Infections of the upper respiratory tract. Clinical syndromes.

Departamento de
Microbiología II
Universidad
Complutense. Madrid
Hospital Universitario Ramón y CajalSERVICIO DE MICROBIOLOGÍA Y PARASITOLOGÍA
Dr. Rafael Cantón
Resistance to new β-lactam-
β-lactamase inhibitor
combinations: a new step in
the muti-drug resistance?
Disclosures
▪ Participation in educational programs
- Angelini
- Beckman
- MSD
- Pfizer
- Roche
- ThemoFisher
- Zambon
▪ Participation in research studies- AstraZeneca
- BioMerieux
- Cepheid
- MSD
▪ Evaluation of clinical trials
- Bayer
- MSD
▪ Why new β-lactam-β-lactamase inhibitor combinations?
▪ Which are the new β-lactam-β-lactamase inhibitor combinations?
▪ How the new β-lactam-β-lactamase inhibitor combinations work?
▪ How is the resistant development? How I can detect it?
▪ How can avoid emergence of resistance?
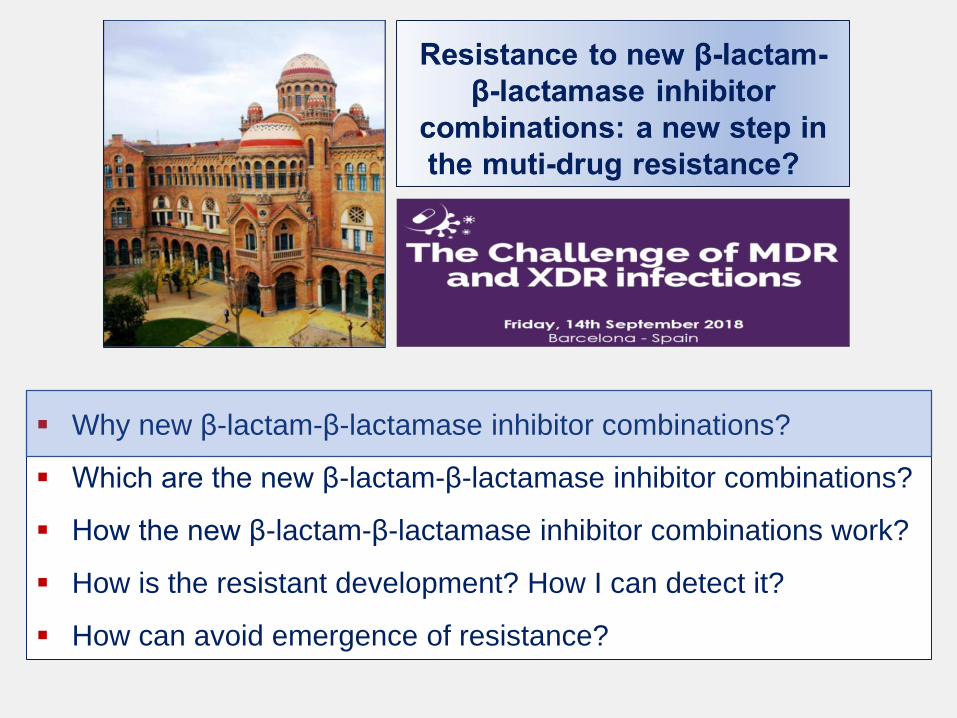
Antibacterial agents in clinical
development: an analysis of the
antibacterial clinical development
pipeline, including tuberculosis.
Geneva: World Health Organization;
2017 (WHO/EMP/IAU/2017.11).
Prioritization of
pathogens to guide
research and
development of
new antibiotics
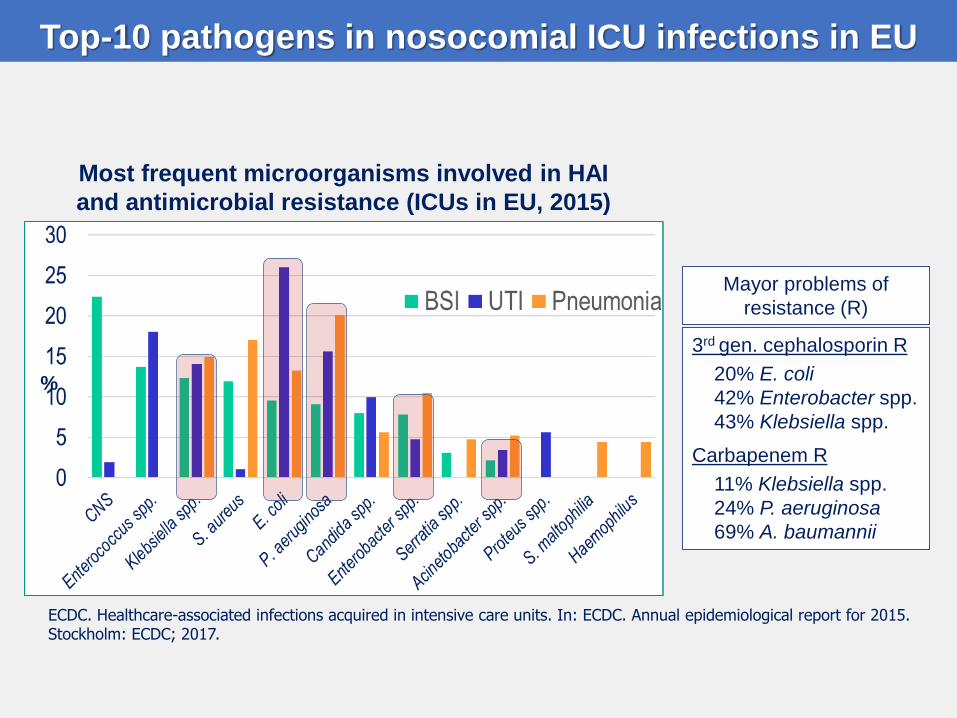
Most frequent microorganisms involved in HAI
and antimicrobial resistance (ICUs in EU, 2015)
%
3rd gen. cephalosporin R
20% E. coli
42% Enterobacter spp.
43% Klebsiella spp.
Carbapenem R
11% Klebsiella spp.
24% P. aeruginosa
69% A. baumannii
Mayor problems of
resistance (R)
ECDC. Healthcare-associated infections acquired in intensive care units. In: ECDC. Annual epidemiological report for 2015. Stockholm: ECDC; 2017.
Top-10 pathogens in nosocomial ICU infections in EU

3rd gen. cephalosporin resistance worldwide
Overall trend in EU region (ATLAS surveillance study, 2016)
Escherichia coli Klebsiella pneumoniae
ATLAS surveillance. Available at: https://atlas-surveillance.com/#/heatmap/resistance. [Accessed April 2018]
Spain: 20.8% Spain: 38.4%

3rd gen. cephalosporin resistance in Europe
(invasive isolates, EARS-net 2016)
Escherichia coli Klebsiella pneumoniae
Antimicrobial resistance surveillance in Europe 2016. Annual Report of the European Antimicrobial Resistance Surveillance
Network (EARS-Net). Stockholm: ECDC; 2017. Available at: https://ecdc.europa.eu/en/publications-data/antimicrobial-
resistance-surveillance-europe-2016. [Accessed April 2018].
15.0% 22.3%

