Effects of 17α-ethynylestradiol-induced cholestasis on the pharmacokinetics of doxorubicin in rats:...
7
2013 http://informahealthcare.com/xen ISSN: 0049-8254 (print), 1366-5928 (electronic) Xenobiotica, 2013; 43(10): 901–907 ! 2013 Informa UK Ltd. DOI: 10.3109/00498254.2013.783250 RESEARCH ARTICLE Effects of 17a-ethynylestradiol-induced cholestasis on the pharmacokinetics of doxorubicin in rats: reduced biliary excretion and hepatic metabolism of doxorubicin Young Hee Choi 1 , Yu Kyung Lee 1 , and Myung Gull Lee 2 1 College of Pharmacy and Research Institute of Pharmaceutical Sciences, Dongguk University-Seoul, Goyang, South Korea and 2 College of Pharmacy, The Catholic University of Korea, Bucheon, South Korea Abstract 1. Since the prevalent hormonal combination therapy with estrogen analogues in cancer patients has frequency and possibility to induce the cholestasis, the frequent combination therapy with 17a-ethynylestradiol (EE, an oral contraceptive) and doxorubicin (an anticancer drug) might be monitored in aspect of efficacy and safety. Doxorubicin is mainly excreted into the bile via P-glycoprotein (P-gp) and multidrug resistance-associated protein 2 (Mrp2) in hepatobiliary route and metabolized via cytochrome P450 (CYP) 3A subfamily. Also the hepatic Mrp2 (not P-gp) and CYP3A subfamily levels were reduced in EE-induced cholestatic (EEC) rats. Thus, we herein report the pharmacokinetic changes of doxorubicin with respect to the changes in its biliary excretion and hepatic metabolism in EEC rats. 2. The pharmacokinetic study of doxorubicin after intravenous administration of its hydrochloride was conducted along with the investigation of bile flow rate and hepatobiliary excretion of doxorubicin in control and EEC rats. 3. The significantly greater AUC (58.7% increase) of doxorubicin in EEC rats was due to the slower CL (32.9% decrease). The slower CL was due to the reduction of hepatic biliary excretion (67.0% decrease) and hepatic CYP3A subfamily-mediated metabolism (21.9% decrease) of doxorubicin. These results might have broader implications to understand the altered pharmacokinetics and/or pharmacologic effects of doxorubicin via biliary excretion and hepatic metabolism in experimental and clinical estrogen-induced cholestasis. Keywords 17a-Ethynylestradiol, cholestasis, cytochrome P450, doxorubicin, hepatic metabolism, hepatobiliary excretion, multidrug resistance-associated protein 2, pharmacokinetics History Received 7 January 2013 Revised 27 February 2013 Accepted 4 March 2013 Published online 10 April 2013 Introduction The hormonal combination therapy with estrogen analogues such as 17a-ethynylestradiol (EE), a synthetic estrogen used for oral contraceptives, is prevalently being used for the contraception in cancer patients and improves the efficacy of cancer chemotherapy (Schwarz et al., 2009). Anticancer actions of estradiol or EE on tumors in mice, rats and humans have been documented (Key, 1995; Rajkumar et al., 2004; Schwarz et al., 2009; Sivaraman et al., 1998; Yao et al., 2000). However, it is true that there are controversial evidences of EE therapy. In addition, EE therapy has been known to cause intrahepatic cholestasis (Eloranta et al., 2001; Savander et al., 2003) and decreases bile flow rate in experimental animal models (Crocenzi et al., 2001; Rodriguez-Garay, 2003). Thus, by these EE-induced changes, therapeutic effect of anticancer drug might be influenced and it seems valuable to investigate (Early Breast Cancer Trialists’ Collaborative Group, 2005). Doxorubicin, an anthracycline anticancer drug, impairs DNA synthesis during tumor cell division and is commonly used for the treatment of ovarian cancer, mammary cancer, lymphoma and osteosarcoma (Rocha et al., 2001; Smylie et al., 2007). The extent of absolute oral bioavailability (F) of doxorubicin is very low (less than 10%) likely due to the extensive hepatic metabolism and biliary excretion in rats (Choi et al., 2011). Doxorubicin is metabolized to its metabolites, doxorubicinol and the forms of alycones, mainly via cytochrome P450 (CYP) 3A subfamily and their glucuronide conjugates (Lee & Lee, 1999; Speeg & Maldonado, 1994). Recently, it was reported that down- regulation of hepatic P-glycoprotein (P-gp) and multidrug resistance-associated protein 2 (Mrp2) directly leads to a reduction in hepatobiliary excretion of doxorubicin in rats and/or humans (Cui et al., 1999; Hidemura et al., 2003; Pauli Magnus & Meier, 2005). The combination use of EE and doxorubicin was known to enhance anticancer effect (Czeczuga-Semeniuk et al., 2004). On the other hand, the induction of intrahepatic cholestasis and reduction of bile flow by EE therapy might affect anticancer effect of doxorubicin in the aspect of the elimin- ation of doxorubicin via biliary excretion and hepatic metabolism. In EE-induced cholestasis (EEC) in rats, an animal model representing the cholestasis state, the impair- ment of Mrp2 and reduction of CYP3A were caused by EE Address for correspondence: Y. H. Choi, College of Pharmacy, Dongguk University-Seoul, Dongguk-lo 32, Ilsandong-gu, Goyang, Gyeonggi-do 410-820, South Korea. Tel/Fax: 1-82-31-961-5212. E-mail: choiyh@ dongguk.edu Xenobiotica Downloaded from informahealthcare.com by Michigan State University on 10/26/14 For personal use only.
-
Upload
myung-gull -
Category
Documents
-
view
214 -
download
0
Transcript of Effects of 17α-ethynylestradiol-induced cholestasis on the pharmacokinetics of doxorubicin in rats:...

