DM update 1 hr march 2018 ho - s3.amazonaws.com · α-Glucosidase Inhibitors Acarbose ......
7
3/14/18 1 DIABETES UPDATE 2018 Steven Ferrucci, OD, FAAO Chief, Optometry, Sepulveda VA Professor, SCCO/MBKU What is diabetes? • DM is a chronic disorder characterized by a lack of insulin or increased resistance to insulin • Insulin is needed for proper uptake of glucose • Clinical result is hyperglycemia • Leads to microvascular damage – retinopathy – nephropathy – neuropathy Diabetes: Magnitude of Complications Diabetic Retinopathy Leading cause of blindness in working age adults Diabetic Neuropathy Leading cause of non-traumatic lower extremity amputations Diabetic Nephropathy Leading cause of end-stage renal disease Stroke Cardiovascular Disease 2- to 4- fold increase in cardiovascular mortality and stroke Diabetes: An Epidemic • > 30 million people in the United States currently have DM 1 – Leading cause of visual loss and new-onset blindness in paRents aged 20 to 74 years 1 – 40% to 45% of Americans diagnosed with DM have some degree of DR 2 • 84 million more people are at high risk (prediabetes) 3 1. NaRonal Diabetes StaRsRcs Report, 2017. Atlanta, GA: NaRonal Center for Chronic Disease PrevenRon and Health PromoRon; 2017. 2. NaRonal Eye InsRtute. h_ps://nei.nih.gov/health/diabeRc/reRnopathy. Accessed January 16, 2018. 3. Centers for Disease Control. h_ps://www.cdc.gov/diabetes/basics/prediabetes.html. Accessed January 16, 2018. Cost of Care • ñ from $172 Billion in 2007 to $245 Billion in 2012- ñ41% – $ 176 B direct costs – $ 69 B indirect • In CA alone, $24.5 Billion (July 2015) • Medical cost 2.3X higher in pts with DM • Care of people with DM accounts for 1 out 5 healthcare dollars in US Traditional Diagnosis: FBS • Fasting blood glucose > 126 mg/dL • OGTT > 200 mg/dL (2 hour sample) • Any random testing >200 mg/dl should be referred for further testing • Random testing > 200 mg/dL with symptoms very suggestive of DM
Transcript of DM update 1 hr march 2018 ho - s3.amazonaws.com · α-Glucosidase Inhibitors Acarbose ......
3/14/18
1
DIABETESUPDATE2018
StevenFerrucci,OD,FAAOChief,Optometry,SepulvedaVA
Professor,SCCO/MBKU
What is diabetes?
• DM is a chronic disorder characterized by a lack of insulin or increased resistance to insulin
• Insulin is needed for proper uptake of glucose • Clinical result is hyperglycemia • Leads to microvascular damage
– retinopathy – nephropathy – neuropathy
Diabetes: Magnitude of Complications
Diabetic Retinopathy
Leading cause of blindness
in working age adults
Diabetic Neuropathy
Leading cause of non-traumatic lower extremity amputations
Diabetic Nephropathy
Leading cause of end-stage renal disease
Stroke
Cardiovascular Disease
2- to 4- fold increase in cardiovascular mortality and stroke
Diabetes:AnEpidemic
• >30millionpeopleintheUnitedStatescurrentlyhaveDM1
– Leadingcauseofvisuallossandnew-onsetblindnessinpaRentsaged20to74years1
– 40%to45%ofAmericansdiagnosedwithDMhavesomedegreeofDR2
• 84millionmorepeopleareathighrisk(prediabetes)3
1. NaRonalDiabetesStaRsRcsReport,2017.Atlanta,GA:NaRonalCenterforChronicDiseasePrevenRonandHealthPromoRon;2017.2. NaRonalEyeInsRtute.h_ps://nei.nih.gov/health/diabeRc/reRnopathy.AccessedJanuary16,2018.3. CentersforDiseaseControl.h_ps://www.cdc.gov/diabetes/basics/prediabetes.html.AccessedJanuary16,2018.
