Cardiovascular β-adrenergic signalingliu.diva-portal.org/smash/get/diva2:395205/FULLTEXT01.pdf2.1...
60
Linköping Studies in Science and Technology. Dissertations No. 1330 Cardiovascular β-adrenergic signaling Maturation and programming effects of hypoxia in a chicken model Isa Lindgren Department of Physics, Chemistry and Biology Linköping University Linköping 2010
Transcript of Cardiovascular β-adrenergic signalingliu.diva-portal.org/smash/get/diva2:395205/FULLTEXT01.pdf2.1...

Linköping Studies in Science and Technology.
Dissertations No. 1330
Cardiovascular β-adrenergic
signaling
Maturation and programming effects of hypoxia in a
chicken model
Isa Lindgren
Department of Physics, Chemistry and Biology
Linköping University
Linköping 2010

Front cover illustrations
Top: Model of a G-protein coupled receptor
Bottom: 19 day-old broiler chicken embryo in ovo. Photo: Isa Lindgren
Copyright © Isa Lindgren 2010, unless otherwise stated
Lindgren, I
Cardiovascular β-adrenergic signaling - Maturation and programming effects of hypoxia in a
chicken model
Available from Linköping University Electronic Press
http://www.ep.liu.se/
ISBN: 978-91-7393-352-0
ISSN 0345-7524
Published articles and figures have been reprinted with the permission of the copyright holder.
Printed by LiU-Tryck, Linköping, Sweden 2010
During the course of the research underlying this thesis, Isa Lindgren was enrolled in Forum
Scientium, a multidisciplinary graduate school at Linköping University, Sweden.
Linköping Studies in Science and Technology. Dissertations No. 1330

“The heart, a center for attraction, Has domination of the whole;
Its bulging muscles are in action From early start till final toll”
From “The Avian Embryo” (1960)
by Alexis Romanoff
“The heart has its reasons which reason knows nothing about” Blaise Pascal


i
ABSTRACT
Despite the importance of β-adrenergic receptors (βARs) in cardiovascular disease, not
much is known about how prenatal hypoxia effects βAR signaling in the postnatal animal.
Thus, the aim of this thesis was to characterize the pre- and postnatal maturation of the
cardiovascular βARs and the effects of chronic prenatal hypoxia on βAR signaling in the
embryo and adult animal using the chicken as experimental model.
βARs belong to the seven-transmembrane receptor family of G-protein coupled
receptors and are crucial for cardiovascular development, growth and regulation. In the
cardiovascular system there are two dominant subtypes, β1AR and β2AR, whose main
ligands are the biogenic catecholamines epinephrine and norepinephrine. When
stimulated, βARs primarily couple to the stimulatory G-protein (Gs) that stimulates
adenylyl cyclase to convert ATP to cAMP. cAMP increases ino- and chronotropy of the
heart and causes relaxation of blood vessels. β2ARs also have the ability to switch to
inhibitory G-protein (Gi) signaling that decreases the cAMP production. To protect the
cardiovascular system from overstimulation, the βARs desensitize and downregulate in
the case of prolonged elevation of catecholamines. This blunts the cardiovascular
response and the mechanisms behind desensitization/downregulation, including the
β2AR switch to Gi signaling, are closely linked to cardiovascular disease and are of
immense importance in medical therapeutics.
Hypoxic stress releases catecholamines and thereby triggers βAR responses and
desensitization/downregulation mechanisms. Hypoxia quite commonly occurs in utero
and it is well known that prenatal insults, like malnutrition or hypoxia, are coupled to an
increased risk of developing adult cardiovascular disease. This is referred to as
developmental programming and constitutes an important and modern field of research.
In this thesis, I show that; 1) the developmental trajectory for organ growth,
especially the heart, is affected by hypoxia, 2) chronic prenatal hypoxia causes cardiac
embryonic βAR sensitization, but causes desensitization postnatally suggesting that
there is a hypoxia-induced “programming” effect on adult β-adrenoceptor function, 3) the
adult βAR desensitization following prenatal hypoxia is linked to a decrease in
β1AR/β2AR ratio, a decrease in cAMP following βAR stimulation with isoproterenol and
an increase in Gαs, 4) the chorioallantoic (CA) membrane arteries display hypoxic
vasoconstriction, but lack α-adrenergic reactivity and 5) hypotension of the chronically
hypoxic chicken embryo is linked to a potent βAR relaxation of the CA vasculature and
an increased βAR sensitivity of the systemic arteries with no changes in heart rate.

ii
In conclusion, chronic prenatal hypoxia causes growth restriction, re-allocation
and has programming effects on the βAR system in the adult. The latter indicates that
the βAR system is an important factor in studying hypoxic developmental programming
of adult cardiovascular disease.

iii
POPULÄRVETENSKAPLIG SAMMANFATTNING
Trots dagens kunskap om adrenalinreceptorer och deras djupa involvering i
hjärtkärlsjukdom känner vi inte till mycket om hur syrebrist (hypoxi) i fosterstadiet
påverkar adrenalinreceptorsignalleringen i den vuxna individens hjärtkärlsystem. Därför
är målet med denna avhandling att karaktärisera mognaden av adrenalinreceptorer i
hjärtkärlsystemet före och efter födseln, samt att undersöka effekten av kronisk
fosterhypoxi på adrenalinreceptorsignallering i både fostret och den vuxna individen.
Detta gör vi genom att använda oss av kyckling som modelldjur.
β-adrenoreceptorer (βARr) utgör en av grupperna av adrenalinreceptorer. Enkelt
uttryckt så är de proteiner insprängda i cellens membran med en del utanför cellen och
en del inuti. De plockar upp signaler på cellens utsida och översätter dem till signaler
inne i cellen genom att koppla till G-proteiner på cellens insida. De två dominerande
subtyperna, β1AR och β2AR, är centrala i hjärtkärlsystemets utveckling, tillväxt och
reglering och de stimuleras främst av adrenalin och noradrenalin. När adrenalin eller
noradrenalin fäster till receptorns yttre del skickas en signal in i cellerna som ökar
hjärtats slagfrekvens och kontraktionskraft, samt utvidgar blodkärlen. För att skydda
hjärtkärlsystemet från överstimulering (t.ex. vid långdragen stress med höga halter
adrenalin) finns det mekanismer för desensitisering och nedreglering av receptorerna.
Detta gör att hjärtat reagerar sämre på adrenalin/noradrenalinstimulering. Mekanismerna
bakom desensitisering/nedreglering är tätt länkade till hjärtkärlsjukdom och är därför
viktiga måltavlor för läkemedel.
Hypoxi är en sorts stress och utlöser därmed utsöndring av adrenalin och
noradrenalin och triggar både ökad hjärtkärlrespons och desensitiserings/nedreglerings-
mekanismer. Att foster utsätts för hypoxi genom tryck på navelsträngen eller nedsatt
funktion av moderkakan är inte helt ovanligt och det är väl känt att onormal stress under
fosterstadiet (t.ex. undernäring eller hypoxi) är kopplat till ökade risker att utveckla
hjärtkärlsjukdom i vuxen ålder och detta kallas för utvecklingsprogrammering. Effekterna
av hypoxi under utvecklingen utgör därför ett viktigt och modernt forskningsområde.
I denna avhandling visar jag att kronisk fosterhypoxi minskar födelsevikten och
ökar βAR-känsligheten i själva fostret, men minskar adrenalinkänsligheten i den vuxna
individen, något som återfinns hos hjärtsjuka personer. Dessa resultat visar på att
fosterhypoxi har en ”programmerande” effekt på vuxen βAR-funktion. Fosterhypoxi ökar
också halten av stimulerande G-protein, men ändrar β1AR/β2AR-proportionerna till fördel
för β2AR i det vuxna hjärtat. Dessa förändringar liknar också de observerade i

iv
hjärtkärlsjukdom och ger ytterligare en fingervisning om att fosterhypoxi leder
till ”programmering” av βAR-systemet. Utöver detta visar jag att choriallantois-
membranets (CAMs) blodkärl (motsvarande moderkakans blodkärl i däggdjur) helt
saknar klassisk adrenalin-inducerad sammandragning och reagerar istället uteslutande
på adrenalin genom utvidgning. Direkt hypoxi kring det isolerade kärlet orsakar däremot
sammandragning. Jag presenterar också bevis för att hjärtfrekvensen hos embryot inte
ändras med kronisk fosterhypoxi och att det observerade blodtrycksfallet hos hypoxiska
kycklingembryon med stor sannolikhet beror på βAR-utvidgningen av CAMs blodkärl.
Den viktigaste slutsatsen från vår studie är att förändringen av vuxen βAR-funktion
genom fosterhypoxi påminner om förändringarna vi ser i hjärtkärlsjukdom. Därmed
kopplas förändringar av βAR-systemet som en möjlig mekanism bakom utvecklings-
programmering av vuxen hjärtkärlsjukdom.

v
PAPERS INCLUDED IN THESIS
PAPER I Lindgren I, Altimiras J . Sensitivity of organ growth to chronically low oxygen levels during incubation in red junglefowl and domesticated chicken breeds. Submitted Student’s contribution: Isa Lindgren carried out the experiments, analyzed the results and contributed to the writing of the paper. PAPER II Lindgren I, Altimiras J. Chronic prenatal hypoxia sensitizes β-adrenoceptors in the embryonic heart but causes postnatal desensitization. Am J Physiol Regul Integr Comp Physiol 2009;297:R258-264. Student’s contribution: Isa Lindgren designed the study and formulated the questions together with Jordi Altimiras. IL executed all experiments, analyzed the data and wrote the paper with some help from Jordi Altimiras. PAPER III Lindgren I . Postnatal β-adrenergic desensitization caused by chronic prenatal hypoxia is linked to an increase in Gαs and decreased β1AR/β2AR ratio. Manuscript Student’s contribution: Isa Lindgren designed the study, carried out the experiments with the help from two students, analyzed the data and wrote the paper guided by Jordi Altimiras. PAPER IV Lindgren I, Zoer B, Altimiras J, Villamor E. Reactivity of chicken chorioallantoic arteries, avian homologue of human fetoplacental arteries. Submitted Student’s contribution: Isa Lindgren executed all experiments with the help of Bea Zoer. IL analyzed all data and contributed to the written paper equally together with the other authors. Experiments were mainly planned and supervised by Eduardo Villamor. PAPER V Lindgren I, Crossley D, Villamor E, Altimiras J. Hypotension in the chronic hypoxic chicken embryo origins in a potent β-adrenergic response of the chorioallantoic arteries and not bradycardia. Submitted Student’s contribution: Isa Lindgren executed all experiments except the cannulation heart rate and blood pressure measurements that were done by Dane Crossley. IL analyzed the data and wrote the paper under main supervision of Jordi Altimiras and partly Eduardo Villamor.

vi

vii
TABLE OF CONTENTS ABSTRACT ................................................................................................................. i
POPULÄRVETENSKAPLIG SAMMANFATTNING .................................................... ii
PAPERS INCLUDED IN THESIS ................................................................................ v
1 G-PROTEIN COUPLED RECEPTORS ....................................................................... 1
1.1 GPCR structure .................................................................................................... 1
1.2 G-proteins ............................................................................................................. 1
1.3 The GPCR signaling cascade ............................................................................. 2
1.4 β-adrenergic receptors ........................................................................................ 5
2 CARDIOVASCULAR β-ADRENOCEPTORS IN HEALTH
AND DISEASE ............................................................................................................ 7
2.1 βAR signaling in the cardiovascular system .................................................... 7
2.2 β2AR cross-signaling and compartmentation ................................................... 9
2.3 βARs in cardiovascular disease ......................................................................... 11
3 DEVELOPMENTAL PROGRAMMING ........................................................................ 13
3.1 Phenotypic plasticity and developmental “windows” ...................................... 13
3.2 Developmental Origins of Health and Disease .................................................. 14
3.3 The beginning - “Barker’s hypothesis” and
the “thrifty phenotype” ....................................................................................... 15
3.4 The “Predictive Adaptive Response” theory .................................................... 16
3.5 Criticism of PAR ................................................................................................... 18
3.6 My definition of developmental programming ................................................... 19
4 HYPOXIC CARDIOVASCULAR REGULATION AND THE ROLE OF β-ADRENERGIC
RECEPTORS .............................................................................................................. 21
4.1 Adult and fetal cardiovascular regulation during hypoxia................................ 21
4.2 Effect of hypoxia on the βAR system ................................................................ 24

viii
5 SUMMARY OF PAPERS ............................................................................................ 27
5.1 Summary Paper I ................................................................................................. 27
5.2 Summary Paper II ................................................................................................. 28
5.3 Summary Paper III ............................................................................................... 28
5.4 Summary Paper IV ............................................................................................... 29
5.5 Summary Paper V ................................................................................................ 30
6 DISCUSSION ............................................................................................................... 31
6.1 Comments on the experimental model .............................................................. 31
6.2 Developmental programming (Papers II and III) ............................................... 31
6.3 Growth and allocation (Paper I) .......................................................................... 32
6.4 Vascular reactivity and cardiovascular response to chronic hypoxia in the
chicken embryo (Papers IV and V) ........................................................................... 33
6.5 Conclusions ......................................................................................................... 34
ACKNOWLEDGEMENTS ...................................................................................................... 37
REFERENCES ....................................................................................................................... 41