2013
http://informahealthcare.com/xenISSN: 0049-8254 (print), 1366-5928 (electronic)
Xenobiotica, 2013; 43(10): 901–907! 2013 Informa UK Ltd. DOI: 10.3109/00498254.2013.783250
RESEARCH ARTICLE
Effects of 17a-ethynylestradiol-induced cholestasis on thepharmacokinetics of doxorubicin in rats: reduced biliary excretionand hepatic metabolism of doxorubicin
Young Hee Choi1, Yu Kyung Lee1, and Myung Gull Lee2
1College of Pharmacy and Research Institute of Pharmaceutical Sciences, Dongguk University-Seoul, Goyang, South Korea and2College of Pharmacy, The Catholic University of Korea, Bucheon, South Korea
Abstract
1. Since the prevalent hormonal combination therapy with estrogen analogues in cancerpatients has frequency and possibility to induce the cholestasis, the frequent combinationtherapy with 17a-ethynylestradiol (EE, an oral contraceptive) and doxorubicin (an anticancerdrug) might be monitored in aspect of efficacy and safety. Doxorubicin is mainly excreted intothe bile via P-glycoprotein (P-gp) and multidrug resistance-associated protein 2 (Mrp2) inhepatobiliary route and metabolized via cytochrome P450 (CYP) 3A subfamily. Also the hepaticMrp2 (not P-gp) and CYP3A subfamily levels were reduced in EE-induced cholestatic (EEC) rats.Thus, we herein report the pharmacokinetic changes of doxorubicin with respect to thechanges in its biliary excretion and hepatic metabolism in EEC rats.2. The pharmacokinetic study of doxorubicin after intravenous administration of itshydrochloride was conducted along with the investigation of bile flow rate and hepatobiliaryexcretion of doxorubicin in control and EEC rats.3. The significantly greater AUC (58.7% increase) of doxorubicin in EEC rats was due to theslower CL (32.9% decrease). The slower CL was due to the reduction of hepatic biliary excretion(67.0% decrease) and hepatic CYP3A subfamily-mediated metabolism (21.9% decrease) ofdoxorubicin. These results might have broader implications to understand the alteredpharmacokinetics and/or pharmacologic effects of doxorubicin via biliary excretion and hepaticmetabolism in experimental and clinical estrogen-induced cholestasis.
Keywords
17a-Ethynylestradiol, cholestasis, cytochromeP450, doxorubicin, hepatic metabolism,hepatobiliary excretion, multidrugresistance-associated protein 2,pharmacokinetics
History
Received 7 January 2013Revised 27 February 2013Accepted 4 March 2013Published online 10 April 2013
Introduction
The hormonal combination therapy with estrogen analogues
such as 17a-ethynylestradiol (EE), a synthetic estrogen used
for oral contraceptives, is prevalently being used for the
contraception in cancer patients and improves the efficacy of
cancer chemotherapy (Schwarz et al., 2009). Anticancer
actions of estradiol or EE on tumors in mice, rats and humans
have been documented (Key, 1995; Rajkumar et al., 2004;
Schwarz et al., 2009; Sivaraman et al., 1998; Yao et al., 2000).
However, it is true that there are controversial evidences of
EE therapy. In addition, EE therapy has been known to cause
intrahepatic cholestasis (Eloranta et al., 2001; Savander et al.,
2003) and decreases bile flow rate in experimental animal
models (Crocenzi et al., 2001; Rodriguez-Garay, 2003). Thus,
by these EE-induced changes, therapeutic effect of anticancer
drug might be influenced and it seems valuable to investigate
(Early Breast Cancer Trialists’ Collaborative Group, 2005).
Doxorubicin, an anthracycline anticancer drug, impairs
DNA synthesis during tumor cell division and is commonly
used for the treatment of ovarian cancer, mammary cancer,
lymphoma and osteosarcoma (Rocha et al., 2001; Smylie
et al., 2007). The extent of absolute oral bioavailability (F)
of doxorubicin is very low (less than 10%) likely due to the
extensive hepatic metabolism and biliary excretion in
rats (Choi et al., 2011). Doxorubicin is metabolized to
its metabolites, doxorubicinol and the forms of alycones,
mainly via cytochrome P450 (CYP) 3A subfamily and
their glucuronide conjugates (Lee & Lee, 1999; Speeg &
Maldonado, 1994). Recently, it was reported that down-
regulation of hepatic P-glycoprotein (P-gp) and multidrug
resistance-associated protein 2 (Mrp2) directly leads to a
reduction in hepatobiliary excretion of doxorubicin in rats
and/or humans (Cui et al., 1999; Hidemura et al., 2003;
Pauli Magnus & Meier, 2005).
The combination use of EE and doxorubicin was known to
enhance anticancer effect (Czeczuga-Semeniuk et al., 2004).
On the other hand, the induction of intrahepatic cholestasis
and reduction of bile flow by EE therapy might affect
anticancer effect of doxorubicin in the aspect of the elimin-
ation of doxorubicin via biliary excretion and hepatic
metabolism. In EE-induced cholestasis (EEC) in rats, an
animal model representing the cholestasis state, the impair-
ment of Mrp2 and reduction of CYP3A were caused by EE
Address for correspondence: Y. H. Choi, College of Pharmacy, DonggukUniversity-Seoul, Dongguk-lo 32, Ilsandong-gu, Goyang, Gyeonggi-do410-820, South Korea. Tel/Fax: 1-82-31-961-5212. E-mail: [email protected]
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

(Crocenzi et al., 2001; Lin et al., 2002; Micheline et al, 2002;
Trauner et al., 1997) and these changes might affect the
elimination of doxorubicin. Therefore, we herein focus on
the pharmacokinetic changes of doxorubicin in EEC rats.
Materials and methods
Chemicals
Doxorubicin hydrochloride was purchased from Bo-Ryung
Pharmaceutical Company (Seoul, South Korea). Daunorubi-
cin hydrochloride (internal standard for high-performance
liquid chromatographic (HPLC) analysis of doxorubicin), EE,
1,2-propanediol, dextran (mol. wt. 65 000), the reduced form
of b-nicotinamide adenine dinucleotide phosphate (NADPH;
as a tetrasodium salt) and tris(hydroxymethyl)aminomethane
(tris)-buffer were purchased from Sigma-Aldrich Corp.
(St. Louis, MO). Other chemicals were of reagent or HPLC
grade.
Animals
The protocols for all animal studies were approved by
Dongguk University Medical Center in Institutional Animal
Care and Use Committee (Seoul, South Korea). Female
Sprague–Dawley rats (6–7 weeks old; weighing 200–230 g)
were purchased from Charles River Company Korea (Orient,
Seoul, South Korea) and maintained in the same conditions as
a reported method (Choi et al., 2010).
