Case Report Treacher Collins Syndrome : An Alternative...
5
199 Treacher Collins Syndrome : An Alternative Airway Management Ruenreong Leelanukrom M.D., MPA,* Petch Wacharasint M.D.* ∫∑§—¥¬àÕ : ∑“߇≈◊Õ°¢Õß Airway Management „π Treacher Collins Syndrome √◊Ëπ‡√‘ß ≈’≈“πÿ°√¡ æ.∫., √ª¡.,* ‡æ™√ «—™√‘π∏ÿå æ.∫.* *¿“§«‘™“«‘—≠≠’«‘∑¬“ §≥–·æ∑¬»“µ√å ®ÿÓ≈ß°√≥å¡À“«‘∑¬“≈—¬ ª∑ÿ¡«—π °√ÿ߇∑æœ 10330 ·≈– mandible ‡≈Á° §≥–ºŸâ√“¬ß“π‰¥â√“¬ß“π∂÷ß°“√„à∑àÕÀ“¬ „®„πºŸâªÉ«¬ Treacher Collins syndrome ∑’Ë¡“√—∫°“√ºà“µ—¥ ‡√‘¡‚Àπ°·°â¡ ‚¥¬¥—¥·ª≈߇∑§π‘§ “two anesthesiologist” √à«¡°—∫°“√„™â soft-tip stylet „π°“√„à∑àÕÀ“¬„® Thai J Anesthesiology 2006 ; 32(3) : 199-203. *Department of Anesthesiology, Faculty of Medicine, Chulalongkorn University, Rama IV Road, Bangkok 10330, Thailand Treacher Collins syndrome ‡ªì𧫓¡º‘¥ª°µ‘·µà °”‡π‘¥∑’Ëæ∫πâÕ¬ ª√–°Õ∫¥â«¬ À“ßµ“‡©’¬ß≈ß, coloboma ¢Õß Àπ—ßµ“, µ“‡≈Á°, choanal atresia, °√–¥Ÿ° zygoma, maxilla, mandible ‡®√‘≠πâÕ¬°«à“ª°µ‘ ÀŸÀπ«° À—«„®º‘¥ª°µ‘ ·≈– Õ“®µ—«‡≈Á°°«à“ª°µ‘ °“√∑” direct laryngoscopy ·≈–„à∑àÕ À“¬„®„πºŸâªÉ«¬°≈ÿà¡π’È®–≈”∫“°°«à“ª°µ‘ ‡æ√“–°√–¥Ÿ° maxilla Introduction Treacher Collins syndrome is a rare mandi- bulofacial disorder and often requires plastic surgery to correct mandibulofacial abnormalities. This syndrome is a great challenge to the anesthesiologist because the distortions of mandibulofacial structures make airway management and tracheal intubation problematic and difficult. Case report A twenty-year-old female, weighing 45 kg, with bilateral malar hypoplasia was scheduled for malar aug- mentation with rapid prototype. She was born at term, with a birth weight of 3.8 kg after the onset of spon- taneous labour and a normal vaginal delivery. The dys- morphic features of this infant suggested a diagnosis of Treacher Collins syndrome and thereafter she was fol- lowed up by the department of plastic surgery regularly. At fifteen years of age, she was admitted to the hospital for reconstruction of left middle ear. Because of predicted difficult airway, after laryngoscopy revealed difficulty in visualizing the larynx (Cormack and Lehane grade IV) with the application of anterior external laryngeal mani- pulation, the airway management was shifted to a size-3 laryngeal mask airway (LMA TM ) under propofol anes- thesia including initial induction dose of 3 mg/kg and total dose of 4.6 mg/kg intravenously, but owing to the Case Report
Transcript of Case Report Treacher Collins Syndrome : An Alternative...

199
Treacher Collins Syndrome : An Alternative Airway Management
Ruenreong Leelanukrom M.D., MPA,*
Petch Wacharasint M.D.*
∫∑§—¥¬àÕ : ∑“߇≈◊Õ°¢Õß Airway Management „π Treacher Collins Syndrome √◊Ëπ‡√‘ß ≈’≈“πÿ°√¡ æ.∫., √ª¡.,* ‡æ™√ «—™√‘π∏ÿå æ.∫.*
*¿“§«‘™“«‘—≠≠’«‘∑¬“ §≥–·æ∑¬»“µ√å ®ÿÓ≈ß°√≥å¡À“«‘∑¬“≈—¬ ª∑ÿ¡«—π °√ÿ߇∑æœ 10330
·≈– mandible ‡≈Á° §≥–ºŸâ√“¬ß“π‰¥â√“¬ß“π∂÷ß°“√„à∑àÕÀ“¬
„®„πºŸâªÉ«¬ Treacher Collins syndrome ∑’Ë¡“√—∫°“√ºà“µ—¥
‡√‘¡‚Àπ°·°â¡ ‚¥¬¥—¥·ª≈߇∑§π‘§ “two anesthesiologist”
√à«¡°—∫°“√„™â soft-tip stylet „π°“√„à∑àÕÀ“¬„®
Thai J Anesthesiology 2006 ; 32(3) : 199-203.
