British Journal of Anaesthesia - MedSpec · BJA (not included) dealing with fluid and sodium loads...
60
BJA British Journal of Anaesthesia South African Excerpts Edition Volume 14 Number 2 2014 pages 53-108 MedSpec Publishing • β-Blockers and cardiac protection: 5 yr on from POISE • Fluid management in association with neonatal surgery: even tiny guys need their salt • Flexion-rotation manoeuvre increases dimension of the acoustic target window for paramedian thoracic epidural access • Comparison of the effects of albumin 5%, hydroxyethyl starch 130/0.4 6%, and Ringer’s lactate on blood loss and coagu- lation after cardiac surgery surgery in patients with moderate vs deep neuro- muscular block British Journal of Anaesthesia Ravi P. Mahajan SOUTH AFRICAN EXCERPTS EDITION Volume 14 Number 2 2014 FACULTY OF PAIN MEDICINE COLLEGE OF ANAESTHETISTS OF IRELAND
Transcript of British Journal of Anaesthesia - MedSpec · BJA (not included) dealing with fluid and sodium loads...

BJA British Journal of Anaesthesia South A
frican Excerpts Edition Volume 14 N
umber 2 2014 pages 53-108 M
edSpec Publishing
• β-Blockers and cardiac protection: 5 yr on from POISE
• Fluid management in association with neonatal surgery: even tiny guys need their salt
• Flexion-rotation manoeuvre increases dimension of the acoustic target window for paramedian thoracic epidural access
• Comparison of the effects of albumin 5%, hydroxyethyl starch 130/0.4 6%, and Ringer’s lactate on blood loss and coagu-lation after cardiac surgery surgery in patients with moderate vs deep neuro-muscular block
British Journal of Anaesthesia Ravi P. Mahajan
SOUTH AFRICAN EXCERPTS EDITION
Volume 14 Number 2 2014
BJA111/3
British Journal of Anaesthesia Volum
e 111 Num
ber 3 September 2013 Pages 321–522
2
ROYAL COLLEGE OF ANAESTHETISTS
FACULTY OF PAIN MEDICINE
COLLEGE OF ANAESTHETISTS OF IRELAND
1
Volume 111, Number 3, September 2013 ISSN 0007-0912 (Print) 1471-6771 (Online)
In this month’s issueNew DOA monitor • Regional anaesthesia outcomes • Quality improvement • HES controversy
Bjaint_111_3_cover.indd 1 10/08/13 11:00 AM


53
BJA EXCERPTS
SOUTH AFRICAN EDITIONPublisherReni RouncivellTel: (012) 657 2327 / Fax: 086 561 5122Cell: 082 441 [email protected]
AdvertisingLelani AdendorffCell: 079 512 [email protected]
Subscriptions & AccountsElizabeth VersteegCell: 072 189 [email protected]
Private Bag X1036, LytteltonSouth Africa 0140
For address changes please contact:Cally Lamprecht: [email protected]
© The Author. Published by Oxford University Press on behalf of the British Journal of Anaesthesia This Specialized Edition is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned, specifically the rights for translation, reprinting, reuse of illustrations, broadcasting, reproduction on CD-ROM, microfilm, online publication, storage in data banks or in any other way.This Specialized Edition contains selected items originally published in the British Journal of Anaesthesia (“BJA”) and is published by arrangement with the British Journal of Anaesthesia on behalf of the Journal and its publisher Oxford University Press. The Chinese Society of Anesthesiology (“CSA”) has obtained the permission of the British Journal of Anaesthesia and OPL to publish the Chinese language Specialized Edition of BJA to distribute to medical professionals within China.No part of this Specialized Edition may be reproduced, electronically or mechanically, including photocopying, resending or in any information storage and retrieval system, or transmitted in any form, by any means, without prior written permission from OPL and the British Journal of Anaesthesia.Please send any permissions/reprint requests to: [email protected] The use of registered names, trademarks etc within this Specialized Edition does not imply, even in the absence of a specific statement, that such names are exempt for the relevant laws and regulations and therefore free for general use.Although great care has been taken in compiling the content of this Specialized Edition, neither OPL nor the British Journal of Anaesthesia are responsible or in any way liable for the accuracy of the information, for any errors, omissions or inaccuracies, or for any consequences arising therefore. CSA is the sole entity responsible for the content published in the Specialized Edition.The publication of an advertisement in this Specialized Edition does not constitute on the part of OPL and the British Journal of Anaesthesia a guarantee or endorsement of the quality or value of the advertised products or services described therein or any of the representations or the claims made by the advertisers with respect to such products or services. No responsibility is assumed by OPL for any injury and/or damage to persons or property as a result of any actual or alleged libellous statements, infringement of intellectual property or privacy rights, or products liability, whether resulting from negligence or otherwise, or from any use or operation of any ideas, instructions, procedures or methods contained in the material therein.
CommentThis edition of BJA(SA) contains a number of articles that are of considerable relevance to clinical practice. An excellent editorial from two well-known experts in the field reviews the current status of the use of beta-blockers in the perioperative period. The editorial ends with a series of practice pointers that can usefully be used to guide clinicians faced with the decision of whether or not to introduce beta-blockade in the immediate perioperative period1. It should be noted that the conclusions are not quite as clear-cut as the original POISE study might have suggested and that the use of differing timings, as well as alternative beta-blocking agents may alter clinical practice in this area. What is clear is that the era of almost uniformly administered perioperative beta-blockade for patients at risk of myocardial ischaemic injury is over.
Another practice-changing intervention that has evolved over the last few years is the revision of fluid composition in paediatrics. An editorial reviews a publication in BJA (not included) dealing with fluid and sodium loads in the perioperative phase2. For many years it was taught that low-sodium containing solutions were appropriate for perioperative paediatric fluid therapy, based on the original studies that were conducted on non-surgical patients. The recognition of hyponatraemia as a major post-operative complication in paediatrics has resulted in a change in emphasis towards crystalloid solutions that contain concentrations of sodium that resemble those in the plasma. It is of interest that the preoperative management of these patients does not appear to pose a risk of hyponatraemia and it is only once the surgical stress occurs that the rise in ADH and other physiological responses to trauma poses the risk that hyponatraemic solutions may result in a potentially lethal reduction in serum sodium in the post-operative period. The perioperative use of solutions containing normal plasma concentrations of sodium in paediatrics should not be routine.
Arbitrary decisions on coagulation management have frequently been controversial, no more so than in the complex field of liver transplantation. Thrombelastography has, for many years, been the mainstay of coagulation management during this procedure and the greater sophistication offered by the ROTEM device may enhance the ability of anaesthetists to make high-quality decisions. The article by Song et al3 examines the utility of very early results from the ROTEM and concludes that excellent data of good clinical relevance can be obtained within the first five minutes of the test allowing early and precise regulation management.
Finally, an interesting ultrasound article has examined positioning of patients for the placement of low-thoracic epidural catheters4. The innovation of a rightward twist of the spine in addition to good flexion appears to offer the best potential access to the thoracic epidural space as judged in this ultrasound study. Whether or not this will apply to upper thoracic anatomy remains to be evaluated, but this approach appears to be one well worth considering where thoracic epidural catheters are to be placed.
1 Foex P, Sear JW. II. β-Blockers and cardiac protection: 5 yr on from POISE. British Journal of Anaesthesia 2014; 112: 206-10
2 Lönnqvist P-A. III. Fluid management in association with neonatal surgery: even tiny guys need their salt. British Journal of Anaesthesia 2014; 112: 404-6
3 Song J-G, Jeong S-M, Jun I-G, Lee H-M, Hwang G-S. Five-minute parameter of thromboelastometry is sufficient to detect thrombocytopenia and hypofibrinogenaemia in patients undergoing liver transplantation. British Journal of Anaesthesia 2014; 112: 290-7
4 Ramsay N, Walker J, Tang R, Vaghadia H, Sawka A. Flexion-rotation manoeuvre increases dimension of the acoustic target window for paramedian thoracic epidural access. British Journal of Anaesthesia 2014; 112: 556-62
BJA EXCERPTS SOUTH AFRICAN EDITION VOLUME 14 NUMBER 2 2014
Editor, South African Excerpts Edition
Professor MFM James, Emeritus Professor, Department of Anaesthesia, University of Cape Town, Faculty of Health Sciences

Editorial Board 2014Editor-in-ChiefR. P. Mahajan, University of Nottingham, UK
EditorsA. R. Absalom, University Medical Center Groningen,The Netherlands
L. Colvin, University of Edinburgh, UK
H. F. Galley, University of Aberdeen, UK
J. G. Hardman, University of Nottingham, UK
H. C. Hemmings, Cornell University, New York, USA
P. S. Myles, Alfred Hospital and Monash University,Australia
M. M. R. F. Struys, University Medical Center Groningen,The Netherlands
J. P. Thompson, University of Leicester, UK
E-letter editor: I. K. Moppett, University of Nottingham, UK
Podcast editor: R. Thomas, London Deanery, UK
Board MembersT. Asai, Kansai Medical University, Japan
A. R. Bodenham, Leeds Teaching Hospitals, UK
D. J. Buggy, Mater Misericordiae University Hospital andUniversity College Dublin, Ireland
K. Hirota, University of Hirosaki, Japan
P. M. Hopkins, University of Leeds, UK
S. J. Howell (Treasurer), University of Leeds, UK
H. Jones, Vice President, Royal College of Anaesthetists
D. G. Lambert (Secretary), University of Leicester, UK
J. A. Langton (Editor-in-Chief Continuing Education inAnaesthesia, Critical Care & Pain), Plymouth Hospitals NHSTrust, UK
P. A. Lonnqvist, Lingrens Children’s Hospital, Stockholm,Sweden
D. Ma, Imperial College London, UK
P. Marhofer, University of Vienna, Austria
A. M. Moller, University of Copenhagen, Denmark
M. G. Mythen, University College London, UK
D. Nolan, Vice President, Royal College of Anaesthetists
E. P. O’Sullivan, President, College of Anaesthetists of Ireland
C. S. Reilly, University of Sheffield, UK
D. J. Rowbotham, University of Leicester, UK
R. D. Sanders, University College London, UK
S. L. Shafer, Columbia University, New York, USA
J. R. Sneyd, Plymouth University Peninsula Schools ofMedicine and Dentistry, Plymouth, UK
J.-P. van Besouw, President, Royal College of Anaesthetists
N. R. Webster (Chairman), University of Aberdeen, UK
Production StaffH. J. Lamb, Senior Production Editor, Oxford University Press K. Heath, Production Editor, Oxford University Press
Please visit the Journal’s World Wide Web site at http://bja.oxfordjournals.org
MIX
FSC® C007785
®
British Journal of Anaesthesia BJA5454


56
BJA E X C E R P T S
For any reference/citations from this selection of items, the source must be given as the original article with full bibliographic detail as given at the top of the first page of each article
SOUTH AFRICAN EDITION Volume 14 Number 2 2014
EDITORIALS
β-Blockers and cardiac protection: 5 yr on from POISEP. Foex and J.W. Sear
Fluid management in association with neonatal surgery: even tiny guys need their saltP.-A. Lönnqvist
REGIONAL ANAESTHESIA
Flexion-rotation manoeuvre increases dimension of the acoustic target window for paramedian thoracic epidural accessN. Ramsay, J.Walker, R. Tang, H. Vaghadia and A. Sawka
CARDIOVASCULAR
Comparison of the effects of albumin 5%, hydroxyethyl starch 130/0.4 6%, and Ringer’s lactate on blood loss and coagulation after cardiac surgeryK. Skhirtladze, E. M. Base, A. Lassnigg, A. Kaider, S. Linke, M. Dworschak and M. J. Hiesmayr
CLINICAL PRACTICE
Evaluation of surgical conditions during laparoscopic surgery in patients with moderate vs deep neuro-muscular blockC. H. Martini, M. Boon, R. F. Bevers, L. P. Aarts and A. Dahan
Five-minute parameter of thromboelastometry is sufficient to detect thrombocytopenia and hypofibrinoge-naemia in patients undergoing liver transplantationJ.-G. Song, S.-M. Jeong, I.-G. Jun, H.-M. Lee and G.-S. Hwang
CONTENTS
61-65
67-69
71-77
78-87
89-96
97-104





1
EXCELLENCE IN EVIDENCE
ADVERTISING
Advertising opportunities in association with our journals include:
■ Display advertising in print and online, with option to geo-target
■ Classified advertising (both in print and online)
■ Sponsored email table of content alerts (eTOCs)
■ Inserts and wrap arounds
For more information visit:
www.oxfordjournals.org/corporate
Email: [email protected]
Tel: +44 (0) 1865 355190
REACH YOUR TARGET AUDIENCE
theglobal endothelial function. However, a development of new(alternative) strategies for the diagnostics and treatment ofendothelial dysfunction in various diseases is required.
Declaration of interestNone declared.
References1 Galley HF, Webster NR. Physiology of the endothelium. Br J Anaesth
2004; 93: 105–13
2 Davignon J, Ganz P. Role of endothelial dysfunction in atheroscler-osis. Circulation 2004; 109: III27–32
3 Johnstone MT, Creager SJ, Scales KM, Cusco JA, Lee BK,Creager MA. Impaired endothelium-dependent vasodilation inpatients with insulin-dependent diabetes mellitus. Circulation1993; 88: 2510–6
4 Boulanger CM. Secondary endothelial dysfunction: hypertensionand heart failure. J Mol Cell Cardiol 1999; 31: 39–49
5 PetersN, Freilinger T,OpherkC, PfefferkornT,DichgansM.EnhancedL-arginine-induced vasoreactivity suggests endothelial dysfunc-tion in CADASIL. J Neurol 2008; 255: 1203–8, doi: 10.1007/s00415-008-0876-9. Epub June 13, 2008
6 Knottnerus IL, TenCateH, Lodder J, Kessels F, vanOostenbruggeRJ.Endothelial dysfunction in lacunar stroke: a systematic review.Cerebrovasc Dis 2009; 27: 519–26
7 Scherbakov N, Sandek A, Martens-Lobenhoffer J, et al. Endothelialdysfunction of the peripheral vascular bed in the acute phaseafter ischemic stroke. Cerebrovasc Dis 2012; 33: 37–46
8 Poredos P, Jezovnik MK. Testing endothelial function and its clinicalrelevance. J Atheroscler Thromb 2013; 20: 1–8
9 Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasive detec-tion of endothelial dysfunction in children and adults at risk of ath-erosclerosis. Lancet 1992; 340: 1111–5
10 Laurent S, Lacolley P, Brunel P, Laloux B, Pannier B, Safar M. Flow-dependent vasodilation of brachial artery in essential hyperten-sion. Am J Physiol 1990; 258 (4 Pt 2): H1004–11
11 Corretti MC, Anderson TJ, Benjamin EJ, et al. International BrachialArtery Reactivity Task Force. Guidelines for the ultrasound assess-ment of endothelial-dependent flow-mediated vasodilation ofthe brachial artery: a report of the International Brachial ArteryReactivity Task Force. J Am Coll Cardiol 2002; 39: 257–65
12 Kuvin JT, Patel AR, Karas RH. Need for standardization of non-invasive assessment of vascular endothelial function. Am Heart J2001; 141: 327–8
13 Kuvin JT, Patel AR, Sliney KA, et al.Assessment of peripheral vascu-lar endothelial function with finger arterial pulse wave amplitude.Am Heart J 2003; 146: 168–74
14 Bonetti PO, Pumper GM, Higano ST, Holmes DR Jr, Kuvin JT,Lerman A. Noninvasive identification of patients with early coron-ary atherosclerosis by assessment of digital reactive hyperemia.J Am Coll Cardiol 2004; 44: 2137–41
15 Hamburg NM, Keyes MJ, Larson MG, et al. Cross-sectional relationsof digital vascular function to cardiovascular risk factors in the Fra-mingham Heart Study. Circulation 2008; 117: 2467–74
16 Bergstrom A, Staalsø JM, Romner B, Olsen NV. Impaired endothelialfunction after aneurysmal subarachnoid haemorrhage correlatesto the arginine:asymmetric dimethylarginine ratio. Br J Anaesth2014; 112: 311–18
17 Bode-Boger SM, Scalera F, Ignarro LJ. The L-arginine paradox: im-portance of the L-arginine/asymmetrical dimethylarginine ratio.Pharmacol Ther 2007; 114: 295–306
18 Staalsø JM, Bergstrom A, Edsen T, Weikop P, Romner B, Olsen NV.Low plasma arginine:asymmetric dimethyl arginine ratios predictmortality after intracranial aneurysm rupture. Stroke 2013; 44:1273–81
British Journal of Anaesthesia 112 (2): 206–10 (2014)Advance Access publication December 15, 2013 . doi:10.1093/bja/aet437
EDITORIAL II
b-Blockers and cardiac protection: 5 yr on from POISEP. Foex and J. W. Sear*
Nuffield Department of Anaesthetics, University of Oxford, John Radcliffe Hospital, Oxford OX3 9DU, UK
* E-mail: [email protected]
For many years, b-blockers have been regarded as the bestdrugs to protect patients with, or at risk for, coronary heartdisease, from perioperative major adverse cardiac events(MACE). This was based on observational studies, randomizedcontrolled trials (RCTs), experts’ opinions, and guidelines. Thestrongest support was expressed in the 1997 guidelines ofthe American College of Physicians,1 after very encouraging
results after administration of atenolol before non-cardiacsurgery byManganoand colleagues.2 Theguideline advocatedthe administration of atenolol to all patients with, or at riskfor, coronary disease undergoing surgery. In the USA, initia-tion of perioperative b-blockade was regarded as having thegreatest strength of evidence in its favour.3 However, a lesssupportive view was expressed in the American College of
BJA Editorial II
206
61

