Cyclovirobuxine D inhibits the currents of HERG potassium channels stably expressed in HEK293 cells
9
Molecular and Cellular Pharmacology Cyclovirobuxine D inhibits the currents of HERG potassium channels stably expressed in HEK293 cells Jing Zhao, Qiaoxu Wang, Jiang Xu, Jun Zhao, Gang Liu, Shuangqing Peng ⁎ Evaluation and Research Centre for Toxicology, Institute of Disease Control and Prevention, Academy of Military Medical Sciences, 20 Dongdajie Street, Fengtai District, Beijing 100071, PR China abstract article info Article history: Received 1 October 2010 Received in revised form 7 March 2011 Accepted 28 March 2011 Available online 12 April 2011 Keywords: Cyclovirobuxine D HEK293 cell HERG Patch clamp Arrhythmia QT prolongation Cyclovirobuxine D (CVB-D) has been widely used for treatment of cardiac insufficiency and arrhythmias in China. The antiarrhythmic and proarrhythmic potential of this drug might be concerned with prolongation of action potential duration and QT interval. Human-ether-a-go-go-related gene (HERG) has an important role in the repolarization of the cardiac action potential. This study investigated for the first time the effect of CVB-D on HERG channels stably expressed in HEK293 cells using the whole-cell patch-clamp technique. CVB-D inhibited HERG current (I HERG ) in a concentration-dependent manner with an IC 50 of 19.7 μM. I HERG blockade required channel activation and was time-dependent, suggesting an open channel block. Moreover, I HERG inhibition by CVB-D was relieved by depolarization to a highly positive membrane potential (+ 80 mV) that favored HERG channel inactivation. These findings suggested that CVB-D inhibit HERG channels in the open states. CVB-D had no effect on HERG current kinetics. Thus, we conclude that CVB-D inhibits HERG encoded potassium channels and this action might be a molecular mechanism for the previously reported APD prolongation and QT interval prolongation with this drug. © 2011 Elsevier B.V. All rights reserved. 1. Introduction Drug-induced prolongation of the electrocardiographic QT inter- val (LQT syndrome) has been associated with occurrence of severe ventricular arrhythmia, torsade de pointes (Haverkamp et al., 2000; Shah, 2004). The most common cause of QT prolongation by drug is the inhibition of the rapidly activating delayed rectifier potassium current (I Kr ), which has an important role in the repolarization of the cardiac action potential (Weirich and Antoni, 1998; Yap and Camm, 1999). The human ether-a-go-go-related gene (HERG or KCNH2) is now widely accepted as encoding the α-subunit of I Kr and the HERG product was found to be a functional K + channel with properties resembling those of I Kr (Sanguinetti et al., 1995; Trudeau et al., 1995). Many drugs are known to block HERG channels and cause acquired forms of QT prolongation, including Class III anti- arrhythmics, antihistamines, antibiotics, and antipsychotics (Witchel and Hancox, 2000; Vandenberg et al., 2001). Therefore, examination of the effects on HERG channels expressed in mammalian cell lines is widely used in the pharmaceutical industry for the assessment of proarrhythmic risk for new drugs (Zhou et al., 1998; Crumb and Cavero, 1999; Picard and Lacroix, 2003; Redfern et al., 2003). Indeed, HERG block is currently the best documented mechanism involved in QT prolongation (Recanatini et al., 2005), and the current regulatory guidelines (CPMP/986/96, 1997; ICH S7B, 2005) recommend the HERG test for identifying drugs with potential QT liabilities. Although drug-screening against recombinant HERG channels is now an important component of cardiac safety-pharmacology during drug development, there is little background data concerning about Chinese herbal medicines. Cyclovirobuxine D (CVB-D, see Fig. 1 for chemical structure), an active steroid alkaloid extracted from Chinese traditional plant Buxus microphylla (Dolejs et al., 1965), is widely used in China for treatment of cardiac insufficiency and arrhythmias (Chinese Pharmacopoeia Commission, 2005), but the exact mechanism of its therapeutic basis is not clear. In an experiment performed on anesthetized dog, CVB-D at low concen- trations could slow the heart rate and prolong QT interval of the electrocardiogram, whereas at higher concentrations CVB-D could induce arrhythmia (Fang et al., 2000). More recent work has sug- gested that one of the important mechanisms of anti-arrhythmia by CVB-D is to prolong action potential duration (APD) and the effective refractory period (ERP) of ventricular muscle. However, excessive prolongation of APD has also the effect of inducing arrhythmia when overdosed (Hu et al., 1981; Chen et al., 2004a). This raises the possibility that CVB-D may cause QT prolongation and cardiac arrhythmia by inhibiting I Kr or HERG channel. Therefore, we hypothesized that CVB-D is likely to act as an inhibiter of HERG current (I HERG ). The present study was conducted to test this hypothesis and to characterize the nature of any observed I HERG blockade. European Journal of Pharmacology 660 (2011) 259–267 ⁎ Corresponding author. Tel./fax: + 86 10 66948462. E-mail address: [email protected] (S. Peng). 0014-2999/$ – see front matter © 2011 Elsevier B.V. All rights reserved. doi:10.1016/j.ejphar.2011.03.039 Contents lists available at ScienceDirect European Journal of Pharmacology journal homepage: www.elsevier.com/locate/ejphar
Transcript of Cyclovirobuxine D inhibits the currents of HERG potassium channels stably expressed in HEK293 cells

European Journal of Pharmacology 660 (2011) 259–267
Contents lists available at ScienceDirect
European Journal of Pharmacology
j ourna l homepage: www.e lsev ie r.com/ locate /e jphar
Molecular and Cellular Pharmacology
Cyclovirobuxine D inhibits the currents of HERG potassium channels stablyexpressed in HEK293 cells
Jing Zhao, Qiaoxu Wang, Jiang Xu, Jun Zhao, Gang Liu, Shuangqing Peng ⁎Evaluation and Research Centre for Toxicology, Institute of Disease Control and Prevention, Academy of Military Medical Sciences, 20 Dongdajie Street, Fengtai District,Beijing 100071, PR China
⁎ Corresponding author. Tel./fax: +86 10 66948462.E-mail address: [email protected] (S. Peng).