*Department of Anesthesiology, Faculty of Medicine, Chulalongkorn University, Rama IV Road, Bangkok 10330, Thailand
Treacher Collins syndrome ‡ªì𧫓¡º‘¥ª°µ‘·µà
°”‡π‘¥∑’Ëæ∫πâÕ¬ ª√–°Õ∫¥â«¬ À“ßµ“‡©’¬ß≈ß, coloboma ¢Õß
Àπ—ßµ“, µ“‡≈Á°, choanal atresia, °√–¥Ÿ° zygoma, maxilla,
mandible ‡®√‘≠πâÕ¬°«à“ª°µ‘ ÀŸÀπ«° À—«„®º‘¥ª°µ‘ ·≈–
Õ“®µ—«‡≈Á°°«à“ª°µ‘ °“√∑” direct laryngoscopy ·≈–„à∑àÕ
À“¬„®„πºŸâªÉ«¬°≈ÿà¡π’È®–≈”∫“°°«à“ª°µ‘ ‡æ√“–°√–¥Ÿ° maxilla
Introduction Treacher Collins syndrome is a rare mandi-
bulofacial disorder and often requires plastic surgery to
correct mandibulofacial abnormalities. This syndrome is
a great challenge to the anesthesiologist because the
distortions of mandibulofacial structures make airway
management and tracheal intubation problematic and
difficult.
Case report A twenty-year-old female, weighing 45 kg, with
bilateral malar hypoplasia was scheduled for malar aug-
mentation with rapid prototype. She was born at term,
with a birth weight of 3.8 kg after the onset of spon-
taneous labour and a normal vaginal delivery. The dys-
morphic features of this infant suggested a diagnosis of
Treacher Collins syndrome and thereafter she was fol-
lowed up by the department of plastic surgery regularly.
At fifteen years of age, she was admitted to the hospital
for reconstruction of left middle ear. Because of predicted
difficult airway, after laryngoscopy revealed difficulty in
visualizing the larynx (Cormack and Lehane grade IV)
with the application of anterior external laryngeal mani-
pulation, the airway management was shifted to a size-3
laryngeal mask airway (LMATM) under propofol anes-
thesia including initial induction dose of 3 mg/kg and
total dose of 4.6 mg/kg intravenously, but owing to the
Case Report

ªï∑’Ë 32 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2549 «‘—≠≠’“√
200
201Thai Journal of AnesthesiologyVol. 32, No. 3, July-September 2006
inadequate depth of anesthesia, laryngospasm had oc-
curred. However, it was successfully treated with intra-
venous succinylcholine 25 mg (1.6 mg/kg). Spontaneous
ventilation became more active and was clinically satis-
factory ; both regular rhythmic of ETCO2 and oxygen
saturation curve and movement of the anesthesia bag was
observed. At the end of the surgery, the laryngeal mask
was removed by the patient’ s herself in the operating
room without complication. On the day of discharge, she
was active, cooperate and no complication was detected.
At sixteen years of age, she was admitted to the
hospital again twice for undergoing multiple sliding
genioplasty and zygomatic osteotomy with iliac bone
graft. Because of the difficulty to visualize the larynx
history, both anesthetic techniques were spontaneous
ventilation and fiberoptic bronchoscope assisted intuba-
tion after inhalation induction of sevoflurane with nitrous
oxide in oxygen. There was no complication of these two
previous anesthesia.
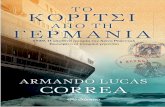
On examination, the patient showed several
dysmorphic features affecting the face. The combination
of microstomia, micrognathia, malar and mandibular
hypoplasia, and auricular defect was presented (Figure 1).