1
1 G-PROTEIN COUPLED RECEPTORS
The key to regulate cell function globally is cell-to-cell communication. This relies on one
cell releasing the transmitter substance and another being specialized for receiving it.
Depending on the nature of the ligand, the signal transduction can take two main
avenues; if the ligand is lipophilic and able to diffuse over the cell membrane, it can
reach cytosolic or nuclear receptors inside the cell. If it is hydrophilic, it could have an
active transporter across the membrane, but more likely it will have its receptor on the
cell surface, i.e. a membrane receptor. Membrane receptors are divided into three main
classes; 1) Ligand gated ion-channels, 2) Enzyme-linked receptors and 3) G-protein
coupled receptors (GPCRs). The GPCR family is the largest of the three (52) and
encompasses over 1000 known receptors (43).
1.1 GPCR structure
The ubiquitous GPCR secondary and tertiary structure is dominated by seven
transmembrane (7TM) α-helices, connected by extra- and intracellular loops, and
arranged in a bundle to create a center core (Fig.1). Clearly, the 7TM regions are
hydrophobic since they span the cell membrane, but the core they create between them
is more or less hydrophilic and is important for ligand binding and the subsequent
conformational change that the binding of the ligand causes (52). TM helix 3 is
suggested to be the main ligand binding site, while TM helix 5 and 6 are involved in
initiating the intracellular signaling cascade (47). The whole structure is built up by a
single amino acid chain with an extracellular N-terminal and an intracellular C-terminal.
While the α-helices are quite homologous, the terminals and loops are subjected to the
largest variations between different GPCRs, thus being involved in giving the receptor its
unique identity and ligand specificity (43, 52). The variations in the intracellular loops and
C-terminus determine G-protein specificity (99) and are the regions of the receptor that
are exposed to intracellular kinases and are therefore important phosphorylation sites.
1.2 G-proteins
The proteins that gave GPCRs their name and are responsible for the first step in the
intracellular signaling cascade are called Guanine nucleotide-binding proteins, or just G-
proteins, and are, just like the GPCRs, highly conserved through evolution. They are
trimeric proteins belonging to the GTPase enzyme group and act as ON/OFF switches

2
regulating cell processes as disparate as sensory perception and cell differentiation (95).
The three subunits that make up a G-protein are named with greek letters as α, β and γ,
with the β and γ being tightly bound to form a βγ complex that is dissociated from the α
subunit (Gα) at the time of activation (70). As hinted by the name, the G-proteins bind
guanine nucleotides and are activated when GTP binds and inactivated by the hydrolysis
of GTP to GDP due to the intrinsic enzymatic activity of the protein (55). The hydrolysis
of GTP is irreversible and to activate the G-protein again, GDP has to be replaced with
GTP by the help of guanine nucleotide-exchange factors, or GEFs (95). The binding site
for the guanine nucleotides are located in the Gα and because of its enzymatic activity it
was long thought that it was only the Gα that was involved in transmitting the signal. We
now know that the βγ complex has its own signaling pathways and that it evokes other
types of responses than the α-mediated signal (63, 85).
The G-protein is mostly referred to by its α-subunit and four different subfamilies of
Gα proteins are known; Gαs (stimulatory), Gαi (inhibitory), Gαq and Gα12 (70). As previously
mentioned, all Gα subunits bind guanine nucleotides to regulate their activity. This is not
to be confused with that Gαs and Gαi are both acting in the pathway where the second
messenger cyclic adenosine monophosphate (cAMP) is generated through conversion
of ATP by adenylyl cyclase (AC). As their names indicate, Gαs stimulates the cAMP
production, while Gαi inhibits it. Gαq acts via phospholipase C to generate the second
messengers IP3 and DAG, while Gα12 couple to GEFs to remodel and regulate the
cellular cytoskeleton (63). The Gαq and Gα12 pathways are however beyond the scope of
this thesis and from hereon only Gαs and Gαi will be considered.
1.3 The GPCR signaling cascade
A ligand can have many different effects on a GPCR depending on what kind of ligand
and what type of GPCR. One thing that all ligand-bound GPCRs do have in common is
that the 7TM regions of the receptor will change their conformation upon agonist
stimulation (70). The conformation of the agonist-bound receptor aids the translocation
of a G-protein to the cell membrane. Once the G-protein/GPCR interaction is established,
the receptor acts as a GEF to exchange the bound GDP to a GTP in the Gα subunit,
thereby activating the Gα, changing its conformation and causing the dissociation of the
βγ complex (63) (Fig. 1). The enzymatic activity of the Gα then hydrolyses GTP to GDP
and the Gα thereby regains its affinity for the βγ complex and re-associates and the

3
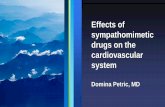
Figure 1. Illustration of the classical G αs-mediated GPCR signaling pathway. Agonist
stimulation of the GPCR leads to a conformation change that allows intracellular interaction with
the trimeric G-protein. The interaction leads to an exchange of GDP to GTP in the Gαs subunit,
making it active and dissociating the G-protein into a free Gαs and a βγ complex. The βγ complex
have disparate pathways for signaling and goes on further to give a cell response, while the
activated Gαs stimulates adenylyl cyclase (AC) to convert ATP cAMP. The cAMP in turn acts like
the second messenger and activates kinases like G-protein coupled receptor kinase (GRK) and
protein kinase A (PKA). The activated kinases phosphorylate different targets to give a cell
response or to desensitize the receptor to further signaling.
effector signal is turned off. Thus, it has been proposed that the duration of the receptor
signal is dependent on the lifetime of the GTP-bound Gα (63).
As previously mentioned, the activated Gαs stimulates AC to catalyze the
conversion of ATP to cAMP. The second messenger cAMP has many targets in the cell,
but in the classical cAMP-mediated pathway the most important proteins it
phosphorylates (and thereby activates) are protein kinase A (PKA) and G-protein
AC
Gas
ß?
cAMP ATP
DissociationGas
ß?
GDP
GTP
PKA(Active)
GRK(Active)
GPCR phosphorylation
CELL RESPONSE
Agonist
AC
Gas
ß?
ß?
cAMP ATP
DissociationGas
ß?
GDP
Gas
ß?
ß?
GDP
GTP
PKA(Active)
GRK(Active)
GPCR phosphorylation
CELL RESPONSE
Agonist

4
coupled receptor kinases (GRKs) (Fig. 2). Once activated, PKA also has many
phosphorylation targets that eventually lead to either a cellular response or an
interruption of the signal, while GRKs are specifically phosphorylating GPCRs to cease
the signal. The phosphorylation decouples the G-protein from its receptor, serving as a
negative-feedback loop (70). The action of making the receptor irresponsive to further
stimulation on the level of G-protein coupling, despite the presence of agonist, is known
as desensitization and is one of many means for fine-tuning and regulation of the signal
and protecting the cell from overstimulation (78). Being quite promiscuous, the activated
PKA may phosphorylate other GPCRs not involved in the initiation of the signal, thus
desensitizing other pathways not related to the one where the PKA activation originated.
This is called heterologous desensitization. Conversely, the GPCR-specific
desensitization carried out by GRKs is called homologous desensitization and mostly
regulates the same pathway it was activated by (70).
Following the phosphorylation-mediated uncoupling of the G-protein from its
GPCR, the fate of the receptor is to go down one of many routes, most of them
intracellular after the receptor has been sequestered from the cell surface. The receptor
can be sequestrated (or internalized) in different ways including clathrin-coated pits and
caveolae (56, 78). The internalization process is in most cases closely related to an
association of the receptor with a group of proteins called β-arrestins. β-arrestins interact
with the phosphorylated parts of the receptor and further block the site for G-protein
binding. In addition to the direct, steric desensitizing action, β-arrestin is involved in
receptor trafficking via clathrin-coated vesicles (70) (Fig. 2). Recently, β-arrestin has also
been demonstrated to be involved in independent signaling through the mitogen-
activated protein kinase (MAPK) pathway by acting as a scaffold for additional proteins
and also in recruiting phosphodiesterases to the cell membrane to speed up the
degradation of cAMP (56). Mediated by β-arrestin or not, once the receptor is in an
intracellular endosome it can either be de-phosphorylated (and thus resensitized) by
phosphatases and brought back to the cell surface for further signaling, or it can simply
be degraded (70) (Fig. 2). Through the MAPK pathway, the protein expression of the
receptor can be regulated and together with endosomal degradation of the receptor
protein, this longer-term regulation of receptor availability is commonly referred to as
receptor downregulation.

5
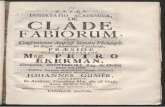
Figure 2. GPCR trafficking. The kinases activated in the GPCR signaling pathway (e.g. GRK)
phosphorylate the intracellular regions of the receptor that are involved in G-protein coupling. The
receptor phosphorylation per se leads to desensitization, but additional desensitizing steps are
possible. This figure depicts how β-arrestin (βArr) associates with the phosphorylated part of the
receptor, further blocking any G-protein interaction. Additionally, the β-arrestin is involved in
recruiting the receptor into clathrin-coated invaginations, leading to sequestration of the receptor
from the cell surface by endocytosis. Once in the endosome, the receptor can either be de-
phosphorylated by phosphatase (P-ase) and returned to the surface for further signaling, or
degraded and thus permanently removed from the signaling cycle.
1.4 β-adrenergic receptors
βARs are a group of GPCRs whose ligands are biogenic amines (primarily the
catecholamines epinephrine and norepinephrine) and there is a plethora of studies of
their structure, signaling pathways and functional regulation. Together with the closely
related α-adrenergic receptor group, they are present in most tissues of the body and
ßArr
Agonist
GRK(Active)
P P Phosphorylation
ßArr
PP
Clathrin-coated
vesicle
Endosome a) Degradation
b) De-phosphorylation
P-aseP P
Receptor recycling
ßArr
Agonist
GRK(Active)
P PP P Phosphorylation
ßArr
PP
PP
Clathrin-coated
vesicle
Endosome a) Degradation
b) De-phosphorylation
P-aseP PP P
Receptor recycling

6
are some of the most studied GPCRs to this date. In fact, the β2AR subtype was one of
the first GPCRs to be crystallized to enable structure determination of the intact receptor,
something that is hard to obtain in GPCRs because of their structural instability in vitro
(74).
There are three known subtypes of βAR receptors; β1, β2 and β3 (48, 89). Although
they can be found throughout the body, β1ARs are found in abundance in the heart,
while β2ARs are classically identified in for example blood vessels and airway smooth
muscle (48). β3ARs are predominantly found in adipose tissue and because their role in
the cardiovascular system is not yet fully understod, it will not be discussed further in this
thesis.
All βARs signal mainly through Gαs. However, β2ARs also have the ability to signal
through Gαi , something that will be discussed in the next chapter. βARs follow the
classical GPCR/Gαs/cAMP pathway and thereby activate both PKA and GRKs. More
specifically, βARs activate GRK2 that is also called β-adrenoceptor kinase 1 (βARK1) due
to its specificity to βARs (89). The targets of the activated PKA include proteins like
phospholamban (PLB) or receptor operated calcium channels (ROCCs) that will result in
an increase in intracellular Ca2+ (89). The mechanisms and cellular response to βAR
stimulation are however different in different cell types and will be discussed further in
the next chapter.

