Effects of the Opiate Antagonist, Naltrexone, on Binging Antecedents and Plasma β-Endorphin...
5
CASE STUDY Effects of the Opiate Antagonist, N altrexone, on Binging Antecedents and Plasma Concentrations IRENE CHATOOR, M.D., BARBARA H. HERMAN, PH.D., AND JENNIFER HARTZLER, B.S. ABSTRACT The effects of the opiate receptor antagonist, naltrexone, were examined on antecedent thoughts of binging and plasma concentrations in an adolescent girl who was hospitalized with bulimia nervosa. Significant decreases in urge to binge were obtained during naltrexone administration compared with control sessions. Baseline plasma concentrations for the bulimic adolescent were not different from those of nonbulimic controls, but plasma increased significantly during naltrexone administration. After discharge from the hospital, the adolescent refused to take naltrexone because she felt she could not deal with her life without the "pleasure of binging." The case points to the interplay of biological and psychological factors in bulimia nervosa. J. Am. Acad. Child Ado/esc. Psychiatry, 1994, 33, 5:748-752. Key Words: naltrexone, binging antecedents, bulimia nervosa, Individuals with bulimia nervosa frequently report a lack of control over their eating behavior, and the compulsive nature of these binge-purge cycles appears to share some similarity with drug addiction. Although various psychosocial factors have been implicated in the etiology of this disorder, there is also the possibility of an underlying biological vulnerability. Specifically, it has been postulated that the opioid system may be involved in the compulsive nature of binging and purging and the loss of control over food Gonas and Gold, 1987; Waller et al., 1986). It has been hypothesized that bulimics have lower levels and may binge and purge to achieve an increase in the release of opioids in the brain that might in turn produce a reduction of anxiety and result Accepted September 15, 1993. Dr. Chatoor is Psychiatric Director, Eating Disorders and Infant Psychiatry Program, Children's National Medical Center (CNMC), Washington, DC, and Associate Professor ofPsychiatry and Behavioral Sciences and ofPediatrics, George Washington University School of Medicine. Dr. Herman is Director, Clinical Opioid Programs, Clinical Trials Branch, Medication Development Division, National Imtitute on Drug Abuse, National Imtitutes of Health, and Senior Science Fellow, Brain Research Center, CNMC, and Associate Research Professor of Pediatrics, George Washington University School of Medicine. Jennifer Hartzler was Research Assistant, Brain Research Center, CNMC. Reprint requests to Dr. Chatoor, Department of Psychiatry, Children's National Medical Center, 111 Michigan Avenue, NW, Washington, DC 20010. 0890-8567/94/3305-0748$03.00/0©1994 by the American Academy of Child and Adolescent Psychiatry. 748 in pleasurable feelings. Consistent with this hypothesis, Waller et al. (1986) reported that bulimics had signifi- cantly lower plasma concentrations than did controls, and Brewerton et al. (1992) found that women with bulimia had significantly lower CSF con- centrations than did the female compar- ison subjects. Fullerton et al. (1988) reported that only when bulimics had vomited were their plasma concentrations of immunoreactive l3-endorphins higher than those of normal controls. There is also evidence that the potent opioid receptor antagonist, naltrexone, may decrease the binges and purges in individuals with bulimia nervosa. In open- trial investigations Jonas and Gold (1987) examined the effects of naltrexone (300 mg daily for 6 weeks) on 20 individuals with antidepressant-resistant bulimia nervosa. Thirteen subjects were treated with naltrexone alone and seven subjects were treated with naltrexone and antidepressant. In the former group, 10 experienced at least a 75% reduction of binging and purging. The seven subjects treated with naltrexone plus antidepres- sant were similar to those treated with naltrexone alone. In a follow-up study (also open-tria!), Jonas and Gold (1988) compared the effectiveness of low doses of naltrexone (50 to 100 mg) to that of high doses of naltrexone (200 to 300 mg) administered daily for 6 weeks in 16 bulimic individuals. Only individuals in the high-dose group showed significant decreases in J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 33:5, JUNE 1994
Transcript of Effects of the Opiate Antagonist, Naltrexone, on Binging Antecedents and Plasma β-Endorphin...