The rats were randomly divided into two groups; control
and EEC groups. In EEC rats, intrahepatic cholestasis was
induced by the daily subcutaneous injection of EE (dissolved
in 1,2-propanediol) at a dose of 10 mg (in 4 mL) kg�1 for five
consecutive days. Control rats were injected with the same
volume of 1,2-propanediol alone (Jin et al., 2009).
Measurement of parameters in cholestasis
The degree of EEC was measured by the determination of bile
acids, alkaline phosphate and testosterone levels in serum
(analyzed by Green Cross Reference Laboratory, Seoul, South
Korea). For the estimation of bile flow rate, the common bile
duct of the rats was cannulated using polyethylene tubing and
the bile flow rate was estimated gravimetrically using the
volume of bile juice and collection periods (Choi et al., 2006).
The rats were euthanized and the total liver weight was
measured (Choi et al., 2006). All steps were conducted in
control and EEC rats.
Intravenous administration of doxorubicinhydrochloride to control and EEC rats
On day 6 after the start of the treatment with EE or 1,2-
propanediol, the surgical procedures including the cannula-
tion of the carotid artery (for blood sampling) and the
jugular vein (for drug administration in the intravenous study)
were conducted as similar as reported methods (Choi et al.,
2006, 2010).
After rats were recovered from the anesthesia and freely
moving, doxorubicin hydrochloride (dissolved in distilled
water) at a dose of 20 mg (in 2 mL) kg�1 as free base
was manually administered via the jugular vein over 1 min
to control (n¼ 6) and EEC (n¼ 7) rats. Blood samples
(approximately 0.22 mL, each) were collected via the carotid
artery at 0 (control), 1, 5, 15, 30, 60, 120, 180, 240, 300, 360,
400 and 480 min after the administration of doxorubicin
hydrochloride. After centrifugation of a blood sample, a
100-mL of supernatant was collected. At the end of 24 h, each
metabolic cage was rinsed with 10 mL of distilled water
and the rinsings were combined with the 24-h urine in urine
collector. All plasma and urine samples were stored at �70 �C(Revco ULT 1490 D-N-S; Western Mednics, Asheville, NC)
until used for the analysis of doxorubicin.
Biliary clearance of doxorubicin after intravenousadministration of its hydrochloride to control andEEC rats
On day 6, the biliary excretion of doxorubicin was measured.
The procedures used for the cannulation of the carotid artery,
the jugular vein and the bile duct (for bile juice sampling)
were similar to reported methods (Choi et al., 2006, 2010).
Blood samples were collected as the same as the intravenous
study mentioned above. The bile samples were collected
between 0–2, 2–6, 6–12 and 12–24 h, respectively. The
volume of bile and the amount of doxorubicin excreted into
the bile were measured (Choi et al., 2006). The biliary
clearance (CLbile) was calculated by dividing the cumulative
amount of doxorubicin excreted into the bile up to 24 h by
the area under the plasma concentration–time curve from time
0 to the last measured time, 24 h (AUC0–24 h).
Net biliary clearance of doxorubicin after intravenousinfusion of its hydrochloride to control and EEC rats
The procedures used for the cannulation of the carotid artery,
the jugular vein and the bile duct were similar to reported
methods (Choi et al., 2006, 2010).
On day 6, a loading dose of doxorubicin hydrochloride
(3.76 mg kg�1 as free base) was administered as intravenous
bolus followed by a constant-rate infusion of 834 and
560 mg h�1 kg�1 as free base in distilled water for control
and EEC rats, respectively, using Harvard infusion pump
(PHD2000, South Natick, MA). After 60 min infusion, the
steady state plasma concentration (Css) of doxorubicin
(at approximately 0.1mg mL�1 in both groups of rats) was
attained and bile was collected at 20-min interval throughout
the experiment. Blood samples were taken at the bile
collection time periods (60, 80, 100 and 120 min after the
infusion was started; Choi et al., 2006). After 120 min
infusion, plasma samples were collected and the rats were
sacrificed. The liver was homogenized with four volumes of
the distilled water and the concentration of doxorubicin in
the liver was measured (Choi et al., 2006). The volume
of bile samples was measured gravimetrically with specific
gravity.
The apparent biliary clearance (CLbile/plasma) based on the
plasma concentration was calculated by dividing the biliary
excretion rate by Css in each collection time period. The net
biliary clearance (CLbile/liver) based on the liver concentration
was calculated by dividing the biliary excretion rate by the
liver concentration (doxorubicin concentration in the liver
at 120 min after starting infusion; Suzuki et al., 2006).
The tissue-to-plasma ratio (T/P) is represented as the ratio of
902 Y. H. Choi et al. Xenobiotica, 2013; 43(10): 901–907
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

the liver concentration/plasma concentration of doxorubicin
(Choi et al., 2006).
Measurement of Vmax, Km and CLint for thedisappearance of doxorubicin in hepatic microsomalfractions from control and EEC rats
The hepatic and intestinal microsomes in control and
EEC rats were prepared based on a reported method (Choi
et al., 2010). The Vmax (the maximum velocity) and Km
(the apparent Michaelis–Menten constant; the concentration
at which the rate is one-half of the Vmax) for the disappearance
of doxorubicin were determined after incubating the above
microsomal fractions (equivalent to 1.0 mg protein); 5 mL of
methanol containing final doxorubicin concentrations of 0.5,
1, 5, 10, 50 and 100 mM; 50 mL of 0.1 M Sørensen phosphate
buffer (pH 7.4) containing 1 mM NADPH; and 0.1 M
phosphate buffer (pH 7.4) which adjusted the final volume
as 0.5 mL. The samples were incubated in a thermomixer
[37 �C, 50 oscillations per min (opm); Eppendorf, Hamburg,
Germany] for 15 min, and then the reaction was terminated by
the addition of 1 mL of acetonitrile containing 5 mg mL�1 of
daunorubicin.
Based on a non-linear regression method (Duggleby,
1995), the kinetic constants (Km and Vmax) for the disappear-
ance of doxorubicin were calculated and the intrinsic
clearance (CLint) for the disappearance of doxorubicin was
calculated by dividing the Vmax by the Km.
Rat plasma protein binding of doxorubicin usingequilibrium dialysis
Using equilibrium dialysis, the protein-binding values of
doxorubicin at 0.1 mg mL�1 were measured in fresh plasma
from control and EEC rats (n¼ 5; each) (Choi et al., 2006).
