Clinical Considerations for Managing Iron Overload in MDS: Analysis From EHA
15
Clinical Considerations for Managing Iron Overload in MDS: Analysis From EHA Aristoteles Giagounidis, MD, PhD Associate Professor of Medicine Head, Hematology/Oncology Clinical Research Unit St. Johannes Hospital Duisburg, Germany
description
Clinical Considerations for Managing Iron Overload in MDS: Analysis From EHA. Aristoteles Giagounidis, MD, PhD Associate Professor of Medicine Head, Hematology/Oncology Clinical Research Unit St. Johannes Hospital Duisburg, Germany. Iron Accumulation Due to Transfusion Therapy in MDS. - PowerPoint PPT Presentation
Transcript of Clinical Considerations for Managing Iron Overload in MDS: Analysis From EHA

Clinical Considerations for Managing Iron Overload in MDS:
Analysis From EHA
Aristoteles Giagounidis, MD, PhDAssociate Professor of Medicine
Head, Hematology/Oncology Clinical Research Unit St. Johannes Hospital
Duisburg, Germany

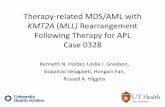
2 units/month
Iron Accumulation Due to Transfusion Therapy in MDS
Serum ferritin ~ 1000 μg/L
Moderate transfusion requirement
Normal body iron: 3-4 g No physiological mechanism to excrete excess iron
24 units/year
≥ 5 g iron/year
Porter JB. Br J Haematol. 2001;115:239-252.

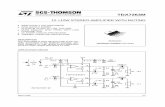
Nonleukemic Cause of Death and Relationship to Iron Overload in MDS
Malcovati L, et al. J Clin Oncol. 2005;23:7594-7603.
Death in low-risk MDSCardiac failure is more common in transfused than in nontransfused patients (P = .01)
N = 467
51
31
8 8
0
25
50
75
100
Cardiac failure
Infection Hemorrhage Hepaticcirrhosis
Perc
enta
gePe
rcen
tage

Assessment of Iron Overload in MDS
• Serum ferritin• MRI
– Heart– Liver
• Prognostic risk category influences management decisions– IPSS – WPSS: incorporates transfusion dependency, karyotype,
WHO subgroup
IPSS = International Prognostic Scoring System; MRI = magnetic resonance imaging

Prognostic Impact of Development of Iron Overload Is Independent of WPSS Score in MDS
* Multivariate analyses including WPSS and development of iron overload (time dependent) (n = 580). Cases with < 3 serum ferritin measurements were excluded.
Sanz G, et al. Presented at 50th Annual Meeting of the American Society of Hematology. San Francisco, CA, 8 December 2008. Abst 640.
WPSS = WHO classification-based Prognostic Scoring System
Overall survival
Variable* HR P valueIron overload 4.34 <.001
WPSS 1.60 <.001
Leukemia-free survival
Variable* HR P valueWPSS 2.24 <.001
Iron overload 2.13 <.001

EHA 2010: Independent Impact of Transfusion Dependence and IO on Survival in MDS
Arnan M, et al. 2010 Annual Meeting of the European Hematology Association. Abst 314.
Survival Time (years)
Cum
ulati
ve P
ropo
rtion
Sur
vivi
ng
Transfusion independent
Transfusion dependentP < .01
0.00 5.00 10.00 15.00 20.00
0.0
0.2
0.4
0.6
0.8
1.0

EPIC: Iron Chelation With Deferasirox Reduces Iron Burden in MDS• After 12 months, significant reductions from baseline observed in:
– Median serum ferritin (-253 ng/mL; P = .002)– Mean ALT (-27.7 ± 37.4 U/L; P < .0001)
Gattermann N, et al. Leuk Res. 2010 [Epub ahead of print].
0
500
1000
1500
2000
2500
3000
Baseline 3 6 9 12
Serum ferritin (ng/mL)
Baseline 3 6 9 12
Time (months)
Med
ian
Seru
m F
erriti
n (n
g/m
L)M
ean ALT (U/L)
ALT (U/L)
Mean actual dose: 19.2 ± 5.4 mg/kg/day
0
10
20
30
40
50
60
70

