Diabetes type 1
31
When your child is too sweet By Dr Liaw Siew Ching
-
Upload
aizatsofian -
Category
Health & Medicine
-
view
184 -
download
0
Transcript of Diabetes type 1

When your child is too sweetBy Dr Liaw Siew Ching


IDDM/ Type I DM
• Introduction• Physiology of diabetes in β cell failure in
type 1 DM• DKA• Long term management of diabetes

• Definition of DM: - Symptoms of diabetes with random blood
sugar >11.1mmol/l or,- Fasting plasma glucose >7.0mmol/l (fast
for 8H) or,- 2 hour postload glucose >11.1mmol/l in
OGTT (glucose load with 75g anhydrous glucose desolved in water or 1.75g/kg)
Introduction

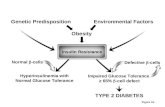
• Type I DM (95%) – Autoimmune destruction of the pancreatic islet cells
• Type 2 DM – A combination of β cell failure and insulin resistant
• Cystic fibrosis-related diabetes• Maturity onset diabetes of the young• Genetic syndromes( Down’s syndrome,
Wolfram syndrome, neonatal diabetes
Aetiology of diabetes in children

• Europe: Scandinavia and the UK have the highest rates of diabetes in Europe. There is a >10-fold difference in incidence across Europe, which might be accounted for in part by the distribution of high-risk HLA-DQ alleles.
• North America: Canada has incidence rates comparable to those of Northern Europe (22/100,000 per year). The US has a lower rate (16/100,000 per year), whereas Mexico has a rate of 1.5/100,000 per year.
• South America: Rates are generally low, except in Argentina and Uruguay.
• Africa (sub-Saharan): Estimated rates are generally low.
• Eastern Mediterranean and the Middle East: Rates vary between 1/100,000 per year (Pakistan) and 8/100,000 per year (Egypt).
• South-East Asia: A steady increase from a low baseline in countries such as India and China. Due to their vast populations, these will make a large contribution to the future global incidence of type 1 diabetes.
• Western Pacific: Rates are low, with the exception of Australia and New Zealand.
Epidemiology
http://www.diapedia.org/type-1-diabetes-mellitus/geography-of-type-1-diabetes#fn:4

Physiology of diabetes in β cell failure in type 1 DM

Physiology of diabetes in β cell failure in type 1 DM
• Lymphocytic infiltration destroying beta cells.• After 80-90% of the beta cells are destroyed, hyperglycemia develops.• 85% patients have circulating islet cell antibodies and detectable anti-
insulin antibodies. Commonly found islet cell antibodies are antibodies against glutamic acid decarboxylase (GAD), an enzyme found within pancreatic beta cells.

Physiology of diabetes in β cell failure in type 1 DM
• Insulin also increases the permiability of many cells to potassium, magnesium and phosphate ions. Insulin activates sodium-potassium ATPases in many cells, causing a flux of potassium into cells.

Classic symptoms
Nausealethargy

Physiology of diabetes in β cell failure in type 1 DM

Diabetic ketoacidosisLow insulin leads to DKA• Liver glycogen mobilization to form glucose• Muscle protein breakdown to form free amino
acids• Adipose tissue breakdown of triglycerides to
form free fatty acids which oxidized to form ketone bodies
• Excess glucose in glomerular filtrate leads to glucosuria.

DKA
Remember : children can die from DKA
Definition• Blood glucose > 11• Venous pH <7.3 or bicarbonate <15mmol/l• Ketonaemia or ketonuria (ketone 2+)

Remember : children can die from DKA
• BSPED Recommended DKA Guidelines 2009

Causes of DKA

Clinical presentation of DKA
• Dehydration, ketosis, acidosis, infection.

Assessment of severity• Present of one or more of the following may indicate severe DKA• Blood ketone over 6mmol/l• HCO3<5mmol/l• pH <7• Potassium <3.5mmol/l• GCS < 12• SPO2 <92%• Low BP• Tachycardia/bradycardia• Anion gap >16

Principle of management• General resuscitation• Confirm diagnosis• Full clinical assessment• Fluid management• Insulin


Management• FM + deficit. Initially use 1/2NS with 3/4g KCL• Continuous low dose intravenous infusion. No need bolus.• Make up a solution of 1 unit per ml of human soluble insulin
(e.g. Actrapid) by adding 50 units (0.5 ml) insulin to 50 ml 0.9% saline in a syringe pump. Attach this using a Y-connector to the IV fluids already running. Do not add insulin directly to the fluid bags.
• Run at 0.1 units/kg/hour (0.1ml/kg/hour). The insulin dose needs to be maintained at 0.1 units/kg/hour to switch off ketogenesis.
• There are some paediatricians who believe that 0.05 units/kg/hour is an adequate dose. There is no firm evidence to support this.

