Dr.T.V.Rao MD ANTIBIOTICS USE, MISUSE, CONSEQUENCES DR.T.V.RAO MD 1.
86
Dr.T.V.Rao MD ANTIBIOTICS USE, MISUSE, CONSEQUENCES DR.T.V.RAO MD 1
-
Upload
nikolas-worland -
Category
Documents
-
view
227 -
download
5
Transcript of Dr.T.V.Rao MD ANTIBIOTICS USE, MISUSE, CONSEQUENCES DR.T.V.RAO MD 1.

Dr.T.V.Rao MD
ANTIBIOTICS USE, MISUSE, CONSEQUENCES
DR.T.V.RAO MD 1

WHAT IS A ANTIBIOTIC• Antibiotic (from the Ancient Greek: ντί – ἀ
anti, "against", and βίος – bios, "life") is a substance or compound that kills bacteria or inhibits its growth. Antibiotics belong to the broader group of antimicrobial compounds, used to treat infections caused by microorganisms, including fungi and protozoa .
DR.T.V.RAO MD 2

• The word antibiotic came from the word antibiosis a term coined in 1889 by Louis Pasteur's pupil Paul Vuillemin which means a process by which life could be used to destroy life
EARLY DEFINITION OF ANTIBIOTIC
DR.T.V.RAO MD 3

BEGINNING OF ANTIBIOTICS WITH DISCOVERY OF PENICILLIN
• The discovery of penicillin has been attributed to Scottish scientist Alexander Fleming in 1928 and the development of penicillin for use as a medicine is attributed to the Australian Nobel Laureate Howard Walter Florey
DR.T.V.RAO MD 4

FLEMING AND PENICILLIN
DR.T.V.RAO MD 5

• Antibiotic: Chemical produced by a microorganism that kills or inhibits the growth of another microorganism
• Antimicrobial agent: Chemical that kills or inhibits the growth of microorganisms
ANTIBIOTIC/ANTIMICROBIAL AGENT
DR.T.V.RAO MD 6

• The word antibiotic came from the word antibiosis a term coined in 1889 by Louis Pasteur's pupil Paul Vuillemin which means a process by which life could be used to destroy life
EARLY DEFINITION OF ANTIBIOTIC
DR.T.V.RAO MD 7

SELMAN WAKSMAN The term "antibiotic"
was coined by Selman Waksman in 1942 to describe any substance produced by a microorganism that is antagonistic to the growth of other microorganisms in high dilution
DR.T.V.RAO MD 8

DISCOVERY OF PENICILLIN AWARDED NOBEL PRIZE
DR.T.V.RAO MD 9

Brief History of Antibiotics• 1928- Penicillin discovered by Fleming
• 1932- Sulfonamide antimicrobial activity discovered {Erlich}•
• 1943- Drug companies begin mass production of penicillin
• 1948- Cephalosporins precursor sent to Oxford for synthesis
• 1952- Erythromycin derived from Streptomyces erythreus
• 1956- Vancomycin introduced for penicillin resistant staphylococcus
• 1962- Quinolone antibiotics first discovered
• 1970s- Linezolid discovered but not pursued
• 1980s- Fluorinated Quinolones introduced, making then clinically useful
• 2000- Linezolid introduced into clinical practiceDR.T.V.RAO MD 10

Antibiotic natural source first description as anti-infective drug
discoverer
sulfanilamide (prontosil 1932
1941
G.Domagk
penicillin Penicillium notatum A.Fleming, Florey, Chain
streptomycin Streptomyces griseus 1944 S.A.Waksman
cephalosporin Cephalosporium acremonium 1945 G.Brotzu
bacitracin Bacillus subtilis 1945
B.A.Johnson
chloramphenicol Streptomyces venezuellae 1947 I.Ehrlich
polymyxin Bacillus polymyxa 1947 C.G.Ainsworth
chlortetracyclin Streptomyces aureofaciens 1948 B.M.Duggar
neomycin Streptomyces fradiae 1949
S.A.Waksman
oxytetracyclin Streptomyces rimosus 1950 A.C.Finlay
DR.T.V.RAO MD 11