7
2 CARDIOVASCULAR β-ADRENOCEPTORS IN
HEALTH AND DISEASE
Although βARs are widespread throughout our bodies and essential in many
physiological processes, they are dominant in the cardiovascular system. Their
significance throughout the lifespan of an organism is demonstrated all the way from
their early embryonic presence when knocking out the βARs is lethal (72), to their
regulation of adult cardiovascular function and involvement in cardiovascular disease
and senescence (84, 96).
2.1 βAR signaling in the cardiovascular system
As previously mentioned, βARs are GPCRs that signal through Gαs, resulting in an
increase of cytosolic cAMP and subsequent activation of kinases like PKA. This same
pathway increases contractility in cardiac muscle and decreases contractility (causes
relaxation) in vascular smooth muscle.
In the heart, one possible target for the activated PKA are the L-type calcium
channels. “L” stands for “Long-lasting” and is based on the fact that the channel is open
for a relatively long time. The long refractory time is one of the features contributing to
the unique characteristics of the heart muscle – the action potentials last longer and
prevent arrhythmias and re-entry of action potentials to enable the cyclic synchronization
of all cardiac cells (90). When PKA phosphorylates the L-type calcium channel, the
channel conductance is not increased, but the mean opening time is, meaning that the
probability for more channels to be open at the same time increases and thereby also
increases the inward calcium current (90). The increased intracellular Ca2+ triggers a
calcium-induced calcium release from ryanodine receptors (RyRs) in the sarcoplasmic
reticulum (SR) and the muscle contracts (53). At the same time, PKA can also
phosphorylate RyRs directly to increase their opening probability (58) (Fig.3). Another
primary target for PKA is PLB in the SR membrane. In its unphosphorylated state, PLB
inhibits the sarco/endoplasmatic reticulum calcium-ATPase (SERCA), a “pump” in the
SR membrane that is responsible for the reuptake of Ca2+. When phosphorylated, the
inhibitory action of PLB on SERCA is lifted and Ca2+ can be pumped back into the SR
(58). This means that, when βARs are stimulated, not only the rate of contraction is
increased, but also the rate of relaxation (lusitropy).

8
In vascular smooth muscle, the relaxation in response to βAR stimulation is
mediated primarily by β2ARs and ascribed to the PKA phosphorylation of PLB and the
subsequent sequestration of Ca2+ from the cytosol by SERCA (84). PKA can also
phosphorylate plasma membrane ion channels to cause an efflux of Ca2+ out of the
cytosol. Ultimately, the decrease of cytosolic Ca2+ is what is causing the βAR-mediated
relaxation in vascular smooth muscle.
Ca2+
Ca2+
PKA(Active)
CONTRACTION
Phosphorylation
L-type Ca 2+ channel
Ca2 +
Ca2+
Ca2+
Ca2 +
Ca2+
P
Channel opening
Ca2+
Ca2+
Ca2+Ca2+
Ca2+
Ca2+
Ca2+
Ca2 +
RyRCa2+
Ca2+-induced Ca 2+ release
SR
P
Ca2+
Ca2+
PKA(Active)
CONTRACTION
Phosphorylation
L-type Ca 2+ channel
Ca2 +
Ca2+
Ca2+
Ca2 +
Ca2+
PP
Channel opening
Ca2+
Ca2+
Ca2+Ca2+
Ca2+
Ca2+
Ca2+
Ca2 +
RyRCa2+
Ca2+-induced Ca 2+ release
SR
P
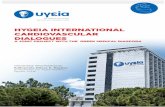
Figure 3. Effect of βAR activation in cardiomyocytes. PKA activated via the βAR/cAMP pathway
phosphorylates the L-type calcium channel and increases its opening probability. Intracellular
calcium (Ca2+) increases and when sensed by the ryanodine receptor (RyR) in the sarcoplasmic
reticulum (SR) membrane, additional Ca2+ is rapidly released into the cytosol and leads to
contraction of the cardiomyocytes. Activated PKA can also directly phosphorylate RyR to cause
Ca2+ release.

9
2.2 β2AR cross-signaling and compartmentation
The Gαs/cAMP signaling pathway is the classical example of βAR signaling. However,
the β2AR has the ability to cross-signal with the Gαi, inhibiting AC, resulting in a
decreased cAMP production (42, 44, 100). The switching between stimulatory and
inhibitory G-protein signaling takes place at higher concentrations of catecholamines. It
is mediated by PKA phosphorylation of the β2AR, which in turn decreases the affinity of
the receptor to Gαs and increases the affinity for Gαi (22). It is also demonstrated that the
βγ complex from pertussis toxin-sensitive G-proteins (i.e. Gi proteins) evokes a separate
signal through the MAPK pathway, further dampening the effect from the initial cAMP
pathway (22). The β2AR G-protein switching is thought of as a protective mechanism of
the βAR system and is shown to be antiapoptotic in the heart (104). This is further
supported by studies of βARs in heart failure, where β1ARs are downregulated to a
larger extent than β2ARs (16, 25). This naturally connects to the fact that decreased
levels of cAMP will lead to decreased activation of kinases such as GRKs and PKA,
consequently leading to a decrease in receptor phosphorylation and subsequent
downregulation. Attenuated relaxant effects on arteries through β2AR-induced Gαi
coupling has been documented (8) and in Papers IV and V of this thesis, Gαi switching of
the β2AR is a probable explanation for our observations in concentration-response
curves to the synthetic βAR agonist isoproterenol in chorioallantoic arteries from the
chicken embryo; at higher concentrations the agonist turned the response from relaxing
to contracting, in some cases contracting the vessel even more than the initial pre-
contraction (Fig. 4, Paper IV). This is further supported by the lack of αAR-mediated
contraction response in the studied vessels (Papers IV and V) and the isoproterenol
stimulation therefore has to be β2AR mediated.

10
Figure 4. Original tracing of the response of a chicken chorioallantoic artery to the β-
adrenoceptor (βAR) agonist isoproterenol (Iso) obtained by wire myography. The βAR-induced
relaxation of blood vessels is primarily mediated by β2ARs signaling through Gαs. However,
β2ARs have the tendency to switch from Gαs to Gαi signaling at higher concentrations of agonist,
which leads to contraction. The trace shows a clear contraction in response to 10-6 M Iso and
higher (concentrations shown as logarithmic values in figure). The vessel was precontracted by
depolarization with 62.5 mM KCl. Modified from Paper IV.
The difference in β2AR signaling compared to β1ARs is also ascribed to the spatial
localization of the receptors in the cell. It has been demonstrated that the cAMP
produced by β2AR stimulation fails to elicit phosphorylation of for example PLB and thus
failing to increase lusitropy (53, 102) and despite the higher cAMP production from β2AR
stimulation compared to β1ARs it is uncoupled from inotropic effects in cardiac cells (58).
Additionally, intact caveolae have been shown to be a requirement for β2AR-mediated
regulation of calcium channels, but nor for β1ARs (7). This growing body of knowledge
has lead to the hypothesis that the β2ARs are compartmentalized in lipid rafts, caveolae
or other spatially defined structures in the cell membrane (58, 85) and a seminal paper
was recently published, showing that β2ARs in the healthy heart are confined to deep
transverse T-tubules, while β1ARs are diffusely spread throughout the cell membrane
(67).
-9
-7
-6
-8
KCl
0.5
N/m
Iso
10 min
-5
-9
-7
-6
-8
KCl
0.5
N/m
Iso
10 min10 min
-5

11
2.3 βARs in cardiovascular disease
Physiological stress is well known to alter βAR signaling since stress is related to the
release of catecholamines that will stimulate βARs and, depending on the duration of the
stress, eventually lead to receptor desensitization and downregulation (83). Stress- or
non-stress induced, heart failure (HF) is connected to an increase in sympathetic activity
(25, 78). The sympathetic nerve endings are the source of the elevated levels of
norepinephrine that can be measured in HF patients (19). The downregulation of βARs
seen in HF due to the sympathetic hyperactivity decreases the contractile response of
the cardiac muscle and the suboptimal cardiac performance thereby fails to meet the
circulatory demands from the body. As an early intervention method, βAR agonist were
used to try to increase cardiac performance, but it showed to be detrimental when it only
reinforced the negative effects from the initial sympathetic overstimulation (77). Contra-
intuitively, βAR blocking has instead been shown to have long-term positive effects in HF
patients and is now an accepted treatment for HF patients (58, 78).
The damages on the heart from βAR overstimulation are proposed to be mainly
through β1AR Gαs signaling and include increased apoptosis, arrhythmia, cardiac
remodeling and hypertrophy (64, 77, 101). In HF, the β1ARs are selectively
downregulated, while the β2AR population is more or less retained (16, 25). Interestingly,
β2AR signaling has been shown to ameliorate HF and have antiapoptotic effects (16, 77,
101) and treating cardiomyocytes with isoproterenol will induce apoptosis in cells
expressing only β1ARs, but not in cells expressing only β2ARs (103) (Fig. 5).
Figure 5. Micrographs of TUNEL stained mouse cardiomyocytes treated with 1 µM isoproterenol
(ISO). Cells expressing only β1ARs are apoptotic (arrows indicating apoptotic condensed nuclei),
while cells expressing only β2ARs are not. Reprinted with permission from Zhu et al., 2001.

12
The protective, antiapoptotic effect of β2ARs is related to the cross-signaling of β2ARs
with Gαi proteins (101). Gαi proteins are up-regulated in HF and although the increase in
Gαi has been proposed to contribute to the decreased inotropy in the failing heart (73), it
might also be a protective measure from the heart to prevent further damage. The long-
term positive effect of βAR blockers has been suggested to be because of the block of
the detrimental β1ARs and promoting antiapoptotic and reverse remodeling effects
mediated by Gαi and β2AR agonists could therefore be a possible treatment for HF due
to the stimulation of protective pathways through Gαi (16).

13
3 DEVELOPMENTAL PROGRAMMING
Things that are dear or interesting to us tend to assimilate many names describing
virtually the same phenomenon – something that is certainly true in our field of work. I
have chosen to call the concept under which I have carried out most of the work
comprising this thesis “developmental programming”, while others have referred to it as
“developmental origins of health and disease” (DOHaD), “fetal programming” or
“predictive adaptive response” (PAR). As confusing as it may seem, these theories and
concepts are of common origin and merely differ in nuance or complexity levels; they all
assume that the embryo and fetus possesses an inherent plasticity and that, due to this
plasticity, changes in the pre- or neonatal environment can trigger physiological and
functional changes that will echo into adulthood.
3.1 Phenotypic plasticity and developmental “windows”
Phenotypic plasticity is defined as the ability of one set genotype to produce different
phenotypes due to changes in the environment and can be seen as the interaction
between genotype and the environment (71). Although quite a simple definition, it is not
as trivial deciding if the plastic phenotype is adaptive or not. Normally, a plastic
phenotype is considered adaptive if it gives a higher fitness in the new environment than
other phenotypes would, but a lower fitness in another environment (75). However, the
fitness associated to the phenotypic change is relative since it also comes with a cost; if
the environment is fluctuating, investing in the “new” phenotype is risky and if the
environment changes back, the fitness received from the initial phenotypic change may
now cause a decrease in fitness. Thus, for a plastic phenotype to be adaptive, i.e.
increasing fitness, the environment needs to be relatively stable. There are also more
direct costs involved in plasticity, such as maintenance of the sensory and regulatory
mechanisms and genetic costs (i.e. when plasticity genes are linked to genes reducing
fitness) (24). So, even if the plastic phenotype per se is beneficial in the new
environment, all of the costs must be taken into account to decide if the phenotype is
truly adaptive or not.
There are many examples of phenotypic plasticity in juvenile or adult animals, such
as crabs increasing their claw size when their prey get thicker shells or Daphnia
developing thick neck spines in the presence of midge larvae that preys on them (23). In
most mammals, however, the greatest plasticity exists during early life before cell

14
differentiation is completed, i.e. it is a developmental plasticity (34). Because cells
eventually do differentiate and differentiation in most cell types is irreversible, the
phenotypic changes induced during the plastic period will eventually also be fixed and
irreversible, which is of uttermost importance if the changes result in a maladaptive
phenotype that will eventually lead to disease – it cannot be reverted. This, however,
also means that it is important when during development an insult takes place. Different
organs have different proliferation periods and different physiological functions have
different timings for onset. Therefore, if the insult takes place during a period of growth,
the outcome can be expected to be less severe than if it takes place during a
proliferation period. These periods of different sensitivity are referred to as critical
windows of development and are different between organs and functions depending on
their maturation at the time of the insult (86).
3.2 Developmental Origins of Health and Disease
Before going into detail about the development of the different views and theories of fetal
events influencing adult health and function, it is in place to shortly review the concept of
Developmental Origins of Health and Disease (DOHaD). DOHaD is quite a modern
concept elaborated from the precedent FOAD (Fetal Origins of Adult Disease) and can
be seen as the “umbrella concept” under which all theories described below are
gathered. The modernization of the concept from FOAD to DOHaD was necessary as
the rapidly growing body of knowledge made it clear that not only fetal events can have
an effect on later disease risks, but events throughout the plastic phase of the organism
(32). Additionally, it was necessary to emphasize health in the concept, both since fetal
events are not restricted to negative, but can also have positive, effects on the postnatal
animal and because prevention and health promotion is an important part of medical
research (32). Nowadays, there is an international society of DOHaD that was set up to
“…promote research into the fetal and developmental origins of disease and involves
scientists from many backgrounds.” (1) and the Journal of Developmental Origins of
Health and Disease that “…publishes leading research in the field of developmental
origins of health and disease (DOHaD), focusing on how the environment during early
animal and human development, and interactions between environmental and genetic
factors, influence health in later life and risk of disease.” (2). Together they represent the
importance and rapid growth of this field of research.

