Differential diagnosis of amyloidosis subtypes
48
Differential diagnosis of amyloidosis subtypes – Diagnosis and pitfalls Efstathios Kastritis Plasma Cell Dyscrasia Unit Department of Clinical Therapeutics National and Kapodistrian University of Athens
Transcript of Differential diagnosis of amyloidosis subtypes

Differential diagnosis of amyloidosis subtypes –
Diagnosis and pitfalls
Efstathios KastritisPlasma Cell Dyscrasia Unit
Department of Clinical Therapeutics National and Kapodistrian University of Athens

Patient’s Case
• 73 years old male • Known MGUS for the past 5 years, followed every ~2 years
by his hematologist • IgG(λ), M-spike: 19.6 g/L• Free K: 40 mg/L, Free L: 183 mg/L, ratio: 0.22, dFLC: 143• Concomitant diseases:
– Diabetes– Mild hypertension
• 6 months ago, the patient presents following symptoms – Fatigue– Mild dyspnea– Mild peripheral edema

Patient’s Case-cont’d
• Cardiac echo– EF: 55%
– IVS: 12 mm, PW: 11 mm
– Tissue Doppler E/E’(average): 13
– Hypokinesia of basal/middle IVS and posterior wall
– Diastolic dysfunction
• Echo conducted while in AF (~70 b/min)
• Positive cTnT is found in the ER
• CA no CAD

Patient’s Case-cont’d
• Symptoms continue and worsen – Difficulty sleeping and climb even a few steps
– Peripheral edema, Jugular veins (+)
– “Dizziness”
– Low blood pressure (90/50 mmHg)
– Lost his appetite and has lost weight
– Purpura over his trunk (receives acenocoumarol)

AL amyloidosis : is it rare ?
.
Ardissino et al. Eur J Pediatr. 2016;175:465-473. Cela et al. Pediatr Blood Cancer. 2017;64. Smith et al. Br J Cancer. 2015;112:1575-1584. Miller et al. Epidemiology. 2004;15:208-215. Ravindran et al. Blood Cancer J. 2016;e486. Roman et al. Cancer
Epidemiol. 2016;42:186-198. Moulard et al. Eur J Haematol. 2014;92:289-297. Quock et al. Blood. 2017;130(suppl 1):5335. Dunn. Hemophilia B. In: Transfusion Med Hemost. 2013;705-710. Blimark et al. Haematologica. 2018;103:506-513. National
Cancer Institute, www.seer.cancer.gov accessed 15 Jun 2018,
1. Kyle RA, et al. Blood 1992; 79: 1817–22; 2. Pinney JH, et al. Br J Haematol 2013;161: 525–32; 3. Hemminki K, et al. BMC Public Health 2012;12: 974; 4. Kyle R et al N Engl J Med 2018; 378 (3), 241-249.
0
10
20
30
40
50
60
70
Ne
w c
ase
s/m
illio
n
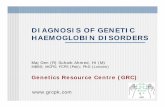
Rough estimate: ~ 1–2/10 of MM incidence1-4
Individuals with pre-existing MGUS have ~8 (range 4–15) times the risk of the general population4
Patients with myeloma may develop amyloidosis during the course of their disease

MGUS progression
MGUS(>3% of population ≥50 years)
Progression
10%90%
Progression to:• Smoldering multiple myeloma• Multiple myelomao 10%-15% of these patients will develop
concomitant light chain (AL) amyloidosis• Other lymphoplasmacellular disorders
Progression to:• AL amyloidosis• Light chain deposition disease• Other M-protein related disorders
Kyle et al. N Engl J Med. 2006;354:1362-1369; Merlini, Palladini. Hematology. 2012;2012:595-603; Dispenzieri et al. Blood Rev. 2012;26:137-154; Desikan et al. LeukemiaLymphoma. 1997;27:315-319; Kyle et al. N Engl J Med. 2018;378:241-249.

Kourelis T et al Am J Hematol 2014
“In patients with “asymptomatic” PCD, symptoms and signs of AL amyloidosis should be solicited, since timely diagnosis is important in AL amyloidosis.”

