Development of Ascites in Compensated Cirrhosis With Severe Portal Hypertension Treated With...
10
nature publishing group ORIGINAL CONTRIBUTIONS LIVER 418 The American Journal of GASTROENTEROLOGY VOLUME 107 | MARCH 2012 www.amjgastro.com INTRODUCTION e natural history of cirrhosis involves the progression from a compensated to a decompensated stage characterized by the development of complications, such as ascites, variceal bleeding, or encephalopathy (1,2). Decompensation is a key event herald- ing the onset of significant morbidity and mortality. Portal hyper- tension (PHT), usually estimated by the hepatic venous pressure gradient (HVPG), is involved in the development of most com- plications of cirrhosis and is the strongest predictor of clinical decompensation (2). Even in the compensated phase of cirrhosis, two stages with different probability of survival have been deline- ated based on the presence or absence of varices (1). Clinically significant PHT is diagnosed when HVPG is ≥ 10 mm Hg as both varices and decompensation of cirrhosis may appear at this point (3,4). However, once this threshold has been reached the relation- ship between changes in HVPG (such as those induced by drug therapy) and development of decompensation has not been suffi- ciently investigated. e prognostic value of HVPG monitoring to predict bleeding is well established (5), but its utility in the predic- tion of other complications is unclear. Ascites is the most frequent complication of cirrhosis and is oſten the first decompensation to appear (6–8). It has been demonstrated that, in patients with decompensated cirrhosis receiving drug therapy to prevent variceal rebleeding, a reduction of HVPG to < 12 mm Hg or ≥ 20% from baseline, in addition to a marked decrease in rebleeding risk, is also associated with a significant reduction of the risk of Development of Ascites in Compensated Cirrhosis With Severe Portal Hypertension Treated With β-Blockers Virginia Hernández-Gea, MD 1 , Carles Aracil, MD 2 , Alan Colomo, MD 1,3 , Isabel Garupera, MD 1 , Maria Poca, MD 1 , Xavier Torras, MD 1,3 , Josep Miñana, MD 2 , Carlos Guarner, MD 1,3 and Càndid Villanueva, MD 1,3 OBJECTIVES: In compensated cirrhosis, a threshold value of hepatic venous pressure gradient (HVPG) ≥10 mm Hg is required for the development of decompensation. However, whether the treatment of portal hypertension (PHT) can prevent the transition into development of ascites once this level has been reached is unclear. Our aim was to assess the relationship between changes in HVPG induced by β-blockers and development of ascites in compensated cirrhosis with severe PHT. METHODS: Eighty-three patients without any previous decompensation of cirrhosis, with large esophageal varices and HVPG ≥12 mm Hg were included. After baseline hemodynamic measurements nadolol was administered and a second hemodynamic study was repeated 1–3 months later. RESULTS: During 53±30 months of follow-up, decompensation occurred in 52 patients (62%) and in 81% of them ascites was the first manifestation. Using receiver operating characteristic curve analysis a decrease in HVPG ≥10% was the best cutoff to predict ascites. As compared with nonresponders, patients with an HVPG decrease ≥10% had a lower probability of developing ascites (19% vs. 57% at 3 years, P < 0.001), refractory ascites ( P = 0.007), and hepatorenal syndrome ( P = 0.027). By Cox regression analysis hemodynamic nonresponse was the best predictor of ascites. By stepwise logistic regression, development of ascites was independently associated with nonresponse, whereas refractory ascites, hepatorenal syndrome, and spontaneous bacterial peritonitis were not. CONCLUSIONS: In patients with compensated cirrhosis and large varices treated with β-blockers, an HVPG decrease ≥10% significantly reduces the risk of developing ascitic decompensation and other related compli- cations such as refractory ascites or hepatorenal syndrome. Am J Gastroenterol 2012; 107:418–427; doi:10.1038/ajg.2011.456; published online 14 February 2012 1 Gastrointestinal Bleeding Unit, Department of Gastroenterology, Servei de Patologia Digestiva, Hospital de la Santa Creu i Sant Pau, Universidad Autonoma de Barcelona, Barcelona, Spain; 2 Department of Gastroenterology, Hospital Arnau de Vilanova, Lleida, Spain; 3 Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd), Barcelona, Spain. Correspondence: Càndid Villanueva, MD, Gastrointestinal Bleeding Unit, Department of Gastroenterology, Servei de Patologia Digestiva, Hospital de la Santa Creu i Sant Pau, Avgda, Universidad Autonoma de Barcelona, Sant Antoni M Claret, 167, Barcelona 08025, Spain. E-mail: [email protected] Received 11 April 2011; accepted 11 October 2011 see related editorial on page 428
Transcript of Development of Ascites in Compensated Cirrhosis With Severe Portal Hypertension Treated With...

nature publishing group ORIGINAL CONTRIBUTIONS LI
VE
R
418
The American Journal of GASTROENTEROLOGY VOLUME 107 | MARCH 2012 www.amjgastro.com
INTRODUCTION Th e natural history of cirrhosis involves the progression from
a compensated to a decompensated stage characterized by the
development of complications, such as ascites, variceal bleeding,
or encephalopathy ( 1,2 ). Decompensation is a key event herald-
ing the onset of signifi cant morbidity and mortality. Portal hyper-
tension (PHT), usually estimated by the hepatic venous pressure
gradient (HVPG), is involved in the development of most com-
plications of cirrhosis and is the strongest predictor of clinical
decompensation ( 2 ). Even in the compensated phase of cirrhosis,
two stages with diff erent probability of survival have been deline-
ated based on the presence or absence of varices ( 1 ). Clinically
signifi cant PHT is diagnosed when HVPG is ≥ 10 mm Hg as both
varices and decompensation of cirrhosis may appear at this point
( 3,4 ). However, once this threshold has been reached the relation-
ship between changes in HVPG (such as those induced by drug
therapy) and development of decompensation has not been suffi -
ciently investigated. Th e prognostic value of HVPG monitoring to
predict bleeding is well established ( 5 ), but its utility in the predic-
tion of other complications is unclear. Ascites is the most frequent
complication of cirrhosis and is oft en the fi rst decompensation
to appear ( 6 – 8 ). It has been demonstrated that, in patients with
decompensated cirrhosis receiving drug therapy to prevent
variceal rebleeding, a reduction of HVPG to < 12 mm Hg or ≥ 20 %
from baseline, in addition to a marked decrease in rebleeding
risk, is also associated with a signifi cant reduction of the risk of
Development of Ascites in Compensated Cirrhosis With Severe Portal Hypertension Treated With β -Blockers Virginia Hern á ndez-Gea , MD 1 , Carles Aracil , MD 2 , Alan Colomo , MD 1 , 3 , Isabel Garupera , MD 1 , Maria Poca , MD 1 , Xavier Torras , MD 1 , 3 , Josep Mi ñ ana , MD 2 , Carlos Guarner , MD 1 , 3 and C à ndid Villanueva , MD 1 , 3
OBJECTIVES: In compensated cirrhosis, a threshold value of hepatic venous pressure gradient (HVPG) ≥ 10 mm Hg is required for the development of decompensation. However, whether the treatment of portal hypertension (PHT) can prevent the transition into development of ascites once this level has been reached is unclear. Our aim was to assess the relationship between changes in HVPG induced by β -blockers and development of ascites in compensated cirrhosis with severe PHT.
