Chapter 12: Quantitatve Methods in Health Care Management Yasar A. Ozcan 1 Chapter 12. Quality...
66
Chapter 12: Quantitat Chapter 12: Quantitat ve Methods in Health ve Methods in Health Care Management Care Management Yasar A. Ozcan Yasar A. Ozcan 1 Chapter 12. Chapter 12. Quality Control Quality Control UCL LCL Sample number 1 3 4 5 6 7 8 9 2 10 11 1 2 CL x +1σ -1σ -2σ -3σ +2σ +3σ R A x A Zone 2 R A x B Zone 2 2 1 R A x C Zone 2 3 1 R A x B Zone 2 2 1 R A x C Zone 2 3 1 R A x A Zone 2
-
Upload
ilene-obrien -
Category
Documents
-
view
229 -
download
12
Transcript of Chapter 12: Quantitatve Methods in Health Care Management Yasar A. Ozcan 1 Chapter 12. Quality...

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 11
Chapter 12.Chapter 12.
Quality ControlQuality ControlUCL
LCL
Sample number
1 3 4 5 6 7 8 92 10 11 12
CL x
+1σ
-1σ
-2σ
-3σ
+2σ
+3σ RAxAZone 2
RAxBZone 22
1
RAxCZone 23
1
RAxBZone 22
1
RAxCZone 23
1
RAxAZone 2

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 22
OutlineOutline Quality in Healthcare Quality Experts Quality Certification TQM & CQI Six-Sigma Monitoring Quality through Control Charts
– Control Charts for Attributes– Control Charts for Variables
Process improvement Methods for Generating New Ideas Tools for Investigation

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 33
A Broad Definition. . .A Broad Definition. . .
Quality refers to the ability of a product or service Quality refers to the ability of a product or service to consistently meet or exceed customer to consistently meet or exceed customer expectationsexpectations
quality in healthcare is evaluated from differing quality in healthcare is evaluated from differing perspectives of providers, recipients and third-perspectives of providers, recipients and third-party payers. party payers.
Most clinicians accept the Institute of Medicine Most clinicians accept the Institute of Medicine (1990) definition: “(1990) definition: “Quality is the extent to which Quality is the extent to which health services for individuals and populations health services for individuals and populations increase the likelihood of desired health increase the likelihood of desired health outcomes and are consistent with current outcomes and are consistent with current professional knowledgeprofessional knowledge.” .”

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 44
What is quality?What is quality?
You are a world renowned surgeon that You are a world renowned surgeon that has just completed a radical new has just completed a radical new surgical technique. There were few surgical technique. There were few complications, largely due to the complications, largely due to the excellence of the hospital’s staff and excellence of the hospital’s staff and technological capabilities.technological capabilities.
QUALITY?QUALITY?

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 55
What is Quality?What is Quality?
You are a patient who has just undergone radical You are a patient who has just undergone radical new surgery. Although the surgery went new surgery. Although the surgery went without technical difficulties, your were upset at without technical difficulties, your were upset at the doctor’s uncaring attitude. Furthermore, the the doctor’s uncaring attitude. Furthermore, the nursing staff often failed to respond to your nursing staff often failed to respond to your calls, and twice you were served meat despite calls, and twice you were served meat despite the fact that you are a vegetarian. Also, there the fact that you are a vegetarian. Also, there was a used bedpan that sat next to your bed for was a used bedpan that sat next to your bed for three days.three days.
QUALITY?QUALITY?

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 66
A question of perspectiveA question of perspective
Quality of care depends upon who is Quality of care depends upon who is making the assessmentmaking the assessment– Clinician-- Clinician-- technical components, adequate technical components, adequate
skills, resources, conditionsskills, resources, conditions– Patients-- Patients-- outcomes, interpersonal processes, outcomes, interpersonal processes,
amenities, overall satisfactionamenities, overall satisfaction– Health Facility Managers-Health Facility Managers- appropriate and appropriate and
effective utilizationeffective utilization– Community-- Community-- availability, access, reputations, availability, access, reputations,
general health status of communitygeneral health status of community