A Spectra/Por 4 membrane (mol. wt. cutoff 12–14 KDa;
Spectrum Medical Industries, Houston, TX) divided a 1 mL
dialysis cell into two compartments and 1 mL of plasma and
isotonic Sørensen phosphate buffer (pH 7.4) containing 3%
(w/v) dextran were spiked to each compartment, respectively.
A 10 mL of doxorubicin solution was spiked into the plasma
compartment. After 24 h, a 100 mL of sample was collected
from each compartment.
HPLC analysis of doxorubicin
Concentrations of doxorubicin in the samples were determined
by a slight modification of a reported HPLC analysis (Lee &
Lee, 1999). A 200 mL of acetonitrile containing 50 ng mL�1 of
daunorubicin hydrochloride was added to 100mL of a
biological sample. After vortex-mixing and centrifugation,
30 mL of the supernatant was directly injected onto a reversed-
phase column (XBridgeTM RP18; 150 mm. ‘.� 4.6 mm. i.d.;
particle size, 5 mm; Waters, Milford, MA). The mobile phase,
0.02 M phosphate buffer:acetonitrile (70:30, v/v), was run at
a flow-rate of 1.0 mL min�1. The excitation and emission
wavelengths of fluorescence detector were 460 and 580 nm,
respectively. The retention times of doxorubicin and dauno-
rubicin were 4.2 and 7.5 min, respectively, and the detection
limit of doxorubicin in rat plasma was 0.01 mg mL�1 based
on a signal to noise ratio of >3.0. The coefficient variation
of doxorubicin (from 0.01 to 100 mg mL�1) was below 9.35%.
Pharmacokinetic analysis
The total area under the plasma concentration–time curve
from time zero to infinity (AUC) was calculated using the
trapezoidal rule–extrapolation method (Chiou, 1978).
The following pharmacokinetic parameters using a non-
compartmental analysis (WinNonlin�; professional edition
version 2.1; Pharsight, Mountain View, CA) were calculated
based on the standard methods (Gibaldi & Perrier, 1982);
the terminal half-life, time-averaged total body, renal and
non-renal clearances (CL, CLR and CLNR, respectively),
mean residence time (MRT) and apparent volume of distri-
bution at a steady state (Vss).
Statistical analysis
To compare the means for the unpaired data, an unpaired
t-test was used as a typical manner. A p-value 50.05 was
considered to be statistically significant and all data are
expressed as mean� standard deviation (SD).
Results
Representative parameters of cholestasis
The parameters in control and ECC rats are listed in Table 1.
EEC rats had significantly smaller body weight gain (2 versus
38 g) on day 6. Relative liver weight was significantly heavier
(31.5% increase), but bile flow rate was significantly slower
(57.9% decrease) by cholestasis (EEC rats). In addition,
serum levels of alkaline phosphate and bile acids were
significantly higher (86.8% and 160% increase, respectively),
but the testosterone level was significantly lower (94.5%
decrease) in EEC rats. These observations suggest that EE
administration led to experimental cholestasis in rats.
Intravenous administration of doxorubicinhydrochloride to control and EEC rats
The mean arterial plasma concentration–time profiles
and pharmacokinetic parameters of doxorubicin following
intravenous administration of its hydrochloride at a dose
of 20 mg kg�1 as free base to control and EEC rats are
shown and listed in Figure 1 and Table 2, respectively.
After intravenous administration to EEC rats, the AUC was
significantly greater (58.7% increase), CL and CLNR were
significantly slower (32.9% and 33.6% decrease, respect-
ively), CLR was significantly faster (133% increase) and Ae0–
24h was significantly greater (280% increase) than that in
control rats. Note that the Ae0–24 h and CLR of doxorubicin
were almost negligible. The Vss values were considerably
large for both control and EEC rats, suggesting that the
affinity of doxorubicin to rat tissues were considerable.
Biliary clearance of doxorubicin after intravenousadministration of its hydrochloride to control andEEC rats
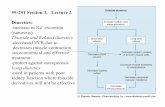
The ratios of doxorubicin dose excreted in 24-h bile were
29.8� 5.35% and 13.9� 6.98% for control and EEC rats,
respectively (Figure 2); they were significantly different. The
CLbile values are listed in Table 3. In ECC rats, the CLbile was
significantly slower (67.0% decrease) than that in control rats.
DOI: 10.3109/00498254.2013.783250 Pharmacokinetics of doxorubicin in cholestatic rats 903
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

Net biliary excretion of doxorubicin afterintravenous infusion of its hydrochloride tocontrol and EEC rats
To investigate the changes in net hepatobiliary excretion
of doxorubicin at steady state, the net biliary clearances
of doxorubicin in control and EEC rats were measured and
are listed in Table 4. No significant differences were
observed between the control and EEC rats in the plasma
concentrations of doxorubicin at steady state (Css; 0.106
and 0.106 mg mL�1, respectively). In EEC rats, the bile flow
rate, biliary excretion rate, CLbile/plasma (representing the
apparent biliary clearance based on the plasma concentra-
tions) and CLbile/liver (representing the actual hepatobiliary
transport function of doxorubicin) were significantly slower
(70.2%, 64.4%, 63.4% and 76.4% decrease, respectively)
than those in control rats. In EEC rats, the concentration of
doxorubicin in the liver and the T/P ratio were significantly
higher and greater (204% and 210% increase, respectively)
than those in control rats.
Table 1. Characteristics of control and EEC rats.
Parameter Control rats (n¼ 4) EEC rats (n¼ 4)
Initial body weight (g) 220� 31.3 222� 46.3Final body weight (g) 258� 6.61 224� 10.8a
Relative liver weight (g final body weight�1) 0.0441� 0.00265 0.0580� 0.00568a
Bile flow rate (mL min�1 g liver�1) 2.90� 0.204 1.22� 0.105b
Serum level � �Alkaline phosphate (U L�1) 190� 39.2 355� 70.5b
Bile acids (mmol L�1) 13.4� 4.56 34.8� 7.32b
Testosterone (ng L�1) 1.78� 0.759 0.0975� 0.0624a
Data are given as the mean� standard deviation (SD). EEC, 17a-ethynylestradiol-induced cholestasis; U, unit.aEEC rats were significantly different (p50.01) from control rats.bEEC rats were significantly different (p50.001) from control rats.