• Blood glucose level <14mmol/l, change the fluid to contain 5% glucose(generally 0.9% saline with glucose and potassium, see 1b above for type of fluid). DO NOT reduce the insulin.
• Some suggest if the initial rate of fall of blood glucose is greater than 5-8 mmol/lper hour, to help protect against cerebral oedema. There is no good evidence for this practice, and blood glucose levels will often fall quickly purely because of rehydration.
• If the blood glucose falls below 4 mmol/l, give a bolus of 2 ml/kg of 10% glucose and increase the glucose concentration of the infusion. Insulin can temporarily be reduced for 1 hour.
• Once the pH is above 7.3, the blood glucose is down to 14 mmol/l, and a glucosecontaining fluid has been started, consider reducing the insulin infusion rate, but to no less than 0.05 units/kg/hour.
• If the blood glucose rises out of control, or the pH level is not improving after 4-6 hours consult senior medical staffand re-evaluate (possible sepsis, insulin errors or other condition), and consider starting the whole protocol again.
• No role of bicarbonate.

HUSM DKA SOP 2009
• Although serum potassium appear normal, but total body potassium is low and worsened with insulin infusion.
Serum Potassium (mmol/l) Replacement<2.5 Fast correction
2.5-3.0 1.5g KCL in each pint
3.0-4.0 1.0g KCL in each pint
4.0-5.5 0.5g KCL in each pint

Target of therapy
• Reduction of blood ketone by 0.5mmol/l/h• Increase bicarb by 3mmol/l/h• Reduce capillary blood sugar by
3.0mmol/l/h• Maintain k+ between 4.0-5.5mmol/l

Resolution of DKA
• pH>7.3 units• Bicarb >15mmol/l• Blood ketone < 0.6mmol/l or urine ketone
nil.
• S/c insulin can be started.

Long Term Management of DM Type I• Principles of insulin therapyGuidelines on dosage:• During the partial remission phase, total daily insulin dose is usually 0.5
IU/kg/day. • Prepubertal children (outside the partial remission phase) usually require
insulin of 0.7–1.0 IU/kg/day.• During puberty, requirements may rise to 1 - 2 IU/kg/day.
Frequently used regimens:Twice Daily Regimens• 2 daily injections of a mixture of a short or rapid acting insulin with and • intermediate-acting insulins (before breakfast and the main evening meal)• Approximately 2/3 intermediate-acting insulin and 1/3 of the total daily
insulin dose is short acting insulin. Ex: Mixtard 70/30• 2/3 of the total daily dose is given in the morning and 1/3 in the evening

Three injections daily•A mixture of short, rapid and intermediate-acting insulins before breakfast; •A rapid-acting analogue or regular insulin alone before afternoon snack •or the main evening meal. And an intermediate- acting insulin before bed.Basal-bolus Regimen•Of the total daily insulin requirements, 40 - 60% should be basal insulin, the rest pre-prandial rapid-acting or regular insulin.•If using regular insulin, inject 20 - 30 min before each main meal (breakfast, lunch; and the main evening meal); if using rapid-acting insulin analogue inject immediately before or after each main meal (e.g. breakfast, lunch; and the main evening meal). •Basal cover is given once daily at bedtime. However sometimes twice daily injections may be needed (the other dose usually before breakfast). •Insulin pump regimens are regaining popularity with a fixed or a variable basal dose and bolus doses with meals.•Patient should learn about carbohydrate counting to adjust dose of pre-prandial insulin.
Long Term Management of DM Type I

Long Term Management of DM Type I

• Australian Clinical Practice Guidelines: Type 1 Diabetes in Children and Adolescents

• Calorie counting• Sick day management• Fasting and surgery
Long Term Management of DM Type I











![Trabalho ..Diabetes Mellitus[1]](https://static.fdocument.org/doc/165x107/5571fec049795991699c0766/trabalho-diabetes-mellitus1.jpg)

![Effects of Seeding on Lysozyme Amyloid Fibrillation in the ... · Alzheimer’s disease, type 2 diabetes, and several systemic amyloidoses [1-3]. These proteins, despite their unrelated](https://static.fdocument.org/doc/165x107/5f66a2f7828269373b7d097b/effects-of-seeding-on-lysozyme-amyloid-fibrillation-in-the-alzheimeras-disease.jpg)
![Journal of Diabetes and Metabolism - OMICS … subjects and normal rats [1-3], and Mudra et al. reported that ... type 2 diabetes treated with or without SU medicine and in healthy](https://static.fdocument.org/doc/165x107/5b2d900b7f8b9adc6e8bd83b/journal-of-diabetes-and-metabolism-omics-subjects-and-normal-rats-1-3-and-mudra.jpg)