0014-2999/$ – see front matter © 2011 Elsevier B.V. Aldoi:10.1016/j.ejphar.2011.03.039
a b s t r a c t
a r t i c l e i n f oArticle history:Received 1 October 2010Received in revised form 7 March 2011Accepted 28 March 2011Available online 12 April 2011
Keywords:Cyclovirobuxine DHEK293 cellHERGPatch clampArrhythmiaQT prolongation
Cyclovirobuxine D (CVB-D) has been widely used for treatment of cardiac insufficiency and arrhythmias inChina. The antiarrhythmic and proarrhythmic potential of this drug might be concerned with prolongation ofaction potential duration and QT interval. Human-ether-a-go-go-related gene (HERG) has an importantrole in the repolarization of the cardiac action potential. This study investigated for the first time the effectof CVB-D on HERG channels stably expressed in HEK293 cells using the whole-cell patch-clamp technique.CVB-D inhibited HERG current (IHERG) in a concentration-dependent manner with an IC50 of 19.7 μM. IHERGblockade required channel activation and was time-dependent, suggesting an open channel block. Moreover,IHERG inhibition by CVB-D was relieved by depolarization to a highly positive membrane potential (+80 mV)that favored HERG channel inactivation. These findings suggested that CVB-D inhibit HERG channels in theopen states. CVB-D had no effect on HERG current kinetics. Thus, we conclude that CVB-D inhibits HERGencoded potassium channels and this actionmight be amolecularmechanism for the previously reported APDprolongation and QT interval prolongation with this drug.
l rights reserved.
© 2011 Elsevier B.V. All rights reserved.
1. Introduction
Drug-induced prolongation of the electrocardiographic QT inter-val (LQT syndrome) has been associated with occurrence of severeventricular arrhythmia, torsade de pointes (Haverkamp et al., 2000;Shah, 2004). The most common cause of QT prolongation by drug isthe inhibition of the rapidly activating delayed rectifier potassiumcurrent (IKr), which has an important role in the repolarization ofthe cardiac action potential (Weirich and Antoni, 1998; Yap andCamm, 1999). The human ether-a-go-go-related gene (HERG orKCNH2) is now widely accepted as encoding the α-subunit of IKr andthe HERG product was found to be a functional K+ channel withproperties resembling those of IKr (Sanguinetti et al., 1995; Trudeauet al., 1995). Many drugs are known to block HERG channels andcause acquired forms of QT prolongation, including Class III anti-arrhythmics, antihistamines, antibiotics, and antipsychotics (Witcheland Hancox, 2000; Vandenberg et al., 2001). Therefore, examinationof the effects on HERG channels expressed in mammalian cell linesis widely used in the pharmaceutical industry for the assessmentof proarrhythmic risk for new drugs (Zhou et al., 1998; Crumband Cavero, 1999; Picard and Lacroix, 2003; Redfern et al., 2003).Indeed, HERG block is currently the best documented mechanisminvolved in QT prolongation (Recanatini et al., 2005), and the
current regulatory guidelines (CPMP/986/96, 1997; ICH S7B, 2005)recommend the HERG test for identifying drugs with potential QTliabilities.
Although drug-screening against recombinant HERG channelsis now an important component of cardiac safety-pharmacologyduring drug development, there is little background data concerningabout Chinese herbal medicines. Cyclovirobuxine D (CVB-D, seeFig. 1 for chemical structure), an active steroid alkaloid extractedfrom Chinese traditional plant Buxus microphylla (Dolejs et al., 1965),is widely used in China for treatment of cardiac insufficiency andarrhythmias (Chinese Pharmacopoeia Commission, 2005), but theexact mechanism of its therapeutic basis is not clear. In anexperiment performed on anesthetized dog, CVB-D at low concen-trations could slow the heart rate and prolong QT interval of theelectrocardiogram, whereas at higher concentrations CVB-D couldinduce arrhythmia (Fang et al., 2000). More recent work has sug-gested that one of the important mechanisms of anti-arrhythmia byCVB-D is to prolong action potential duration (APD) and the effectiverefractory period (ERP) of ventricular muscle. However, excessiveprolongation of APD has also the effect of inducing arrhythmiawhen overdosed (Hu et al., 1981; Chen et al., 2004a). This raises thepossibility that CVB-D may cause QT prolongation and cardiacarrhythmia by inhibiting IKr or HERG channel. Therefore, wehypothesized that CVB-D is likely to act as an inhibiter of HERGcurrent (IHERG). The present study was conducted to test thishypothesis and to characterize the nature of any observed IHERGblockade.

Fig. 1. Chemical structure and chemical formula of cyclovirobuxine D.
260 J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
2. Materials and methods
2.1. Cell line maintenance
Experiments were performed on a HEK293 cell line that stablyexpressing HERG gene (purchased from Avian Company, Canada). Cellswere continuously maintained and passaged using the Dulbecco'sModified Eagle Medium (DMEM, Gibco) supplemented with 10% (v/v)fetal bovine serum (FBS, Hyclone), 100 U/ml penicillin, 100 U/mlstreptomycin, and 2 mmol/l L-glutaminate at 37 °C in an incubatorwith 5% CO2 and 95% atmospheric air.
2.2. Solutions and drugs
The composition of the bath solution was (in mM): NaCl 136; KCl5.4; MgCl2 1.0; CaCl2 1.0; HEPES 10; and glucose 10; pH adjustedto 7.35 with NaOH. The pipette solution contained (in mM): KCl 130;MgCl2 1.0; EGTA 10; HEPES 10; and MgATP 5; pH adjusted to 7.3 withKOH.
Cyclovirobuxine D (purity is 99%) was purchased from NanjingZelang Medical Technology Co. Ltd (Nanjing, China). It was dissolvedto 50 mM in ethanol and stored at −20 °C and was diluted to thefinal concentration immediately before the experiment. The maxi-mum concentration of ethanol used was never in excess of 0.2%by volume. As reported by Paul et al. (2002), we also found that thisconcentration has no effect on IHERG. E-4031 (purchased from SigmaAldrich) was used as a positive control.
2.3. Electrophysiological recordings
Currents were recorded at room temperature (20–22 °C), usingthe whole-cell patch-clamp technique. Patch-pipettes were pulled(Narishige PC10) and fire-polished to 2–5 MΩ (Narishige MF830).Recordings of membrane currents were made using a Multiclamp700B amplifier (Axon Instruments) and a CV-70 headstage, sampledat 10 kHz and filtered at 2 kHz. Voltage-clamp commands weregenerated using Clampex 10.2 (Axon Instruments). Data wererecorded via a Digidata 1440A interface (Axon Instruments). Pipetteand cell capacitance were compensated in all experiments. Between60% and 80% of the series resistance was also compensated.Extracellular media were exchanged using a gravity-fed bathperfusion system (BPS-8, ALA Scientific Instruments), and the flowrate was 8×10−3 ml/s. The distance of the flow pipette from the cellremained approximately 150 μm and the pipette tip diameter was300 μm.