METHODS: Eighty-three patients without any previous decompensation of cirrhosis, with large esophageal varices and HVPG ≥ 12 mm Hg were included. After baseline hemodynamic measurements nadolol was administered and a second hemodynamic study was repeated 1 – 3 months later.
RESULTS: During 53 ± 30 months of follow-up, decompensation occurred in 52 patients (62 % ) and in 81 % of them ascites was the fi rst manifestation. Using receiver operating characteristic curve analysis a decrease in HVPG ≥ 10 % was the best cutoff to predict ascites. As compared with nonresponders, patients with an HVPG decrease ≥ 10 % had a lower probability of developing ascites (19 % vs. 57 % at 3 years, P < 0.001), refractory ascites ( P = 0.007), and hepatorenal syndrome ( P = 0.027). By Cox regression analysis hemodynamic nonresponse was the best predictor of ascites. By stepwise logistic regression, development of ascites was independently associated with nonresponse, whereas refractory ascites, hepatorenal syndrome, and spontaneous bacterial peritonitis were not.
CONCLUSIONS: In patients with compensated cirrhosis and large varices treated with β -blockers, an HVPG decrease ≥ 10 % signifi cantly reduces the risk of developing ascitic decompensation and other related compli-cations such as refractory ascites or hepatorenal syndrome.
Am J Gastroenterol 2012; 107:418–427; doi: 10.1038/ajg.2011.456; published online 14 February 2012
1 Gastrointestinal Bleeding Unit, Department of Gastroenterology, Servei de Patologia Digestiva, Hospital de la Santa Creu i Sant Pau, Universidad Autonoma de Barcelona , Barcelona , Spain ; 2 Department of Gastroenterology, Hospital Arnau de Vilanova , Lleida , Spain ; 3 Centro de Investigaci ó n Biom é dica en Red de Enfermedades Hep á ticas y Digestivas (CIBERehd) , Barcelona , Spain . Correspondence: C à ndid Villanueva, MD , Gastrointestinal Bleeding Unit, Department of Gastroenterology, Servei de Patologia Digestiva, Hospital de la Santa Creu i Sant Pau, Avgda, Universidad Autonoma de Barcelona , Sant Antoni M Claret, 167, Barcelona 08025 , Spain . E-mail: [email protected] Received 11 April 2011; accepted 11 October 2011
see related editorial on page 428

© 2012 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
419
LIV
ER
Development of Ascites in Compensated Cirrhosis
ascites, spontaneous bacterial peritonitis (SBP), hepatorenal syn-
drome, and also with an improvement in survival ( 9,10 ). However,
whether pharmacological treatment of PHT by reducing portal
pressure can prevent the transition of compensated cirrhosis into
development of ascites is unclear, particularly in the stage with
varices in which the risk of decompensation is higher. Further-
more, predictors of development of ascites in patients with com-
pensated cirrhosis and severe PHT remain undefi ned.
Th e aim of this study was to elucidate the relationship between
the changes in induced by β -blocker on PHT and development of
fi rst ascitic decompensation in patients with compensated cirrho-
sis, severe PHT, and large esophageal varices treated for primary
prophylaxis of bleeding. Other predictive factors of development
of ascites were also investigated.
METHODS All consecutive patients referred to our Hepatic Hemodynamic
Laboratory for entering into a program of prevention of fi rst
variceal bleeding episode were considered for inclusion in this
study. Patients were enrolled between January 2001 and January
2008, and were followed up until July 2009. Informed consent was
obtained from all the patients and the hospital ’ s ethics committee
approved the protocol.
Selection of patients Cirrhotic patients with large esophageal varices and without any
previous episode of gastrointestinal bleeding or previous his-
tory of ascites, jaundice, or encephalopathy were eligible. Cir-
rhosis was diagnosed by liver biopsy or by unequivocal clinical
and echographic fi ndings. Esophageal varices were diagnosed
by endoscopy performed in the previous 6 months by any of the
members of our bleeding unit and those with a diameter > 5 mm
were defi ned as large.
Th e NIEC (North Italian Endoscopie Club) index, a score which
includes Child-Pugh class and endoscopic parameters (size of
varices and red wale marks), was used to predict variceal bleeding
risk ( 11,12 ).
Exclusion criteria included contraindications to β -blockers,
hepatocellular carcinoma, Child-Pugh score > 10, splanchnic
venous thrombosis, age < 18 or > 80 years, treatment with diuret-
ics or with vasoactive drugs, and comorbidity expected to decrease
life expectancy to < 1 year.
Hemodynamic measurements and study design Hemodynamic studies were performed aft er an overnight fast.
Under local anesthesia, a catheter introducer was placed in the
right internal jugular vein using the Seldinger technique and was
used to advance, under fl uoroscopic guidance, a 7-F balloon-
tipped catheter into the right main hepatic vein and a Swan-Ganz
catheter into the pulmonary artery. Portal pressure was measured
as the HVPG, which is the diff erence between wedged and free
hepatic venous pressure. All intravascular pressure measurements
were performed in triplicate using a previously calibrated, highly
sensitive transducer, with external zero at the mild-axiliary line.
Permanent recording of tracings was obtained. Th e occluded
position was checked by the absence of refl ux aft er injection of
contrast medium. Cardiopulmonary pressures and cardiac out-
put were also measured. Electrocardiography, arterial pressure,
heart rate, and oxygen saturation were monitored noninvasively
throughout the study with an automatic monitor. To assess the
prognostic value of acute β -blockers test in a single hemody-
namic study, aft er completing baseline hemodynamic measure-
ments, a single intravenous bolus of 0.15 mg / kg of propranolol
was administered and 20 min later hemodynamic measurements
were repeated.
Continuous treatment with nadolol was started immediately aft er
the baseline hemodynamic study. Nadolol was administered orally
with a starting dose of 40 mg once daily. Th is was subsequently
adjusted over 1 – 2 weeks, with a stepwise increase or decrease of
20 mg every 2 – 3 days up to the maximum tolerate dose without
reducing resting heart < 50 beats per minute or up to 240 mg per day.
A second hemodynamic study was repeated 1 – 3 months later to
evaluate chronic response. Hemodynamic response was not pre-
defi ned.
Sodium restricted diet, without fl uid restriction, was indicated
in all cases. Nadolol was used for primary prophylaxis of variceal
bleeding. Endoscopic variceal ligation was indicated in case of
intolerance to β -blockers.
Follow-up Aft er inclusion, patients were followed at months 1 and 3, and
every 6 months thereaft er. Each visit included physical examina-
tion, blood tests, and abdominal ultrasound. Treatment adher-
ence was assessed by extensive interrogation with the patient and
relatives and by heart rate measurements. Follow-up data were
gathered for at least 18 months or until liver transplantation or
death. Th e end points evaluated were development of ascites or
complications of ascites (refractory ascites, SBP, hepatorenal syn-
drome). Development of other decompensations (bleeding and
encephalopathy) and death from any cause were also evaluated.