Cardiology/American Heart Association (ACC/AHA) guideline2007.4 b-Blockers were considered to protect against myocar-dial ischaemia (as we had found in an RCT 20 yr earlier),5 theymay reduce the risk ofmyocardial infarction and cardiac deathin patients with known coronary artery disease. This followedthe realization that someRCTs did not showstatistically signifi-cant cardiac protection. Indeed, several studies did not showastatistically significant reduction in cardiac mortality,6–10 ornon-fatal myocardial infarction.11–15
A meta-analysis by Devereaux and colleagues16 of all RCTsof perioperative b-blockade failed to show statistically signifi-cant protection. These data were the justification for thePOISE trial.
In 2008, the POISE study,17 the largest RCT in perioperativemedicine ever undertaken, showed statistically and clinicallysignificant cardiac protection but revealed an increase in all-cause mortality, disabling strokes, and hypotension. Becauseof the much smaller size of all previous RCTs, these risks mayhave been present but had never reached statistical signifi-cance. Subsequent meta-analysis confirmed both cardiacprotection and significant risks associated with the initiation ofb-blockadeshortlybeforesurgery.18The resultofPOISEwascri-ticized, especially the potential for high doses ofmetoprolol tobe administered, and the choice of slow-releasemetoprolol.19
In 2009, new guidelines on the management of patientswith heart disease undergoing non-cardiac surgery were pub-lished on both sides of the Atlantic by the ACCF/AHA20 andtheEuropeanSocietyof Cardiology (ESC) endorsedby theEuro-pean Society of Anaesthesiology (ESA),21 respectively. Bothsets of guidelines recommended to continue long-term treat-ment with b-blockers, to avoid high-dose b-blockade, andto consider the introduction of b-blockers in patients withknowncoronaryarterydisease, patientswith reversible ischae-mia on stress test, and in those at risk for coronary arterydisease undergoing high-risk surgery, especially vascularsurgery.20 The European guideline regarded the above recom-mendationsasClass I (asopposed toClass IIa for theAmericanguidelines) and was more liberal suggesting that b-blockadecould be initiated in patients undergoing intermediate-risksurgery (Class IIa).21 Both groups of experts advocated titra-tion of b-blockade to slow heart rates (ESC 60–70 beatsmin21; ACCF/AHA 60–80 beats min21) with the limit of atleast 100 mm Hg systolic arterial pressure before administra-tion of the next dose of b-blocker (ESC), or no hypotension(ACCF/AHA). Both advocated starting b-blockade at least 7days, preferably 30 days before surgery. However, there isonly limited supporting evidence for this approach.
In respect of the recommendation to continue chronicb-blockade perioperatively, there is good evidence fromobser-vational studies22–24 and one RCT25 to support the continuingof chronic b-blockade during anaesthesia and surgery. Thecase for discontinuing therapy was first put forward by Cran-dell26 who stated that ‘antihypertensive drugs interfered withhaemodynamic adjustments and could cause profound car-diovascular collapse in patients subjected to the stress of an-aesthesia and surgery’. This approach was extended tob-blockers.27 However, more recent studies have shown that
discontinuing therapy is associated with significant increasesin perioperative morbidity and mortality.22–24 Indeed, main-taining chronic therapyhasbeen shownbyWallaceandcollea-gues24 to be associated with a similarly improved outcomewhen compared with patients receiving acute perioperativeb-blockade. In contrast, Ellenberger and colleagues28 foundthat chronic therapy was superior to the introduction ofb-blockers within the first 2 days of surgery.
We are now in 2013. The interpretation of existing data,coupled with new research, needs to be reconsidered. First,there is the problem of the alleged intellectual misconductrelating to the studies from Poldermans and colleagues atthe Erasmus Medical Center. However, the correspondencebetween Poldermans and the Editor of the American Journalof Medicine29 in response to the commentary by Chopra andEagle30 does nothing to throw a clearer light on the overallpicture.
Newmeta-analysisThe second new development is the publication of a newmeta-analysis by Bouri and colleagues31 which excludeswhat they regard as ‘insecure’ studies—namely, DECREASE32
and DECREASE IV33 trials from the Erasmus Medical Center.Based on data from nine other clinical trials (10 529 patients),the investigators report that the treatment of patients under-going non-cardiac surgery and receiving b-blockers accordingto the existing recommendations of the AACF/AHA or ESCguidelines was subject to a significant 27% increase in the all-causemortality risk. Translated into figures relevant to the UK,thiswould imply that thedrugs couldhave resulted in.10 000surgical deaths per year had guidelines been strictly followed!In addition, their use may be associated with a 73% increasein the incidence of non-fatal stroke, and 51% increased inci-dence of hypotension. On the benefit side, there was a 27%reduction in non-fatal myocardial infarction. If we return tothe analysis of Bangalore and colleagues,18 they show similaroutcomes, where any benefit of b-blockade is driven by trialswith a high intrinsic risk for bias—namely, DECREASE andDECREASE IV.
When should we start b-blockersIn respect of the early start of b-blockade advocated by thecurrent guidelines,20 21 only four studies have used this ap-proach,8 13 32 33 and in two of them, b-blockade was notshown to be beneficial. In contrast, in two studies from Polder-mans’ group, early administration (at least 7 days beforesurgery) was beneficial. All the other RCTs started b-blockadethe day of surgery. While an early start is logical, new data donot support this. Wallace and colleagues24 collated observa-tion in more than 37 000 non-cardiac operations. A protocolfor perioperative b-blockade was available in their institutionbutwasnotmandatory.Patientswere followed for1yr. Survivalwas best for those who had been given a b-blocker at the timeof surgery, followed by those who had been maintained onb-blockade. Poorer survival was noted for those not on ab-blocker; worst outcome (unsurprisingly) was in those in
Editorial II BJA
207
62

whom b-blockade had been withdrawn. Thus, in the groups ofpatients in whom b-blockade is supported by the currentguidelines, late start, if early start was not possible shouldnot preclude the introduction of b-blockade.
Another indication for perioperative b-blockade may be toobtund the adrenergic responses to noxious stimuli or to reducemyocardial ischaemia. Our analysis of 14 studies (n¼1298patients) showsthis single-dose treatment tobeeffective in re-ducing perioperative myocardial infarction [odds ratio (OR)0.17 (0.044–0.203), seven studies] and myocardial ischaemia[0.22 (0.135–0.353), eight studies]. These treatments werenot associated with significant hypotension or bradycardia.
b-Blocker formulationThere has been controversy in respect of the choice of slow-release metoprolol in POISE. A large observational study byWallace and colleagues34 has shown in 3789 patients on con-tinuing b-blockade that atenolol was associated with betterprotection in terms of 30 day and 1 yrmortality thanmetopro-lol. Today, bisoprolol is used increasingly frequently and mayalso prove to be more protective than metoprolol.
Existing guidelinesGuidelines20 21 underline that initiating b-blockade periopera-tively should be limited to high-risk patients. This was largelybasedon thedata fromavery largecohort studybyLindenauerand colleagues.35 The revised cardiac risk index (RCRI) wasused to categorize cardiac risk. As the data concerned theyears 2000 and 2001 and the management of patients withcoronary artery disease have changed with the introductionof coronary stenting, especially in patientswith acute coronarysyndromes, it is interesting to see that observational data col-lected between 2005 and 2010 by London and colleagues36
confirm that the benefits of b-blockade are only significantin patients with an RCRI of more than 1. The ACCF/AHA guide-line20 recommended perioperative b-blockade in patients un-dergoing high-risk surgery, especially vascular surgery. However,the observational study of London and colleagues36 did notconfirmbenefits of exposure tob-blockade in vascular surgicalpatients irrespective of theRCRI. This is surprising andmore re-search is needed in this group of patients.
b-Blocker titrationThe recommendation of close titration of b-blockade with thegoal of a heart rate of 60–70 beats min21 is in principle desir-able because of the need tomaintain a long diastolic period tomaximizeflow innarrowedcoronaryarteries. However, there isthe riskof severe bradycardiaand cardiac failure asobserved ina meta-analysis by Beattie and colleagues.37 As hypotensionwas found in POISE to be an important contributor to peri-operative strokes, the suggestion that 100 mm Hg systolic ar-terial pressure is sufficient before giving the next dose of theb-blocker is at least questionable. The current recommenda-tion of the ACCF/AHA towithhold theb-blocker if there is hypo-tension (undefined) seems more logical as even moderately
hypertensive patients presenting for surgery may suffer com-plications if their arterial pressure decreases to and remainsat 100 mm Hg for a prolonged period.
Anaemia and b-blockadeAn observational study by Beattie and collagues38 has shownthat as the nadir of haemoglobin decreases, the risk of MACEincreases as the reduction reaches 60% of control and ismuch higher in b-blocked than in non-b-blocked patients.Similarly, LeManachandcolleagues39 found thatperioperativeb-blockade was associated with an overall reduction in post-operative cardiac events. Hence, while cardiac protection wasobserved in those patients with low perioperative bleeding,patients receivingb-blockerswhoexperienced severebleedinghadhighermortalityandan increased frequencyofmultiorgandysfunction syndrome. These important observations requireconfirmation in future studies because they may indicate aneed to revise the threshold for blood transfusion in patientson b-blockers.
What for the future?On August 5, 2013, a joint statement by the ACCF/AHA andESC40 stated: ‘Our respective committees are undertaking acareful analysis of all relevant validated studies and always in-corporate new trials and meta-analyses into our evidencereview. In the interim, our current joint position is that the ini-tiation of beta-blockers in patients who will undergo non-cardiac surgery should not be considered routine, but shouldbe considered carefully by each patient’s treating physicianon a case-by-case basis’.
Beforenewguidelinesare published,whatmaybea reason-able approach to perioperative b-blockade?
† Currentb-blockade should bemaintained,with theprevi-ously mentioned caveat of a potential risk in patientsdeveloping severe perioperative anaemia.
† Initiating b-blockade should be limited to high-riskpatients undergoing high-risk surgery, especially inthose who would be given b-blockade for co-existingmedical reasons, that is, known coronary artery disease,reversible ischaemia on stress test.
† High-dose b-blockade should be avoided.† Titration is recommended, but the ACCF/AHA guide-
line for heart rate (60–80 beats min21) is probablymore appropriate owing to the risk of bradycardia withhigher doses of b-blockade that can occur with thelower limit (60–70 beats min21) advocated by the ESCguideline.
† Titration should include clear instruction for each patientas to the level of arterial pressure required before thenext dose of the b-blocker is given, as a function of pre-operative arterial pressure, as avoidance of hypotensionis important.
† Startingb-blockade and titrating its effects overat least 7days is logical. However, startingb-blockadeon thedayofsurgery may still be legitimate where there is a clear
BJA Editorial II
208
63

indication, such as the administration of a single preme-dicant dose to prevent exaggerated haemodynamicresponses to laryngoscopy and intubation; or provideanxiolysis by reducing adrenergic responses; or preventperioperative myocardial ischaemia.
† Metoprolol appears to be inferior to atenolol and in thefuture, bisoprolol is likely to become the drug of choiceonce more research has been carried out.
† As anaemia has been shown to markedly increase therisk of adverse cardiac events and mortality in theface of b-blockade, consideration should be given to in-crease the threshold for blood transfusion in thesepatients.
Declaration of interestNone declared.
References1 PaldaVA,DetskyAS. Perioperativeassessmentandmanagementof
risk fromcoronaryarterydisease.AnnInternMed1997;127: 313–28
2 ManganoDT, LayugEL,WallaceA, Tateo I. Effect ofatenolol onmor-tality and cardiovascularmorbidity after noncardiac surgery. Multi-center Study of Perioperative Ischemia Research Group. N Engl JMed 1996; 335: 1713–20
3 Making Health Care Safer: A Critical Analysis of Patient Safety Prac-tices.EvidenceReport/TechnologyAssessment.Number43.Chapter57. Practices rated by strength of evidence, Table 57.1, 622. Rock-ville, MD: Agency for Healthcare Research and Quality. U.S. Depart-ment of Health and Human Services. Available from http://archive.ahrq.gov/clinic/ptsafety/pdf/ptsafety.pdf (accessed22August 2013)
4 Fleisher LA, Beckman JA, Brown KA, et al.ACC/AHA 2007 guidelinesonperioperative cardiovascularevaluationand care for noncardiacsurgery: executive summary: a report of the American College ofCardiology/American Heart Association Task Force on PracticeGuidelines (Writing Committee to Revise the 2002 Guidelines onPerioperative Cardiovascular Evaluation for Noncardiac Surgery):developed in collaborationwith theAmerican Societyof Echocardi-ography, American Society of Nuclear Cardiology, Heart RhythmSociety, Society of Cardiovascular Anesthesiologists, Society forCardiovascularAngiographyandInterventions,Society forVascularMedicine and Biology, and Society for Vascular Surgery. Circulation2007; 116: 1971–96
5 StoneJG,FoexP, SearJW,JohnsonLL,KhambattaHJ, TrinerL.Riskofmyocardial ischaemiaduringanaesthesia in treatedanduntreatedhypertensive patients. Br J Anaesth 1988; 61: 675–9
6 Brady AR, Gibbs JS, Greenhalgh RM, Powell JT, Sydes MR. Periopera-tivebeta-blockade (POBBLE) forpatientsundergoing infrarenalvas-cular surgery: results of a randomized double-blind controlled trial.J Vasc Surg 2005; 41: 602–9
7 ZauggM,BestmannL,Wacker J,etal.Adrenergic receptorgenotypebut not perioperative bisoprolol therapymay determine cardiovas-cular outcome in at-risk patients undergoing surgery with spinalblock: the Swiss Beta Blocker in Spinal Anesthesia (BBSA) study: adouble-blinded, placebo-controlled, multicenter trial with 1-yearfollow-up. Anesthesiology 2007; 107: 33–44
8 Bayliff CD,MasselDR, InculetRI,et al.Propranolol for thepreventionof postoperative arrhythmias in general thoracic surgery. AnnThorac Surg 1999; 67: 182–6
9 Juul AB, Wetterslev J, Kofoed Enevoldsen A, Callesen T, Jensen G,Gluud C. The Diabetic Postoperative Mortality and Morbidity
(DIPOM) trial: Rationale and design of a multicenter, randomized,placebo-controlled, clinical trial ofmetoprolol for patientswith dia-betes mellitus who are undergoing major noncardiac surgery. AmHeart J 2004; 147: 677–83
10 Yang H, Raymer K, Butler R, Parlow J, Roberts R. The effects of peri-operative beta-blockade: results of the Metoprolol after VascularSurgery (MaVS) study, a randomized controlled trial. Am Heart J2006; 152: 983–90
11 Lai RC, Xu MX, Huang WQ, Wang XD, Zeng WA, Lin WQ. Beneficialeffects of metoprolol on perioperative cardiac function of elderlyesophageal cancer patients. Ai Zheng 2006; 25: 609–13
12 Liu Y, HuangCL, HeM, Zhang LN, Cai HW, GuoQL. Influences of peri-operative metoprolol on hemodynamics and myocardial ischae-mia in elderly patients undergoing noncardiac surgery. ZhongNan Da Xue Xue Bao Yi Xue Ban 2006; 31: 249–53
13 Magnusson J, Thulin T, Werner O, Jarhult J, Thomson D. Haemo-dynamic effects of pretreatment with metoprolol in hyperten-sive patients undergoing surgery. Br J Anaesth 1986; 58:251–60
14 UrbanMK, Markowitz SM, GordonMA, Urquhart BL, Kligfield P. Post-operative prophylactic administration of beta-adrenergic blockersin patients at risk for myocardial ischemia. Anesth Analg 2000;90: 1257–61
15 Jakobsen CJ, Blom L. Effect of pre-operative metoprolol on cardio-vascular and catecholamine response and bleeding during hyster-ectomy. Eur J Anaesthesiol 1992; 9: 209–15
16 Devereaux PJ, BeattieWS, Choi PT, et al.How strong is the evidencefor the use of perioperative beta blockers in non-cardiac surgery?Systematic review and meta-analysis of randomised controlledtrials. Br Med J 2005; 331: 313–21
17 DevereauxPJ,YangH,YusufS,etal.Effectsofextended-releasemeto-prolol succinate in patients undergoing non-cardiac surgery (POISEtrial): a randomised controlled trial. Lancet 2008; 371: 1839–47
18 Bangalore S, Wetterslev J, Pranesh S, Sawhney S, Gluud C,Messerli FH. Perioperative beta blockers in patients having non-cardiac surgery: a meta-analysis. Lancet 2008; 372: 1962–76
19 Poldermans D, Devereaux PJ. The experts debate: perioperativebeta-blockade for noncardiac surgery—proven safe or not? ClevClin J Med 2009; 76: S84–92
20 Fleisher LA, Beckman JA, Brown KA, et al. 2009 ACCF/AHA focusedupdate on perioperative beta blockade incorporated into theACC/AHA 2007 guidelines on perioperative cardiovascular evalu-ation and care for noncardiac surgery: a report of the Americancollege of cardiology foundation/American heart associationtask force on practice guidelines. Circulation 2009; 120(Suppl. 4):e169–276
21 PoldermansD, Bax JJ, BoersmaE, et al.Guidelines for pre-operativecardiac risk assessment and perioperative cardiacmanagement innon-cardiac surgery: the Task Force for Preoperative Cardiac RiskAssessment and Perioperative Cardiac Management in Non-cardiac Surgery of the European Society of Cardiology (ESC) andendorsed by the European Society of Anaesthesiology (ESA). EurHeart J 2009; 30: 2769–812
22 Shammash JB, Trost JC, Gold JM, Berlin JA, Golden MA, Kimmel SE.Perioperative beta-blocker withdrawal and mortality in vascularsurgical patients. Am Heart J 2001; 141: 148–53
23 HoeksSE, ScholteOp, ReimerWJ, vanUrkH,et al. Increaseof 1-yearmortality after perioperative beta-blockerwithdrawal in endovascularand vascular surgery patients. Eur J Vasc Endovasc Surg 2007; 33:13–9
24 Wallace AW, Au S, Cason BA. Association of the pattern of use ofperioperativebeta-blockadeandpostoperativemortality.Anesthe-siology 2010; 113: 794–805
Editorial II BJA
209
64

25 Ponten J, Biber B, Bjuro T, Henriksson BA, Hjalmarson A. Beta-receptor blocker withdrawal. A preoperative problem in generalsurgery? Acta Anaesthesiol Scand Suppl 1982; 76: 32–7
26 CrandellDL. Theanesthetichazards inpatientsonantihypertensivetherapy. J Am Med Assoc 1962; 179: 495–500
27 Viljoen JF, Estafanous FG, Kellner GA. Propranolol and cardiacsurgery. J Thorac Cardiovasc Surg 1972; 64: 826–30
28 Ellenberger C, Tait G, Beattie WS. Chronic beta blockade is asso-ciated with a better outcome after elective noncardiac surgerythan acute beta blockade: a single-center propensity-matchedcohort study. Anesthesiology 2011; 114: 817–23
29 Poldermans D. Scientific fraud or a rush to judgment? Am J Med2013; 126: e5–6
30 Chopra V, Eagle KA. Perioperative mischief: the price of academicmisconduct. Am J Med 2012; 125: 953–5
31 Bouri S, Shun-Shin MJ, Cole GD, Mayet J, Francis DP. Meta-analysisof secure randomised controlled trials of b-blockade to preventperioperative death in non-cardiac surgery. Heart Online 2013Advance Access published on 31 July 2013, doi: 10.1136/heartjnl-2013-304262
32 Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol onperioperative mortality and myocardial infarction in high-riskpatients undergoing vascular surgery. Dutch EchocardiographicCardiac Risk Evaluation Applying Stress Echocardiography StudyGroup. N Engl J Med 1999; 341: 1789–94
33 Dunkelgrun M, Boersma E, Schouten O, et al. Bisoprolol and flu-vastatin for the reduction of perioperative cardiac mortalityand myocardial infarction in intermediate-risk patients
undergoingnoncardiovascular surgery: a randomized controlledtrial (DECREASE-IV). Ann Surg 2009; 249: 921–6
34 Wallace AW, Au S, Cason BA. Perioperative beta-blockade: atenololis associated with reduced mortality when compared to metopro-lol. Anesthesiology 2011; 114: 824–36
35 Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B,Benjamin EM. Perioperative beta-blocker therapy and mortalityafter major noncardiac surgery. N Engl J Med 2005; 353: 349–61
36 LondonMJ,Hur K, Schwartz GG,HendersonWG.Association of peri-operativebeta-blockadewithmortalityandcardiovascularmorbid-ity followingmajor noncardiac surgery. J AmMed Assoc 2013; 309:1704–13
37 BeattieWS, Wijeysundera DN, Karkouti K, McCluskey S, Tait G. Doestight heart rate control improve beta-blocker efficacy? An updatedanalysis of thenoncardiac surgical randomized trials.AnesthAnalg2008; 106: 1039–48
38 Beattie WS, Wijeysundera DN, Karkouti K, et al. Acute surgicalanemia influences the cardioprotective effects of beta-blockade:a single-center, propensity-matched cohort study. Anesthesiology2010; 112: 25–33
39 Le Manach Y, Collins GS, Ibanez C, et al. Impact of perioperativebleeding on the protective effect of beta-blockers during infrarenalaortic reconstruction. Anesthesiology 2012; 117: 1203–11
40 ACCF/AHA, ESC. Joint Statement: issued by theAmericanCollege ofCardiology, American Heart Association and the European Societyof Cardiology. 2013. Available from www.escardio.org.about/press/press-releases/pr-13/Pages/joint-statement-perioperative-guidelines.aspx (accessed 10 August 2013)
British Journal of Anaesthesia 112 (2): 210–12 (2014)doi:10.1093/bja/aet431
EDITORIAL III
Perioperative immunity: is there an anaesthetic hangover?R. D. Sanders1,2,31 Department of Anaesthesia and 2 Surgical Outcomes Research Centre, National Hospital for Neurology and Neurosurgery, University CollegeLondon Hospital, Queen Square, London WC1N 3BG, UK3Wellcome Department of Imaging Neuroscience, University College London, London, UK
E-mail: [email protected]
While the cross-talk between the nervous and immunesystems is slowly being unravelled,1 important commonalitiesbetween the two systems suggest that anaesthetics mayimpact profoundly on the immunity,2 similar to the nervoussystem.3 For example, many immune cells are ‘excitablecells’, have plasma membranes that depolarize (e.g. themacrophage membrane after phagocytosis),4 and expressneurotransmitter receptors like neurones.1 2 5 Immune cellsexpress g-amino butyric type A (GABAA) receptors, an anaes-thetic target for benzodiazepines, propofol and the volatileanaesthetics.2 5 An important target of ketamine, nitrousoxide, xenon, the N-methyl-D-aspartate (NMDA) receptor
may also be expressed.6 Expression of these receptors mayexplain accumulating data suggesting that many anaestheticdrugs exert important functional effects on immune cells2 (al-though the reader is recommended to read the article onopioids by Al-Hashimi and colleagues7 reviewing evidence forimmune cell opioid receptor expression). The diffuse natureof receptor expression of neurotransmitter receptors1 2 5
mean that anaesthetic effects on immunity may includealtered innateandacquired inflammatory responses.2 It ispos-sible that the functional consequences of these effects mayinclude increased vulnerability to infection8–10 and cancer.11
However, reducing intraoperative inflammation may be a
BJA Editorial III
210
65