15
3.3 The beginning - “Barker’s hypothesis” and the “thrifty phenotype”
Although DOHaD might represent the modern view of early life effects on adult health,
all big ideas have their antecedents. In 1977, the Norwegian scientist Forsdahl published
a paper where he noted that coronary heart disease mortality in a cohort of men over 40
was correlated with the infant mortality from the same region at the time the men were
born (29). About 10 years later, Barker and colleagues awoke a world interest around
the same subject when they published a series of now highly cited papers that founded a
new area of research (11, 12). Similar to Forsdahl in 1977, they managed to provide
epidemiological evidence for the relationship between infant mortality in 1921-25 and
coronary heart disease mortality in 1968-78 based on prosperity and nutritional status of
the British regions studied (11). Following the initial study, they further showed a
correlation between low birth weight and increased risk of ischemic heart disease in
adulthood (12). From these important studies arose what we now know as “the Barker’s
hypothesis”, something that Barker himself defines as when: “…undernutrition in utero
permanently changes the body’s structure, function and metabolism in ways that lead to
(…) disease in later life” (10).
Since the introduction of the hypothesis almost 30 years ago, countless studies
have verified the theory, firmly establishing that intrauterine growth restriction is
correlated to many adult diseases, not only cardiac disease, but also diabetes type 2,
obesity and hypertension (27, 76). However, it is a hypothesis that encompasses only
the relationship between low birth weight and adult disease and so, after having
prevailed for a long time, the Barker’s hypothesis has been suggested to have served its
purpose and that, although it will always be the base for the whole research field, it is
time to move on and use the findings to investigate the actual mechanisms behind the
observed phenomenon to be able to assess new targets for intervention and thereby
prevention (68).
In 1992, Barker and colleagues presented another refined and extended
hypothesis based on the previous “Barker’s hypothesis” that they called “the thrifty
phenotype” (39). The new hypothesis was already narrowing the old hypothesis down to
a more defined field of interest, namely pancreatic development and type-2 diabetes. In
their review (39), they link poor intrauterine growth to changes in glucose-insulin
metabolism leading to insulin-resistance. Since then, many more epidemiological studies
in humans have presented evidence of the relation between impaired fetal growth due to

16
malnutrition and metabolic syndrome and the body of empirical data from animal models
is vast as reviewed by Bertram and Hanson (14).
Another important addition to the hypothesis was that of uterine conditions giving
a “hint” of what is to be expected in postnatal life, meaning that if nutrition is sparse, the
organism can interpret the low nutritional level as a signal to adapt its metabolism to low
food conditions and thereby be prepared for the life conditions after birth. If the postnatal
diet is instead rich, the adult would suffer a higher risk of developing type-2 diabetes
when it faces the high metabolic load (92).
Although the thrifty phenotype hypothesis started off focusing on metabolic disease, it
has later been established that it is a general model that can be applied in evaluating the
effect of intrauterine experience on all organ systems (69, 92).
3.4 The “Predictive Adaptive Response” theory
As mentioned in the introduction to this chapter, the different theories around the role of
the developmental environment on future health are very similar, but they do, however,
emphasize quite different aspects. Building on the “thrifty phenotype” hypothesis,
Bateson et al. suggested that the early organism receives information while in the
prenatal environment about the quality of the postnatal environment, much like a
“weather forecast” (13, 94). The adaptations induced by the “sensing” of the environment
to come was not seen as ideal, but more making the most of a bad situation (92).
The “Predictive Adaptive Response” theory (PAR) was coined by Gluckman and
Hanson in the beginning of the 21st century and takes the “forecasting” hypothesis even
further (33, 34). PAR emphasizes the importance of the fetal/young animals’ prediction
of the future environment and they partly define PARs as being “…induced by
environmental factors acting in early life, most often in pre-embryonic, embryonic or fetal
life, not as an immediate physiological adaptation, but as a predictive response in
expectation of some future environment” (34). In other words, this suggests that the
altered growth trajectories and physiological changes induced in the fetus by an
environmental challenge are not just to help the fetus cope with the immediate challenge
and survive until birth, but more importantly, describe the challenge (eg. nutrient
availability) as a “cue” from the mother, preparing the fetus of what is to come. If the
challenge is true, i.e. the postnatal nutritional status matches the one experienced by the
fetus, the animal is presumably well adapted and the “prediction” is correct, thus there is
a fitness benefit. However, if the experienced nutritional status is low and the postnatal is

17
adequate (e.g. in the case of placental malfunction), there is a nutritional mismatch, i.e.
the prediction is faulty and the maladaptation may lead to adult disease (34). To put it
very simply, one can say that PAR is really a form of developmental plasticity, but with a
predictive power (36).
Additionally, the PAR theory tries to distinguish the relevance of severity of the
fetal/neonatal challenge; it is only a PAR if the challenge works within the scope of the
organism’s plasticity (34). If it is too severe, the fetus will not be able to cope and the
challenge will thus be disruptive. On that scale, between the PAR-inducing and the
disruptive intensity of the challenge, is a gray area where the organism is forced to
“cope” with the environment, a “coping” that might encompass simply homeostatic
changes or more drastic changes necessary to ensure survival that might leave traces
that will affect the fitness of the adult individual (37) (Fig.6).
PARs or not, this is an important issue when interpreting empirical data; are we
measuring what we can call “PAR mismatch” or “programming effects” or are we
measuring disruptive damage? There is no easy answer to that question, but it is one
that should be kept in mind when analyzing data. In addition to the initial focus mainly on
nutritional shortage, Gluckman et al. (37) extended the theory to also include nutritional
excess as a potential cue that would either be disruptive or cause a mismatch (Fig.6).

18
Deficitdisruption
’Coping ’
PARs
Fitn
ess
Substrate availability
”Scope” of plasticity
Excessdisruption
’Coping ’
Very low Very high
Deficitdisruption
’Coping ’
PARs
Fitn
ess
Substrate availability
”Scope” of plasticity
Excessdisruption
’Coping ’
Very low Very high
Figure 6. Suggested relationship between early life substrate availability (e.g. nutrients, oxygen
etc.) and adult fitness according to the “predictive adaptive response” (PAR) hypothesis. PARs
are induced within the “scope” of plasticity. Intense challenges forces the organism to “cope” with
the challenge through remodeling/adjusting to assure survival, but may cause a disadvantage in
adulthood. Extremely high or low substrate availability causes disruption, e.g. malformation or
growth retardation. Modified from Gluckman, Hanson, Spencer and Bateson, 2005.
3.5 Criticism of PAR
Members of the group which formulated the PAR theory are very active members of the
DOHaD research community and have published many papers and books in the field,
firmly establishing PAR as a valid theory (32-37, 40, 50). However, being one of the
biggest theories in the field, it has not passed uncriticized.
Altimiras and Milberg (2005) question the term “predictive adaptive” by stressing
the need for a stimulus to receive a response, pointing out that adaptation can only be
based on factors currently present and cannot be based on those in the future, i.e. they
cannot be “predictive” (4). Wells (2007) goes further in his criticism to say that the PARs
concept is flawed for several reasons; firstly, he questions the validity of the “prediction”
in a long-lived species like humans (93, 94). Unlike a prediction in a species with short

19
generation time, a correct prediction of the postnatal life can be hard to make in a long-
lived species since the probability that the environment will change is large. Secondly,
he claims that PAR overlooks the fact that mammalian fetuses are robustly protected
from external perturbations due to the mother’s own buffering capacity, and will thus
never get correct information about the external world, only cues that have already been
modified and translated by the mother (92, 93). This goes hand in hand with that the
mother’s fitness is maximized if her offspring is strong and wants to protect her fetus
from disturbances. Wells emphasizes that, because of the maternal-offspring fitness
trade-off during pregnancy and the implications that this conflict has for maternal fitness
especially, the trajectory of the fetus is controlled by the status of the mother and
therefore not “predictive”, but rather backward-looking (93). This is further supported by
Kuzawa (54) that suggests that growth responses to short-term environmental
fluctuations are more about adopting the maternal phenotype and thereby adjust, not to
small periodical changes, but to a longer history of fluctuations that has influenced the
previous generations. This supposedly “smoothes out” fluctuation peaks, or the “noise”
of seasonality and enables the fetus to actually adjust according to longer term trends
(54). Lastly, Wells argues that the structure of the group in social animals, like humans,
will have an impact on the nutritional status of different mothers in the group, even
though the physical environment is the same. Social hierarchy will make a female of
lower social status receive less food. To maintain high fitness, it is therefore best for a
lower ranked mother to have a small progeny since it is likely that the offspring also will
be low in rank and receive less food (93).
3.6 My definition of developmental programming
In this jungle of expressions and definitions of the DOHaD phenomenon, I have chosen
to talk about “developmental programming” to describe my work. Although the full term
“developmental programming” is not as clearly defined as the theories presented above,
Lucas (1992) defined “programming” as: “…programming occurs when an early stimulus
or insult, operating at a critical or sensitive period, results in a permanent or long-term
change in the structure or function of the organism” (59). Barker and colleagues
sometimes use the expression “fetal programming” (9, 38), but for the same reason
presented for the change from FOAD to DOHaD, I have chosen to use the term
“developmental programming” to encompass both pre- and postnatal growth and not just
in utero events.

20

21
4 HYPOXIC CARDIOVASCULAR REGULATION AND THE ROLE
OF β-ADRENERGIC RECEPTORS
When a vertebrate is faced with oxygen deficit caused by for example physical activity or
altitude, there are several mechanisms that will set in to regulate cardiovascular function
and retain homeostasis. These mechanisms are different between species and have
different onsets during development.
4.1 Adult and fetal cardiovascular regulation during hypoxia
The cardiovascular response to hypoxia in adult mammals is not uniform, since it is
complicated by ventilatory actions that affect the heart rate (HR) and blood pressure
(BP). When faced with hypoxaemia1, or low blood oxygen, chemoceptors in the carotid
bodies (located close to the bifurcation of the carotid artery in the neck) sense the low
pO2. This triggers an efferent reflex response that includes both increased vagal activity
that potentially could lower heart rate and increased sympathetic tone that could
increase blood pressure (62). However, the chemoreflex primarily affects the pulmonary
ventilation and the cardiovascular response is thereby subjected to secondary ventilatory
effects; vagal activity is suppressed by the activity of inspiratory neurons and pulmonary
stretch receptors and the outcome of HR and BP may therefore be different depending
on the respiratory response (49). In spontaneously breathing adult animals, hypoxia
leads to hyperventilation that can cause tachycardia or bradycardia combined with either
vasoconstriction or vasodilatation depending on the animal model (62). When pulmonary
ventilation is controlled, however, tachycardic and vasodilatory responses are
completely abolished and unmask bradycardia and vasoconstriction as the “true”
chemoreflex-induced response of the cardiovascular system (49).
In one of the most common fetal hypoxia models, the fetal sheep, the chemoreflex
is present relatively early (51) and the magnitude is dependent on age together with the
depth and duration of the hypoxic insult (91). Hypoxia has no effect on fetal breathing
movements in the sheep fetus, which is not unexpected since fetal breathing movements
have no role in gaseous exchange (31). Without the ventilatory effects, the
cardiovascular response to hypoxia in the near-term sheep fetus is therefore similar to
1 Note that hypoxaemia is used when talking about low partial pressure of oxygen in the blood in particular, while hypoxia is used as a wider concept, mostly referring to the oxygen level of the environment the organism is in. Hypoxaemia is often a result of hypoxia, but in this thesis I use hypoxia indifferently.

22
the one in the adult with controlled ventilation; hypoxia induces an initial bradycardia and
increased peripheral vascular resistance mediated by carotid chemoreceptors (31) (Fig.
7). The increase in systemic blood pressure is instrumental in the redistribution of
cardiac output (CO) to crucial organs like the heart, brain and adrenals on behalf of
organs such as the kidneys and liver (28, 66). If the hypoxic episode is prolonged, the
release of catecholamines will oppose the vagal tone and eventually restore HR (28).
In the model used for this thesis, the chicken embryo, the cardiac response to
hypoxia differs from that of the fetal sheep. As shown by microsphere injections, the
redistribution of CO in response to hypoxia is present also in the chicken (66), but both
the vagal and sympathetic limb of the reflex are non-functional, suggesting that
cardiovascular control relies mainly on humoral factors such as epinephrine (20). The
acutely hypoxic chicken embryo is bradycardic, possibly due to direct effects of low
oxygen on the cardiac muscle (21), and hypotensive. In Paper V we investigate the
effect of chronic hypoxia on BP and HR, something that will be further discussed in
Chapter 6.