CASE STUDY
Effects of the Opiate Antagonist, N altrexone, on BingingAntecedents and Plasma ~-Endorphin Concentrations
IRENE CHATOOR, M.D., BARBARA H. HERMAN, PH.D., AND JENNIFER HARTZLER, B.S.
ABSTRACT
The effects of the opiate receptor antagonist, naltrexone, were examined on antecedent thoughts of binging and plasma
~·endorphin concentrations in an adolescent girl who was hospitalized with bulimia nervosa. Significant decreases in urge
to binge were obtained during naltrexone administration compared with control sessions. Baseline plasma ~-endorphin
concentrations for the bulimic adolescent were not different from those of nonbulimic controls, but plasma ~·endorphins
increased significantly during naltrexone administration. After discharge from the hospital, the adolescent refused to
take naltrexone because she felt she could not deal with her life without the "pleasure of binging." The case points to
the interplay of biological and psychological factors in bulimia nervosa. J. Am. Acad. Child Ado/esc. Psychiatry, 1994,
33, 5:748-752. Key Words: naltrexone, binging antecedents, bulimia nervosa, ~·endorphin.
Individuals with bulimia nervosa frequently report alack of control over their eating behavior, and thecompulsive nature of these binge-purge cycles appearsto share some similarity with drug addiction. Althoughvarious psychosocial factors have been implicated inthe etiology of this disorder, there is also the possibilityof an underlying biological vulnerability.
Specifically, it has been postulated that the opioidsystem may be involved in the compulsive nature ofbinging and purging and the loss of control over foodGonas and Gold, 1987; Waller et al., 1986). It hasbeen hypothesized that bulimics have lower~-endorphin levels and may binge and purge to achievean increase in the release of opioids in the brain thatmight in turn produce a reduction ofanxiety and result
Accepted September 15, 1993.Dr. Chatoor is Psychiatric Director, Eating Disorders and Infant Psychiatry
Program, Children's National Medical Center (CNMC), Washington, DC,and Associate Professor ofPsychiatry and Behavioral Sciences and ofPediatrics,George Washington University School ofMedicine. Dr. Herman is Director,Clinical Opioid Programs, Clinical Trials Branch, Medication DevelopmentDivision, National Imtitute on Drug Abuse, National Imtitutes of Health,and Senior Science Fellow, Brain Research Center, CNMC, and AssociateResearch Professor of Pediatrics, George Washington University School ofMedicine. Jennifer Hartzler was Research Assistant, Brain Research Center,CNMC.
Reprint requests to Dr. Chatoor, Department of Psychiatry, Children'sNational Medical Center, 111 Michigan Avenue, NW, Washington, DC20010.
0890-8567/94/3305-0748$03.00/0©1994 by the American Academyof Child and Adolescent Psychiatry.
748
in pleasurable feelings. Consistent with this hypothesis,Waller et al. (1986) reported that bulimics had significantly lower plasma ~-endorphin concentrations thandid controls, and Brewerton et al. (1992) found thatwomen with bulimia had significantly lower CSF concentrations of~-endorphin than did the female comparison subjects. Fullerton et al. (1988) reported thatonly when bulimics had vomited were their plasmaconcentrations of immunoreactive l3-endorphins higherthan those of normal controls.