13 Mariani PJ, Cooney N. Air embolism’s new scarlet letter. UnderseaHyperb Med 2009; 36: 407–8
14 SoudayV, Radermacher P,Asfar P. Cerebral arterial gasembolism—a race against time! Crit Care Med 2013; 41: 1817–9
15 Ploner F, Saltuari L, Marosi MJ, Dolif R, Salsa A. Cerebral air emboliwith use of central venous catheter in mobile patient. Lancet1991; 338: 1331
16 Fracasso T, Karger B, Schmidt PF, Reinbold WD, Pfeiffer H. Retro-grade venous cerebral air embolism from disconnected centralvenous catheter: an experimental model. J Forensic Sci 2011;56(Suppl. 1): S101–4
17 Butler BD, Bryan-BrownC, Hills BA. Paradoxical air embolism: trans-capillary route. Crit Care Med 1983; 11: 837
18 ImanishiM,NishimuraA, TabuseH,MiyamotoS, Sakaki T, Iwasaki S.Intracranial gasonCTaftercardiopulmonary resuscitation: 4 cases.Neuroradiology 1998; 40: 154–7
19 Muth CM, Shank ES. Gas embolism.NEngl JMed2000;342: 476–82
20 Ely EW, Hite RD, Baker AM, Johnson MM, Bowton DL, Haponik EF.Venous air embolism from central venous catheterization: a needfor increased physician awareness. Crit CareMed 1999; 27: 2113–7
21 Lai D, Jovin TG, Jadhav AP. Cortical vein air emboli with gyriforminfarcts. JAMA Neurol 2013; 70: 939–40
22 Vachalova I, Ernst S, Vynogradova I, Wohrmann S, Heckmann JG.Cerebral air embolism via port catheter and endoscopic retrogradecholangio-pancreatography. Springerplus 2013; 2: 477
23 Bothma PA, Brodbeck AE, Smith BA. Cerebral venous air embolismtreated with hyperbaric oxygen: a case report. Diving Hyperb Med2012; 42: 101–3
24 WeeninkRP,HollmannMW,vanHulstRA.Animalmodelsof cerebralarterial gas embolism. J Neurosci Methods 2012; 205: 233–45
25 Bothma P, Rice N. Hyperbaric oxygen does not improvecerebral function when started 2 or 4 hours after cerebral arterialgas embolism in swine: online letter to the editor. Crit Care Med2013, in press
British Journal of Anaesthesia 112 (3): 404–6 (2014)Advance Access publication 23 December 2013 . doi:10.1093/bja/aet436
EDITORIAL III
Fluid management in association with neonatal surgery: eventiny guys need their saltP.-A. Lonnqvist1,21 Section of Anaesthesiology and Intensive Care, Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden2 Paediatric Anaesthesia, Intensive Care and ECMO services, Karolinska University Hospital-Solna, SE-171 76 Stockholm, Sweden
E-mail: [email protected]
Thepracticeofgiving i.v. fluidsaspartof routinepaediatric carewas established during the 1950s, and important initial ques-tions to answer were what type of solution to give and atwhat infusion rates. In 1957, Holliday and Seger1 published aseminal manuscript, recommending the well-known ‘4-2-1rule’, which almost immediately was adopted as a worldwidestandard. The composition of a normal i.v. maintenance fluidwas however somewhat more difficult to determine but washeavily influenced by the composition of normal breast milk,which has a sodium content in the range of 10–40 mmollitre21.2 Thus, effectively hypotonic glucose solutions with alowsodiumcontentcame intowide-spreadusemaybebestex-emplified by the British 4% glucose 0.18% sodium (‘four and afifth’).3 The history since the 1950s has shown that the ap-proach described above works sufficiently well in the vastnumber of routine paediatric cases.
However, using the standard Holliday and Segar volumerecommendations paired together with the use of an i.v. solu-tion with a sodium concentration that diverges substantiallyfrom that of the extracellular fluid does become a problem ina situation of a neuroendocrine stress response, either pro-voked by surgery or significant medical illness. The reason for
this is that the stress response includes a substantiallyincreased secretion of anti-diuretic hormone (ADH) that willresult in retention of free water. A physiologically more appro-priateapproachduring these circumstances is tousea solutionwith a close to physiological concentration of sodium (120–140 mmol litre21) combined with the administration of areduced infusion volume compared with the normal situation(50–70% of normal infusion rate).4 5 If not adhering to amore physiological approach, the stage is set for dilutionalhyopnatraemia that can be life-threatening or even fatal.6–11
The insight that the paediatric use of i.v. low sodium solu-tions was unsuitable in the context of a stress response andthat a sodium content closer to that of extracellular fluid ismore appropriate was published as early as 1964.12 However,since no appropriate i.v. solutions were commercially madereadilyavailablebythemanufacturers, the regimenofusingef-fectively hypotonic solutions in associationwith paediatric an-aesthesia and surgery has continued in many centres even tothis day. A questionnaire-based study from 2001 reportedthat 97% of UK-based anaesthetists routinely used effectivelyhypotonic i.v. solution intraoperatively in children.13 A similarstudy published in 2006, also surveying the UK practice,
BJA Editorial III
404
67

reported nomajor changeof practicewith amajority of anaes-thetists still using hypotonic solutions both intraoperativelyand after operation (66% and 87%, respectively) and asmanyas11%admitted that theyevenused the samehypoton-ic solutions for volume replacement.14
Aparamount initiative to set things straightwas takenby theFrench paediatric anaesthesia community in the early 1990s,spearheaded by Murat and colleagues. In a number of clinicalstudies, they could show that the perioperative use of an i.v. so-lution made available by the Paris pharmacy (Polyionique B66,0.9% glucose with sodium 120 mmol litre21) did keep plasmasodium within the normal range during the postoperativeperiod and did also avoid clinically relevant hypo- or hypergly-caemia.15–17 Furthermore, the use of this type of i.v. solutionhasalsobeen found considerably safer should there occurunin-tentional over-infusionor if itwould beused for volume replace-ment.18 This taken together with a still ongoing UK NationalInquiry into the tragicoutcomesof theuseofhypotonic i.v. solu-tions in ill children19 and expert opinion3 20–23 has led to newand more appropriate recommendations.24–26 Currently,proper i.v. solutions are commercially available in a number ofindividual European countries and hopefully soon the mainmanufacturers of i.v. solutions will provide such solutionsreadily available to clinicians in all European countries.26
Thus, currently the use of an intra- and postoperative i.v. so-lution containing close to physiological concentrations ofsodium is recommended in children .6 months of age.17
However, until now, data for children 0–6 months of agehave been scarce27 and recommendations have mainly beenbased on extrapolations based on normal physiology com-bined with the insight that even our smallest children canand will respond with a relevant neuroendocrine stress re-sponse when subjected to surgical procedures.28 29 Studiesfocused on neonates and small infants in this context havebeen largely lacking.
It is therefore with great pleasure and satisfaction that wenow can enjoy the results of yet another French initiative,which provide us with much sought after information in thisregard. In this issue of the BJA, Edjo-Nkilly and colleagues30
report data generated from34neonates (0–7 days old) under-goingavarietyofneonatal surgical procedures. Themain focusof their studywasto investigate theeffect onplasmasodium inrelation to the amount of freewater that was administered i.v.during the perioperative period. Despite the inherent problemswith standardization associated with this type of study, theauthorshavebeenable toprovideuswith twonewandvery im-portant pieces of insight in the neonatal context, apart fromidentifying a 12% overall incidence of postoperative hypona-traemia in this group of neonates.
First, the reduction in plasma sodium correlated only to theamount of free water that is administered intraoperativelyand not to the amount of free water administered beforeoperation. This makes sense for two reasons. Based ondecades of clinical experience using regular i.v. maintenancesolutions containing a low content of sodium, we know thatnormal children without any major ongoing stress response(as is the case before surgery) will be able to handle such
infusions without any risk of hyponatraemia. Thus, the lack ofcorrelation to preoperative free water administration appearsintuitively correct. However, as surgery commences, the neu-roendocrine stress response will be initiated, including a rapidincrease in ADH, which in turn will render the child unable tohandle thechallenge representedbycontinuedadministrationof effectivelyhypotonic solutions. Secondly, intraoperative freewater administration in excess of 6.5ml kg21 h21 was found tobeassociatedwithapostoperative reduction inplasmasodium(≥4 mmol litre21) with a sensitivity and specificity of 0.7 and0.5, respectively. This provides us with a very useful guidelineto how much free water can be allowed during neonatalsurgery with regard to the risk of producing clinically relevantpostoperative hyponatraemia.
The data now published by Edjo-Nkilly and colleagues lendsupport forextending thecurrentpaediatricconsensus regard-ing intra- and immediately postoperative use of i.v. solutionscontaining �1% glucose with a near to normal content ofsodium (120–140 mmol litre21)26 to also include infants ,6monthsof age. Thus, giveour little guys their salt duringanaes-thesia and surgery!
Declaration of interestP.-A.L. is amemberof theBJAEditorial Boardand isalsoSectioneditor/Editorial Board member of Paediatric Anaesthesia.
References1 Holliday MA, Segar WE. The maintenance need for water in paren-
teral fluid therapy. Pediatrics 1957; 19: 823–32
2 KooWW,GuptaJM.Breastmilksodium.ArchDisChild1982;57: 500–2
3 Cunliffe M, Potter F. Four and a fifth and all that. Br J Anaesth 2006;97: 274–7
4 Holliday MA, Seger WE. Reducing errors in fluid therapy manage-ment. Pediatrics 2003; 111: 424–5
5 Paut O, Lacroix F. Recent developments in the perioperative fluidmanagement for the paediatric patient. Curr Opin Anaesthesiol2006; 19: 268–77
6 Arieff AI. Postoperative hyponatraemic encephalopathy followingelective surgery in children. Paediatr Anaesth 1998; 8: 1–4
7 Arieff AI, Ayus JC, Fraser CL. Hyponatraemia and death or perman-ent brain damage in healthy children. BrMed J 1992; 304: 1218–22
8 PautO,RemondC, LagierP, FortierG,Camboulives J. Severehypona-tremic encephalopathy after pediatric surgery: report of sevencases and recommendations for management and prevention.Ann Fr Anesth Reanim 2000; 19: 467–73
9 Hanna S, Tibby SM, Durward A, Murdoch IA. Incidence of hypona-traemia and hyponatraemic seizures in severe respiratory syncytialvirus bronchiolitis. Acta Paediatr 2003; 92: 430–4
10 Moritz ML, Ayus JC. Prevention of hospital-acquired hyponatremia:a case for using isotonic saline. Pediatrics 2003; 111: 227–30
11 Cladis FP, Bykowski M, Schmitt E, et al. Postoperative hyponatremiafollowing calvarial vault remodeling in craniosynostosis. PaediatrAnaesth 2011; 21: 1020–5
12 Fock G. Fluid therapy in appendicitis with peritonitis in children.Nord Med 1964; 71: 237–40
13 SoderlindM, Salvignol G, Izard P, Lonnqvist PA.Use of albumin, bloodtransfusion and intraoperative glucose by APA and ADARPEFmembers: a postal survey. Paediatr Anaesth 2001; 11: 685–9
Editorial III BJA
405
68

14 Way C, Dhamrait R,Wade A,Walker I. Perioperative fluid therapy inchildren: a surveyof current prescribingpractice.Br J Anaesth2006;97: 371–9
15 Hongnat JM, Murat I, Saint-Maurice C. Evaluation of current paedi-atric guidelines for fluid therapy using two different dextrose hy-drating solutions. Paediatr Anaesth 1991; 1: 95–100
16 DuboisMC, Gouyet L,Murat I, Saint-Maurice C. Lactated Ringerwith1% dextrose: an appropriate solution for peri-operative fluidtherapy in children. Paediatr Anaesth 1992; 2: 99–104
17 Geib I, Dubois MC, Gouyet L, Murat I, Saint-Maurice C. Perioperativeperfusion in children: evaluation of a newperfusion solution.AnnFrAnesth Reanim 1993; 12: 6–10
18 Witt L,OsthausWA,LuckeT,etal.Safetyofglucose-containingsolu-tions during accidental hyperinfusion in piglets. Br J Anaesth 2010;105: 635–9
19 The inquiry into hyponatremia-related deaths. Available from http://www.ihrdni.org/index/latest-news.htm
20 Berleur MP, Dahan A, Murat I, Hazebroucq G. Perioperative infu-sions in paediatric patients: rationale for using Ringer-lactate so-lutionwith lowdextroseconcentration. J Clin PharmTher2003;28:31–40
21 Duke T, Molyneux EM. Intravenous fluids for seriously ill children:time to reconsider. Lancet 2003; 362: 1320–3
22 Lonnqvist PA. Inappropriate perioperative fluid managementin children: time for a solution?! Paediatr Anaesth 2007; 17:203–5
23 Brouh Y, Paut O, Tsimaratos M, Camboulives J. Postoperative hypo-natremia in children: pathophysiology, diagnosis and treatment.Ann Fr Anesth Reanim 2004; 23: 39–49
24 National PatientSafetyAgency/Patient safetyalertNo22:Reducingthe risk of hyponatraemia when administering intravenous infu-sions to children. Available from http://www.nrls.npsa.nhs.uk/resources/type/alerts/?Entryid45=59809&p=3
25 Murat I, Dubois MC. Perioperative fluid therapy in pediatrics.Paediatr Anaesth 2008; 18: 363–70
26 Sumpelmann R, Becke K, Crean P, et al. German Scientific WorkingGroup for Paediatric Anaesthesia. European consensus statementfor intraoperative fluid therapy in children. Eur J Anaesthesiol2011; 28: 637–9
27 Sumpelmann R, Mader T, Eich C, Witt L, Osthaus WA. A novelisotonic-balanced electrolyte solution with 1% glucose for intrao-perative fluid therapy in children: results of a prospectivemulticen-tre observational post-authorization safety study (PASS). PaediatrAnaesth 2010; 20: 977–81
28 Murat I, Humblot A, Girault L, Piana F. Neonatal fluidmanagement.Best Pract Res Clin Anaesthesiol 2010; 24: 365–74
29 StraußJM,SumpelmannR.Perioperativefluidmanagement in infantsand toddlers.Anasthesiol IntensivmedNotfallmedSchmerzther2013;48: 264–71
30 Edjo Nkilly G, Michelet D, Hilly J, et al. Postoperative decrease inplasma sodiumconcentration after infusion of hypotonic intraven-ous solutions in neonatal surgery. Br J Anaesth 2014; 112: 540–5
British Journal of Anaesthesia 112 (3): 406–9 (2014)doi:10.1093/bja/aet591
EDITORIAL IV
History of anaesthesia in Colombia: periods of developmentB. Ocampo1,2* and J. E. Pena2,3,4
1 Titular professor, Caldas University (Universidad de Caldas), Manizales, Caldas, Colombia2 Ex presidente, ex Former, Colombian Society of Anaesthesiology and Reanimation (Sociedad Colombiana de Anestesiologıa y Reanimacion),Bogota, DC, Colombia3 Universidad El Bosque, Bogota, DC, Colombia4 Emeritus Fundacion Santa Fe de Bogota, Bogota, DC, Colombia
* Corresponding author. E-mail: [email protected]
The written history of anaesthesia is dominated by the devel-opments in English-speaking parts of the world; there is littlewritten or read on the developments in Latin America. Inthis editorial, based on a qualitative historical research,1 wepresent a brief overviewof six historical periods of the develop-ment of anaesthesia in Colombia.
First period: pre-anaesthetic era (beforeOctober 16, 1846)It is known that surgical experiments were few during thisperiod, and that the techniques for controlling pain were
empirical. Surgical procedures were carried out with the useof substances such as opium, mandrake, and other remediespopular at the time.
In this period, the most relevant events were those relatedto increase in health institutions, hospitals, and universities,where medical attention and experimental surgery started todevelop. These institutions later became essential sites forthe development of the speciality in Colombia.
In commonwith the restof theworld, following thefirst suc-cessful public demonstration of ether anaesthesia by WilliamT. G. Morton at Massachusetts General Hospital (NorthAmerica), October 16, 1846 marked the historical birth of an-aesthesia in Colombia.
BJA Editorial IV
406
69


