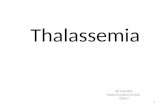
Effects of monotherapy and combined therapy on LPI...Over- expressed in E thalassemia 66.000 pg/ml...
40
Time (hours) 0 12 10 8 6 4 2 14 28 24 20 16 12 8 32 LPI (μM) Deferiprone 75 mg/kg/day Reproduced from Cabantchik ZI, et al. Best Pract Res Clin Hematol. 2005;18:277-87. Effects of monotherapy and combined therapy on LPI LPI (μM) Time (hours) mg/kg/day DFO 40 0 12 10 8 6 4 2 14 28 24 20 16 12 8 32 Deferiprone 75 mg/kg/day DFO 40 mg/kg/day LPI (μM) 0 12 10 8 6 4 2 14 28 24 20 16 12 8 DFO 40 mg/kg/day Time (hours) 32
Transcript of Effects of monotherapy and combined therapy on LPI...Over- expressed in E thalassemia 66.000 pg/ml...

Time (hours)
0
12
10
8
6
4
2
14
28 24 20 16 12 8 32
LPI (μM
)
Deferiprone 75 mg/kg/day
Reproduced from Cabantchik ZI, et al. Best Pract Res Clin Hematol. 2005;18:277-87.
Effects of monotherapy and combined therapy on LPI
LPI (μM
)
Time (hours)
mg/kg/day DFO 40
0
12
10
8
6
4
2
14
28 24 20 16 12 8 32
Deferiprone 75 mg/kg/day DFO 40 mg/kg/day
LPI (μM
)
0
12
10
8
6
4
2
14
28 24 20 16 12 8
DFO 40 mg/kg/day
Time (hours) 32

Chelation Therapy 47 patients
Combination DFO + DFP
Desferrioxamine Deferasirox Total N0 of Patients
Diagnosis
9 5 21 36 Thalassemia Major
2 0 6 24 Thalassemia Intermedia
0 1 2 37 Sickle Cell Anemia
0 0 1 34 Sickle Cell Thalassemia
11 6 30 131 Total
1 patient – DFP + DFX

Conclusions: Cardiac Iron Chelation Deferoxamine (DFO)
Major cardiac mortality with long-term use. Slow cardiac iron clearance - High dose IV.
Deferiprone (DFP) Cardiac iron clearance > deferoxamine. Can be combined with deferoxamine.
Deferasirox (DFX) Removes cardiac iron including EF effect. Randomised controlled data are awaited.
Combination Therapy DFO + DFX or DFP + DFX still in trial

Hepcidin Increased serum iron
concentration
Iron deficiency
Anemia
Hypoxia
Hemolysis
Blood loss

Iron overload
Hepcidin
LPS
IL-6
Inflammation
Infections Decreased serum iron
concentration

Iron overload Iron deficiency
Anemia
Hypoxia
Hemolysis
Blood loss
Hepcidin
LPS
IL-6
Inflammation
Infections
? How does the liver express Hepcidin in thalassemia?

Hepcidin in β-thalassemia Results

Iron overload Iron deficiency
Anemia
Hypoxia
Hemolysis
Blood loss
Hepcidin
LPS
IL-6
Inflammation
Infections
? Hepcidin expression in thalassemia
Increased Erythropoiesis
Increased GDF 15

NTBI - LPI Non Transferrin Bound Iron
Labile Plasma Iron Absent in healthy people. Increased in iron overload. Present when transferrin saturation is
above 80 %. Probable important role in toxicity. Target for Iron chelators.

Labile Cell Iron (LCI)
LCI
Iron Absorption
Transferrin
Increased Influx
Hemosiderosis
Altered Metabolism Friederich Ataxia Sideroblastic Anemia
Altered Efflux Anemia of Chronic Disease Ferroportin Disease
LCI should be maintained at constant level
Transferrin Receptors

GDF 15 Growth Differentiation Factor 15
Member of GDF β superfamily. Expressed in erythroblastic maturation. Over-expressed in β thalassemia
66.000 pg/ml vs 450 pg/ml. Tanno T et al - Nature 9:1096/2007.
In β thalassemia the erythroid compartment is expanded – Extramedullary Erythropoiesis
GDF 15 may inhibit hepcidine in thalassemia and contribute to Iron overload.

Erythroferrone
Bleeding or erythropoietin administration induced the release of this erythroid factor.
Erythroferrone is produced by the erythroblasts and suppress hepcidin.
Low hepcidin allowed intestinal iron absorption.
Leon Kautz – Presented in ASH Meeting – December 2013

Iron Regulation in β Thalassemia
Erythropoiesis
GDF 15 or Erythroferrone ?
Hepcidine
Iron absorption
Hemolysis Blood Transfusions
Transferrin Saturation > 75 %
INCREASED FERRITIN
Non Transferrin Bound Iron
Labile Cell Iron
CELL TOXICITY
Cardiac and Endocrine

β Thalassemia Intermedia
Clinical phenotype between transfusion dependent Thalassemia Major and asymptomatic Thalassemia Trait.
Considerable variability in clinical spectrum and in blood transfusion requirements.
Commonly maintain Hgb level 6 – 8 gr/dl. Interaction with α thalassemia:
α deletion or ααα.