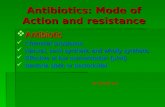
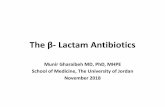
1920 1930 1940 1950 1960 1970 1980 1990 2000
ertapenem
tigecyclin daptomicin linezolid
telithromicin quinup./dalfop. cefepime ciprofloxacin aztreonam norfloxacin imipenem cefotaxime clavulanic ac. cefuroxime gentamicin cefalotina nalidíxico ac. ampicillin methicilin vancomicin rifampin chlortetracyclin streptomycin pencillin G prontosil
The development
of anti-infectives …
Development of anti-microbials
DR.T.V.RAO MD 12

• Bacteriostatic - Antimicrobial agents that reversibly inhibit growth of bacteria are called as bacteriostatic (Tetracycline's, Chloramphenicol )
• Bactericidal – Those with an irreversible lethal action on bacteria are known as bactericidal ( Penicillin, Isoniazid )
DEFINITION
DR.T.V.RAO MD 13

• Antimicrobial agents – that are produced synthetically but have action similar to that of antibiotics and are defined as chemotherapeutic agents
• Eg Sulphonamides, Quinolones.
CHEMOTHERAPEUTIC AGENTS
DR.T.V.RAO MD 14

IDEAL ANTIBIOTIC Toxic to microbes, and not to humans Bactericidal rater than bacteriostatic Effective against broad range of bacteria Should not be allergic and hypersensitive
reactions Should be active in plasma, and other body
fluids Desired levels should be reached rapidly and
maintained for adequate period of time. Should not give drug resistance, long shelf life, Cheaper
DR.T.V.RAO MD 15

• Drugs differ on their capabilities to act at different sites on bacteria.
• Some drugs have more than one site of action
HOW DRUGS ACT
DR.T.V.RAO MD 16

RESISTANCE AND SUSCEPTIBILITY
• Determined by in vitro activity, pharmacologic characteristics, and clinical evaluation.
• The minimal inhibitory concentration (MIC) can be comfortably exceeded by doses tolerated by the patient.
•Susceptible - implies their MIC is at a concentration attainable in the blood or other body fluid at the recommended dose.
•Resistant - MIC is not exceeded by normally attainable levels
DR.T.V.RAO MD 17

MAJOR MECHANISMS OF ANTIMICROBIAL DRUGS
• 1 Inhibition of cell wall synthesis• 2 Inhibition of cell membrane function• 3 Inhibition of protein synthesis ( inhibition
of translation and transcription of genetic material)
• 4 Inhibition of nucleic acid synthesis.
DR.T.V.RAO MD 18

Inhibition of cell wall synthesis
Target: block peptidoglycan (murein) synthesis
Peptidoglycan
Polysaccharide (repeating disaccharides of N-acetyl glucosamine and N-acetylmuramic acid) + cross-linked pentapeptide
Pentapeptide with terminal D-alanyl-D-alanine unit required for cross-linking
Peptide cross-link formed between the free amine of the amino acid in the 3rd position of the peptide & the D-alanine in the 4th position of another chain
DR.T.V.RAO MD 19

Inhibition of cell wall synthesis
.A -lactam antibiotics
inhibit transpeptidation reaction (3rd stage) to block peptidoglycan synthesis involves loss of a D-alanine from the pentapeptide
Steps:
a. binding of drug to PBPs
b. activation of autolytic enzymes (murein hydrolases) in the cell wall
c. degradation of peptidoglycan
d. lysis of bacterial cell
DR.T.V.RAO MD 20

Inhibition of cell wall synthesis
.A -lactam antibiotics
Penicillin binding proteins (PBPs)
enzymes responsible for:
a. cross-linking (transpeptidase)
b. elongation (carboxypeptidase)
c. autolysis
DR.T.V.RAO MD 21