The results of preoperative laboratory investigations were
unremarkable. On the operative day, to minimize the risk
of airway obstruction, no premedication drug was given
before induction. A flexible fiberoptic bronchoscope
(FOB ; Olympus LF-2) was readily available. Standard
monitors including non-invasive blood pressure, electro-
cardiogram, pulse oximetry were applied. Venous access
was not difficult and a 18-G intravenous catheter was
sited in the dorsum of left hand. After preoxygenation
with 100% oxygen, anesthesia was induced with sevo-
flurane and spontaneous ventilation was continuously
maintained with sevoflurane titration up to 8%. As the
level of anesthesia deepened, mask ventilation became
difficult because of micrognathia, however, the 100%
peripheral oxygen saturation (SpO2) was well maintained
from her spontaneous ventilation. After the first laryn-
goscopy revealed difficulty in visualizing the larynx
(Cormack and Lehane grade IV) with the application of
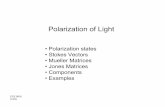
anterior external laryngeal manipulation, the second
attempted direct laryngoscopy was done by more ex-
perienced anesthesiologist and the “two anesthesiologist
technique” was performed by one manipulated the
laryngoscope and larynx and the other inserted the tube
(Figure 2). At this time, the epiglottis was visualized
and revealed the larynx grade I. However, due to mi-
Figure 1 The typical appearance of treacher Collins syn- drome : antimongoloid biquity of the palpebreal fissures, microstomia, microtia, micrognathia, cho- anal atresia, hypoplasia of the zygoma, maxillary, and mandibular bones
Figure 2 The modified “two anesthesiologist technique” was illustrated by one anesthesiologist mani- pulated the laryngscope and larynx and the other one inerted thesoft tip stylet

ªï∑’Ë 32 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2549 «‘—≠≠’“√
200
201Thai Journal of AnesthesiologyVol. 32, No. 3, July-September 2006
crostomia appearance and anterior location of the larynx,
the tracheal tube was difficult to pass into the oral
cavity. This problem was solved successfully by using
the soft-tip stylet (Rusch no.3) inserted into the trachea
under direct visualization (Figure 3). Then, the Mallin-
ckrodt tracheal tube (PVC, 7.0 mm ID, 9.6 mm OD)
Discussion Treacher Collins syndrome was characterized by
Treacher Collins.1 This syndrome, which is also referred
to as mandibulofacial dysostosis, consists of down-
slanting palpebral fissures, colobomata of the lower
eyelid, scantly lower eyelashes, malar hypoplasia, and
micro-or retrognathia. There is a palatal cleft in 35% of
patients, and additional 30 to 40% have congenital
palatopharyngeal incompetence.2,3 Ear anomalies are
common and vary from minor malformation to severe
microtia which the operation is needed as described in
this case. Hearing loss is common, and can occur secon-
dary to atresia of the auditory canals or ossicular
malformation of the middle ear. The most life-threatening
concomitant morbidities in patients with Treacher Collins
syndrome are respiratory problems and respiratory
failure. Initially, there conditions were thought to be
secondary to glossoptosis. More recently, it has been
shown that the anatomy of the airway plays a major
role in determining the risk of airway compromise.
Patients with Treacher Collins syndrome might have
basicranial kyphosis, narrowing of the pharynx, and
severe microretrognathia with deficient ramal height.4,5
Patient with this syndrome may present anesthetic
problems involving difficulties in intubation and mask
fit. In addition, the space in the oral cavity that needed
to be displaced during laryngoscopy was diminished.6
Various techniques of airway management in Treacher
Collins syndrome were reported.7-10 But every approach
has its drawbacks. Bahk et al. reported a four-year-old
patient with Treacher Collins syndrome. The difficult
airway was managed by fibreoptic assisted intubation
through LMA.8 They did not attempt direct laryngoscopy
before inserting the LMA, so we did not know whether
intubation via direct laryngoscope was possible. Inser-
tion of LMA with owing to the light level of anes-
thesia, laryngospasm, coughing, or breath holding are
the potential complications. There have been several
reports of failure to correctly place the LMA and ven-
Figure 3 A soft-tip stylet (Rusch no.3)
was railroaded and advanced into the trachea. Finally,
the soft-tip stylet was removed. Spontaneous breathing
was maintained during airway procedure. Fiberoptic
laryngoscopy was not performed. Anesthesia was main-
tained with nitrous oxide 66% in oxygen and isoflurane
titration to clinical endpoints of heart rate and blood
pressure. Intravenous morphine was administered for
intraoperative and postoperative analgesia. The muscle
relaxant for maintenance was atracurium 25 mg intra-
venously. The anesthesia and surgery were uneventful
and lasted 360 min. There were no signs or symptoms
of upper airway obstruction observed. The tracheal tube
was removed in the operating room when the patient
demonstrated spontaneous eye opening, purposeful mo-
vement and adequate spontaneous ventilation. The patient
was transferred to the recovery unit and discharged
home 2 days later with good health.