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 77
Quality MeasurementQuality Measurement
Clinicians-- Clinicians-- cure rates, mortality, morbiditycure rates, mortality, morbidity Patients-- Patients-- patient satisfaction surveyspatient satisfaction surveys Health facility managers-- Health facility managers-- cure rates, cure rates,
mortality, morbidity, intermediate process mortality, morbidity, intermediate process measures (patient falls, infection rates, measures (patient falls, infection rates, medication errors, appropriate staffing, etc.)medication errors, appropriate staffing, etc.)
Community-- Community-- area service distribution, area service distribution, insurance coverage, incidence and prevalence insurance coverage, incidence and prevalence rates, etc.rates, etc.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 88
Figure 12.1 Quality Measurement
Structure Process Outcome
InputsConversion Process
(Throughput) Outputs
Patient,provider labor
equipmentsupplies, etc.
Various hospitaland medical servicestransform poor health
to wellness for patients(diagnosis, procedures,
treatments)
Treated Patient

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 99
Quality MeasurementQuality Measurement
Another way to look at the maintenance of quality is how mistakes are to be avoided – design mistake-proof processes across the whole spectrum of the care, to reduce undesired outcomes.
Variance in diagnostic and therapeutic interventions and the associated errors hamper the delivery of safe, effective patient care and add to poor outcomes.
To minimize the variation and the errors – sometimes euphemistically called “quality gaps” – and work toward completely eliminating them are major goals for healthcare systems.
Quality Gaps

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1010
Quality MeasurementQuality Measurement
Chassin (1998) classifies the underlying causes of “quality gaps” into three categories:
1) Over-utilization. When the potential benefit of a therapy is less than its risk, overuse of health services affects the quality of care. Pressures for overuse of services may come from either providers or patients.
2) Under-utilization. A patient’s lack of insurance or insurance that has high co-payments and deductibles can cause under-utilization of necessary health care.
3) Miss-utilization. Avoidable complications, negligent care, mistakes, and mishaps create miss- utilization of services. Healthcare providers who generate such conditions harm the quality of patient care and produce poor outcomes; they also waste the organization’s resources and increase lengths of stay.
Quality Gaps

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1111
Quality MeasurementQuality Measurement
Healthcare providers do have an arsenal of methods to deal effectively with the problems affecting quality of care.
They include the programs called quality control (QC), total quality management (TQM), continuous quality improvement (CQI), reengineering, and Six-Sigma.
All these programs include data gathering, analysis and statistical monitoring to identify the problem and its cause.
Nevertheless, the crux of the solution to quality problems lies in changing human behavior, changing minds to perform care in new ways.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1212
Quality ExpertsQuality Experts
Deming-- poor quality caused by the system, not employees; management’s responsibility to correct system;” use 14 points to reduce variation caused by special causes (correctable) and not common (random) causes of variation.
Juran-- 80% of defects are controllable; three elements: quality planning, quality control, and continual quality improvement
Crosby-- zero defects; quality is free Isikawa-- cause and effect diagrams, quality circles

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1313
Organizations can earn awards or achieve certification/accreditation by international organizations or by their own trade organizations; for instance, hospitals are evaluated periodically by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO).
For the medical group practices, the Medical Group Management Association (MGMA) is the principal voice. MGMA leads the profession and assists members through information, education, networking and advocacy” (MGMA, 2004).
Quality is always a major concern in those advocacy and accreditation bodies.
Quality CertificationQuality Certification

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1414
Quality CertificationQuality Certification ISO 9000 Set of international standards on quality management and Quality
assurance, critical to international Business ISO 9000 series standards, briefly, require firms to document their quality-
control systems at every step (incoming raw materials, product design, in-process monitoring and so forth) so that they’ll be able to identify those areas that are causing quality problems and correct them.
ISO 9000 requires companies to document everything they do that affects the quality of goods and services.
– Hierarchical approach to documentation of the Quality Management
System

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1515
Total Quality Management
A philosophy that involves everyone in an organization in the quest for quality, with customer satisfaction as the driving force
TQM involves:– finding what customers want– designing services to meet customer needs– designing mistake proof delivery process
“pakayoke”– monitoring results and continuous
improvement

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1616
TQM, cont.TQM, cont. TQM requires:
– continual improvement– competitive benchmarking– employee empowerment– team approaches– knowledge of tools
Quality at the source-- each worker responsible for his/her own work
Quality function deployment-- involve customers in service design