Inhibition of cell wall synthesis
.A -lactam antibiotics
Lysis of bacterial cell
o Isotonic environment cell swelling rupture of bacterial cell
o Hypertonic environment – microbes change to protoplasts (gram +) or spheroplasts (gram -) covered by cell membrane swell and rupture if placed in isotonic environment
DR.T.V.RAO MD 22

PENICILLINS AND CEPHALOSPORINS
Pencillin and cephalosporins act inhibiting Trans peptidases, the enzyme catalyses the final linking step in synthesis of peptidoglycan.
Due to this reason Pencillin in bactericidal for grwoing bacteria since new peptidoglycan is synthesized at that stage only.
In nongrwoing cells pencillin is inactive An intact beta – lactum is essential for
antibacterial activity of pencillinsDR.T.V.RAO MD 23

CLASSIFICATION OF PENCILLINS• Natural
Benzyl penicillin
Phenoxymethyl penicillin Penicillin v
Semi synthetic and pencillase resistant
1 Methicillin 2 Nafcillin 3 Cloxacillin 4 Oxacillin 5 Floxacillin
DR.T.V.RAO MD 24

PENICILLINASE (B LACTAMASE)
Figure 20.8DR.T.V.RAO MD 25

• Penicilinase-resistant penicillins
• Carbapenem: very broad spectrum
• Monobactams: Gram negative
• Extended-spectrum penicillins
• Penicillins + -lactamase inhibitors
SEMI SYNTHETIC PENICILLINS
DR.T.V.RAO MD 26

OTHER INHIBITORS OF CELL WALL SYNTHESIS
• Cephalosporins• 2nd, 3rd, and 4th
generations more effective against gram-negatives
Figure 20.9DR.T.V.RAO MD 27

EXTENDED SPECTRUM PENCILLINS
Aminopencillins - Ampicillin, Amoxycillin Carboxypencillins – Carbencillin, Ticarcillin Ureidopencillin - PiperacillinResistance to penicillin is due to pencillinase commonly
called as ßlactamaseThe enzyme opens Betalactum ring hydrolytically and thus
converts the antibiotic to inactive pencillonic acid.
DR.T.V.RAO MD 28

• Clavulinic acid which is a product of Strept.clavuligerus
• Acts against the Staphylococcal beta ßlactamase.
• And plasmid mediated Betalactamase of Gram negative bacteria.
• Salbactum – this is a semisyntetic sulfone derivative with weak antibacterial activity
INHIBITORS TO BETALACTAMASE
DR.T.V.RAO MD 29

• Like penicillin acts similar
• Products of the molds of genus Cephalosporium except cefoxilin
• Divided into 4 generation of Cephalosporins depending on the spectrum of activity.
CEPHALOSPORINS
DR.T.V.RAO MD 30

• Cephalosporins are grouped into "generations" based on their spectrum of antimicrobial activity. The first Cephalosporins were designated first generation while later, more extended spectrum Cephalosporins were classified as second generation Cephalosporins.
DIFFERENT GENERATIONS OF CEPHALOSPORINS
DR.T.V.RAO MD 31

Cephalosporins are divided into 3 generations:
1st generation: Cephelexin, cefadroxil, cephradine
2nd generation: Cefuroxime, cefaclor
3rd generation: cefotaxime, Ceftazidime, cefixime - these give the best CNS penetration
4th and 5th generation Cephalosporins are already available
MAJOR GENERATIONS OF CEPHALOSPORINS
DR.T.V.RAO MD 32

• Cephalosporins are grouped into "generations" based on their spectrum of antimicrobial activity. The first cephalosporins were designated first generation while later, more extended spectrum cephalosporins were classified as second generation cephalosporins.
BASIS OF GENERATIONS IN CEPHALOSPORINS
DR.T.V.RAO MD 33

• Each newer generation of cephalosporins has significantly greater gram-negative antimicrobial properties than the preceding generation, in most cases with decreased activity against gram-positive organisms. Fourth generation cephalosporins, however, have true broad spectrum activity
ADVANTAGES WITH NEWER GENERATIONS
DR.T.V.RAO MD 34

