Myocardial NF-κB activation is essential for zebrafish heart ...

University of LjubljanaFaculty of Mathematics and Physics
Physics department
Seminar 1b-1. year, II. cycle program
Electrodynamics
of
human heart
author: Bor Kavcic
supervisor: prof. dr. Rudolf Podgornik
Ljubljana, May 31, 2013
Abstract
In this seminar we focus on heart electrodynamics. Firstly, some essential anatomy and physiol-ogy are presented. Based on latter we describe clinical approach to measuring electrical propertiesof heart with ECG – this section is based on basic electrodynamics. After this brief presentationsome biophysical models of activation potential formation and propagation are derived. Last sec-tion presents numerical simulations of heart contraction; section is based on research of BarcelonaSupercomputer Center project, named Alya Red.

Seminar I May 31, 2013
Contents
1 Introduction 3
2 Heart anatomy 3
3 Physiology of heart 4
4 Scalar and vector electrocardiogram 6
4.1 Interpretation of ECG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
5 Cardiac cells 9
5.1 Purkinje fiber . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95.2 One-dimensional fibers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
6 Numerical simulations 11
6.1 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
7 Conclusion 14
2


Seminar I May 31, 2013
thoracic cavity. Between both layers is pericardial fluid, which enables smooth heart movement. Innerpericardium layer is called epicardium and it is outer layer of heart wall. Middle, thick muscular layeris called myocardium; it is syncytium of cardiac muscle cells. Heart contraction is synchronized withelectric pulses from sinoatrial node (SA node), which is located just below superior vena cava on theright atrium [1]. Electrical pulse is propagated through the atria by the atrial cells. Because septumcells are not excitable, the barrier is bridged with bundle of His-a fiberish tissue shown on fig. 1b. Itoriginate from atrioventricular node (AV node) and continues to collection of fiber, called Purkinje fibers.Mentioned AV and SA node and fiber network (with some additional non mentioned bundles) are shownon fig. 1b.
3 Physiology of heart
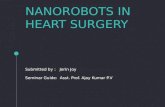
In this section physiology and cardiac cycle itself are presented, based on [1, 4]. Firstly, we name differentstages of cardiac cycle with its successive steps and properties of each – see tab. 1. It is important tounderstand exact sequence in cycle, because every step is electrically synchronized. Stages of cardiaccycle are schematically shown on fig. 2.
Figure 2: Block diagram of macroscopic steps. In the first step of the process, activation potential propagatesthrough tissue, causing muscle tissue (myocytes) to contract. Ventricle shrinkage is then manifested by pressurechange, causing blood to flow, Ref. [5].
Steps in cardiac cycle
Name AV valves Semilunar valves Properties
I. Early diastole open closed− whole heart is relaxed,− ventricles are expanding and fill-
ing.
II. Atrial systole open closed− atria contract and pump blood,− additional 10-40% filling of ven-
tricles.
III. Isovolumic ventricularcontraction
closed closed− ventricular myocytes begin to
contract,− ventricular volume unchanged.
IV. Ventricular ejection closed open− ventricles fully contract,− pump blood to the rest of the
body.
V. Isovolumic ventricularrelaxation
open closed− ventricles relax,− ventricle volume unchanged,− atria expand and are filling.
Table 1: Successive steps of cardiac cycle.
4


