DRUGS FOR BRONCHIAL ASTHMA - Medico...
13
DRUGS FOR BRONCHIAL ASTHMA DRUGS AFFECTING BRONCHIAL TONE SITES OF ACTION OF ANTI-INFLAMMATORY DRUGS IN ASTHMA
Transcript of DRUGS FOR BRONCHIAL ASTHMA - Medico...

DRUGS FOR BRONCHIAL ASTHMA
DRUGS AFFECTING BRONCHIAL TONE
SITES OF ACTION OF ANTI-INFLAMMATORY DRUGS IN ASTHMA

CLASSIFICATION OF DRUGS FOR ASTHMA A) Bronchodilators
1. Selective β2 receptor agonists: Salbutamol, Torbutaline, Salmeterol, Formoterol, Bambuterol
2. Non-selective sympathomimetics: Epinephrine, Ephedrine, Isoprenaline
3. Anti-cholinergics: Ipratropium, Tiotropium, Oxitropium
4. Methylxanthines: Teophylline, Aminophylline
B) Anti-Inflammatory Drugs
1. Corticosteroids i. Oral: Prednisone, Prednisolone, Methylprednisolone
ii. Parenteral: Methylprednisolone, Hydrocortisone iii. Inhalational: Beclomethasone, Fluticasone, Budesonide, Triamcinolone, Flunisolide
2. Mast cell stabilisers: Sodium cromoglycate, Nedocromil 3. Leukotriene modulators
i. 5-lipoxygenase inhibitor: Zileuton ii. Cysteinyl leukotriene receptor antagonists: Montelukast
4. Monoclonal anti-IgE antibody: Omalizumab 5. Miscellaneous: Nitric oxide donors
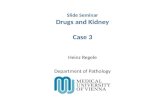
SELECTIVE β2 RECEPTOR AGONISTS
Short acting (short term relievers): Salbutamol, Terbutaline
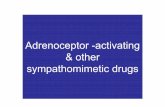
Long acting (long term prevention): Salmeterol, Formoterol, Bambuterol MOLECULAR MECHANISM OF AIRWAY SMOOTH MUSCLE RELAXATION Adrenergic drugs β2 receptors
Bronchial smooth Mast cells muscle cells ↑ CAMP production Bronchial relaxation ↓ mediators release ↓ inflammation
Adenylyl cyclase
stimulate

BENEFICIAL EFFECTS
Mainstay – reversible airway obstruction (asthma)
Caution – Blood pressure instability, ischaemic heart disease patients
Additional anti-inflammatory property (drawback desensitization due to down-regulation of β2 receptors)
Selectivity to β2 receptors minimal cardiac stimulation and minimal side effects
Inhaled medication targeted, more β2 selective and lessens systemic side effects
Improve mucociliary transport
Effective and fastest bronchodilator property SABA VS. LABA
SABA (Short acting β2 receptor agonists) LABA (Long acting β2 receptor agonists)
They bind to active site of β2 adrenoreceptor
Less lipid soluble
Early onset of action (<5 minutes), persists for 4-6 hours
Orally, inhalational (metered dose/dry powder/nebuliser), I.V. and I.M. route
Drug of choicefor acute attacks of asthma
Terbutaline is safe bronchodilator in pregnancy
They bind to active site and exo-site of β2 adrenoreceptor
Highly lipid soluble
Delayed onset
Inhalational and oral route
Indicated in nocturnal asthma and long-term prevention of asthma
ADVERSE EFFECTS
Minimal if inhaled (preferred)
Oral route Muscle tremors (direct + β2 in skeletal muscle) Tachycardia (chronotropic β2 and in high doses, β1 receptor is activated) Hyperglycaemia (↑ gluconeogenesis and ↑ glycogenolysis) Hypotension (peripheral vasodilatation)
Continued use Desensitization/down-regulation of receptors Diminished responsiveness to the previous dose Prevented by concurrent use of glucocorticoids (there is risk of ↓ K+)
Aerosol preparations – myocardial toxicity (fluorocarbons)

