Chinese Guideline of Diagnosis and treatment of … › wp-content › uploads › 2020 › 03 ›...
30
Bin Cao, MD China-Japan Friendship Hospital Ins4tute of Respiratory Medicine, Chinese Academy of Medical Science Na4onal Clinical Research Center for Respiratory Diseases [email protected] 18, March 2020 Chinese Guideline of Diagnosis and treatment of COVID-19 (7 th Version)
Transcript of Chinese Guideline of Diagnosis and treatment of … › wp-content › uploads › 2020 › 03 ›...

BinCao,MDChina-JapanFriendshipHospital
Ins4tuteofRespiratoryMedicine,ChineseAcademyofMedicalScienceNa4onalClinicalResearchCenterforRespiratoryDiseases
[email protected],March2020
ChineseGuidelineofDiagnosisandtreatmentofCOVID-19(7thVersion)

2
n Belongtotheβgenus;Haveenvelopes;Roundoroval;diameterbeing60to140nm
n showed 79.0% nucleo4de iden4ty with the sequence of SARS-CoV and51.8%iden4tywiththesequenceofMERS-CoV.
SevereAcuteRespiratorySyndromeCoronavirus-2
n Sensi4ve to ultraviolet and heat. 75% ethanol,chlorine-containing disinfectant, perace4c acid,and chloroform can effec4vely inac4vate thevirus.
n Chlorhexidinewasnoteffec4ve

3
EpidemiologyofCOVID-19globally n COVID-19hasspreadtotheworldrapidly.—— Athreatoftheword
h"ps://www.who.int/docs/default-source/coronaviruse/situa7on-reports/20200317-sitrep-57-covid-19.pdf?sfvrsn=a26922f2_4

4
PathogenicchangesofsevereCOVID-19inlung
XiaohongYaoetal.ChineseJournalofPathology.2020,49(2020-03-15).
n The pathological features in lungs greatly resemble those seen inSARSandMERSinfec4on
n bilateraldiffusealveolardamagewithcellularfibromyxoidexudates
hyalinemembraneforma4on(bluearrow)
Hyalinemembraneforma4on(bluearrow)
Inters44almononuclearinflammatoryinfiltrates Inters44almononuclearinflammatoryinfiltrates
Inters44almononuclearinflammatoryinfiltrates
Thrombusinpulmonaryarterioles(blackarrow)

5
SevereAcuteRespiratorySyndromeCoronavirus-2
n Viralpar4cleinAlveolartypeIIcells(Electronmicroscopy)
ZheXuetal.LancetRespirMed.2020.DOI:10.1016/S2213-2600(20)30076-X

6
PathogenicchangesofsevereCOVID-19inotherorgans n Degenera4onandnecrosisofparenchymalcells,forma4onofhyaline
thrombusinsmallvessels,andpathologicalchangesofchronicdiseaseswereobservedinotherorgansand4ssues
n Decreasednumbersoflymphocyte,celldegenera4onandnecrosiswereobservedinspleen
ZheXuetal.LancetRespirMed.2020.DOI:10.1016/S2213-2600(20)30076-X

7
DiagnosIccriteriaofCOVID-19——Suspectedcases Suspectedcases
Epidemiologicalhistory(≤14days) Clinicalsymptoms Ø travel/residenceinWuhananditssurrounding
areas,orothercommuni4eswhereCOVID-19hasbeenfound
Ø feverand/orrespiratorysymptoms
Ø contactwithCOVID-19pa4ents Ø imagingcharacteris4csofCOVID-19
Ø Contactwithpa4entswithfeverorrespiratorysymptomsandfromWuhananditssurroundingareas,orfromcommuni4eswhereCOVID-19hasbeenfound
Ø NormalordecreasedofWBC;NormalordecreasedofLymphocytes
Ø Clusteredcases
n AnyonecriteriaofEpidemiologicalhistory+AnytwoClinicalsymptomsn Allthreeclinicalsymptoms