Ascites were defi ned by the presence of signs and symptoms
suggestive of ascites on physical examination and was always con-
fi rmed on ultrasonography or paracentesis. Th e diagnostic criteria
for refractory ascites, hepatorenal syndrome, and SBP were those
proposed by the International Ascites Club ( 13 ). Gastrointestinal
bleeding was defi ned as any episode of hematemesis or melena,
or both, that occurred during the follow-up and was evaluated by
emergency endoscopy. Variceal bleeding was defi ned according to
the Baveno IV criteria ( 14 ). Any death occurring during follow-up
was recorded. Patients lost to follow-up were censored as alive the
day of the last visit.
Statistical analysis Statistical analysis was performed according to an intention-to-
treat strategy.
Categorical variables, which are reported as frequencies, were
compared using the Fisher exact test. Continuous variables, which
were reported as mean values ± standard deviations, were com-
pared using the unpaired Student ’ s t -test or the nonparametric

The American Journal of GASTROENTEROLOGY VOLUME 107 | MARCH 2012 www.amjgastro.com
420 LI
VE
R
Hern á ndez-Gea et al.
Mann – Witney rank-sum test. Actuarial probabilities were calcu-
lated according to the Kaplan – Meier method and compared using
the Long-rank test. Follow-up was censored at the time of death,
liver transplantation, or last visit. Th e possible role of confound-
ing variables was investigated with the Cox proportional hazards
regression analysis or with stepwise logistic regression (SLR) anal-
ysis, by introducing covariates that were related to the analyzed
events in a univariate analysis ( P ≤ 0.1). Th e maximum number of
variables included in the multivariate analysis was 1 per 5 – 10 out-
comes. Th e contribution of each signifi cant variable to the risk of
reaching the end point was estimated by the relative hazard with
its 95 % confi dence interval (CI). Stratifi cation according to diff er-
ent risk subsets groups, with respect to ascites development, was
made by classifi cation-and-regression-tree analysis. All P values
were two-tailed and the level of values of less statistical signifi -
cance was taken at P < 0.05. Th e relationship between the sensitiv-
ity and specifi city of the HVPG value at diff erent cutoff points, as
a predictor of ascites development during follow-up, was evalu-
ated from a receiver operating characteristic (ROC) curve. Cal-
culations were performed with SPSS18 statistical package (SPSS,
Chicago, III).
RESULTS From a group of 204 patients eligible for the study, 121 had one
or more exclusion criteria of whom 94 had previous history of
ascites. Th e remaining 83 were fi nally included. During a mean
follow-up of 53 ± 30 months, 52 patients (62 % ) decompensate. Th e
fi rst decompensation to appear was ascites in 42 / 52 cases (81 % ),
variceal bleeding in 9 / 52 (17 % ), and encephalopathy in only 1.
Overall, 49 patients (59 % ) developed ascites, 13 patients (16 % )
SBP, and 11 (13 % ) patients hepatorenal syndrome. In all, 14
patients (17 % ) had a fi rst variceal bleed, hepatocellular carcinoma
occurred in 12 (14 % ), 5 underwent liver transplantation and 25
patients (30 % ) died.
Nine patients (11 % ) did not receive nadolol. Th is was because
of treatment nonadherence in two patients and due to complica-
tions in seven patients. Th e second hemodynamic study was not
performed in fi ve patients because of decision of the attending
physician in three and refusal to in two. Four of them developed
ascites.
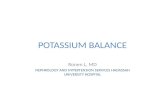
Hemodynamic response to β -blockers and decompensation of cirrhosis Th e diagnostic accuracy to predict development of ascites
as measured by changes in HVPG while receiving chronic
treatment with nadolol was evaluated using ROC curve analysis
( Figure 1 ) and discriminative ability was good ( c statistic, 0.84;
95 % CI, 0.73 – 0.92). Th e optimal cutoff point was a ≥ 10 % reduc-
tion in HVPG, with 87 % sensitivity and 80 % specifi city. Accord-
ingly, patients were classifi ed as hemodynamic responders when
the HVPG decreased by ≥ 10 % from baseline.
Compared with nonresponders, responders had better NIEC
index, better degree of β -blockade, and a trend toward better
adherence to treatment with nadolol. Th ere were no other
diff erences between responders and nonresponders in baseline
data ( Table 1 ).
Compared with nonresponders, responders had a lower risk
of developing ascites ( Figure 2 ). In all, 11 responders (27 % ) and
34 nonresponders (89 % ) had ascites during the follow-up period
( P < 0.001). Th e likelihood of ascites was also lower in responders in
an analysis excluding the nine patients (three responders) who did
not receive nadolol due to complications or nonadherence (48 %
vs. 18 % at 2 years, P = 0.001). To treat ascites, diuretics were used
in 32 (74 % ) nonresponders vs. 11 (27 % ) responders ( P < 0.001). As
compared with nonresponders, responders also have a lower prob-
ability of developing refractory ascites ( Figure 2 ) and hepatorenal
syndrome. Transient hypovolemia-induced renal failure occurred
in two responders (5 % ) and in fi ve nonresponders (13 % ; P = 0.28).
Th ere was a trend toward a lower probability of developing SBP in
responders (7 % vs. 2 % at 2 years, P = 0.4).
As expected, the likelihood of fi rst bleeding was signifi cantly
higher in nonresponders (17 % vs. 5 % at 2 years, P = 0.001), as
well as the likelihood of a fi rst variceal bleeding (14 % vs. 5 % at 2
years, P = 0.01). Th e probability of developing encephalopathy was
slightly lower in responders, although the diff erence was not sig-
nifi cant (16 % vs. 6 % at 2 years, P = 0.14).
By SLR, both fi rst bleeding (hazard ratio (HR) = 6.3, 95 % CI = 1.1 –
35; P = 0.03) and ascites (HR = 14.5, 95 % CI = 4 – 53; P < 0.001) were
independently associated with hemodynamic nonresponse. In
another SLR model that included ascites, refractory ascites, hepa-
torenal syndrome, and SBP, only development of ascites was inde-
pendently associated with hemodynamic nonresponse (HR = 22,
95 % CI = 7 – 77; P < 0.001).
Acute hemodynamic response to β -blockers and development of ascites Using ROC curve analysis, the discriminative ability of acute
HVPG changes aft er intravenously administration of propranolol
Sen
sitiv
ity
1 - Specificity
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
Figure 1 . Receiver operating characteristic curves of acute and chronic response to β -blockers for development of ascites. Continuous line repre-sents hepatic venous pressure gradient (HVPG) changes after the chronic administration of nadolol and discontinuous line represents HVPG changes after the acute administration of intravenously propranolol. The diagnostic performance of chronic changes was better than that of acute changes, with c statistic of 0.84 (0.73 – 0.92) vs. 0.74 (0.61 – 0.84), P = 0.04.