Klebsiella pneumoniae
Carbapenem (meropenem) resistance worldwideOverall trend in EU region (Atlas surveillance study, 2016)
ATLAS surveillance. Available at: https://atlas-surveillance.com/#/heatmap/resistance. [Accessed April 2018].
Escherichia coli
Spain: 0% Spain: 2.2%
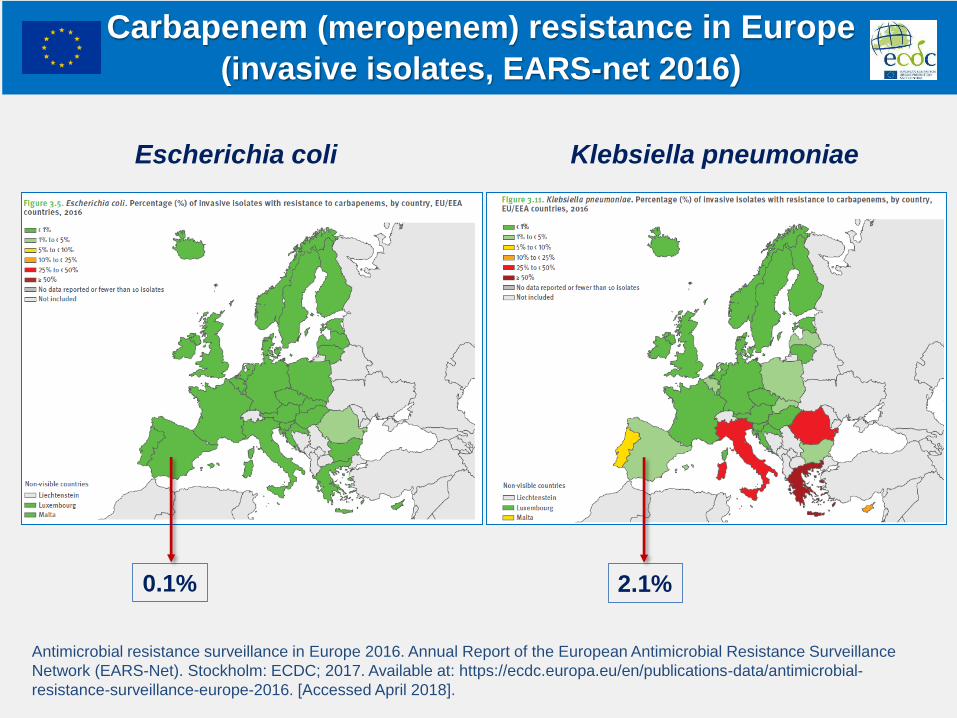
Carbapenem (meropenem) resistance in Europe
(invasive isolates, EARS-net 2016)
Escherichia coli Klebsiella pneumoniae
Antimicrobial resistance surveillance in Europe 2016. Annual Report of the European Antimicrobial Resistance Surveillance
Network (EARS-Net). Stockholm: ECDC; 2017. Available at: https://ecdc.europa.eu/en/publications-data/antimicrobial-
resistance-surveillance-europe-2016. [Accessed April 2018].
0.1% 2.1%
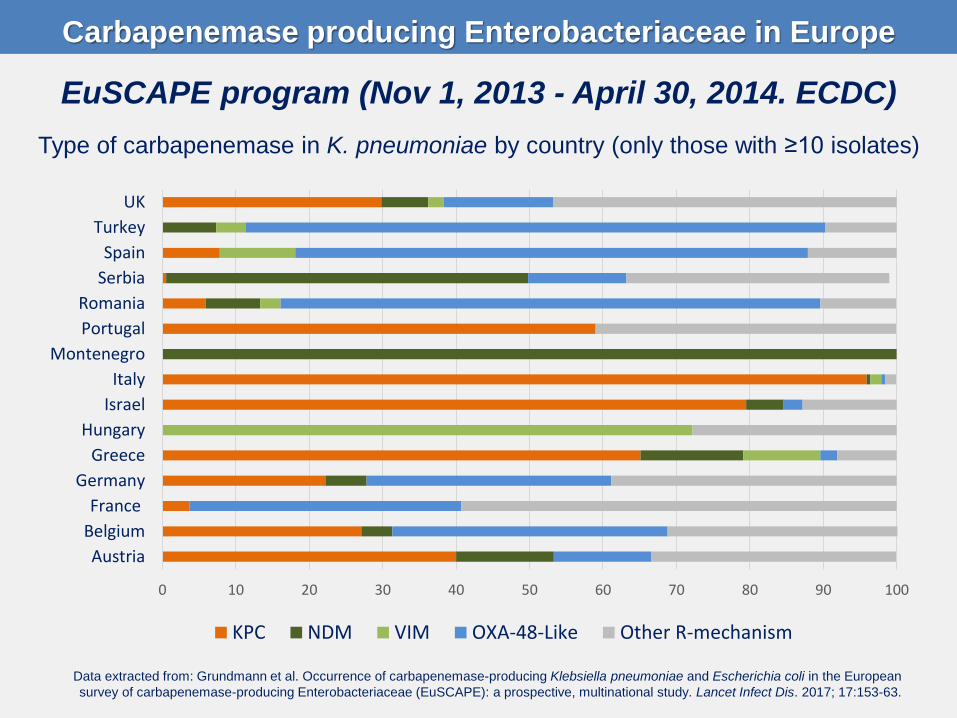
Carbapenemase producing Enterobacteriaceae in Europe
0 10 20 30 40 50 60 70 80 90 100
Austria
Belgium
France
Germany
Greece
Hungary
Israel
Italy
Montenegro
Portugal
Romania
Serbia
Spain
Turkey
UK
KPC NDM VIM OXA-48-Like Other R-mechanism
EuSCAPE program (Nov 1, 2013 - April 30, 2014. ECDC)
Type of carbapenemase in K. pneumoniae by country (only those with ≥10 isolates)
Data extracted from: Grundmann et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European
survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect Dis. 2017; 17:153-63.
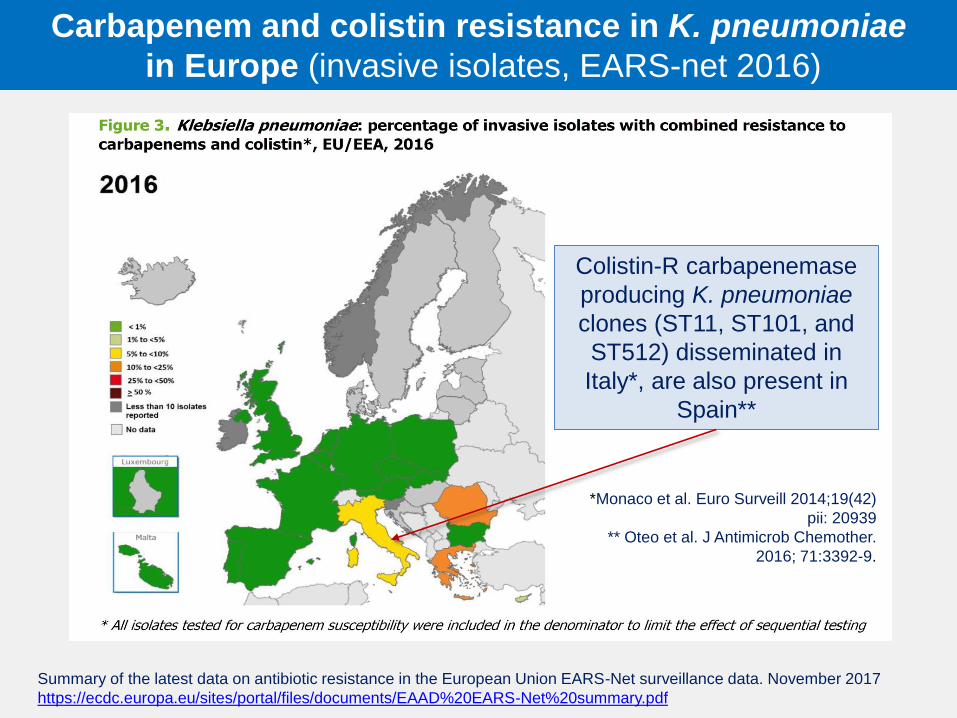
Carbapenem and colistin resistance in K. pneumoniae
in Europe (invasive isolates, EARS-net 2016)
Summary of the latest data on antibiotic resistance in the European Union EARS-Net surveillance data. November 2017
https://ecdc.europa.eu/sites/portal/files/documents/EAAD%20EARS-Net%20summary.pdf
Colistin-R carbapenemase
producing K. pneumoniae
clones (ST11, ST101, and
ST512) disseminated in
Italy*, are also present in
Spain**
*Monaco et al. Euro Surveill 2014;19(42)
pii: 20939
** Oteo et al. J Antimicrob Chemother.
2016; 71:3392-9.