• Imipenem: a carbapenem with a broader spectrum of activity against Gram positive and negative aerobes and anaerobes. Needs to be given with cilastatin to prevent inactivation by the kidney.
OTHER DRUGS
DR.T.V.RAO MD 35

• Quinolones are the first wholly synthetic antimicrobials. The commonly used Quinolones.
• Act on the DNA gyrase which prevents DNA polymerase from proceeding at the replication fork and consequently stopping synthesis.
QUINOLONES
DR.T.V.RAO MD 36

• Aminoglycosides are group of antibiotics in which amino sugars liked by glycoside bonds
• Eg Streptomycin,
• Act at the level of Ribosome's and inhibits protein synthesis
• Other Aminoglycosides –
Gentamycin, neomycins,paromomycins,tobramycins Kanamycins and spectinomycins
AMINOGLYCOSIDES
DR.T.V.RAO MD 37

DR.T.V.RAO MD 38

• Broad spectrum antibiotic produced by Streptomyces species
• 1. Oxytetracycle, chlortetracycle and tetracycline
• Tetracyclnes are bacteriostatic drugs inhibits rapidly multiplying organisms
• Resistance develops slowly and attributed to alterations in cell membrane permeability to enzymatic inactivation of the drug
TETRACYCLINE'S
DR.T.V.RAO MD 39

• Chloramphenicol is bacteriostatic drug
• Can produce bone marrow depression
• Chloramphenicol interferes with protein synthesis.
CHORAMPHENICOL
DR.T.V.RAO MD 40

• Contain macro cyclic lactone ring Erythromycin. Is popularly used drug
• Other drugs Roxithromycin,Azithromycin
• Inhibits the protein synthesis.
• Used as alternative to pencillin allergy patients.
MACROLIDES,AZALIDES,KETOLIDES
DR.T.V.RAO MD 41

DR.T.V.RAO MD 42

• Lincomycins
Clindamycin resembles Macrolides in biting site and antimicrobial activity.
Streptogramins
Quinpristin / dalfopristin
useful in gram positive bacteria
OTHER ANTIMICROBIAL AGENTS
DR.T.V.RAO MD 43

• Major anaerobes – Anaerobic cocci, clostridia and Bactericides are susceptible to Benzyl pencillin
• Bact.fragilis as well as many other anaerobes are treatable with Erythromycin,Lincomycin, tetracycline and Chloramphenicol
• Clindamycin is effective against many strains of Bacteroides
ANTIBIOTICS IN ANAEROBES
DR.T.V.RAO MD 44

• Since the discovery of Metronidazole in 1973 since then it was identified as leading agent anaerobes.
• But also useful in treating parasitic infections
Trichomonas, Amoebiasis and other protozoan infections.
METRONIDAZOLE IN ANAEROBIC INFECTIONS
DR.T.V.RAO MD 45

• Since the discovery of Metronidazole in 1973 since then it was identified as leading agent anaerobes.
• But also useful in treating parasitic infections
Trichomonas, Amoebiasis and other protozoan infections.
METRONIDAZOLE IN ANAEROBIC INFECTIONS
DR.T.V.RAO MD 46

• Other beta-lactams include:
• Aztreonam: a monocytic beta-lactam, with an antibacterial spectrum which is active only against Gram negative aerobes, including Pseudomonas aeruginosa, Neisseria meningitidis and N. gonorrhoea.
OTHER BETA-LACTAMS INCLUDE
DR.T.V.RAO MD 47

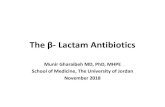
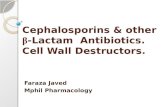
Emergence of Antibiotic-Resistant Bacteria
Cohen; Science 1992;257:1050
Gram-negative rods
Enterococcus sp.
N. gonorrhoeae
H. influenzae
M. catarrhalis
S. pneumoniae
1950 1960 1970 1980 1990
S aureus
Penicillin
Ampicillin
3rd gen Cephalosporins
Quinolones
DR.T.V.RAO MD 48