© 2012 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
421
LIV
ER
Development of Ascites in Compensated Cirrhosis
Table 1 . Characteristics of chronic hemodynamic responders and nonresponders at admission and during follow-up a
Responders �
( N =40)
Non-responders ( N =38) P value
Sex (M / F) 21 / 19 17 / 21 0.32
Age (years) 62 ± 10 63 ± 10 0.83
Cause of cirrhosis ( % ) 0.21
Alcohol 7 (17) 7 (18)
HCV 25 (62) 23 (60)
Alcohol + HCV 7 (17) 4 (10)
Associated diseases ( % ) 19 (47) 17 (45) 0.82
Albumin (g / l ) 35 ± 6 34 ± 5 0.15
Bilirubin ( μ mol / l) 35 ± 60 36 ± 26 0.93
Prothrombin time, INR 1.24 ± 0.5 1.27 ± 0.5 0.21
Creatinine ( μ mol / l) 85 ± 16 82 ± 13 0.38
Hemoglobin (g / l) 124 ± 19 116 ± 22 0.11
Platelet count ( × 10 − 3 ) 102 ± 50 104 ± 53 0.86
Child-Pugh class, A / B / C ( % ) 37 (92) / 2 (5) / 1 (2)
32 (84) / 6 (16) / 0
0.19
Child-Pugh score 6.5 ± 1.6 7.2 ± 1.7 0.10
MELD score 10 ± 4 12 ± 4 0.09
NIEC index 27 ± 4 31 ± 5 0.001
Variceal grade, II / III ( % ) b 35 (87) / 5 (13)
35 (92) / 3 (8)
0.49
Red weal marks ( % ) 15 (37) 16 (42) 0.82
Gastric varices ( % ) c 3 (7) 1 (3) 0.62
Hemodynamic variables (baseline values and chronic changes) d
Baseline pulmonary artery pressure (mm Hg)
17.9 ± 5 16.3 ± 4 0.14
Change from baseline ( % ) + 21 ± 47 + 12 ± 37 0.39
Baseline pulmonary wedge pressure (mm Hg )
11.1 ± 5 9.8 ± 4 0.19
Change from baseline ( % ) + 41 ± 66 + 22 ± 59 0.22
Baseline right atrial pressure (mm Hg )
6.5 ± 3 5.5 ± 3 0.49
Change from baseline ( % ) + 95 ± 72 + 63 ± 83 0.21
Baseline heart rate (beats / min)
77 ± 13 77 ± 11 0.86
Change from baseline ( % ) − 27 ± 13 − 12 ± 20 0.001
Decrease by > 10 % from baseline ( % )
39 (97) 24 (63) < 0.001
Decrease by > 25 % from baseline ( % )
23 (58) 11 (29) 0.01
Baseline mean arterial pressure (mm Hg)
89 ± 12 87 ± 11 0.44
Change from baseline ( % ) − 4 ± 10 − 4 ± 11 0.86
Baseline cardiac output (l / min) 7.1 ± 1.7 7.3 ± 1.9 0.42
Change from baseline ( % ) − 18 ± 16 − 15 ± 13 0.01
Table 1 . Continued
Responders
( N =40)
Non-responders ( N =38) P value
Decrease by > 10 % from baseline ( % )
33 (85) 21 (58) 0.02
Systemic vascular resistance (dyn.s / cm 5 )
1,000 ± 336 951 ± 303 0.51
Change from baseline ( % ) + 17 ± 31 + 12 ± 27 0.52
Baseline WHVP (mm Hg) 27.0 ± 5 25.1 ± 5 0.11
Change from baseline ( % ) − 5 ± 15 + 5 ± 22 0.02
Baseline FHVP (mm Hg) 9.6 ± 3 8.3 ± 4 0.15
Change from baseline ( % ) + 28 ± 47 + 27 ± 80 0.91
Baseline HVPG (mm Hg) 17.4 ± 3 16.8 ± 3 0.45
Change from baseline ( % ) − 19 ± 6 + 1 ± 13 < 0.001
Decrease by 20 % from baseline ( % )
17 (42) 0 < 0.001
Decrease to < 12 mm Hg ( % ) e 12 (30) 1 (3) 0.002
Follow-up
Nadolol dose (mg per day) 73 ± 35 64 ± 48 0.41
Withdrawal of nadolol ( % ) f 2 (5) 7 (8) 0.08
Compliance: good / fair / poor ( % ) g
33 (83) / 5 (12) / 2 (5)
23 (60) / 9 (24) / 6 (16)
0.08
Abstinence from alcohol ( % ) 9 / 14 (64) 6 / 11 (54) 0.69
Hepatocellular carcinoma ( % ) 6 (15) 6 (16) 0.99
Duration of follow-up (months) 0.43
Mean 54 ± 30 59 ± 30
Median 52 63
Range 6 – 96 9 – 96
Lost of follow-up ( % ) h 4 (10) 1 (3) 0.61
F, female; FHVP, free hepatic venous pressure; INR, International Normalized Ratio; M, male; HVPG, hepatic venous pressure gradient; NIEC, North Italian Endoscopie Club; WHVP, wedge hepatic venous pressure . a Patients were considered responders when in the second hemodynamic study, performed after 1 – 3 months of treatment with nadolol, the HVPG decreased by > 10 % from baseline. Plus-minus values are means ± s.d. b Grade I denotes varices that were fl attened by insuffl ation (all had red weal marks), grade II varices that were not fl attened by insuffl ation and were sepa-rated by areas of normal mucosa, and grade III confl uent varices that were not fl attened by insuffl ation. c Patients with esophageal and fundal varices (gastroesophageal varices type 2 according to Sarin’s classifi cation). d Baseline values and values obtained in the second hemodynamic study. e The fi nal value of HVPG was < 12 mm Hg in 13 patients. Only in 1 of them (of the responders group) the fi nal value of HVPG was < 10 mm Hg. f Two patients among responders and seven patients among nonresponders did not receive nadolol because of side-effects (six nonresponders) or nonadher-ence (two nonresponderss). These nine patients received endoscopic variceal ligation for primary prophylaxis of bleeding. g Adherence to treatment was considered good when doses of nadolol were rarely or never missed, fair when one or less doses were missed per week on average, and poor when ≥ 2 doses were missed per week. h Three patients in the responders group were lost to follow-up between at 31 and 60 months, and 1 patient in the nonresponders group was lost to follow-up at 41 month. � Patients were considered acute hemodynamic responders when the HVPG decreased by ≥ 10 % from baseline in the acute test to intravenous propranolol performed during the baseline study.

The American Journal of GASTROENTEROLOGY VOLUME 107 | MARCH 2012 www.amjgastro.com
422 LI
VE
R
Hern á ndez-Gea et al.
independent predictors of development of ascites, whereas base-
line glomerular fi ltration rate and systemic vascular resistance
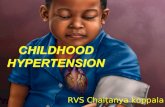
were not. Th e classifi cation-and-regression-tree method identi-
fi ed chronic hemodynamic response as the best single predictor
for development of acites ( Figure 3 ). In responders, the MELD
score provided additional prognostic value. A simple risk tree
identifi ed groups with ascites development ranging from 18 to
89 % ( Figure 3 ).
Patients who develop ascites had a signifi cantly higher rate of
fi rst variceal bleeding and of encephalopathy, than patients with-
out ascites. In all, 13 patients developed both ascites and variceal
bleeding. In seven of them (54 % ), ascites occurred before bleeding
and in three patients (23 % ) both decompensations occurred at the
same time. In all, 18 patients developed both ascites and encepha-
lopathy. In nine of them (50 % ), ascites occurred before and in six
patients (33 % ) both decompensations occurred at the same time.
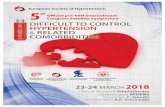
Survival and development of decompensation Th e probability of survival was signifi cantly better in patients who
remained compensated than in those who developed an initial
decompensation of PHT (ascites, bleeding, or encephalopathy;
Figure 4 ). Twenty-three decompensated patients (44 % ) died (all
had ascites), as compared with two (6 % ) compensated. Death was
related to liver failure in 13 patients, to hepatocellular carcinoma
in 5, to bleeding in 4, sepsis in 2, and was unrelated with liver
disease in 1 patient.