CostofCare
• ñfrom$172Billionin2007to$245Billionin2012-ñ41%– $176Bdirectcosts– $69Bindirect
• InCAalone,$24.5Billion(July2015)• Medicalcost2.3XhigherinptswithDM• CareofpeoplewithDMaccountsfor1out5healthcaredollarsinUS
Traditional Diagnosis: FBS
• Fasting blood glucose > 126 mg/dL • OGTT > 200 mg/dL (2 hour sample) • Any random testing >200 mg/dl should be referred
for further testing • Random testing > 200 mg/dL with symptoms very
suggestive of DM
3/14/18
2
Newer Diagnosis: HgbA1c
• Tells blood sugar control over 3 months – normal range 4% to 6% – 6-6.5 Pre-Diabetes – ≥ 6.5 would be indicative of DM – First major change in 30 years – In adults and children, not pregnant women
• Advantages: – Convenience: no fasting – More accurate: average over 3 months
MedicalManagementofDM
DRUGCLASS EXAMPLESGeneric(Trade)
Biguanide Meeormin(Glucophage®)
α-GlucosidaseInhibitors Acarbose(Precose®),miglitol(Glyset®)
Sulfonylureas Glipizide(Glucotrol®),glyburide(Micronase®),glimepiride(Amaryl®)
MegliRnides Repaglinide(Prandin®),nateglinide(Starlix®)
TZDs(glitazones) Pioglitazone(Actos),rosiglitazone(Avandia®)
DPP-4Inhibitors(dipepRdylpepRdase-4inhibitors)
SitaglipRn(Januvia®),saxaglipRn(Onglyza®),linaglipRn(Tradjenta®),aloglipRn(Nesina)
SGLT2Inhibitors(sodium-glucosecotransporter2inhibitors)
Canagliflozin(Invokana®),dapagliflozin(Farxiga®),empagliflozin(Jardiance®)
OralAgents1
1. GarberAJ,etal.AmericanAssociaRonofClinicalEndocrinologistscomprehensivediabetesmanagementalgorithm2013consensusstatement.EndocrPract.2013;19(3):536-557.
MedicalManagementofDM
DRUGCLASS EXAMPLESGeneric(Trade)
GLP-1Agonists(increRnmimeRcs) LiragluRde(Victoza®),exenaRde(Bye_a®),exenaRdeER(Bydureon®),dulagluRde(Trulicity™),albigluRde(Tanzeum®)
AmylinAnalogs PramlinRde(Symlin®)
InjectableNon-InsulinAgents1
1. GarberAJ,etal.AmericanAssociaRonofClinicalEndocrinologistscomprehensivediabetesmanagementalgorithm2013consensusstatement.EndocrPract.2013;19(3):536-557.
MedicalManagementofDM
DRUGCLASS EXAMPLESGeneric(Trade)
BasalInsulin Glargine(Lantus®),detemir(Levemir®),glargineU-300(Toujeo®)
Rapid-AcRngInsulinAnalogs Aspart(NovoLog®),lispro(Humalog®),glulisine(Apidra®),lisproU-200(Humalog®U-200)
PremixedInsulin 70:30,75:25,50:50(Humulin®,Novolin®)
RegularInsulin U-500(Humulin®R)
InhaledInsulin
Afrezza
InsulinTherapy1,2
1. GarberAJ,etal.AmericanAssociaRonofClinicalEndocrinologistscomprehensivediabetesmanagementalgorithm2013consensusstatement.EndocrPract.2013;19(3):536-557.2. AmericanDiabetesAssociaRon.Insulinbasics.h_p://www.diabetes.org/living-with-diabetes/treatment-and-care/medicaRon/insulin/insulin-basics.html.AccessedOctober14,2015.