Seminar I May 31, 2013
4 Scalar and vector electrocardiogram
Electrocardiogram (ECG) is a diagnostic tool which allows physicians to evaluate the heart function.First cardiogram was made at the end of 19th century by A. Muirhead. Action potential of the heartgenerates an electrical potential field that can be measured on the body surface.
The body is a volume conductor – during action potential spread, current spread throughout thebody.
One can get more information about time development of the action potential, if multiple leads areused – this is called vector ECG. Assuming body is ohmic, basic electrodynamics gives us:
I = −σ∇φ, (1)
where σ denotes conductivity tensor. It is inhomogeneous (because body itself is inhomogeneous) andanisotropic (fiber nature of some tissues, eg. muscle fibre, neural system). Continuity equation andconservation of current gives us:
∇ · I = −∇ · (σ∇φ) = S. (2)
In equation S denotes all currents sources. The spreading action potential is well approximated as asurface of current dipoles (the current source and sink together form the dipole). In principle, if strengthand location (ie. distribution) of current dipoles and conductivity tensor for whole body were known,one could solve Poisson eq. (2). Described problem is known as forward problem of electrocardiography,and it is still unsolved.
Physicians are usually interested in inverse problem – by knowing surface potential, they would like todetermine sources. This problem is also unsolved and it is called inverse problem of electrocardiography.Inverse problem is mathematically unstable – let us demonstrate with an example. If one observes pointcharge, caused potential obeys ϕ = e/4πε0r. On the distance, greater than its radius, homogeneously(isotropic is enough) charged sphere gives the same law, if its charge is
∫
ρdV = e. We cannot determinesource distribution from knowing surface potential.
Due to complexity of the problem, simplifications are in order. One could define heart electric dipolevector
H(t) =
∫
V
JdV, (3)
where J represents electric dipole density at each point of the heart and V denotes heart volume. Anothersimplification is assuming body is homogeneous conductor and infinitely bigger than the heart. Electricdipole potential [8] at any point can be written as:
φ(r, t) =H(t) · r
4πε0r3. (4)
Therefore, one needs three measurements to determine electric heart dipole vector H – we must em-phasize that one must not confuse it with magnetic field strength which has same symbol in standardelectromagnetism. We define so called lead vectors lr as:
lr =r
4πε0r3hence φ(r, t)s = lr ·H(t). (5)
We can assume, that lr has the same direction as a vector from the heart to the point where recording ismade. As previously said, three ECG leads would suffice to determine heart dipole vector. Nonetheless,additional leads give better information – interesting enough, measurement with three electrodes givesa result within 85% of whole information.
It is also important to emphasize the fact that potential is screened. Our body is mostly made ofwater in which many ions are dissociated. Screening will not be discussed in this seminar.
Every procedure in medicine is standardized; cardiologists use twelve leads. The first three weresettled by Einthoven and are still used today: left arm (LA), right arm (RA) and left leg (LL). Becausefield is invariant for constant change in potential [8], one cannot measure absolute potential – onlydifference between pairs of leads. We define:
VI = φLA − φRA, (6a)
VII = φLL − φRA, (6b)
VIII = φLL − φLA. (6c)
6

Seminar I May 31, 2013
Because∮
φ = 0, we know that VI +VIII = VII. One can define three lead vector with: Lj = lj ·H whereVj = |Lj | for j = I, II and III.
Figure 4: Einthoven triangle with associated lead vectors. Ref. [1]
Vector ECG is actually time-varying vector loop, which can be seen on fig. 5. Because lead voltage isa dot product of two vectors, a change in amplitude suggests either a change in amplitude of the heartvector or a change in direction of the heart vector.
Figure 5: Loop of heart dipole vector. Ref. [1]
4.1 Interpretation of ECG
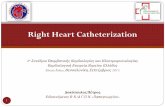
Let us connect physiological differences in heart tissue with ECG recording. Potential differences areobserved whenever the current sources are sufficiently strong. Figure 6 shows three such events. Firstevent, denoted as P wave is a measurement of action potential spreading through the atria. Next event is
Figure 6: Cellular transmembrane potential – upper figure – and ECG signal. Ref. [1]
7