8
DiagnosIccriteriaofCOVID-19——Confirmedcases
Confirmedcases E4ologicalorserologicalevidences
Nucleicacidtes4ng
n SARS-CoV-2RNAwasposi4vedetectedbyreal4meRT-PCR
n Viralgenesequenceishighlyhomologoustoknownnewcoronaviruses
Seruman4bodytes4ng
n SARS-CoV-2specificIgMandIgGareposi4veinserum
n SARS-CoV-2specificIgGisdetectablefromnega4vetoposi4ve
n SARS-CoV-2specificIgGan4body4tershowsa4-foldorhigherchangebetweenthetwosetsofserumsamplesfromacuteandrecoveryphase
Suspectcases+oneofeIologicalorserologicalevidences

9
IgG/IgMDynamicchangesofAdultswithCOVID-19
ZhongLiuetal.unpublisheddata

10
TransmissionandincubaIonofCOVID-19
MedianincubaIonperiod4-5.2daysThe95thpercenIleofthedistribuIonwas12.5days
BasicreproducIvenumberR0=2.2-2.95
n COVID-19paIentsincludingtheasymptoma4cinfectedpeoplearethemainsourceofinfec4on
n Routeoftransmissionn Respiratorydropletsandclosecontactn Long-4meexposuretotheenvironmentwithahighconcentra4onsofaerosoln Environmentcontaminatedbyfeces/urine→aerosolorcontacttransmission
n Allthepopula4onaregenerallysuscep4ble
YWangetal.ZhonghuaLiuXingBingXueZaZhi.41(4),476-479;QunLietal.NEnglJMed.DOI:10.1056/NEJMoa2001316GuanWJetal.NEnglJMed.2020.doi:10.1056/NEJMoa2002032

11
DiseasespectrumofCOVID-19
81%
14%
5%
mild severe criIcaln 81%weremildstatusn Nopneumoniaormildpneumonia
n 14%wereseverestatusn DyspneaorRespiratoryRate≥30/minor
SpO2<93%orPaO2/FiO2<300mmHgn Lunginfiltrates>50%within24to48
hoursn 5%werecriIcalillstatus
n Needsmechanicalven4la4onn Shockn Complicatedwithotherorganfailure
requiredICUadmission ZunyouWuetal.JAMA.2020.DOI:10.1001/jama.2020.2648

12
ClinicalfeaturesofCOVID-19paIents SymptomsandcomplicaIons N%
Fever 98%
Cough 76%
Myalgiaorfa4gue 44%
Sputumproduc4on 28%
Diarrhea 3%
WBC≤10×109/L 70%
Lymphocytopnia 63%
ALT>40U/L 37%
Cr>133mmol/L 10%
LDH>243U/L 73%
Hypersensi4vetroponinI>28pg/ml 12%
Procalcitonin<0.1ng/ml 69%
Acuterespiratorydistresssyndrome 29%
SymptomsandcomplicaIons N%
Acutecardiacinjury 12%
Acutekidneyinjury 7%
Sep4cshock 7%
Secondaryinfec4on 10%
HuangCetal.Lancet.2020;395(10223):497-506.

13
ClinicalcourseofCOVID-19——SevereandcriIcalillness
FeiZhouetal.Lancet.2020.DOI:10.1016/S0140-6736(20)30566-3
n Dura4onofdyspneawas13daysinsurvivorsn 45%survivorss4llhadcoughondischargen Mediandura4onofviralsheddingwas20days,couldprolongas37daysn lymphocytecountwaslowestonday7aoerillnessonsetandimprovedduringhospitalisa4onin
survivorsbutwhereasseverelymphopeniawasobservedun4ldeathinnon-survivors.

