Enhanced Peripheral γδT Cells Cytotoxicity Potential in Patients with HBV-Associated...
9
Click here to load reader
Transcript of Enhanced Peripheral γδT Cells Cytotoxicity Potential in Patients with HBV-Associated...

Enhanced Peripheral γδT Cells Cytotoxicity Potential in Patientswith HBV-Associated Acute-On-Chronic Liver Failure MightContribute to the Disease Progression
Min Chen & Peng Hu & Hui Peng & Weiqun Zeng &
Xiaofeng Shi & Yu Lei & Huaidong Hu & Dazhi Zhang &
Hong Ren
Received: 15 November 2011 /Accepted: 21 February 2012 /Published online: 14 March 2012# Springer Science+Business Media, LLC 2012
AbstractBackground The current study explored the characteristics ofγδ T cells in the blood of HBV-associated acute-on-chronicliver failure (HBV-ACLF) patients and examined the relation-ship between γδ T cells and the clinical parameters.Methods Blood samples were obtained from 26 patientswith HBV-ACLF, 40 patients with chronic hepatitis B virus(HBV) infection (CHBV), and 25 healthy controls (HC).The frequencies of γδ T cells, subtype Vδ1T or Vδ2T, andCD45RO+γδ T cells were determined using flow cytometry.Intracellular cytokine staining analysis was used to evaluatethe proportion of the IFN-γ-, TNF-α-, or IL-17-producingγδ T cells, and CD107a- or granzyme B-positive γδ T cells.Results We found that the proportion of γδ T cells in bloodsamples from HBV-ACLF patients was much lower than insamples from CHBV patients or healthy controls. Afterstimulation with PMA and ionomycin, γδ T cells from
HBV-ACLF patients produced the greatest amount of TNF-α or IL-17 among the three groups. Granzyme B- or CD107a-positive γδ T cells were significantly more frequent than inCHBV or control samples. There was a negative correlationbetween the percent of TNF-α+γδ T cells and ALT or ASTlevels, and between the percent of CD107a+γδ T cells andTBiL or DBiL levels.Conclusions These results suggest that γδ T cells mightparticipate in liver injury in HBV-ACLF patients by produc-ing increased amounts of inflammatory cytokines and/orcytotoxicity ability. These findings provide novel informa-tion regarding the pathogenesis of HBV-ACLF.
Keywords Chronic hepatitis B .γδ Tcells . HBV-associatedacute-on-chronic liver failure . inflammatory cytokine
Hepatitis B virus (HBV) infection is one of the most serioushealth problems worldwide. There is considerable heteroge-neity in the observed clinical manifestation of personsinfected with HBV from asymptomatic carrier, acute infec-tion, to chronic hepatitis B depending on viral and hostfactors. About 95% of adult patients resolve hepatitis Binfection as determined by HBsAg seroclearance. Approxi-mately 5% of infected individuals develop chronic HBV(CHBV) infection, severe sequelae such as the liver cirrho-sis, liver cancer, or acute-on-chronic liver failure (ACLF)may occur as the disease progresses [1–3]. ACLF is a severelife-threatening clinical syndrome characterized by jaundice,coagulopathy, hepatic encephalopathy, and a high mortalityrate. More than 80% of all ACLF cases in China are asso-ciated with CHBV infection and occur in patients withCHBV, CHBV-related chronic liver cirrhosis, or in chronicasymptomatic HBV carriers [4, 5].
Electronic supplementary material The online version of this article(doi:10.1007/s10875-012-9678-z) contains supplementary material,which is available to authorized users.
M. Chen (*) : P. Hu :W. Zeng :X. Shi :Y. Lei :H. Hu :D. Zhang :H. Ren (*)Key Laboratory of Molecular Biology for Infectious Diseases,Ministry of Education, Institute for Viral Hepatitis,Department of Infectious Diseases, Second Affiliated Hospital,Chongqing Medical University,No.74 Lin Jiang Rd., Yu Zhong District,400010 Chongqing, People’s Republic of Chinae-mail: [email protected]: [email protected]
H. PengDepartment of Laboratory Medicine, Second Affiliated Hospital,Chongqing Medical University,No.74 Lin Jiang Rd., Yu Zhong District,400010 Chongqing, People’s Republic of China
J Clin Immunol (2012) 32:877–885DOI 10.1007/s10875-012-9678-z

Although the mechanism underlying the development ofACLF is not completely clear, it has been reported in mul-tiple studies that immune-mediated liver injury might playan important role in the pathogenesis of ACLF. Notably, alarge percent of necrotic hepatocytes and a high level ofinflammatory infiltrate have been observed in the liver ofmany ACLF patients. Non-antigen specific immune cells,such as NK cells, and bystander activation of cytotoxic Tcells, IL-17-producing CD4+ T cells, and NKT cells, haveall been demonstrated to mediate hepatocyte death. Inflam-matory cytokines are also critical for the development oflethal necroinflammatory liver disease in ACLF patients andin the fulminant hepatitis mouse model. Elevated serumlevels of several cytokines and soluble cytokine receptors,including TNF-α, sTNF-αR1, sTNF-αR2, IL-2, IL-2R, IL-4, IL-6, IL-8, IL-10, and interferon-γ, have been describedin patients with ACLF [6–10].