23
Figure 7. Cardiovascular response to hypoxia in the near-term sheep fetus. Intact fetuses (solid
lines) experience hypoxic bradycardia (top) and an increase in peripheral vascular resistance
(bottom), while carotid denervated fetuses (dashed lines) do not, demonstrating that the initial
hypoxic response in the late fetal sheep are due to a functional chemoreflex mediated through the
carotid chemoreceptors. Modified from Giussani et al. 1993.
220
200
180
160
140
120
Normoxia Hypoxia Normoxia
Hea
rt r
ate
(BP
M)
5
4
3
2
1
0Fem
ora
l va
scul
ar
resi
stan
ce
(mm
Hg
min
ml
-1)
60 min
220
200
180
160
140
120
Normoxia Hypoxia Normoxia
Hea
rt r
ate
(BP
M)
5
4
3
2
1
0Fem
ora
l va
scul
ar
resi
stan
ce
(mm
Hg
min
ml
-1)
60 min60 min

24
4.2 Effect of hypoxia on the βAR system
Hypoxia is an environmental stress. The physiological response to stress is linked to the
release of catecholamines and elevated levels of catecholamines are indeed
documented in both the hypoxic adult and fetus (17, 18, 21, 60, 65). However, elevated
catecholamines and hypoxia have different effects on adult and embryonic βARs.
Hypoxia or infusion of βAR agonists in the intact adult elicit the classical βAR
regulation pathway of desensitization and downregulation with a concomitant loss of
surface receptors in both the cardiac and vascular tissue (5, 41, 98). However, the
hypoxia-induced loss of βAR-mediated cAMP production in adult hearts can be restored
by normoxic recovery (45).
In the fetus and neonate, βAR regulation differs from the adult. In contrast to the
adult desensitization, Auman et al. (2001, 2002) have shown that infusion of βAR
agonists do not desensitize the βARs, but rather sensitizes them. We found similar
results in response to chronic hypoxia in Paper II where we show that, despite the loss
of surface receptors, there is an increase in sensitivity of the system. The fetal and
neonatal βAR sensitization has been linked to a higher concentration of β2ARs in the
fetal/neonatal heart (6) and the fact that β2ARs 1) are resistant to downregulation and
have a protective effect on the heart, 2) do not induce cardiomyocytes enlargement
(hypertrophy) like β1ARs do (the increased volume-to-area ratio directly means
decreased sensitivity) and 3) have, in opposite to in the adult, contractile effects in the
neonatal heart (101). Although we found that there is an increase of Gαi in the chronically
hypoxic chicken embryo heart (Unpublished data, Isa Lindgren 2010), the contractile
effect of β2ARs is thought to be because of the lack of Gαi coupling in the fetal heart and
that Gαi coupling is aquired with maturation (101). The increased βAR sensitivity has also
been linked to an increase in Gαs/AC coupling and altered expression of AC subtypes
promoting a more active isoform of AC (79).
The effects of hypoxia on βARs described above are implicitly related to the
increased release of catecholamines based on that the observations are made in intact
animals where catecholamines have been shown to increase with hypoxia (see
beginning of this section). This is also supported by similar results from studies where
catecholamines have been infused. However, in addition to the secondary hypoxic effect
on βARs through increased levels of catecholamines, hypoxia per se has been shown to
have an effect on βARs (61). Marsh and Sweeney (1989) incubated cultured embryonic
chicken cardiomyocytes myocytes in hypoxia induced a >50% decrease of cell surface

25
βARs that was restored to control values with re-oxygenation (61). This is interesting
since these cardiomyocytes are isolated and thereby not subjected to catecholamine
stimulation of adrenomedullary or sympathetic origin. There is, however, evidence of
intrinsic cardiac adrenergic cells (ICA cells) in the fetal heart releasing epinephrine and
norepinephrine that can affect the pacing rate of spontaneously beating cardiomyocyte
cultures (46). Whether hypoxia stimulates ICA cell catecholamine release or hypoxia per
se is the reason for the hypoxic βAR downregulation is not yet known, but it is an
interesting question that warrants further investigation.

26

27
5 SUMMARY OF PAPERS
The first foundation for our future life and health is laid during fetal development and
understanding developmental processes and what influences them is therefore of great
interest and importance. In this thesis I have looked at not only the cardiovascular β-
adrenergic signaling system, but also how it is altered by chronic prenatal hypoxia
connected to the progression of growth and development throughout fetal life. The β-
adrenoceptors are of particular interest, since they are crucial for cardiovascular
development, function and regulation and also since hypoxia trigger the release of their
main ligands epinephrine and norepinephrine.
5.1 Paper I
Lindgren I, Altimiras J . Sensitivity of organ growth to chronically low oxygen levels
during incubation in red junglefowl and domesticated chicken breeds. Submitted
Chicken domestication has resulted in the appearance of numerous phenotypic traits
connected to animal productivity (egg laying or meat production). This paper
demonstrates that some of these traits are already present during embryonic
development and this makes some breeds more susceptible to environmental
manipulation such as oxygen shortage. In the paper we use a modeling approach to
illustrate the effects of hypoxia and developmental age on organ growth, built on organ
mass data from different developmental stages. In particular, we show that the
developmental trajectory for cardiac growth is affected by hypoxia. Because βARs are
closely related to cardiac development and growth (72), this observation alone prompted
the follow-up work on cardiac function in papers II and III. The paper is also an
interesting contribution to the discussion about developmental plasticity, allocation
theory and the evolutionary significance of plasticity/developmental programming.

28
5.2 Paper II
Lindgren I, Altimiras J. Chronic prenatal hypoxia sensitizes β-adrenoceptors in the
embryonic heart but causes postnatal desensitization. Am J Physiol Regul Integr Comp
Physiol 2009;297:R258-264.
Prenatal oxygen deficit (hypoxia) is correlated with low birth weight, which is in turn
correlated with increased risk of adult morbidity like diabetes and cardiovascular disease.
This phenomenon is referred to as developmental programming and in this light we
describe how chronic prenatal hypoxia affects βAR density and sensitivity in both
embryonic and juvenile broiler chicken hearts, since β-adrenoceptors are crucial for the
embryonic development and adult function of the heart. Broiler eggs were incubated in
normoxia or hypoxia (14% O2) throughout development and one batch from each
treatment was also hatched and raised to 14 or 35 days of age. Based on [3H]CPG-
12177 binding in ventricular tissue slices and concentration-response curves to
epinephrine in electrically paced muscle strip preparations, we found that chronic
prenatal hypoxia increases the pEC50 (i.e. sensitivity) of epinephrine-stimulated cardiac
strips in the 19 day embryo, despite a significant decrease of receptor density. At the
same time, we found that the prenatal hypoxia did not affect receptor density in the 35
day old juvenile chickens, but caused βARs desensitization. 14 day old chickens were
not affected. This supports that prenatal hypoxia has a “programming” effect on adult β-
adrenoceptor function that may be an indication of early symptoms of heart failure.
5.3 Paper III
Lindgren I . Postnatal β-adrenergic desensitization caused by chronic prenatal hypoxia
is linked to an increase in Gαs and decreased β1AR/β2AR ratio. Manuscript
This paper is the continuation of paper II and is an attempt to explain the β-adrenergic
desensitization seen in the 35 day juvenile chickens suffering from chronic prenatal
hypoxia. Others have suggested that altered receptor sensitivity could depend on a
decrease in β1AR/β2AR subtype ratio (since β2ARs do not significantly contribute to
contraction in the adult heart) and Gαs/Gαi protein (more Gαi could potentially increase the
probability of β2AR switching, thus inhibiting cAMP production) (6, 79, 101). We
investigated the β1AR/β2AR subtype ratio using selective [3H]CPG-12177 binding in

29
ventricular tissue slices by blocking β1ARs (CGP-20712A) or β2ARs (ICI-118,551).
Gαs/Gαi protein expression levels were determined by Western blot on cardiac whole-
tissue preparations and cAMP produced in response to βAR stimulation with
isoproterenol was measured with an immunological assay. The significantly lower cAMP
level in prenatally hypoxic hearts compared to the controls supported our previous
observations in Paper II of βAR desensitization in 5 week chickens prenatally exposed to
hypoxia. We also found that there is indeed a decrease in β1AR/β2AR ratio. Surprisingly,
Gαs increased in prenatally hypoxic hearts and not Gαi as hypothesized. When again
considering the lower cAMP accumulation in response to βAR stimulation however, the
increased Gαs seems to be inactive and might not be recruited to the cell membrane,
something that is necessary for taking part in the signaling. Based on that the 8 month-
old chicken exposed to prenatal hypoxia display cardiomyopathy, we speculate that what
we see in our 5 week chickens is a phenotype of early cardiac failure.
5.4 Paper IV
Lindgren I, Zoer B, Altimiras J, Villamor E. Reactivity of chicken chorioallantoic
arteries, avian homologue of human fetoplacental arteries. Submitted
The chorioallantoic (CA) membrane is the avian homologue to the mammalian placenta,
but nothing is yet known about the vasoreactivity of this vascular bed. Characterizing the
vascular reactivity of the CA arteries throughout development is essential to fully
understand the hemodynamics of the embryo since a large proportion of vascular
volume is contained within the extraembryonic circulation. In this paper we used wire
myography techniques to perform concentration-response curves in isolated CA arteries
to contracting (KCl [4.75-125mM], the thromboxane A2 mimetic U46619 [1nM-1µM],
endothelin-1 [ET-1; 1nM-100nM] and α1 adrenoceptor agonist phenylephrine [Phe;
10nM-100mM]) and relaxing agents (acetylcholine [ACh; 10nM-100mM], the nitric oxide
donor sodium nitroprusside [SNP; 10nM-100mM], the β-adrenergic agonist isoproterenol
[Iso; 1nM -1mM] and the adenylate cyclase activator forskolin [Forsk; 1nM-10mM]). In
the relaxation experiments the vessels were pre-contracted with either 62.5 mM KCl or
U46619. We also carried out experiments of acute hypoxia on the vessels and our
results show that CA arteries share many of the characteristics of placental arteries, but
also that they do not react to Phe (indicating lack of αAR receptors), that they contract,
rather than relax, to ACh and that they display vasoconstriction to acute hypoxia. In

30
addition to supplying us with information to better understand the hemodynamic
regulation of the chicken embryo, the obtained results suggest that it is an interesting
model artery for studying the mechanisms of hypoxic vasoconstriction.
5.5 Paper V
Lindgren I, Crossley D, Villamor E, Altimiras J. Hypotension in the chronic hypoxic
chicken embryo origins in a potent β-adrenergic response of the chorioallantoic arteries
and not bradycardia. Submitted
Despite the increasing importance of the embryonic chicken as a model to study
development, cardiovascular responses to hypoxia and developmental programming of
adult disease, the hypoxic hemodynamic response and regulation is still not fully
understood. In this paper we try to answer the question if the chronic hypoxic chicken
embryo is hypotensive like the acutely hypoxic embryo (21) and if this possible
hypotension is due to chorioallantoic (CA) artery β-adrenoceptor-mediated relaxation
and/or bradycardia. We measured heart rate both acutely by cannulation on day 19 of
incubation and continuously throughout development by a non-invasive impedance
method. Additionally, blood pressure was measured in the cannulated embryos.
Concentration-response curves to isoproterenol and forskolin in normoxic and hypoxic
CA and femoral arteries were obtained by wire myography of isolated vessels. We found
that heart rate was not changed in the chronic hypoxic chicken embryo and that CA
arteries were not affected by hypoxia, but displayed a potent β-adrenergic relaxation
together with an increased βAR sensitivity of the hypoxic femoral vessels. This suggests
that the CA vascular bed, together with an increased vasorelaxation of the systemic
arteries, is an important contributor to the hypoxic hypotension response in the chicken
embryo, while heart rate is not involved.