REGIONAL ANAESTHESIA
Flexion-rotation manoeuvre increases dimensionof the acoustic target window for paramedian thoracicepidural accessN. Ramsay, J. Walker, R. Tang, H. Vaghadia* and A. Sawka
DepartmentofAnesthesiology,VancouverGeneralHospital, VancouverCoastalHealth, 855West12thAvenue,Vancouver, BC, CanadaV5Z1M9
* Corresponding author. E-mail: [email protected]
Editor’s key points
† The best patient position foridentifying the thoracicepidural space is debated.
† This volunteer study usedultrasound to visualize theposterior longitudinal ligamentand hence identify the thoracicepidural space.
† Using 108 dorsal table tiltand flexion with right rotationvia a paramedian approachimproved the acoustic targetarea.
† This position mayfacilitate epidural catheterplacement but furtherstudies are needed.
Background. The posterior longitudinal ligament (PLL) has been found to be a reliablemeasure of the acoustic target window for lumbar spinal anaesthesia and a predictivetool for difficult spinals. Currently, there is limited information on the PLL in thethoracic spine and its potential use for optimizing the acoustic target window duringthoracic epidural placement. This study examined the effects of changes in bodyposition on the length of the PLL as a measure of the acoustic target window forparamedian thoracic epidural access.
Methods. We performed thoracic ultrasonography on 30 adult volunteers to measurethe length of the PLL at the T9/10 interspace, in five different positions: P1, neutral; P2,thoracic and lumbar flexion; P3, as in position 2 with dorsal table tilt to 108; P4, as inposition 2 with 458 rightward shoulder rotation; and P5, as in position 2 with 458leftward shoulder rotation.
Results. Themean (SD) PLL length increased significantly from9.9 (3.9)mm in P1 to 11.7(3.4)mm in P2, 12.9 (3.1)mm in P3, and13.8 (4.0)mm in P4 (P,0.01,,0.01, and,0.01,respectively). Themean PLL length in P3 and P4 was also significantly longer comparedwith P2 (P,0.01 and 0.01, respectively).
Conclusions. In volunteers, flexion with 108 dorsal table tilt and flexion with rightrotation significantly increased the length of the ipsilateral PLL, compared with thestandard flexed sitting position, as visualized by paramedian ultrasonography at thelevel of T9/10.
Keywords: anaesthetic techniques, epidural; monitoring, ultrasound
Accepted for publication: 11 September 2013
Thoracic epidural anaesthesia is a commonly used techniqueto provide postoperative analgesia. Although Pages1 firstdescribed lumbar epidural anaesthesia, it was Dogliotti,2 whodescribed the upright sitting position with lumbar flexion forthoracic epidural anaesthesia. This position continues to bedescribed essentially unchanged in modern textbooks of an-aesthesia.3 However, there is limited research on optimizingpatient position to facilitate thoracic epidural placement andno objective evidence to support one position over another.Anotherchallenge indetermining theeffect of patientpositionon neuraxial access is the lack of suitable technology. PlainX-rays lack sufficient resolution and most commercially avail-able CT and MRI scanners will not accommodate subjects ina sitting position; fluoroscopy and CT scans also subject
individuals to radiation exposure. Neuraxial ultrasonographyis harmless in this regard and provides a dynamic real-timeassessment of the relevant anatomy, the effect of positionchanges on the size of the acoustic window for epidural andspinal insertion.4 5
Theparamedianapproach for thoracicepiduralanaesthesiahas the advantage of decreased incidence of dural puncture,vascular puncture, and paraesthesias.6 Grau and colleagues7
demonstrated that the paramedian approach also providesan optimal ultrasound ‘acoustic’ windowbetween the thoracicvertebrae for visualizing pertinent structures in the epiduralspace. Furthermore, comparison of ultrasonography of thethoracic epidural space with magnetic resonance imaginghas shown satisfactory correlation between the two with an
British Journal of Anaesthesia 112 (3): 556–62 (2014)Advance Access publication 6 January 2014 . doi:10.1093/bja/aet385
& The Author [2014]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
71

acceptable degree of precision in the depiction of structures.7
This approach overcomes the steep angulation of overlapp-ing spinous processes and narrow intervertebral spaces,compared with a midline approach.7 8 Although changes inthe dimensions of the interspinous space and ligamentumflavum, as measured by ultrasonography, are proposed to beimportant factors in determining successful midline neuraxialneedle insertion in the lumbar region, they have limited utilityin the thoracic regionbecause the ligamentumflavum is thin inthe thoracic region and there is acoustic interference from thesteeplyangledspinousprocesses.5 9–13 Inaddition, theposter-iorcomplex (ligamentumflavum,epidural space,andposteriordura) isnotconsistentlyvisible so that itsdimensionscannotbeutilizedasaguide to thewidthof the interlaminarwindow.13 Inprevious descriptions of ultrasound-guided neuraxial techni-ques, the importance of sonographic visualization of the PLLas a guidance structure for neuraxial puncture has beenemphasized, because even though the PLL is part of the anter-ior aspect of the epidural space, clear visualization of the PLL isindicative of an ‘open acoustic window’, with an unobstructedpath to thedurabetweenthe laminae, andmayprovide indica-tion of the technical difficulty associated with neuraxialaccess.13–15 The posterior longitudinal ligament (PLL) can beeasily visualized in the thoracic region via a paramedian viewand ithasbeenvalidatedasa reliable screening tool fordifficultspinal anaesthesia.4 13 15 The purpose of this study was tomeasure the ‘acoustic target area’ (defined as the visualizedlength of the PLL), at the T9–10 interspace, by paramedianultrasonography in five seated positions (neutral, traditionalflexed, flexed with 108 of dorsal table tilt, flexed with rotationto the right side, and flexed with rotation to the left side).We hypothesized that flexion and rotation may increase thedimension of this acoustic target area, and theoreticallyfacilitate thoracic epidural needle insertion.
MethodsThis study was approved by the Clinical Research Ethics Boardof the University of British Columbia on September 14, 2012,and registered with the Office of Research Services of the Uni-versity of British Columbia (H12-02141). Informed writtenconsent was obtained from 30 healthy volunteer subjectsrecruited at Vancouver General Hospital. Inclusion criteriawere the ability to achieve the five positions expected in thestudy and to provide written informed consent. We excludedvolunteers with a history of spinal trauma, spinal surgery,or congenital spinal abnormality and allergy to ultrasoundgel. Age, weight, height, and BMI were recorded for eachparticipant.
All volunteers were sitting on a height-adjustable operatingtheatre table with feet fully supported, to bend the hips andknees to 908. Spinal ultrasonography was performed in fivestudy positions (Figs 1 and 2):
P1. Neutral: no back flexion/extension.P2. Flexion: slouching of the shoulders with lumbarflexion and exaggeration of the thoracic kyphosis witharms around a pillow at chest level.
P3. Table tilt: as in position 2 and dorsal table tilt to 108.P4. Right rotation: as in position 2 and 458 rightward shoul-der rotation.P5. Left rotation: as in position 2 and 458 leftward shoulderrotation.
Table tilt angle was limited to 108 because 158 was not toler-ated by patients in a previous study;9 table tilt was measuredusing the Tiltmeter application (Integrasoft, Bridgewater, NJ,USA) on an iPhone 3G (Apple, Cupertino, CA, USA) and con-firmed using a protractor with a hanging weight.9
Using a 2–5 MHz curvilinear transducer (Ultrasonix, Rich-mond, BC, Canada), the T9/10 intervertebral level was identi-fied, by scanning in a longitudinal paramedian plane fromthe sacral plateau and moving cranially counting eachlaminae.16 Secondary confirmation of the level was performedbymanual palpation of the spinous processes from the level ofthe sacral plateau. We chose to study the T9/10 level becausean epidural catheter at this level has the potential of providingdermatomal analgesia for most thoracic and abdominal pro-cedures and is the level most often used in our centre. A rightlongitudinal paramedian plane was used to achieve optimalimages.17 16 The laminae were identified by the ‘sawtooth’ultrasound pattern and the ligamentum flavum/posteriorduravisualizedasabrighthyperechoic line. ThePLLandposter-ior vertebral body were visualized as a deeper hyperechoicstructure and identified in all images.
Two experienced fellows (N.R., J.W.) in anaesthesiology(.50 neuraxial ultrasound scans) performed the scans andmeasurements but could not be blinded to patient position.The first anaesthesiologist (N.R.) performed all the ultrasoundscans and the second anaesthesiologist (J.W.) measured andrecorded the length of the most superficial and inferioraspects of the PLL using the onscreen caliper tool. The firstanaesthesiologist was blinded to the actual distances mea-sured. The process of scanning and measurement wasrepeated in the same sequence for each of the five study posi-tions in all subjects. The entire scans were recorded as a videofile and re-measured by a third anaesthesiologist (R.T.),blinded to the patient positions and blinded to PLL measure-ments made by the second anaesthesiologist (J.W.). Thissecond data set of PLL measurements was used to quantifyinter-observer agreement
Sample size was estimated based on data from a compar-able studyusinga1mmchange in targetareadimensions, a1mm SD, an a of 0.05, and a power of 90% to yield a sample sizeof 16 subjects.9 Since an epidural needle is �1 mm in diam-eter, any increase in target area dimensions of 1 mm can betheoretically important in determining successful access tothe epidural space. After statistical consultation, we esti-mated a sample size of 30 volunteers would be adequate toshowsignificant change in themean lengthof thePLL (acous-tic target area) in anyof the fivepositions. The datawere ana-lysed using repeated-measures analysis of variance, inpairwise comparisons for measurements of the mean PLLlength in each of the positions (with the Bonferroni adjust-ment tomaintainP,0.05). Testsof normalitywereperformed
Optimizing the thoracic epidural window through positioning BJA
557
72

with the Kolmogorov–Smirnov (Lilliefors’ significance correc-tion) and the Shapiro–Wilk checks. Intraclass coefficients(one-way random effects model) were used to evaluate thereliability and repeatability of the PLL measurements
performed by the two different anaesthesiologists. All dataanalyses were conducted using Statistical Package for theSocial Sciences (SPSS) software (Version 20.0), IBM Corpor-ation, Armonk, NY, USA.
A
B
Fig1 With thesubjects seated in thestandardflexedpositionwith legs supportedandcradlingapillow, theywereasked to rotate their shoulders toa 458 angle (A). The spine is shown in the rotated position (B) with the inset depicting the effect on the T9/10 vertebrae. The original position of thevertebrae is shown with the grey shadow. Spine flexion separates the spinous processes and rotation further opens up the interlaminar space bycausing the T9 spinous process to move away from the T10 lamina. This potentially increases the target area for epidural placement.
BJA Ramsay et al.
558
73

Results
Thirty volunteers participated; of which, 20 weremales and 10females. Themean (SD) agewas 39.4 (10.1) yr; BMIwas 24 (3.8)kg m22, with the mean height and weight being 174 (9.8) cmand 72.9 (3.8) kg, respectively.
In all eligible cases, the epidural space at T9–10 was easilyidentified on ultrasonography and the quality of ultrasoundimages was comparable with previous studies.4 7–9 The char-acteristic acoustic shadow was seen anterior to the laminaecorresponding to that of T9 and T10. The ligamentum flavumwas seen as a hyperechoic structure and deeper to it was thehyperechoic PLL. The quality of the PLL images (Fig. 3) wasgood (Weed score .9).4 The superior and inferior limits of thePLL were sufficiently and clearly demarcated on the imagesto enable precise measurement of length with the onscreencaliper tool.
In all subjects, all images were successfully saved andarchived, and there was no loss of data during screen capturemode, measurement mode, and archive retrieval mode.There was a progressive and significant increase in the lengthof the PLL in positions 2, 3, and 4 when compared with theneutral position 1, as shown in Table 1. In comparison withthe standard flexed position for epidural insertion (P2), a 108table tilt in addition to flexion (P3) and rotation (ipsilateral tothe transducer) with flexion (P4) significantly increased thelength of the visualized PLL (Table 1). Rotation (contralateralto the transducer) with flexion (P5) did significantly changethe PLL length compared with position 1 but not comparedwith position 2. The correlation coefficient for measurement
of the PLL length by the two independent anaesthesiologistswas 0.612 (P,0.05).
DiscussionIn this study, wemeasured the length of the PLLwith ultrason-ography to estimate the size of the interlaminar ‘acoustictarget window’ for thoracic (T9–10) paramedian epiduralaccess. We demonstrated that compared with the traditionalflexed position for epidural placement, flexion with 108 dorsaltable tilt and flexion with right rotation significantly increasedthe visualized length of the PLL as a measure of the acoustictarget window.
The PLLasmeasured in our studyand in previous studies is acomposite echo of the anterior dura, PLL, and posterior verte-bral body as it is not possible to delineate these structures asseparate entities using currently available ultrasound technol-ogy.4 7 8DistinguishingbetweenthePLL,anteriordura,andver-tebral body is difficult and not relevant for the objective of ourstudy. The rationale for using the PLL is based on the premisethat an ‘open acoustic window’ is suggestive of an unobstruct-ed path of the ultrasound energy to pass between the laminaethrough the dura, to the PLL. The PLL has previously been vali-dated as a useful tool for assessment of the acoustic targetwindow for neuraxial needle placement in the lumbar spine.In 60 adults undergoing lower extremity joint surgery underspinal anaesthesia, Weed and colleagues4 demonstratedthat the positive predictive value of a low PLL score (0–8, indi-cative of poor visibility) was 82%, which was associated with agreater numberof needle passes and increased technical diffi-culty with lumbar spinal anaesthesia. The positive likelihoodratio of a low PLL score was 12.8 and the negative likelihoodratio was 0.55, indicating that poor PLL visualization isassociated with a high diagnostic yield for identification oftechnical problems with neuraxial access. The rationale forusing the paramedian view is based on the study by Grau andcolleagues16 who imaged the spine in 60 individuals andfound that the paramedian approach provided superiorimages of the neuraxial structures and a larger paramedianwindow compared with transverse and midline longitudinalapproaches.
Visualization of the PLL and the clinical relevance of theobserved changes in PLL length with position in our studyalso merit further discussion. Like Chin and colleagues,13 14 18
we found that the PLL was easily identifiable in all subjects inthe thoracic region and was a reliable landmark for measure-ment. Interestingly, Jones and colleagues9 demonstrated anincrease in the size of the acoustic target area by applicationof dorsal table tilt in the lumbar region but could not demon-strate any effect on interlaminar distances. However, we didnotmeasure ligamentumflavum lengthas it is thin in the thor-acic region and could not be reliably seen byultrasound.13 15 17
In addition, the interlaminar distances were not measuredbecause the corresponding measurement points on thelaminae could not reliably be identified when subjectschanged positions. The PLL, however, was the one structurethat could be reliably visualized in the thoracic region in our
Fig 2 Illustration of 108 dorsal table tilt position. The subject in theimage is demonstrating the P3 position (slouching of the shoulderswith lumbar flexion and exaggeration of the thoracic kyphosis witharmsaroundapillowatchest levelaccompaniedby108dorsal tabletilt).
Optimizing the thoracic epidural window through positioning BJA
559
74

study and in part this could be due to the significantly largeracoustic window to shadow ratio in the paramedian view16
and the image quality of the PLL (Fig. 3) was good (Weedscore .9).4
Our principal findingwas that dorsal table tilt and rotationalmovements of the spine increased the acoustic target area inthe thoracic spine as indicated by the length of the PLL. Theor-etically, a larger ‘target window’ should translate into adecreased incidence of bony contact and improve thesuccess rate for correct placement of a needle for thoracic epi-dural anaesthesia. Themagnitude of changes in themean PLLlength (from 9.9 to 13.8mm) found in our study is comparablewith changes in the mean ligamentum flavum length (from10.7 to 11.2 mm) reported by Jones and colleagues.9 Sincean epidural needle is �1 mm in diameter, changes of suchmagnitude could theoretically make a difference in successful
access to the epidural spaceand is therefore clinically relevant.Our findings could also provide a scientific basis to a manage-ment algorithmwhereby difficult epidural access in the stand-ardpositioncouldbe followedbyanattempt inoneof theotherpositions presented in this study.
Explanation of our findings is based on the functionalanatomy and biomechanics of the spine.19 In the lumbarspine, flexion is the principal mechanism for widening theinterspinous and interlaminar spaces to facilitate neuraxialaccess. In the thoracic region, the thoracic vertebrae permitflexion and rotation of the spine to open the interlaminarspace.19 Based on published literature on kinematics and bio-mechanics of the spine, flexion of the spine at each interspaceincreases moving caudally down the thoracic spine; with 3–58of movement at T1–2 and increasing to 6–208 at T11–12.19
Maximal flexion at the T9–10 interspace studied here has
Table 1 Lengths of the PLL (in mm) visualized by right-sided paramedian ultrasonography, at T9/10 intervertebral level, in five differing positionsmean (SD), and summaryof statistical differences between the neutral position (P1) and posterior–anterior flexion (P2) comparedwith eachof theother study positions
Volunteer position P1 (Neutral) P2 (PA flexion) P3 (PA flexion anddorsal table tilt to 1088888)
P4 (PA flexion and right(ipsilateral rotation)
P5 (PA flexion and left(contralateral rotation)
Posterior longitudinalligament length
9.9 (3.958) 11.79 (3.427) 12.9 (3.144) 13.83 (4.027) 11.14 (3.159)
P-value compared withposition P1
,0.01 ,0.01 ,0.01 ,0.05
P-value compared withposition P2
,0.01 ,0.01 ,0.01 0.1
Fig3 Paramedian longitudinal ultrasound image showing the lamina, ligamentumflavum(LF)/posteriordura (PD), and thePLL/posterior vertebralbody (PVB) between the lamina of T9 and T10.
BJA Ramsay et al.
560
75

been reported to be 88. The application of dorsal table tilt mostlikely augments the degree of comfortable flexion achieved bya patient in the standard flexed position. Rotation of the spinein either direction at each interspace decreases moving caud-ally down the spine; at T1–2, there is between 48 and 148 ofmovement, at T9–10, there is 3–58 and decreases to 2–38 atT11–12.19 20 With rotation, there is separation of the adjacentlaminae and the spinous process sweeps away from themidline to open up the interlaminar space. This has not beenpreviously studied as a potential manoeuvre to aid in epiduralplacement.
In this study, the ultrasoundoperatorand the anaesthesiol-ogistmaking the initial measurements could not be blinded tothe patient position. To minimize reactive bias, the scanninganaesthesiologist was not allowed to see the PLL measure-ments and all PLL measurements were made by the secondanaesthesiologist after all five scans had been saved in eachpatient. To further address observer and measurement bias,an independent consultant, blinded to the volunteer positionsand previous PLL measurements, re-measured the PLL lengthonthearchived imagesassuggestedbyJonesandcolleagues.9
These datawere utilized to obtain an intraclass correlation co-efficient showing good agreement between the twomeasure-ments of PLL length. The order in which volunteers werepositioned for scanning was not randomized because it wasnot practical or conducive to a systematic scanning technique.All our volunteerswereyoungandhealthyandhadnodifficultyassuming the required positions. Elderly, obese, and pregnantpatients may not be able to tolerate these positions, so ourstudy results may not be applicable to all populations. Twooperators identified the start and endpoints of the visualizedPLL to minimize structural identification error. The intrinsicsoftware calculated thenumerical value tominimizemeasure-ment inaccuracies. An important limitation of our study is thatalthough the visualized portion of the PLL is increased inflexion-dorsal table tilt and flexion-right rotation, it can onlybe postulated that this increase in the ‘acoustic targetwindow’ will translate into easier epidural insertion. Eventhough the study byWeed and colleagues4 is highly supportiveof PLL as a predictor of difficult neuraxial insertion, the samecannot be said for our study until further validation in theform of clinical studies, which correlate PLL length in thethoracic region with the level of difficulty for epidural needleinsertion.
We conclude that positioning the patient with either 108 ofdorsal table tilt in flexion or right rotation in flexion increasesinterlaminar space as measured by an increased PLL length.Further clinical studies are required to determine if these posi-tions improve the success rate of thoracic epidurals and allowfor an easier and more efficient insertion.
Authors’ contributionsN.R.: design, conduct of study, data analysis, and manuscriptpreparation; J.W.: design, conduct of study, data analysis,and manuscript preparation; R.T.: study design, conduct of
study, and manuscript preparation; H.V.: study design andmanuscript preparation; A.S.: conduct of studyandmanuscriptpreparation.
AcknowledgementsWe thank Boris Kuzeljevic, Statistician, for help with statisticalanalysis andAshley Pui-Yee Hui, MScBMC Candidate 2015 (Uni-versity of Toronto), for Figure 1 illustration.
Declaration of interestR.T. and A.S. both received equipment and travel support fromUltrasonix and acted as consultants for Ultrasonix in 2012.
FundingThisworkwas supported by internal Department of Anesthesi-ology funding only.
References1 Pages F. Anestesia Metamerica. Rev Sanid Mil Madr 1921; 11:
351–96 (in Spanish)
2 Dogliotti A. A new method of block anaesthesia. Segmental peri-dural spinal anaesthesia. Am J Surg 1933; 20: 107–18
3 Miller RD, Eriksson LI, Fleisher LA,Wiener-Kronish JP.Miller’s Anaes-thesia, 7th Edn. Philadelphia: Churchill Livingstone Elsevier, 2009
4 Weed JT, Taenzer AH, Finkel KJ, Sites BD. Evaluation of pre-procedure ultrasound examination as a screening tool for difficultspinal anaesthesia. Anaesthesia 2011; 66: 925–30
5 Brinkmann S, Germain G, Sawka A, Tang R, Vaghadia H. Is there aplace for ultrasound in neuraxial anesthesia? Imaging Med 2013;5: 177–86
6 Podder S, Kumar N, Yaddanapudi LN, Chari P. Paramedian lumbarepidural catheter insertion with patients in the sitting position isequally successful in the flexed and unflexed spine. Anesth Analg2004; 99: 1829–32
7 GrauT, LeipoldR,DelormeS,MartinE,MotschJ.Ultrasound imagingof thethoracicepidural space.RegAnesthPainMed2002;27: 200–6
8 ChinKJ,KarmakarMK,PengP.Ultrasonographyof theadult thoracicand lumbar spine for central neuraxial blockade. Anesthesiology2011; 114: 1459–85
9 Jones AR, Carle C, Columb M. Effect of table tilt on ligamentumflavum length measured using ultrasonography in pregnantwomen. Anaesthesia 2013; 68: 27–30
10 Abo A, Chen L, Johnston P, Santucci K. Positioning for lumbar punc-ture in children evaluated by bedside ultrasound. Pediatrics 2010;125: 1149–53
11 Sandoval M, Shestak W, Sturmann K, Hsu C. Optimal patient pos-ition for lumbar puncture, measured by ultrasonography. EmergRadiol 2004; 10: 179–81
12 Brinkmann S, Tang R, Sawka A, Vaghadia H. Assessment of a realtime ultrasound guided spinal technique using SonixGPS inhuman cadavers. Can J Anaesth 2012; 59: 1156–7
13 Chinn KJ, Karmakar MK, Peng P. Ultrasonography of the adult thor-acic and lumbar spine for central neuraxial blockade. Anesthesi-ology 2011; 114: 1459–85
14 Chinn KJ, Perlas A, Singh M, et al. An ultrasound assisted approachfacilitates spinal anesthesia for total joint arthroplasty. Can JAnaesth 2009; 56: 643–50
Optimizing the thoracic epidural window through positioning BJA
561
76