γδ T cells are distinct from αβ T cells (the conventionalCD4+ and CD8+ T cells), and express the γ and δ chains ofthe T cell receptor (TCR). There are two major subtypes,Vδ1 and Vδ2 T cells. γδ T cells have several innate cell-likefeatures, a unique and broadly functional repertoire, andparticipate in immune responses both early and late aseffector cells and/or immune regulators. They may also playimportant roles in early recognition of conserved stress-induces ligands, pathogen clearance via directly killing ofinfected cells or producing inflammatory cytokines, or reg-ulating immune responses [11–13]. Further research hasdemonstrated that γδ T cells participated in a variety ofimmunopathogenesis-associated processes induced by viral,parasitic, or bacterial infection, or by autoimmune reactions[14–17]. In our previous report, it was demonstrated that theproportion of γδ T cells in peripheral blood increased andthere was a decrease in the percent of Vδ2 T cells in patientswith chronic hepatitis B [18].
In the current study, we evaluated the characteristics ofγδ T cells in patients with HBV-related ACLF and exam-ined if γδ T cells were one of the mediating factors in thedevelopment of HBV-ACLF. We performed detailed immune
phenotyping and immune function analysis of γδ T cells inHBV-ACLF patients and investigated the relationship with theclinical parameters.
Patients and Methods
Patients
All patients enrolled in this study were from the secondaffiliated hospital of Chongqing Medical University.Twenty-six HBV-ACLF patients, forty patients with CHBV,and twenty-five healthy controls (HC) were enrolled in thisstudy, and the general characteristics of all patients and HCare summarized in Table I. CHBV patients met the diagnos-tic criteria developed by the AASLD or Chinese Society ofHepatology, and were positive for serum HBsAg, HBeAg orHBeAb, HBcAb, and HBV-DNA (≥104 copies/mL) formore than 6 months. All ACLF patients had a history ofCHBV and developed acute jaundice (total bilirubin≥85 μmol/L), coagulopathy (prothrombin activity<40%),and even hepatic encephalopathy, ascites, or hepatorenalsyndrome. None of the patients were treated with any anti-HBVagent for at least 6 months prior to enrollment. Patientswere excluded if they were co-infected with other hepatitisviruses or had other liver diseases, such as hepatocellularcarcinoma, autoimmune disease, or alcoholic hepatitis.Blood samples from HBV-ACLF patients were obtained at1 day to 1 week after diagnosis. The study protocol wasapproved by the ethics committee of the second affiliatedhospital of Chongqing Medical University and written in-formed consent was obtained from each subject prior toblood sampling.
Determination of Clinical Parameters
All liver function parameters (e.g., ALT, AST, TBiL, andDBiL) were evaluated using an automatic biochemistryanalyzer. The main serum markers of hepatitis B, including
Table I Clinical parameters ofenrolled subjects (data wereshown as median and range)
Abbreviations: HC healthy con-trol; CHBV chronic hepatitis Bvirus infection; HBV-ACLFHBV-associated acute-on-chronic liver failure; ALT alanineaminotransferase; AST aspartateaminotransferase; TBIL total bil-irubin; DBIL direct bilirubin;PTA prothrombin activity; HBVhepatitis B virus; HBeAg e anti-gen of hepatitis B virus
Patients HC CHBV HBV-ACLF
Cases 25 40 26
Age(year) 40(24–51) 29.5(20–46) 40.5(26–78)
Sex(m/f) 14/11 31/9 21/5
ALT(U/L) 22(7–33) 199.5(95–1178) 206(61–1443)
AST(U/L) 22(19–28) 89(30–698) 187(75–966)
TBIL(umol/L) 11.3(9.2–15.7) 19.8(8.8–625.1) 427.6(102–932.1)
DBIL(umol/L) 1.9(0.4–3.6) 9.3(1.1–408.9) 326.7(92.3–658.8)
PTA(%) 94(86–100) 92(82–100) 29(11–39)
HBeAg(+/−) 0/25 33/7 18/8
Serum HBV DNA [lg(copies/mL)] 0 6.9(4.4–8.9) 6.3(4.1–7.6)
878 J Clin Immunol (2012) 32:877–885

HBsAg, HBsAb, HBeAg, HBeAb, and HBcAb, wereassayed using the Roche electrochemical luminescencemethod. Serum HBV-DNA was quantitatively determinedusing a fully automated real-time PCR machine (Roche).Additionally, prothrombin activity was measured using anautomated coagulation system. The clinical parameters ofthese subjects were shown in Table I.