Th e probability of survival was lower in patients who developed
ascites than in those who did not ( Figure 4 ), in patients who had
was good ( c statistic, 0.74; 95 % CI, 0.61 – 0.84; Figure 1 ). Th e
diagnostic performance of acute HVPG changes was worse than
that of chronic changes (diff erence between areas = 0.12 ± 0.05,
P = 0.04). Th e optimal cutoff point for acute changes was a > 9 %
reduction in HVPG and this threshold was used to defi ne acute
response. As compared with nonresponders, acute respond-
ers had a signifi cantly lower risk of developing a fi rst episode of
ascites (17 % vs. 49 % at 2 years, P = 0.005), lower risk of refractory
ascites (5 % vs. 18 % at 2 years, P = 0.03), and a trend toward lower
probability of developing hepatorenal syndrome (11 % vs. 0 % at 2
years, P = 0.3).
Predictors of risk of fi rst ascitic decompensation Patients who developed fi rst ascitic decompensation had lower
baseline systemic vascular resistance and lower glomerular fi ltra-
tion rate than patients who remained compensated. Th e baseline
MELD score was also signifi cantly higher in patients who devel-
oped ascites. Th ere were no other diff erences in baseline clinical
and hemodynamic parameters between patients who develop
ascites and patients compensated ( Table 2 ). Both, the rate of acute
and chronic hemodynamic response were signifi cantly lower in
patients who developed ascites. Th e incidence of fi rst variceal
bleeding and the incidence of encephalopathy were signifi cantly
higher in patients who had ascites than in those who had not. No
other parameters during follow-up were diff erent between patients
who had or had not ascites ( Table 2 ). In the multivariate analysis,
chronic hemodynamic nonresponse (HR = 3.2; 95 % CI = 1.5 – 6.4)
and baseline MELD score < 9 (HR, 1.9; 95 % CI = 1.0 – 3.50) were
Pro
babi
lity
of b
eing
free
of a
scite
s
1.0a
b c
0.8
0.6
0.4
0.2
0.0
040
Patients at riskResponders
Nonresponders
Responders
Nonresponders
32 26 21 18 16 11 8 6 41236111315192438
12 24 36 48 60 72 84 96 108 120 Months
Pro
babi
lity
of b
eing
free
of r
efra
ctor
y as
cite
s
Pro
babi
lity
of b
eing
free
of h
epat
oren
al s
yndr
ome1.0
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.0
Responders
Nonresponders
Responders
Nonresponders
0 12 24 36 48 60 72 84 96 108
120 Months 0 12 24 36 48 60 72 84 96 10
812
0 Months
Figure 2 . Probability of ascites ( a ), refractory ascites ( b ), and hepatorenal syndrome ( c ) according to hemodynamic response (defi ned as a decrease in hepatic venous pressure gradient decrease > 10 % from baseline). As compared with nonresponders (dashed line), hemodynamic responders (continuous line) have a signifi cantly higher probability of developing: ( a ) ascites ( P < 0.001), ( b ) refractory ascites ( P = 0.007), and ( c ) hepatorenal syndrome ( P = 0.027).

© 2012 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
423
LIV
ER
Development of Ascites in Compensated Cirrhosis
Table 2 . Characteristics of patients who developed a fi rst ascitic decompensation and patients who remained compensated, at admission and during follow-up a
Remained compensated
( N =34)
Developed ascites ( N =49) P value
Sex (M / F) 20 / 14 20 / 29 0.12
Age (years) 63 ± 12 66 ± 9 0.18
Cause of cirrhosis ( % ) 0.53
Alcohol 8 (23) 7 (14)
HCV 18 (53) 33 (67)
Alcohol + HCV 5 (15) 6 (12)
Associated diseases ( % ) 18 (53) 29 (59) 0.60
Albumin (g / l) 38 ± 6 37 ± 5 0.26
Bilirubin ( μ mol / l) 22 ± 28 24 ± 14 0.77
Prothrombin time, INR 1.2 ± 1.6 1.2 ± 1.5 0.62
Urea (mmol / l) 6.1 ± 1.9 5.9 ± 2.9 0.77
Creatinine ( μ mol / l) 85 ± 16 82 ± 13 0.38
Glomerular fi ltration rate (ml / min per 1.73 m 2 ) b
83 ± 15 73 ± 15 0.007
Serum sodium (mmol / l) 140 ± 3 139 ± 3 0.29
Hemoglobin (g / l) 125 ± 24 126 ± 20 0.93
Platelet count ( × 10 − 3 ) 97 ± 42 87 ± 47 0.77
Child-Pugh class, A / B / C ( % ) 31 (91) / 2 (6) / 1 (3)
40 (82) 9 (18) / 0
0.13
Child-Pugh score 5.6 ± 1.2 5.8 ± 0.9 0.31
MELD score 7.4 ± 3 8.8 ± 3 0.05
NIEC index 25 ± 3 24 ± 3 0.42
Variceal grade, II / III ( % ) 28 (76) / 6 (18)
47 (90) / 2 (4)
0.12
Red weal marks ( % ) 16 (47) 16 (33) 0.14
Gastric varices ( % ) 2 (6) 2 (4) 0.99
Hemodynamic variables (baseline values and chronic changes) c
Baseline pulmonary artery Pressure (mm Hg)
17.9 ± 5 17.43 ± 5 0.68
Change from baseline ( % ) 15 ± 48 18 ± 38 0.77
Baseline pulmonary wedge pressure (mm Hg)
11.4 ± 4 10.1 ± 4 0.14
Change from baseline ( % ) 27 ± 70 35 ± 59 0.61
Baseline right atrial pressure (mm Hg)
6.8 ± 3 5.6 ± 3 0.15
Change from baseline ( % ) 85 ± 136 75 ± 89 0.83
Baseline heart rate (beats / min)
75 ± 11 79 ± 12 0.21
Change from baseline ( % ) − 24 ± 14 − 18 ± 19 0.08
Decrease by > 10 % from baseline ( % )
23 (85) 32 (80) 0.35
Decrease by > 25 % from baseline ( % )
11 (41) 16 (40) 0.32
Table 2 . Continued
Remained compensated
( N =34)
Developed ascites ( N =49) P value
Baseline mean arterial pressure (mm Hg)
89 ± 12 86 ± 11 0.28
Change from baseline ( % ) − 3 ± 12 − 6 ± 8 0.24
Baseline cardiac output (l / min) 6.9 ± 1.8 7.5 ± 1.9 0.13
Change from baseline ( % ) − 16 ± 14 − 15 ± 15 0.93
Decrease by > 10 % from baseline ( % )
16 (67) 23 (62) 0.07
Systemic vascular resistance (dyn.s / cm 5 )
1053 ± 383 908 ± 263 0.05
Change from baseline ( % ) 17 ± 33 13 ± 26 0.53
Baseline WHVP (mm Hg) 26.6 ± 5 26.0 ± 5 0.62
Change from baseline ( % ) − 6 ± 14 4 ± 21 0.03
Baseline FHVP (mm Hg) 10.2 ± 3 8.6 ± 3 0.09
Change from baseline ( % ) 19 ± 48 34 ± 74 0.29
Baseline HVPG (mm Hg) 16.4 ± 3 17.5 ± 3 0.11
Change from baseline ( % ) − 18 ± 9 − 4 ± 15 < 0.001
Decrease by 10 % from baseline ( % )
29 (88) 11 (24) < 0.001
Decrease to < 12 mm Hg ( % ) d 11 (33) 2 (4) 0.0012
Follow-up
Nadolol dose (mg per day) 64 ± 35 82 ± 39 0.34
Withdrawal of nadolol ( % ) e 3 (9) 6 (12) 0.39
Compliance: good / fair / poor ( % ) 28 (82) / 4 (12) / 2 (6)
32 (65) / 11 (23) / 6 (12)
0.23
Abstinence from alcohol ( % ) 9 / 12 (75) 8 / 13 (61) 0.67
Variceal bleeding 1 (3) 13 (26 % ) 0.006
Encephalopathy 5 (16) 18 (39) 0.04
Hepatocellular carcinoma ( % ) 4 (12) 8 (16) 0.64
Duration of follow-up (months) 0.22
Mean 47 ± 29 57 ± 30
Median 48 60
Range 6 – 96 6 – 96
Lost of follow-up ( % ) f 3 (9) 2 (5) 0.58