NON-SELECTIVE SYMPATHOMIMETICS
Epinephrine & Ephedrine (α & β)
Isoprenaline (β1 & β2)
Non-selective action cardiac side effects (↑ blood pressure, tachycardia, arrhythmia)
Epinephrine Can cause effective and rapid bronchodilatation Drug of choice for acute asthma till β1 agonists were available Rarely used due to cardiac side effects (tachycardia, hypertension, worsening of
angina, myocardial infarction and arrhythmias)
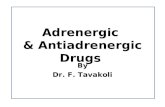
ANTI-CHOLINERGICS
Act as pharmacological antagonists of acetylcholine released from parasympathetic fibres
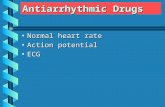
Ipratropium, Tiotropium & Oxitropium (aerosol) MOLECULAR MECHANISMS OF AIRWAY SMOOTH MUSCLE CONTRACTION
Acetylcholine acts on M3 receptor of airway smooth muscle cells and mucous glands ↓
Cause ↑in cGMP ↓
CGMP activates phospholipase C, PIP2 is converted into IP3 ↓
Release of Ca2+ from sarcoplasmic reticulum ↓
Bronchodilation ROLE IN ASTHMA
Less effective than selective β2 agonists
Also blocks M2 presynaptic autoreceptors (↑ acetylcholine release) ↓ Rx efficacy
Relieved by inhalational route (MDI, rotacaps, nebulizer)
Delayed onset of action (>30 minutes)
Poor absorption into systemic circulation (quartenary compounds)
Lacks classic anti-cholinergic side effects)
Additional to brochodilatory action, they also decrease mucous secretion (unlike atropine, lesser drying effect on mucous no mucous plugs)
No effect on late asthmatic response (inflammatory stage)
Second line drugs in moderate to severe asthma used as an adjuvant to β2 agonists/glucocorticoids (longer duration)
Action of acetylcholine is blocked by anti-
cholinergics, hence cause
bronchoconstriction

METHYLXANTHINES
Natural alkaloids: Caffeine, Theophylline, Theobromine
Beverages: coffee, tea, chocolate
Drugs: Theophylline, Aminophylline, Diprophylline
Mechanism of action: Inhibition of PDE-IV (eosinophils & mast cells) Inhibition of PDE-III (airway smooth muscle) Adenosine receptor inhibitor (bronchodilation)
Exhibits bronchodilatory + anti-inflammatory + immunomodulatory
Increase mucous clearance
Used in combination with β2 agonists – asthma and chronic obstructive pulmonary disease PHARMACOKINETICS OF THEOPHYLLINE
Absorption Well absorbed orally (sustained release preparation – SR)
Rectal absorption – suppositories (erratic)
Distribution
Distributed to all tissues
Crosses placenta
Secreted in milk
50% PPB (plasma protein binding)
Metabolism
Metabolized extensively in liver by CYP1A2 (>85%)
Metabolizing enzymes are saturable
At higher doses, first order kinetics (t1/2: 4-6 hours) zero order kinetics disproportionate ↑ plasma concentration
Prolongation of t1/2: 60 hours
Excretion Unchanged in urine (10%)
Elimination rate is variable
Varies according to age, comorbidities and concurrent medications
FACTORS AFFECTING ELIMINATION RATE (CLEARANCE) OF THEOPHYLLINE
Faster elimination Slower elimination
Children (t1/2: 3-5 hours)
Smoking
Cystic fibrosis
Hyperthyroidism
Adults (t1/2: 7-12 hours)
Elderly >60 years
Premature infants
Hypothyroidism
Cirrhosis
Congestive heart failure
Febrile viral illness, pneumonia
↓ breakdown of CAM ↑ cAMP