Surface Phenotyping of Whole Blood or White Blood Cells(WBCs)
The following fluorochrome-conjugated monoclonal anti-bodies (mAb) were purchased from BD Bioscience (LaJolla, CA, USA): PerCP-conjugated anti-CD3 mAb (cloneSK7), FITC-conjugated anti-CD4 mAb (clone RPA-T4),PECy7-conjugated anti-CD8 mAb (clone RPA-T8), allo-phycocyanin (APC)-conjugated anti-TCR γδ mAb (cloneB1), PE-conjugated anti-Vδ2 mAb (clone B6), PECy7-conjugated anti-CD3 mAb (clone SK7), FITC-conjugatedanti-CD56 mAb(clone NCAM16.2) and PE-conjugatedanti-CD45RO-PE mAb (clone UCHL1). FITC-conjugatedanti-Vδ1 mAb was purchased from Thermo Fisher Scientif-ic (Rockford, IL, USA, clone TS8.2). The staining proce-dure was performed according to the instructions providedby the manufacturer. In brief, the appropriate volume ofantibody was added to 100 μL fresh peripheral anticoagu-lated blood, and incubated 15 to 30 min in the dark at 4°C.Erythrocytes were lysed using BD FACSTM lysing solution,and cells were washed in PBS supplemented with 1% fetalcalf serum (FCS). Stained cells were stored at 2 to 8°C untilanalyzed using the FACS Canto II flow cytometer (BDImmunocytometry System, San Jose, CA, USA). Data wereanalyzed using FACSDiva 2.0 software (BD Immunocy-tometry System).
For the determination of HBV-specific CD8+ T cells, theWBCs were obtained from whole blood of HLA-A2+patients with erythrocytes lysis using PBS containing0.85% NH4CL. Then the HBc18-27-specific CD8+ T cellswere labeled with PE-conjugated HLA-A2 class I pentamers(Proimmune, Oxford, UK) bearing the HBc18-27 epitopefor 10 min at 37°C. After washed with FACS buffer, thecells were stained with FITC–conjugated anti-CD8 mAb(BD Bioscience, La Jolla, CA, USA, clone SK1) for30 min at 4°C followed by fixation with 4% paraformalde-hyde. At least 105 target cells were analyzed by flowcytometry.
Intracellular Staining
Cells were stained as described elsewhere with a minormodification. Briefly, total leukocytes were adjusted toabout 5×106/mL in RPMI 1640 culture media supple-mented with 10% FCS and stimulated with 100 ng/mL
phorbol myristate acetate (PMA) plus 1 μg/mL ionomycinfor 4 h in the presence of the secretion inhibitors monensinand brefeldin A (BD Bioscience). Cells were then stainedwith APC-conjugated anti-TCR γδ mAb, followed bywashing with PBS, and fixation using 4% paraformalde-hyde. Stained cells were permeabilized using 0.1% saponin(Sigma, St. Louis, MO, USA). Then, cells were incubatedwith FITC-conjugated anti-IFN-γ (eBioscience, San Diego,CA, USA clone 4S.B3), PE-conjugated anti-TNF-α (BDBioscience, clone Mab11), PE-conjugated anti-IL-17 (eBio-science, clone eBio64DEC17), PE-conjugated anti-CD107a(BD Bioscience, clone H4A3), or FITC-conjugated anti-Granzyme B (BD Bioscience, clone GB11) for 30 min at4°C. Finally, cells were washed with PBS, and stored at 2 to8°C until analyzed using the FACS Canto II flow cytometer(BD Immunocytometry System, San Jose, CA, USA). Datawere analyzed using FACSDiva 2.0 software (BD Immuno-cytometry System).
Statistical Analysis
All data were analyzed using SPSS 13.0 software (SPSSInc, Chicago, IL). Data were expressed as the median andrange. The Kruskal-Wallis Test (non-parametric, two-tailed,and unpaired) was performed to test the differences betweenthe groups, and the difference of every two groups wastested using the Mann–Whitney U test. Spearman’s rankcorrelation test was used for correlation analysis. Differ-ences were considered statistically significant at p<0.05.