MedicalManagementofDM
INSULINPUMPTHERAPYCOMPANY
EXAMPLES
Medtronic MiniMed®530G,Paradigm®Revel™
Tandem t:slim®,t:flex®
Insulet OmniPod®
Animas® Vibe™,OneTouch®Ping®
Accu-chek® Combo
InsulinDeliveryDevices
Current recommendations for DM
• Control BS levels – HgbA1c < 7
• Control HTN – <120/80
• Control Cholesterol levels – Total cholesterol < 200
• No smoking • Exercise • Yearly foot exams, dental exams, and dilated retinal
exams
3/14/18
3
Diabetic Retinopathy
• Leading cause of blindness 20-74 year old • 8-12% of all new cases of legal blindness • 50,000 Americans legally blind • Early diagnosis and treatment can decrease
vision loss by 50-60% • Factors which influence development of DR
– duration of disease – control of BS – Control of HTN
DuraRonofdisease
• Type1Pts:– ReRnopathyrarein1st3-5years– Aner10yrs,60%havesomereRnopathy– Aner20yrs,almostalwayspresent
• 50-60%PDR• Type2:
– ≈20%to39%havereRnopathyatRmeofdiagnosis
– Aner15years,60-80%havesomereRnopathy• 20%chanceofPDR
ControlofBloodSugar
• DCCT Trial: 1993 – Intensive blood glucose control reduced risk of
developing retinopathy by 76% – Slowed the progression by 54% if already had
retinopathy • UKPDS: 1998
– for every 1% decrease in HgbA1C there is a 35% reduction in risk for retinopathy
– 34% reduction in retinopathy progressing with good HTN control
Clinically Significant Macular Edema (CSME)
• Characteristics – retinal thickening at or within 500 microns (1/3 DD) of
center of macula – hard exudates at or within 1/3 DD if associated with
thickening of adjacent retina – thickening greater than 1 DD in size part of which is
within 1 DD of center of macular • May occur at any stage of retinopathy
CSME
• Level of Retinopathy – mild NPDR≈ 3%
incidence of DME – moderate to severe
NPDR ≈40% – Proliferative ≈ 71%
• Type 2: Duration and Insulin – no insulin
• 10 years 5% • 20 years 15%
– on insulin • 10 years 10% • 20 years 30-35%
DME
• OlddefiniRonsbeingreplacedwithneweronesbasedonOCTfindings– Central– Noncentral
• OCTbestwaytoevaluatereRnaforDME• DMEresponsibleformorecasesofmoderatevisuallossinptswithType2DMthanDR
• Newtreatments
3/14/18
4
Widefield Widefield
DME: Traditional Treatment FML
• ETDRS – 3711 pts, 22 centers, 10 years – Established focal macular laser (FML) as treatment
for CSME • PROS:
– Reduced risk of moderate vision loss by 50% – 95% chance of maintaining vision when guidelines
followed • CONS:
– 12% lost >15 letters at 3 years – <3% gained 15 letters – Diffuse, chronic, lipid deposits respond poorly
Steroids for DME
• Early2000’s,beforeanR-VEGF,IVTwaslookedattreatmentforDME– InhibitreducRonofPGs– Decreasespermeability– MaydecreaseVEGFproliferaRon
• DRCR.netOphthalmologySeptember2008• 848eyeswithCSMEandVAfrom20/40to20/320wereevaluated– At2yrs,laserismoreeffecRveandhasfewersideeffectsthaneither1or4mgintravitrealtriamcinolone
antiVEGF
• Lucentis, Avastin, Eylea • Shown in multiple studies to be beneficial