Meropenem
Antimicrobial resistance worldwide in P. aeruginosa
Overall trend in EU region (Atlas surveillance study, 2016)
ATLAS surveillance. Available at: https://atlas-surveillance.com/#/heatmap/resistance. [Accessed April 2018].
Ceftazidime
Spain: 25.7% Spain: 18.5%
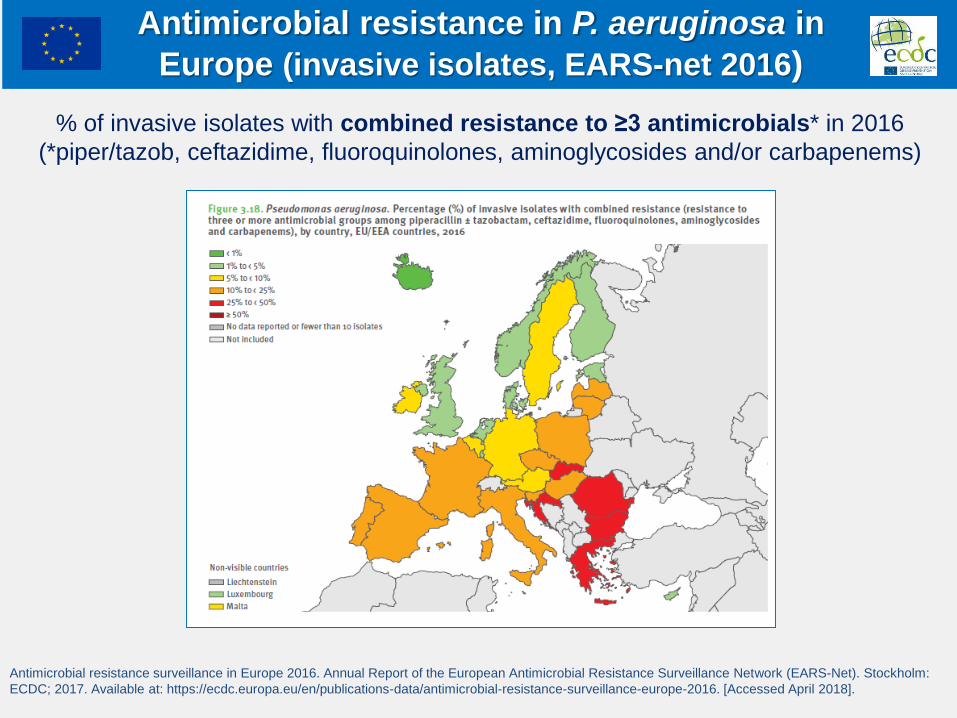
Antimicrobial resistance in P. aeruginosa in
Europe (invasive isolates, EARS-net 2016)
% of invasive isolates with combined resistance to ≥3 antimicrobials* in 2016
(*piper/tazob, ceftazidime, fluoroquinolones, aminoglycosides and/or carbapenems)
Antimicrobial resistance surveillance in Europe 2016. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Stockholm:
ECDC; 2017. Available at: https://ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2016. [Accessed April 2018].

▪ Why new β-lactam-β-lactamase inhibitor combinations?
▪ Which are the new β-lactam-β-lactamase inhibitor combinations?
▪ How the new β-lactam-β-lactamase inhibitor combinations work?
▪ How is the resistant development? How I can detect it?
▪ How can avoid emergence of resistance?

0
2
4
6
8
10
12
14
16
18
1983-1987 1988-1992 1993-1997 1998-2002 2003-2007 2008-2012 2013-2017 2018-
nu
mb
er
of
ne
w a
nti
mic
roib
ials
Years
Ceftobiprole (2013)
Telavancin (2014)
Dalbavancin (2015)
Tedizolid (2015)
Oritavancin (2015)
Ceftolozane-tazobactam (2015)
Ceftazidime-avibactam (2016)
Delafloxacin (2017)
Ozenoxacin (2017)
Meropenem-vaborbactam (2017)
Antibacterial agents approved by FDA and/or EMA
Ceftaroline (2010)
Fidaxomicin (2012)
Delamanid (2012)
Bedaquiline (2012)
Updated from Shlaes et al. AACh 2013, 57:4605-7
Plazomicin (2018)
Eravacycline (2018)
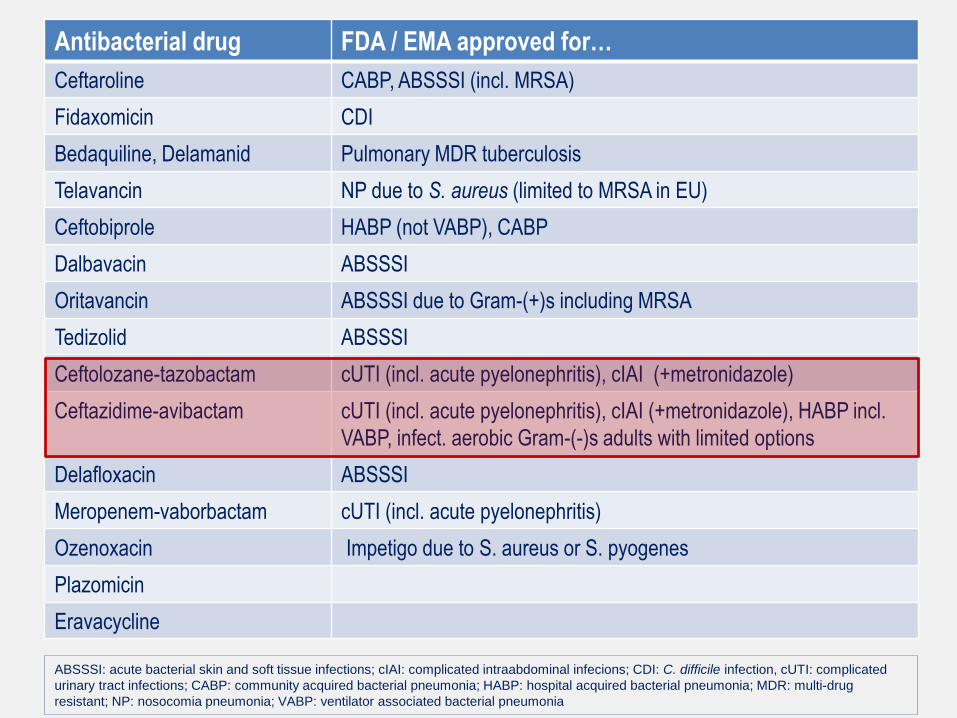
Antibacterial drug FDA / EMA approved for…
Ceftaroline CABP, ABSSSI (incl. MRSA)
Fidaxomicin CDI
Bedaquiline, Delamanid Pulmonary MDR tuberculosis
Telavancin NP due to S. aureus (limited to MRSA in EU)
Ceftobiprole HABP (not VABP), CABP
Dalbavacin ABSSSI
Oritavancin ABSSSI due to Gram-(+)s including MRSA
Tedizolid ABSSSI
Ceftolozane-tazobactam cUTI (incl. acute pyelonephritis), cIAI (+metronidazole)
Ceftazidime-avibactam cUTI (incl. acute pyelonephritis), cIAI (+metronidazole), HABP incl.
VABP, infect. aerobic Gram-(-)s adults with limited options
Delafloxacin ABSSSI
Meropenem-vaborbactam cUTI (incl. acute pyelonephritis)
Ozenoxacin Impetigo due to S. aureus or S. pyogenes
Plazomicin
Eravacycline
ABSSSI: acute bacterial skin and soft tissue infections; cIAI: complicated intraabdominal infecions; CDI: C. difficile infection, cUTI: complicated
urinary tract infections; CABP: community acquired bacterial pneumonia; HABP: hospital acquired bacterial pneumonia; MDR: multi-drug
resistant; NP: nosocomia pneumonia; VABP: ventilator associated bacterial pneumonia
▪ Why new β-lactam-β-lactamase inhibitor combinations?
▪ Which are the new β-lactam-β-lactamase inhibitor combinations?
▪ How the new β-lactam-β-lactamase inhibitor combinations work?
▪ How is the resistant development? How I can detect it?
▪ How can avoid emergence of resistance?