Results
The Proportion of γδ T Cells, Subtype Vδ1T or Vδ2T, andCD45RO+ γδ T Cells in HBV-ACLF Patients
The proportion of total γδ T cells was compared betweenthe three groups (Fig. 1). The median percent of γδ T cellsin the CD3+ population was 10.3%, 10.7%, or 4.8% in theHC (n025), CHBV (n040), or HBV-ACLF (n026) patients,respectively. The proportion of total γδ T cells in HBV-ACLFpatients was statistically significantly lower than in HC orCHBV patients (p<0.001). For the HBV-ACLF patients, theaverage percent of Vδ1T cells was 21.4% (data shown asmedian), which was significantly higher than in HC (10.3%)(p<0.01); average percent of Vδ2T cells was 66.9%, whichwas significantly lower than in HC (81.2%) (p00.004). How-ever, there was no significant differences between the CHBVandHBV-ACLF patients (Vδ1T: 17.3% vs. 21.4%, respective-ly; Vδ2T: 75.7% vs. 66.9%, respectively) (p>0.05) (Fig. 2).
Based on the Vδ1 T cell percentage, HBV-ACLF patientscould be subdivided into two subgroups: patients with highnumbers of Vδ1T cells and patients with relatively low
J Clin Immunol (2012) 32:877–885 879

numbers. Thirteen patients displayed a high percentage of Vδ1T cells (> 21.4%, which was the average percent of Vδ1 T cellin the HBV-ACLF group), and the other thirteen were relativelylow (≤ 21.4%). However, the clinical parameters and the
proportion of immune cells were not statistically significantlydifferent between the two subgroups (data not shown).
The CD45RO memory phenotype of γδ T cells was alsocompared between the three groups. The proportion of
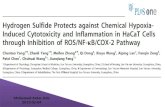
Fig. 1 A typical FACS result of the directly cell surface staining (dotplots) of peripheral blood, and the intracellular staining (histogramplots) of WBC stimulated with PMA and ionomycin in the patientswith HBV-ACLF. The results showed the proportion of γδ T (%CD3),CD4+ T (%CD3), CD8+ T (%CD3), CD3-CD56+ NK (%lymphocyte),
or CD3+CD56+ NKT (%lymphocyte) cells,then the percentage ofCD45RO + γδ T cells, or the Vδ1 or Vδ2 T in total γδ T cells. Wecould also obtain the proportion of IFN-γ+, TNF-α+, IL-17+,CD107a+, or granzyme B+ γδT cells from the figure
880 J Clin Immunol (2012) 32:877–885

CD45RO+ γδ T cells in HBV-ACLF patients (43.5%) wassignificantly higher than in CHBV patients (30.7%) (p00.028) or HC (15.8%) (p<0.001) (Fig. 2).
Differences in the Percent of CD4+ T, CD8+ T, NK, or NKTCells Among the HBV-ACLF, CHBV, or HC Groups
In addition to the phenotypic evaluation of γδ T cells, thepercentage of CD4+ T, CD8+ T, NK, or NKT cells was alldetermined using flow cytometry (Figs. 1 and 2). The aver-age proportion of NK cells in HBV-ACLF (n026) (7.4%)was significantly lower than in either CHBV patients (n040) (10.0%) (p00.038) or HCs (n025) (14.9%) (p<0.001).The average NKT percentage in HBV-ACLF patients (3.7%)was significantly increased compared to HC (1.8%) (p<0.001), but there was no difference compared to CHBVpatients (2.9%) (p>0.05). An increase in the CD4+ T cellpercent in HBV-ACLF patients (62.9%) was also found com-pared to the CHBV patients (51.5%) (p<0.001) or HC(50.3%) (p<0.001). In contrast, the average proportion ofCD8+ T cells in HBV-ACLF (33.4%) was statistically signif-icantly lower compared to the HC group (36.3%) (p00.042).
Besides, the frequency of peptide HBc18-27-specificCD8+ T-cells was also determined in the blood of 7 HLA-A2+ CHBV patients or 7 HLA-A2+ HBV-ACLF patients.The representative FACS figures were showed in the Sup-plementary Figure 1. The results showed the average per-centage of HBV-specific CD8+ T cells was 0.6% (median)for the CHBV patients or 0.7% for HBV-ACLF patients.There were no significant differences between these twogroups (p>0.05).