for DME – RISE
• 18.1% of pts in sham gained ≥ 15 letters vs. 44.8% (0.3 mg) or 39.2% (0.5 mg)
• 2.6 letters gained in sham vs. 12.5 (0.3mg) or 11.9 (0.5mg)
– RIDE – READ – VISTA – VIVID
OPTIONS
• Lucentis FDA approved for DME Feb 2015
• Eylea FDA approved for DME July 2016 • Avastin not FDA approved, but widely
used • Steroid implants
– Illuvien FDA approved Sept 2014 – Ozurdex FDA approved Sept 2014
3/14/18
5
Protocol –T: Lucentis vs Avastin vs Eylea for DME
• Oneyear
• Eyleagained13.3le_ers• LucenRs11.2• AvasRn9.7• NostaRsRcaldifference
• IfVAwas20/50orworse• Eyleagained18.9• LucenRs14.2• AvasRn11.8• StaRsRcally,Eyleabe_er
Protocol –T
• 2 year results – No statistically significant difference between 3
drugs, even in those worse than 20/50 • But better acuity with Eylea
– Bottom line: • It may matter which drug • May matter more with worse vision • Economics may dictate
– In order to justify use of lucentis/eylea vs avastin, price would have to decrease by 70-80%
PDR: Traditional Treatment PRP
• ETDRS – Established benefit of immediate PRP in patients
with PDR • PROS
– Showed an overall reduction rate of severe vision loss (ie 5/200) of approximately 50% in treated vs. untreated eyes
– <4% chance of severe vision loss in 5 years w/ tx • CONS
– Decreased VF – Decreased night vision – CME
Protocol S
• Non-inferior study evaluating Lucentis vs. PRP
• 55 sites, 203 pts with PRP, 191 with Lucentis, as frequent as q 4 weeks
• At 2 years: – VA improved 2.8 letters with Lucentis vs. 0.2
with PRP – More VF loss with PRP:. 531db vs. 213db loss – More vitrectomies in PRP group: 15% vs 4%
3/14/18
6
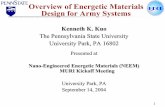
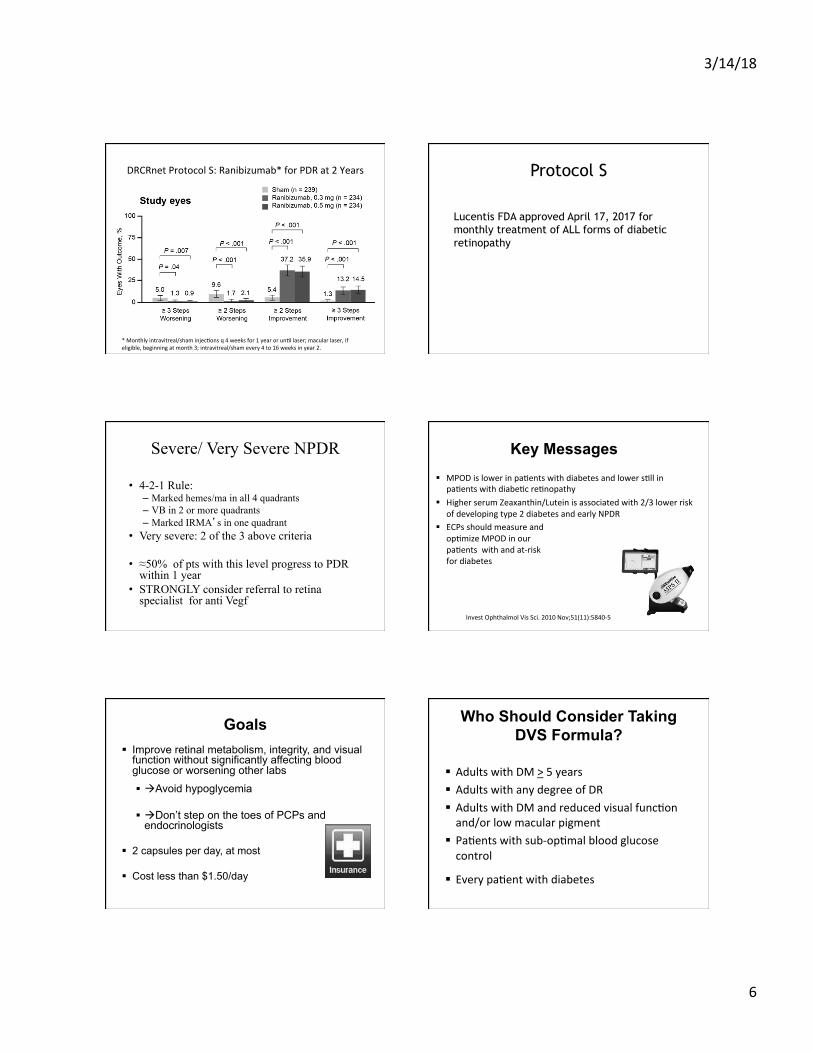
DRCRnetProtocolS:Ranibizumab*forPDRat2Years
*Monthlyintravitreal/shaminjecRonsq4weeksfor1yearorunRllaser;macularlaser,ifeligible,beginningatmonth3;intravitreal/shamevery4to16weeksinyear2.
Protocol S
Lucentis FDA approved April 17, 2017 for monthly treatment of ALL forms of diabetic retinopathy
Severe/ Very Severe NPDR
• 4-2-1 Rule: – Marked hemes/ma in all 4 quadrants – VB in 2 or more quadrants – Marked IRMA’s in one quadrant
• Very severe: 2 of the 3 above criteria
• ≈50% of pts with this level progress to PDR within 1 year
• STRONGLY consider referral to retina specialist for anti Vegf
Key Messages § MPODislowerinpaRentswithdiabetesandlowersRllin
paRentswithdiabeRcreRnopathy§ HigherserumZeaxanthin/Luteinisassociatedwith2/3lowerrisk
ofdevelopingtype2diabetesandearlyNPDR§ ECPsshouldmeasureand
opRmizeMPODinourpaRentswithandat-riskfordiabetes
InvestOphthalmolVisSci.2010Nov;51(11):5840-5
Goals § Improve retinal metabolism, integrity, and visual
function without significantly affecting blood glucose or worsening other labs
§ àAvoid hypoglycemia
§ àDon’t step on the toes of PCPs and endocrinologists
§ 2 capsules per day, at most
§ Cost less than $1.50/day
Who Should Consider Taking DVS Formula?