There is also evidence that the potent opioid receptorantagonist, naltrexone, may decrease the binges andpurges in individuals with bulimia nervosa. In opentrial investigations Jonas and Gold (1987) examinedthe effects of naltrexone (300 mg daily for 6 weeks)on 20 individuals with antidepressant-resistant bulimianervosa. Thirteen subjects were treated with naltrexonealone and seven subjects were treated with naltrexoneand antidepressant. In the former group, 10 experiencedat least a 75% reduction of binging and purging. Theseven subjects treated with naltrexone plus antidepressant were similar to those treated with naltrexone alone.In a follow-up study (also open-tria!), Jonas and Gold(1988) compared the effectiveness of low doses ofnaltrexone (50 to 100 mg) to that of high doses ofnaltrexone (200 to 300 mg) administered daily for 6weeks in 16 bulimic individuals. Only individuals inthe high-dose group showed significant decreases in
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 33:5, JUNE 1994

binge eating or purging with naltrexone. Mitchell andcoworkers (1989) failed to find significant reductionsin binge eating or vomiting episodes in 16 normalweight bulimic women when they were treated witha low dose of naltrexone (50 mg daily for 3 weeks).In summary, these studies with adult women suggestthat high doses of naltrexone may decrease binge eatingand purging, but additional dose-response studies areneeded to evaluate this suggestion.
In the present case of an adolescent girl with bulimianervosa, we examined whether naltrexone might affectantecedent thoughts of binging and whether this effectwas dose-related. In addition, the effects of naltrexoneon plasma concentrations of ~-endorphinwere examined. Here we wanted to determine whether opiatereceptor antagonism would increase plasma~-endorphin concentrations of a bulimic individual ashas been reported to occur for normal controls (Kostenet aI., 1986).
METHOD
Subjects
The bulimic subject (S.B.) was a 15-year-old girl of normalweight (55 kg, 1.65 m, body mass index = 20) who was initiallyreferred for evaluation because of shoplifting and truancy fromschool. During the diagnostic interview S.B. admitted to bingeeating and purging, and was diagnosed as bulimic using DSMIII-R (American Psychiatric Association, 1987) criteria. She had astrong history of depression, obesity, alcohol, and drug abuse infirst- and second-degree relatives on both sides of the family. Shereported a striking preoccupation with sweets and an inabiliry tostop eating them once she started. In addition, she admitted tobeing unable to stop once she statted to dtink alcohol.
S.B. was hospitalized for bulimia nervosa. During the firsthospitalization, because of a concomitant major depressive episode,she statted imipramine therapy (150 mg daily) and a protocol ofregulated eating for 4 weeks. S.B. responded well to this treatment.Mter discharge from the hospital, she completely avoided eatinganything sweet and remained free of bulimic symptoms for 6months. However, after this period, during a time of intense familystress, S.B. statted the most severe binge-purge cycles in herhistory in which she would engage in several binge episodes whileconsuming 60 laxatives daily. Because of her severe condition andthe lack of response to outpatient treatment, including individualpsychotherapy, family therapy, and increasing dosages of imipramine, S.B. was hospitalized for a second time during which theeffects of naltrexone were evaluated. On admission, imipraminewas discontinued because S.B. insisted it did not help her preoccupation with binging, which she considered to be her major problem.During the hospitalization, S.B. received individual psychotherapy,family therapy, and group therapy with other eating disorderspatients and began a protocol of supervised eating designed forpatients with bulimia nervosa to prevent binging and purging and
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 33:5. JUNE 1994
EFFECTS OF NALTREXONE ON BINGING
to stabilize weight. On day 10 of the hospitalization, she startedthe naltrexone protocol.
In addition, six normal-weight female subjects, 16 to 19 yearsof age, were used as normal controls in this study. The controlstested in the nonbulimic range according to the results of theEating Attitudes Test (Garner et aI., 1982) and the Bulimia Test(Smith and Thelen, 1984).
Procedure
Because conventional treatments for bulimia nervosa had failedin S.B., it was decided that an experimental but promising treatmentsuch as naltrexone might be worthwhile. Accordingly, the proposeddesign was presented to an expedited Institutional Review Boardcommittee of the hospital and permission to do the study wasgranted. Because of three factors detailed below, an ascending doseresponse series was chosen to detect the effects of naltrexone.First, this is the design recommended by the Food and DrugAdministration for a Phase 1 study for testing a relatively newdrug in children and adolescents (see Herman, 1990, 1991; Hermanet aI., 1987, 1989b). Second, unlike naloxone, which has a relativelyshott half-life, the duration of naltrexone approaches 24 hoursafter moderate oral doses (Martin et aI., 1973). Naltrexone is apotent opioid receptor antagonist which, unlike naloxone, retainsmuch of its efficacy when administered by oral route (Martin et aI.,1973). Accordingly, a double-blind design in which doses wererandomly administered might have obscured drug effects due todrug carry-over into baseline or placebo trials. Third, since thehospitalization was limited to 1 month, the long half-life ofnaltrexone prohibited a randomly administered dose series of naltrexone and placebo.