β Thalassemia Intermedia
Th Major Thalassemia Intermedia Th Minor

βThalassemia Intermedia Clinical signs
Extramedullary erythropoiesis: minimal to extremely severe. Bone deformities and tumor like masses leading to nerve or spinal cord compression.
Splenomegaly: Minimal to severe. Arthritis. Ulcus cruris

Hg F synthesis induction in β Thalassemia Intermedia
Erythropoietin – Rachmilewitz – 1991.
Hydroxyurea -
Antioxidants – Curcumin vs Coenzyme Q10 - Fucharoen – Thailand.
Arginine Butyrate ± Hu or Epo

β THALASSEMIA HYDROXYUREA TREATMENT
0123456789
10
Hgb
(gr/d
l)
Before 3 6 12 24 36 48 60Months
Ha’Emek Ped Hem - 2008

β THALASSEMIA HYDROXYUREA TREATMENT
12.7
0.5 0.10
2
4
6
8
10
12
14
Blo
od T
rans
fusi
ons
U
nits
/ pa
tient
Before (-2 ys - 0)
After Tx (0 - + 2ys)
After Tx (+ 3ys / +4ys)
Ha’Emek Ped Hem - 2008 * 15 Units transfused because pregnancy (HU suspended)
*

β THALASSEMIA HYDROXYUREA TREATMENT
Conclusions No significant increase in Hgb levels. Hgb F – return to baseline levels (βo). Significant decrease in Blood transfusions
requirement transfusion independent. Xmn1 – a prognostic factor of response.
(Frequency in normal population 0.32 – 0.35).
α mutation – irrelevant. Better feeling at the onset of treatment.

SCA – Clinical Presentation SCA is characterized by chronic hemolytic
anemia and a variety of crises:
- Vaso-occlusive crises - Hemolytic crises - Acute chest syndrome - Acute splenic sequestration - Aplastic crises - Infections: Encapsulated bacteria
(S Pneumoniae) and Osteomyelitis. - Priapism. - Avascular necrosis of femoral or
humeral head.

SCA Frontal Brain Infarct

Who is at risk? Ethnic origin is critical!

Sickle Cell Anemia in Israel (129 patients)
59
52
10 8
Sickle Cell β Thalassemia
Others
Sickle Cell Disease
Others SC Disease – 3 SD Disease – 1 S Hgb Lepore – 1 CβThalassemia - 3
Emek Medical Center - Afula Shneider Medical Center – Petach Tikva Meyer – Rambam Medical Center - Haifa Dana Medical Center – Tel Aviv Sharey Tzedek – Jerusalem Hadassah Medical Center – Jerusalem Soroka Medical Center – Beer Sheva Missing Data - Tzafed
Hgb CC

Sickle Cell Anemia in Israel Patients Ethnic Origin
106
1 7
Afro American
African
Israel Arabs – Bedouins - Saudiarabia - Jordan - Sudan - African
Others SC Disease – 3 SD Disease – 1 S Hgb Lepore – 1 CβThalassemia - 3

The origin of Sickle Cell in Israel
The geographical dispersion of the SCA gene – Tel Aviv University -Yael Levi - 1990
Arab India

The origin of Sickle Cell in Israel Genetic characterization of sickle-cell anemia in Israeli Arabs Kirschmann C, Shalmon L, Goshen Y, Zaizov R. Harefuah. 1987 Nov 1;113(9):201-4. The origin of sickle cell alleles in Israel Deborah Rund, Naomi Kornhendler, Oded Shalev, and Ariella Oppenheim. Human Genetics – 85:521-524;1990 Arab families: Benin haplotype Central African Republic (Bantu) haplotype Jewish Family: Benin haplotype.

Blood Transfusions in SCD
Hemolytic crises. Acute splenic sequestration. Acute chest syndrome. Hypersplenism – common in
Sβ Thal. Aplastic crises. Stroke Prevention
- Primary due to TCD findings. - Secondary after first stroke.

Inflammation in SCD (1)
Endothelial Function in Patients with Sickle Cell Anemia during and after SC Crises.
High levels of endothelial adhesion molecules
(VCAM-1) and inflammatory markers (CD 40) in steady state and not only in crises.
Study Limitations: 10 patients and short period of follow up.
Bloom A & al – J Thromb & Thrombolysis 19:83-86;2005

Inflammation in SCD (2)
Oxidative stress and inflammation in iron overloaded patients with β thalassemia or
sickle cell disease.
Increased IL 6, IL 5 and IL 10 compared to thalassemia.
NTBI increased in thalassemia compared to SCD.
γ tocopherol, a NO selective antioxidant is increased in SCD.
Walter PB et al. Br J Hem 135:254-263;2006.