F, female; FHVP, free hepatic venous pressure; INR, International Normalized Ratio; M, male; HVPG, hepatic venous pressure gradient; NIEC, North Italian Endoscopie Club; WHVP, wedge hepatic venous pressure. a Patients included had not previous decompensations. Development of ascites was always confi rmed by ultrasonography or paracentesis. Plus-minus values are means ± s.d. See footnotes in Table 1 . b Glomerular fi ltration rate was estimated from serum creatinine with the Modifi -cation of Diet in Renal Disease equation. c Baseline values and values obtained in the second study performed after 1 – 3 months of treatment with nadolol. d Only in one patient (of the compensated group) the fi nal value of HVPG was < 10 mm Hg. e Three patients of the compensated group and six of the ascites group did not receive nadolol because of side-effects. These nine patients received endo-scopic variceal ligation for primary prophylaxis of bleeding. f Three patients in the compensated group were lost to follow-up between at 31 and 60 months, and two patients in the ascites group were lost to follow-up at 41 and 47 months.

The American Journal of GASTROENTEROLOGY VOLUME 107 | MARCH 2012 www.amjgastro.com
424 LI
VE
R
Hern á ndez-Gea et al.
in HVPG and ascites development. Heterogeneous stages of cir-
rhosis, with diff erent prognosis, were included in these studies,
meaning patients with compensated and decompensated disease,
with previous history of ascites in many cases. Another impor-
tant limitation of these studies was the subjective defi nition used
for ascites development, even including worsening of preexisting
ascites. To deal with these limitations the current study specifi -
cally select an homogeneous group of patients with compensated
cirrhosis and without any previous decompensation, but at high
risk of decompensation indicated by the presence of HVPG
≥ 12 mm Hg and large varices, who were treated with nonselective
β -blockers for primary prophylaxis of bleeding. Our results pro-
vide additional evidence on the contribution of PHT to the pro-
gression of cirrhosis, showing that once clinically signifi cant PHT
is reached, it is still possible to reduce the probability of develop-
ing ascites by achieving a decrease in HVPG ≥ 10 % from baseline.
Otherwise ascites will develop in the majority of patients (up to
90 % ) without such a reduction in HVPG. In agreement with pre-
vious observations ( 9,10,15 ), the current study shows that hemo-
dynamic response also decreases the risk of refractory ascites and
hepatorenal syndrome. However, SLR analysis showed that only
ascites, and neither hepatorenal syndrome nor refractory ascites,
was independently associated with hemodynamic response. Th is
suggests that, in compensated cirrhosis, hemodynamic response
reduces the risk of complications related with ascites by decreas-
ing the probability of developing ascites.
Predictors of ascites development have not been clearly estab-
lished. Previous studies have shown that several parameters refl ect-
ing liver and circulatory dysfunction, such as bilirubin, MELD,
arterial hypotension, urinary sodium excretion, or plasma renin
activity, provide prognostic information on development of ascites
( 4,7,8,16 – 18 ). Th is is clinically sound because both, liver and cir-
culatory dysfunction, are involved in the development of ascites as
well as PHT ( 16 – 18 ). In keeping with this, the current study clearly
demonstrates that lack of hemodynamic response is a strong pre-
dictor of ascites. We also found that patients who developed ascites
had worse liver function, as indicated by a higher MELD score, and
had changes related to the circulatory dysfunction that accompanies
the progression of cirrhosis, such as a greater arterial vasodilatation
indicated by a lower systemic vascular resistance. However, clas-
sifi cation-and-regression-tree analysis showed that hemodynamic
nonresponse provides the strongest prognostic information on the
risk of developing ascites, whereas MELD score may be helpful to
identify patients at risk despite achieving a hemodynamic response.
Th e defi nition of response in this study diff ers from the tradi-
tional criteria of an HVPG decrease > 20 % . However, this criterion
was established in decompensated cirrhosis with previous variceal
bleeding and frequently also with ascites ( 19,20 ). In keeping with
our results, several studies have shown that in earlier stages of cir-
rhosis, with less severe PHT, a lower threshold reduction in HVPG
may be enough to prevent decompensation ( 4,21 ). In compensated
cirrhosis with moderate PHT (HVPG > 6 mm Hg) and absence of
varices, a 10 % threshold reduction in HVPG was independently
associated with a reduced risk of developing either varices or
variceal bleeding and also lower risk of cirrhotic decompensation
hepatorenal syndrome than in those who had not (70 % vs. 90 % at
3 years, P < 0.001) and in patients who had SBP vs. those who had
not (82 % vs. 89 % at 3 years, P = 0.03). Th e probability of survival
was also lower in patients who had a fi rst variceal bleeding than
in non-bleeders ( Figure 4 ), in patients who had encephalopathy
vs. those who had not (85 % vs. 90 % at 3 years, P = 0.004), and in
chronic hemodynamic nonresponders vs. responders ( Figure 4 ).
Among the diff erent causes of decompensation, development
of ascites (HR = 7.7, 95 % CI = 1.8 – 23.3; P < 0.01) and fi rst bleeding
(HR = 5.01, 95 % CI = 2.1 – 11.3; P < 0.01), but not encephalopathy,
were independent predictors of death by backward stepwise Cox
proportional hazards regression analysis. Among the complica-
tions of ascites, development of refractory ascites (HR = 4.1, 95 %
CI = 1.8 – 9.3; P < 0.01) was the only independent predictor of death,
whereas hepatorenal syndrome and SBP were not.
DISCUSION Th is study shows that in compensated cirrhosis with severe PHT
and large esophageal varices a reduction in HVPG > 10 % from
the baseline (considered hemodynamic response) lowers the risk
of decompensation. In addition to a reduced risk of fi rst variceal
bleeding, hemodynamic responders had lower probability of fi rst
ascitic decompensation. Complications of ascites, such as refrac-
tory ascites and hepatorenal syndrome, were also less frequent
in responders. Previous studies have shown that development of
ascites is mainly dependent on the progression of PHT ( 2 ). An
increase in HVPG above 10 mm Hg dramatically increases the
risk of transition from a compensated to a decompensated stage
( 4 ). However, beyond this threshold the contribution of changes
in HVPG to the risk of ascites has not been clearly established.