A single-blind design (subject was blind to drug) was usedconsisting of 2 days of baseline, 2 days of placebo, 2 days eachof 0.5, 1.0, 1.5, and 2.0 mg/kg of naltrexone (doses from 25 to100 mg), followed by 2 days of placebo, and 2 days of baseline.The drug was given when the subject was in a fasted state at 7:00A.M. On the second test days, blood was obtained at 8:00 A.M.
followed by breakfast, i.e., blood samples were obtained 1 hourafter drug administration. Every evening (between 8:00 P.M. and10:00 P.M.) the subject filled out a rating scale describing thoughtsand feelings related to bulimia nervosa. The scale included aseparate item for urge to binge and for preoccupation with sweetswhich the subject rated as not at all (0), a little (1), pretry much(2), and very much (3). Separate ratings were assigned for themorning, afternoon, and evening. The final score for these twomeasures was obtained by summing values across the three dailysessions, with a minimum score of 0 and a maximum score of 9.A separate scale included urge to binge after eating sweets ratedas 0 (no) or 1 (yes). The sweets included two chocolate chipcookies given daily after lunch (between 12:00 noon and 12:30P.M.). The purpose of these scales was to evaluate possible differencesbetween placebo and naltrexone conditions. The validity for determining differences between bulimics and normal subjects hasnot yet been determined. The scales were collected the morningof the next day.
Blood was collected in vacutainer tubes for ~-endorphin (10mL in EDTA) and placed immediately on ice, and the plasmawas stored at -70°C until assay time. In addition, blood for liverfunction tests (glutamic-oxaloacetic transaminase and glutamicpyruvic transaminase) was drawn on a weekly basis. Plasma~-endorphin was measured by radioimmunoassay using kits obtained from ImmunoNuclear Corp. (Stillwater, MN). Details arepresented in Herman et al. (1988).
749

CHATOOR ET AL.
B.B., P, 15 y.o.
1
urge to binge after eating sweets. There was someevidence of a carryover effect of naltrexone, inasmuchas the urge to binge also did not occur during bothdays of postdrug placebo (P2) and day 1 of the postdrugbaseline (B2), which were, respectively, administered24, 48, and 72 hours after 2.0 mg/kg of naltrexone.
Data averaged over day 1 and day 2 appear to suggestthat preoccupation with sweets was also decreased bynaltrexone. Using predrug values as the control scores(Bl + PI, 4.75 ± 0.48), higher doses of naltrexone(1.5 mg/kg + 2 mg/kg, 1.25 ± 0.48) appeared todecrease preoccupation with sweets, although this comparison just failed to achieve a conventional level ofstatistical significance (t [3] = 2.94, P = .06). Althoughlow doses of naltrexone (0.5 mg/kg + 1.0 mg/kg,3.25 ± 0.86) appeared to decrease preoccupation withsweets, these effects were not significantly differentfrom predrug control values (p > .10). Once again,there was evidence of a carryover effect of naltrexone,inasmuch as postdrug control scores for preoccupationwith sweets (P2 + B2, 1.00 ± 1.00) were significantlylower than predrug control scores (Bl + PI, 4.75 ±0.86) (t [3] = 7.83, P < .005).
Baseline plasma ~-endorphin concentrations for S.B.(6.97 ± 0.47 pmol/L) were not significantly differentfrom those of six female, nonbulimic controls (6.36± 1.31 pmol/L) (t [8] = 0.36, P > 1.0). Plasma~-endorphin concentrations obtained at 0.5, 1.0, and1.5 mg/kg of naltrexone appeared to be higher thaneach of the other.four control values. Indeed, increasesup to 48% (about two standard deviations) from themean plasma control value were obtained at the 1.0and 1.5 mg/kg naltrexone doses.