Time (min)
0 6 12 18 24
Cum
ulat
ive
bilia
ry e
xcre
tion
of in
trav
enou
s do
se (
%)
0
5
10
15
20
25
30
35
*
**
*
Figure 2. Mean Cumulative biliary excretion of doxorubicin after intra-venous administration of its hydrochloride at a dose of 20 mg kg–1 tocontrol (f; n¼ 4) and EEC (*; n¼ 4) rats. Bars represent standarddeviations. *EEC rats were significantly different (p50.01) fromcontrol rats.
Time (min)
0 120 240 360 480
Pla
sma
conc
entr
atio
n of
dox
urub
icin
(µg
/ml)
0.01
0.02
0.05
0.1
0.2
0.5
1
2
5
10
20
50
100
Figure 1. Mean arterial plasma concentration–time profiles of doxo-rubicin after intravenous administration of its hydrochloride at a dose of20 mg kg–1 to control (f; n¼ 6) and EEC (*; n¼ 7) rats. Bars representstandard deviations.
Table 2. Pharmacokinetic parameters of doxorubicin after intravenousadministration of its hydrochloride at a dose of 20 mg kg�1 to control andEEC rats.
Parameter Control rats (n¼ 6) EEC rats (n¼ 7)
Initial body weight (g) 230� 35.6 225� 56.3Final body weight (g) 262� 7.53 220� 11.6a
AUC (mg min mL�1) 138� 18.5 219� 26.3b
Terminal half-life (min) 384� 229 657� 358MRT (min) 256� 162 368� 246CL (mL min�1 kg�1) 139� 18.5 93.3� 10.9b
CLR (mL min�1 kg�1) 0.675� 0.333 1.57� 0.451 c
CLNR (mL min�1 kg�1) 138� 17.7 91.7� 12.0b
Vss (mL kg�1) 37 600� 8700 34 200� 18 800Ae0–24 h (% of dose) 0.482� 0.239 1.83� 0.473 c
Data are given as the mean� standard deviation (SD). EEC, 17a-ethynylestradiol-induced cholestasis; AUC, total area under the plasmaconcentration–time curve from time zero to infinity; MRT, meanresidence time; CL, time-averaged total body clearance; CLR, time-averaged renal clearance; CLNR, time-averaged non-renal clearance;Vss, apparent volume of distribution at steady state; Ae0–24h, percentageof the dose excreted in the urine up to 24 h.
aEEC rats were significantly different (p50.01) from control rats.bEEC rats were significantly different (p50.05) from control rats.cEEC rats were significantly different (p50.001) from control rats.
904 Y. H. Choi et al. Xenobiotica, 2013; 43(10): 901–907
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

Vmax, Km and CLint for the disappearance ofdoxorubicin in hepatic microsomes from controland EEC rats
Based on the relationships between concentrations of doxo-
rubicin and velocity for the disappearance of doxorubicin in
hepatic microsomes, the Vmax, Km and CLint for the disappear-
ance of doxorubicin from control and EEC rats are listed
in Table 5. The Vmax in EEC rats was significantly slower
(28.4% decrease) than that in control rats, suggesting that
the maximum velocity for the disappearance of doxorubicin
was significantly slower in EEC rats. However, the Km values
were comparable between the two groups of rats, suggesting
that the affinity of the enzyme(s) for doxorubicin was not
affected by EE treatment. As a result, the CLint in EEC rats
was significantly slower (21.9% decrease) than that in control
rats. These data suggest that the hepatic metabolism of
doxorubicin in EEC rats was significantly decreased by EE
treatment.
Measurement of rat plasma protein binding ofdoxorubicin using equilibrium dialysis
Protein-binding values of doxorubicin in fresh rat plasma
from control and EEC rats were 71.3� 21.5% and 68.9�31.7%, respectively; they were not significantly different.
The adsorption of doxorubicin to the equilibrium dialysis
apparatus, which included the semi-permeable membrane,
was almost negligible, and 91.3–99.3% of the spiked amounts
of doxorubicin were recovered from the both plasma and the
buffer compartments.
Discussion
Since EE showed an antitumor activity (Rajkumar et al.,
2004; Sivaraman et al., 1998), EE treatment has possibility
in cancer patients as one of the frequent medications with
co-administration of anti-cancer drugs. However, as a
clinical counterpart of oral contraceptive-induced cholestasis
(Rodriguez-Garay, 2003), an induction of cholestasis might
be a point to be monitored. Experimental intrahepatic
cholestasis induced by EE treatment is a widely used animal
model. Doxorubicin is mainly eliminated by biliary excretion
and metabolism in the liver (Choi et al., 2011). Thus, the
correlation of metabolic enzymes and transporters between
rats and humans are the important points. The sequential
homologies of CYPs (including CYP3A subfamily) between
rat and human are more than 70%; there are generally
conserved regions (for P-450 reductase, heme and signal
peptide) which cause this similarity (Soucek & Gut, 1992;
Zawaira et al., 2008). P-gp and Mrp2 in rats have orthologues
in humans, facilitating experimental approaches (Scheffer
et al., 2000; Stephens et al., 2001).
Considering that doxorubicin is a substrate of both P-gp
and Mrp2 (Hidemuraet al., 2003; Speeg & Maldonado, 1994),
it is reasonable to speculate the effects of P-gp and Mrp2 on
hepatobiliary excretion of doxorubicin in EEC rats. However,
the protein expression of P-gp was already reported to be
comparable between the control and EEC rats (Muhlfeld
et al., 2003). Thus, the effect of Mrp2 for the hepatobiliary
excretion of doxorubicin (Muhlfeld et al., 2003) was
considered in this study. In addition, even though Mrp3 was
reported to increase in ECC rats (Ruiz et al., 2007), Mrp3 was
not involved for the elimination of doxorubicin (Zelcer et al.,
2001). Down-regulation of Mrp2 in the liver is known to
cause cholestatic liver injury via inhibition of biliary excre-
tion of bile acids (Borst & Elferink, 2002; Crocenzi et al.,
2001). Based on the decreased mRNA levels of Mrp2
(Jin et al., 2009), the elevated hepatic level of bile acids as
well as diminished bile flow rate appear to be responsible for
the reduction of Mrp2 in EEC rats (Table 1). Also CYP
3A4 was inactivated by EE as mechanism-based manner
(Lin et al., 2002). Thus, the present in vivo and in vitro studies
using rats might provide a meaningful forecast of the effect of
Table 4. Parameters on net hepatobiliary clearance of doxorubicin incontrol and EEC rats at steady state.