AL Amyloidosis patients visit several physicians until
they get diagnosed
Lousada et al Adv Ther. 2015; 32(10): 920–928.
The correct diagnosis was most frequently done by a hematologist/oncologist(only in 34.1% of cases)

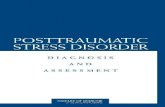
AL Amyloidosis: Clinical Presentation
65%71%
18%22% 20%
10%
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Heart Kidneys Liver PNS Purpura CTS SoftTissue
Data: Department of Clinical Therapeutics

AL Amyloidosis: Clinical signs and syndromes
Symptoms:Weight Loss, Dyspnea at Exertion, Postural hypotension, Peripheral neuropathy, Diarrhea, Peripheral edema, purpura, Carpal tunnel syndrome
8%
25%21%
13% 14%
10%6%
2% 1%0%
5%
10%
15%
20%
25%
30%
1 2 3 4 5 6 7 8 9
>90% of patients with AL present with symptoms from at least 2 different organ systems
Number of different symptoms
Data: Department of Clinical Therapeutics

AL Amyloidosis signs and symptoms
Modified from Merlini et al BLOOD, 27 JUNE 2013, VOLUME 121, NUMBER 26
Patient with suspected
systemic AL amyloidosis
Red flags for AL
• Unexplained high NT-proBNP
• Albuminuria
Signs and symptoms of AL
• Lethargy, fatigue• Weight loss• Peripheral Edema• Heart failure• Diarrhea/constipation• Peripheral and/or
autonomic neuropathy• Postural hypotension• Purpura

Amyloidosis – Echocardiography

Amyloidosis – Cardiac MRI

Amyloidosis – Bone and other new tracers

Amyloid typeOrgan involvement
Heart Kidney Liver PNS ANS Soft tiss.
AL amyloidosis ++ ++ + + + +
Hereditary ATTR amyloidosis ++ - ++ + (+)
Hereditary AApoAI amyloidosis ++ + ++ - - -
AA (reactive) amyloidosis ++ + - + -
Senile systemic amyl. (wtTTR)
median age 78++ - - - - -
Many different amyloid types can affect the heart

Amyloid typeOrgan involvement
Heart Kidney Liver PNS ANS Soft tiss.
AL amyloidosis ++ ++ + + + +
Hereditary ATTR amyloidosis ++ - ++ + (+)
Hereditary AApoAI amyloidosis ++ + ++ - - -
AA (reactive) amyloidosis ++ + - + -
Afib - + - - - -
Many different amyloid types can affect the kidneys

Diagnosis of Amyloidosis requires tissue biopsy
1. Fernández de Larrea C Blood 2015;125:2239-2244 2.
Tissue biopsy required
Target organ biopsy
Peripheral tissue biopsy (fat, salivary
etc)
Typing ?
Tissue of choice: abdominal fat1
Innocuous, fast, inexpensive:
sensitivity 75–80%,
specificity 80–100%
In ATTR sensitivity <30%2

Correct diagnosis of Amyloidosis requires typing
1Merlini G, et al. Expert Rev Hematol. 2014 Feb;7(1):143-56.2Geller HI, et al Mayo Clin Proc. 2017;92(12):1800-1805;
3Phull P et al Amyloid 2018;25(1):62-67.
Different types of amyloid have the same microscopic / ultramicroscopic appearance and all amyloid types stain positive with Congo Red1
Different types of amyloid may give similar or identical clinical presentations
MGUS is very common in subjects >65 years (those affected by ATTRwt)
The prevalence of MGUS in patients with ATTR is as high as 23%–39%1,2,3
! Different types of amyloid have different prognosis and management

Immunohistochemistry:– Better in fresh tissue
– Low sensitivity and specificity1
– Abs not optimized
– Expertise required
Immunoelectron microscopy: sensitive and specific but limited availability2
Genetic testing: easily available, reasonable cost
Proteomics– Gold standard by ISA recommendations3,4
– Available in few centers around the world
– Expensive and laborious
Amyloid typing
1 Gilbertson JA, et al J Clin Pathol. 2015;68(4):314-7; 2Fernández de Larrea C et al Blood 2015;125:2239-2244;3Brambilla F et al Blood 2012;119(8):1844-7; 4Vrana JA et al Haematologica 2014;99(7):1239-47

Non-invasive Diagnosis of cardiac ATTR

⁹⁹mTc-DPD-scintigraphyWechalekar et al. Lancet. 2016 Jun 25;387(10038):2641-2654
Non-invasive Diagnosis of cardiac ATTR
AL Patient ATTRwt Patient

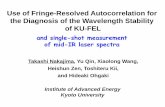
Diagnostic algorithm for patients with suspected amyloid cardiomyopathy
Gillmore JD, et al. Circulation. 2016;133:2404–2412