DISCUSSION
This study demonstrated that the adolescent tolerated the administration of naltrexone without experiencing any side effects. Acute administration of thesame doses ofnaltrexone has not been found to produceany significant effects on cardiovascular or liver functionin autistic children and adolescents (Campbell et al.,1989; Herman et al., 1989a, 1993). The results of thestudy suggest that high doses of naltrexone (1.5 and2.0 mg/kg) significantly decreased antecedent thoughtsassociated with bulimia nervosa in this 15-year-oldbulimic girl. There also appeared to be a carryovereffect in the placebo condition which followed the
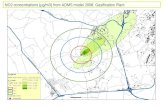
oL---JL-----l_---l_----L_---L--,-----L_....L._--'- _
B1 P1 0.5 1.0 1.5 2.0 P2 B2Naltrexone (mg/kgl
Fig. 1 Effects of baseline (Bl, B2), placebo (PI, P2), and naltrexone(0.5, 1.0, 1.5, and 2.0 mg/kg) on the urge to binge (summed over dailymorning, afternoon, and evening rating sessions) in a bulimic l5-year-oldgirl. Data are averaged across day 2 of baseline, placebo, and drugadministration.
Where possible, data were analyzed using Student's t tests (twotailed), and statistical significance was assumed if p < .05.
RESULTS
S.B. experienced no side effects while participatingin the study, and her liver function tests remainedwithin normal limits. There was no consistent effectof naltrexone on any of the feelings (sad, happy, angry,relaxed) rated by the subject. The following data (mean± SEM) are averaged across day 1 and 2 for each ofthe following conditions: baseline 1 (BO, placebo 1(PO, naltrexone doses (0.5, 1.0, 1.5, 2.0), baseline 2(B2), placebo 2 (P2).
There was no consistent effect of naltrexone on urgeto binge summed over day 1 by comparing controlscores (Bl + PI + B2 + P2, 2.25 ± 1.32) withnaltrexone scores (0.5 + 1.0 + 1.5 + 2.0 mg/kg, 2.05± 0.95) (t [3] = 0.42, P > .10) (data not shown). Bycomparison a significant naltrexone effect was obtainedon day 2 where urge to binge sum scores were significantly higher on control days (Bl + PI + B2 + P2,4.50 ± 0.50) than on naltrexone days (0.5 + 1.0 +
1.5 + 2.0 mg/kg, 1.50 ± 0.50) (t [3] = 3.67, P < .05)(Fig. 1).
The effects of naltrexone on urge to binge aftereating sweets (two cookies after lunch) were also tested.Using predrug values as the control group (Bl + PI,mean = 1.0), the higher doses of naltrexone (1.0, 1.5,and 2.0 mg/kg, mean = 10) appeared to decrease the
750 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 33:5, JUNE 1994

administration of2 mg/kg naltrexone (also see Hermanet al., 1987; Herman, 1991). Naltrexone has a relativelylong half-life in plasma (Verebey et al., 1976), andresults of a positron emission tomography study indicate that naltrexone binds to opioid receptors in thenormal adult living human brain for as long as 1 weekafter the administration of a moderate dose (Lee et al.,1988). Accordingly, such data provide indirect supportfor the hypothesis that there may be significant brainopioid receptor concentrations of naltrexone on itssecond versus first day of administration and even afterdiscontinuation of the drug. These data may indicatethat relatively high doses of naltrexone are neededto produce significant effects on antecedent thoughtsassociated with bulimia nervosa. Further support forthis hypothesis is provided by our finding that theurge to binge after eating sweets was reduced afteradministration of high doses of naltrexone (1.5 and2.0 mg/kg, i.e., 50, 75, and 100 mg) but not afterthe lower dose (0.5 mg/kg, 25 mg). Similarly, highdoses of naltrexone (1.5 and 2.0 mg/kg) appeared tohave a greater effect in decreasing preoccupation withsweets than did low doses of naltrexone. These dataare consistent with the recent findings of Jonas andGold (I988) indicating that high but not low dosesof naltrexone are capable of significantly decreasingbinge eating and purging in bulimic women. This mayalso explain the failure of Mitchell et al. (I989) tofind significant effects of low doses of naltrexone (0.5to 1.0 mg/kg) in bulimic women.