Ceftazidime Avibactam
• 3rd gen. cephalosporin active against
Enterobacteriaceae and P. aeruginosa
• Affected by
- AmpC derepression
- ESBL (partial) and carbapenemases
- Porin or efflux pumps
• β-lactamase inhibitor with the highest
inhibitor spectrum
• Inhibitor of different β-lactamase classes
- A (ESBLs and KPCs)
- C (AmpC)
- D (ESBLs and OXA-48-type)
Approved for:
- Complicated urinary tract infection (including acute pyelonephritis)
- Complicated intra-abdominal infections (associated with metronidazole)
- Hospital-acquired pneumonia (including ventilator-associated pneumonia)
- Infections in adults due to aerobic Gram-negative infections with limited options
Sharma R, et al. Clin Ther 2016;38:431-44; Rodríguez-Baño J, et al. Clin Microbiol Rev 2018;31.pii: e00079–17; Ceftazidime-avibactam SPC.
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR-Product_Information/human/004027/WC500210234.pdf [Accessed April 2018]
Ehmann DE et al. Proc Natl Acad Sci. 2012;29:11663–11668; 3. Aktaş Z, et al. Int J Antimicrob Agents 2012;39:86-9.

Inhibited by avibactam
Serin-enzymes
A C D
Zinc enzymes
B
B-LACTAMASES
Active site
Nucleotidic
sequence
CARBAPENEMASES
(METALO-β-LACTAMASES
VIM, NDM, IMP, …)
ESBL (CTX-M)
CARBAPENEMASES
(KPC)
CARBAPENEMASES
(OXA-48)AmpC
Bush & Bradford. Cold Spring Harb Perspect Med. 2016; 6(8). pii: a025247
β-lactamase classification

CAZ, ceftazidime; CAZ–AVI, ceftazidime–avibactam
López-Hernández I, et al. Activity of ceftazidime-avibactam against multidrug-resistance Enterobacteriaceae expressing combined
mechanisms of resistance. Enferm Infecc Microbiol Clin 2017;35:499–504.
CAZ and CAZ–AVI* MIC distributions in ESBL and/or
AmpC producing K. pneumoniae isolates in Spain

*Ceftazidime–avibactam is the property of Pfizer. CAZ, ceftazidime; CAZ–AVI, ceftazidime–avibactam; KPC, K. pneumoniae carbapenemase;
MBL, metallo-β-lactamase OXA, oxacillinase.
Jonge BL, et al. In vitro susceptibility to ceftazidime-avibactam of carbapenem-nonsusceptible Enterobacteriaceae isolates collected during the
INFORM Global Surveillance Study (2012 to 2014). Antimicrob Agents Chemother. 2016;60:3163–9.
0
10
20
30
40
50
60
70
80
90
100
0,0
1
0,0
3
0,0
6
0,1
2
0,2
5
0,5 1 2 4 8
16 32 64
128
>12
8
CAZ CAZ-AVI
0
50
100
150
200
250
300
0,0
1
0,0
3
0,0
6
0,1
2
0,2
5
0,5 1 2 4 8
16 32 64
128
>12
8
CAZ CAZ-AVI
0
5
10
15
20
25
30
35
40
45
50
0,01
0,03
0,06
0,12
0,25 0,
5 1 2 4 8
16 32 64
128
>128
CAZ CAZ-AVI
0
20
40
60
80
100
120
140
0,01
0,03
0,06
0,12
0,25 0,
5 1 2 4 8
16 32 64
128
>128
CAZ CAZ-AVI
Carbapenemase-negative KPC-positive, MBL-negative
OXA-48-like positive, MBL-negative MBL positive
CAZ vs. CAZ–AVI* in carbapenem nonsusceptible
Enterobacteriaceae (INFORM Global Surveillance study, 2012-2014)

Torrens et al. Antimicrob Agents Chemother 2016; 60:6407-10
% of susceptible isolates
All isolates (n=190) AmpC hyperp. (n=46) Multi-drug-R (n=63)
CAZ CAZ-AVI MER CAZ CAZ-AVI MER CAZ CAZ-AVI MER
64.7 91.1 77.4 10.9 76.1 41.3 27.0 77.8 74.1
CAZ and CAZ–AVI* MIC distributions in
bacteriemic P. aeruginosa isolates in Spain

Ceftolozane Tazobactam
• 4th gen. cephalosporins derived from ceftazidime
(higher PBP affinity)
• High intrinsic activity against Pseudomonas
aeruginosa, including those with efflux/AmpC
hyperexpression and/or porin deficiency
• Partially affected by ESBLs and fully affected by
carbapenemases
• Suicide inhibitor
• Inhibitor of class A β-lactamases,
including ESBls but not KPCs
• Scarce inhibition of class C (AmpC)
and null of class D (OXAs)
Approved for: - complicated UTI (including acute pyelonephritis)
- complicated intraabdominal infection (associated with metronidazol)
Scott LJ. Drugs 2016; 76:231-42