2.4. Data analysis and presentation
Data were analyzed using Clampfit 10.2 (Axon Instruments), Excel2000 and Origin 8 (MicroCal) software. Data are presented as mean±standard error of the mean (S.E.M.). Statistical comparisons weremade using paired Student's t-tests or one-way analysis of variance(ANOVA). P values of less than 0.05 were taken as statistically
significant. Quantitative fits to data were made using the equationslisted below.
The IC50 value was estimated from best-fit results with sigmoidalconcentration–response function:
I = Imax–Iminð Þ.
1 + 10X− log IC50� �
+ Imin
where I denotes normalized current; Imax, maximal current, Imin,minimal current; X, concentration of test compound in log scale; andIC50, concentration at 50% of maximal inhibition.
Voltage-dependent activation curves for IHERG were fit with theBoltzmann function:
Activation parameter = 1= 1+ exp V0:5–Vmð Þ=k½ �ð Þ
where Activation parameter denotes the fraction of channels activatedat any test potential Vm, and V0.5 and k denote the half-maximalactivation voltage and slope factor, respectively.
The inactivation curves were fit with the following Boltzmannfunction:
Inactivation parameter = 1– 1= 1+ exp V0:5–Vmð Þ= k½ �ð Þ½ �
where Inactivation parameter denotes the fraction of channelsavailable for activation at any test potential Vm, and V0.5 and k denotethe half-maximal inactivation voltage and slope factor, respectively.
3. Results
3.1. Concentration dependence of IHERG inhibition by CVB-D
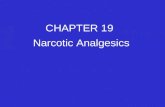
E-4031, a methanesulfonanilide drug, is thought in cardiac cells toblock IKr with high selectivity. The sensitivity of our transfected HERGchannels to the E-4031 was studied firstly. IHERG was elicited byrepetitive (every 10 s) application of a 2-s step depolarization froma holding potential of −80 mV to +20 mV followed by a 2-srepolarization to −50 mV. Upon depolarization, the activation gateopens (activation), and the inactivation gate closes (inactivation). Bycontrast, upon repolarization, the activation gate closes (deactiva-tion), and the inactivation gate opens (recovery from inactivation).Currents were measured at a steady-state firstly in normal bath andthen in the presence of drug for 10 min. E-4031 (1 μM) inhibited IHERGrapidly as drug block developed and the HERG tail current wascompletely blocked (Fig. 2A). Peak IHERG tail amplitudes were used toquantify the degree of IHERG inhibition. Fig. 2B shows the concentra-tion dependence of IHERG inhibition by E-4031, and the dose–responsecurve for E-4031 block showed an IC50 of 0.042 μM. Treatment with30 μM CVB-D produced a progressive inhibition of IHERG over 8 min ofdrug application (Fig. 2C). Fig. 2E shows a recording of IHERG in control,5 min after the addition of 20 μM CVB-D and 3 min following wash-out of the drug, the blocking effects were reversed gradually fol-lowing washout. The time-course of the effect on IHERG of differentconcentrations of CVB-D (1, 10, 30 and 100 μM) is shown in Fig. 2D.CVB-D treatment caused an apparent concentration-dependentreduction in the magnitude of IHERG. Depending upon the concentra-tion of CVB-D, the development of IHERG block appeared to occurrapidly in the first 200 s after beginning treatment. Lower concentra-tion of CVB-D (1 and 10 μM) caused amore gradual decline in current.The blockade reached a nearly steady-state level within 5 to 6 min.Fig. 2F depicts the inhibition of peak IHERG tail current by variousconcentrations of CVB-D after a 5-min exposure. Fractional blockin the presence of 1, 10, 30, and 100 μM CVB-D was 12.3±4.7%(PN0.05), 21.7±16.1% (Pb0.01), 57.7±7.5% (Pb0.01) and 71.2±5.1% (Pb0.01), respectively. The concentration–response relationshipwas determined and the estimated IC50 was 19.7 μM (Fig. 2G).

Fig. 2. Concentration-dependent inhibition of IHERG. (A) Representative traces of IHERG in control and after 30, 60, 90 and 200 s of exposure to 1 μME-4031 indicating that the currentis E-4031 sensitive. IHERG was elicited by the voltage protocol shown in the inset. (B) Concentration–response relationship for peak tail current by E-4031. (C) Representative traces ofIHERG in control and after 30, 90, 240 and 480 s of exposure to 30 μM CVB-D. (E) Representative currents in the absence, presence (5 min) and following wash off (3 min) of 20 μMCVB-D. (D) Time course of reduction of IHERG by different concentrations of CVB-D (1, 10, 30 and 100 μM). (F) Mean (±S.E.M.) fractional block calculated after a 5-min exposure todifferent concentrations of CVB-D (n=3–6 cells per concentration; **Pb0.01 vs. control). (G) Concentration–response curve of IHERG by CVB-D. The curve was constructed by plottingpeak tail currents relative to pretreatment control levels against the concentrations of the blockers (n=3–6 cells per concentration).
261J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
3.2. Current–voltage relationship for IHERG and blockade by CVB-D
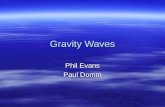
The effects of drug on IHERG were further investigated by applyingvoltage-command from a holding membrane potential of −80 mV toa range of test-potentials (from −50 mV to +60 mV in 10 mV steps,to activate outward step current), and each test pulse was followedby a repolarization step to −50 mV (to record tail current). Repre-sentative current traces are shown before and during exposureto E-4031 (Fig. 3A) and CVB-D (Fig. 3D). Under control conditions,the depolarizing steps activated outward step currents, reaching amaximum value at about 0–10 mV. Depolarizing steps to even greaterpositive values caused a current decrease progressively. Fig. 3B andE shows the current–voltage (I–V) relationships of IHERG at theend of the depolarizing steps (step current) in the absence and inthe presence of 1 μM E-4031/20 μM CVB-D. The I–V relationshipsexhibited the characteristic bell-shape that increased from −40 mVto +10 mV and decreased with further depolarization because offast C-type inactivation (Smith et al., 1996). After the depolarizingsteps, repolarization to −50 mV induced tail currents, which had an
amplitude even larger than that of step currents during depolariza-tion. This is a characteristic property of IHERG, and is due to a rapidrecovery from inactivation and a slow deactivation mechanism(Sanguinetti et al., 1995). The tail currents increased with voltageand then plateaued at test potential positive to +10 mV. E-4031(1 μM) inhibited tail currents completely at all test potentials(Fig. 3C). At more positive test potentials, 20 μM CVB-D exerted acomparatively larger effect on IHERG than it did at more negativepotentials. The I–V relations for IHERG tails showed little divergencebetween control and CVB-D at more negative potentials, withincreased divergence apparent at −10 mV and at potentials morepositive to this (Fig. 3F).