We failed to find any significant difference in plasma~-endorphin concentrations in our bulimic subject incomparison with those in normal, nonbulimic controls.This is consistent with Fullerton and coworkers' (1988)more recent findings that differences in plasma~-endorphin concentrations in bulimic subjects versusthose in normal subjects were obtained only in bulimicswho vomited. We also observed a significant increaseof ~-endorphinduring the administration ofnaltrexonein this bulimic subject, and similar naltrexone-inducedincreases in l3-endorphin have been reported in adultformer opiate addicts (Kosten et al., 1986) and in asmall percentage of children and adolescents with autism (Herman, 1991). If bulimics achieve a raise in~-endorphin levels when they binge and purge, theelevation of ~-endorphin concentrations after the administration of naltrexone would explain the therapeutic effect of naltrexone on antecedent thoughts of
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 33:5. JUNE 1994
EFFECTS OF NALTREXONE ON HINGING
binging in this adolescent and may be the biologicalmechanism by which naltrexone is effective in thetreatment of bulimia.
Considering the findings of this study and the literature on the treatment of bulimia nervosa with naltrexone, it was recommended to the adolescent and herparents that she take naltrexone 1.5 mg/kg daily. WhileS.B. was hospitalized, her parents had decided to separate and refused further family therapy. However, S.B.continued in individual therapy while living with hermother. A few weeks after discharge from the hospital,the mother of S.B. reported that S.B. had stoppedtaking naltrexone and had resumed binging. WhenS.B. was questioned about this, she explained thatnaltrexone had taken away her urge to binge but thather relationship with her parents was so stressful thatshe did not want to give up the "only pleasure in herlife," her binging. Consequently, if she did not takethe naltrexone, she could at least "look forward to thebinge of the day." S.B. reassured her therapist thatinstead of taking laxatives, she had taken up running,which made her feel "high" and would take care ofthe extra calories of her daily binge.
This clinical information and the findings from thiscase study pose interesting questions regarding theetiology and treatment of bulimia nervosa. S.B. camefrom a family with numerous depressive and addictivedisorders, ranging from food to alcohol and drugs.The adolescent herself described her preoccupation andloss of control when eating sweets in the same wayshe and her father described being unable to stop oncethey started to drink alcohol. Whenever this younggirl felt in control of her life, she abstained fromsweets and from alcohol. However, when she becamedepressed, or when she experienced stressful life situations, she turned to food for comfort and occasionally,when in the company of her peers, resorted to alcoholto "pick herself up." Although naltrexone seemed torelieve her preoccupation with sweets and binging, itdid not affect her experience of distress and depression.Consequently, when she felt overwhelmed and unableto cope with her family situation, she made a consciousdecision to discontinue naltrexone and to resume herdaily binging.
This case study illustrates a strong interaction between depression, stress, and bulimia nervosa and pointsto an addictive nature of bulimia nervosa. It posessome interesting questions in regard to the choice of the
751

CHATOOR ET AL.
addictive substance, since this adolescent girl becameprimarily "addicted" to food, whereas her father hadbecome addicted to alcohol. Above all, this case illustrates the complexity of the interplay of biological andpsychological factors in the pathogenesis and treatmentof bulimia nervosa.