§ AdultswithDM>5years§ AdultswithanydegreeofDR§ AdultswithDMandreducedvisualfuncRonand/orlowmacularpigment
§ PaRentswithsub-opRmalbloodglucosecontrol
§ EverypaRentwithdiabetes
3/14/18
7
Summary of Facts § TheDiVFuSSformulasignificantlyimprovedvisualfuncRon,
diabeRcperipheralneuropathysymptoms,bloodlipidsandhsCRPinpaRentswithestablisheddiabetes-withoutsignificantlyaffecRngbloodsugarcontrol
§ TheDiVFuSSformulasignificantlyincreasedMPOD§ TheDiVFuSSformularepresentsanovel&complementary
strategytoexcellentmetaboliccontrolfordisrupRngthepathobiologyofdiabeRcreRnopathyandcorrecRngvisualfuncRondeficitscommonindiabetes
§ Noadverseeventsoccurredduringthestudy§ AvailableasEyePromise®DVSFormula
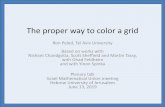
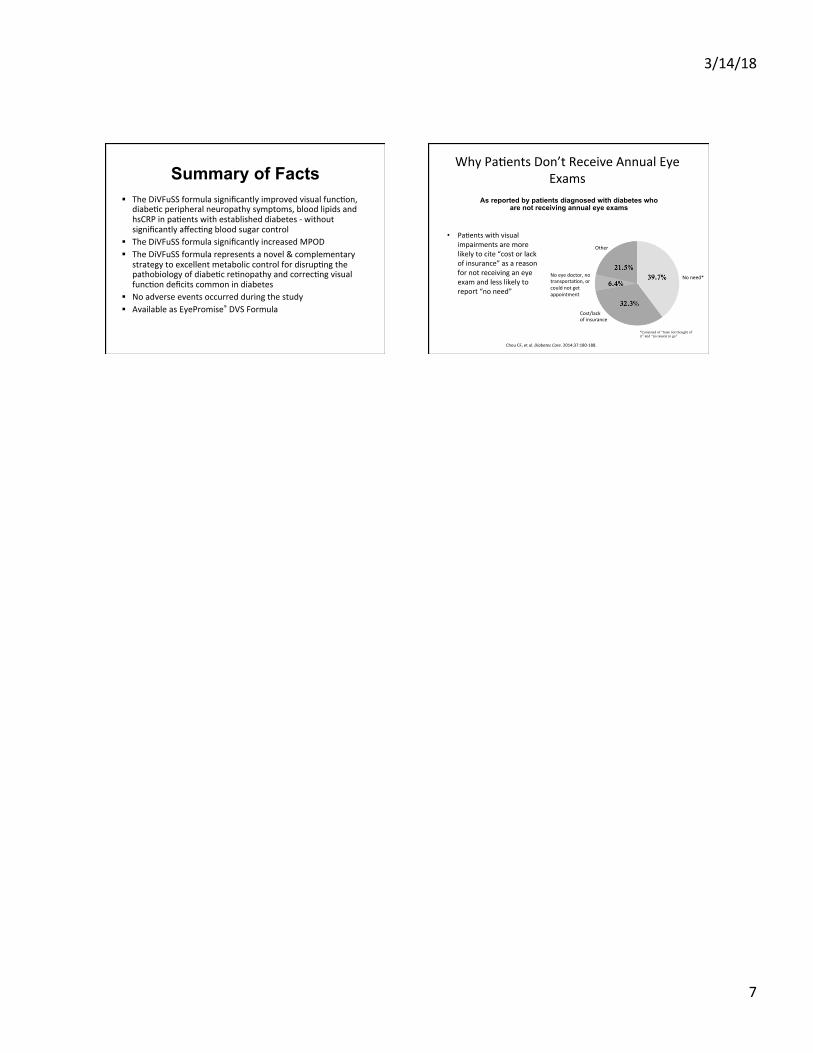
WhyPaRentsDon’tReceiveAnnualEyeExams
• PaRentswithvisualimpairmentsaremorelikelytocite“costorlackofinsurance”asareasonfornotreceivinganeyeexamandlesslikelytoreport“noneed”
ChouCF,etal.DiabetesCare.2014;37:180-188.
As reported by patients diagnosed with diabetes who are not receiving annual eye exams
Noneed*
Cost/lackofinsurance
Noeyedoctor,notransportaRon,orcouldnotgetappointment
Other
*Consisted of “have not thought of it” and “no reason to go”