14
Healthycontrol
ICU care
No ICU care
0
10
20
30
4080
100
120
pg/m
l
IFN-γp < 0·01
p = 0·27p < 0·01
Healthycontrol
ICU care
No ICU care
0
5
10
15
20
25
pg/m
l
IL-2p = 0·26
p = 0·04p = 0·02
Healthycontrol
ICU care
No ICU care
0
5
10
15
20
pg/m
l
MIP-1a
p = 0·01
p = 0·02p < 0·01
Healthycontrol
ICU care
No ICU care
0
50
100
150
200
pg/m
l
TNF-α
p = 0·03
p = 0·01p < 0·01
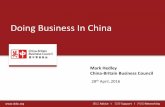
InflammaIonofCOVID-19——SevereandcriIcalillness
All rights reserved. No reuse allowed without permission. author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
The copyright holder for this preprint (which was not peer-reviewed) is the.https://doi.org/10.1101/2020.02.16.20023671doi: medRxiv preprint
All rights reserved. No reuse allowed without permission. author/funder, who has granted medRxiv a license to display the preprint in perpetuity.
The copyright holder for this preprint (which was not peer-reviewed) is the.https://doi.org/10.1101/2020.02.16.20023671doi: medRxiv preprint
n IL-1β,IL-6,G-SCF,IP-10,andMCP1weresignificantlyelevated
n Peripherallymphocytecounts,mainlyTcellsweresubstan4allyreducedinsevereCOVID-19pa4ents
Host-directedtherapiesmightbeanopIon
HuangC,etal.Lancet2020;395(10223):497-506; LiuJ,etal.BMJ2020;publishedonlineFeb19.

15
SARS-CoV-2Viralsepsis——FromBedsidetoBench
n Pneumonia,Respiratoryfailure,Acuterespiratorydistresssyndrome
n Metabolicacidosisandinternalenvironmentdisorders
n Acutekidneyinjuryn Acutecardiacinjuryn ………
MulI-organdysfuncIon
RenL,etal.ChinMedJ2020;DOI:10.1097/CM9.0000000000000722;HuangC,etal.Lancet2020;395(10223):497-506HuiLi,etal.2020;unpublished,underrevision
——ViralSepsis