15 Karmakar M, Li X, Kwok WH, et al. Sonoanatomy relevant forultrasound-guided central neuraxial blocks via theparamedianap-proach in the lumbar region. Br J Radiol 2012; 85: 262–9
16 Grau T, Rudiger W, Horter J, Conradi R, Martin E, Motsch J. Parame-dian access to the epidural space: the optimum window for ultra-sound imaging. J Clin Anesth 2001; 13: 213–7
17 Furness G, Reilly M, Kuchi S. An evaluation of ultrasound imagingfor identification of lumbar intervertebral level. Anaesthesia 2002;57: 277–80
18 ChinKJ,RamloganR,ArzolaC,SinghM,ChanV.Theutilityofultrasoundimaging in predicting ease of performance of spinal anesthesia in anorthopedic patient population. Reg Anesth Pain Med 2013; 38: 34–8
19 White AA, Panjabi MM. Kinematics of the Spine. Clinical Biomechan-ics of the Spine, 2nd Edn. Boston: Lippincott Williams & Wilkins,1990; 102–23
20 Gregersen G, Lucas D. An in vivo study of the axial rotation of thehuman thoracolumbar spine. J Bone Joint Surg Am 1967; 49:247–62
Handling editor: J. P. Thompson
BJA Ramsay et al.
562
77

CARDIOVASCULAR
Comparison of the effects of albumin 5%, hydroxyethyl starch130/0.4 6%, andRinger’s lactate onblood loss and coagulationafter cardiac surgeryK. Skhirtladze1, E. M. Base1*, A. Lassnigg1, A. Kaider2, S. Linke1, M. Dworschak1 and M. J. Hiesmayr1
1 DivisionofCardiothoracicandVascularAnaesthesiologyandIntensiveCareMedicine,DepartmentofAnaesthesiology,General IntensiveCareand Pain Medicine, Medical University of Vienna, Vienna, Austria2 Centre forMedical Statistics, Informatics and Intelligent Systems, Section for Clinical Biometrics, Medical Universityof Vienna, Vienna, Austria
* Corresponding author. E-mail: [email protected]
Editor’s key points
† The perioperative use ofcolloid solutions haspotential benefits in cardiacsurgical patients, but mayaffect coagulation.
† In this randomized study of240 patients, the use ofhigh volumes of colloid(50 ml kg21 day21) had noeffect on the primaryoutcomemeasure, blood lossfrom chest drains.
† However, blood transfusionrequirements were lowerwhen a crystalloids-onlyfluids regimen was used.
† The infusion of high volumesof colloids caused morehaemodilution and hadgreater adverse effects oncoagulation.
Background. Infusionof5%humanalbumin (HA)and6%hydroxyethyl starch130/0.4 (HES)during cardiac surgery expand circulating volume to a greater extent than crystalloids andwould be suitable for a restrictive fluid therapy regimen. However, HA and HES may affectblood coagulation and could contribute to increased transfusion requirements.
Methods. We randomly assigned 240 patients undergoing elective cardiac surgery toreceive up to 50 ml kg21 day21 of either HA, HES, or Ringer’s lactate (RL) as the maininfusion fluid perioperatively. Study solutions were supplied in identical bottles dressed inopaque covers. The primary outcome was chest tube drainage over 24 h. Bloodtransfusions, thromboelastometry variables, perioperative fluid balance, renal function,mortality, intensive care unit, and hospital stay were also assessed.
Results. Themedian cumulative blood loss was not different between the groups (HA: 835,HES: 700, and RL: 670ml). However, 35%of RL patients required blood products, comparedwith 62% (HA) and64%(HESgroup; P¼0.0003). Significantly,more studysolutionhad to beadministered in the RL group compared with the colloid groups. Total perioperative fluidbalance was least positive in the HA group [6.2 (2.5) litre] compared with the HES[7.4 (3.0) litre] and RL [8.3 (2.8) litre] groups (P,0.0001). Both colloids affected clotformation and clot strength and caused slight increases in serum creatinine.
Conclusions.Despite equal blood loss fromchest drains, both colloids interferedwith bloodcoagulation and produced greater haemodilution, which was associated with moretransfusion of blood products compared with crystalloid use only.
Keywords: blood loss; coagulation; colloids; fluid regime; Ringer’s lactate; rotationthromboelastometry; transfusion
Accepted for publication: 16 August 2013
Controversy exists about the optimal perioperative fluid man-agement in patients undergoing major surgery. Prevention offluid overload intraoperatively has been associated with lesspostoperative complications.1 In addition, the transfusion ofpacked red blood cells (PRBCs) is associated with increasedmorbidity and mortality after cardiac surgery.2 Thus, avoidingtransfusion might also be important to improve outcome ofpatients undergoing cardiac procedures.
Crystalloids, in the formof Ringer’s lactate (RL), and colloidssuch as hydroxyethyl starches and 5% human serum albumin(HA) are commonly used for intraoperative fluidmanagementduring heart surgery. The latter two have a more profoundvolumeexpansioneffect than crystalloids andwould therefore
be more suitable for a restrictive fluid therapy.3 However,hydroxyethyl starch solutions have been shown to impair co-agulation4 5 and renal function.6–11 Six per cent hydroxyethylstarch 130/0.4 [Voluvenw] (HES) is a newer generation tetra-starch formulation with a lower molecular weight,whichmight affect coagulation to a lesser degree than hydro-xylethyl starch solutions with higher molecular weight.12–15
However, a recent meta-analysis stated that insufficient dataare available for the effect of HES on the bleeding tendencyin cardiac patients.16 In comparison with HES, HA has beenused since the 1970s during cardiac surgery mainly for tworeasons: first, HA is able to coat the fluid pathway surfaceand thereby reduces platelet activation and consumption
British Journal of Anaesthesia 112 (2): 255–64 (2014)Advance Access publication 29 October 2013 . doi:10.1093/bja/aet348
& The Author [2013]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
78

with concomitant release of inflammatory mediators.3 17–19
Secondly, HA prevents a substantial decrease in colloid oncoticpressure.20 Likewise, RL has also been used for many yearsduring heart surgery, either as the sole replacement fluid or incombinationwithHAorHES.21Since largevolumesaregenerallyadministered throughout the procedure, even RL might influ-ence coagulation via dilution of coagulation factors.
Wehypothesized that6%HES130/0.4would increase bloodloss fromthechestdrains. Thus, themainobjectiveof our studywas to compare external blood loss fromchest drains betweengroups receiving HA 5%, 6% HES 130/0.4, or RL as the maininfusion during cardiac surgery. Blood transfusions, totalperioperative fluid balance, thromboelastometry variables,course of serum creatinine and platelet count, intubationtime, intensive care unit (ICU), and hospital stay were alsoassessed.
MethodsParticipants
This randomized, double-blind, single-centre trial, which wasconducted over the course of four consecutive years at our de-partment was approved by the institutional review board andreported to the national regulatory authority (Gov Identifier:NCT 01174719). All 240 patients provided written informedconsent before inclusion. Inclusion criteriawere: patientsunder-goingelective cardiovascular surgery [i.e. coronaryarterybypassgrafting (CABG), valve repair or replacement, and surgery of theascending aorta] on cardiopulmonary bypass (CPB). Exclusioncriteria were known allergy to hydroxyethyl starch or albumin,preoperative anaemia, emergencies, treatment with acetylsali-cylic acid ,3 days before surgery, GPIIbIIIa antagonists use,7 days before surgery, coagulation disorders [i.e. INR .1.2,activated partial thromboplastin time (aPTT) .40 s, plateletcount,100 g litre21], BMI.40 kgm22, left ventricular ejectionfraction ,20%, renal dysfunction defined as serum creatinine.1.5 mg dl21, proven heparin-induced thrombocytopenia, anddanaparoid or lepirudin treatment during the month beforethe operation.
Randomization, fluid regimen, and blinding
Eligible patients were randomized into three groups compris-ing 80 patients each with the following fluid regimens:
HAgroup: 5%albumin up to 50ml kg21 day21, additional RLas required;HESgroup:6%HES130/0.4upto50mlkg21day21,additionalRL as required;RL group: RL up to 50 ml kg21 day21, additional RL asrequired.
An independent IT specialist was in charge of randomization,which was performed using a random number generator.The local pharmacy prepared the study solutions that weresupplied in identical 250 ml bottles. Blinding was performedwith the help of opaque covers that were placed around thebottles and the infusion sets.
Procedures
Anaesthesia was induced with midazolam (0.1 mg kg21),propofol (1.0–1.5mg kg21), fentanyl (3–10mg kg21), and cisa-tracurium (0.2 mg kg21) and maintained with sevoflurane(target BIS value 40–50), and fentanyl (0.05–0.1 mg kg21
min21). Fluid administration was started with 250–500 ml ofthe study solution during induction of anaesthesia. The CPBcircuit was primed with 1500 ml study solution together with5000 IE heparin, and 100 ml mannitol 20%. Patients receivedeither aprotinin (106 IU after anaesthesia induction plus 106
IU added to the CBP prime) or tranexamic acid (either 1.0 or1.5 g after anaesthesia induction plus the same dosage inthe CPB prime according to the patient’s body weight andrenal function). Tranexamic acid was used as antifibrinolyticafter November 2007 when sale of aprotinin was suspendedby Bayer. After anticoagulation with heparin (300 IE kg21)and achieving an activated clotting time (ACT) .400 s, CPBwas performed using non-pulsatile flow at 2.5 litre min21
m22, a non-heparin-coated circuit, and a membrane oxygen-ator (QuadroxTM, Maquet, Hirrlingen, Germany, or DidecoCompactflowTM,Mirandola, Italy).Mild-to-moderatehypother-mia was induced (30–348C) and norepinephrine was given ifnecessary to maintain a mean arterial pressure . 60 mm Hg.Buckbergcardioplegic solutionwasused formyocardialpreser-vation. Additional RL was added to the extracorporeal circuitwhen filling of the CPB reservoir was insufficient. During andafter weaning from CPB, transoesophageal echocardiographywas used to monitor myocardial performance and theimpact of fluid loading and inotropic support on ventricularfunction. Further fluid management and also vasopressorsand/or inotropic usewasat thediscretionof theattending con-sultantandnotcontrolledbyprotocol.All studycaseswereper-formedbyexperienced cardiac anaesthesia fellows supervisedby senior cardiac anaesthesiologists. Intraoperative fluidtherapy with study solution was restricted to two-thirds ofthe maximally allowed daily dose (i.e. 33.3 ml kg21). It wasassumed that anaesthesia and surgery would require agreater fluid load than the immediate postoperative period.Additional fluid requirements were met with RL in order toavoid accidental overdosage of either of the two colloids. Thelast third of the study solution (i.e. 16.7 ml kg21) was kept forthe initial volume replacement in the ICU that also guaranteedthat the totalpermitteddosewouldnotbeadministeredwithina short period of time.
Rotation thromboelastometry (ROTEMw Pentapharm CO,Munich, Germany) ex vivo coagulation variables were exam-ined using predefined tests: INTEM (ellagic acid activatedintrinsic pathway) and FIBTEM (with platelet inhibitor cytocha-lasin D, evaluating the contribution of fibrinogen to clot forma-tion).22 The samples were analysed within 120 s after bloodwas drawn from the central venous catheter and coagulationwas initiatedwithactivatorsusingasemi-automatedelectron-ic pipette systemaccording to themanufacturer’s instructions.Coagulation was allowed to proceed for 50 min. AutomaticROTEM variables were: clotting time (CT), clot formation time(CFT), a-angle, maximum clot firmness (MCF), and clot lysis.
BJA Skhirtladze et al.
256
79

These variables have been validated using standard coagula-tion tests.22 23 ROTEM quality control measures were under-taken weekly by our laboratory staff. Reference rangesfor ROTEM thromboelastometry variables were taken from amulti-centre investigation.24
Blood transfusion was performed according to STS-SCAtransfusionguidelines.25 26 Transfusion triggers for the transfu-sionof PRBCswere: haemoglobin (Hb) concentrationsof≤7.0gdl21 during and ≤8.0–9.0 g dl21 after CPB.
Administration of fresh-frozen plasma, platelets, and co-agulation factors was based predominantly on ROTEM vari-ables and the pre- and postoperative coagulation profile ofeach patient. After appropriate reversal of residual heparin,fresh-frozen plasma and factor concentrates were given inthe presence of prolonged CT and CFTINT and normal ACT.Fibrinogen was given when MCFFIB was ,8 mm, and plateletswere transfusedwhenMCFFIB was.8mm. In the ICU, Normo-testw .1.5, aPTT.60 s, fibrinogen concentration,1 g litre21,and platelet count ,50×109 litre21 prompted transfusion offresh-frozen plasma, platelets, or both.
Outcome variables
The primary outcome variables were clinical bleeding basedon chest tube drainage over the first 24 h after CPB. Secondaryoutcomes were transfusion of PRBCs, fresh-frozen plasma,platelets, fibrinogen, factor concentrate, changes in Hb,thromboelastometry variables, and the total amount ofstudy solution, total amount of administered fluid, fluidbalance, intubation time, and length of hospital stay. Further-more, the units of PRBC transfused within the second and thesixth postoperative day (POD), andalso the course of Hb, plate-lets, and creatinine until POD 6 were compared between thegroups. D creatinine was calculated as maximal creatininevaluewithin 48 hminus baseline creatinine.27 Since aprotininewas replaced by tranexamic acid during the investigationperiod, we also compared utilization of these agentsbetween the groups. Hb levels were compared at the start ofanaesthesia (baseline), after release of the aortic cross-clamp(surgery), upon arrival in the ICU, 24 h after surgery, and on themorning of the sixth POD. The length of stay in the ICU andmortality within 90 days were recorded as safety variables.
Statistical analysis
The sample size calculation was based on data from our insti-tutional data bank, where the actual blood loss from 99 CABGpatients was found to be 714 ml with a standard deviation(SD) of 370 ml. The study was powered to detect a differencein blood loss of 185 ml (i.e. half SD) between the active control(RL) and HA or HES with a type I error rate of 0.05 and apowerof 0.08 fora two-sided t-testwith correction formultiplecomparisons. Consequently, a sample size of 80 patients pergroup was required.
Data are given as mean (SD). Non-normally distributed vari-ables are expressed as median (25% and 75% percentiles).Non-parametric statistical tests were used for analysis if nonormal distribution could be achieved by log transformation.
Analyses of variance models were used for comparison ofthe log-transformed cumulative blood loss over 24 h aftersurgery, the infused study medication, and the cumulativepostoperative fluid balance over 24 h between the threegroups. Repeated-measures analyses of covariance (ANCOVA)modelswereused to test fordifferences in the log-transformedMCFFIB and CFTINT values between study groups, consideringbaseline values as covariates and time (arrival at the ICU vs24 h after surgery) as repeated factor. Repeated-measureANCOVA was also used for comparison of Hb, platelets, andcreatinine levels between the groups, additionally consideringvalues during surgery in the model. For all pair-wise compari-sons between the study groups, the Tukey post hoc test wasused to adjust for multiple comparisons. The non-parametricKruskal–Wallis test was used to test for differences innon-study fluids, cumulative dose of study fluid expressed asml kg21 day21, crystalloid to colloid ratio, intubation time,urine output, and D creatinine values between the groups.Thex2 testwasused tocompare frequenciesofpatients receiv-ing PRBC, FFP, platelets, fibrinogen, and factor concentratesbetween study groups. All P-values are reported as results oftwo-sided tests and values of,0.05were considered statistic-ally significant.
ResultsA total of 240 patients randomized into three groups wereincluded in the study. Patients’ characteristics and intra- andpostoperative data are shown in Table 1. Four patients wereexcluded for the following reasons: one patient from the HAgroup developed urticaria after induction of anaesthesia andthe study was terminated as a possible allergic reaction tothe study solution could not be ruled out. Another threepatients, two from the HA group and one from the RL group,were either haemodynamically unstable or became hypoxae-mic after CPB and required either support with an intraaorticballoon pump or ECMO. Minor violations of the study protocoloccurred in two patients. One patient mistakenly received1000 ml Voluvenw and another patient 600 ml of HA duringthe ICU stay within the study period, without being excludedfrom the study. Unblinding revealed that both patients werein the HES group. However, in the first patient, the cumulativeamount of colloids (HES as study solution and additional Volu-venw) did not exceed 50ml kg21 day21. In the second patient,the sum of the administered study solution and the given HAwas also within the tolerable range of 50 ml kg21 day21.Owing to inappropriate filling of an HA bottle with HES by ourpharmacy, the HES group comprised 81 patients and the HAgroup only 79; of whom, three patients had to be excluded asmentioned above. The recruitment profile is depicted as aCONSORT flow diagram in Figure 1.
Although there was a trend towards lower blood loss overchest tubes in the RL group, the primary study endpoint,namely chest tube drainage over 24 h after surgery, was notsignificantly different between the groups (P¼0.085; Table 2).Therewas, however, a significant group difference in the quan-tity of blood transfusion (P¼0.0004). Patients in the RL group
Fluid therapy and transfusion in cardiac surgery BJA
257
80