The IHERG blockade by CVB-D was assessed with other twodifferent voltage protocols: the fully activated I–V protocol and theinstantaneous I–V protocol. A depolarizing pulse to +60 mV, whichinduced a full activation and to inactivate HERG channels, wasfollowed by various levels of test pulses between −100 and +50 mV(Fig. 4A). The prepulse potential at +60 mV was positive enough toinduce full conductance of the HERG channels but also rendered a

Fig. 3. Current–voltage relationship for IHERG and blockade by CVB-D. (A and D) Representative traces of IHERG under control conditions and after application of 1 μM E-4031/20 μMCVB-D. Currents were recorded by applying depolarizing test pulses from a holding potential of−80 mV to various potentials between−50 mV and+60 mV in 10-mV incrementsfor 2-s, followed by a repolarization step to −50 mV for 2-s. (B and C) I–V relationships for step currents measured at the end of depolarizing step and peak tail currents by 1 μME-4031. (E and F) Normalized I–V relationships for step currents and peak tail currents before and after 20 μM CVB-D (n=5; *Pb0.05 vs. control).
262 J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
large number of channels in the inactivated state. The normalized datawere averaged and plotted against the test potential. The fullyactivated I–V relationship showed a typical inward rectification ofthe HERG channel due to the rapid inactivation. CVB-D reduced thecurrent at some potentials between −30 and +20 mV (Fig. 4B). Thereversal potential was not changed, indicating that CVB-D did notaffect the ion-selectivity of HERG channels. To evaluate the IHERGblockade under conditions by which HERG channel rectification wasremoved, the instantaneous I–V protocol shown in Fig. 4C was used.A 2-s depolarizing pulse to +40 mV to inactivate the HERG channels,followed by a prepulse to −80 mV for 10 ms. This prepulse wassufficiently long to allow rapid recovery of channels from inactivationbut short enough to prevent significant channel deactivation.Following the recovery prepulse, a series of test pulses was deliveredto potentials ranging from −120 mV to +20 mV. CVB-D reduced thecurrent with increasing test potentials, and the proportion of theblockade did not change significantly between −50 and +20 mV(Fig. 4D).
3.3. Time dependence of IHERG inhibition by CVB-D
In order to study the time-dependent development of IHERGinhibition on membrane depolarization, two experimental pro-tocols were used. In the first, a sustained (10-s) depolarizing stepto +10 mV from−80 mV was applied in the absence of drug to elicitcontrol IHERG. It was then discontinued whilst cells were equilibratedin 20 μMCVB-D for 5 min, after which it was re-applied. Fig. 5A showsthe representative traces in the absence and presence of CVB-D, thesetraces diverged rapidly following depolarization. The fractional blockwas calculated at different time-points throughout the protocol andthe mean fractional block data were plotted against time (Fig. 5B).
Inhibition developed progressively with time on depolarization,with no significant increase in blockade after ~1500 ms. Fig. 5Cshows an enlargement of the first 1500 ms of the mean fractionblock, and indicates that the blockade did show time-dependence,with blockade developing over the first 400–500 ms of the pulse(Pb0.001).
We also used a second protocol to assess accurately the time-course of development of inhibition over short periods followingdepolarization. The IHERG was activated by an ‘envelope of tails’protocol (Du et al., 2006), in which the amplitude of IHERG tailsfollowing test potentials of increasing duration (30 to 600 ms) ismeasured (Fig. 6A). IHERG tail amplitude increased with pulse durationover the first few pulses, and then reached a steady maximalamplitude. The time courses of current activation were demonstratedby two sets of plots in Fig. 6B. Data were also analyzed by plottingfractional block of IHERG tail against each of the different duration test-pulses (Fig. 6C), and the plot shows that IHERG blockade by CVB-Dwith brief depolarizations was less than that with longer durationpulses, which indicates the blockade varied significantly with testpulse duration (Pb0.05). Considered collectively, the data in Figs. 5and 6 indicate that inhibition of IHERG by CVB-D was strongly time-dependent and was contingent upon channel gating.
3.4. Relief of IHERG inhibition by strong membrane depolarization
The time dependence of IHERG blockade by CVB-D shown in Figs. 5and 6 is consistent with an open channel blocking mechanism, but itcan be difficult to distinguish between open- and inactivated-stateblockade (When the membrane is at depolarized potentials, much ofthe HERG channel population is in an inactivated state). Therefore, weemployed an additional protocol. This comprised a sustained (10-s)

Fig. 4. Current–voltage relationship for IHERG determined with the fully activated I–V protocol (A) and the instantaneous I–V protocol (C). (A) In the fully activated I–V protocol,currents were obtained by depolarization to+60 mV for 2-s to reach a steady-state level before repolarization to potentials from−100 mV to+50 mV. (B) The peak currents beforeand after CVB-D during repolarization steps were plotted as a function of voltage (n=5; *Pb0.05 vs. control). (C)With the instantaneous I–V protocol, currents were recorded after a2-s depolarization to +40 mV, followed by a 10-ms repolarizing step to−80 mV to reverse the rapid inactivation and then a 400-ms depolarization to potentials ranging−120 and+20 mV. (D) Normalized I–V relationships for instantaneous currents before and after 20 μM CVB-D (n=6; *Pb0.05 vs. control).
263J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
depolarization from −80 mV to +10 mV, by incorporating a 4-s stepto +80 mV (Fig. 7A). The protocol was applied in control solution,was discontinued while the cell was exposed to 20 μM CVB-D for5 min, and was then reapplied in the presence of drug. In controlsolution, IHERG amplitude decreased markedly during the period of+80 mV, reflecting the fact that the transition of HERG channels fromactivated state into the inactivated state. In the presence of CVB-D,
Fig. 5. Time-dependent inhibition of IHERG during a sustained depolarization. (A) Representatthe first trace elicited after a 5-min exposure to 20 μM CVB-D. (B) Fractional block of IHERG ploblock over the first 1500 ms of the protocol, time-dependence of inhibition was observed d
IHERG at +10 mV was inhibited to a greater extent than at +80 mV.Mean fractional block data are plotted before (2000 ms), during(5000 ms) and after (9000 ms) the step to+80 mV (Fig. 7B). It showsthat blockade during +80 mV step (5000 ms) was significantlydecreased compared to that at +10 mV before (2000 ms) this step(Pb0.05). These data suggest that CVB-D primarily binds to the open/activated channel state.
ive currents elicited by a 10-s depolarizing step to+10 mV, in the absence (control) andtted against time following onset of depolarization. (C) Plots of mean level of fractionaluring the first ~500 ms of the pulse (n=6).