16
AbnormalcoagulaIoniscommoninsevereCOVID-19 1
5
10
15
20
25
30
35
40
45
50
55
Articles
8 www.thelancet.com Published online March 9, 2020 https://doi.org/10.1016/PII
might be directly caused by SARS-CoV-2 infection, but further research is needed to investigate the pathogenesis of sepsis in COVID-19 illness.
Cardiac complications, including new or worsening heart failure, new or worsening arrhythmia, or myocardial infarction are common in patients with pneumonia. Cardiac arrest occurs in about 3% of inpatients with pneumonia.21 Risk factors of cardiac events after pneumonia include older age, pre-existing cardiovascular diseases, and greater severity of pneumonia at presen-tation.22 Coronary heart disease has also been found to be associated with acute cardiac events and poor outcomes in influenza and other respiratory viral infections.22–24 In this study, increased high-sensitivity cardiac troponin I during hospitalisation was found in more than half of
those who died. The first autopsy of a 53-year-old woman with chronic renal failure in Jinyintan Hospital showed acute myocardial infarction (data not published [A: Can you provide information on where you obtained this information (eg, personal correspondence with some-one?)]). About 90% of inpatients with pneumonia had increased coagulation activity, marked by increased d-dimer concentrations.25 In this study, we found d-dimer greater than 1 µg/L is associated with fatal outcome of COVID-19. High levels of d-dimer have a reported asso-ciation with 28-day mortality in patients with infection or sepsis identified in the emergency department.26 Contri-butory mechanisms include systemic pro-inflammatory cytokine responses that are mediators of atherosclerosis directly contributing to plaque rupture through local inflammation, induction of procoagulant factors, and haemodynamic changes, which predispose to ischaemia and thrombosis.27–29 In addition, angiotensin converting enzyme 2, the receptor for SARS-CoV-2, is expressed on myocytes and vascular endothelial cells,30,31 so there is at least theoretical potential possibility of direct cardiac involvement by the virus. Of note, interstitial mononuclear inflammatory infiltrates in heart tissue has been document in fatal cases of COVID-19, although viral detection studies were not reported.32
The level and duration of infectious virus replication are important factors in assessing the risk of trans mission and guiding decisions regarding isolation of patients. Because coronavirus RNA detection is more sensitive than virus isolation, most studies have used qualitative or quantitative viral RNA tests as a potential marker for infectious coronavirus. For SARS-CoV, viral RNA was detected in respiratory specimens from about a third of patients as long as 4 weeks after disease onset.33 Similarly, the duration of MERS-CoV RNA detection in lower respiratory [A: specimens?] persisted for at least 3 weeks,34,35 whereas the duration of SARS-CoV-2 RNA detection has not been well characterised. In the current study, we found that the detectable SARS-CoV-2 RNA persisted for a median of 20 days in survivors and that it was sustained until death in fatal cases. This has important implications for both patient isolation decision making and guidance around the length of antiviral treatment. In severe influenza virus infection, prolonged viral shedding was associated with fatal outcome and delayed antiviral treatment was an independent risk factor for prolonged virus detection.36 Similarly, effective antiviral treatment might improve outcomes in COVID-19, although we did not observe shortening of viral shedding duration after lopinavir or ritonavir treatment in the current study. Randomised clinical trials for lopinavir–ritonavir (ChiCTR2000029308) and of intravenous remdesivir (NCT04257656, NCT04252664) in treatment of COVID-19 [A: Addition correct?] are currently in progress.
Our study has some limitations. First, due to the retrospective study design, not all laboratory tests were done in all patients, including lactate dehydrogenase,
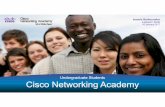
Figure 2: Temporal changes in laboratory markers from illness onset in patients hospitalised with COVID-19Figure shows temporal changes in d-dimer (A), lymphocytes (B), IL-6 (C), serum ferritin (D), high-sensitivity cardiac troponin I (E), and lactate dehydrogenase (F). Differences between survivors and non-survivors were significant for all timepoints shown, except for day 4 after illness onset for d-dimer, IL-6, and high-sensitivity cardiac troponin I [A: Addition correct?]. COVID-19=coronavirus disease 2019. IL-6=interleukin-6.
4 7 10 13 16 19 22 4 7 10 13 16 19 25220Hi
gh-s
ensit
ivity
card
iac t
ropo
nin
I (ng
/mL)
Days from illness onset
0
50200
150
250100
300150350
200400
250 450
300500
550350 600
E F
Lact
ate d
ehyd
roge
nase
(U/L
)
4 7 10 13 16 19 4 7 10 13 16 190
IL-6
(pg/
mL)
0
6 500
12 1000
18
24
1500
30
2000
2500
C DSe
rum
ferri
tin (µ
g/L)
Days from illness onset
4 7 10 13 16 19 22 4 7 10 13 16 19 22 250
D-di
mer
(µg/
L)
0·0
60·40·2
0·612
0·818
1·0241·2301·4
361·6
42 1·848 2·0
A B
Lym
phoc
yte
coun
t (×1
09 per
L)
2·5
5·56·8 6·6 6·1
7·0
6·3
236
332
323
243
390
302
397 388
198
590
200
301
413
528
217240
8·8
9·5
1·50·5
2·6
14·416·7
0·6 0·7 1·0 0·5
0·600·67
0·520·54 0·49 0·54
0·420·44
1·080·91
0·971·18
1·201·41 1·42
1·43
42·2
35·6
23·8
0·60·3
12·010·7
11·7
17·2
26·4
1025
1646 1645 1698
2000 2000
432
635
447546531393
22·055·7
57·6
134·5
290·6
24·74·1 4·4 2·5 2·5 3·83·3
SurvivorsNon-survivors
20TL1767
n SignificantlyincreasedD-dimerandFDPwereassociatedwithpoorprognosis
n Vascularendotheliuminflamma4onExtensiveintravascularmicrothrombosisonautopsy
n Vascular endothelial cells express high levelsofACE2
AnIcoagulaIontherapyshouldbeiniIatedforsevereCOVID-19paIentsifotherwisecontraindicated.
ZhouF,etal.Lancet2020;DOI:10.1016/S0140-6736(20)30566-3; HammingI,etal.JPathol2004;203(2):631-7.
D-Dimer> 1ug/mlwasindependentriskfactorofin-hospitaldeath

17
SARS-CoV-2RNAdetecIoninCOVID-19paIents n SARS-CoV-2 RNA could be detected in nasopharyngeal swabs, sputum, lower
respiratorytractsecre4ons,blood,fecesusingRT-PCRand/orNGSmethodsn Posi4veratewashigherinlowerrespiratorytractspecimenn Thespecimensshouldbesubmiqedfortes4ngassoonaspossibleaoercollec4on
88,90%
73,30%
60,00%
82,20%
72,10%61,30%
0,0
0,2
0,4
0,6
0,8
1,0
Sputumsample Nasalswabs Throatswabs
milddisease severedisease
WeiZhangetal.EmergMicrobesInfect,9(1),386-389;YangYetal.medRxiv2020.