Previous studies focused on the prevention of variceal hemor-
rhage have shown that a reduction in HVPG to < 12 mm Hg or
≥ 20 % from baseline, in addition to lower risk of bleeding, is also
associated with a decreased risk of ascites ( 9,10 ). However, con-
troversial results have been reported ( 15 ). Th is may be due to
methodological diff erences among studies. None of them was
specifi cally designed to evaluate the relationship between changes
Overall83 cases,
49 (59%) developed ascitic decompensation
Hemodynamic responders40 cases
11 (27%) developed ascites
MELD score >107 cases
5 (71%) developed ascites
MELD score >1033 cases
6 (18%) developed ascites
Hemodynamic nonresponders38 cases
34 (89%) developed ascites
Figure 3 . Classifi cation-and-regression-tree (CART) analysis for develop-ment of ascites. CART analysis identifi ed hemodynamic nonresponse as the most effi cient fi rst splitting variable of risk of developing ascites. MELD score provides additional prognostic value in responders. In 5 of the 83 patients included, hemodynamic response could not be assessed because the second hemodynamic study was not performed (4 of them developed ascites).

© 2012 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
425
LIV
ER
Development of Ascites in Compensated Cirrhosis
( 3,4 ). In a recent study from our unit, this threshold reduction was
the best cutoff to predict fi rst bleeding in patients with large varices
under primary prophylaxis ( 21 ). In that study, we also observed
that hemodynamic responders had a lower risk of development or
worsening of ascites ( 21 ). However, more than 50 % of the patients
included had previous history of ascites precluding an appropriate
evaluation of the relationship between changes in HVPG and pro-
gression into decompensation.
Another relevant fi nding in this study was the prognostic value of
acute response to β -blockers on long-term risk of ascites. Although
the prognostic ability was inferior than that of chronic response, as
indicated by a lower area under ROC curve, the predictive value of
acute response, in a single hemodynamic study, on long-term risk of
decompensation was accurate as shown in previous studies ( 21,22 ).
Both endoscopic variceal ligation and β -blockers are currently rec-
ommended as fi rst-line option in primary prophylaxis of bleeding
( 23 ). Our fi ndings show that a single hemodynamic study with an
acute test is able to predict patients in whom β -blockers may pro-
vide relevant additional benefi t. Th is in turn suggests that restricting
EVL, a therapy with potential for severe side-eff ects, to acute non-
responders may improve the effi cacy of prophylactic treatment in
compensated cirrhosis, but requires further investigation.
In compensated cirrhosis mortality largely depends on the pro-
gression of liver disease to decompensation ( 1,2 ). Accordingly, in the
current study the majority of deaths occurred aft er either ascites or
bleeding and as expected we found that development of decompen-
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 26 48 60 72 84 96 108 120
Decompensted
Compensted1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 26 48 60 72 84 96 108 120
Non-ascitic
Ascitic
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 26 48 60 72 84 96 108 120
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 26 48 60 72 84 96 108 120
RespondersNon-bleeders
Bleeders
Pro
babi
lity
of s
urvi
val
Pro
babi
lity
of s
urvi
val
Pro
babi
lity
of s
urvi
val
Pro
babi
lity
of s
urvi
val
Non responders
a b
c d
Figure 4 . Probability of survival according to development of any fi rst decompensation ( a ), development of ascites ( b ), development of fi rst bleeding ( c ), and according to hemodynamic response ( d ). ( a ) The probability of survival was signifi cantly better in patients who remained compensated (continu-ous line) than in those who did not (dashed line) and developed a fi rst decompensation of portal hypertension (ascites, bleeding, or encephalopathy; P = 0.008). ( b ) Survival was worse in patients who developed ascites (dashed line) than in those who did not (continuous line; P = 0.006). ( c ) Survival was worse in patients with fi rst bleeding (dashed line) than in non-bleeders (continuous line; P = 0.01). ( d ) Survival was worse in hemodynamic nonresponders (dashed line) than in responders (continuous line; P = 0.04).
sation had a robust predictive value of mortality. Both development
of ascites and bleeding had independent predictive value of death.
In keeping with previous studies ( 5,9,10,19,20 ), we also found that
hemodynamic response was the strongest predictor of decompensa-
tion of cirrhosis, which will ultimately determine survival.
A possible limitation of this study is related to the population
investigated. We included patients in compensated phase of cir-
rhosis and in the stage with large esophageal varices. Whether the
results can be applied to patients without varices or with decom-
pensated cirrhosis remains to be determined. However, it has been
shown that an HVPG decrease ≥ 10 % is an independent predictor
of decompensation in compensated cirrhosis without varices and
with mild PHT (with HVPG ≥ 6 mm Hg) ( 4 ). In decompensated cir-
rhosis, it has been shown that an HVPG decrease ≥ 20 % may avoid
complications such as ascites ( 9,10 ). Whether a lesser decrease in
HVPG may be enough to prevent ascites in these patients remains
to be determinate. Another potential limitation is related to the fact
that the study was not blinded and this may have introduced a bias.
It is unlikely, however, as the hemodynamic response was not pre-
defi ned and all consecutive patients referred primary prevention of
bleeding were included and prospectively followed for development
of decompensation. Th e absence of a control group, without treat-
ment with β -blockers, does not allow to ascertaining whether other
cofactors may have induce an improvement of PHT or may have
account for development of ascites. However, it has been shown that
hemodynamic response, either induced by therapy or spontaneous,

The American Journal of GASTROENTEROLOGY VOLUME 107 | MARCH 2012 www.amjgastro.com
426 LI
VE
R
Hern á ndez-Gea et al.
WHAT IS NEW HERE 3 In compensated cirrhosis with severe portal hypertension
(indicated by the presence of large esophageal varices), when β -blockers achieve a reduction in HVPG > 10 % , the risk of progress to decompensation decreases signifi cantly.
3 In addition to a lower probability of fi rst variceal bleeding, hemodynamic responders (with an HVPG reduction > 10 % ) had a signifi cantly lower probability of developing ascites, refractory ascites, and hepatorenal syndrome.
3 Hemodynamic nonresponse provides the strongest prog-nostic information on the risk of develop ascites, whereas MELD score may be helpful to identify patients at risk despite achieving a hemodynamic response
3 The prognostic value of acute hemodynamic response to β -blockers on long-term risk of ascites was accurate, although it was inferior to that of chronic response.
REFERENCES 1 . D ’ Amico G , Garcia-Tsao G , Pagliaro L . Natural history and prognostic indi-
cators of survival in cirrhosis: a systematic review of 118 studies . J Hepatol 2006 ; 44 : 217 – 31 .
2 . Garcia-Tsao G , Friedman S , Iredale J et al. Now there are many (stages) where before there was one: In search of pathophysiological classifi cation of cirrhosis . Hepatology 2010 ; 51 : 1445 – 9 .
3 . Groszmann RJ , Garcia-Tsao G , Bosch J , et al. , for the Portal Hypertension Collaborative Group . Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis . N Engl J Med 2005 ; 353 : 2254 – 61 .