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1717
Controlling QualityControlling Quality
Quality control focuses on the conversion of inputs into outputs, i.e., the processes
Goal is to reduce the need for inspection of control efforts
Quality assurance efforts occurring during production of services are referred to as statistical process control

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1818
Plan
DoAct
Check
Figure 12.2 The Deming Wheel/Shewhart Cycle

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 1919
Continuous Quality ImprovementContinuous Quality Improvement
A philosophy seeking to make never-ending improvements to the process of converting inputs into outputs
Kaizen-- Japanese term referring to CI Environment must be conducive to CI
– appropriate vision statement, strategies, tactics– management style encouraging trust, openness– adherence to stated philosophy– reward/incentive systems

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2020
The CQI is a detailed version of a PDSA cycle that comprises:
1) selecting a process that needs an improvement 2) studying and documenting the current process seeking
ways to improve it3) designing an improved process 4) implementing the new process5) monitoring and evaluation6) documenting the process if it worked successfully and
publicizing it through the healthcare organization 7) if it did not achieve its goals, re-starting from step 1.
Continuous Quality ImprovementContinuous Quality Improvement

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2121
Six-SigmaSix-Sigma
•Six- Sigma is one of the latest quality improvement concepts to have emerged during the 1990’s. Its name comes from the measure of variation from the normal distribution (six standard deviations).
•Adopting a six-sigma strategy as a quality goal sets tolerance levels for errors (defectives) to levels that occur only 3.4 times per million observations.
•The defect rates in healthcare can be defined in such distinct areas as public health, inpatient care, ambulatory care, and so on.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2222
Six-SigmaSix-Sigma
Healthcare organizations have reduced the deaths caused by anesthesia from 25-50 per million cases to 5 per million cases since the 1980s through improved monitoring techniques, adaptation of practice guidelines, and other systematic approaches to reduce errors.
This is one area that comes very close to six sigma standards (Chassin, 1998).

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2323
Six-SigmaSix-SigmaDeployment of six-sigma to improve the quality ofhealthcare and delivery performance can beconsidered in the following areas:
a) Clinical excellenceb) Service deliveryc) Service costs, and d) Patient satisfaction.
The deployment can use either of these methodological sequences: DMAIC: define, measure, analyze, improve, and control DMADV: define, measure, analyze, design, and verify.
DMAIC is generally used to improve existing systems that havefallen the below six-sigma levels,
DMADV is used to design and develop new processes or productsat six-sigma levels (Stahl, Shultz, and Pexton, 2003).

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2424
Six-SigmaSix-SigmaThe essence of six-sigma methodologies is both improvement of the knowledge and capability of employees, and also changes behavior through training. Thus six-sigma employs a classification system that identifies education and training for employees, project managers and executives.
Emulating karate honors, certification is granted at Green Belt (GB), Black Belt (BB) and Master Black Belts (MBB) levels.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2525
Six-SigmaSix-SigmaGreen Belts (GBs) are the employees who have taken the training courses on implementing the projects.
Black Belts (BBs) are the project leaders, whose training may be more intensive; they may complete several projects a year depending upon their size and scope.
Master Black Belts (MBBs) are generally assigned to an area that needs improvement (for example, human resources), to ensure that objectives are set, targets are identified, plans are made, and resources are secured to implement the projects in their assigned area.
MBBs may oversee many six-sigma projects at a time, working with various BBs.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2626
Six-SigmaSix-SigmaSix-sigma projects require BBs and MBBs to have expertise in basic statistical tools such as Pareto Diagrams, descriptive and higher level statistics including regression, and statistical modeling techniques as well as control processes.
In addition to statistical concepts, they are expected understand project management, finance, leadership, measurement through socio-metric (survey) analysis, reliability and validity.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2727
Six-SigmaSix-Sigma
Examples of successful six-sigma deployments in healthcare include:
•reduction of emergency room diversions •fewer errors in operating rooms’ cart materials•reduced bloodstream infections in an ICU, and •improved radiology turnaround time (Stahl, Shultz, and Pexton, 2003).