Intracellular Expression of IFN-γ, TNF-α, or IL-17 by γδ TCells in HBV-ACLF Patients
After PMA and ionomycin stimulation, there were moreIFN-γ+ γδ T cells from HBV-ACLF patients (n026)(73.9%) compared to samples from HC samples (n025)(45.3%) (p<0.001), but there was no difference comparedto the CHBV samples (n040) (70.9%) (Figs. 1 and 2)(p>0.05). HBV-ACLF patients exhibited a much higher
Fig. 2 a and b boxplots showed the results of cell surface staining ofwhole blood in HC (n025), CHBV (n040), or HBV-ACLF (n026)group. The statistics results displayed the lowest γδ T or NK percent-age, or highest CD45RO+γδ T or CD4+T percentage in HBV-ACLFpatients among the three groups. Meanwhile, the results also showedthe increaced Vδ1 T, NKT percentage or the decreaced Vδ2 T orCD8+T percentage in HBV-ACLF patients when compared to the HCgroup, but there was no different when compared to the CHBV group.The intracellular staining results of the HC (n025), CHBV (n040), orHBV-ACLF (n026) group were represented in the (c) boxplots. It wasshowed the the frequency of IFN-γ, TNF-α, or IL-17 producing γδ Tcells or the CD107+ or granzyme B+γδ T cells was all increased inpatients with HBV-ACLF. (*: p<0.05, **:p<0.01)
�
J Clin Immunol (2012) 32:877–885 881

proportion of TNF-α+ γδ T cells (26.7%) than CHBVpatients (11.5%) (p<0.001) or the HC group (11.7%)(p<0.001). Moreover, IL-17-producing γδ T cells werealso more prevalent in the HBV-ACLF samples than inCHBV or HC samples (0.7%, 0.3%, or 0.3%, respectively)(p<0.001).
We further compared the proportion of the cytokine-producing γδ T cells between the HBV-ACLF and addition-al 4 patients with autoimmune hepatitis (AIH). The resultswere displayed in the Supplementary Table 1. The frequen-cy of total blood γδ T cells in these 4 AIH patients was11.1% (median), which showed higher than that in the HBV-ACLF patients (4.8%). Moreover, it was observed that thepercentage of IFN-γ+ γδ T cells in these 4 AIH patients(median was 58.1%) was lower than that in the HBV-ACLFpatients, but these AIH patients showed a higher percentageof TNF-α+ or IL-17+ γδ T cells (30.6%, or 1.0%) than thatin the HBV-ACLF patients.
Furthermore, the longitudinal analysis of the frequencyof γδ T-cells or the cytokine-producing γδ T-cells in 4HBV-ACLF in-patients were carried out firstly during theirfirst 24 h of hospitalization, and secondly when dischargedfrom the hospital. The results showed that the proportion oftotal γδ T or the IFN-γ, TNF-α+, or IL-17+ γδ T cells in thepatients at the time of admission was not significantly dif-ferent from that after hospitalization.
CD107a and Granzyme B Expression in γδ T Cells in HBV-ACLF Patients
γδ T cells cytotoxicity is one of the most important func-tions of these T cells. Therefore, CD107a and granzyme Bexpression, indicators of degranulation or cytotoxicity, wasevaluated in the three groups (Figs. 1 and 2). The medianpercentage of CD107a+ or granzyme B+ γδ T cells in HBV-ACLF group (n026) was 60.3% and 69.1%, respectively,which was significantly higher than in either the CHBV (n040) or HC groups (n025) (CD107a: 34.9% and 33.7%;Granzyme B: 50.5% and 33.3%, respectively) (p<0.01).
The Correlation Between the Proportion of Total γδ T Cellsor Specific γδ T Cell Subsets and Clinical Parameters in theHBV-ACLF Patients
Determination of the Spearman correlation coefficient indi-cated that the frequency of CD45RO+ γδ T cells was neg-atively correlated to the total bilirubin (TBiL) level (p00.039). Additionally, the proportion of TNF-α+ γδ T cellswas negatively correlated to both the ALT (p00.047) andAST level (p00.020). Furthermore, the CD107+ γδ T per-centage was also negatively correlated with either TBiLlevel (p00.032) or direct bilirubin (DBiL) level (p00.012).
No other correlation evaluated displayed statistical signifi-cance (Fig. 3).
The Relationship Between γδ T Cells and Other ImmuneCells in HBV-ACLF Patients
The correlation test analyses also demonstrated that thefrequency of total γδ T cells was positively correlated tothe percent of NKT cells (p00.012), and the proportion ofCD45RO+ γδ T cells was positively correlated with thepercent of NK cells (p00.023). Moreover, the frequency ofIL-17+ γδ T cells was positively correlated with the propor-tion of NKT cells (p00.018). There was also a positivecorrelation between the proportion of CD107a+ γδ T cellsand granzyme B+ γδ T (p<0.001) (Fig. 3).