18
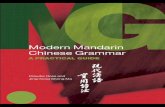
FeaturesofCTscanofCOVID-19
HeshuiShietal.LancetInfectDis.2020.DOI:10.1016/S1473-3099(20)30086-4
56-year-oldmanDay3aoersymptomonsetFocalground-glassopacity
74-year-oldwomanDay10aoerillnessonsetBilateral,peripheralground-glassopacity
61-year-oldwomanDay20aoersymptomonsetBilateralandperipheralpredominantconsolida4on
63-year-oldwomanDay17aoersymptomonsetBilateral,peripheralmixedpaqern;Airbronchogram;Pleuraleffusion
n Common:bilaterallunginvolvement(79%);peripheraldistribu4on(54%);diffusedistribu4on(44%)
ground-glassopacity(65%);withoutseptalthickening(65%).
n Lesscommon:nodules(6%),cys4cchanges(10%),bronchiolectasis(11%),pleuraleffusion(5%).
n Notobserved:Tree-in-budsigns,masses,cavita4on,andcalcifica4ons

19
FeaturesofimaginechangeoverIme
Ctscanbeforeillnessonset ≤1weeka\er
symptomonset >1weekto2weeksa\ersymptomonset
>2weeksto3weeksa\ersymptomonset
HeshuiShietal.LancetInfectDis.2020.DOI:10.1016/S1473-3099(20)30086-4

20
RapiddeterioraIononCTscan-case1 Male,70yearsold
2020-1-28Day9a\erillnessonset
2020-2-1Day13a\erillnessonset. Died2weekslater.

21
Male,62yearsold
2020-2-7Day12a\erillnessonset
2020-2-7Day19a\erillnessonset.Died15dayslater
RapiddeterioraIononCTscan-case2

22
RenL,etal.ChinMedJ2020;DOI:10.1097/CM9.0000000000000722HuangC,etal.Lancet2020;395(10223):497-506.RenL,etal.ChinMedJ2020;DOI:10.1097/CM9.0000000000000722HuangC,etal.Lancet2020;395(10223):497-506.
IsolaIonandSupporttreatmentofCOVID-19 n Allconfirmedpa4entsshouldbeisola4on.n Suspectedcaseshouldbetreatedinisola4oninasingleroomn HospitalandICUadmissiondecisionwasaccordingtodiseaseseverityn Strengtheningsupporttreatment(mostpa4entscomplicatedwithhypoproteinemia)
n sufficientcaloricn waterandelectrolytebalance
n Oxygentherapyn Closelymonitoringvitalsignandlaboratory(progressrapidlyinseverepaIents)
n WBC;Lymphocyten Biochemicalindicators(liverenzyme,myocardialenzyme,renalfunc4on.etc)n Markerofinflamma4on(serumferri4n,IL-6,cytokine)n Chestimaging

23
TreatmentopIonsforsevereorcriIcalCOVID-19 Respiratorysupport
Circulatorysupport
Renalreplacementtherapy
Convalescentplasma
treatment
BloodpurificaIontreatment
Immunotherapy
OthertherapeuIcmeasures

AnIviralintervenIons
n So far, no specific antiviral against SARS-CoV-2 has been proved
n Clinically evaluated drugs:
n Lopinavir/ritonavir monotherapy (LOTUS China, ChiCTR2000029308): completed, manuscript accepted, online tomorrow
n Promising results
n CAP China Remdesivir 1 (mild-moderate pneumonia, NCT04252664): ongoing
n CAP China Remdesivir 2 (severe-critical pneumonia, NCT04257656): ongoing
Emmie de Wit et al. Nature Reviews Microbiology 2016; 14, 523–534 Timothy P Sheahan; Nat Commun 2020; 11 (1), 222 Yeming wang, et al. Trial, 2020, under peer review