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2828
Quality Measurement and Control TechniquesQuality Measurement and Control TechniquesProcess Variability
In the delivery of health care, there are many occasions when an error can happen in the tasks performed by various clinical staff.
Often the same task may not even be performed the same way for all patients, though minor alterations within defined limits can be acceptable.
When provider performance falls beyond acceptable limits, the errors that occur require investigation and correction.
In order to detect noteworthy variations in process, or tendencies that may cause unacceptable levels of errors, healthcare managers must monitor the processes for quality, using various charts.
The intent of the monitoring is to distinguish between randomrandom and non-randomnon-random variation.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 2929
Quality Measurement and Control TechniquesQuality Measurement and Control TechniquesProcess Variability
The common variations in process variability that are caused by natural incidences are in general not repetitive, but various minor factors due to chance and are called randomrandom variation. If the cause of variation is systematic, not natural, and thesource of the variation is identifiable, the process variationis called non-randomnon-random variation.
In healthcare, non-random variation may occur by notfollowing procedures, using defective materials, fatigue,carelessness, or not having appropriate training ororientation to the work situation, among many reasons.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3030
Quality Measurement and Control TechniquesQuality Measurement and Control TechniquesProcess Variability
Process variation is the range of natural variabilityin a process for which healthcare managers usecontrol charts to monitor the measurements. If thenatural variability or the presence of randomvariation exceeds tolerances set by control charts,then the process is not meeting the designspecifications.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3131
Set design specificationsfor process capability
Pro
cess
Va
riab
ility
UCL
LCL
Process variability meetsand exceeds specifications
Process variabilitydoes not meetdesign specifications
Figure 12.3 Process Capability

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3232
Figure 12.4 Control Limits, Random and Nonrandom Sample Observations
UpperControlLimit(UCL)
LowerControlLimit(LCL)
ProcessMean
Sample number
1 3 4 5 6 7 8 92 10 11 12
Non-random
α/2
α/2
95
.5%
+2σ
-2σ

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3333
Control Charts for Attributes
When process characteristics can be counted, attribute-based control charts are the appropriate way to display the monitoring process.
If the number of occurrences per unit of measure can be counted, or there can be a count of the number of bad occurrences but not of non-occurrences, then ac-chart is the appropriate tool to display monitoring.
Counting also can occur for a process with only two outcomes, good or bad (defective); in such cases p-chart is the appropriate control chart.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3434
Control Charts for Attributes: c-Chart
czcUCL
czcLCL

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3535
Control Charts for Attributes: c-Chart
Example 12.1The number of infections from the Intensive Care Unit (ICU) at the ABC Medical Center over a period of 24 months is obtained. These numbers are the counts of stool assay positive for toxin, segregated by month. The patient population and other external factors such as change in provider have been stable.
Months Infections in ICU
Year 1 Year 2
January 3 4
February 4 3
March 3 6
April 4 3
May 3 4
June 4 3
July 5 5
August 3 6
September 4 3
October 3 3
November 7 6
December 4 3
Total 47 49The nurse manager who serves on the quality team wants to discover whether the infections are in control within 95.5% confidence limits.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3636
Control Charts for Attributes: c-Chart
SolutionIf we consider each month as a sample of bad quality outcomes, for 24 samples we have a total of 96 quality defects (infections), and the average would be:
c = 96/24 = 4.0.
Since the z-value for 95.5% confidence level is equal to 2, using formulas we obtain:
.82*24424 czcUCL
.02*24424 czcLCL

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3737
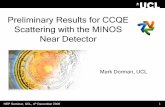
Figure 12.5 ABC Medical Center Infection Control Monitoring
UCL=8
LCL=0
Sample number
1 3 4 5 6 7 8 92 10 11 12 13 14 15 16 17 18 19 20 2221 23 24
Infe
ctio
ns
pe
r m
on
th
4c

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3838
Control Charts for Attributes: p-Chart
The proportion of defects in a process can be monitored using a p-chart that has binomial distribution as its theoretical base. The center of the p-chart represents the average for defects and LCL and UCL are calculated as:
nppzp )1( UCL
nppzp )1( LCL