received fewer PRBCs compared with HA (P¼0.0015) and HESpatients (P¼0.0002). In addition, the percentage of patientsreceiving either PRBCs or any blood product was significantlylower in the RL group. In contrast, there was no difference forboth variables when HA and HES patients were compared(Table 2). Most units of PRBC were given perioperativelyduring the first 24 h. There were no significant group differ-ences in the number of PRBC units transfused within PODs 2–6 [HA: 2.04 (0.45); HES: 2.14 (0.79); RL: 2.15 (0.91) P¼0.544].Most PRBC units transfused during this period were orderedbetween POD 3 and 5. No significant inter-group differenceswere noted for transfused FFPandplatelets. A greater percent-age of patients in both colloid groups received fibrinogen.Regarding the amount of coagulation factor concentrates, nosignificant differences were found between the three groups.
Changes inHb levelsover timeandbetweenthegroupsweresignificantly different (Fig. 2). During surgery, Hb significantly
declined from baseline in all groups. However, patients in theRL group showed the least decline during surgery (P,0.0001)and at arrival in the ICU (P,0.0001). Twenty-four hours aftersurgery, patients in the HA group presented with the lowestHb values compared with the HES (P,0.0001) and the RLgroup (P,0.0001). No difference was observed between HESand RL patients at this time point. Likewise, no differencewas noted in Hb values among the three groups on POD 6[HA: 10.1 (1.3), HES: 10.3 (1.1) RL: 10.2 (1.1)]. Similar changeswere found for platelet count until POD 6 (Fig. 3B).
ROTEM thromboelastometry variables are depicted inTable 3. MCFFIB values decreased in all groups during surgerybut remained within the reference range in the HA and theRL groups. The lowest value was observed in the HES group atarrival in the ICU (P,0.0001). An increase in MCFFIB valueswas found in all groups between arrival in the ICU and 24 hafter surgery (P,0.0001). Values in the HA group were
Table 1 Patients’ characteristics and perioperative data. HA, 5%human serumalbumin; HES, 6%hydroxyethyl starch 130/0.4; RL, Ringer’s lactate;ESL, logistic EuroSCORE; BMI, bodymass index; LVEF, left ventricular ejection fraction; CABG, coronaryartery bypass grafting; VR, valve replacementor reconstruction; Combined procedure: valve and CABG surgery, or double valve replacement or valve replacement with composite graft; CPB,cardiopulmonary bypass; ACC, aortic cross-clamp; ICU, intensive care unit; vasopressors use is defined according to SOFA score; RRT, renalreplacement therapy. Values are either: numbers (n), percentages (%), means (SD), medians (25/75% percentile), or medians (lowest–highestvalue). *P,0.05 compared with colloid groups
HA (n576) HES (n581) RL (n579)
Patient characteristics
Male/female (n) 53/23 52/29 61/18
Age (yr) 66 (23–85) 67 (28–87) 67 (24–87)
BMI (kg m22) 27 (4) 27 (4) 27 (4)
ESL 5 (6) 6 (6) 5 (5)
LVEF (%)
.50 33 34 33
30–50 29 36 35
,30 34 33 33
Type of surgery (%)
CABG 37 33 30
VR 29 37 34
Combined procedure 32 32 36
Duration (min)
Anaesthesia 333 (74) 328 (76) 314 (55)
CPB 107 (32) 99 (42) 105 (40)
ACC 70 (23) 64 (29) 71 (28)
Use of antifibrinolytics (n)
Aprotinin 24 24 25
Tranexamic acid 52 55 54
Use of vasopressors (%) 70 75 72
Low 59 54 56
High 11 21 16
Postoperative data
Time to extubation (min) 580 (455/735) 562 (485/824) 530 (450/725)
ICU stay (day) 1 (1/16) 1 (1/48) 1 (1/16)
Hospital stay (day) 14 (7/66) 14 (8/55) 13 (6/164)
D Creatinine0–48 h (mg dl21) 0.06 (20.02/0.15) 0.02 (20.05/0.11) 20.02* (20.13/0.07)
RRT (n) 2 1 0
Mortality 90 day (n) 2 1 0
BJA Skhirtladze et al.
258
81

significantly lower at this time point when compared with theHES (P¼0.027) and the RLgroup (P,0.001). No statistically sig-nificant difference was found between the RL and the HESgroups (P¼0.083). CFTInt values increased intraoperatively.They were significantly different (P,0.0001) between thegroups on ICU arrival with the highest values being detectedin the HES group and the lowest in the RL group. Twenty-fourhours after surgery, the HA group showed significantly pro-longed CFTInt than patients of the RL (P,0.0001) and the HESgroups (P¼0.004). No significant difference was foundbetween the HES and the RL groups at this time (P¼0.193).
We recorded statistically significant group differencesregarding the total amount of infused study solution
(P¼0.0024). We observed no difference between the colloidgroups but significant differences between HA and RL(P¼0.0051), and also HES and RL, respectively (P¼0.0016;Table 4). Similarly, the fluid balance was significantly differentbetween the groups (P,0.0001). The HES group had a morepositive total fluid balance than the HA group (P¼0.0116),and the RL group an increased fluid balance compared withboth HES (P¼0.0262) and HA (P,0.0001). The crystalloid tocolloid ratio was lower in the HA relative to the HES group(P¼0.028). There were no group differences regarding urineoutput (P¼0.952, Table 4). Serumcreatinine levelswere signifi-cantly higher in the HA group immediately after surgery whencompared with the HES and RL groups and remained elevated
Enrolment
Allocation
Follow-up
Analysis
Assessed for eligibility (n=2548)
Randomized (n=240)
Allocated to HA (n=80)• Received allocated intervention (n=79)• Did not receive allocated intervention (inappropriate filling by dispensary) (n=1)
Lost to follow-up (haemodynamicinstability) (n=2)
Discontinued intervention(urticaria) (n=1)
Analysed (n=76)• Excluded from analysis (n=0)
Analysed (n=81)• Excluded from analysis (n=0)
Analysed (n=79)• Excluded from analysis (n=0)
Lost to follow-up (n=0)
Discontinued intervention (n=0)
Lost to follow-up (haemodynamicinstability) (n=1)
Discontinued intervention (n=0)
Allocated to HES (n=80)• Received allocated intervention (n=81)• Did not receive allocated intervention (inappropriate filling by dispensary) (n=1)
Allocated to RL (n=80)• Received allocated intervention (n=80)
Excluded (n=2308)• Not meeting inclusion criteria (n=1484: n=878 (antiplatelet drugs) n=606 (serum creatinine >1.5 mg dl–1)• Declined to participate (n=204)• Logistic reasons (n=620)
Fig 1 Consort 2010 flow diagram.
Fluid therapy and transfusion in cardiac surgery BJA
259
82

in relation to theRLgroup24hafter surgery (Fig. 3A).DCreatin-ine only increased in the colloid groups (Table 1).
Ten patients, seven in the HES and three in the HA group,required reexploration for bleeding, either on the day ofsurgery or on POD 1. One patient in the HES and one in theHA group, and also two patients of the RL group had reopera-tions after POD 5. Three patients died within 90 days, one inthe HES group (1.2%) and two in the HA group (2.5%) (Table 1).
Usage of the two different antifibrinolytic agents was notsignificantly different between the groups (P¼0.982; Table 1).
DiscussionThis is the first randomized controlled trial that directly com-pares the new-generation 6% hydroxyethyl starch 130/0.4[Voluvenw] (HES) and HA against RL for fluid managementduring cardiac surgery. Two hundred and forty patients wereincluded and randomized in three groups with 80 patients
per group. We used large volumes of fluid, as 50 ml kg21
day21 is the upper recommended daily limit for HES. We delib-erately chose this dosage to maximize the chance of demon-strating a significant effect. We found that fluid therapy withneither study solution caused increased external blood lossvia chest tubes after operation. However, transfusion of PRBCand transfusion of any blood product during the first 24 h ofthe study were increased in both colloid groups, both intra-operatively and after operation.
Table2 Chest tubedrainageand transfusionsuntil the first 24hafter surgery.HA, 5%humanserumalbumin;HES, 6%hydroxyethyl starch130/0.4;RL, Ringer’s lactate; PRBCs, packed red blood cells; FFP, fresh frozen plasma. Chest tube drainage and PRBCs are expressed as median (25/75%percentiles). All other variables are depicted as percentages. P-value as determined by univariate analysis
HA (n576) HES (n581) RL (n579) P-value
Chest tube drainage (ml) 835 (545/1253) 700 (540/1090) 670 (455/1015) 0.0850
PRBCs (ml) 300 (0/600) 300 (0/600) 0 (0/300) 0.0004
PRBCs (units) 1 (0/2) 1 (0/2) 0 (0/1) 0.0004
PRBCs intraoperative (ml) 0 (0/600) 0 (0/600) 0 (0/300) 0.0119
PRBCs postoperative (ml) 0 (0/275) 0 (0/250) 0 (0/0) 0.0333
FFP (%) 8 10 5 0.5152
Platelets (%) 7 14 5 0.1186
Fibrinogen (%) 12 16 4 0.0383
Factor concentrate (%) 3 6 3 0.3921
Percentage of patients receiving
PRBCs (%) 58 61 34 0.0013
Any blood product (%) 62 64 35 0.0003
18HAHESRL16
14
12
Hae
mog
lobi
n (g
dl–1
)
10
8
6
4Baseline
×–×–
×–
×
– ×
–
×
–
Surgery
×
–
×–
×–
×
–×–
×
–
* #
Arrival in ICU
* #
×
–
×
–
×–
×– ×–
×–
After 24 h
*
×
–
×
–×–
×– ×– ×–
POD 6
×–
×–
×–
×
–
×–
×–
Fig 2 Course of Hb concentration. *P,0.05 HA vs RL; #P,0.05 HESvs RL; WP,0.05 HES vs HA.
1.4A
B
* #
* #
1.3
1.2
1.1
1.0
Cre
atin
ine
(mg
dl–1
)P
late
lets
(10
9 lit
re–1
)
0.9
0.8
0.7
0.6
0.5
300
250
200
150
100
50
Baseline Arrival in ICU After 24 h POD 6
Baseline Arrival in ICU After 24 h POD 6
HAHESRL
HAHESRL
Fig 3 Time course of creatinine (A). *P,0.01 HA vs HES and RL;#P,0.0248 HA vs RL and platelets (B). *P,0.0001 RL vs HA andHES; #P,0.0156 HA vs HES.
BJA Skhirtladze et al.
260
83

Our results are in line with published studies andmeta-analyses comparing crystalloids and colloids for cardiacsurgery. Colloids at all times produced a less positive fluidbalance yet postoperative bleeding often did not differbetween crystalloids and colloids.3 28 Studies comparingalbumin with non-protein colloids during cardiac surgery werein the majority in favour of albumin regarding transfusionrequirements and mortality.29–31 However, in those studies,oldergenerationstarcheswereusedwhichconsistedofhighmo-lecular weight molecules with high molar substitution and thenew-generation HES 130/0.4 6% was not included. In contrast,perioperative volume replacement with up to 50 ml kg21 HESor 50ml kg21 4% human serumalbumin in children undergoingcongenital heart surgery resulted in fewerallogenic blood trans-fusions in the HES group compared with the albumin group(median: 18 vs 29 ml kg21).32 This was explained by a more
profound haemodilution induced by 4% albumin. Both colloidswere, however, not compared against a crystalloid solution.
In a recentmeta-analysis byNavickis and colleagues, it wasconcluded that hydroxyethyl starches were associated withincreased blood loss, reoperation for bleeding, and bloodproduct transfusion in relation to albumin after adult cardiacsurgery. However, insufficient data still are available forHES.16 Previous trials investigating blood loss and transfusionrequirements in adult cardiac surgery patients to date eithercompared HES with hydroxyethyl starch 200/0.533 34 or HESwith crystalloids.35 36 In two smaller studies (n¼15 pergroup), Schramko and colleagues compared HES withRinger’s acetate and 4% gelatine37 and with hydroxyethylstarch 200/0.5 and 4% albumin, respectively.34 The latter,however, had no study arm with a crystalloid solution as anactive control. No difference in blood loss and transfusion
Table 3 Thromboelastometry analysis. HA, 5% human serum albumin; HES, 6% hydroxyethyl starch 130/0.4; RL, Ringer’s lactate; CFT, clotformation time;MCF,maximal clot firmness.P-valuesaregivenasdeterminedbyunivariateanalysis. *P,0.05RLvsHES; #P,0.05HAvsRL; †P,0.05HES vs HA; NS, not significant (according to post hoc analysis). Values are expressed as medians (25/75% percentile)
HA (n576) HES (n581) RL (n579) P-value
CFTINT (reference range: 40–100 s)
Baseline 69 (57/82) 69 (57/81) 74 (64/83) NS
Arrival in ICU 137 (111/175)# 185 (137/253)† 107 (85/138)* ,0.0001
After 24 h 100 (85/125)# 89 (75/112)† 84 (71/109) 0.0042
MCFFIB (reference range: 9–25 mm)
Baseline 19 (15/22) 19 (15/22) 18 (15/21) NS
Arrival in ICU 10 (9/13)# 7 (6/10)† 13 (11/17)* ,0.0001
After 24 h 15 (13/19)# 18 (14/21)† 18 (16/20) 0.0266
Table 4 Perioperative fluids, fluid balance, and urine output. HA, 5% human serum albumin; HES, 6% hydroxyethyl starch 130/0.4; RL, Ringer’slactate. Values for fluid balance are expressed asmeans (SD). Study solution, non-studyfluids, cumulative doses of studysolution asml kg21 day21,crystalloid to colloid ratio, and urine output as non-normally distributed values are expressed asmedians (25/75% percentile). P-value is given forthe univariate analysis. Non-study fluids are including crystalloid solutions, analgesics, antibiotics, and glucose–electrolytes. Fluid balance wascalculated from infused study solution, non-study fluids, transfusions, fibrinogen, factor concentrate, and urine output and also blood loss fromdrainage
HA (n576) HES (n581) RL (n579) P-value
Study solution (ml)
Intraoperative 2500 (2250/3000) 2500 (2250/2750) 3000 (2500/3500) ,0.0001
Postoperative 750 (500/1000) 625 (500/1000) 750 (500/1000) 0.7717
Total 3250 (2750/3750) 3000 (2750/3500) 3500 (3000/4000) 0.0027
Non-study fluids
Intraoperative 2800 (2250/3557) 2350 (1900/2900) 3450 (2474/4350) ,0.0001
Postoperative 4757 (3102/5407) 5450 (4380/7090) 5570 (4350/6800) 0.0003
Total 7504 (5378/9147) 7870 (6902/10 220) 8700 (7419/11 143) 0.0006
Fluid balance (ml)
Intraoperative 3969 (1173) 3573 (1125) 4836 (1298) ,0.001
Postoperative 2272 (1874) 3755 (2454) 3565 (2190) 0.0114
Total 6228 (2456) 7365 (2980) 8336 (2810) ,0.0001
Study solution (ml kg21 day21) 44 (34/49) 42 (35/48) 47 (41/49) 0.0084
Crystalloid to colloid ratio 1.4 (0.9/2) 1.7 (1.2/2.5) NA 0.0281
Urine output0–24 h (ml) 2705 (2010/3455) 2734 (1980/3400) 2930 (2070/3540) 0.9518
Fluid therapy and transfusion in cardiac surgery BJA
261
84

requirement was found between HES and hydroxyethyl starch200/0.5 given at a median dose of 33 ml kg21. After dual anti-platelet therapy,Leeandcolleaguesalsocouldnotfindadiffer-ence in perioperative blood loss between crystalloids and HESwhen administered up to 30ml kg21. Furthermore, Tiryakiogluand colleagues did not observe a negative effect on chest tubedrainageandneed for transfusionwhen1500mlHESwasusedfor CPB prime instead of Ringer. Although the novel HES prep-aration was reported to have only aminimal effect on haemo-stasis,15 HES impaired fibrin formation and clot strength aftercardiac surgery following a total dose of 15 and 28 ml kg21
but did not negatively affect blood loss.34 37 Similarly, in thestudy by Choi and colleagues,38 both 500 ml HES and 500 mlHA in the pump prime negatively affected blood coagulationin patients undergoing mitral valve surgery. In contrast todata published by Schramko and colleagues,34 both colloids(i.e. HA as well) equally prolonged fibrin formation and fibrinbuild-up, depressed thea-angle, depressed themaximal amp-litude, and shear elasticmodulus. Presumably, the HES and HAgroups therefore also showed no difference in intra- and post-operativeblood loss, in theamountof co-administered colloidsand crystalloids, in urine output, and in the amount of trans-fused units of PRBC, FFP, and platelets. Again, both colloidswere not compared against a crystalloid solution.
In contrast, patients in this trial received up to 50 ml kg21
study solution. Therefore, dilution of coagulation factors andalso platelets and platelet dysfunction should even be morepronounced. This could account for the increased CFTINT inboth colloid groups and the decreased MCFFIB in the HESgroup on arrival in the ICU. A slight increase in CFTINT wasalsonoticed in theRLgroup. ThemedianCFTINTvalues returnedto normal in all groups after 24 h. Changes of CFTINTandMCFFIBwere most distinct in the HES group, whereas in the RL group,changes were least. We chose these two ROTEM variables asthey were most affected after infusion of HES—even atsmaller doses.37 All patients in our study routinely receivedantifibrinolytic drugs and hyperfibrinolysis was not observedin any patient. Whereas enhancement of fibrinolysis,39 deple-tion of circulating coagulation factors40 and reduced plateletcount can be detected by ROTEM, impairment of platelet func-tion due to CPB,41 and the administration of HES14 42 and HA18
might be better tracked by specific platelet function tests.41 Aswe did not perform such tests, we cannot comment on theimpact of both colloids on platelet function in the present trial.
Nevertheless, the difference in transfusion requirements inour study can be explained either by the negative impact ofthe twocolloids onblood coagulationbut also by themorepro-found haemodiluting effect, which decreased Hb levels earlierbelow7.0andbelow8–9gdl21,whichwereour triggers to givePRBCduring and after CPB, respectively. This would explain thefact thatmore units of PRBCwere transfused in theHES andHAgroups, both intraoperativelyand immediatelyafteroperation.In contrast, fluid management with RL in this study was asso-ciated with the lowest rate for transfusion of blood products,but also with a more positive fluid balance. Albumin, HES,and RL are not considered equipotent intravascular volumeexpanders, but their relative potencies are variable.
Crystalloids are generally considered to be less potentvolume expanders than colloids, which initially increaseplasma oncotic pressure, preload, and cardiac output.Albumin had a plasma volume expanding potency that is40% higher than that of saline.43 In relation to HA, thevolume expansion effect of HES seems to be rather small.1011 Accordingly, fluid balance in this study was highest in theRL group and lowest in the HA group, whereas fluid balancein the HES group was intermediate. This is also reflected bythe crystalloid to colloid ratio that was lower in the HA groupin relationtoHES. Thevolumeexpansioneffectwasmainlypro-nounced intraoperatively, wheremore non-study fluids had tobe given in the RL group, particularly to maintain adequatefilling of the CPB reservoir. Vasopressor use was not differentbetween our groups, which is in line with previous studiesthat compared HES with control fluids.11 44 45
As has been shown previously, perioperative transfusion ofPRBCs and the necessity for reexplorations are strongly asso-ciatedwith increasedmortality, andalso pulmonaryand infec-tious complications.2 Although mortality was low in our trial,which was not powered to detect group differences in mortal-ity, the three patients who died within 90 days had been allo-cated to the HES and the HA groups, respectively. Similarly,reoperations due to bleeding complications were numericallyhigher in the two colloid groups.
This study has several limitations. It was conducted as adouble-blind, randomized, controlled trial to detect significantgroup differences in external blood loss via the inserted chesttubes. Itwasnot powered todetect differences inmajorcompli-cations (e.g. re-exploration, renal replacement therapy), andmortality. Much larger trials would have been needed toanswer those questions. However, the observed positive D cre-atininevalues in bothcolloidgroups indicate that thesepatientswereat increasedrisk for renal replacement therapyandgreatermortality.27 Furthermore, group differences in transfusion ofanybloodproductandPRBCwerehighlysignificant,which signi-fies that the trial was sufficiently powered to detect suchdifferences. Although there was no strict protocol for volumesubstitutionwhen comparedwithvasopressor use, fluid admin-istration in all groups was guided by the results from the trans-oesophageal echo exam and by clinical experience of a seniorstaff anaesthesiologist who had profound knowledge in trans-oesophageal echocardiography. The incidence of pruritus, apatient-relevant safety outcome variable, whose pathogeneticmechanism is tissue storage of starch molecules,46 was notrecorded. In a previous study that specifically addressed thisissue, we found that 4.6% of patients treated with HES wereaffected.47 However, several weeks may elapse after exposureto hydroxyethyl starches until onset of pruritus, which compli-cates proper assessment of groups at risk.
We conclude that all three fluid therapies did not affect ourmain outcome variable, namely chest tube drainage over 24 haftercardiac surgerywith CPB. However, the transfusion rateofPRBCsorofanybloodproductwashigher inbothcolloidgroups,since the transfusion trigger was reached earlier due tomore profound haemodilution in conjunction with a negativeimpact of HES and HA on blood coagulation. In addition, as D
BJA Skhirtladze et al.
262
85