4 . Ripoll C , Groszmann R , Garcia-Tsao G et al. Hepatic venous pressure gardient predicts clinical descompensation in patients with compensated cirrhosis . Gastroenterology 2007 ; 133 : 481 – 8 .
5 . D ’ Amico G , Garcia-Pagan JC , Luca A et al. Hepatic vein pressure gradient reduction and prevention of variceal bleeding in cirrhosis: a systematic review . Gastroenterology 2006 ; 131 : 1611 – 24 .
6 . Gines P , Quintero E , Arroyo V et al. Compensated cirrhosis: natural history and prognostic factors . Hepatology 1987 ; 7 : 122 – 8 .
7 . Sangiovanni A , Prati GM , Fasani P et al. Th e natural history of compensat-ed cirrhosis due to hepatitis C virus: a 17-year cohort study of 214 patients . Hepatology 2006 ; 43 : 1303 – 10 .
8 . Sanyal AJ , Banas C , Sargeant C et al. Similarities and diff erences in outcomes of cirrhosis due to nonalcoholic steatohepatitis and hepatitis C . Hepatology 2006 ; 43 : 682 – 9 .
9 . Villanueva C , L ó pez-Balaguer JM , Aracil C et al. Maintenance of hemo-dynamic response to treatment for portal hypertension and infl uence on complications of cirrhosis . J Hepatol 2004 ; 40 : 757 – 65 .
10 . Abraldes JG , Tarantino I , Turnes J et al. Hemodynamic response to phar-macological treatment of portal hypertension and long-term prognosis of cirrhosis . Hepatology 2003 ; 37 : 902 – 8 .
11 . Beppu K , Inokuchi K , Koyanagi N et al. Prediction of variceal hemorrhage by esophageal endoscopy . Gastrointest Endosc 1981 ; 27 : 213 – 8 .
12 . Th e North Italian Endoscopic Club for the study and treatment of esophageal varices . Prediction of the fi rst variceal hemorrhage in patients with cirrhosis of the liver and esophageal varices . N Engl J Med 1988 ; 319 : 983 – 9 .
13 . Arroyo V , Gin è s P , Gerbes AL et al. Defi nition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis . Hepatology 1996 ; 23 : 164 – 76 .
14 . De Franchis R . Evolving consensus in portal hypertension. Report of the Baveno III consensus workshop on methodology of diagnosis and therapy in portal hypertension . J Hepatol 2005 ; 43 : 167 – 76 .
15 . Turnes J , Garcia-Pagan JC , Abraldes JG et al. Pharmacological reduction of portal pressure and long-term risk of fi rst variceal bleeding in patients with cirrhosis . Am J Gastroenterol 2006 ; 101 : 506 – 12 .
16 . Wong F , Liu P , Allidina Y et al. Pattern of sodium handling and its consequences in patients with preascitic cirrhosis . Gastroenterology 1995 ; 108 : 1820 – 7 .
17 . Wong F , Liu P , Blendis L . Sodium homeostasis in the chronic sodium load-ing in pre-ascitic cirrhosis . Gut 2001 ; 49 : 847 – 51 .
is an independent predictor of decompensation in compensated
cirrhosis without varices ( 4 ). Whether treatment of PHT, with
β -blockers or other drugs, can prevent the development of ascites as
suggested by our study should be confi rmed in future randomized
control trial.
In conclusion, the results of this study indicate that in patients with
compensated cirrhosis and severe PHT with large varices, achieving
an HVPG decrease > 10 % from baseline with β -blockers provides
a signifi cant reduction on the risk of fi rst ascitic decompensation.
Hemodynamic responders also have lower risk of other decompen-
sations related with ascites, such as refractory ascites and hepato-
renal syndrome, in addition to lower risk of variceal bleeding.
ACKNOWLEDGMENTS We thank the nursing and medical staff of the Gastrointestinal
Bleeding Unit and the Semi-Critical Unit of the Hospital de la Santa
Creu i Sant Pau for their cooperation in this study. We also thank
Mr X. Diez for his technical support in hemodynamic studies.
CONFLICT OF INTEREST Guarantor of the article: Candid Villanueva, MD.
Specifi c author contributions: All authors have contributed to
data interpretation and approved the fi nal version of the manuscript.
Virginia Hernández-Gea was responsible for study design, data
acquisition, draft ing of the manuscript, and data analysis. Carles
Aracil and Alan Colomo were responsible for study design,
manuscript revision, and data analysis. Isabel Graupera and Maria
Poca were responsible for data acquisition. Carlos Guarner, Josep
Miñana, and Xavier Torras were responsible for critical review of
the study design and manuscript revision. Candid Villanueva made
substantial contribution to the conception and design of the project,
interpretation of the data, manuscript draft ing, and overall supervi-
sion of the project.
Financial support: Th is study has been supported in part by a Grant
from the Fondo de Investigaciones Sanitarias (EC08 / 00087) and by
the Fundaci ó Investigaci ó Sant Pau (CAIBER).
Potential competing interests: None.
Study Highlights
WHAT IS CURRENT KNOWLEDGE 3 Ascites is the most frequent complication of cirrhosis and
is often the fi rst decompesation to appear. Predictors of ascites development are not known.
3 In compensated cirrhosis, the risk of developing ascites appears when the hepatic venous pressure gradient (HVPG) is 10 mmHg.
3 Once this threshold has been reached the relationship between changes in HVPG and development of decompen-sation has not been clarifi ed.
3 In patients with decompensated cirrhosis receiving drug therapy to prevent variceal rebleeding, a reduction of HVPG 20 % from baseline is associated with a signifi cant reduction of the risk of ascites. Whether changes in HVPG (induced by treatment) can prevent the transition of compensated cir-rhosis into development of ascites has not been established.

© 2012 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
427
LIV
ER
Development of Ascites in Compensated Cirrhosis
18 . Blendis L , Wong F . Th e natural history and management of hepatorenal disorders: from pre-ascites to hepatorenal syndrome . Clin Med 2003 ; 3 : 154 – 9 .
19 . Feu F , Garc í a-Pag á n JC , Bosch J et al. Relation between portal pressure response to pharmacotherapy and risk of recurrent variceal haemorrhage in patients with cirrhosis . Lancet 1995 ; 346 : 1056 – 9 .
20 . Villanueva C , Mi ñ ana J , Ortiz J et al. Endoscopic ligation compared with combined treatment with nadolol plus isosorbide mononitrate to prevent recurrent variceal bleeding . N Engl J Med 2001 ; 345 : 647 – 55 .
21 . Villanueva C , Aracil C , Colomo A et al. Acute hemodynamic response to beta-blockers and prediction of long-term outcome
in primary prophylaxis of variceal bleeding . Gastroenterology 2009 ; 137 : 119 – 28 .
22 . La Mura V , Abraldes JG , Raff a JC et al. Prognostic value of acute hemo-dynamic response to i.v. propranolol in patients with cirrhosis and portal hypertension . J Hepatol 2009 ; 51 : 279 – 87 .
23 . Garcia-Tsao G , Sanyal A , Grace ND , et al. , and the Practice Guidelines Committee of the American Association for the Study of Liver Diseases, the Practice Parameters Committee of the American College of Gastroenterology . Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis . Hepatology 2007 ; 46 : 922 – 38 .