Inhibited by avibactam
Serin-enzymes
A C D
Zinc enzymes
B
B-LACTAMASES
Active site
Nucleotidic
sequence
CARBAPENEMASES
(METALO-β-LACTAMASES
VIM, NDM, IMP, …)
ESBL (CTX-M)
CARBAPENEMASES
(KPC)
CARBAPENEMASES
(OXA-48)AmpC
Bush & Bradford. Cold Spring Harb Perspect Med. 2016; 6(8). pii: a025247
β-lactamase classification
Inhibited by tazobactam
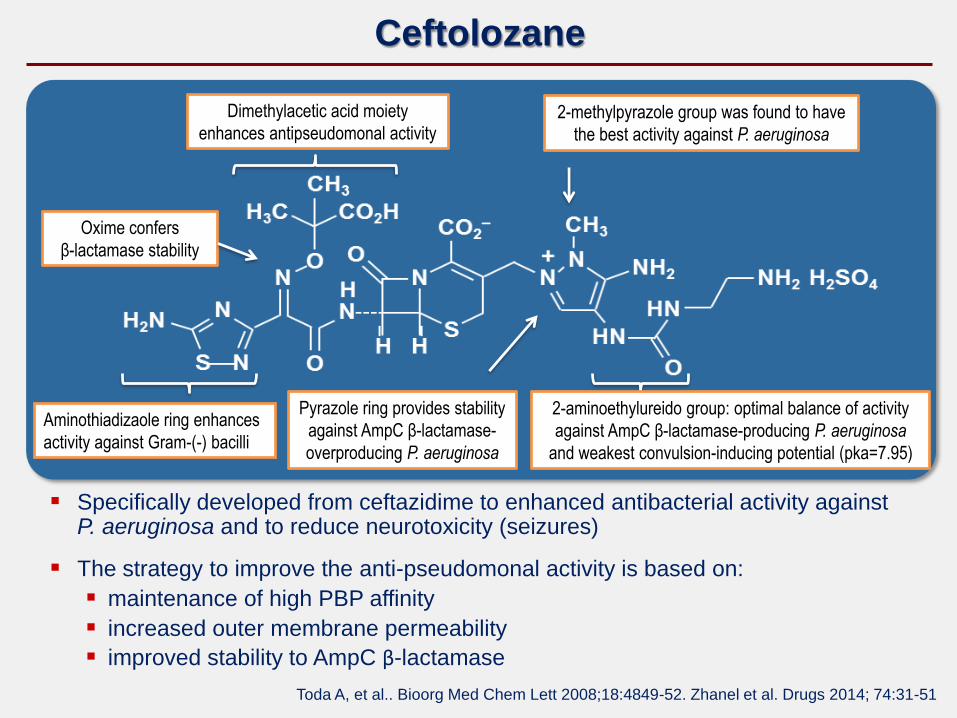
▪ Specifically developed from ceftazidime to enhanced antibacterial activity against P. aeruginosa and to reduce neurotoxicity (seizures)
▪ The strategy to improve the anti-pseudomonal activity is based on:
▪ maintenance of high PBP affinity
▪ increased outer membrane permeability
▪ improved stability to AmpC β-lactamase
Toda A, et al.. Bioorg Med Chem Lett 2008;18:4849-52. Zhanel et al. Drugs 2014; 74:31-51
Dimethylacetic acid moiety
enhances antipseudomonal activity
Oxime confers
β-lactamase stability
2-aminoethylureido group: optimal balance of activity
against AmpC β-lactamase-producing P. aeruginosa
and weakest convulsion-inducing potential (pka=7.95)
2-methylpyrazole group was found to have
the best activity against P. aeruginosa
Pyrazole ring provides stability
against AmpC β-lactamase-
overproducing P. aeruginosa
Aminothiadizaole ring enhances
activity against Gram-(-) bacilli
Ceftolozane

Study (no. of P. aeruginosa)Ceftazidime-avibactam Ceftolozane-tazobactam
% S MIC50/MIC90 % S MIC50/MIC90
Buehrle AAC 2016 (n=38) 92% 1 / 8 92% 1 / 4
Gonzalez Ann Lab Med 2017 (n=45) 82% 2 / 16 87% 1 / 8
Grupper AAC 2017 (n=290) 81% 1 / 8 91% 1 / 4
Humphries AAC 2017 (n=309)* 62% ND 73% ND
Wi AAC 2018 (n=42)** 71.4% 8 / 16 95% 2 / 4
Sader JAC 2018 (n=423) 96.2% - 96.5 -
*Isolates included if resistant to >1 antipseudomonal β-lactam (ceftazidime, cefepime, meropenem,
imipenem or piperacillin-tazobactam)
Ceftazidime-avibactam vs. ceftolozane-tazobactam
in Pseudomonas aeruginosa
▪ Different studies document in vitro activity of both antimicrobials against
multi-drug resistant (MDR) P. aeruginosa isolates
▪ At least 6 studies evaluated the activity of both antimicrobials in parallel
against P. aeruginosa, including MDR populations
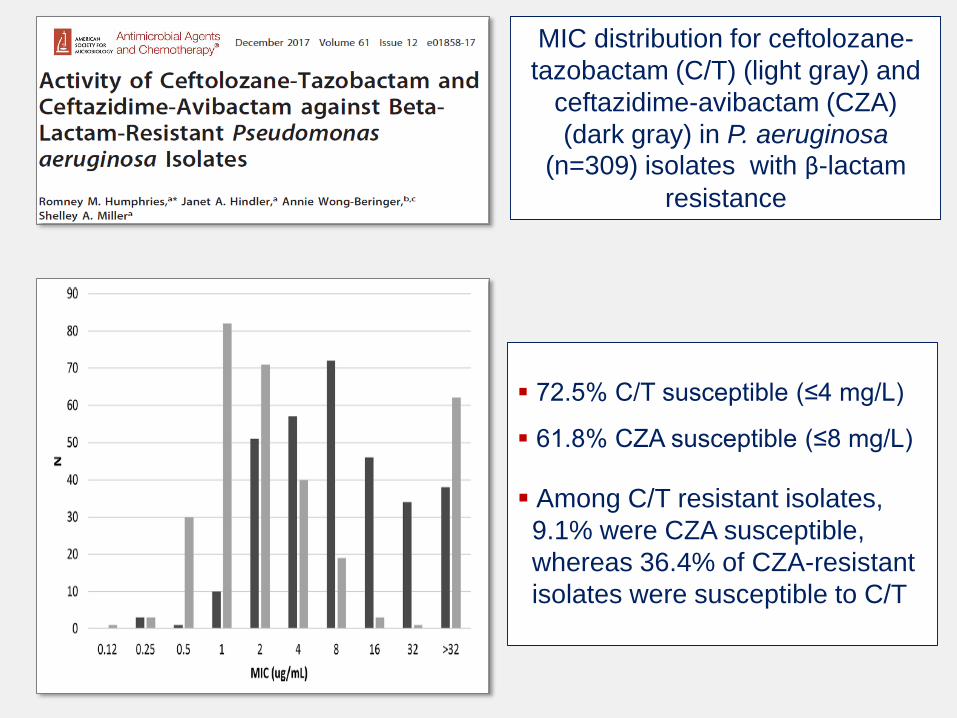
MIC distribution for ceftolozane-
tazobactam (C/T) (light gray) and
ceftazidime-avibactam (CZA)
(dark gray) in P. aeruginosa (n=309) isolates with β-lactam
resistance
▪ 72.5% C/T susceptible (≤4 mg/L)
▪ 61.8% CZA susceptible (≤8 mg/L)
▪ Among C/T resistant isolates,
9.1% were CZA susceptible,
whereas 36.4% of CZA-resistant
isolates were susceptible to C/T

Resistance profiles of P. aeruginosa
(n=309) that were resistant at least to
piperacillin-tazobactam, ceftazidime,
cefepime, imipenem or meropenem
In all situations, C/T susceptibility was higher that that of CZA