Fig. 6. Time-dependent inhibition of IHERG by an envelope voltage protocol. (A) Representative currents elicited by a depolarization to +20 mV with duration of 30 to 600 ms in30 ms increments, followed by a repolarization to −50 mV, IHERG tail amplitude reflected the extent of IHERG activation produced during the pulse to +20 mV. (B) Time-course ofcurrent activation. Peak tail currents relative to control maximum tail current were plotted for control and after 20 μM CVB-D. (C) Fractional block of IHERG following pulses ofdifferent duration (n=6).
264 J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
3.5. Effects on kinetics of IHERG by CVB-D
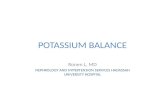
Drugs that block ion channels often alter kinetics of channel gating.The effects of CVB-D on activation, onset of inactivation, recovery frominactivation and steady-state inactivation of IHERG were examined.
The activation curves were constructed by plotting the normalizedIHERG tail currents against corresponding depolarization voltages(Fig. 8A). The mean half-maximal activation voltage (V1/2) was−26.08±0.7 mV in the control and −24.98±1.0 mV in CVB-D(PN0.05); the corresponding κ was 10.01±0.5 and 8.95±0.9,respectively (PN0.05), with the IHERG activation relations in controland CVB-D closely overlying one another (Fig. 8B).
The voltage dependence of IHERG steady-state inactivation wasassessed using a 3-step protocol (Fig. 8C). A 2-s duration pulse from
Fig. 7. Relief of blockade by strong membrane depolarization. (A) Representativecurrents in response to a modified long-pulse protocol with an additional 4-s step to+80 mV. Arrows indicate traces obtained in control and 20 μM CVB-D. (B) Fractionalblock of IHERG measured at +10 mV (2000 ms), at +80 mV (5000 ms) and at +10 mVagain (9000 ms). P values shown indicate the significant reduction in IHERG block levelproduced by the strong depolarization to +80 mV compared to that at +10 mV, butafter membrane potential was returned to +10 mV, there was no significant increase(n=5).
−80 mV to +40 mV was followed by a brief (10 ms) step to a rangeof potentials between −120 mV and +20 mV to relieve IHERG inac-tivation to differing extents. Membrane potential was then steppedback to +40 mV and the magnitude of the resulting current reflectedthe population of channels available for activation. In Fig. 8D, thecurrents during the third step (to +40 mV) were normalized andplotted against the test pulse, giving the steady-state inactivationcurve. In control and CVB-D, the inactivation V1/2 was −69.64±2.9 mV and −57.89±1.5 mV (PN0.05), with corresponding κ of26.17±2.8 and 17.23±1.4 (PN0.05). Thus, CVB-D did not alter thevoltage-dependence of IHERG inactivation.
To examine whether CVB-D would affect the onset of inactivation,IHERG was fully activated and inactivated by a depolarizing to +40 mVfor 2-s, then repolarized to −100 mV for 10 ms to allow channelrecovery from inactivation but not enough for channel deactivation, atest step was then applied to observe inactivation time constant(Fig. 8E). The inactivation time constant was measured by fitting asingle exponential function to the decaying current trace. The onsetof inactivation was accelerated at −30 and −20 mV, but there wereno significant differences between control and drug application inwide range of voltages (Fig. 8F). CVB-D has little effect on the rates ofinactivation.
The recovery time from inactivation of IHERG was examined usingthe dual-pulse protocol (Fig. 8G). The cells were depolarized to 60 mVfor 2-s to inactivate HERG channels and then repolarized to potentialsbetween −100 and −20 mV. The rising phase of the currentrepresents the rapid recovery of HERG channels from inactivated toopen states and was fitted to a mono-exponential function, and therecovery time constant was plotted against the test potentials(Fig. 8H). There was no significant difference before and after 20 μMCVB-D application.
4. Discussion
4.1. Characteristics of IHERG blockade by CVB-D
This report is the first to detail the effects of the CVB-D on voltage-dependent HERG channels cloned from the human heart. The majoradvantage of heterologous HERG expression in the electrophysiolog-ical assays is the lack of overlapping and potentially contaminatingcurrents in the recordings from native cardiomyocytes. Potassiumefflux through HERG is a major determinant of repolarization andaction potential duration (APD) in ventricular cardiomyocytes.Blockade of IHERG lengthens APD and leads to QT interval prolongation.Previous studies have shown that CVB-D produced protective effectsagainst atrial fibrillation induced by CaCl2-Ach in mice (Wang et al.,1996). On atrial fibrillation induced by aconitine, ouabain or adrenaline

Fig. 8. Effects of CVB-D on HERG channel gating kinetics. (A) Representative traces of IHERG activation. Voltage protocol was the same as used in Fig. 3A. (B) Normalized peak tailcurrent amplitudes before and after application of drug (n=7). Smooth curves are best fits of the data to a Boltzmann function (see Materials and methods). (C) Representativecurrent tracing for steady-state inactivation. Following a 2-s step to +40 mV, 10-ms pulses were applied to potentials between −120 mV and +20 mV, followed by a stepto +40 mV. (D) Normalized steady-state inactivation curves under control and 20 μM CVB-D (n=7). The data were fitted with a Boltzmann function (see Materials and methods).(E) Representative current tracing for IHERG onset of inactivation by the protocol in Fig. 4C. (F) The time constants for the onset of inactivation are plotted against the membranepotential (n=5; *Pb0.05 vs. control). (G) Representative current tracing for IHERG recovery from inactivation by the protocol in Fig. 4A. (H) The time constants for the recovery frominactivation are plotted against the membrane potential (n=5).