31
6 DISCUSSION
6.1 Comments on the experimental model
The chicken model used in my studies is an increasingly used model to study hypoxic
effects on prenatal growth and development (30, 57, 81, 97, 105), much because it
enables manipulation without confounding maternal effects. The chicken genome is
sequenced (88), which adds additional value to the model.
Commercially, the broiler chicken grows to 2.6 kg in 6 weeks after hatching. The
rapid growth of especially muscle mass puts a heavy load on the cardiovascular system
to supply the tissues with oxygen and nutrients. This predisposes the broilers to develop
cardiovascular disease already as juveniles and because we know that cardiovascular
problems can occur already before adulthood2, 5 week animals are suitable for studies
of fetal programming of cardiovascular disease. However, rearing the birds in line with
commercial breeding is not suitable for research animals and thus our birds did not grow
quite as fast as indicated above.
Although lower levels of oxygen can be successfully used in experiments of acute
or intermittent hypoxia, the level of hypoxia in my chronic experiments is between 15-
14% O2. The choice of oxygen concentration is based on pilot experiments where I
found that, in a chronic setting, 12% O2 killed all embryos after day 11 of incubation with
a peak mortality at Hamilton-Hamburger stage 25-26 (corresponding to day 5).
6.2 Developmental programming (Papers II and III)
If you boil down the information presented so far in this thesis, you end up with quite a
simple trail of events: Developmental hypoxia leads to fetal growth restriction, fetal
growth restriction leads to increased risk of adult cardiovascular disease and adult
cardiovascular disease is closely related to changes in the βAR system. Despite the
seemingly obvious connection between low birth weight - adult cardiovascular disease -
βARs, there is not much known about possible programming effects of prenatal hypoxia
on the adult βAR system. In one of the few studies on programming effects of βAR
function, Rohlicek et al. (2005) show that 10 days of hypoxia with subsequent normoxic
recovery in the neonatal rat does not change the βAR density in the adult heart, but
decreases cAMP production, likely due to changes in AC levels. Because of the evident
lack of data on fetal programming effects of hypoxia on the βAR system and its
2 Adulthood defined as after sexual maturity, approximately 20 weeks of age in the chicken.

32
importance in cardiovascular disease, one of the most important aims with this thesis
was to investigate whether prenatal hypoxia has a programming effect on adult βAR
function or not. I show in Paper II that it does; chronic prenatal hypoxia in the chicken
increases βAR sensitivity in the embryo, but has no effect in the 2 week old postnatal
animal. However, in the 5 week old chicken, βAR sensitivity to epinephrine is decreased.
It is important to consider all three of these stages when discussing whether this is
programming or not; the fact that the 2 week old chicken is unaffected and that the
desensitizing effect occurs later in life is key. In Paper III we look for possible
mechanisms behind this desensitization and find that the β1AR/β2AR ratio is decreased,
resembling what is seen in adult individuals suffering from cardiovascular disease,
suggesting that my 5 week old chickens might be in the early stage of developing heart
failure. This is further supported by a study from Tintu et al. (2009) showing how 8
month-old chickens prenatally exposed to hypoxia display left ventricular dilatation
cardiomyopathy and cardiac remodeling (87). Surprisingly, I also found an increase in
Gαs, the opposite to the hypothesized increase in Gαi. However, a mere increase of Gαs
does not necessarily mean that the expressed proteins are available for signaling. The
protein increase could be in the unavailable cytosolic fraction, or the coupling of the βAR
to the Gαs could be affected through elevated receptor phosphorylation due to an
increase in GRKs or an increase in β-arrestin availability to block the receptors (58).
Additionally, even if Gαi do not increase, it has been shown that the functional activity of
Gαi is increased (26), which would contribute to the decreased βAR response. My
suggestions for further studies is the expression and activity of AC isoforms, cell
fractionation of G-proteins, Gαs functional activity and the activity and abundance of GRK
and β-arrestin in the prenatally hypoxic heart. My ultimate conclusion from Paper II and
III is however, that prenatal hypoxia does have a programming effect on adult βAR
function.
6.3 Growth and allocation (Paper I)
Another important part of this thesis is dealing with the effect of hypoxia on growth and
resource allocation – a foundation for discussing the growth restriction factor of
developmental programming. It is established that the organism has a basal energy
budget for maintaining minimal functionality and all energy available on top of that is
allocated to growth, reproduction, fat storage and physical activity (54). Consequently, if
energy availability is on the verge to what is required for maintaining basal function,

33
there will be a re-allocation of energy to save the most vital functions and organs to
secure survival. In the case of prenatal hypoxia where oxygen is the limiting metabolic
factor, the re-allocation from growth to preserving vital functions is illustrated by the re-
distribution of cardiac output away from the carcass towards the heart, brain and
adrenals (66). This contributes to the well-established fetal growth reduction and sparing
of the before mentioned organs. I show in Paper I that the sparing is different in different
strains of chickens. The heart and the liver are spared in the early broiler embryo, but
stunted in the late embryo. Considering that about 50% of the embryonic growth takes
place in the last five days of incubation (80) and that it is the period when the oxygen
demand reaches its peak, hypoxia has a greater impact on growth in the end of
incubation. This is emphasized by the fact that the loss of embryonic mass in response
to 14% O2 is absent at day 7, 10% at day 11 and around 30% at day (unpublished data,
Isa Lindgren, 2010). It is possible that my level of hypoxia is not affecting the early
embryo because its oxygen demand is low, but that it is detrimental in the late embryo
because of its higher metabolic rate. Referring back to Fig. 6 in Chapter 3, the milder
hypoxic insult in the early embryo could be speculated to be within the “coping” section
of the graph, making the best of the situation and thus being able to re-allocate
resources to spare the heart. Later on in development when the intensity of the hypoxia
is increased due to higher oxygen demand, it might be so severe that it pushes the
response into the “disruptive” zone, leading to the recess of all organ growth. A future
perspective to organ growth and resource allocation in the chicken is to decrease the
severity of the hypoxia (tentatively by inducing intermittent hypoxia) to investigate
whether sparing of the heart can be kept until hatching. Broberg et al. (2003) show that a
10-day period of anemia in the fetal sheep actually increases the contractile function of
the adult heart in response to hypoxia (15), something that would be very interesting to
attempt in the chicken due to its rapid postnatal growth and subsequent tissue hypoxia.
6.4 Vascular reactivity and cardiovascular response to chronic hypoxia in
the chicken embryo (Papers IV and V)
Despite the popularity of the chicken embryo as a model to study development and
hypoxic response (30, 57, 81, 97, 105), the understanding of something as basal as the
cardiovascular regulation in response to chronic hypoxia is still incomplete.

34
Crossley et al. (2003) hypothesizes that the hypotension seen in the acutely
hypoxic chicken is due to βAR dilatation of the CAM. Because the basic vasoreactivity of
the CAM has never been assessed, I started by characterizing the contractile and
relaxant responses of the CAM (Paper IV). With the integrative cardiovascular response
to chronic hypoxia in mind, my most important findings were that the CA arteries did not
contract to phenylephrine (indicating lack of αARs), but relaxed to both βAR stimulation
by isoproterenol and AC stimulation by forskolin. I also found that CA arteries share
many of its relaxing and contracting responses with placental vessels to common
vasoactive drugs such as endothelin-1 and sodium nitroprusside. A quite significant
exception, however, was a substantial contraction to acetylcholine in K+ pre-contracted
vessels. CA arteries, like placental, also display hypoxic vasoconstriction indicating an
oxygen sensing capability. For future studies it would be interesting and important to
define the hypoxic vasoconstriction of the CA arteries and the impact it has on the
hemodynamics of the chicken in hypoxia. This is not, however, within the scope of this
thesis.
The characterization of CA arteries in Paper IV was important per se, since it is a
large vascular bed with previously unknown vasoreactivity. It was also the necessary
foundation for Paper V where I investigated the BP and HR response to chronic hypoxia.
The baroreflex is not well developed in the chicken embryo (3) and in the absence of a
baroreflex, a drop in HR is positively correlated to BP, i.e. low HR leads to hypotension. I
showed in Paper V, however, that HR is not lower in chronically hypoxic embryos, and
thus not contributing to the hypotension. Instead, I showed that CA arteries display a
potent βAR relaxation that is not altered with hypoxia and that femoral (systemic)
arteries βAR relaxation was increased with hypoxia. Thus, what is likely causing the
hypotension in the hypoxic chicken embryo is βAR stimulation by increased levels of
catecholamines.
The results from Papers IV and V are important not only to elucidate new aspects
of fetal cardiovascular regulation, but also to understand mechanistics behind βAR
regulation. Tissue-specific βAR regulation has been described before (5) and it is
apparent that βARs in the CAM and the femoral vessels are differently regulated under
identical conditions. An interesting dimension to this discussion is the role of innervation;
Ruijtenbeek et al. (2000) has demonstrated hyperinnervation of the femoral artery in
hypoxic chicken embryos (82), while I have shown that the CAM is not innervated (Paper
IV). The sympathetic innervation in the chicken embryo, although present, has been

35
suggested not to be functional until very late in incubation (21), but might be involved in
the disparate regulation of systemic vs. extra-embryonic vascular βARs.
6.5 Conclusions
With this thesis I have further defined and refined the prenatally hypoxic chicken model
and used it to show that chronic prenatal hypoxia causes growth restriction, re-allocation
and that it has programming effects on the βAR system in the adult. The latter indicates
that the βAR system is an important factor in studying hypoxic developmental
programming of adult cardiovascular disease.

36

37
ACKNOWLEDGEMENTS
I would like to dedicate my first thank you to my supervisor Jordi. Not just because it is
expected from you to thank your supervisor first when writing your acknowledgements,
but because it is from the very depth of my heart when I say that I am so incredible
grateful to have had you as my supervisor. You saw something in me (I am still not sure
I understand what, because you asked me at my interview how I would compensate for
not being so book smart or exceptionally bright…) and gave me the opportunity of a life
time when you took me on as you PhD student. There is so much I have to say, but at
least let me thank you for your never ending commitment, your stamina, drive and
enthusiasm, your contagious interest in science and teaching, your wit, your cheeriness,
your know-how, your straightforwardness, your way of always fighting for what you
believe in and for rubbing all of the above off on me. Thanks for teaching me that a
physiology lab is just as much a work-shop and that all physiologists need to know how
to solder. Thanks for all the fun and laughs, but also for being an ******* sometimes, only
so that I could realize later that you were only being honest and teaching me reality,
independence and trusting my own ways – it took me sometime to realize that (even if
you see him as your science hero) sometimes your boss does not know everything and
you might just be right yourself! At last, thank you for just being the crazy, happy
Spaniard that makes coming into work everyday a treat and adventure! It is with a heavy
heart and with the deepest respect for you as a person and a researcher that I leave
your (our!) lab, but you promised me you would be my life-long friend and mentor and I
will hold you to it! Thanks also to your wonderful family for putting up with the both of us
and for all the great times we have had together.
Secondly, I would like to thank the other Spanish keystone of my PhD - my co-
supervisor Eduardo Villamor. Thank you for taking me in to your lab in Maastricht and
teaching me so much about vascular physiology in only three months. 40% of my papers
in this thesis are the products of my work in your lab and that is not even covering all the
data we produced – one cannot call that anything but a productive collaboration! Thank
you for always being so enthusiastic and encouraging, it was a true pleasure working in
you lab and it certainly helped me get my new job! Thanks also to the rest of my
colleagues at the University hospital of Maastricht for making my stay so much fun.
I am also very grateful to Carl-Gunnar Runemark and colleagues at Lantmännen
SweHatch in Väderstad. Thanks for being so helpful and accommodating throughout the
years we have collected the eggs for our research at your hatching facility.