Discussion
ACLF is defined as “acute hepatic insult manifesting asjaundice and coagulopathy, complicated within 4 weeks byascites and/or encephalopathy in a patient with previouslydiagnosed or undiagnosed chronic liver disease.” In Asia,chronic hepatitis or cirrhosis related to HBV is the maincause of liver diseases that have the potential to developACLF [1, 2, 4, 5]. Although the pathophysiologic mecha-nisms of HBV-ACLF are not clear, acute systemic inflamma-tory responses, induced by a predominantly proinflammatorycytokine profile, is thought to be the most important reason forthe transition from chronic hepatitis or stable cirrhosis toACLF. The high level of serum cytokines and soluble cyto-kine receptors, including TNF-α, sTNF-αR1, sTNF-αR2, IL-2, and IFN-γ, have been detected in HBV-ACLF patients [4,5]. What are the underlying mechanisms mediating this cyto-kine release? In recent studies related to the HBV-ACLF, itwas demonstrated that NK, NKT, or other innate cells werehyperfunctional and were very important sources of thesecytokines [7–10]. However, the involvement of γδ T cells inthe production of inflammatory cytokines or in HBV-ACLFhas not been examined.
γδ T cells are known to be very important sources ofinflammatory cytokines, including IFN-γ, TNF-α, andIL-17 [11, 13, 19]. Our previous study demonstrated thatpatients with CHBV had a lower proportion of Vδ2 Tcells compared to the healthy control subjects [18].Therefore, in the current study we sought to determinewhat changes in the immunophenotype or immunofunc-tion of γδ T cells occurred in HBV-ACLF patients andif γδ T cells played an important role in the pathogen-esis of HBV-ACLF by performing an in-depth character-ization of the immunophenotype, inflammatory cytokineproduction, or cytotoxic function of peripheral γδ T cellsin HBV-ACLF.
882 J Clin Immunol (2012) 32:877–885

First, the results demonstrated that the proportion of γδ Tcells in HBV-ACLF was much lower than in CHBV patientsor HCs. Notably, in HBV-ACLF patients, the percent ofCD8+ T and CD3+CD56+ T cells were also decreased com-pared to CHBV patients and the HC group. γδ T, CD8+ T,and CD3+CD56+ T cells may all express CD107a or gran-zyme B and possess cytotoxic activity; all of these immunecells may also be important cellular sources of inflammatorycytokines. It has been suggested that these cytolytic cells
might participate in the process of ACLF, and a decreasedpercentage of these peripheral blood cells may imply thatthey are sequestered in the liver or other organs, or beexhausted during disease development. In the current study,we found that the percent of CD8+ or γδ T cells was higherin HBV-ACLF patients than in the HC group. This was notobserved for NKT cells, which may be due to the fact thatthese cells are more prevalent in the liver. And we furtherinvestigated the frequency of HBc18-27-specific CD8+ T-
Fig. 3 (A) Figures represented the correlation analysis results betweenthe γδ T cells and the clinical parameters. The (A) figures showed thenagative correlation between the CD45RO+γδ T cells percentage andTBIL level, TNF-α+γδ T cells percentage and ALT or AST level, orCD107+ γδ T cells percentage and TBIL or DBIL level. The (B)
figures showed the positive correlation between the CD45RO+γδ Tcells percentage and the NK percentage, between the NKT percentageand the proportion of γδ T or IL-17+ γδ T cells, or between theCD107+ γδ T percentage and the granzyme B+γδ T percentage
J Clin Immunol (2012) 32:877–885 883

cells in HBV-ACLF patients, and observed that there wereno significantly differences between HBV-ACLF group andCHBV group. These results support the idea that the non-specific immune cells play very important role in the HBV-ACLF development.
In humans, circulating γδ T cells are mainly comprised ofthe Vδ2 (>70%) and Vδ1 subsets. However, during somebacterial or viral infections, such as HIV, the proportion ofVδ1 T cells increases very high [11, 12]. In our study, weobserved an increase in the percentage of Vδ1 T cells but adecrease in the percentage of Vδ2 T cells in HBV-ACLFcompared to HCs, but not CHBV patients. It has beensuggested that either the generation of more Vδ1 T cells orthe elimination of Vδ2 T cells might contribute to ACLF.Vδ1 T cells are the main γδ T cell subset in the liver;therefore, an increase in the proportion of peripheral Vδ1T cells might indicate that they also increased in the liver.There are other subtypes besides subtype Vδ1T or Vδ2Tcells, and we could learn about their percentage from Fig. 1,but the statistical results showed no significant differencesamong these three groups (data not shown).
