.Curr Opin Pulm Med 2004; 10: 425.
37. Bissell DM. Chronic liver injury, TGF-beta, and cancer. ExpMol Med 2001; 33: 179–90.
38. Boyd NF, Dite GS, Stone J, et al. Heritability of mammo-graphic density, a risk factor for breast cancer. N Engl J Med2002; 347: 886–94.
39. Moutasim KA, Jenei V, Sapienza K, et al. Betel-derivedalkaloid up-regulates keratinocyte alphavbeta6 integrin expres-sion and promotes oral submucous fibrosis. J Pathol 2011;223: 366–77.
40. Stamenkovic I. Matrix metalloproteinases in tumor invasionand metastasis. Semin Cancer Biol 2000; 10: 415–33.
41. Schuppan D, Ruehl M, Somasundaram R, Hahn EG. Matrix asa modulator of hepatic fibrogenesis. Semin Liver Dis 2001; 21:351–72.
42. Sawada S, Murakami K, Murata J, Tsukada K, Saiki I.Accumulation of extracellular matrix in the liver induces high
metastatic potential of hepatocellular carcinoma to the lung. IntJ Oncol 2001; 19: 65–70.
43. Thomasset N, Lochter A, Sympson CJ, et al. Expression ofautoactivated stromelysin-1 in mammary glands of transgenicmice leads to a reactive stroma during early development. AmJ Pathol 1998; 153: 457–67.
44. Parks WC, Shapiro SD. Matrix metalloproteinases in lungbiology. Respir Res 2001; 2: 10–9.
45. Korpi JT, Kervinen V, Maklin H, et al. Collagenase-2 (matrixmetalloproteinase-8) plays a protective role in tongue cancer.Br J Cancer 2008; 98: 766–75.
46. Marsh D, Suchak K, Moutasim KA, et al. Stromal features arepredictive of disease mortality in oral cancer patients. J Pathol2011; 223: 470–81.
47. Kusukawa J, Sasaguri Y, Morimatsu M, Kameyama T.Expression of matrix metalloproteinase-3 in stage I and IIsquamous cell carcinoma of the oral cavity. J Oral MaxillofacSurg 1995; 53: 530–4.
48. Kusukawa J, Harada H, Shima I, Sasaguri Y, Kameyama T,Morimatsu M. The significance of epidermal growth factorreceptor and matrix metalloproteinase-3 in squamous cellcarcinoma of the oral cavity. Eur J Cancer B Oral Oncol 1996;32B: 217–21.
Acknowledgements
This work was supported by grants from the National Natural Science
Foundation of China (305400083).
Conflict of interest
None declared.
J Oral Pathol Med
avb6 integrin and collagen fibre in OSCC
Li et al.
10