Seminar I May 31, 2013
called QRS complex and is the most prominent of all; action potential is propagating through ventricles.The recovery (or repolarization) of ventricles is seen as T wave. Recovery of atria is to weak to be seenon ECG; SA node firing, AV nodal conduction and Purkinje fiber propagation are also not detected byECG due to insufficient tissue mass and small extracellular currents.
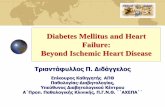
Scalar ECG is fundamental tool for detection of rhythm abnormalities, such as different arrhythmias(also called dysrhythmias). If there are multiple P waves, clinician can diagnose atrial flutter, shownon fig. 7a. In the case of atrial flutter, there is still some periodicity in QRS complex. If there is lessperiodicity, cardiologist can suspect atrial fibrillation, seen on fig. 7b. Rapid repetition of QRS complexes
(a)
(b)
Figure 7: Figures show two different dysrhythmias; fig. (a) shows atrial flutter pattern – multiple P wavesare easily seen. Figure (b) shows pattern connected with atrial fibrilation – there is high irregularity in QRScomplexes Ref. [11]
is ventricular tachycardia, fig. 8a, highly irregular pattern of ventricular activation is called ventricular
fibrillation, seen on fig. 8b. Broadening of the QRS complex suggests slower propagation than normal –
(a)
(b)
Figure 8: Figures show ECG recording of two different ventricular arrhythmias. Figure (a) shows ventriculartachychardia, fig. (b) shows ventricular fibrillation. Ref. [11]
conduction failure in the Purkinje network is suspected. Extra deflections correspond to extrasystoles,arising from sources other than the SA or AV nodes.
Vector ECG is even more informative. Amplitude of QRS complex reflects the amount of musclemass involved in propagation. If it is extraordinary large, ventricular hypertrophy is suspected. This isa condition where ventricles’ walls are thicker than usual. Direction of dipole vector can tell us whichventricle is affected – eg. if ECG vector is leftward form normal, it suggests left ventricular hypertrophy.If an amplitude decrease is accompanied by rightward change in orientation, a diagnosis of myocardial
infarction in the left ventricle is suggested; if oriented leftward, right ventricle myocardial infarction issuspected. Heart vector is deflected away from the location of infarction. Search for dysrhythmias is alsopossible with Fourier analysis – for further reading article [12] is advised.
8


Seminar I May 31, 2013
Differential equations for m(t), n(t) and h(t) have the form:
dw
dt= αw(1− w)− βww, (12)
where w = m,n, h. αw and βw take form of:
αw, βw =C1 exp
(
V−V0
C2
)
+ C3(V − V0)
1 + C4 exp(
V−V0
C5
) (13)
Constants Ci and V0 are determined numerically, based on measurements of Purkinje fiber potential.Their values are shown in tab. 2. Even though Noble model is inaccurate it reproduces same shape
C1 C2 [mV] C3 [mV−1] C4 C5 V0[mV]αm 0 - 0.1 -1 -15 -48βm 0 - -0.12 -1 5 -8αh 0.17 -20 0 0 - -90βh 1 ∞ 0 1 -10 -42αn 0 - 0.0001 -1 -10 -50βn 0.002 -80 0 0 - -90
Table 2: Numerical values of constants in eq. (13) for Noble model.
as measured action potential in Purkinje fiber tissue as shown on fig. 10. Again, we must emphasizephysiological inaccuracy of Noble model – its concept is important because of its generality.
Figure 10: Potential for described Noble model. Ref. [1]
5.2 One-dimensional fibers
One can model [1] cardiac fiber by considering simple one-dimensional collection of cylindrical cells ofperimeter p, coupled in end-to-end fashion via gap junctions, seen on fig. 3b. Relying on [19] propagationin each cell is described by cable equation:
p
(
Cm∂V
∂t+ Iion
)
=∂
∂x
(
1
rc
∂Vi
∂x
)
= −∂
∂x
(
1
re
∂Ve
∂x
)
, (14)
with rc =Rc
Aiand re = Re
Ae, where Rc and Re are resistivities of intracellular and extracellular space, Ai
and Ae are the average cellular and extracellular cross-sectional areas. Each cell’s length is L; at theend of the cell, there is a jump in intracellular potential, intracellular current − 1
rc∂Vi
∂x on the other handmust be continuous. Assuming that gap junctions are ohmic resistors, the drop in the potential acrossthe junction is proportional to the through the junction:
[Vi]
rg=
1
rc
∂Vi
∂x, (15)
10