ªï∑’Ë 32 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2549 «‘—≠≠’“√
202
203Thai Journal of AnesthesiologyVol. 32, No. 3, July-September 2006
tilation through it after induction of general anesthesia.11
The original “two anesthesiologist” technique
described that one anesthesiologist manipulated the
laryngoscope with one hand and applied pressure on the
larynx with the other hand. In this way, optimum pres-
sure can be applied to bring the larynx into view. The
other anesthesiologist inserted the tracheal tube.12 How-
ever, microstomia in this patient limited the oral space
for tracheal tube insertion. We solved this problem by
inserting a soft-tip stylet (Rusch 3) into the trachea as
a Gum Elastic Bougie.TM The tracheal tube was then
loaded and advanced into the trachea. The soft-tip stylet
was smaller and hence it was easier to insert into the
trachea than tracheal tube with minimal tissue trauma.
This technique was useful for patient who had difficulty
in visualization of the larynx with microstomia.
In conclusion, Treacher Collins syndrome is a
syndrome associated with difficult mask ventilation and
difficult intubation. The anesthetic and airway manage-
ment should be prepared promptly for difficult airway.
However, when fibreoptic bronchoscope, laryngeal mask
airway or any invasive airway procedure are not avai-
lable, the direct laryngoscopy with the modified “two
anesthesiologist technique” with the soft-tip stylet as-
sisted tracheal intubation is a useful alternative airway
management.
References
1. Treacher CE. Case with symmetrical congenital notches in the outer part of each lid and defective development of the malar bones. Trans Opthalmol Soc UK 1900 ; 20 : 190-2.
2. Gorlin RJ, Toriello HV, Cohen MM Jr. Hereditary Hearing Loss and Its Syndromes. New York : Oxford University Press 1995 ; 62-5.
3. Dixon MJ. Treacher Collins syndrome. Hum Mol genet 1996 ; 5 : 1391-6.
4. Shapira J, Gleicher H, Moskovitz M, Peretz B. Respiratory arrest in Treacher Collins syndrome : Implications for dental management : Case report. Pediatr Dent 1996 ; 18 : 242-4.
5. Arvystas M, Shprintzen RJ. Craniofacial morphology in Treacher Collins syndrome. Cleft Palate Craniofac J 1991 ; 28 : 226-31.
6. Berry FA. Anesthesia for the child with a difficult airway. In : Berry FA, ed. Anesthetic management of difficult and routine pediatric patients. 2nd ed. Churchill Livingstone, New York 1990 : 142-67.
7. Miyabe M, Dohi S, Homma E. Tracheal intubation in an infant with Treacher-Collins syndrome-pulling out the tongue by a forceps (letter). Anesthesiology 1985 ; 62 : 213-4.
8. Bahk JH, Han SM, Kim SD. Management of difficult airways with a laryngeal mask airway under propofol anesthesia. Paediatr Anaesth 1999 ; 9 : 163-6.
9. Bahk JH, Kim JK, Kim CS. Use of the laryngeal mask airway to preoxygenate in a pediatric patient with Treacher-Collins syndrome. Paediatr Anaesth 1998 ; 8 : 273-6.
10. Bucx MJL, Grolman W, Kruisinga FH, et al. The prolonged use of the laryngeal mask airway in a neonate with airway obstruction and Treacher Collins syndrome. Case report. Paediatr Anaesth 2003 ; 13 : 530-3.
11. Benumof JL. The laryngeal mask airway and the ASA difficult airway algorithm. Anesthesiology 1996 ; 84 : 686-9.
12. Brown TCK, Fisk GC. Anaesthesia for Children, 2nd edn. Oxford: Blackwell Scientific Publications, 1992 ; 116-7.

ªï∑’Ë 32 ©∫—∫∑’Ë 3 °√°Æ“§¡-°—𬓬π 2549 «‘—≠≠’“√
202
203Thai Journal of AnesthesiologyVol. 32, No. 3, July-September 2006
Treacher Collins Syndrome : An Alternative Airway Management
Abstract
Treacher Collins stndrome is a rare congenital disorder characterized by antimongoloid obiquity of the
palpebral fissures, coloboma, microphthalmia, choanal atresia, hypoplasia of the zygoma, maxillary and mandibular
bones, deafness, congenital heart defects, and occasionally dwarfism. The anesthetic challenge is difficult airway
from hypoplasia of maxillary, and mandibular bones which make direct visualization of the larynx and intubation
difficult. We present a case of this syndrome who was successfully intubated with the modified “two anesthesiologist
technique” with soft-tip stylet assisted tracheal intubation
Keywords : Treacher Collins syndrome, anesthesia, two anesthesiologist technique, soft-tip stylet assisted tracheal
intubation