creatinine increase solely occurred in these two groups,patients treated with these agentsmay also face an increasedlikelihood for kidney injury. Consequently, the use of largeamounts of HES and HA in elective cardiovascular surgery, asit was the case in this trial, might be harmful, since it appearsto be associated with an increased risk for blood transfusionand the need for renal replacement therapy.
Authors’ contributionsK.S.: patient recruitment, data collection, and writing manu-script. E.M.B.: generation of study protocol, administration ofstudy for Ethics committee and local authority, patient recruit-ment, writing and editing manuscript, and correspondingauthor. A.L.: generation of study protocol and editing manu-script. A.K.: statistical analysis. S.L.: data collection and prepar-ation of tables and figures. M.D.: patient recruitment andmanuscript editing. M.J.H.: generation of study protocol andfund raising.
AcknowledgementsWe thank the medical staff of the Department of Cardiothor-acic and Vascular Anaesthesiology and Intensive Care Medi-cine for their kind support.
Declaration of interestNone declared.
FundingFresenius Kabi supported the trial by refunding the expensesfor the study nurse and for all disposable articles. Thecompany was provided with the complete set of data ofthis investigation. Fresenius Kabi neither interfered with theinterpretation nor with the compilation of the manuscript.
References1 Holte K, Kehlet H. Fluid therapy and surgical outcomes in elective
surgery: a need for reassessment in fast-track surgery. J Am CollSurg 2006; 202: 971–89
2 Surgenor SD, Kramer RS, Olmstead EM, et al. The association ofperioperative red blood cell transfusions and decreased long-termsurvival after cardiac surgery. Anesth Analg 2009; 108: 1741–6
3 Russell JA, Navickis RJ, Wilkes MM. Albumin versus crystalloid forpump priming in cardiac surgery: meta-analysis of controlledtrials. J Cardiothorac Vasc Anesth 2004; 18: 429–37
4 Treib J, Haass A, Pindur G. Coagulation disorders caused byhydroxyethyl starch. Thromb Haemost 1997; 78: 974–83
5 de Jonge E, Levi M, Buller HR, Berends F, Kesecioglu J. Decreasedcirculating levels of vonWillebrand factorafter intravenousadminis-trationofa rapidlydegradablehydroxyethylstarch(HES200/0.5/6) inhealthy human subjects. Intensive Care Med 2001; 27: 1825–9
6 Cittanova ML, Leblanc I, Legendre C, Mouquet C, Riou B, Coriat P.Effect of hydroxyethylstarch in brain-dead kidney donors on renalfunction in kidney-transplant recipients. Lancet 1996;348: 1620–2
7 Dart AB, Mutter TC, Ruth CA, Taback SP. Hydroxyethyl starch (HES)versus other fluid therapies: effects on kidney function. CochraneDatabase Syst Rev 2010; 1: CD007594
8 Schortgen F, Girou E, Deye N, Brochard L. The risk associated withhyperoncotic colloids in patients with shock. Intensive Care Med2008; 34: 2157–68
9 Zarychanski R, Abou-Setta AM, Turgeon AF, et al. Association ofhydroxyethyl starch administration with mortality and acutekidney injury in critically ill patients requiring volume resuscitation:a systematic reviewandmeta-analysis. J AmMedAssoc 2013; 309:678–88
10 Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med 2012;367: 124–34
11 Myburgh JA, Finfer S, Bellomo R, et al.Hydroxyethyl starch or salinefor fluid resuscitation in intensive care. N Engl J Med 2012; 367:1901–11
12 Jungheinrich C, SauermannW, Bepperling F, Vogt NH. Volume effi-cacy and reduced influence on measures of coagulation usinghydroxyethyl starch130/0.4 (6%)withanoptimised invivomolecu-lar weight in orthopaedic surgery: a randomised, double-blindstudy. Drugs R D 2004; 5: 1–9
13 Konrad CJ, Markl TJ, Schuepfer GK, Schmeck J, Gerber HR. In vitroeffects of different medium molecular hydroxyethyl starchsolutions and lactated Ringer’s solution on coagulation usingSONOCLOT. Anesth Analg 2000; 90: 274–9
14 Franz A, Braunlich P, Gamsjager T, Felfernig M, Gustorff B,Kozek-Langenecker SA. The effects of hydroxyethyl starches ofvarying molecular weights on platelet function. Anesth Analg2001; 92: 1402–7
15 Kozek-Langenecker SA. Effects of hydroxyethyl starch solutions onhemostasis. Anesthesiology 2005; 103: 654–60
16 Navickis RJ, Haynes GR,WilkesMM. Effect of hydroxyethyl starch onbleeding after cardiopulmonary bypass: a meta-analysis of rando-mized trials. J Thorac Cardiovasc Surg 2012; 144: 223–30
17 Palanzo DA, Zarro DL, Manley NJ, Montesano RM, Quinn M,Gustafson PA. Effect of surface coating on platelet count dropduring cardiopulmonary bypass. Perfusion 1999; 14: 195–200
18 Adrian K, Mellgren K, Skogby M, Friberg LG, Mellgren G,Wadenvik H.Theeffect of albuminpriming solutiononplatelet activationduringexperimental long-term perfusion. Perfusion 1998; 13: 187–91
19 DiNardo J. Physiology and techniques of extracorporeal circulationin the pediatric patient. Pediatric Cardiac Anesthesia, 4th Edn.Lippincott Williams &Wilkins, 2005; 228–52
20 Ohqvist G, Settergren G, Bergstrom K, Lundberg S. Plasma colloidosmotic pressure during open-heart surgery using non-colloidor colloid priming solution in the extracorporeal circuit. ScandJ Thorac Cardiovasc Surg 1981; 15: 251–5
21 SadeRM,StroudMR,CrawfordFAJr,Kratz JM,DearingJP,BartlesDM.A prospective randomized study of hydroxyethyl starch, albumin,and lactatedRinger’s solution as primingfluid for cardiopulmonarybypass. J Thorac Cardiovasc Surg 1985; 89: 713–22
22 TheusingerOM,Nurnberg J, Asmis LM, Seifert B, SpahnDR. Rotationthromboelastometry (ROTEM) stability and reproducibility overtime. Eur J Cardiothorac Surg 2010; 37: 677–83
23 Rugeri L, Levrat A, David JS, et al.Diagnosis of early coagulation ab-normalities in trauma patients by rotation thrombelastography.J Thromb Haemost 2007; 5: 289–95
24 Lang T, Bauters A, Braun SL, et al. Multi-centre investigation onreference ranges for ROTEM thromboelastometry. Blood CoagulFibrinolysis 2005; 16: 301–10
25 Ferraris VA, Brown JR, Despotis GJ, et al. 2011 update to theSociety of Thoracic Surgeons and the Society of CardiovascularAnesthesiologists blood conservation clinical practice guidelines.Ann Thorac Surg 2011; 91: 944–82
Fluid therapy and transfusion in cardiac surgery BJA
263
86

26 Ferraris VA, Ferraris SP, Saha SP, et al. Perioperative bloodtransfusion and blood conservation in cardiac surgery: theSociety of Thoracic Surgeons and the Society of CardiovascularAnesthesiologists clinical practice guideline. Ann Thorac Surg2007; 83: S27–86
27 Lassnigg A, Schmid ER, Hiesmayr M, et al. Impact of minimalincreases in serum creatinine on outcome in patients aftercardiothoracic surgery: do we have to revise current definitions ofacute renal failure? Crit Care Med 2008; 36: 1129–37
28 HimpeD.Colloidsversuscrystalloidsasprimingsolutions forcardio-pulmonary bypass: a meta-analysis of prospective, randomisedclinical trials. Acta Anaesthesiol Belg 2003; 54: 207–15
29 Wilkes MM, Navickis RJ, Sibbald WJ. Albumin versus hydroxyethylstarch in cardiopulmonarybypass surgery: ameta-analysis of post-operative bleeding. Ann Thorac Surg 2001; 72: 527–33
30 SedrakyanA,GondekK,PaltielD, ElefteriadesJA.Volumeexpansionwith albumin decreases mortality after coronary artery bypassgraft surgery. Chest 2003; 123: 1853–7
31 Knutson JE, Deering JA, Hall FW, et al. Does intraoperative heta-starch administration increase blood loss and transfusion require-ments after cardiac surgery? Anesth Analg 2000; 90: 801–7
32 Hanart C, Khalife M, De Ville A, Otte F, De Hert S, Van der Linden P.Perioperative volume replacement in children undergoing cardiacsurgery: albumin versus hydroxyethyl starch 130/0.4. Crit CareMed 2009; 37: 696–701
33 Kasper SM, Meinert P, Kampe S, et al. Large-dose hydroxyethylstarch 130/0.4 does not increase blood loss and transfusionrequirements in coronary artery bypass surgery compared withhydroxyethyl starch 200/0.5 at recommended doses. Anesthesi-ology 2003; 99: 42–7
34 Schramko AA, Suojaranta-Ylinen RT, Kuitunen AH, Kukkonen SI,Niemi TT. Rapidly degradable hydroxyethyl starch solutionsimpair blood coagulation after cardiac surgery: a prospective ran-domized trial. Anesth Analg 2009; 108: 30–6
35 Lee JS, Ahn SW, Song JW, Shim JK, Yoo KJ, Kwak YL. Effect ofhydroxyethyl starch 130/0.4 on blood loss and coagulation inpatients with recent exposure to dual antiplatelet therapy under-going off-pump coronary artery bypass graft surgery. Circ J 2011;75: 2397–402
36 Tiryakioglu O, Yildiz G, Vural H, Goncu T, Ozyazicioglu A, Yavuz S.Hydroxyethyl starch versus Ringer solution in cardiopulmonary
bypass prime solutions (a randomized controlled trial).J Cardiothorac Surg 2008; 3: 45
37 SchramkoA, Suojaranta-Ylinen R, KuitunenA, Raivio P, Kukkonen S,Niemi T. Hydroxyethylstarch and gelatin solutions impair blood co-agulation after cardiac surgery: a prospective randomized trial. Br JAnaesth 2010; 104: 691–7
38 ChoiYS, ShimJK,HongSW,KimJC,KwakYL. Comparingtheeffectsof5%albuminand6%hydroxyethyl starch130/0.4oncoagulationandinflammatory response when used as priming solutions for cardio-pulmonary bypass.Minerva Anestesiol 2010; 76: 584–91
39 Jamnicki M, Zollinger A, Seifert B, Popovic D, Pasch T, Spahn DR.Compromised blood coagulation: an in vitro comparison of hydro-xyethyl starch 130/0.4 and hydroxyethyl starch 200/0.5 usingthrombelastography. Anesth Analg 1998; 87: 989–93
40 ScholsSE, LanceMD, FeijgeMA,etal. Impaired thrombingenerationand fibrin clot formation in patients with dilutional coagulopathyduring major surgery. Thromb Haemost 2010; 103: 318–28
41 Velik-Salchner C, Maier S, Innerhofer P, et al. An assessment of car-diopulmonary bypass-induced changes in platelet function usingwhole blood and classical light transmission aggregometry: theresults of a pilot study. Anesth Analg 2009; 108: 1747–54
42 Stogermuller B, Stark J, Willschke H, Felfernig M, Hoerauf K,Kozek-Langenecker SA. The effect of hydroxyethyl starch 200 kDon platelet function. Anesth Analg 2000; 91: 823–7
43 Finfer S, Bellomo R, Boyce N, French J, Myburgh J, Norton R. A com-parison of albumin and saline for fluid resuscitation in the intensivecare unit. N Engl J Med 2004; 350: 2247–56
44 Bayer O, Reinhart K, Kohl M, et al. Effects of fluid resuscitationwith synthetic colloids or crystalloids alone on shock reversal,fluid balance, and patient outcomes in patients with severesepsis: a prospective sequential analysis. Crit Care Med 2012; 40:2543–51
45 Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy andpentastarch resuscitation in severe sepsis. N Engl J Med 2008; 358:125–39
46 Bork K. Pruritus precipitated by hydroxyethyl starch: a review.Br J Dermatol 2005; 152: 3–12
47 Base EM, Standl T, Lassnigg A, et al. Efficacy and safety ofhydroxyethyl starch 6% 130/0.4 in a balanced electrolyte solution(Volulyte) during cardiac surgery. J Cardiothorac Vasc Anesth2011; 25: 407–14
Handling editor: J. P. Thompson
BJA Skhirtladze et al.
264
87


Evaluation of surgical conditions during laparoscopic surgeryin patients with moderate vs deep neuromuscular blockC. H. Martini1†, M. Boon1†, R. F. Bevers2, L. P. Aarts1 and A. Dahan1*
1 Department of Anesthesiology and 2 Department of Urology, Leiden University Medical Centre, P5-Q, Leiden 2300 RC, The Netherlands
* Corresponding author. E-mail: [email protected]
Editor’s key points
† Surgical conditions maybeaffectedbythedepthofneuromuscular block.
† This small study assessedconditions rated on afive-point scale by a singlesurgeon duringretroperitoneallaparoscopic procedures.
† Surgical conditions wererated significantly betterunder deepneuromuscular block.
† The rating of surgicalconditions on videoanalysis differedmarkedlybetween anaesthetistsand the surgeon.
Background. The routine use of neuromuscular blocking agents reduces the occurrence ofunacceptable surgical conditions. In some surgeries, such as retroperitoneal laparoscopies,deep neuromuscular block (NMB) may further improve surgical conditions compared withmoderate NMB. In this study, the effect of deep NMB on surgical conditions was assessed.
Methods. Twenty-four patientsundergoingelective laparoscopic surgery for prostatectomyornephrectomy were randomized to receive moderate NMB (train-of-four 1–2) using thecombination of atracurium/mivacurium, or deep NMB (post-tetanic count 1–2) using high-dose rocuronium. After surgery, NMB was antagonized with neostigmine (moderate NMB),or sugammadex (deep NMB). During all surgeries, one surgeon scored the quality of surgicalconditions using a five-point surgical rating scale (SRS) ranging from 1 (extremely poorconditions) to 5 (optimal conditions). Video images were obtained and 12 anaesthetistsrated a random selection of images.
Results. Mean (standard deviation) SRS was 4.0 (0.4) during moderate and 4.7 (0.4) duringdeep NMB (P,0.001). Moderate block resulted in 18% of scores at the low end of the scale(Scores 1–3); deep block resulted in 99% of scores at the high end of the scale (Scores 4and 5). Cardiorespiratory conditions were similar during and after surgery in both groups.Between anaesthetists and surgeon, there was poor agreement between scores ofindividual images (average k statistic 0.05).
Conclusions. Application of the five-point SRS showed that deep NMB results in an improvedquality of surgical conditions comparedwithmoderate block in retroperitoneal laparoscopies,without compromise to the patients’ peri- and postoperative cardiorespiratory conditions.
Trial registration. The study was registered at clinicaltrials.gov under number NCT01361149.
Keywords: laparoscopy; nephrectomy; neuromuscular block; prostatectomy; rocuronium;sugammadex; urological surgical procedures
Accepted for publication: 22 August 2013
Administration of muscle relaxation is essential in a variety ofprocedures as it causes an improvement of surgical conditions.For example, King and colleagues1 demonstrated that theroutine use of neuromuscular blocking agents reduced the fre-quency of unacceptable surgical conditions in radical prosta-tectomies. Improvement of surgical conditions may be evenmore important when the surgeon has to work in a narrowspace surrounded by muscles such as in the case of retroperi-toneal laparoscopic surgery. Itmaybeargued that in retroperi-toneal laparoscopic surgery, a deep neuromuscular block(NMB), with train-of-four (TOF) values of 0 and a post-tetaniccount (PTC) of 1–2, would further improveworking conditions.However, the use of deep NMB may come with complicationsincluding long-reversal times, incomplete recovery of
neuromuscular function compromising respiratory, andupper airway function, or the return of NMB after a period ofseeminglynormalneuromuscular function (recurarization).1–3
The development of sugammadex enables rapid reversal ofdeep NMB. Sugammadex is a modified g-cyclodextrin, espe-cially created to bind the free plasma molecules of the neuro-muscular blocking agent rocuronium to which it has highaffinity.4 Recent studies demonstrate that sugammadexproduces rapid reversal of deep NMB after administrationof high-dose rocuronium.5 Theoretically, the combination ofrocuronium and sugammadex makes it possible to achievedeep NMB and consequently further improve surgical condi-tions in retroperitoneal laparoscopic surgery without thefear for prolonged reversal times or incomplete recovery of
† C.H.M. and M.B. contributed equally to this paper.
British Journal of Anaesthesia 112 (3): 498–505 (2014)Advance Access publication 15 November 2013 . doi:10.1093/bja/aet377
& The Author [2013]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
89