ParameterControl rats
(n¼ 4)EEC rats(n¼ 4)
Initial body weight (g) 235� 35.1 230� 54.1Final body weight (g) 269� 6.29 224� 4.79a
Css (mg mL�1) 0.106� 0.00499 0.103� 0.00603Bile flow rate (mL min�1 g liver�1) 3.62� 0.210 1.08� 0.0731a
Biliary excretion rate(mg min�1 kg�1)
3.59� 0.469 1.28� 0.145a
CLbile/plasma (mL min�1 kg�1) 33.9� 4.26 12.4� 1.14a
CLbile/liver (g min�1 kg�1) 3.37� 1.28 0.795� 0.312b
Concentration in liver (mg g�1) 0.596� 0.153 1.81� 0.487b
T/P 5.61� 1.38 17.4� 4.28b
Data are given as the mean� standard deviation (SD). EEC, 17a-ethynylestradiol-induced cholestasis; CSS, plasma concentration atsteady state; CLbile/plasma, apparent biliary clearance; CLbile/liver, netbiliary clearance; T/P, ratio of liver concentration/plasmaconcentration.
aEEC rats were significantly different (p50.001) from control rats.bEEC rats were significantly different (p50.01) from control rats.
Table 3. Parameters on biliary clearance of doxorubicin in control andEEC rats.
Parameter Control rats (n¼ 4) EEC rats (n¼ 4)
Initial body weight (g) 223� 25.9 220� 16.5Final body weight (g) 252� 9.30 228� 21.4a
Relative liver weight(g final body weight�1)
0.0405� 0.627 12.4� 0.479a
CLbile (mL min�1 kg�1) 37.9� 2.73 12.5� 0.509b
Data are given as the mean� standard deviation (SD). EEC, 17a-ethynylestradiol-induced cholestasis; CLbile, time-averaged biliaryclearance.
aEEC rats were significantly different (p50.05) from control rats.bEEC rats were significantly different (p50.01) from control rats.
Table 5. Km, Vmax and CLint for the disappearance of doxorubicin inhepatic microsomes from control and EEC rats.
ParameterControl rats
(n¼ 4)EEC rats(n¼ 4)
Km (mM) 20.6� 1.20 19.0� 4.41Vmax (nmol min�1 mg protein�1) 0.461� 0.0206 0.330� 0.0711a
CLint (mL min�1 mg protein�1) 0.0224� 0.00204 0.0175� 0.00269a
Data are given as the mean� standard deviation (SD). EEC, 17a-ethynylestradiol-induced cholestasis; Km, apparent Michaelis–Mentenconstant (the concentration at which the rate is one-half of the Vmax);Vmax, maximum velocity; CLint, intrinsic clearance.
aEEC rats were significantly different (p50.05) from control rats.
DOI: 10.3109/00498254.2013.783250 Pharmacokinetics of doxorubicin in cholestatic rats 905
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

EE-induced cholestasis on the pharmacokinetics of doxo-
rubicin with respect to the changes in Mrp2 and CYP3A
subfamily.
We first measured the in vivo pharmacokinetics of
doxorubicin after intravenous administration of its hydro-
chloride to control and EEC rats. The Ae0–24 hs of doxorubicin
were less than 1.83% of the dose in both groups of rats
(Table 2), suggesting that intravenous doxorubicin was almost
completely eliminated via the liver in rats. After intravenous
administration of doxorubicin hydrochloride, the significantly
greater AUC of doxorubicin in EEC rats was due to the
slower CL and CLNR than those in control rats (Table 2).
The significantly slower CLNR could be due to the decreased
biliary excretion (Figure 2 and Table 3) and hepatic metab-
olism of doxorubicin (Table 5) in EEC rats compared with
control rats.
To confirm the difference in the biliary excretion of
doxorubicin between control and EEC rats (Figure 2), we
measured the hepatobiliary clearance with continuous intra-
venous infusion. Hepatobiliary excretion consists of the
uptake from the sinusoidal side into the hepatocytes and
the efflux from the inside of the hepatocytes out into the
bile across the canalicular membrane. Since P-gp already
has been reported to be comparable between control and
cholestasis state and Mrp3 was not involved for the elimin-
ation of doxorubicin as mentioned above, Mrp2 activity in the
second step of hepatic biliary excretion was investigated in
this study. Both significantly slower CLbile/plasma and CLbile/
liver in EEC rats (Table 4) suggested that there is a difference
in doxorubicin transport ability via Mrp2 in hepatobiliary
excretion compared to control rats. As Mrp2 is located on the
bile canalicular membrane of hepatocytes (Hidemura et al.,
2003), Mrp2 might be included for the hepatobiliary excretion
of doxorubicin and the decreased mRNA levels of Mrp2
affected the reduced CLbile/liver of doxorubicin in EEC rats as
reported because the protein expression level of the trans-
porter determinates its function to a great degree (Jin et al.,
2009). Similarly, impairment in bile flow rate under
cholestasis was reported to be accompanied by down-
regulation of Mrp2 in the liver for the secretion of bile salts
and/or other bile constituents (Pauli-Magnus & Meier, 2005),
which plays an important role in elimination of drugs most
likely by biliary excretion (Borst & Elferink, 2002; Chan
et al., 2004; Vlaming et al., 2006). Furthermore, the organic
cation transporters as well as other unidentified phenomena
related to the uptake of doxorubicin seemed to be responsible
for the uptake of doxorubicin into the hepatocytes and affect
the hepatobiliary excretion (Okabe et al., 2005).
In aspect of the metabolic changes in doxorubicin in EEC
rats, the significantly slower CLNR of doxorubicin (Table 2)
could be due to the decreased CYP3A subfamily in EEC rats
(Lin et al., 2002). In in vitro hepatic microsomal studies,
the significant slower CLint was due to the decreased Vmax in
EEC rats (Table 5), indicating the maximum velocity for
the disappearance (primarily metabolism) of doxorubicin was
decreased in EEC rats because of the decreased CYP3A.