Int J Antimicrob Agents. 2015; 46:502-10
Antibiotic % S
C/T 94.4
CAZ 76.0
MER 64.6
P/T 63.6
IMP 60.0
LEV 61.6

▪ Why new β-lactam-β-lactamase inhibitor combinations?
▪ Which are the new β-lactam-β-lactamase inhibitor combinations?
▪ How the new β-lactam-β-lactamase inhibitor combinations work?
▪ How is the resistant development? How I can detect it?
▪ How can avoid emergence of resistance?
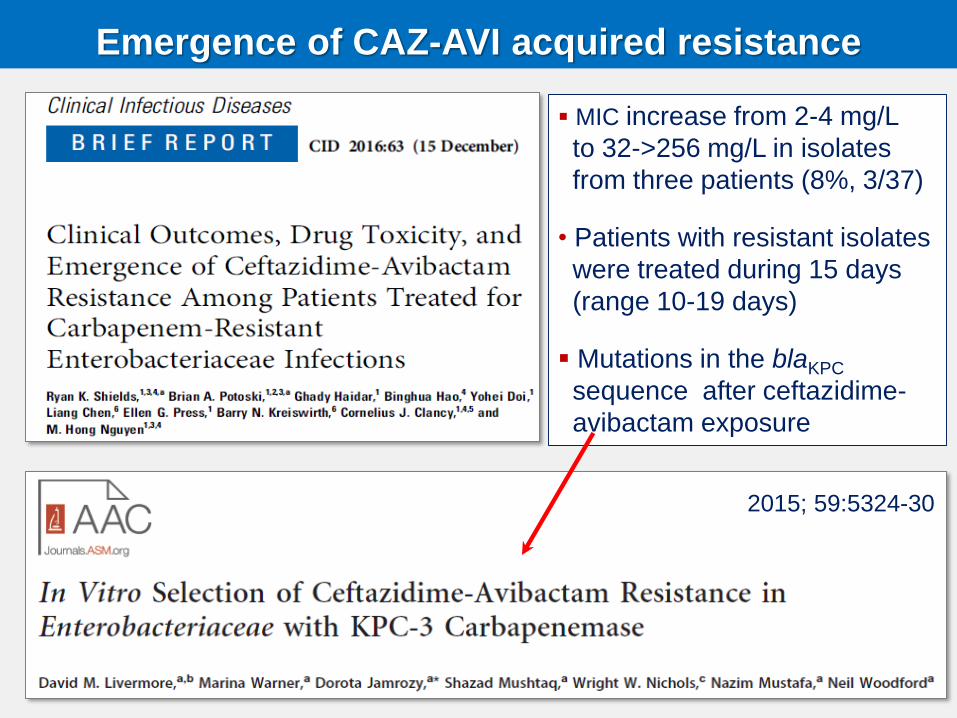
▪ MIC increase from 2-4 mg/L
to 32->256 mg/L in isolates
from three patients (8%, 3/37)
• Patients with resistant isolates
were treated during 15 days
(range 10-19 days)
▪ Mutations in the blaKPC
sequence after ceftazidime-
avibactam exposure
Emergence of CAZ-AVI acquired resistance
2015; 59:5324-30
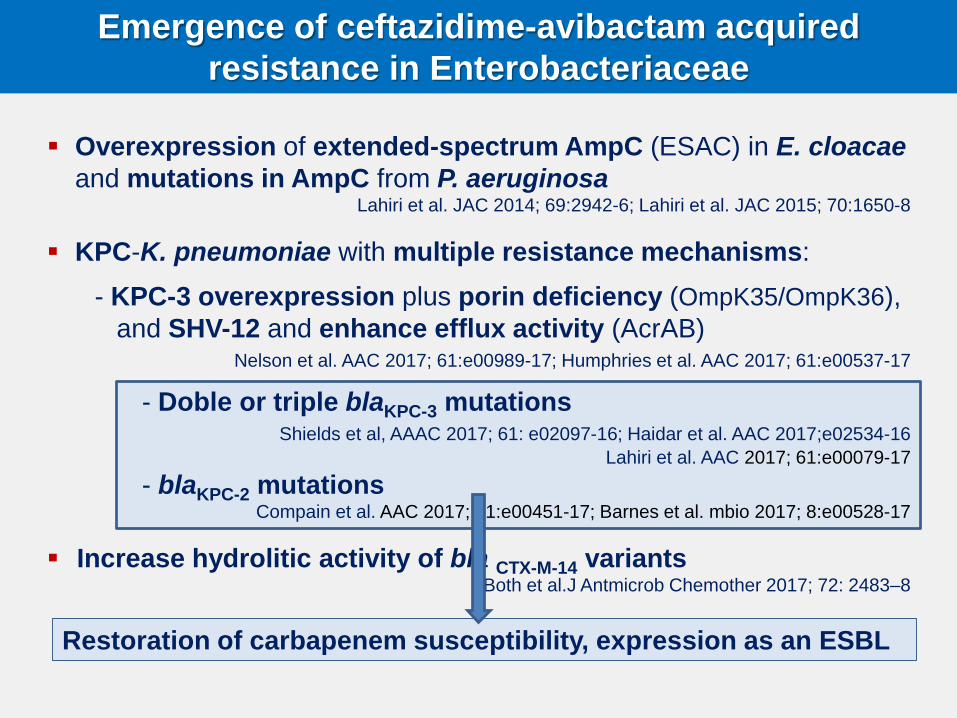
Emergence of ceftazidime-avibactam acquired
resistance in Enterobacteriaceae
▪ Overexpression of extended-spectrum AmpC (ESAC) in E. cloacae
and mutations in AmpC from P. aeruginosaLahiri et al. JAC 2014; 69:2942-6; Lahiri et al. JAC 2015; 70:1650-8
▪ KPC-K. pneumoniae with multiple resistance mechanisms:
- KPC-3 overexpression plus porin deficiency (OmpK35/OmpK36),
and SHV-12 and enhance efflux activity (AcrAB)Nelson et al. AAC 2017; 61:e00989-17; Humphries et al. AAC 2017; 61:e00537-17
- Doble or triple blaKPC-3 mutationsShields et al, AAAC 2017; 61: e02097-16; Haidar et al. AAC 2017;e02534-16
Lahiri et al. AAC 2017; 61:e00079-17
- blaKPC-2 mutationsCompain et al. AAC 2017; 61:e00451-17; Barnes et al. mbio 2017; 8:e00528-17
▪ Increase hydrolitic activity of bla CTX-M-14 variantsBoth et al.J Antmicrob Chemother 2017; 72: 2483–8
Restoration of carbapenem susceptibility, expression as an ESBL