265J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
in isolated guinea pig atria, the effects of CVB-Dwere similar to those ofamiodarone (Wang et al., 1996; Zhang et al., 2001). Moreover, theincrease of QT interval in anesthetized dogs receiving CVB-D suggestedthe involvement of K+ channel blockade (Chen et al., 2004a). Based onthese results of animal studies, we had examined the effect of CVB-Don HERG channels using a whole-cell patch-clamp technique. Wefound that CVB-D inhibited IHERG in a concentration-dependentmanner with an IC50 of 19.7 μM, indicating that CVB-D has thepotential to induce APD prolongation, which is probably one ofthe pro-arrhythmic mechanisms of CVB-D in overdose. Indeed, CVB-Dhas been reported to block a variety of other ion channels, includingtransient outward potassium current (Ito), inwardly rectifying potas-sium channel (IK1; Chen et al., 2003) and L-type calcium current (ICa-L;Chen et al., 2003, 2004b). Hu et al. showed that CVB-D opened the KATP
channel to inhibit the Ca2+ influx to protect cardiomyocytes (Huet al., 2007). Moreover, it has been found that CVB-D affectsintracellular Ca2+ homeostasis by both promoting a discharge ofintracellular pools and by interfering with the operation of store-dependent channels (Na+/Ca2+ channels) via plasma membranedepolarization (Grossini et al., 2005). As we known, these cardiac ionchannels are responsible for the onset and maintaining of the cardiacaction potential, interactions of nonselective HERG channel blockerswith other cardiac ion channels may mitigate or exacerbate theprolongation of APD (Martin et al., 2004). Therefore, it is possible thatCVB-D possesses a multiple mode of action. To understand themechanisms underlying electrophysiological changes by CVB-D inthe action potential and ECG, it is important to determine the effects ofthis drug on ion channels other than HERG.

266 J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
The results of this study provide insight into the nature of IHERGblockade by CVB-D. The depressant effect of CVB-D on HERG waspartially reversible by washing with drug free solution, and this isconsistent with APD recovery seen in ventricular muscle after wash-out of the drug. Blockade of IHERG required channel activation, andthe blockade developed after channels opened (Figs. 3 and 4). Thedata obtained using the envelope voltage protocol indicate that theblockade increased over ~300 ms, and the extent of current activationsignificantly influenced the blocking effect, which indicates thatchannel opening is required for the blockade of IHERG by CVB-D. Also,during a sustained depolarization, the level of blockade developedrapidly over the first 400–500 ms, and it is similar to those reportedfluvoxamine, citalopram and doxepin (Duncan et al., 2007; Witchelet al., 2002; Milnes et al., 2003), but differ significantly from themethanesulfonanilides, for which little blockade is observed initially,with progressive development of blockade during seconds of themaintained depolarization (Snyders and Chaudhary, 1996). Giventhe unusual gating kinetics of the HERG channel (open, inactiveand closed), these features suggested that CVB-D bind to the open orinactivated channel state. In order to distinguish between open andinactivated channel blocking mechanisms, we found that depolariza-tion to +80 mV further reduced fractional block (Fig. 7), and thesedata suggest that CVB-D has a higher binding affinity for the openstate than for the inactivate state. Normalized I–V relationshipsfor instantaneous currents before and after 20 μM CVB-D also suggestthat CVB-D binds to HERG channels that are in the open state.These characteristics are similar to those of other open-channelblockers, including cisapride, vesnarinone, mesoridazine and amba-silide (Rampe et al., 1997; Kamiya et al., 2001; Su et al., 2004; Walkeret al., 2000). These drugs require channel opening to bind to siteswithin the inner cavity of the channel. Thus, drugs only get access totheir receptor site when the channel opens (Carmeliet, 1993; Kamiyaet al., 2008). Finally, CVB-D did not change other channel kinetics(activation, onset of inactivation, recovery from inactivation,and steady-state inactivation), which indicates that the drug blocksHERG channels without changing either activation or inactivationproperty (Fig. 8).
4.2. Clinical implications
In clinical practice, for the treatment of arrhythmias, anginapectoris and cardiac insufficiency, the usual daily dosage of CVB-Dis very low (2–6 mg), and the IC50 (19.7 μM) was higher than thetherapeutic concentration in healthy volunteers (Cmax: 0.013±0.003 μM/6 mg i.v.; He et al., 2008). Thus, CVB-D might have a lesspowerful effect on QT interval prolongation within its therapeuticdose range. But in patients with several risk factors included structuralheart disease (myocardial infarction, heart failure, valvular disease, orcardiomyopathy), hypokalemia, or in patients concurrently receivingother QT interval prolonging drugs, the inhibition of IHERG by CVB-D isof greater concern. Hepatic impairment, bradycardia, and atrioven-tricular block also increase the risk of TdP (Yap and Camm, 2003).
More recently, it has been found that some herbal products (e.g.sophocarpine, sophoridine, matrine, oxymatrine, resveratrol, acehy-tisine hydrochloride) in clinics for treating cardiovascular diseasescould inhibit IHERG recorded from HEK293 cells (Zhao et al., 2009;Zhang et al., 2007; Zhao et al., 2007; Huang et al., 2009). Aconitine (atraditional Chinese herb which is documented to have potentcardiotoxicity), berberine and rhynchophylline have been found toblock IHERG expressed on Xenopus laevis oocytes (Li et al., 2010; Li et al.,2001; Gui et al., 2005). HERG channel may be one of the key targetsites explaining both the therapeutic effects and the potentialcardiotoxicity with these herbs. In patients taking herbal supple-ments, ephedra, bitter orange and licorice have been reported tocause QT interval prolongation and cardiac arrhythmias (Haller andBenowitz, 2000; Theoharides, 1997; Jordan et al., 2004; Firenzuoli
et al., 2005; Bocker and Breithardt, 1991; Eriksson et al., 1999), but themechanism is not clear. There is a need for increased consideration inherb safety testing.
4.3. Conclusion
In conclusion, the present results demonstrate that CVB-D is a low-affinity inhibitor of HERG. Its electrophysiological features indicatethat CVB-D is consistent with an open channel state blocker. HERGinhibition could be a molecular mechanism of CVB-D inducing APDprolongation and QT interval prolongation.
Disclosure/conflict of interest
The authors state no conflict of interest.
Acknowledgment
This project was supported by the National Key Project on DrugDevelopment from the Ministry of Science and Technology of China(2009ZX09501-034).
References
Bocker, D., Breithardt, G., 1991. Induction of arrhythmia by licorice abuse. Z. Kardiol. 80,389–391.
Carmeliet, E., 1993. Use-dependent block and use-dependent unblock of the delayedrectifier K+ current by almokalant in rabbit ventricular myocytes. Circ. Res. 73,857–868.