Since doxorubicin is a drug with a low hepatic extraction
ratio (50.24; Ballet et al., 1987), its hepatic clearance
(metabolism) depends on the hepatic intrinsic free drug
clearance (CL0int) for the disappearance of doxorubicin and
the free fraction of doxorubicin in the plasma, fu (Wilkinson
& Shand, 1975). The CL0int � fu is the intrinsic total drug
clearance. The significantly slower CLNR of doxorubicin in
EEC rats (Table 2) could have been supported by the slower
in vitro hepatic CLint for the disappearance of doxorubicin
(Table 4). The contribution of fu to CLint seemed to be
negligible because fus plasma were comparable between two
groups of rats. Thus, the decreased protein expression of
hepatic CYP3Asubfamily in EEC rats seemed to contribute
the changes in pharmacokinetics (including hepatic metabol-
ism) of doxorubicin in rats. Mottino et al. (2002) and Lin et al.
(2002) reported that EE reduced the Mrp2 and CYP3A
activities, respectively. These changes directly affected the
pharmacokinetic changes of doxorubicin: the decreased
biliary excretion of doxorubicin and bile flow rate by the
reduced Mrp2 activity and decreased CLint and increased
AUC (decreased CLNR) by the reduction of hepatic metab-
olism of doxorubicin via hepatic CYP3A.
The estimated CLR as fu of doxorubicin (CLR,fus) were
2.35 and 5.05 mL min�1 kg�1 in control and EEC rats,
respectively. These values, 2.35 and 5.05 mL min�1 kg�1,
were considerably slower than and close to the reported
glomerular filtration rate (as measured by creatinine clear-
ance), 5.24 mL min�1 kg�1, in rats (Davies & Morris, 1993).
The above data indicate that doxorubicin is reabsorbed in
rat renal tubules in control rats and excreted mainly via
glomerular filtration in ECC rats. In ECC rats, reabsorption
of doxorubicin was inhibited. The faster CLR,fu (by 115%) of
doxorubicin in EEC rats could be due to the up-regulated
Mrp2 in the kidney as a compensatory mechanism in
cholestatic state (Denk et al., 2004). Although the Ae0–24 h
values were almost negligible, Ae0-24 h and CLR in EEC rats
were significantly greater and faster than those in control rats,
respectively (Table 2), and these results support the compen-
satory mechanism of Mrp2 in the kidney.
In conclusion, the reduction of hepatic Mrp2 and CYP3A
subfamily causes the greater AUC (slower CLNR) of doxo-
rubicin in EEC rats due to the decreased biliary excretion
and hepatic metabolism of doxorubicin. Since a variety of
substrates are subjected to being transported via Mrp2 and/or
CYP3A subfamily, the regulation may have broader implica-
tions for the understanding of the altered pharmacokinetics
and/or pharmacologic effects of relevant substrate drugs
in experimental, as well as in clinical estrogen-induced
cholestasis.
Declaration of interest
This study was supported by the Dongguk University
Research Foundation Fund of 2010.
The authors declare that they have no conflicts of interest
to declare.
References
Ballet F, Vrignaud P, Robert J, et al. (1987). Hepatic extraction,metabolism and biliary excretion of doxorubicin in the isolatedperfused rat liver. Cancer Chemother Pharmacol 19:240–5.
Borst P, Elferink RO. (2002). Mammalian ABC transporters in healthand disease. Ann Rev Biochem 71:537–92.
Chan LM, Lowes S, Hirst BH. (2004). The ABCs of drug transportin intestine and liver: efflux proteins limiting drug absorption andbioavailability. Eur J Pharm Sci 21:25–51.
906 Y. H. Choi et al. Xenobiotica, 2013; 43(10): 901–907
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.

Chiou WL. (1978). Critical evaluation of the potential error inpharmacokinetic studies using the linear trapezoidal rule methodfor the calculation of the area under the plasma level–time curve.J Pharmacokinet Biopharm 6:539–46.
Choi YH, Kim SG, Lee MG. (2006). Dose-independent pharmacokin-etics of metformin in rats: hepatic and gastrointestinal first-passeffects. J Pharm Sci 95:2543–52.
Choi YH, Lee U, Lee BK, Lee MG. (2010). Pharmacokinetic interactionbetween itraconazole and metformin in rats: competitive inhibition ofmetabolism of each drug by each other via hepatic and intestinalCYP3A1/2. Br J Pharmacol 161:815–29.
Choi JS, Piao YJ, Kang KW. (2011). Effects of quercetin on thebioavailability of doxorubicin in rats: role of CYP3A4 and P-gpinhibition by quercetin. Arch Pharm Res 34:607–13.
Crocenzi FA, Sanchez Pozzi EJ, Pellegrino JM, et al. (2001). Beneficialeffects of silymarin on estrogen-induced cholestasis in the rat: a studyin vivo and in isolated hepatocyte couplets. Hepatology 34:329–39.
Cui Y, Konig J, Buchholz JK, et al. (1999). Drug resistance andATP-dependent conjugate transport mediated by the apical multidrugresistance protein, MRP2, permanently expressed in human andcanine cells. Mol Pharmacol 55:929–37.
Czeczuga-Semeniuk E, Solczynski S, Dabrowska M, et al. (2004).The effect of doxorubicin and retinoids on proliferation, necrosis andapoptosis in MCF-7 breast cancer cells. Folia Histochem Cytobiol 42:221–7.
Davies B, Morris T. (1993). Physiological parameters in laboratoryanimals and humans. Pharm Res 10:1093–5.
Denk GU, Soroka CJ, Takeyama Y, et al. (2004). Multidrug resistance-associated protein 4 is up-regulated in liver but down-regulated inkidney in obstructive cholestasis in the rat. J Hepatol 40:585–91.
Duggleby RG. (1995). Analysis of enzyme progress curves by nonlinearregression. Meth Enzymol 249:61–90.
Early Breast Cancer Trialists’ Collaborative Group. (2005). Effectsof chemotherapy and hormonal therapy for early breast cancer onrecurrence and 15-year survival: an overview of the randomised trials.Lancet 365:1687–717.
Eloranta ML, Heinonen S, Mononen T, Saarikoski S. (2001). Risk ofobstetric cholestasis in sisters of index patients. Clin Genet 60:42–5.
Gibaldi M, Perrier D. (1982). Pharmacokinetics. 2nd ed. New York:Marcel Dekker.
Hidemura K, Zhao YL, Ito K, et al. (2003). Shiga-like toxin II impairshepatobiliary transport of doxorubicin in rats by down-regulation ofhepatic P glycoprotein and multidrug resistance-associated proteinMrp2. Antimicrob Agents Chemother 47:1636–42.