EPIC: Iron Chelation With Deferasirox Reduced LPI at Each Time Point
Gattermann N, et al. Leuk Res. 2010 [Epub ahead of print].
Mean LPI (+SD) pre- and post-deferasirox administration at baseline and after repeat doses
*P < .0001; †P = .0037 vs pre-administration at baseline.LPI = labile plasma iron.
Mea
n LP
I (μm
ol/L
)
**
†
Normal threshold
(n = 225) (n = 222) (n = 210) (n = 220) (n = 165) (n = 164) (n = 147) (n = 138)

Matched-Pair Analysis: Iron Chelation Therapy vs Transfusion Therapy Only in MDS
• Retrospective matched-pair analysis:– 94 MDS patients undergoing long-term chelation therapy – 93 patients in Düsseldorf MDS Registry receiving supportive care only
• Pairs matched according to age at diagnosis, gender, MDS type (WHO classification), and IPSS score
• All patients had iron overload (serum ferritin > 500 ng/mL)• Patients were followed until death or June 30, 2009
Aim: To evaluate survival in patients with MDS following chelation therapy by matched-pair analysis
Fox F, et al. Blood. 2009;114(11):abst 1747.

Matched-Pair Analysis Results: Patient Survival
Fox F, et al. Presented at ASH 2009 [Blood. 2009;114(11):abst 1747].
Iron chelation group
Supportive care group P value
Mortality during observation period 52% 58%
Median survival 74 mo 49 mo 0.002
Cumulative risk of AML transformation 5 years after diagnosis
19% 18% 0.73 (NS)
AML = acute myeloid leukemia

Survival and Causes of Death in IPSS Low-Risk or INT-1 Patients with MDS by Chelation History
• Multivariate analysis of data from regularly transfused patients followed for 2.5 yrs (N = 97)
• No significant difference in causes of death between the 2 groups (P = .51)
• Multivariate Cox analysis: adequate chelation strongest independent factor associated with better OS
Pts chelated ≥ 6 mo (n = 53)
Nonchelated pts
(n = 44) P valueMortality during follow-up 51% 73% --
Median OS 124 mo 53 mo < .0003
Rose C, et al. Leuk Res. 2010;34:864-870.
OS = overall survival

RBC-transfusion-dependent MDS
Serum ferritin > 1000 µg/L
Risk score
YES NO
RA, RARS, RCMD, RCMD-RS, 5q−
Low and Int-1
WPSS
IPSS
RAEB
Int-2and High
Co-morbidities?
Iron chelation?
Iron Chelation in MDS: Patient Selection
Gattermann N, et al. Hematol Oncol Clin North Am. 2005;19(suppl 1):18-25.
RAEB = refractory anemia with excess blasts

Iron Chelator Treatment Selection in MDS: Considerations
Deferoxamine Deferiprone Deferasirox
Delivery route Parenteral8-24 hr x 5-7 d/wk Oral, TID Oral, QD
Half-life (hrs) .5 2-3 12-16
Common toxicities
• Infusion-site reaction
• Allergic reaction• Auditory• Ocular
• Neutropenia• Agranulocytosis• Nausea/vomiting• Arthropathy
• Transient nausea• Diarrhea• Rash• Renal toxicity
Greenberg PL, et al. JNCCN. 2009;7(Suppl 9):S1-S16.

Ongoing Studies
• TELESTO: Myelodysplastic Syndromes (MDS) Event-Free Survival With Iron Chelation Therapy Study – Phase 3, multicenter, randomized, double-blind,
placebo-controlled trial of deferasirox in patients with Low/Int-1–risk MDS and transfusional iron overload
– Primary endpoint: Event-free survival (composite endpoint including death and nonfatal events related to cardiac and liver function)
– Secondary endpoints: overall survival, TSH, glucose-tolerance testing, IPSS score, change in hematologic function expressed in total number of blood transfusions

Conclusions
• Transfusion dependency and iron overload: adverse effects on morbidity and mortality of patients with MDS– Particular issue in low-risk MDS due to longer-term transfusion
therapy
• Assessment: serum ferritin, liver/heart MRI, IPSS/WPSS prognostic scoring
• Iron chelation shown to reduce iron burden and LPI, improve survival in patients with MDS and iron overload
• Treatment selection considerations with iron chelators: – Efficiency, administration route/treatment compliance, tolerability
in primarily elderly patients