DR.T.V.RAO MD 49

ANTIBIOTIC RESISTANCE Antibiotic resistance is the ability of a micro organism
to withstand the effects of antibiotics. It is a specific type of drug resistance. Antibiotic resistance evolves naturally via natural selection acting upon random mutation, but it can also be engineered by applying an evolutionary stress on a population. Once such a gene is generated, bacteria can then transfer the genetic information in a horizontal fashion (between individuals) by plasmid exchange.
DR.T.V.RAO MD 50

ANTIBIOTIC PRESSURE AND RESISTANCE IN BACTERIA
WHAT IS IT ?
• ”Selection pressure of antibiotics has led to the emergence of antibiotic-resistant bacteria.”
• Antibiotics can effect bacteria unrelated to the targeted infectious agent; these may be “normal” flora, leading to the emergence of resistant mutants inhabiting the same environment.
Baquero et al., International Report 1996;23:819DR.T.V.RAO MD 51

• All antibiotics do NOT kill bacteria in the same way.
• Various classes of antibiotics work on different aspects of bacterial replication.
ANTIBIOTIC PRESSURE AND RESISTANCE IN BACTERIA
HOW DOES IT OCCUR?
DR.T.V.RAO MD 52

RESISTANCE AND SUSCEPTIBILITY
• Determined by in vitro activity, pharmacologic characteristics, and clinical evaluation.
• The minimal inhibitory concentration (MIC) can be comfortably exceeded by doses tolerated by the patient.
• Susceptible - implies their MIC is at a concentration attainable in the blood or other body fluid at the recommended dose.
• Resistant - MIC is not exceeded by normally attainable levels
DR.T.V.RAO MD 53

DR.T.V.RAO MD 54

• In spite discovery of several antibiotics several microorganisms attained resistance.
• The major factor contributing to persistence of infectious disease has been the tremendous capacity of microorganisms for circumventing the action of inhibitory drugs.
• The drug resistance continues to be a threat for usefulness of the chemotherapeutic agents.
DRUG RESISTANCE
DR.T.V.RAO MD 55

RESISTANCE
ORIGIN OF DRUG RESISTANCE
NON-GENETIC
1. Metabolically inactive organisms may be phenotypically resistant to drugs – M. tuberculosis
2. Loss of specific target structure for a drug for several generations
3. Organism infects host at sites where antimicrobials are excluded or are not active – aminoglycosides (e.g. Gentamicin) vs. Salmonella enteric fevers (intracellular)
DR.T.V.RAO MD 56

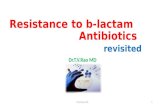
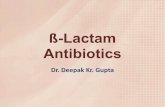
Folic acid synthesis
ß-lactams & Glycopeptide (Vancomycin)
50 50 5030 30 30
DNA
mRNA
Ribosomes
PABA
DHFA
THFA
Cell wall synthesis
DNA gyrase
Quinolones
Protein synthesis inhibition
Protein synthesis inhibitionTetracycline's
Protein synthesis mistranslation
Macrolides & Lincomycins
Cohen. Science 1992; 257:1064
DNA-directed RNA polymerase
Rifampin
Aminoglycosides
Sulfonamides
Trimethoprim
DR.T.V.RAO MD 57

• The resistant strains arise either by mutation and selection or by genetic exchange in which sensitive organisms receive the genetic material ( part of DNA) from the resistant organisms and the part of DNA carries with it the information of mode of inducing resistance against one or multiple antimicrobial agents.
ORIGIN OF DRUG RESISTANT STRAINS
DR.T.V.RAO MD 58

< Inappropriate specimen selection and collection
< Inappropriate clinical tests
< Failure to use stains/smears
< Failure to use cultures and susceptibility tests
Practices Contributing to Misuse of Antibiotics
DR.T.V.RAO MD 59

< Use of antibiotics with no clinical indication (eg, for viral infections)
< Use of broad spectrum antibiotics when not indicated
< Inappropriate choice of empiric antibiotics
Inappropriate Antibiotic Use
DR.T.V.RAO MD 60