REFERENCES
American Psychiatric Associarion (1987), Diagnostic and Statistical ManualofMental Disorders, 3rd edition-revised (DSM-III-R). Washingron, DC:American Psychiatric Association
Brewerron TO, Lydiard RB, Laraia MT, Shook JE, Ballenger JC (1992),CSF bera-endorphin and dynorphin in bulimia nervosa. Am J Psychiatry 149:1086-1090
Campbell M, Overall JE, Small AM et al. (1989), Naltrexone in autisticchildren: an acute open dose range rolerance trial. JAm Acad ChildAdolesc Psychiatry 28:200-206
Fullerton DT, Swift WJ, Getro q, Carlson IH, Gutzmann LD (1988),Differences in the plasma beta-endorphin levels ofbulimics. InternationalJ ofEating Disorders 7:191-200
Garner OM, Olmsted MP, Bohr Y, Garfinkel PE (1982), The eatingattitudes test: psychometric features and clinical correlates. PsycholMed 12:871-878
Herman BH (1990), A possible role of proopiomelanocortin peptides inself-injurious behavior. Prog Neuropsychopharmacol Bioi Psychiatry14(suppl):S109-S 139
Herman BH (1991), Effects of opioid antagonists in the tteatment ofautism and self-injurious behavior. In: Mental Retardation: DevelopingPharmacotherapies, Ratey JJ, ed. Washingron, DC: American PsychiatricPress, pp 107-137
Herman BH, Arthur-Smith A, Hammock MK, Josephs S (1988), Ontogenyofbeta-endorphin and cortisol in the plasma ofchildren and adolescents.J Clin Endocrinol Metab 67:186-190
752
Herman BH, Asleson GS, Powell A, Borghese IF, Ruckman R, FitzgeraldC (1993), Cardiovascular and other physical effects of acute administration of naltrexone in autistic children. Journal of Child and AdolescentPsychopharmacology 3: 157-168
Herman BH, Hammock MK, Arthur-Smith A et aI. (1987), Naltrexonedecreases self-injurious behavior. Ann NeuroI22:550-552
Herman BH, Hammock MK, Arthur-Smith A, Kuehl K, Appelgate K(l989a), Effects of acute administration of naltrexone on cardiovascularfunction, body temperature, body weight and serum concentrations ofliver enzymes in autistic children. Dev Pharmacol Ther 12:118-127
Herman BH, Hammock MK, Egan J, Arthur-Smith A, Chatoor I, Werner A(l989b), Role for opioid peptides in self-injurious behavior: dissociationfrom auronomic nervous system functioning. Dev Pharmacol Ther12:81-89
Jonas JM, Gold MS (1987), Naltrexone in the treatment of bulimia. In:The Psychobiology ofBulimia, Hudson JI, Pope HG, eds. Washington,DC: American Psychiatric Press, pp 117-127
Jonas JM, Gold MS (1988), The use of opiate antagonists in treatingbulimia: a study of low-dose versus high-dose naltrexone. PsychiatryReview 24: 195-199
Kosten TR, Kreek MJ, Ragunath J, Kleber HD (1986), A preliminary studyof beta-endorphin during chronic naltrexone maintenance treatment inex-opiate addicts. Life Sci 39:55-59
Lee MC, Wagner HN, Tanada S, Frost JJ, Bile AN, Dannals RF (1988),Duration of occupancy of opiate receptors by naltrexone. J NuclMed 29:1207-1211
Martin WR, Jasinski DR, Mansky PA (1973), Naltrexone, an antagonistfor the treatment of heroin dependence: effects in man. Arch GenPsychiatry 28:784-791
Mitchell JE, Christenson G, Jennings Jet al. (1989), A placebo-conrrolled,double-blind cross-over study ofnaltrexone hydrochloride in outpatientswirh normal weight bulimia. J Clin PsychopharmacoI9:94-97
Smith MC, Thelen MH (1984), Development and validation of a test forbulimia. J Consult Clin Psychol 52:862-872
Verebey K, VolavkaJ, Mule SJ, Resnik RB (1976), Naltrexone: disposition,metabolism, and effects after acute and chronic dosing. Clin PharmacolTher 20:315-328
Waller DA, Kiser RS, Hardy BW, Fuchs J, Feigenbaum LP, Uarry R(1986), Eating behavior and plasma beta-endorphin in bulimia. Am JClin Nutr 44:20-23
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 33:5, JUNE 1994