Giampaolo Merlini, Angela Dispenzieri , Vaishali Sanchorawala , Stefan O. Schönland , Giovanni Palladini, Philip N. Hawkins and Morie A. Gertz Nature Reviews Disease Primers (2018) 4:38

Diagnostic algorithm for amyloidosis
Suspicion of Amyloidosis
Is a monoclonal protein present?
MIg present MIg absent
Fat aspirateNon invasive imaging if
heart involvement ?
Fat aspirate (+) Fat aspirate (-)
Adapted from Merlini et al J Clin Oncol 2011

Diagnostic algorithm for amyloidosis
Suspicion of Amyloidosis
Is a monoclonal protein present?
MIg absent
Is MIg truly absent?
Were all available methods for MIg detection used ?• Serum Ifx• Urine Ifx• Serum FLCs

Detection of the Monoclonal immunoglobulin
• The amount of monoclonal protein is usually small
– Median serum M-peak < 0.5 gr/dl
– Negative serum IFx in 27%
– Median serum involved FLC : 160 mg/L
– Abnormal FLC ratio in 85%
– Negative urine IFx in ~ 40%
• Need to combine all available methods to identify the clonal light chain 1
Data: Department of Clinical Theurapeutics
1Palladini et al Clin Chem. 2009 Mar;55(3):499-504
commercial sIFE and uIFE : 96% sFLC: 76%. combination of sIFE & sFLC: 96% sIFE+uIFE+sFLCs: 100%

New methods to assess M-proteins using mass spectrometry
Mills JR et al Clinical Chemistry 2016

New methods to assess M-proteins using mass spectrometry
Milani P et al Am J Hematol 2017
N=6 with s‐IFE and FLC ratio (+) had serum MASS‐FIX (-)When serum and urine MASS‐FIX, only one LC MGUS missed. Serum/urine‐MASS‐FIX detected M‐proteins in 18 patients with negative s/u/PEL/IFE and sFLC
N=257 patients with paired samples

Diagnostic algorithm for amyloidosis
Suspicion of Amyloidosis
Is a monoclonal protein present?
MIg present
Fat aspirate
Fat aspirate (-)
What are the options ? 1. Repeat Fat aspirate
• increases slightly sensitivity 2. biopsy other tissue
• Salivary gland, gum: safe, increases sensitivity
3. biopsy target organ • Increases sensitivity, assess
feasibility & safety

CR remains the diagnostic standard experienced pathology lab is needed
False negative:– Thin sections
– Small amount of tissue
False positive: – Staining of elastin
– elastotic dermis, hyaline deposits in colloid milium, deposits of lipid proteinosis or hyaline material
– connective tissue that has been subjected to cautery
Congo Red for diagnosis of Amyloidosis
Flores-Fernandez A Biotechnic & Histochemistry 2011, 86(5): 293–301

New dyes and methods to stain and identify amyloid
• Novel amyloid-binding compounds have been developed
• New luminescent dyes– conjugated oligothiophenes
• fluorescent CR analogues – (E,E),-1-bromo-2,5-bis-(3-hydroxycarbonyl-4-hydroxy)styrylbenzene (BSB)
– (E,E)-1-fluoro-2,5-bis-(3-hydroxycarbonyl-4-hydroxy)styrylbenzene (FSB)
• Congo red fluorescence
Sjölander D, Amyloid. 2015;22(1):19-25. ; Sjölander D, Amyloid. 2016;23(2):98-108. ; Ando Y, Lab Invest. 2003;83(12):1751-1759. Sato K, Eur J Med Chem. 2004;39(7):573-578. ; Higuchi M Nat Neurosci. 2005;8(4):527-533. ; Tasaki M J Pathol. 2018 ; Giorgadze TA, Cytopathol. 2004;31(5):300-306. ; Linke RP. Virchows Arch. 2000;436(5):439-448. ; Clement CG Hum Pathol. 2014 Aug;45(8):1766-72.