< Inappropriate dose - ineffective concentration of antibiotics at site of infection
< Inappropriate route - ineffective concentration of antibiotics at site of infection
< Inappropriate duration
Inappropriate Drug Regimen
DR.T.V.RAO MD 61

ANTIBIOTIC RESISTANCE Antibiotic resistance is a specific type of drug
resistance when a microorganism has the ability of withstanding the effects of antibiotics. Antibiotic resistance evolves via natural selection acting upon random mutation, but it can also be engineered by applying an evolutionary stress on a population. Once such a gene is generated, bacteria can then transfer the genetic information in a horizontal fashion (between individuals) by conjugation, transduction, or transformation.
DR.T.V.RAO MD 62

PLASMIDS • Plasmid seem to be ubiquitous in bacteria, May encode genetic
information for properties
1 Resistance to Antibiotics
2 Bacteriocins production
3 Enterotoxin production
4 Enhanced pathogen city
5 Reduced Sensitivity to
mutagens
6 Degrade complex organic molecules
DR.T.V.RAO MD 63

RESISTANCE TRANSFER FACTORRTF
Plasmids – helps to spread multiple drug resistance Discovered in 1959 Japan Infections caused due to Shigella spread resistance to
following Antibiotics Sulphonamides Streptomycin Choramphenicol, Tetracycline
DR.T.V.RAO MD 64

RTF Shigella + E.coli
excreted in the stool resistant to several drugs in vivo and vitro
Plasmid mediated –transmitted by Conjugation
Episomes spread the resistance
DR.T.V.RAO MD 65

TRANSPOSONS AND R FACTOR
R forms may have evolved as a collection of Transposons
Each carrying Genes that confers resistance to one or several Antibiotics
Seen in Plasmids, Microorganisms AnimalsLaboratory Manipulations are called as Genetic
Engineering
DR.T.V.RAO MD 66

• If a bacterium carries several resistance genes, it is called multiresistant or, informally, a superbug. The term antimicrobial resistance is sometimes use to explicitly encompass organisms other than bacteria
MULTI DRUG RESISTANT PATHOGENS
DR.T.V.RAO MD 67

• Resistance arises due to Biochemical changes
Increased synthesis of drug antagonist
Decreased permeability to drug
Increased destruction of inhibitor
BIOCHEMICAL MECHANISMS OF DRUG RESISTANCE
DR.T.V.RAO MD 68

Mutation
• Usually one drug
• Low degree of resistance
• Increasing dose can benefit
• Prevented by combination of drugs
• Low virulence of bacteria
Transferable
• Multiple drugs
• High degree of resistance
• Increasing dose do not benefit
• Can not be prevented by combination of drugs
• High virulence of bacteria
DIFFERENTIATION OF MUTATION AND TRANSFERABLE DRUG RESISTANCE
DR.T.V.RAO MD 69

PLASMID MEDIATED DRUG RESISTANCE
Sulphonamides --- Reduce permeability
Erythromycin ---- Modification of ribosome's
Tetracyclnes ----- Reduced permeability
Chloramphenicol ---- Acetylation of drug
Streptomycin ----- Adenylation of drug
Pencillin ----- Hydrolysis of lactum ring
DR.T.V.RAO MD 70

• Many antibiotic resistance genes reside on plasmids facilitating their transfer. If a bacterium carries several resistance genes, it is called multiresistant or, informally, a superbug. The term antimicrobial resistance is sometimes used to explicitly encompass organisms other than bacteria
ANTIBIOTICS RESISTANCE AND PLASMIDS
DR.T.V.RAO MD 71

• Antibiotic resistance has become a serious problem in both developed and underdeveloped nations. By 1984 half of those with active tuberculosis in the United States had a strain that resisted at least one antibiotic. In certain settings, such as hospitals and some childcare location
ANTIBIOTIC RESISTANCE THREAT TO HUMANS AND ANIMALS
DR.T.V.RAO MD 72

BETWEEN 1962 AND 2000, NO MAJOR CLASSES OF ANTIBIOTICS WERE INTRODUCED
Fischbach MA and Walsh CT Science 2009 DR.T.V.RAO MD 73