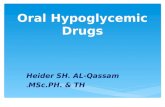
ADVERSE EFFECTS OF METHYLXANTHINES
Has a narrow safety margin (therapeutic window)
Therapeutic plasma range: 10-20 µg/ml
Dose dependent toxicity: >20 µg/ml
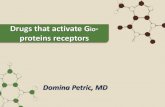
Systems affected: GIT, CNS and CVS Relationship between plasma concentration of
theophylline to its effects
Toxic effect
Therapeutic effect
Sub-therapeutic effect
>60 µg/ml: death
>40 µg/ml: seizures, diuresis, fever, arrhythmias
>30 µg/ml: tachypnoea, flush, hypotension
>20 µg/ml: nausea, vomiting
DRUG INTERACTIONS WITH THEOPHYLLINE 1) Agents which ↑ CYP1A2 (enzyme inducers) decrease theophylline concentration
Drugs: Phenytoin, Rifampicin, Phenobarbitone, Carbamazepine
Charcoal broiled meat
Smoking 2) Agents that inhibit theophylline metabolism
Drugs: Erythromycin, Ciprofloxacin, Cimetidine, Oral contraceptives, Allopurinol 3) Theophylline enhances the effects of sympathomimetics, digitalis, furosemide, hypoglycaemic
agents, oral anticoagulants THERAPEUTIC USES OF METHYLXANTHINES
Management of bronchial asthma
Treat chronic obstructive pulmonary disease (COPD)
Dyspnoea associated with pulmonary oedema that develops from congestive heart failure DRUGS FOR MANAGING “LATE ASTHMATIC RESPONSE” WITH ANTI-INFLAMMATORY PROPERTY Mainly a prophylactic role – “controllers of symptoms”
Corticosteroids: Systemic & Inhalational
Mast cell stabilizers : Inhalational
Leukotriene (LT) modulators : Oral
Anti-IgE antibody: S.C. / I.V.
20
10
0
Plasma conc.
(µg/ml)

CORTICOSTEROIDS
Inhaled/Systemic corticosteroids mainstay for Rx of moderate to severe asthma – “preventers” of attack
Anti-inflammatory and immunosuppressant
↓ mucosal oedema & bronchial hyper reactivity to allergens
Symptomatic reliefs, improve airflow, retard disease progression, reduce asthma exacerbations
Long term – adverse effects with oral CS are worse than asthma itself, tapering dose essential
Prophylaxis and treatment of seasonal and perennial allergy DRUGS
Oral: Prednisone, Prednisolone, Methylprednisolone
Parenteral: Methylprednisolone, Hydrocortisone
Inhalational: Beclomethasone, Fluticasone, Budesonide, Triamcinolone, Flunisolide, Ciclesonide
ROUTES OF ADMINISTRATION
Inhalation: ↑ topical action, ↓airway remodeling, ↓inflammation, long term treatment of asthma & COPD (combination with SABA/LABA)
Systemic: Severe chronic asthma when not controlled by other drugs – shift to inhaled steroid Following severe acute asthma (7-10 days) – oral corticosteroids Status asthmaticus – start with I.V., then switch to oral
Intranasal spray: Allergic rhinitis, nasal polyposis ADVERSE EFFECTS
Inhalational: dryness of mouth, voice changes & oral candidiasis
Ciclesonide: higher topical:systemic ratio
Oral: short courses (<2 weeks) – no HPA (hypothalamic-pituitary-adrenal) axis
Parenteral: used during status asthmaticus only for a brief period oral route (Hydrocortisone hemisuccinate)

MAST CELL STABILIZERS
Sodium cromoglycate & Nedocromil sodium (inhalation)
Inhibit degranulation of mast cells (all inflammatory cells)
Inhibit release of histamine, leukotrienes, platelet activating factor, interleukins
Prevent bronchospasm/asthma by allergens
Decrease frequency and severity of attacks
Effect over 4 weeks and lasts 2 weeks after discontinuation MECHANISM OF ACTION
THERAPEUTIC USES
Prophylaxis of chronic & seasonal asthma: long term in mild to moderate cases (not in acute)
Prophylaxis allergic rhinitis (nasal spray)
Allergic conjunctivitis (eye drops)
Preferred in patient having multiple allergic disorders ADVERSE EFFECTS
Inhalational: least systemic side effects
Cromoglycate inhalation: throat irritation, cough, arthralgia, headache
Mast cell degranulation