Seminar I May 31, 2013
where [Vi] denotes the jump in intracellular potential and rg is effective gap-junctional resistance. Weassume that there is no transmembrane currents across the ends of the cell into the small extracellulargap that separates the cells. The extracellular potential and currents are continuous, unaffected by thegap junctions.
One can find steady-state solution of this problem analytically. Ionic current Iion = V/Rm = (Vi −Ve)/Rm, where Rm is transmembrane resistance per unit area. We look for geometrically decayingsolution:
Vξ(x+ L) = µVξ(x) where ξ = i, e and µ < 1. (16)
Space constant λg relates to µ through µ = e−L/λg . Steady-state solution is:
(
Vi
Ve
)
n
= µn
(
φi
φe
)
. (17)
Further we assume that total current is zero:
1
rc
∂φi
∂x+
1
rc
∂φe
∂x= 0 (18)
Combining eq. (14) and eq. (18) and defining φ = φi − φe we get:
φ = α1 exp(λx) + α2 exp(−λx), (19)
where λ2 = pRm
(rc + re) and
φi =rc
rc + reφ+ β and φe = −
rerc + re
φ+ β. (20)
To determine all unknown constants we need four equations – boundary conditions are continuity ofcurrent
φ′
e(L) = µφ′
e(0) φ′
i(L) = µφ′
i(0) (21)
and requiring continuity of extracellular potential and jump condition for intracellular potential:
φe(L) = µφe(0) and µφi(0)− φi(L) =rgrc
φ′
i(L). (22)
Constants are determined numerically
α1 = µ−1
E, (23a)
α2 = µ− E, (23b)
β = 2re(µ− E)(µ− 1
E )
µ− 1, (23c)
where E = eλL. Constant µ < 1 is a root of characteristic equation
rgλ
rc + re=
Rg
λL= 2
(µ− 1
E )(µ− E)
µ(E − 1
E ). (24)
Solution for experimentally gathered data is shown on fig. 11.
6 Numerical simulations
Previous sections demonstrated complexity of heart physiology. One can easily see that numerical sim-ulations of heart requires powerful cluster computers and smart algorithms. Secondly, one must providesufficiently detailed data about heart tissue (eg. fiber directions, density, ionic concentration, etc.). Phys-iologically accurate models must be used to be as close to reality as possible. In this section simulationand results of project Alya Red of Barcelona Supercomputing Center (BSC) are briefly presented [21].
11


Seminar I May 31, 2013
6.1 Results
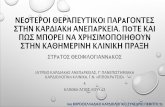
One must simulate potential propagation sufficiently accurate. Taking models, analog to ones previouslydescribed is sec. 5, BSC calculations gave potential propagation shown on fig. 13. Nondescribed mod-els and additional measurements gave 8 ms delay between passing of potential wavefront and musclecontraction. Further measurements were made during research to characterize mechanical properties ofmuscle tissue. Taking everything into account, whole heart beat can be simulated.
Figure 13: Time evolution of activation potential. One can easily spot SA node firing initial signal, followed byanother stimuli, which fires with 30 ms delay. Shown simulation results have a resolution of 0.2-0.15 mm, whichis comparable with medical images nowadays. Figure shows six time-equidistant frames, time interval is 2000 ms.Simulation was calculated on 500 cores and computation time was approximately 15 minutes. Ref: [21].
At current moment, hydrodynamics is not taken into account. When so, simulation would make an-other step closer to reality – eg. pathologies connected with malfunction of heart valves could be studied.Successive beat steps are best seen on video [25]; some of them are shown on fig. 14. Idea behind simu-
(a) (b)
(c) (d)
Figure 14: Figures show four different stages of heart beat – it is easily seen how different sections of the heartcontract at different times. Ref. [25].
lations is to gather knowledge about different sources of pathologies of heart diseases, which is essentialfor further development of new clinical technics and pharmaceutical drugs. When normal beating is es-
13