EXTENDED-SPECTRUM Β-LACTAMASES
• β-lactamases capable of conferring bacterial resistance to
• the penicillins
• first-, second-, and third-generation cephalosporins
• aztreonam
• (but not the cephamycins or carbapenems)• These enzymes are derived from group 2b β-lactamases (TEM-1, TEM-2, and
SHV-1)
• differ from their progenitors by as few as one AADR.T.V.RAO MD 74

CARBAPENEMASES• Ability to hydrolyze penicillins, cephalosporins, monobactams,
and carbapenems• Resilient against inhibition by all commercially viable ß-
lactamase inhibitors• Subgroup 2df: OXA (23 and 48) carbapenemases• Subgroup 2f : serine carbapenemases from molecular class A:
GES and KPC • Subgroup 3b contains a smaller group of MBLs that
preferentially hydrolyze carbapenems• IMP and VIM enzymes that have appeared globally, most frequently in
non-fermentative bacteria but also in Enterobacteriaceae
DR.T.V.RAO MD 75

• KPCs are the most prevalent of this group of enzymes, found mostly on transferable plasmids in K.
pneumonia
• Substrate hydrolysis spectrum includes
cephalosporins and carbapenems
K. PNEUMONIA CARBAPENEMASES)
DR.T.V.RAO MD 76

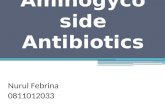
Nordmann P et al. LID 2009
K.PNEUMONIAE CARBAPENEMASE-PRODUCING BACTERIA
DR.T.V.RAO MD 77

Antibiotic resistance
“Antibiotic resistance continues to plague antimicrobial
chemotherapy of infectious diseases” Keith. Poole. J Antimicrob Chemother 2005; 56: 20-51
“Evolution of bacteria towards resistance… …is unavoidable because it represents a particular aspect of the general evolution of bacteria that is unstoppable”
Patrice Courvalin. Emerg Infect Dis 2005; 11: 1507-
6
“Antibiotic resistance has resulted in a continuous need for new therapeutic alternatives”
Carl Erik Nord. Clin Microbiol Infect 2004;10 (Supp 4)
“There is a need to re-invigorate antimicrobial development, which has been downgraded by major pharmaceutical houses”
David Livermore. Lancet Infect Dis 2005; 5:450-59
DR.T.V.RAO MD 78

< Inappropriate specimen selection and collection
< Inappropriate clinical tests
< Failure to use stains/smears
< Failure to use cultures and susceptibility tests
Practices Contributing to Misuse of Antibiotics
DR.T.V.RAO MD 79

< Use of antibiotics with no clinical indication (eg, for viral infections)
< Use of broad spectrum antibiotics when not indicated
< Inappropriate choice of empiric antibiotics
Inappropriate Antibiotic Use
DR.T.V.RAO MD 80

• Optimize patient evaluation
• Adopt judicious antibiotic
• prescribing practices
• Immunize patients
PHYSICIANS CAN IMPACT PATIENTS
DR.T.V.RAO MD 81

• Optimize consultations with other clinicians
• Use infection control measures
• Educate others about judicious use of antibiotics
PHYSICIANS CAN IMPACT OTHER CLINICIANS
DR.T.V.RAO MD 82

ANTIBIOTIC PRESSURE AND RESISTANCE IN
BACTERIA: CONCLUSIONS
• Bacteria evolve resistance to antibiotics in response to environmental pressure exerted by the use of antibiotics.
• Many of these bacteria are significant pathogens.
• Our responsibility to our community is to use antibiotics prudently, for appropriate indications.
DR.T.V.RAO MD 83

ARE WE OVERUSING ANTIBIOTICS
DR.T.V.RAO MD 84

DEDICATED HANDWASHING HAS MANY SOLUTIONS TO PREVENT SPREAD OF DRUG RESISTANT STRAINS
DR.T.V.RAO MD 85

• Programme created by Dr.T.V.Rao MD for Medical Professionals in the
Developing World
• Email• [email protected]
DR.T.V.RAO MD 86