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 3939
Example 12.2The indicator Family Satisfaction, which is part of the National Hospice and Palliative Care Organization’s survey, reflects the percentage of respondents who would not recommend the hospice services to others. The following data are from Holistic Care Corporation’s completed surveys from 200 families each month during a year, showing the number of respondents each month who expressed dissatisfaction with the organization’s services.
Control Charts for Attributes: p-Chart
Months Dissatisfied Patient
Families
PercentDissatisfied
January 12 0.060
February 14 0.070
March 16 0.080
April 14 0.070
May 25 0.125
June 14 0.070
July 15 0.075
August 16 0.080
September 14 0.070
October 14 0.070
November 24 0.120
December 14 0.070
Total 192 0.080
The manager in charge of quality wishes to construct a control chart for this data within 95.5% confidence intervals.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4040
Solution:First, we need to estimate the proportion mean,
Total number of quality infractions 192 192 = -------------------------------------------- = ----------- = ------- = .08 Total number of observations 12 (200) 2400
Since the z value for the 95.5% confidence level is equal to 2.0, using formulas we obtain:
Control Charts for Attributes: p-Chart
p
.118.0208. 200)08.1(08.
UCL
.042.0208. 200)08.1(08.
LCL

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4141
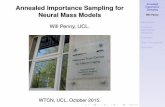
Figure 12.6 Holistic Care Corporation’s Quality Monitoring
UCL=.118
LCL=0.042
Sample number
1 3 4 5 6 7 8 92 10 11 12
Pro
po
rtio
n o
f F
am
ilie
s D
issa
tisfie
d
08.p

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4242
Figure 12.7 Use of Mean and Range Charts
UCL
LCL
ProcessMean
Range indicatorMean indicator
UCL
LCL
Stable mean, increasing range process
Increasing mean, stable range process

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4343
Mean Charts - Standard Deviation Approach.
Control Charts for Variables
zxUCL
In general the population standard is unknown, and so the average of sample means )(x
and the standard deviation of sample distribution σx
are used to construct the confidence limits as:
x
zxLCL x
where σ x ns /
.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4444
Example 12.3With a time-motion study, the IV startup process has been examined in a medical center nursing unit for five weekdays to determine whether in the future, additional training of nurses is required. Each day 9 new patients’ IV startups were observed and the measurements recorded in minutes, as shown below. Construct 99.7% (z = 3) confidence limits for IV startup times.
Control Charts for Variables: Mean Chart, σ Method
Observation Day-1 Day-2 Day-3 Day-4 Day-5
1 5.1 4.9 5.5 6.1 6.0
2 5.4 5.7 5.6 5.8 5.2
3 5.5 6.3 5.3 5.9 6.3
4 5.8 7.5 4.9 6.0 5.0
5 5.6 5.8 5.2 6.2 5.5
6 5.8 5.9 5.4 5.7 5.1
7 5.3 5.5 6.4 4.8 5.9
8 4.9 5.8 7.5 6.3 5.3
9 6.2 5.5 5.8 5.9 4.8

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4545
SolutionObservation means for each day (sample) are calculated and are shown in the last rows of the following table.
Control Charts for Variables: Mean Chart, σ Method
x
Sample Day-1 Day-2 Day-3 Day-4 Day-5
5.51 5.88 5.73 5.86 5.46
s 0.6
x = (5.51+5.88+5.73+5.86+5.46) ÷ 5 = 5.69.
with z = 3, n = 9 observations per sample (day), and s = 0.6, we obtain:
.29.6)2.0(369.5)9/6.0(369.5 UCL
.09.5)2.0(369.5)9/6.0(369.5 LCL

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4646
Mean Charts - Range Approach.
Control Charts for Variables
Another way to construct a mean chart is to use the average of sample distribution ranges,. This approach requires a factor to calculate the dispersion of the control limits.
.
RAxUCL 2
RAxUCL 2
Where A2 is a factor from Table 12.1