Diagnostic algorithm for amyloidosis
Suspicion of Amyloidosis
Is a monoclonal protein present?
MIg present
Fat aspirate
Fat aspirate (+)
Typing

Can we use bone scintigraphy to
differentiate AL from ATTR ?
Gillmore JD, et al. Circulation. 2016;133:2404–2412

N=292 patients with AL amyloidosis
178/292 (61%) had no cardiac uptake on 99mTc-DPD scintigraphy
114/292 (39%) had cardiac uptake on 99mTc-DPD scintigraphy. – 85 had Perugini grade 1 uptake
– 20 had Perugini grade 2 uptake
– 9 had Perugini grade 3 uptake.
NT-proBNP, hsTnT Mayo stage III/IIIB higher in those with positive scans
The overall survival of patients with positive 99mTc-DPD scintigraphy was 6 months vs. 14 months in those negative scans
On a multivariate analysis, positivity on 99mTc-DPD scintigraphy was an independent predictor of survival.
Can we use bone scintigraphy to
differentiate AL from ATTR ?
J Zheng / A Wechalekar ISA meeting Kumamtoto 2018

Monoclonal Gammopathy in patients with ATTRwt
Phull P, et al Amyloid. 2018 Mar;25(1):62-67.

N=113 consecutive patients with ATTRwtMean age: 75 years, 97% males, 97% whites Monoclonal gammopathy was present in 26 patients (23%), 24 of whom had monoclonal protein present and 2 others who met criteria for light chain MG. Most clones (12 of 20 [60%]) were λ restricted.
Mayo Clin Proc. 2017;92(12):1800-1805

Retrospective analysis of n=143, cardiac biopsy proven amyloidosisATTR: in 81 (57%) AL : in 62 (43%)SPEP/UPEP/IFE was positive in 56/62 with AL , sFLC was abnormal in 53/62SPEP/UPEP/IFE was positive in 20/81 with ATTR, sFLC was abnormal in 8/81
SPEP/UPEP/IFE was poor predictor of AL amyloid : specificity (75%; 95% CI, 65-83%) and positive predictive value (PPV 74%; 95% CI, 63–82%).
FLC assay was a better predictor of AL amyloid : specificity (90%, 95% CI, 82–95%) andPPV (87%, 95% CI, 76–93%).

Proteomics for amyloid typing
Blood 2012
Haematologica 2014

The complementary role of histology and proteomics
for diagnosis and typing of systemic amyloidosis
Rezk T , Gilbertson JA et al J Pathol Clin Res. 2019

Fernandez de Larrea C et al Blood 2015

MALDI Mass Spectrometry Imaging: A Novel Tool for the
Identification and Classification of Amyloidosis
Winter M et al Proteomics 2017, 17, 1700236

Typing with LC/MS is the gold standard
– Availability
– Cost
Immunoelectron microscopy
– Availability
– Cost
Typing of amyloid deposits

Which patients to consider for typing by IEM or MS?(in a center that does not have access to either..)
• Positive bone scintigraphy and monoclonal protein present (especially if heart is the only involved organ or heart+PNS)
• Amyloid deposit in vital organ (kidney, heart, liver) that is not typed and no monoclonal protein is present (and genetic testing negative?)
• Other?

Fat aspirate in diabetic patients using insulin
• a 79‐year‐old female with Type 1 DM for 46 years, on recombinant insulin,
• presented to Cardiology with exertional dyspneaRBBB, 1st degree AV block; echo: concentric LV hypertrophy, IVS: 15 mm.
• NTproBNP: 2178 pg/ml
• CKD without proteinuria, hade tingling in hands and feet and she had lost 30 lbs.
• A fat aspiration was Congo red positive.
D'Souza A, et al Am J Hematol. 2012 Nov;87(11):E131-2.

N= 9 cases with either two types concurrently (N=8) or several years after the initial diagnosis (N=1)
ATTR in all nine cases
AL in 7/9 cases was the second amyloid type AA in 1/9 cases was the second type AIns was the second type

Giampaolo Merlini, Angela Dispenzieri , Vaishali Sanchorawala , Stefan O. Schönland , Giovanni Palladini, Philip N. Hawkins and Morie A. Gertz Nature Reviews Disease Primers (2018) 4:38

Going back to the case…
• Cardiac MR: consistent with amyloidosis
• Fat aspirate:
– Congo red (+)
• BM biopsy:
– Congo red (+)
– 15% BM plasma cells
• Should we wait for the results of typing or Congo red (+) is enough in this patient?
Tc99m-PYP Negative

Conclusions / Summary
• Suspicion is the first step to diagnose amyloidosis
• If the degree of suspicion is high investigation should continue despite initial negative results
• Need to combine all methods to confirm or exclude the presence of monoclonal gammopathy
• Clinical judgment is not enough but is required !
• Amyloid needs typing, but not all patients can be typed in routine practice