Inflammation in SCD (2)
The biology of SCD may show increased inflammation and increased levels of protective anti oxidants compared with thalassemia. Walter PB et al. Br J Hem 135:254-263;2006.
p SCD Th M Parameter 0.033 15 ± 5.6 9.2 ± 7.2 Liver Iron (mg/g dw)
<0.001 2515 ± 1153 1868 ± 1042 Ferritin (µg/l) 0.014 64.5 ± 23 82.5 ± 21 Tf Saturation (%)
<0.001 1.9 ± 2.1 4.0 ± 1.6 NTBI (µmol/l)

Relationship of liver iron to duration of transfusion therapy. The significant correlation (P < .001) between transfusion duration, in months, and liver iron on biopsy specimen.
Harmatz P et al. Blood 2000;96:76-79
©2000 by American Society of Hematology

Relationship of liver iron to duration of transfusion therapy.
Harmatz P et al. Blood 2000;96:76-79
Plasma Ferritin did not correlate to liver iron. Mean Ferritin 2686 ± 1039 ng/dl.
Fever, infection, inflammation and hepatic dysfunction affects ferritin levels – All are present in SCD.
Mild to moderate abnormalities of inflammation or fibrosis in 16 out of 20 patients.

Relationship of liver iron to duration of transfusion therapy.
Harmatz P et al. Blood 2000;96:76-79
Liver iron score correlate to fibrosis and not to inflammation severity.
Intensity of iron staining in Kupffer cells is greater than in the hepatocytes (p<0.001)
Overflow of iron from the Kupffer cells to the hepatocytes?
In SCD may be a different response to iron overload in the liver compared to Thalassemia.

Sickle cell vs Thalassemia on Chronic Transfusion
Patient characteristic Thalassemia (n=30) SCD (n=43)
Age 18 ± 2 15 ± 1
Ys transfused 12 ± 2 6 ± 1
Serum Ferritin 2122 ± 289 2916 ± 233 Liver Iron 15 ± 2 14 ± 1 Cardiac disease 20 % 0 Growth delay 27 % 9 % Gonadal Failure 33 % 0 Liver Fibrosis > 0 81 % 39 %
Vichinsky – Am J Hem 2005

Sickle cell vs Thalassemia Hemosiderosis
“Despite prolonged exposure to Iron, NO SCD patients demonstrated elevated cardiac iron by T2* MRI or abnormal function !!! In contrast to 42 % of the thalassemia patients with similar iron exposure”
Wood et al, Blood 2004.

Iron Overload in Sickle Cell β0 Thalassemia
No cardiac symptoms No arrhythmias Chest X rays: 40
- 4 cardiac enlargement (Age 37, 33, 31 and 19 ys).
ECG: Normal. ECHO: Normal SF in 22 / 23 pts.
Mild cardiomyopathy in 1 (7 ys - BT) T2*MRI – 10 patients – No iron in myocardium
Ghoti, Rachmilewitz, Konen et al, ASH – 2008. European Journal of Hematolgy 84:59–63,2010.
Emek Ped Hem - 2009

Iron Overload in SCD
0
50
100
150
200
250
Tran
sfer
rin (m
cgr/d
l)
SCA Sthal Th Major Th Int0
50
100
150
200
250
Seru
m Ir
on (m
cgr/d
l)
SCA Sthal Th Major Th Int
0102030405060708090
100
Tran
sfer
rin
Satu
ratio
n (%
)
SCA Sthal Th Major Th Int0
500
1000
1500
2000
2500
3000
3500
Seru
m F
errit
in (n
g/dl
)
SCA Sthal Th Major Th Int
** p = <0.001 - SCD vs Thal

Iron Overload in SCD NTBI and LPI results
SCA Sickle β Thal
β Thal Major
β Thal Intermedia
NTBI (Units) No Positive (>0.7) p = <0.001
0 ± 0.1 (0)
0 ± 0.1 (0)
0.56 ± 0.52 (14)
0.5 ± 0.65 (3)
LPI (Units) No Positive (>0.7) p = 0.017
0.1 ± 0.2 (1)
0 ± 0.1 (0)
0.22 ± 0.33 (3)
0.2 ± 0.35 (1)
Ha’Emek Ped Hem - 2009

Iron Overload in Sickle Cell Disease
Less Blood requirements than Thalassemia. Ferritin levels above 1000 ng/dl after age 10. Mean Transferrin saturation under 40 %. Absent or Minimal levels of NTBI and LPI. No chelation therapy provided.
Ha’Emek Ped Hem - 2007