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4747
Table 12.1 Factors for Determining Control Limits for Mean and Range Charts (for 3-sigma or 99.7% confidence level)
Sample Sizen
Factor for Mean Chart, A2
Factors for Range Chart
LCL, D3 UCL, D4
2 1.88 0 3.27
3 1.02 0 2.57
4 0.73 0 2.28
5 0.58 0 2.11
6 0.48 0 2.00
7 0.42 0.08 1.92
8 0.37 0.14 1.86
9 0.34 0.18 1.82
10 0.31 0.22 1.78
Source: p. 143, Operations Management by Rusell & Taylor, 1995.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4848
Example 12.4During 5 weekdays, each day the number minutes spent for each of 10 patient registration operations were observed in a time study as follows:
Control Charts for Variables: Mean Chart, Range Method
Observation Day-1 Day-2 Day-3 Day-4 Day-5
1 10.2 10.3 8.9 9.5 10.5
2 9.7 10.9 10.5 9.7 10.2
3 10.3 11.1 8.9 10.5 10.3
4 8.9 8.9 10.5 9.8 10.9
5 10.5 10.5 9.8 8.9 11.1
6 9.8 9.7 10.2 10.5 9.8
7 10.0 8.9 8.9 10.4 9.5
8 11.3 10.5 10.5 8.9 9.7
9 10.7 9.8 9.7 10.5 10.5
10 9.8 11.3 10.5 9.8 8.8

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 4949
SolutionThe overall mean for each sample and range is required to apply the formulas, using the range approach. Here each day is considered as a sample. The range is calculated by taking the difference between the maximum and minimum of each sample (day). The, mean for each day also is calculated and shown as follows:
Control Charts for Variables: Mean Chart, Range Method
x
Sample Day-1 Day-2 Day-3 Day-4 Day-5
Maximum 11.3 11.3 10.5 10.5 11.1
Minimum 8.9 8.9 8.9 8.9 8.8
Range 2.4 2.4 1.6 1.6 2.3
10.12 10.19 9.84 9.85 10.13
x = (10.12+10.19+9.84+9.85+10.13) ÷ 5 = 10.03.
R = (2.4+2.4+1.6+1.6+2.3) ÷ 5 = 2.06.
UCL = 10.03 + 0.31 (2.06) = 10.67.
LCL = 10.03 – 0.31 (2.06) = 9.39.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5050
Range Charts
Control Charts for Variables
Process dispersion is best monitored by range charts. The control limits for range charts are constructed using factors. To calculate LCL, factor score D3 is obtained from a factor chart (Table 12.1) based on the number of observations in the sample distributions. Similarly, to calculate UCL, factor score D4 is required. Control limits for range charts using these factor scores are then constructed as follows:
.
RDUCL 4
RDLCL 3

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5151
Example 12.5Use the information provided in example 12.4 to construct a range chart.
Solution
For n = 10, D3 and D4 from Table 12.1 are 0.22 and 1.78, respectively. Using formulas we obtain:
Control Charts for Variables: Range Chart
UCL = 1.78 (2.06) = 3.67.
LCL = .22 (2.06) = 0.45.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5252
Investigation of Control Chart Patterns
A pattern in a control chart described by a sequence of observations that have similar characteristics is called a “run.” A simple classification of sample observations with respect to the center line that identify consecutive patterns is called an Above/Below run, or A/B run.
Up (U) and down (D) runs is another way to classify and observe patterns. To classify sample observations as U or D, the first observation is used as a reference point
.
Run-Based Pattern Tests.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5353
Figure 12.8 Identification of Runs
UCL
LCL
Sample number
1 3 4 5 6 7 8 92 10 11 12
A B B BB BA A A A A A
D D DDDDUU DU U*
Observed runs
6
5
1 2 43 65
1 2 3 54
CL

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5454
Investigation of Control Chart Patterns
Control chart patterns identified by runs require statistical testing of whether the runs are within expectations and hence the patterns are random, or beyond expectations and hence non-randomness is present. It has been shown that runs are distributed approximately normally (Stevenson, 2002, p.436) and using the z-test the significance of too few or too many observed runs can be determined as follows:
.
Run-Based Pattern Tests.
runsofdeviationdardS
runsExpectedrunsObservedz
tan
A z-value within ±2, which provides 95.5% confidence level, would show that the runs are random; however, beyond these values ≤ ±2 ≥, a non-random presence would be shown.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5555
Investigation of Control Chart Patterns
It is necessary to calculate the expected runs and their standard deviations. The formulas for expected A/B or U/D runs and their standard deviations are as follows:
.
Run-Based Pattern Tests.
12
)( / N
runE BA4
1)( /
Nrun BA
3
12)( /
NrunE DU 90
2916)( /
Nrun DU