Emergence of CAZ-AVI resistance and restoration of
carbapanem susceptibility in KPC producing K. pneumoniae
Time-kill responses of CAZ-AVI
resistant Klebsiella pneumoniae to
meropenem (● no drug, ▲ 4xMIC,
x 8xMIC, ■ 16 μg/mL)
Etest results for meropenem and
CAZ-AVI against baseline isolate
(left) and follow-up isolate (right)
▪ Restoration of meropenem susceptibility among CAZ-AVI resistant
K. pneumoniae during CAZ-AVI treatment
Shields et al. Open Forum Infect Dis. 2017; 4(3):ofx101
▪ In-vitro selection of CTL-TAZ resistance requires multiple mutations
leading to over expression and structural modifications of AmpC
Cabot et al. AAC 2014; 58:3091-9
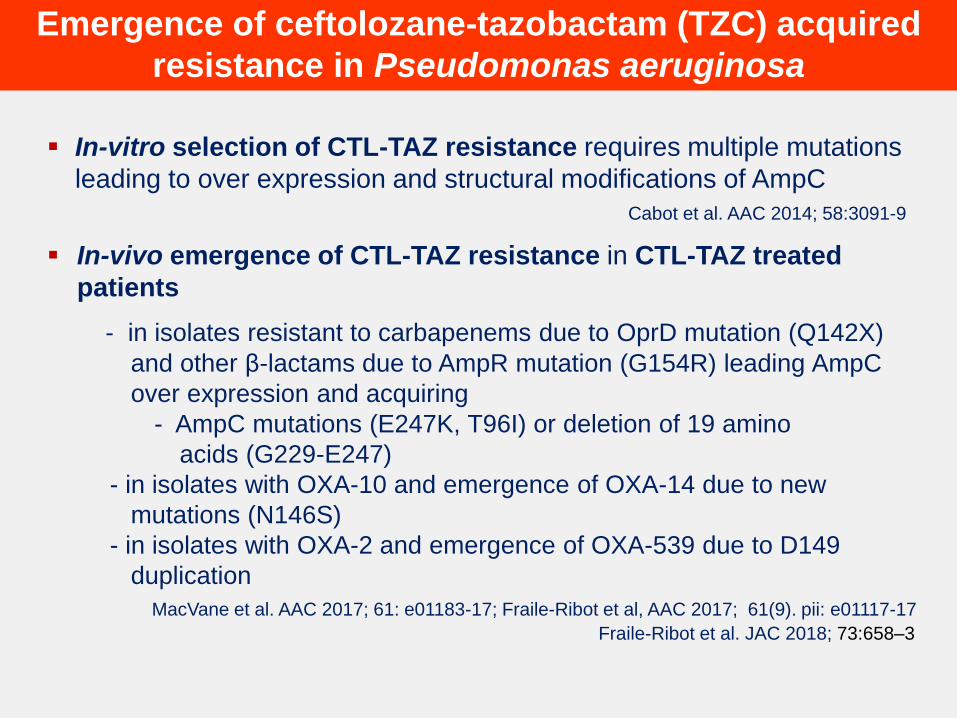
▪ In-vivo emergence of CTL-TAZ resistance in CTL-TAZ treated
patients
- in isolates resistant to carbapenems due to OprD mutation (Q142X)
and other β-lactams due to AmpR mutation (G154R) leading AmpC
over expression and acquiring
- AmpC mutations (E247K, T96I) or deletion of 19 amino
acids (G229-E247)
- in isolates with OXA-10 and emergence of OXA-14 due to new
mutations (N146S)
- in isolates with OXA-2 and emergence of OXA-539 due to D149
duplication
MacVane et al. AAC 2017; 61: e01183-17; Fraile-Ribot et al, AAC 2017; 61(9). pii: e01117-17
Fraile-Ribot et al. JAC 2018; 73:658–3
Emergence of ceftolozane-tazobactam (TZC) acquired
resistance in Pseudomonas aeruginosa
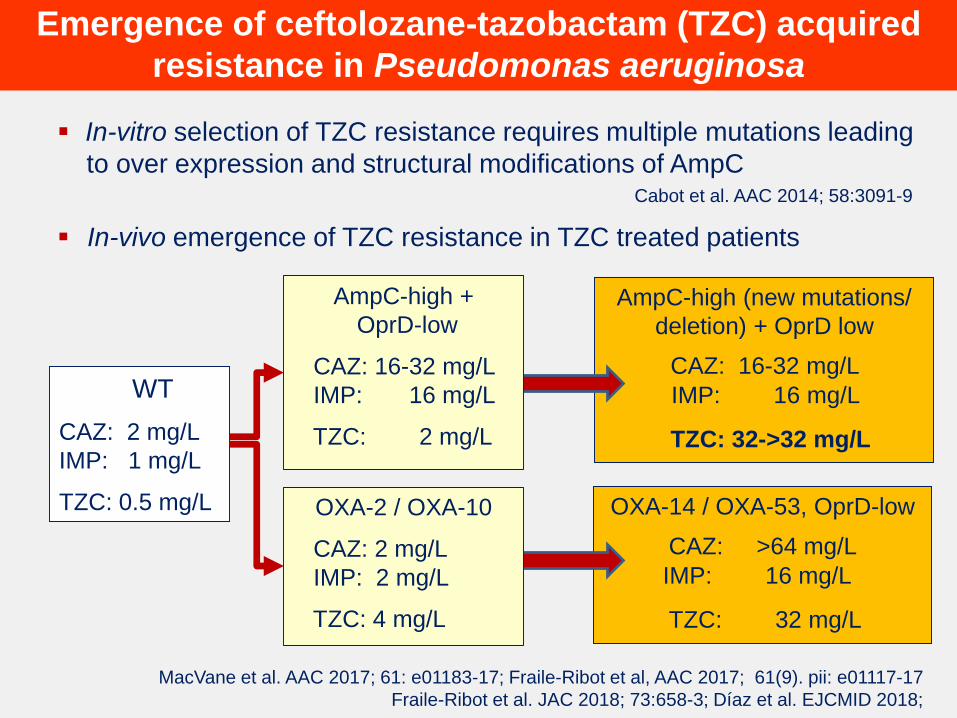
▪ In-vitro selection of TZC resistance requires multiple mutations leading
to over expression and structural modifications of AmpCCabot et al. AAC 2014; 58:3091-9
▪ In-vivo emergence of TZC resistance in TZC treated patients
MacVane et al. AAC 2017; 61: e01183-17; Fraile-Ribot et al, AAC 2017; 61(9). pii: e01117-17
Fraile-Ribot et al. JAC 2018; 73:658-3; Díaz et al. EJCMID 2018;
AmpC-high (new mutations/
deletion) + OprD low
CAZ: 16-32 mg/L
IMP: 16 mg/L
TZC: 32->32 mg/L
OXA-14 / OXA-53, OprD-low
CAZ: >64 mg/L
IMP: 16 mg/L
TZC: 32 mg/L
WT
CAZ: 2 mg/L
IMP: 1 mg/L
TZC: 0.5 mg/L
AmpC-high +
OprD-low
CAZ: 16-32 mg/L
IMP: 16 mg/L
TZC: 2 mg/L
OXA-2 / OXA-10
CAZ: 2 mg/L
IMP: 2 mg/L
TZC: 4 mg/L
Emergence of ceftolozane-tazobactam (TZC) acquired
resistance in Pseudomonas aeruginosa