38
Thanks to all my wonderful colleagues throughout my years at Biology, you all
contributed to that it has always been interesting, rewarding and fun to come in to work.
Special thanks to Johan B for all the good ol’ years sharing an office, to the loyal Friday
beer crew for making Friday afternoons half an hour shorter and to Magnus E and Ida G
(the two people in Biology except me who know what working for Jordi is like!) for always
being there when I need to vent and for putting an extra smile on my face, preferably
over lunch ☺. Thanks also to all the students that have passed through the lab for the
effort that you made, but mostly for teaching me a whole lot about myself, forcing me to
be a “boss”.
Thanks to my chemistry posse – Daniel K, Roz, Alma, Ina and the others – not
only for your support and being good friends through my last year of my PhD, but for
making my life with one foot in integrative physiology and one foot in biochem sooo
much easier with all your know-how! You are all stars and super-brains ☺.
A big thank you to Stefan Klintsröm, director of Forum Scientium, and all of the
Forum students for enriching my time as a PhD student. Through Forum I have not only
made many friends and learned about new places, ideas and techniques, but also
gained important knowledge about the part of science you cannot learn from books –
communicating science, research politics and life after your PhD.
Science is a lot of fun, but sometimes you need to take your mind off things, and
what better way to do it than with friends from back-in-the-days – thank you my
wonderful, sassy, honest, loving and caring Matfors-girls of “fnittergänget” - Lisa, Martina,
Backlund and Bengtsson - for putting things in perspective and loving me for who I am.
Thanks to my fellow PhD girls outside LiTH, Dana, Kattis, Anneli and Sanna for being
such a source of inspiration (and red wine!). Thanks also to the rest of my Linköping-
gang through the years (no one mentioned, no one forgotten - there are too many of you,
but you know who you are!) for putting up with me constantly yapping about my work.
You have kept my feet on the ground and made me feel that I am not alone when things
have been tough!
Now to the most important people behind the scenes – my wonderful, wonderful
family. To my extended family through David and Miras – I am so happy that you (and
your families) are part of ours and I can not explain how great it feels having you
interested in my progress and cheering me on. Thank you Fredriks family for always
being so wonderful, interested and encouraging. You make me feel like a superstar!
Thank you to the two best sisters anyone could ever have – Kim and Moa. Your bare

39
presence means so much to me and it does not matter how stressed I might be – with
you guys I am relaxed, because I know I do not have to accomplish anything or perform
around you, just be me. Love you dearly. An extra thanks to Kim and David for making
me and Moa aunties to the most wonderful little Albert and Betty on the planet!
A mere thank you does not seem enough when it comes to my fantastic parents,
but it will have to do; thank you for giving me the best childhood one can ever ask for
and a rock solid foundation of always feeling loved and safe. I only dare throwing myself
into almost anything because I know I always have you backing me up. I am very lucky
to have you as my parents and I love you so much. An extra thanks to mom for always
taking the time to answer my questions about plants and animals and thus founding my
interest for biology from the time I was a toddler. Deep inside I am sure we all knew that
I was going to be a scientist one day…
My last thank you is directed to the most important person in my life – Fredrik. I
guess it is kind of weird or cliché to say thank you for loving me, but - thank you for
loving me so unconditionally! Thanks for believing in me, for making everyday
(EVERYDAY!) sunny and fun, for being so truly good-hearted, for listening to my
looooong harangues about work, thanks for making my friends and family love you and
thanks for always making me feel like I am invincible! And people, listen to this – thank
you for (voluntarily!) taking care of aaaall the cleaning, planning, laundry, cooking and
shopping for the last THREE MONTHS of my PhD! What a man! YEAH! Moving to the
US will be a piece of cake with you by my side and I am so excited about all the fun we
have to look forward to together! And whatever career path you may choose – I will
support you wholeheartedly, just like you have supported me. I love you.
Ps. Oh, and a big thanks to me – keep doing what you are doing Isa, you kick ass! ☺
Isa ”Bäst-i-världen-och-så-jävulskt-snygg-och.smart” Lindgren, August 2010

40

41
REFERENCES
1. International Society for Developmental Origins of Health and Disease,
http://www.mrc.soton.ac.uk/dohad/, 2010.
2. Journal of Developmental Origins of Health and Disease
http://journalscambridgeorg/action/displayJournal?jid=DOH.
3. Altimiras J, Crossley DA, II. Control of blood pressure mediated by baroreflex
changes of heart rate in the chicken embryo (Gallus gallus). Am J Physiol 278: R980-
R986, 2000.
4. Altimiras J, Milberg P. Letter regarding article by Khan et al. "Predictive adaptive
responses to maternal high-fat diet prevent endothelial dysfunction but not hypertension
in adult rat offspring". Circulation: e166, 2005.
5. Auman JT, Seidler FJ, Slotkin TA. Regulation of fetal cardiac and hepatic beta -
adrenoceptors and adenylyl cyclase signaling: terbutaline effects. Am J Physiol Regul
Integr Comp Physiol 281: R1079-1089, 2001.
6. Auman JT, Seidler FJ, Tate CA, Slotkin TA. Are developing β-adrenoceptors able to
desensitize? Acute and chronic effects of beta -agonists in neonatal heart and liver. Am
J Physiol Regul Integr Comp Physiol 283: R205-217, 2002.
7. Balijepalli RC, Foell JD, Hall DD, Hell JW, Kamp TJ. Localization of cardiac L-type
Ca2+ channels to a caveolar macromolecular signaling complex is required for β2-
adrenergic regulation Proc Natl Acad Sci U S A 103: 7500-7505, 2006.
8. Baloglu E, KizIltepe Ö, Gürdal H. The role of Gi proteins in reduced vasorelaxation
response to β-adrenoceptor agonists in rat aorta during maturation. Eur J Pharmacol
564: 167-173, 2007.
9. Barker DJP. Fetal programming of coronary heart disease. Trends Endocrinol Metab
13: 364-368, 2002.
10. Barker DJP. The origins of the developmental origins theory. J Intern Med 261: 412-
417, 2007.
11. Barker DJP, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart
disease in England and Wales. The Lancet 327: 1077-1081, 1986.
12. Barker DJP, Osmond C, Winter PD, Margetts B, Simmonds SJ. Weight in infancy
and death from ischaemic heart disease. The Lancet 334: 577-580, 1989.
13. Bateson P, Barker DJP, Clutton-Brock T, Deb D, D'Udine B, Foley RA,
Gluckman P, Godfrey KM, Kirkwood T, Mirazón Lahr M, McNamara J, Metcalfe NB,

42
Monaghan P, Spencer HG, Sultan SE. Developmental plasticity and human health.
Nature 430: 419-421, 2004.
14. Bertram CE, Hanson MA. Animal models and programming of the metabolic
syndrome: Type 2 diabetes. Br Med Bull 60: 103-121, 2001.
15. Broberg CS, Giraud GD, Schultz JM, Thornburg KL, Hohimer AR, Davis LE.
Fetal anemia leads to augmented contractile response to hypoxic stress in adulthood.
Am J Physiol Regul Integr Comp Physiol 285: R649-655, 2003.
16. Brodde O-E, Bruck H, Leineweber K. Cardiac Adrenoceptors: Physiological and
Pathophysiological Relevance. J Pharmacol Sci 100: 323-337, 2006.
17. Cohen WR, Piasecki GJ, Jackson BT. Plasma catecholamines during hypoxemia
in fetal lamb. Am J Physiol Regul Integr Comp Physiol 243: R520-525, 1982.
18. Cohen WR, Piasecki GR, Cohn HE, Young JB, Jackson BT. Adrenal secretion of
catecholamines during hypoxemia in fetal lambs. Endocrinology 114: 383-390, 1984.
19. Cohn JN, Levine TB, Olivari MT, Garberg V, Lura D, Francis GS, Simon AB,
Rector T. Plasma norepinephrine as a guide to prognosis in patients with chronic
congestive heart failure. N Engl J Med 311: 819-823, 1984.
20. Crossley DA, II, Altimiras J. Ontogeny of autonomic control of cardiovascular
function in the domestic chicken Gallus gallus. Am J Physiol 279: R1091-R1098, 2000.
21. Crossley DA, II, Burggren WW, Altimiras J. Cardiovascular regulation during
hypoxia in embryos of the domestic chicken Gallus gallus. Am J Physiol Regul Integr
Comp Physiol 284: R219-226, 2003.
22. Daaka Y, Luttrell LM, Lefkowitz RJ. Switching of the coupling of the β2-adrenergic
receptor to different G proteins by protein kinase A. Nature 390: 88-91, 1997.
23. DeWitt TJ, Sheiner SM. Phenotypic plasticity. New York: Oxford University Press,
2004.
24. DeWitt TJ, Sih A, Wilson DS. Costs and limits of phenotypic plasticity. Trends Ecol
Evol 13: 77-81, 1998.
25. Dzimiri N. Regulation of β-Adrenoceptor Signaling in Cardiac Function and Disease.
Pharmacol Rev 51: 465-502, 1999.
26. Feldman AM, Jackson DG, Bristow MR, Cates AE, Van Dop C.
Immunodetectable levels of the inhibitory guanine nucleotide-binding regulatory proteins
in failing human heart: Discordance with measurements of adenylate cyclase activity and
levels of pertussis toxin substrate. J Mol Cell Cardiol 23: 439-452, 1991.

43
27. Fernandez-Twinn DS, Ekizoglou S, Wayman A, Petry CJ, Ozanne SE. Maternal
low-protein diet programs cardiac beta-adrenergic response and signaling in 3-mo-old
male offspring. Am J Physiol Regul Integr Comp Physiol 291: R429-436, 2006.
28. Fletcher AJW, Gardner DS, Edwards CMB, Fowden AL, Giussani DA.
Development of the ovine fetal cardiovascular defense to hypoxemia towards full term.
Am J Physiol Heart Circ Physiol 291: H3023-3034, 2006.
29. Forsdahl A. Are poor living conditions in childhood and adolescence an important
risk factor for arteriosclerotic heart disease? Br J Prev Soc Med 31: 91-95, 1977.
30. Giussani DA, Salinas CE, Villena M, Blanco CE. The role of oxygen in prenatal
growth: studies in the chick embryo. J Physiol 585: 911-917, 2007.
31. Giussani DA, Spencer JAD, Moore PJ, Bennet L, Hanson MA. Afferent and
efferent components of the cardiovascular reflex responses to acute hypoxia in term
fetal sheep. J Physiol 461: 431-449, 1993.
32. Gluckman PD, Hanson MA. Developmental origins of health and disease.
Cambridge: Cambridge University Press, 2006.
33. Gluckman PD, Hanson MA. The developmental origins of the metabolic syndrome.
Trends Endocrinol Metab 15: 183-187, 2004.
34. Gluckman PD, Hanson MA. The Fetal Matrix. Cambridge: Cambridge University
Press, 2005.
35. Gluckman PD, Hanson MA. Living with the Past: Evolution, Development, and
Patterns of Disease. Science 305: 1733-1736, 2004.
36. Gluckman PD, Hanson MA, Spencer HG. Predictive adaptive responses and
human evolution. Trends Ecol Evol 20: 527-533, 2005.
37. Gluckman PD, Hanson MA, Spencer HG, Bateson P. Environmental influences
during development and their later consequences for health and disease: implications for
the interpretation of empirical studies. Proc R Soc Biol Sci Ser B 272: 671-677, 2005.
38. Godfrey KM, Barker DJP. Fetal programming and adult health. Public Health Nutr 4:
611-624, 2001.
39. Hales CN, Barker DJ. Type 2 (non-insulin-dependent) diabetes mellitus: the thrifty
phenotype hypothesis. Diabetologia 35: 595-601, 1992.
40. Hanson M, Gluckman P. Endothelial dysfunction and cardiovascular disease: the
role of predictive adaptive responses. Heart 91: 864-866, 2005.

44
41. Hayes JS, Wyss VL, Schenck KS, Cohen ML. Effects of prolonged isoproterenol
infusion on cardiac and vascular responses to adrenoceptor agonists. J Pharmacol Exp
Ther 237: 757-763, 1986.
42. He J-Q, Balijepalli RC, Haworth RA, Kamp TJ. Crosstalk of β-Adrenergic Receptor
Subtypes Through Gi Blunts β-Adrenergic Stimulation of L-Type Ca2+ Channels in
Canine Heart Failure. Circ Res 97: 566-573, 2005.
43. Hermans E. Biochemical and pharmacological control of the multiplicity of coupling
at G-protein-coupled receptors. Pharmacol Ther 99: 25-44, 2003.
44. Heubach JF, Blaschke M, Harding SE, Ravens U, Kaumann AJ. Cardiostimulant
and cardiodepressant effects through overexpressed human β2-adrenoceptors in murine
heart: regional differences and functional role of β1-adrenoceptors. Naunyn
Schmiedebergs Arch Pharmacol 367: 380-390, 2003.
45. Hrbasova M, Novotny J, Hejnova L, Kolar F, Neckar J, Svoboda P. Altered
myocardial Gs protein and adenylyl cyclase signaling in rats exposed to chronic hypoxia
and normoxic recovery. J Appl Physiol 94: 2423-2432, 2003.
46. Huang M-H, Friend DS, Sunday ME, Singh K, Haley K, Austen KF, Kelly RA,
Smith TW. An intrinsic adrenergic system in mammalian heart. J Clin Invest 98: 1298-
1303, 1996.
47. Ji TH, Grossmann M, Ji I. G-protein coupled receptors. J Biol Chem 273: 17299-
17302, 1998.
48. Johnson M. The b-adrenoceptor. Am J Respir Crit Care Med 158: S146-S153, 1998.
49. Jordan D, Marshall J. Cardiovascular regulation. London: Portland Press, 1995.
50. Khan I, Dekou V, Hanson M, Poston L, Taylor P. Predictive adaptive responses to
maternal high-fat diet prevent endothelial dysfunction but not hypertension in adult rat
offspring. Circulation 110: 1097-1102, 2004.
51. Kiserud T, Jauniaux E, West D, Ozturk O, Hanson MA. Circulatory responses to
maternal hyperoxaemia and hypoxaemia assessed non-invasively in fetal sheep at 0.3-
0.5 gestation in acute experiments. BJOG 108: 359-364, 2001.
52. Kobilka BK. G protein coupled receptor structure and activation. Biochim Biophys
Acta 1768: 794-807, 2007.
53. Kuschel M, Zhou Y-Y, Cheng H, Zhang S-J, Chen Y, Lakatta EG, Xiao R-P. Gi
Protein-mediated Functional Compartmentalization of Cardiac β2-Adrenergic Signaling J
Biol Chem 274, 1999.