To evaluate the percentage of memory γδ T cells, theexpression of CD45RO on γδ T cells was determined. Therewas a much higher proportion of CD45RO+ γδ T cells inHBV-ACLF patients than in either the CHBV patients or theHCs, indicating the development of increased memory γδ Tcells. This finding could suggest γδ T cells have the poten-tial to recognize HBV-related or bystander antigens andproduce a quick and robust immune response.
Furthermore, the production of different types of cyto-kines might promote the varied immunofunction of γδ Tcells; therefore, it was very important to determine theintracellular cytokine expression profile of γδ T cells inHBV-ACLF patients. After stimulation with PMA and ion-omycin, the γδ T cells in HBV-ACLF displayed robustproduction of IFN-γ, TNF-α, and IL-17. The dramaticallyincreased proportion of inflammatory cytokine-secreting γδT cells might result in the development of a high level ofserum inflammatory cytokines in HBV-ACLF patients. Ad-ditionally, in HBV-ACLF patients, the intracellular expres-sion of granzyme B and CD107a in γδ T cells wassignificantly higher than in CHBV patients or HCs. There-fore, these results demonstrated increased cytotoxic poten-tial of γδ T cells in HBV-ACLF. Some other studies alsoindicated that the cytotoxicity activity of γδ T cells wasimproved in salmonella infections or other infection dis-eases [17–21]. In our study, IFN-γ, TNF-α, or IL-17 cyto-kine production was determined in both the αβ T-cells andthe γδ T cells in some HBV-ACLF patients, and the resultssuggested that the γδ T cells were more powerful in cyto-kine production than αβ T-cells (Supplementary Figure 2) .
As we know, lymphocytes infiltration and proinflamma-tory cytokine release are also the key steps in AIH [22]. To
learn about whether there were any similar changes in theproportion of γδ T cells in AIH as in HBV−ACLF, wefurther investigated the proportion of γδ T cells or thecytokine-producing γδ T cells in the AIH patients. Andsome different changes were indicated in our results, whichshowed a lower percentage of IFN-γ+γδ T and a higherpercentage of total γδ T, TNF-α+, or IL-17+ γδ T cells inAIH patients than that in HBV-ACLF patients. These resultsmight reveal the different role of different cytokine in thedevelopment of ACLF or AIH.
Finally, the relationship between the distinct character-istics of γδ T cells and measurable clinical parameters orother immune cells was also examined. There was a positivecorrelation between the percent of NKT cells and total γδ Tor IL-17+ γδ T cells, and between the proportion of NK cellsand CD45RO+ γδ T cells, indicating a potential, similar rolefor NK, NKT, or γδ T cells in the development of HBV-ACLF. Notably, there was a negative correlation betweenthe clinical parameter and the percent of γδ T cells, includ-ing the correlation between the percent of TNF-α+ γδ Tcells and the ALT or AST level, and between the percent ofCD107a+ γδ T cells and TBiL or DBiL levels. These resultsindicated that γδ T cells might accumulate in the liver andparticipate in the process of liver injury, and then becomeexhausted.
Collectively, our results demonstrate that, in HBV-ACLFpatients, γδ T cells produce significant levels of inflamma-tory cytokines and are cytotoxic. A number of these char-acteristics were also positively correlated with NK or NKTcells, but negatively correlated with the liver function.There, these results highlight the possible role of γδ T cellsin the development of high serum levels of inflammatorycytokines and/or the exacerbated liver injury associated withHBV-ACLF.
Acknowledgment We thank all the patients or healthy donors en-rolled in this study for their kindly understanding and supporting. Wealso thank the faculty of the department of infectious disease whocontribute to subjects screening and blood sample collection. Thisstudy is supported by the National Natural Science Foundation ofChina (30901264, 30930082), the National Science and Technologymajor Project of China (No.2008ZX10002-006), National Grand Pro-gram on Key Infectious Disease (2007CB512900), the Program forChangjiang Scholars and Innovative Research Team in University (No.IRT08720), Medical Science Foundation Project of Health Bureau ofChongqing Province (2011-2-152), and Natural Science FoundationProject of CQ CSTC (2009BB5264).
References
1. Liang TJ. Hepatitis B: the virus and disease. Hepatology. 2009;49(5 Suppl):S13–21.
2. Liaw YF, Chu CM. Hepatitis B virus infection. Lancet. 2009;373(9663):582–92.
884 J Clin Immunol (2012) 32:877–885

3. Di Bisceglie AM. Hepatitis B and hepatocellular carcinoma. Hep-atology. 2009;49(5 Suppl):S56–60.
4. Wu Z, Han M, Chen T, Yan W, Ning Q. Acute liver failure:mechanisms of immune-mediated liver injury. Liver Int. 2010;30(6):782–94.
5. Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, etal. Acute-on-chronic liver failure: consensus recommendations ofthe Asian Pacific Association for the study of the liver (APASL).Hepatol Int. 2009;3(1):269–82.
6. Zhai S, Zhang L, Dang S, Yu Y, Zhao Z, Zhao W, et al. The ratio ofTh-17 to Treg cells is associated with survival of patients withacute-on-chronic hepatitis B liver failure. Viral Immunol. 2011;24(4):303–10.
7. Shi F, Zhang JY, Zeng Z, Tien P, Wang FS. Skewed ratios betweenCD3(+) T cells and monocytes are associated with poor prognosisin patients with HBV-related acute-on-chronic liver failure. BiochemBiophys Res Commun. 2010;402(1):30–6.
8. Zhang JY, Zhang Z, Lin F, Zou ZS, Xu RN, Jin L, et al.Interleukin-17-producing CD4(+) T cells increase with severityof liver damage in patients with chronic hepatitis B. Hepatology.2010;51(1):81–91.
9. Zhang Z, Zou ZS, Fu JL, Cai L, Jin L, Liu YJ, et al. Severedendritic cell perturbation is actively involved in the pathogenesisof acute-on-chronic hepatitis B liver failure. J Hepatol. 2008;49(3):396–406.
10. Zou Z, Li B, Xu D, Zhang Z, Zhao JM, Zhou G, et al. Imbalancedintrahepatic cytokine expression of interferon-gamma, tumor ne-crosis factor-alpha, and interleukin-10 in patients with acute-on-chronic liver failure associated with hepatitis B virus infection. JClin Gastroenterol. 2009;43(2):182–90.
11. Bonneville M, O’Brien RL, Born WK. Gammadelta T cell effectorfunctions: a blend of innate programming and acquired plasticity.Nat Rev Immunol. 2010;10(7):467–78.
12. Born WK, Yin Z, Hahn YS, Sun D, O’Brien RL. Analysis ofgamma delta T cell functions in the mouse. J Immunol. 2010;184(8):4055–61.
13. Casetti R, Martino A. The plasticity of gamma delta T cells: innateimmunity, antigen presentation and new immunotherapy. Cell MolImmunol. 2008;5(3):161–70.
14. Ajuebor MN, Jin Y, Gremillion GL, Strieter RM, Chen Q,Adegboyega PA. GammadeltaT cells initiate acute inflammation andinjury in adenovirus-infected liver via cytokine-chemokine cross talk.J Virol. 2008;82(19):9564–76.
15. Barcy S, De Rosa SC, Vieira J, Diem K, Ikoma M, Casper C, et al.Gamma delta+T cells involvement in viral immune control ofchronic human herpesvirus 8 infection. J Immunol. 2008;180(5):3417–25.
16. Dandekar AA, O’Malley K, Perlman S. Important roles for gammainterferon and NKG2D in gammadelta T-cell-induced demyelin-ation in T-cell receptor beta-deficient mice infected with a corona-virus. J Virol. 2005;79(15):9388–96.
17. Tseng CT, Miskovsky E, Houghton M, Klimpel GR. Characteriza-tion of liver T cell receptor gammadelta T cells obtained fromindividuals chronically infected with hepatitis C virus (HCV):evidence for these T cells playing a role in the liver pathologyassociated with HCV infection [J]. Hepatology. 2001;33(5):1312–20.
18. Chen M, Zhang D, Zhen W, Shi Q, Liu Y, Ling N, et al. Character-istics of circulating T cell receptor gamma-delta T cells fromindividuals chronically infected with hepatitis B virus (HBV): anassociation between V(delta)2 subtype and chronic HBV infection.J Infect Dis. 2008;198(11):1643–50.
19. Silva-Santos B. γδ cells making IL-17. Blood. 2011;118(1):3–5.20. Berndt A, Pieper J, Methner U. Circulating gamma delta T cells in
response to Salmonella enterica serovar enteritidis exposure inchickens. Infect Immun. 2006;74(7):3967–78.
21. Jonasson R, Andersson M, Råsbäck T, Johannisson A, Jensen-Waern M. Immunological alterations during the clinical and recov-ery phases of experimental swine dysentery. J Med Microbiol.2006;55(Pt 7):845–55.
22. Mieli-Vergani G, Vergani D. Autoimmune hepatitis. Nat Rev Gas-troenterol Hepatol. 2011;8(6):320–9.
J Clin Immunol (2012) 32:877–885 885