Chen, Z.Q., Hu, S.J., Shi, W.Y., Du, J., Shen, Y., Xia, Q., 2004a. Electrophysiologic study ofthe biphasic effects of cyclovirobuxine D on arrhythmias. Zhongguo Zhong Xi Yi JieHe Za Zhi 24, 1010–1013.
Chen, Q.W., Shan, H.L., Wang, H., Li, Z., Yang, B.F., 2003. Mechanisms of cyclovirobuxineD on APD prolongation in rat ventricular myocytes. J. Chin. Pharmaceu. Sci. 12,142–147.
Chen, Q.W., Shan, H.L., Sun, H.L., Wang, H., Yang, B.F., 2004b. Effects of cyclovirobuxineD on intracellular Ca2+ and L-type Ca2+ current in rat ventricular cardiomyocytes.Yao Xue Xue Bao 39, 500–503.
Chinese Pharmacopoeia Commission, 2005. Pharmacopoeia of People's Republic ofChina, Part I, 2005 ed. Chemical Industry Press, Beijing, p. 276.
Crumb, W., Cavero, I.I., 1999. QT interval prolongation by non-cardiovascular drugs:issues and solutions for novel drug development. Pharm. Sci. Technolo. Today 2,270–280.
Dolejs, L., Hanus, V., Voticky, Z., Tomko, J., 1965. Alkaloids from Buxus sempervirens. III.Mass spectral fragmentation. Collect. Czechoslov. Chem. Commun. 30, 2869–2874.
Du, X., Lu, D., Daharsh, E.D., Yao, A., Dewoody, R., Yao, J.A., 2006. Dimethyl sulfoxideeffects on hERG channels expressed in HEK293 cells. J. Pharmacol. Toxicol. Methods54, 164–172.
Duncan, R.S., McPate, M.J., Ridley, J.M., Gao, Z., James, A.F., Leishman, D.J., Leaney, J.L.,Witchel, H.J., Hancox, J.C., 2007. Inhibition of the HERG potassium channel by thetricyclic antidepressant doxepin. Biochem. Pharmacol. 74, 425–437.
Eriksson, J.W., Carlberg, B., Hillorn, V., 1999. Life-threatening ventricular tachycardiadue to liquorice-induced hypokalaemia. J. Intern. Med. 245, 307–310.
Fang, T.H., Xue, P.F., Jing, S.E., Zhang, S.W., 2000. The cardiac toxicity of cyclovirobuxineD studied on dog. In: Liang, B.W., Zhang, Z.W. (Eds.), Huangyangning, Cardiovas-cular and Cerebrovascular Diseases. Lantian Press, Beijing, pp. 197–200.
Firenzuoli, F., Gori, L., Galapai, C., 2005. Adverse reaction to an adrenergic herbal extract(Citrus aurantium). Phytomedicine 12, 247–248.
Grossini, E., Avanzi, G., Gallicchio, M., Molinari, C., Vacca, G., Bellomo, G., 2005.Regulation of Ca2+ movements by cyclovirobuxine D in ECV304 endothelial cells.Pharmacol. Res. 52, 154–161.
Gui, L., Li, Z.W., DU, R., Yuan, G.H., Li, W., Ren, F.X., Li, J., Yang, J.G., 2005. Inhibitory effectof rhynchophylline on human ether-a-go-go related gene channel. Sheng Li XueBao 57, 648–652.
Haller, C.A., Benowitz, N.L., 2000. Adverse cardiovascular and central nervous systemevents associated with dietary supplements containing ephedra alkaloids. N. Engl.J. Med. 343, 1833–1838.
Haverkamp, W., Breithardt, G., Camm, A.J., Janse, M.J., Rosen, M.R., Antzelevitch, C.,Escande, D., Franz, M., Malik, M., Moss, A., Shah, R., 2000. The potential for QTprolongation and proarrhythmia by non-antiarrhythmic drugs: clinical andregulatory implications. Report on a policy conference of the European Society ofCardiology: Eur. Heart J., 21, pp. 1216–1231.
He, J., Wang, Y., Ren, X.L., Pan, G.X., Yang, J.F., Wang, B.H., Huang, Y.Y., Gao, X.M., 2008.Rapid determination of cyclovirobuxine D in human plasma by HPLC-MS and it'spharmacokinetics study. Tianjin J. Tradit. Chin. Med. 25, 419–421.
Hu, S.L., Zhou, L.H., Fan, S.F., 1981. Experimental analysis of the anti-arrhythmic andarrhythmia-inducing actions of cyclovirobuxine D. Zhongguo Yao Li Xue Bao 2,101–107.

267J. Zhao et al. / European Journal of Pharmacology 660 (2011) 259–267
Hu, D., Liu, X., Wang, Y., Chen, S., 2007. Cyclovirobuxine D ameliorates acute myocardialischemia by K(ATP) channel opening, nitric oxide release and anti-thrombosis. Eur.J. Pharmacol. 569, 103–109.
Huang, X., Yang, Y., Zhu, J., Dai, Y., Pu, J., 2009. The effects of a novel anti-arrhythmicdrug, acehytisine hydrochloride, on the human ether-a-go-go related gene Kchannel and its trafficking. Basic Clin. Pharmacol. Toxicol. 104, 145–154.
Jordan, S., Murty, M., Pilon, K., 2004. Products containing bitter orange or synephrine:suspected cardiovascular adverse reactions. CMAJ. 171, 993–994.
Kamiya, K., Mitcheson, J.S., Yasui, K., Kodama, I., Sanguinetti, M.C., 2001. Open channelblock of HERG K(+) channels by vesnarinone. Mol. Pharmacol. 60, 244–253.
Kamiya, K., Niwa, R., Morishima, M., Honjo, H., Sanguinetti, M.C., 2008. Moleculardeterminants of hERG channel block by terfenadine and cisapride. J. Pharmacol. Sci.108, 301–307.
Li, Y.F., Tu, D.N., Xiao, H., Du, Y.M., Zou, A.R., Liao, Y.H., Dong, S.H., 2010. Aconitine blocksHERG and Kv1.5 potassium channels. J. Ethnopharmacol. 131, 187–195.
Li, B.X., Yang, B.F., Zhou, J., Xu, C.Q., Li, Y.R., 2001. Inhibitory effects of berberine on IK1,IK, and HERG channels of cardiac myocytes. Acta Pharmacol. Sin. 22, 125–131.