45
54. Kuzawa CW. Fetal origins of developmental plasticity: Are fetal cues reliable
predictors of future nutritional environments? Am J Hum Biol 17: 5-21, 2005.
55. Lambright DG, Noel JP, Hamm HE, Sigler PB. Structural determinants for
activation of the [alpha]-subunit of a heterotrimeric G protein. Nature 369: 621-628, 1994.
56. Lefkowitz RJ. Seven transmembrane receptors: something old, something new.
Acta Physiol 190: 9-19, 2007.
57. Lindgren I, Altimiras J. Chronic prenatal hypoxia sensitizes β-adrenoceptors in the
embryonic heart but causes postnatal desensitization. Am J Physiol Regul Integr Comp
Physiol 297: R258-264, 2009.
58. Lohse MJ, Engelhardt S, Eschenhagen T. What Is the Role of β-Adrenergic
Signaling in Heart Failure? Circ Res 93: 896-906, 2003.
59. Lucas A. Programming by early nutrition in man. In: The childhood environment and
adult disease. Chichester: John Wiley & Sons, 1991, p. 38-55.
60. Maher JT, Manchanda SC, Cymerman A, Wolfe DL, Hartley LH. Cardiovascular
responsiveness to beta-adrenergic stimulation and blockade in chronic hypoxia. Am J
Physiol 228: 477-481, 1975.
61. Marsh JD, Sweeney KA. β-adrenergic receptor regulation during hypoxia in intact
cultured heart cells. Am J Physiol 256: H275-H281, 1989.
62. Marshall JM. Peripheral chemoreceptors and cardiovascular regulation. Physiol Rev
74: 543-594, 1994.
63. McCudden CRM, Hains DR, Kimple J, Siderovski DP, Willard FS. G-protein
signaling: back to the future. Cell Mol Life Sci 62: 551–577, 2005.
64. Morisco C, Zebrowski DC, Vatner DE, Vatner SF, Sadoshima J. β-Adrenergic
Cardiac Hypertrophy is Mediated Primarily by the β1-Subtype in the Rat Heart. J Mol
Cell Cardiol 33: 561-573, 2001.
65. Mulder ALM, Miedema A, De Mey JGR, Giussani DA, Blanco CE. Sympathetic
control of the cardiovascular response to acute hypoxemia in the chick embryo. Am J
Physiol Regul Integr Comp Physiol 282: R1156-R1163, 2002.
66. Mulder ALM, Van Golde JC, Prinzen FW, Blanco CE. Cardiac output distribution in
response to hypoxia in the chick embryo in the second half of the incubation time. J
Physiol (London) 508: 281-287, 1998.
67. Nikolaev VO, Moshkov A, Lyon AR, Miragoli M, Novak P, Paur H, Lohse MJ,
Korchev YE, Harding SE, Gorelik J. β2-Adrenergic Receptor Redistribution in Heart
Failure Changes cAMP Compartmentation. Science 327: 1653-1657, 2010.

46
68. Palinski W, Napoli C. Impaired Fetal Growth, Cardiovascular Disease, and the
Need to Move on. Circulation 117: 341-343, 2008.
69. Petry CJ, Desai M, Ozanne SE, Hales CN. Early and late nutritional windows for
diabetes susceptibility. Proc Nutr Soc 56: 233-242, 1997.
70. Pierce KL, Premont RT, Lefkowitz RJ. Seven transmembrane receptors. Nat Rev
Mol Cell Biol 3: 639-650, 2002.
71. Pigliucci M. Phenotypic plasticity. Beyond nature and nurture. Baltimore
London: The John Hopkins University Press, 2001.
72. Portbury AL, Chandra R, Groelle M, McMillian MK, Elias A, Herlong JR, Rios M,
Roffler-Tarlov S, Chikaraish DM. Catecholamines act via a β-adrenergic receptor to
maintain fetal heart rate and survival. Am J Physiol Heart Circ Physiol 284: H2069-
H2077, 2003.
73. Post SR, Hammond HK, Insel PA. β-adrenergic Receptors and Receptor Signaling
in Heart Failure. Annu Rev Pharmacol Toxicol 39: 343-360, 1999.
74. Rasmussen SGF, Choi H-J, Rosenbaum DM, Kobilka TS, Thian FS, Edwards
PC, Burghammer M, Ratnala VRP, Sanishvili R, Fischetti RF, Schertler GFX, Weis
WI, Kobilka BK. Crystal structure of the human β2 adrenergic G-protein-coupled
receptor. Nature 450: 383-387, 2007.
75. Relyea RA. Costs of Phenotypic Plasticity. Am Nat 159: 272-282, 2002.
76. Remacle C, Bieswal F, Reusens B. Programming of obesity and cardiovascular
disease. Int J Obes Relat Metab Disord 28: S46-S53.
77. Rengo G, Lymperopoulos A, Koch W. Future G protein-coupled receptor targets
for treatment of heart failure. Curr Treat Options Cardiovasc Med 11: 328-338, 2009.
78. Rockman HA, Koch WJ, Lefkowitz RJ. Seven-transmembrane-spanning receptors
and heart function. Nature 415: 206-212, 2002.
79. Rohlicek CV, Viau S, Trieu P, Hébert TE. Effects of neonatal hypoxia in the rat on
inotropic stimulation of the adult heart. Cardiovasc Res 65: 861-868, 2005.
80. Romanoff AL. Biochemistry of the avian embryo. A quantitative analysis of prenatal
development. NY: John Wiley and sons, 1967.
81. Ruijtenbeek K, De Mey JGR, Blanco CE. The Chicken Embryo in Developmental
Physiology of the Cardiovascular System: A Traditional Model with New Possibilities. Am
J Physiol 283: 549-551, 2002.

47
82. Ruijtenbeek K, Janssen GMJ, Kessels CGA, Fazzi GE, Blanco CE, De Mey JGR.
Chronic hypoxia increases arterial sympathetic innervation in chick embryo. J Physiol
(London) 523P: 41P-42P, 2000.
83. Santos IN, Spadari-Bratfisch RC. Stress and cardiac β-adrenoceptors. Stress: The
International Journal on the Biology of Stress 9: 69-84, 2006.
84. Schutzer WE, Mader SL. Age-related changes in vascular adrenergic signaling:
clinical and mechanistic implications. Ageing Res Rev 2: 169-190, 2003.
85. Steinberg SF. The Molecular Basis for Distinct β-Adrenergic Receptor Subtype
Actions in Cardiomyocytes. Circ Res 85: 1101-1111, 1999.
86. Symonds ME, Stephenson T, Gardner DS, Budge H. Long-term effects of
nutritional programming of the embryo and fetus: mechanisms and critical windows.
Reprod Fertil Dev 19: 53-63, 2006.
87. Tintu A, Rouwet E, Verlohren S, Brinkmann J, Ahmad S, Crispi F, van Bilsen M,
Carmeliet P, Staff AC, Tjwa M, Cetin I, Gratacos E, Hernandez-Andrade E, Hofstra
L, Jacobs M, Lamers WH, Morano I, Safak E, Ahmed A, le Noble F. Hypoxia Induces
Dilated Cardiomyopathy in the Chick Embryo: Mechanism, Intervention, and Long-Term
Consequences. PLoS ONE 4: e5155, 2009.
88. Wallis JW, Aerts J, Groenen MAM, Crooijmans RPMA, Layman D, Graves TA,
Scheer DE, Kremitzki C, Fedele MJ, Mudd NK, Cardenas M, Higginbotham J, Carter
J, McGrane R, Gaige T, Mead K, Walker J, Albracht D, Davito J, Yang S-P, Leong S,
Chinwalla A, Sekhon M, Wylie K, Dodgson J, Romanov MN, Cheng H, de Jong PJ,
Osoegawa K, Nefedov M, Zhang H, McPherson JD, Krzywinski M, Schein J, Hillier
L, Mardis ER, Wilson RK, Warren WC. A physical map of the chicken genome. Nature
432: 761-764, 2004.
89. Wallukat G. The β-Adrenergic Receptors. Herz 27, 2002.
90. van der Heyden MAG, Wijnhoven TJM, Opthof T. Molecular aspects of adrenergic
modulation of cardiac L-type Ca2+ channels. Cardiovasc Res 65: 28-39, 2005.
91. Wassink G, Bennet L, Booth LC, Jensen EC, Wibbens B, Dean JM, Gunn AJ.
The ontogeny of hemodynamic responses to prolonged umbilical cord occlusion in fetal
sheep. J Appl Physiol 103: 1311-1317, 2007.
92. Wells JCK. Environmental Quality, Developmental Plasticity and the Thrifty
Phenotype: A Review of Evolutionary Models. Evol Bioinform 3: 109-120, 2007.
93. Wells JCK. Flaws in the theory of predictive adaptive responses. Trends Endocrinol
Metab 18: 331-337, 2007.

48
94. Wells JCK. Is early development in humans a predictive adaptive response
anticipating the adult environment? Trends Ecol Evol 21: 424-425, 2006.
95. Vetter IR, Wittinghofer A. The Guanine Nucleotide-Binding Switch in Three
Dimensions. Science 294: 1299-1304, 2001.
96. White M, Roden R, Minobe W, Khan MF, Larrabee P, Wollmering M, Port JD,
Anderson F, Campbell D, Feldman AM. Age-related changes in β-adrenergic
neuroeffector systems in the human heart. Circulation 90: 1225-1238, 1994.
97. Villamor E, Kessels CG, Ruijtenbeek K, van Suylen RJ, Belik J, de Mey JG,
Blanco CE. Chronic in ovo hypoxia decreases pulmonary arterial contractile reactivity
and induces biventricular cardiac enlargement in the chicken embryo. Am J Physiol
Regul Integr Comp Physiol 287: R642-651, 2004.
98. Voelkel NF, Hegstrand L, Reeves JT, McMurty IF, Molinoff PB. Effects of hypoxia
on density of β-adrenergic receptors. J Appl Physiol 50: 363-366, 1981.
99. Wong SK-F. G Protein Selectivity Is Regulated by Multiple Intracellular Regions of
GPCRs. NeuroSignals 12: 1-12, 2002.
100. Xiao R-P, Avdonin P, Zhou Y-Y, Cheng H, Akhter SA, Eschenhagen T,
Lefkowitz RJ, Koch WJ, Lakatta EG. Coupling of β2-Adrenoceptor to Gi Proteins and
Its Physiological Relevance in Murine Cardiac Myocytes. Circ Res 84: 43-52, 1999.
101. Xiao R-P, Cheng H, Zhou Y-Y, Kuschel M, Lakatta EG. Recent Advances in
Cardiac β2-Adrenergic Signal Transduction. Circ Res 85: 1092-1100, 1999.
102. Zhou YY, Cheng H, Bogdanov KY, Hohl C, Altschuld R, Lakatta EG, Xiao RP.
Localized cAMP-dependent signaling mediates β2-adrenergic modulation of cardiac
excitation-contraction coupling. Am J Physiol Heart Circ Physiol 273: H1611-1618, 1997.
103. Zhu W-Z, Zheng M, Koch WJ, Lefkowitz RJ, Kobilka BK, Xiao R-P. Dual
modulation of cell survival and cell death by β2-adrenergic signaling in adult mouse
cardiac myocytes Proc Natl Acad Sci U S A 98: 1607-1612, 2001.
104. Zhu W, Zeng X, Zheng M, Xiao R-P. The enigma of β2-adrenergic receptor
signaling in the heart. The good, the bad, and the ugly. Circ Res 97: 507-509, 2005.
105. Zoer B, Cogolludo AL, Perez-Vizcaino F, De Mey JG, Blanco CE, Villamor E.
Hypoxia sensing in the fetal chicken femoral artery is mediated by the mitochondrial
electron transport chain. Am J Physiol Regul Integr Comp Physiol 298: R1026-1034.