Jin HE, Hong SS, Choi MK, et al. (2009). Reduced antidiabetic effectof metformin and down-regulation of hepatic Oct1 in rats withethynylestradiol-induced cholestasis. Pharm Res 26:549–59.
Key TJ. (1995). Hormones and cancer in humans. Mutat Res 333:59–67.Lee HJ, Lee MG. (1999). Effects of dexamethasone on the pharmaco-
kinetics of adriamycin after intravenous administration to rats.Res Commun Mol Pathol Pharmacol 105:87–96.
Lin HL, Kent UM, Hollenberg PF. (2002). Mechanism-based inactiva-tion of cytochrome P450 3A4 by 17 alpha-ethynylestradiol: evidencefor heme destruction and covalent binding to protein. J Pharmacol ExpTher 301:160–7.
Micheline D, Emmanuel J, Serge E. (2002). Effect of ursodeoxycholicacid on the expression of the hepatocellular bile acid transporters(Ntcp and bsep) in rats with estrogen-induced cholestasis. J PediatrGastroenterol Nutr 35:185–91.
Mottino AD, Cao J, Veggi LM, et al. (2002). Altered localization andactivity of canalicular Mrp2 in estradiol-17beta-D-glucuronide-induced cholestasis. Hepatology 35:1409–19.
Muhlfeld A, Kubitz R, Dransfeld O, et al. (2003). Taurine supplemen-tation induces multidrug resistance protein 2 and bile salt export pump
expression in rats and prevents endotoxin-induced cholestasis. ArchBiochem Biophys 413:32–40.
Okabe M, Unno M, Harigae H, et al. (2005). Characterization of theorganic cation transporter SLC22A16: a doxorubicin importer.Biochem Biophys Res Commun 333:754–62.
Pauli-Magnus C, Meier PJ. (2005). Hepatocellular transporters andcholestasis. J Clin Gastroenterol 39:S103–10.
Rajkumar L, Guzman RC, Yang J, et al. (2004). Prevention of mammarycarcinogenesis by short-term estrogen and progestin treatments.Breast Cancer Res 6:R31–7.
Rocha AB, Lopes RM, Schwartsmann G. (2001). Natural products inanticancer therpay. Curr Opin Pharmacol 1:364–9.
Rodriguez-Garay EA. (2003). Cholestasis: human disease and experi-mental animal models. Ann Hepatol 2:150–8.
Ruiz ML, Villanueva SSM, Luquita MG, et al. (2007). Beneficial effectof spironolatone administration on ethylestradiol-induced cholestasisin the rat: involvement of up-regulation of multidrug resistance-associated protein 2. Drug Metab Dispos 35:2060–6.
Savander M, Ropponen A, Avela K, et al. (2003). Genetic evidence ofheterogeneity in intrahepatic cholestasis of pregnancy. Gut 52:1025–9.
Scheffer GL, Kool M, Heijn M, et al. (2000). Specific detectionof multidrug resistance proteins MRP1, MRP2, MRP3, MRP5, andMDR3 P-glycoprotein with a panel of monoclonal antibodies. CancerRes 60:5269–77.
Schwarz EB, Hess R, Trussell J. (2009). Contraception for cancersurvivors. J Gen intern Med 24:401–6.
Sivaraman L, Stephens LC, Markaverich BM, et al. (1998). Hormone-induced refractoriness to mammary carcinogenesis in Wistar-Furthrats. Carcinogenesis 19:1573–81.
Smylie MG, Wong R, Mihalcioiu C, et al. (2007). A phase II, open label,monotherapy study of liposomal doxorubicin in patients withmetastatic malignant melanoma. Invest New Drugs 25:155–9.
Soucek P, Gut I. (1992). Cytochromes P-450 in rats: structures,functions, properties and relevant human forms. Xenobiotica 22:83–103.
Speeg KV, Maldonado AL. (1994). Effect of the nonimmunosuppressivecyclosporin analog SDZ PSC-833 on colchicine and doxorubicinbiliary secretion by the rat in vivo. Cancer Chemother Pharmacol 34:133–6.
Stephens RH, O’Neill CA, Warhurst A, et al. (2001). Kinetic profiling ofP-glycoprotein-mediated drug efflux in rat and human intestinalepithelia. J Pharmacol Exp Ther 296:584–91.
Suzuki T, Zhao YL, Nadai M, et al. (2006). Gender-related differences inexpression and function of hepatic P-glycoprotein and multidrugresistance-associated protein (Mrp2) in rats. Life Sci 79:455–61.
Trauner M, Arrese M, Soroka CJ, et al. (1997). The rat canalicularconjugate export pump (Mrp2) is down-regulated in intrahepatic andobstructive cholestasis. Gastroenterology 113:255–64.
Vlaming ML, Mohrmann K, Wagenaar E, et al. (2006). Carcinogen andanticancer drug transport by Mrp2 in vivo: studies using Mrp2(Abcc2) knockout mice. J Pharmacol Exp Ther 318:319–27.
Wilkinson GR, Shand DG. (1975). A physiological approach to hepaticdrug clearance. Clin Pharmacol Ther 18:377–90.
Yao K, Lee ES, Bentrem DJ, et al. (2000). Antitumor action ofphysiological estradiol on tamoxifem-simulated breast tumors grownin athymic mice. Clin Cancer Res 6:2028–36.
Zawaira A, Matimba A, Masimirembwa C. (2008). Prediction of sitesunder adaptive evolution in cytochrome P450 sequences and theirrelationship to substrate recognition sites. Pharmacogenet Genomics18:467–76.
Zelcer N, Saek T, Reid G, et al. (2001). Characterization of drugtransport by the human multidrug resistance protein 3 (ABCC3).J Biol Chem 276:46400–7.
DOI: 10.3109/00498254.2013.783250 Pharmacokinetics of doxorubicin in cholestatic rats 907
Xen
obio
tica
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n St
ate
Uni
vers
ity o
n 10
/26/
14Fo
r pe
rson
al u
se o
nly.



![Doxorubicin-induced cardiotoxicity is suppressed by ...levels of E2 and P4 in rats can be used as a proxy to identify the estrous stage [29]. The four sequential stages ... peutic](https://static.fdocument.org/doc/165x107/608a3c40950a1c68db795833/doxorubicin-induced-cardiotoxicity-is-suppressed-by-levels-of-e2-and-p4-in-rats.jpg)