Martin, R.L., McDermott, J.S., Salmen, H.J., Palmatier, J., Cox, B.F., Gintant, G.A., 2004. Theutility of hERG and repolarization assays in evaluating delayed cardiac repolari-zation: influence of multi-channel block. J. Cardiovasc. Pharmacol. 43, 369–379.
Milnes, J.T., Crociani, O., Arcangeli, A., Hancox, J.C., Witchel, H.J., 2003. Blockade of HERGpotassium currents by fluvoxamine: incomplete attenuation by S6 mutations atF656 or Y652. Br. J. Pharmacol. 139, 887–898.
Paul, A.A., Witchel, H.J., Hancox, J.C., 2002. Inhibition of the current of heterologouslyexpressed HERG potassium channels by flecainide and comparison with quinidine,propafenone and lignocaine. Br. J. Pharmacol. 136, 717–729.
Picard, S., Lacroix, P., 2003. QT interval prolongation and cardiac risk assessment fornovel drugs. Curr. Opin. Investig. Drugs 4, 303–308.
Rampe, D., Roy, M.L., Dennis, A., Brown, A.M., 1997. Amechanism for the proarrhythmiceffects of cisapride (Propulsid): high affinity blockade of the human cardiacpotassium channel HERG. FEBS Lett. 417, 28–32.
Recanatini, M., Poluzzi, E., Masetti, M., Cavalli, A., De Ponti, F., 2005. QT prolongationthrough hERG K(+) channel blockade: current knowledge and strategies for theearly prediction during drug development. Med. Res. Rev. 25, 133–166.
Redfern, W.S., Carlsson, L., Davis, A.S., Lynch, W.G., MacKenzie, I., Palethorpe, S., Siegl,P.K., Strang, I., Sullivan, A.T., Wallis, R., Camm, A.J., Hammond, T.G., 2003.Relationships between preclinical cardiac electrophysiology, clinical QT intervalprolongation and torsade de pointes for a broad range of drugs: evidence for aprovisional safety margin in drug development. Cardiovasc. Res. 58, 32–45.
Sanguinetti, M.C., Jiang, C., Curran, M.E., Keating, M.T., 1995. Amechanistic link betweenan inherited and an acquired cardiac arrhythmia: HERG encodes the IKr potassiumchannel. Cell 81, 299–307.
Shah, R.R., 2004. Pharmacogenetic aspects of drug-induced torsade de pointes:potential tool for improving clinical drug development and prescribing. Drug Saf.27, 145–172.
Smith, P.L., Baukrowitz, T., Yellen, G., 1996. The inward rectification mechanism of theHERG cardiac potassium channel. Nature 379, 833–836.
Snyders, D.J., Chaudhary, A., 1996. High affinity open channel block by dofetilide ofHERG expressed in a human cell line. Mol. Pharmacol. 49, 949–955.
Su, Z., Martin, R., Cox, B.F., Gintant, G., 2004. Mesoridazine: an open-channel blocker ofhuman ether-a-go-go-related gene K+ channel. J. Mol. Cell. Cardiol. 36, 151–160.
Theoharides, T.C., 1997. Sudden death of a healthy college student related to ephedrinetoxicity from a ma huang-containing drink. J. Clin. Psychopharmacol. 17, 437–439.
Trudeau, M.C., Warmke, J.W., Ganetzky, B., Robertson, G.A., 1995. HERG, a humaninward rectifier in the voltage-gated potassium channel family. Science 269, 92–95.
Vandenberg, J.I., Walker, B.D., Campbell, T.J., 2001. HERG K+ channels: friend and foe.Trends Pharmacol. Sci. 22, 240–246.
Walker, B.D., Singleton, C.B., Tie, H., Bursill, J.A., Wyse, K.R., Valenzuela, S.M., Breit, S.N.,Campbell, T.J., 2000. Comparative effects of azimilide and ambasilide on the humanether-a-go-go-related gene (HERG) potassium channel. Cardiovasc. Res. 48, 44–58.
Wang, Y.X., Zheng, Y.M., Tan, Y.H., Sheng, B.H., 1996. Anti-atrial fibrillation effects ofcyclovirobuxine-D and its electrophysiological mechanism studied on guinea pigatria. Yao Xue Xue Bao 31, 481–486.
Weirich, J., Antoni, H., 1998. Rate-dependence of antiarrhythmic and proarrhythmicproperties of class I and class III antiarrhythmic drugs. Basic Res. Cardiol. 93,125–132.
Witchel, H.J., Hancox, J.C., 2000. Familial and acquired long QT syndrome and thecardiac rapid delayed rectifier potassium current. Clin. Exp. Pharmacol. Physiol. 27,753–766.
Witchel, H.J., Pabbathi, V.K., Hofmann, G., Paul, A.A., Hancox, J.C., 2002. Inhibitoryactions of the selective serotonin re-uptake inhibitor citalopram on HERG andventricular L-type calcium currents. FEBS Lett. 512, 59–66.
Yap, Y.G., Camm, A.J., 1999. Arrhythmogenic mechanisms of non-sedating antihista-mines. Clin. Exp. Allergy 29, 174–181.
Yap, Y.G., Camm, A.J., 2003. Drug induced QT prolongation and torsades de pointes.Heart 89, 1363–1372.
Zhang, Y., Du, J., Zhang, Y., Sun, H.L., Pan, Z.W., Lu, Y.J., Li, B.X., Yang, B.F., 2007. Effectsof matrine, oxymatrine and resveratrol on HERG channel expression. Yao Xue XueBao 42, 139–144.
Zhang, Y.Y., Wang, J.P., Li, P.F., Chen, B.L., Li, D., Yuan, H.L., 2001. Effect ofHuangyangning enhanced tablet on antiarrhythmia and increasing coronaryblood flow. Chin. J. Clin. Pharm. 10, 310–313.
Zhao, X.L., Gu, D.F., Qi, Z.P., Chen, M.H., Wei, T., Li, B.X., Yang, B.F., 2009. Comparativeeffects of sophocarpine and sophoridine on hERG K+ channel. Eur. J. Pharmacol.607, 15–22.
Zhao, W.X., Qi, Z.P., Bai, Y.L., Zhang, Y., Zhao, X.L., Lu, Y.J., Li, B.X., Yang, B.F., 2007. Effectof resveratrol on function of HERG K+ channels. Chin. Pharmacol. Bull. 23, 865–867.
Zhou, Z., Gong, Q., Ye, B., Fan, Z., Makielski, J.C., Robertson, G.A., January, C.T., 1998.Properties of HERG channels stably expressed in HEK 293 cells studied atphysiological temperature. Biophys. J. 74, 230–241.