25
CAP-ChinaRemdesivirtrialsongoingforCOVID-19 Standardcare+Remdesivir
Standardcare+Placebo
Primaryoutcome:Clinicalimprovementonday28Secondaryoutcome:The4mefromrandomiza4ontoclinicalimprovement
Totalcourseoftreatment: 10days
2:1randomiza4on
Illnessonset
≤12days Screen enroll
hospitaliza4on 24 h
Followup
Day0
Remdesivir:Firstdosage:200mgivqd×1days;
Con4nuous100mgqd×9days
Placebo:50mlqd×10days
Day1 Day3 Day5 Day7 Day10 Day14 Day21 Day28
n TheclinicaltrailofRemdesivirtreatmentforsevereCOVID-19isongoing

26
AnIviralforCOVID-19:otherpotenIalchoices
n Alpha-interferon:5MU,atomiza4oninhala4ontwicedailyn Ribavirin:usedtogetherwithinterferonorlopinavir/ritonavir,500mgtwiceor
three4mesofintravenousinjec4ondaily,nolongerthan10daysn Chloroquinephosphate:500mgbidfor7daysforadultsaged18-65withbody
weightover50kg;500mgbidforDays1&2,and500mgdailyforDays3-7foradultswithbodyweightbelow50kg
n Arbidol:200mgthree4medailyforadults,nolongerthan10daysn Convalescentplasmatreatment: infusiondose200-500ml(4-5ml/kg)×2n Favipiravir

27
UseofcorIcosteroidissIllcontroversial
n Onlyforpa4entswithrapidprogressivedeteriora4onoxygena4on, radiology
imagingandexcessiveinflamma4on
n Contraindica4ons:allergy;un-controlleddiabetes;uncontrolledhypertension;
glaucoma;GIbleeding;immunodepression;lymphocytelessthan300/ul;severe
bacterialand/orfungalinfec4ons
n Shortterm,3-5days
n Low-moderatedosagen nomorethanmethylprednisolone1-2mg/kg/day
LianghanShangetal.Lancet.2020.h"ps://doi.org/10.1016/PIIZhaoJP,etal.ZhonghuaJieHeHeHuXiZaZhi2020;43:E007(inChinese).

28
DilemmaofARB/ACEi n LeqerfromProf.GiovannideSimone,Chair,CouncilonHypertension,EuropeanSociety
ofCardiology
n An4-RASmedsofcoursereduceangio-IIac4vity,whichisgoodforlung
inflammatoryresponse.
n However,toomuchinhibi4onofangio-IImightincreaseACE2ac4vity,because
angio-IIincreaseACE2cleavagethroughAT1R-ac4vatedTNF-alfa-ACE,andthis
mightnotbegoodfortheCOVID-19ac4on.
n BinCao’responsetoProf.GiovannideSimone
n Inourcohort,48%(26/48)non-survivorshadhypertension,whereasthe
percentageofhypertensionwasonly23%(32/137)insurvivors.TheORfor
hypertensioninANOVAis3.05(1.57-5.92).
n Nodefiniteanswertotheques4onofARB/ACEi ZhouF,etal.Lancet2020;DOI:10.1016/S0140-6736(20)30566-3

29
DischargecriteriaofCOVID-19
n Bodytemperatureisbacktonormalformorethanthreedays
n Respiratorysymptomsimprovedobviously
n Pulmonaryimagingshowsobviousabsorp4on
n Twoconsecu4venega4venucleicacidtestsforrespiratory
specimens(samplingintervalbeingatleast24hours)

30
Allhealth-careworkersinvolvedinthediagnosisandtreatmentofpaIentsinWuhan
China-Japan Friendship Hospital Chen Wang; Yeming Wang; Fei Zhou; Guohui Fan; Hui Li; Zhibo Liu; Yi Zhang
UniversityofVirginiaFrederickGHaydenOxfordUniversityPeterWHorby
HuaZhongUniversityLiangLiu
Wuhan Jinyintan Hospital Wuhan Tongji Hospital
Wuhan Lung Hospital The Central Hospital of Wuhan
Zhongnan Hospital of Wuhan University Renmin Hospital of Wuhan University
Union Hospital Wuhan First hospital
Wuhan Third hospital Wuhan Fourth hospital
Cooperators:
Acknowledgements