LEUKOTRIENE ANTAGONIST
Zileuton – blocks leukotriene receptor & leukotriene synthesis
Montelukast, Zafirlukast – leukotriene receptor blocker
Antagonise – leukotriene receptor mediated actions like bronchospasm, eosinophil accumulation in lung, bronchus inflammation, hyper reactivity
THERAPEUTIC USES
Prophylactic treatment of mild to moderate asthma as adjuvants with inhaled corticosteroids or selective β2 agonists
Prophylaxis in severe asthma: permit reduction in steroid dose, rescue β2 inhalation
Effective in aspirin induced asthma ADVERSE EFFECTS
Gastrointestinal distress, headache, rashes, eosinophilia
Churg-Strauss syndrome (vasculitis with eosinophilia)
Zileuton: hepatotoxic
MONOCLONAL ANTI-IGE ANTIBODY
The allergic cascade is interrupted by omalizumab
Omalizumab is a monoclonal antibody
It neutralizes free IgE in circulation
Little IgE available to bind mast cell to release mediators
Reserved for resistant asthma cases
Not useful for acute attacks or status asthmaticus
High cost limits its use as first line drug

DRUGS & DEVICES USED FOR ADMINISTRATION
INHALATIONAL DRUGS
β2 agonists: Salbutamol, Terbutaline, Salmeterol, Formoterol
Anti-cholinergics: Ipratropium, Tiotropium
Mast cell stabilizer: Cromoglycate
Glucocorticoids DRUG PARTICLE SIZE
Large particles – settle on oropharynx
1-5µm diameter – deposits on bronchioles
Very fine particles are exhaled out
Slow and deep inbreathing & hold the breath after inhalation * Inhalation devices: 10% drug reaches lung AEROSOLS
Drug in solution Metered dose inhaler (MDI) Nebulizer
Dry powder inhalers Rotahaler Spinhaler/Twisthaler
METERED DOSE INHALER (MDI)
Actuation – coordination with deep inspiration
Device – carried along, convenient
Improve drug delivery: spacer, face mask
Don’t require synchronized coordination with inspiration

Advantages of using a spacer
Improves drug delivery
Does not require synchronized coordination with inspiration
Increases inhaled to swallowed drug ratio
Decreases deposition of larger particles in the mouth (candidiasis) NEBULIZER
Produces mist of drug solution by pressurized air or O2
Inhaled through mouthpiece or face mask
Used at bed side
Severe episodes of asthma – kids and elderly
More drugs can be mixed simultaneously
ROTAHALER
Rotacap – capsule containing drug
Punctured while rotating the cap
Drug is aerosolized by inspiratory air flow
Requires high velocity of airflow (kids, elderly and sick patients)
Powder – irritate, cough, spasm SPINHALER/TWISTHALER
Keep drug
Use it
Reset to use again

STATUS ASTHMATICUS
Hydrocortisone hemisuccinate 100 mg I.V., followed by 100 mg 4th hourly infusion
Nebulized salbutamol (5 mg) + ipratropium (0.5 mg)
Salbutamol 4 mg I.M. (inhaled drug don’t reach smaller bronchi – severe narrowing/plugging)
High flow humidified oxygen inhalation
Intubation & mechanical ventilation
Sodium bicarbonate + saline – correct dehydration
Antibiotics – treat infection
ASTHMA SEVERITY CLASSIFICATION
Clinical course, severity
Daytime asthma symptoms
Night time awakenings
FEV1, PEF
Intermittent <1/week 2 and <2/month >80% predicted. Daily
variability <20%
Mild persistent ≥1/week but not daily >2/month >80% predicted. Daily variability is 20-30%
Moderate persistent Daily >1/week >60% but <80% predicted.
Variability >30%
Severe persistent Persistent, which limit
normal activity Daily
<60% predicted. Variability >30%

CHOICE OF DRUG FOR MANAGEMENT OF VARIOUS TYPES OF ASTHMA
Step-wise guidelines are recommended
After asthma control for 3-6 months, reduction of medication stepwise
Types Steps Drug therapy
Seasonal asthma – Regular inhaled: cromoglycates or low dose
steroids
Episodes: inhaled SABA
Mild episodic asthma Step 1
Inhaled SABA
Mild chronic asthma with occasional exacerbation
Step 2
Regular inhaled: cromoglycates or low dose steroids
Moderate asthma with frequent
Step 3
↑ dose inhaled corticosteroids + LABA
Additional: theophylline
Severe asthma Step 4 High doses inhalational corticosteroids + LABA
Additional: Leukotriene antagonist/oral theophylline/oral β2 agonist/inhaled ipratropium
Not controlled severe asthma
Step 5
High inhaled steroid + LABA
Add oral steroid