Seminar I May 31, 2013
tablished, research can focus on inducing malformations on different segments of physiology: conductingerrors, insufficient contraction, etc.
7 Conclusion
In seminar various aspects of heart electrodynamics were presented. Brief walkthrough physiology andanatomy set foundation for later discussion. We have shown that ionic currents are cornerstone of po-tential formation. Potential modeling is based on systems of non-linear differential equations. Numericalsolving is computer based, which takes out the beauty of analytical results. One-dimensional propa-gation is a limiting case for a “paper-solving”. Nonetheless, models are sufficiently accurate for nextphase: whole heart beat simulation. Latter is presented in sec. 6. Simulations are currently at testingand parameter setting phase. Preliminary results shows excellent matching between simulations andactual (normal) heart beat. Once the normal heart beat is fully understood, researchers could proceedto study of pathologies.
References
[1] J. Keener and J. Sneyd, Mathematical Physiology, II: System Physiology, (Springer, New York, 2009).
[2] http://www.texasheartinstitute.org/HIC/Anatomy/anatomy2.cfm, (reachable May 31, 2013)
[3] http://en.wikipedia.org/wiki/Sinoatrial_node, (reachable May 31, 2013).
[4] A. C. Guyton and J. E. Hall, Textbook of Medical Physiology, 12th edition, (Saunders Elsevier, Philadelphia, 2006).
[5] P. Lafortune, R. Arıs, M. Vazquez and G. Houzeaux, Int. J. Numer. Meth. Biomed. Engng. 28, 72 (2012).
[6] http://histologyolm.stevegallik.org/node/146, (reachable May 31, 2013).
[7] http://medicinembbs.blogspot.com/2011/02/heart-musclesas-pump-and-functions-of.html, (reachable May 31,2013).
[8] R. Podgornik and A. Vilfan, Elektromagnetno polje, (DMFA zaloznistvo, Ljubljana, 2012)
[9] http://geekymedics.com/2011/03/05/understanding-an-ecg/, (reachable May 31, 2013)
[10] http://studentnursediaries.wordpress.com/2011/06/08/the-ecg-made-even-easier/, (reachable May 31, 2013)
[11] http://www.learnekgs.com/, (reachable May 31, 2013).
[12] H. Gothwal, S. Kedawat and R. Kumar, J. Biomedical Sc. and Eng. 4, 289 (2011).
[13] A. L. Hodgkin and A. F. Huxley, Journal of physiology 117, 500 (1952).
[14] http://en.wikipedia.org/wiki/Current_source, (reachable May 31, 2013).
[15] http://en.wikipedia.org/wiki/Hodgkin%E2%80%93Huxley_model, (reachable May 31, 2013).
[16] http://en.wikipedia.org/wiki/Reversal_potential, (reachable May 31, 2013).
[17] Noble D., Journal of Physiology 160, 317 (1962).
[18] R. E. McAllister, D. Noble and R. W, Tsien, Journal of Physiology 251, 1 (1975).
[19] J. Keener and J. Sneyd, Mathematical Physiology, I: Cellular Physiology, (Springer, New York, 2009).
[20] http://en.wikipedia.org/wiki/Diffusion, (reachable May 31, 2013).
[21] M. Vazquez, R. Arıs, G. Houzeaux, R. Aubry, P. Villar J. Garcia-Barnes, D. Gil and F. Carreras, Int. J. Numer. Meth.Biomed. Engng. 27, 1911 (2011).
[22] http://bradyonthebrain.wordpress.com/tag/dan-siegel/, (reachable May 31, 2013).
[23] http://yoshihitoyagi.com/projects/MasterProject/dti/, (reachable May 31, 2013).
[24] http://getbetterhealth.com/tag/diffusion-tensor-imaging, (reachable May 31, 2013).
[25] http://www.bsc.es/computer-applications/alya-red-ccm, (reachable May 31, 2013).
14