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5656
Example 12.6Determine the presence/absence of non-randomness for the example presented in Figure 12.8, with 95.5% confidence limits. SolutionThe example has twelve observations, so N=12. Using the formulas we get:
Investigation of Control Chart Patterns
0.712
12)( / BArunE 66.175.2
4
11
4
112)( /
BArun
67.73
1)12*2()( /
DUrunE 35.181.1
90
163
90
29)12*16()( /
DUrun
60.066.1
76/
BAz
98.135.1
67.75/
DUz conclude that U/D runs exhibit randomness.
conclude that the A/B runs exhibit randomness.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5757
Investigation of Control Chart Patterns
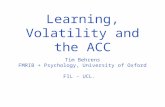
An alternative method that is often used by quality control software packages is called the “zone test.” The essence of the zone test rests on deviation from the center line by 1-sigma, 2-sigma, or 3-sigma limits. Zone C, zone B and Zone A are identified by these limits, respectively.
To create the zones, the formulas for constructing mean chart with range approach formulas are used. Those formulas, presented earlier, use A2 from Table 12.1, and the values for this table were calculated for 3-sigma levels (or 99.7% confidence level). Thus, in constructing the zones, one must reduce the A2 factor proportionately, according to the sigma level. Since A2 is designated for 3-sigma, for 2-sigma 2/3 of A2, and for 1-sigma 1/3 of A2 would be appropriate. The zone formulas can be written as:
.
Zone Tests.
RAxAZone 2
RAxBZone 22
1
RAxCZone 23
1

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5858
Figure 12.9 Zone test
UCL
LCL
Sample number
1 3 4 5 6 7 8 92 10 11 12
CL x
+1σ
-1σ
-2σ
-3σ
+2σ
+3σ RAxAZone 2
RAxBZone 22
1
RAxCZone 23
1
RAxBZone 22
1
RAxCZone 23
1
RAxAZone 2

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 5959
Process Improvement
Methods for Generating New Ideas:
The 5W2H Approach Brainstorming Nominal Group Technique Interviewing Focus Groups Quality Circles “Kaizen Teams” Benchmarking.
.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6060
Process Improvement
Tools for Investigating the Presence of Quality Problems and Their Causes
Check SheetHistogram Scatter Diagram Flow ChartCause-and-Effect Diagram Pareto Chart
.

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6161
Figure 12.10. A Check Sheet and Corresponding Histogram for Emergency Room Wait Times
WeeksWeeks
AA
Wait time to Wait time to register >10 register >10
minutesminutes
BB
Registration Registration time > 5 time > 5 minutesminutes
CC
Wait time for Wait time for MD > 15 MD > 15 minutesminutes
11 ////// ////////////
22 //////// // //
33 //////////// ////// ////////////
44 // //// //////////
55 //////////// //// //////////
0
1
2
3
4
5
6
Week 1 Week 2 Week 3 Week 4 Week 5
A
B
C

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6262
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0 5 10 15 20
Number of Infections per Month
Mo
rbid
ity
Ra
teFigure 12.11 Scatter Diagram

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6363
E.D. MDRequests X-ray
Obtain Form
Hand WritePatient
DemographicInformation
NO
YES
1
Physician Completes Form
Computer-Prepared FormAvailable?
Figure 12.12 A Flow Chart for the X-Ray Order Process in an Emergency Department

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6464
PatientWait TooLong
Equipment/MaterialRewards
People
Methods/Processes FunctionsStructure
Tests not coordinated
Delays in ordering tests
Test Errors
Boring Environment
Lack of Supplies
Lack of ER Beds
Design isnot efficient
Lack of automatedsystem
Lab/Rad./ERDepts. report to different VPs
Lack of Feedback
Lack of incentives
Too many steps
Hospital roomnot available ifadmitted
Private MDsnot on site
Lack of transporters
Figure 12.13 Cause and Effect Diagram

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6565
100%
75%
50%
25%
0Lack of info.
to patientToo many
stepsDelays intest orders
Lack of automation
Ineffective/voluminous
documentation
Other
80%
Figure 12.14 Pareto Diagram

Chapter 12: Quantitatve Chapter 12: Quantitatve Methods in Health Care Methods in Health Care ManagementManagement
Yasar A. OzcanYasar A. Ozcan 6666
The End