▪ Why new β-lactam-β-lactamase inhibitor combinations?
▪ Which are the new β-lactam-β-lactamase inhibitor combinations?
▪ How the new β-lactam-β-lactamase inhibitor combinations work?
▪ How is the resistant development? How I can detect it?
▪ How can avoid emergence of resistance?
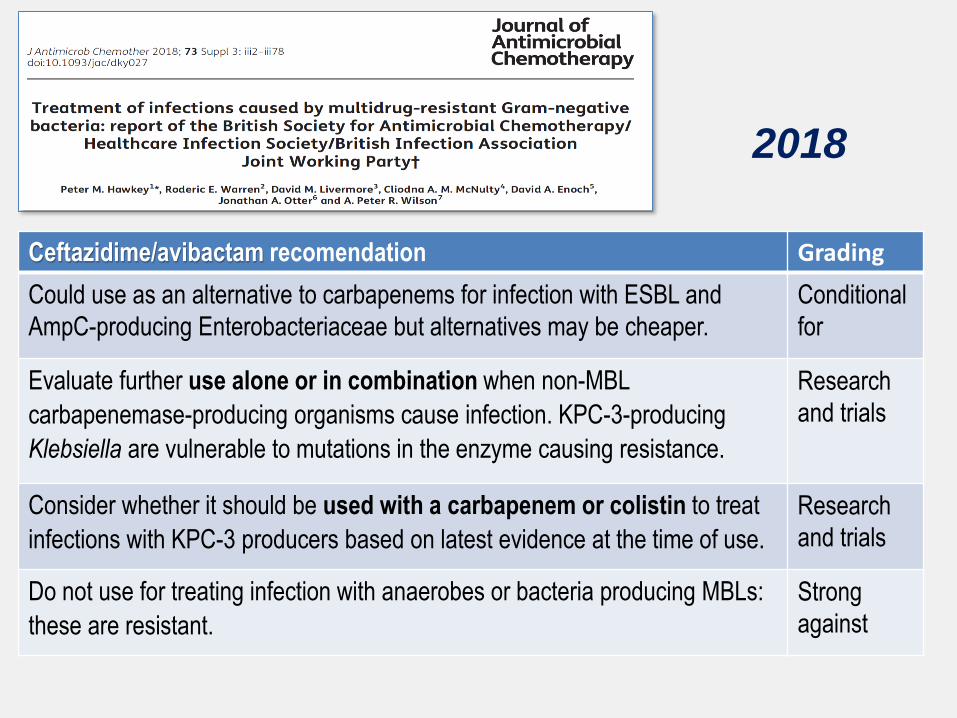
2018
Ceftazidime/avibactam recomendation Grading
Could use as an alternative to carbapenems for infection with ESBL and
AmpC-producing Enterobacteriaceae but alternatives may be cheaper.
Conditional
for
Evaluate further use alone or in combination when non-MBL
carbapenemase-producing organisms cause infection. KPC-3-producing
Klebsiella are vulnerable to mutations in the enzyme causing resistance.
Research
and trials
Consider whether it should be used with a carbapenem or colistin to treat
infections with KPC-3 producers based on latest evidence at the time of use.
Research
and trials
Do not use for treating infection with anaerobes or bacteria producing MBLs:
these are resistant.
Strong
against
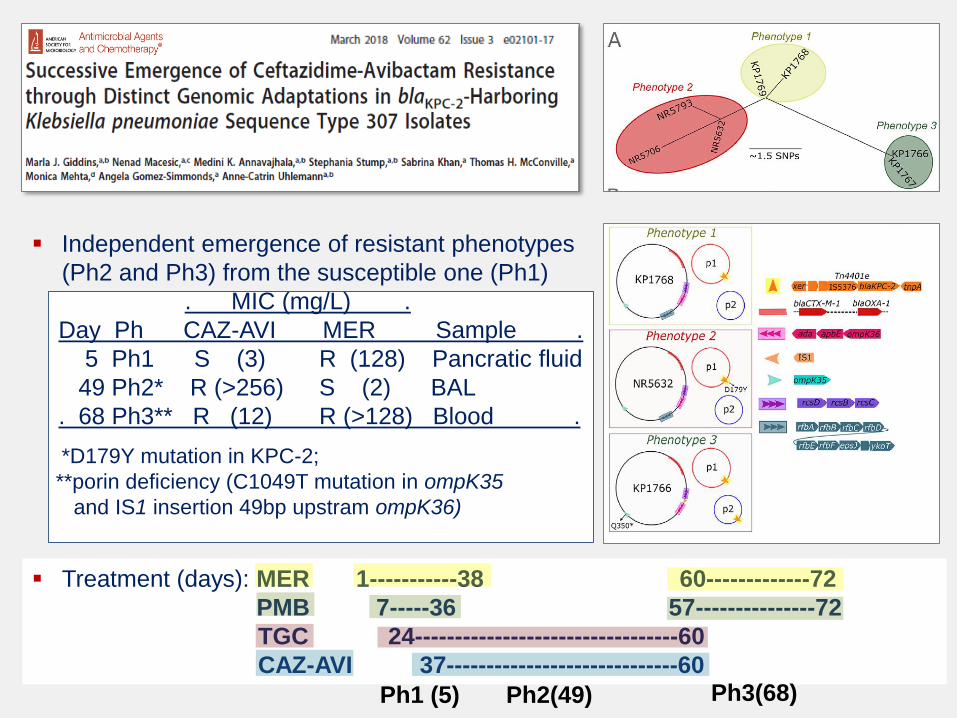
▪ Independent emergence of resistant phenotypes
(Ph2 and Ph3) from the susceptible one (Ph1)
. MIC (mg/L) .
Day Ph CAZ-AVI MER Sample .
5 Ph1 S (3) R (128) Pancratic fluid
49 Ph2* R (>256) S (2) BAL
. 68 Ph3** R (12) R (>128) Blood .
*D179Y mutation in KPC-2;
**porin deficiency (C1049T mutation in ompK35
and IS1 insertion 49bp upstram ompK36)
▪ Treatment (days): MER 1-----------38 60-------------72
PMB 7-----36 57---------------72
TGC 24---------------------------------60
CAZ-AVI 37-----------------------------60
Ph2(49) Ph3(68)Ph1 (5)

▪ The combination did not suppress
ceftazidime-avibactam resistance
▪ Colistin + ceftazidime-avibactam
did not provide a benefit over
ceftazidime-avibactam alone
against most CRE isolates.

2018
Ceftolozane/tazobactam recomendations Grading
Use to treat susceptible infections with P. aeruginosa resistant to
ceftazidime.
Conditional for
Use as an alternative to carbapenems to treat urinary or intraabdominal
infection involving ESBL-producing E. coli. Caution may be needed when
treating infections with ESBL-producing Klebsiella spp. owing to a higher
resistance rate.
Conditional for
Do not use for infections due to AmpC- or carbapenemase producing
Enterobacteriaceae or MBL/ESBL-producing P. aeruginosa.
Strong against
Risk of resistance development is increased when
P. aeruginosa have increased ceftazidime MICs
▪ New β-lactam-β-lactamase inhibitor combinations are needed to
address current resistance landscape
▪ The use of this new combinations does not exclude the possibility
of resistance development
▪ Resistance development of new β-lactam-β-lactamase inhibitor
combinations can be phenotypically recognized
▪ Resistance development of new β-lactam-β-lactamase inhibitor
combinations can not be excluded when using in combination
with other antibiotic classes

Acknowledgements

Departamento de
Microbiología II
Universidad
Complutense. Madrid
Hospital Universitario Ramón y CajalSERVICIO DE MICROBIOLOGÍA Y PARASITOLOGÍA
Dr. Rafael Cantón
Resistance to new β-lactam-
β-lactamase inhibitor
combinations: a new step in
the muti-drug resistance?







![ARDS & SEVERE HYPOXEMIAevaggelismos-hosp.gr/files/epistimoniki_enosi/02... · absence of Pneumothorax or ↑ Vt? ... [=Vt/Crs] LUNG: What do we need to avoid? • Hypoxemia • Ventilator-associated](https://static.fdocument.org/doc/165x107/5e9ac115fd0edd1d2c61726a/ards-severe-hypoxemiaevaggelismos-hospgrfilesepistimonikienosi02.jpg)