neuromuscular function. However, the association betweenthe depth of NMB and surgical conditions has not beenevaluated as yet.
In the current study, we investigated the effect of a deepNMB (TOF 0, PTC 1–2) against a moderate block (TOF 1–2) onsurgical conditions in patients undergoing retroperitoneal lap-aroscopic surgery foraprostatectomyor (partial) resectionof akidney. Surgical conditions were rated using a five-pointsurgical rating scale (SRS) by one dedicated surgeon withample experience in these surgeries (R.F.B.). We hypothesizethat deep NMB is associated with improved ratings by thesurgeon. Secondary end points of our study included theassessment of the level of agreement between anaesthetists(theprovidersof theNMBagentsandconsequently responsiblefor a large part of the surgical conditions) and surgeon in termsof their rating of the surgical conditions. To that end, 30 s videoimages of the surgical field, obtained at the time of scoring bythe surgeon, were rated by the anaesthetists.
MethodsThe study (acronym BLISS trial) was carried out between No-vember 2012 and February 2013 at the Leiden UniversityMedical Centre (Leiden, The Netherlands) and was performedaccording to guidelines of Good Clinical Practice and Good Re-searchPractice.Approvalof theprotocolwasobtained fromtheinstitutional reviewboard (CommissieMedischeEthiek, Leiden,The Netherlands). Patients scheduled to undergo an electivelaparoscopic prostatectomy or nephrectomy (partial or total)were approached 2 weeks before surgery and received oraland written information about the study. All patients whowere willing to participate gave written informed consentbefore enrolment. The studywas registeredat clinicaltrials.gov(NCT01361149); theprotocolwaspublishedearlieronline.6 Thedesign of the studywas randomized (deepNMB against stand-ard or moderate block) and blinded (the surgical team, the re-search team and the anaesthetists who scored the videowereall blinded to the treatment); the attending anaesthetist wasnot blinded. Randomizationwas performed using a computer-generated randomization code. The codewas presented to theattending anaesthetistwhoprepared themedication and tookcare of patient dosing during anaesthesia.
Patients enrolled in the study had prostate or renal diseaseand were all eligible for surgical resection by laparoscopicapproach. All procedures were performed by one surgeon(R.F.B.). Excluded from participation were patients with ASAclass .III, age ,18 yr, inability to give informed consent,known or suspected neuromuscular disease, allergy to medi-cation to be used during anaesthesia, a (family) history ofmalignant hyperthermia, renal insufficiency (serumcreatinine.2 times normal, urine output ,0.5 ml kg21 h21, glomerularfiltration rate ,60 ml h21, or proteinuria), previous retroperi-toneal surgery, and a body mass index of ≥35 kg m22.
Perioperative protocol
All patients received total i.v. anaesthesia with propofol andsufentanil. During the procedure, routine monitoring was
applied [electrocardiography, arterial blood pressure, heartrate, electroencephalographicmonitoringusing thePhilipsbis-pectral index (BIS) module system (Philips, Eindhoven, TheNetherlands)]. Propofol dosing was such that BIS valuesremained within the range of 40–50. Additionally, thecardiac output was measured non-invasively using an inflat-able finger cuff attached to the Nexfin haemodynamicmonitor (bmeye, Amsterdam, The Netherlands).
Withrespect toNMBthepatientswere randomlyassignedtoone of the two treatment groups:
Group 1: moderate NMB, in which the goal was to realize amoderate NMB (TOF 1–2 twitches). NMB was induced withabolusdoseof atracuriumof0.5mgkg21, followedbyacon-tinuous infusion of mivacurium of 0.5 mg kg21 h21. In thecase of deviations from the target TOF values, the pumpspeed could be increased or decreased or a bolus dosecouldbegiven.Thiswas left to thediscretionof theattendinganaesthetist. We used atracurium/mivacurium in Group 1rather than low-dose rocuronium, as this combination isthe current standard of care in our hospital. This approachenables us to qualify our current local practice against anew paradigm, which is deep NMB for the chosen surgicalprocedures.Group2: deepNMB, inwhich thegoalwas to realizeablockofzero twitches in the TOF, but 1–2 twitches in the PTC. To thatend, patients received a loading dose of rocuronium of 1.0mg kg21 followed by a continuous infusion of 0.6 mg kg21
h21. In the case of deviations from the target TOF and PTC,the pump speed could be increased or decreased or abolus dose could be given. This was left to the discretion ofthe attending anaesthetist.
In the case of poor or extremely poor surgical conditions (asscored by the surgeon, see below), mivacurium or rocuroniuminfusion rates were increased by 20% after the administrationof a bolus dose of 15 mg.
At the end of surgery, all patients received a reversal agent:neostigmine after a moderate NMB (1–2 mg combined with0.5–1 mg atropine) and sugammadex (4 mg kg21) after adeep NMB. Extubation occurred when the TOF ratio was .0.9.
Administration of all drugs was performed by the attendinganaesthetistsandnotcorresponded to thesurgical teamor theanaesthesia research team.
Monitoring
Neuromuscular function using an acceleromyograph wasmeasured at the wrist (TOF-watch-SX, MSD BV, Oss, The Neth-erlands). The TOF-watch generates an electrical stimulus tothe ulnar nerve and measures contractions of the adductorpollicis muscle (causing adduction of the thumb) through asensor attached to the tip of the thumb. The thumb wasplaced in a flexible adaptor that applied a constant preloadto the thumb. Before administration of any NMB agent, thedevice was calibrated according the specifications of themanufacturer. To thatend, beforeadministrationof anyneuro-muscular blocking agent, but after induction of general anaes-thesia, the following procedures were conducted to
Surgical conditions during laparoscopy BJA
499
90

standardize the neuromuscularmonitoring: (i) application of atetanic ulnar nerve stimulation (50 Hz for 5 s); (ii) calibration ofthe TOF watch; and (iii) performing a series of TOF measure-ments ensuring that the TOF ratio differs by ,5% betweenmeasurements. If the TOF ratio differed by .5% the TOFwatch was recalibrated. The TOF ratio was normalized to thevalues obtained during the calibration procedure. After thesesteps, the neuromuscular blocking agent was administeredaccording to protocol.
The number of thumb twitches upon electrical stimulationof theulnarnervewasmeasuredand recorded.At15min inter-vals, the TOFwasmeasured and in the case of TOF¼0, this wasfollowed by the PTC. In our study, a TOFof 1–2 reflects a stand-ard block and a PTC of 1–2 reflects a deep NMB. Finally, whenfour twitches were present in the TOF, the ratio of the fourthto the first twitch was determined (the TOF ratio).
Surgical rating scale
During the laparoscopicprocedure, the surgeon scored thesur-gicalworking conditions at 15min intervals according toafive-point ordinal scale ranging from 1 (extremely poor conditions)to 5 (optimal conditions) (Table 1). Extremely poor (Score 1)indicates that the surgeon is unable towork because of cough-ing or of the inability to obtain a visible field because of inad-equate muscle relaxation; poor (Score 2) indicates that thereis a visible field, but the surgeon is severely hampered by inad-equate muscle relaxation with continuous muscle contrac-tions, movements, or both; acceptable (Score 3) indicatesthat the there is a wide visible field but muscle contractions,movements, or both occur regularly; good (Score 4) indicatesawideworking field with sporadicmuscle contractions, move-ments, or both; excellent (Score 5) indicates a wide visibleworking field without any movement or contractions. In the
case of a sudden deterioration of conditions additional mea-surements could be added. The feasibility of this method ofscoring was investigated during five surgical procedures notincluded in the study.
Video images
Eachtimethesurgeon ratedthesurgical conditionsa30svideoimage was captured using a camera connected to the endo-scopic probe placed in the retroperitoneal surgical space. Theprocedure was such that the images collected give a visualindication of the surgical condition at the time of scoring. Arandomized subset of these images (n¼10) was presented to12 anaesthetists with ample experience in giving anaesthesiafor urological laparoscopic procedures. Theywereasked togivea rating to the surgical condition using the same five-pointscale as used by the surgeon. These anaesthesia expertswere blinded to the level of NMB and goals of the study.
Data acquisition
The following clinical variables were collected on the caserecord form for further analysis: anaesthesia-related variables[drug dosages, BIS, time from reversal to optimal extubationconditions (TOFratio.0.9)], haemodynamic variables (arterialblood pressure, heart rate, cardiac output, and cardiac index),ventilatory variables (tidal volume, breathing rate, and breath-ing pressure), surgical variables (SRS, intra-abdominal pres-sure, and duration of surgery), and post-anaesthesiacare-related variables [time spent in the post-anaesthesiacare unit (PACU), respiratory rate, oxygen saturation, painscore (on an 11-point numerical rating scale from 0, no pain,to 10, most severe pain imaginable), occurrence of nausea/vomiting and sedation (on a five-point scale ranging from 0,normal alertness to 5, not aroused by a painful stimulus)]. Re-current observations were made at 15 min intervals bothduring anaesthesia and in the PACU.
Sample size and statistical analysis
Thesamplesizewasbasedontheexpectationof thesurgeonforthe distribution of the surgical ratings between the two treat-ment conditions: rating during the moderate block¼5 occursin 10% of cases, 4 in 20%, 3 in 55% 2 in 10%, and 1 in 5%;rating during the deep block¼5 in 70% of cases, 4 in 20%, 3 in10%, 2 in 0%, and 1 in 0%. These anticipated frequenciesresult in an odds ratio of 21 for optimal conditions (SRS¼5) vsnon-optimal conditions (SRS,5). Ten thousand simulationswere performed to obtain the power for a given sample sizewithmoderate block as a fixed distribution and a simulated dis-tributionof thedeepblockconditionassumingproportionalityofthe odds ratiowith an odds ratio of 21 and analysing the resultswith a proportional oddsmodel using the score test. The powerranged from82%ata sample sizeof 14 (7 in eachgroup) to97%(n¼12 per group). A sample size of 24 was chosen to take intoaccount any margin of uncertainty around the effect size.
The data analysis was based on the intent-to-treat ap-proach. The primary end point of the study was the influenceof the depth of the NMB on the SRS. For each patient, the
Table 1 The surgical rating score
1 Extremely poor conditions: the surgeon is unable to workbecause of coughing or because of the inability to obtain avisible laparoscopic field because of inadequate musclerelaxation. Additional neuromuscular blocking agents must begiven
2 Poor conditions: there is a visible laparoscopic field, but thesurgeon is severely hampered by inadequatemuscle relaxationwith continuousmuscle contractions, movements, or bothwiththe hazard of tissue damage. Additional neuromuscularblocking agents must be given
3 Acceptable conditions: there is a wide visible laparoscopic fieldbut muscle contractions, movements, or both occur regularlycausing some interferencewith the surgeon’swork. There is theneed for additional neuromuscular blocking agents to preventdeterioration
4 Good conditions: there is a wide laparoscopic working field withsporadic muscle contractions, movements, or both. There is noimmediate need for additional neuromuscular blocking agentsunless there is the fear of deterioration
5 Optimal conditions: there is a wide visible laparoscopic workingfield without any movement or contractions. There is no needfor additional neuromuscular blocking agents
BJA Martini et al.
500
91

final score was the average of all 15 min SRS values. Thetreatment effect on the final score was tested using at-test (SigmaPlot version 12.5, Systat Software, Inc., SanJose, CA, USA). Secondary end points were (i) the assessmentof the level of agreement between anaesthetists andsurgeon in terms of their rating of the surgical conditionsand (ii) the effects of level of NMB on haemodynamic vari-ables during surgery, time to TOF.0.9, and relevant vari-ables in the PACU (pain rating, sedation levels, andcardiorespiratory variables). All variables were averagedover time to get an indication of their mean value. Treatmenteffects were evaluated on the average data by t-test.
The scores of each of the 12 anaesthetists were comparedwith that of the surgeon’s score using the k statistic (alsoknown as Cohen’s k) and population Bland–Altman ana-lysis.7–9 The k statistic calculates the agreement between apair of scores over and above what is expected from chance,where k¼[P(A)–P(E)]/[1–P(E)], P(A) is the proportion ofscores that agree and P(E) is the proportion of scores thatwould agree by chance.7 8 Kappa values between 0 and 0.2are indicative of poor to slight agreement, values between0.2 and 0.4 indicate fair agreement, 0.4 and 0.6 moderateagreement, 0.6 and 0.8 substantial agreement, and 0.8 and 1near complete to complete agreement.10 Bland–Altmanplots give the difference between paired measurements(scores) against the mean of the values, which results invalues for bias and limits of agreement to describe howclosely measurements from two sources are related.9
All values presented are mean (SD) unless otherwise stated.P-values ,0.05 were considered significant.
ResultsA total of 30 patients were screened. In four patients, one ormoreexclusioncriteriaweremet. Theotherswere randomized.
Two patients withdrew consent before treatment; two othersreplaced them. See Figure 1 for the flow chart of the study.Patient characteristics are given in Table 2 showing that thetwo treatment groups were similar in physical characteristics,gender, types of surgery, and haemodynamic variables.Duration of surgery was similar between treatment groupsand ranged from 80 to 240 min with average surgical timesof 141 and 144 min for standard care and deep NMB,respectively (Table 3).
Anaesthesia
Depth of anaesthesia, as measured by the BIS of the electro-encephalogram,was similar between treatment groups [mod-erate block 42 (5) vs deep block 44 (6)]. NMB in patientsreceiving a standard treatment was moderate with anaverage TOF of 2.2 (0.9) during surgery. Patients receiving adeep NMB had zero twitches in the TOF and 1.6 (1.5) twitchesin the post-tetanic count. During surgery, the dosagesof the anaesthetic (propofol) or analgesic (sufentanil), theintra-abdominal pressure and haemodynamic variables weresimilar between treatments (Table 3).
Rating of surgical conditions during laparoscopicsurgery
The rating of the surgical field was significantly differentbetween treatments with a mean rating of 4.0 (0.4) (range3.5–4.5, median 3.9) during a moderate NMB with TOF 1–2and 4.7 (0.4) (range 4.0–5.0, median 4.9) during a deep blockwith PTC 1–2 (P,0.001, Fig. 2). The distribution of all ratingstaken during surgery is shown in Figure 3. From these data,the significant difference between the moderate (TOF 1–2)and deep (PTC 1–2) blocks is apparent from the fact that18% of scorings during moderate block was in the SRS rangeof 1–3 (scores rated as less than good), while 99% of scoring
Assessed for eligibility:n=30 patients
Enrolled/randomized: n=26
Excluded: n=4
Withdrawal of consent: n=2
Allocated to intervention: n=24
n=12n=12
Moderate NMB (TOF=1–2) Deep NMB (PTC=1–2)
Fig 1 Study flow chart.
Surgical conditions during laparoscopy BJA
501
92

in thedeepblockwas in the SRS range4–5 (goodandexcellentscores). Variability in the individual ratings was higher for ablock with TOF¼1–2 (mean coefficient of variation of ratings
of surgical sessions 26%) compared with block with TOF¼0and PTC¼1–2 (5%).
Measurements after surgery
Reversal of the NMB in patients with a deep block with sugam-madex resulted in acceptable extubation conditions (TOF ratio.0.9) after 5.1 (2.4)min. In contrast, similar extubation condi-tions were obtained after 10.9 (4.9) min (P,0.01) in patientswith TOF 1–2 and reversal with neostigmine. In the PACU, nodifferences were observed in respiration, pain, and sedationlevels (Table 4).
Rating of surgical condition by anaesthetists
A random set of 10 video images was scored by 12 anaesthe-tists. The distribution of the surgeon’s ratings of these 10images is shown in Figure 4A; the corresponding distributionof ratings of the anaesthetists is shown in Figure 4B. Comparedwith the surgeon their ratings were skewed to the right andagreement with the surgeon’s ratings was poor (agreementbetween scores ranged from 0 to 40%). The k statistic was0.05 (range 20.25 to 0.25). The Bland–Altman analysisresulted in a significant bias of 20.43 (0.21) (P¼0.03) andlarge limits of agreement of 2.87 and –3.72, and a between-subject variance of 0.25 (Fig. 4C).
DiscussionThis is thefirststudy toassess the impactofadeepNMB(PTC1–2) on surgicalworking conditions. Themain results of our studyare: (i) a deep NMB (TOF 0 and PTC 1–2) is associated withhigher (i.e. improved) ratings from the surgeon comparedwithamoderateNMB (TOF1–2)during laparoscopicprostatec-tomies and nephrectomies, indicating a significant improve-ment of surgical conditions; (ii) ratings from anaesthetistsand surgeon of video images of the surgical field showed
Table3 Measurementsduring surgery.NMB, neuromuscular block;BIS, bispectral index; TOF, train-of-four; PTC, post-tetanic count;SRS, five-point surgical rating scale; AP, arterial pressure; HR, heartrate; CO, cardiac output; CI, cardiac index. Values are mean (SD).*P,0.001 vsmoderate NMB
Moderate NMB(TOF 1–2)
Deep NMB(PTC 1–2)
Duration of surgery(min) (range)
141 (50) (80–240) 144 (35) (90–195)
BIS 42 (5) 44 (6)
Propofol (g) 1.6 (0.8) 1.6 (0.4)
Sufentanil (mg) 73 (30) 78 (22)
Rocuronium (mg) 223 (81)
Atracurium (mg) 37 (10) –
Mivacurium (mg) 41 (24) –
TOF 2.2 (0.9) 0
PTC – 1.6 (1.5)
SRS 4.0 (0.4) 4.7 (0.4)*
Retroperitonealpressure (kPa)
1.5 (0.05) 1.4 (0.2)
AP systolic (kPa) 15.3 (2.6) 15.4 (1.7)
AP systolic (mm Hg) 115 (20) 116 (13)
AP diastolic (kPa) 9.1 (0.9) 9.2 (1.2)
AP diastolic (mm Hg) 68 (7) 69 (9)
HR (min21) 67 (10) 69 (13)
CO (litre min21) 4.9 (1.4) 5.6 (2.0)
CI (litre min21 m22) 2.5 (0.8) 2.8 (0.9)
Table 2 Patient characteristics and screening measurements. Allvalues are mean (SD) unless otherwise stated. BMI, body massindex; ABP, arterial blood pressure; HR, heart rate; CO, cardiacoutput; CI, cardiac index. Haemodynamic measurements wereobtained before induction of anaesthesia
Moderate NMB(n512)
DeepNMB (n512)
Prostate surgery (n) 7 7
Renal surgery (n) 5 5
Gender (M/F) 10/2 10/2
Age (median, range) 59 (28–74) 60 (24–70)
Weight (kg) 83 (14) 83 (10)
Height (cm) 180 (10) 180 (9)
BMI (kg m22) 25.8 (3.2) 25.9 (3.9)
ABP systolic (kPa) 19.6 (2.1) 18.9 (1.5)
ABP systolic (mm Hg) 147 (16) 142 (11)
ABP diastolic (kPa) 11.2 (2.2) 11.5 (1.6)
ABP diastolic (mm Hg) 84 (15) 86 (12)
HR (min21) 71 (12) 73 (15)
CO (litre min21) 5.9 (1.6) 5.8 (2.4)
CI (litre min21 m22) 3.0 (0.8) 3.1 (1.0)
5.0
P<0.001
4.5
3.5
3.0Moderate NMB Deep NMB
4.0
Sur
gica
l rat
ing
scal
e
Fig2 Surgical ratings by the surgeonduring laparoscopic surgeriesusing thefive-point SRS (see Table1). Squares denote the individualmean ratings obtained during surgery. Circles are the mean of themeans (SD). Standard indicates standard of care; deep NMB, deepneuromuscular block.
BJA Martini et al.
502
93

little agreement. In the current study, we chose to study retro-peritoneal laparoscopicsurgeries for twourologicalprocedures[prostatectomy and (partial) nephrectomy] as these proce-dures are confined to a narrowworking spacewhere adequate(deep)muscle relaxation is of high importance and aneffect ofless optimal muscle relaxation on the quality of the surgicalfield is rapidly apparent.
Surgical rating scale
The five-point rating scale used in our study was developed inclose cooperation with the surgeon involved in our project,who has ample experience in the performed procedures. Itwas decided that while the scoring system should integrateall qualitative aspects that are important to the surgeonwhen judging the surgical working field, it should remain assimple as possible. A scoring system with .5 points was
initially considered, suchasan11-pointnumericalquantitativescale (e.g. numerical rating or visual analogue scales from 0 to10, cf. Ref. 8); however, it was decided to rank the surgical fieldqualitatively from extremely poor, via poor, acceptable, goodto optimal conditions (see Table 1 for an explanation of the dif-ferent ratings). Further, to reduce variability in scoringbetweenassessors just one surgeonwas requested to score the surgicalfield inour study.Oursystemissimilar tootherscoringsystems.For example, the Clinical Global Impression (CGI) rating scale isa seven-point qualitative scale in which physicians rate theseverity of a patient’s mental illness relative to the physician’spast experience.11 The CGI and our scoring systems are sub-jective but in our case the ample experience of the surgeongives credibility to the procedure. Indeed, the results of ourstudy indicate that the surgeon was able to discriminatebetween a moderate and a deep NMB. The difference of 0.7points (a difference of 18%) was regarded as important andclinically significant by the surgical team. We argue that theability of our scoring system to discriminate between two dis-tinctanaesthetic regimes indicates thevalidityof thefive-pointSRS we developed.
Still, our study should be considered a proof-of-concept trialand further validation of the SRS is mandatory. Therefore, oneshould be cautious in extrapolation of our results to other pro-cedures and other surgeons. Other surgeonsmay rate the sur-gical condition differently and other procedures may require adifferentanaesthetic, surgicalapproach,orboth. Inanattemptto get an indication of the ability of other surgeonswith ampleexperience in laparoscopic surgery toapply thescoring system,we invited eight surgeons, specialized in laparoscopic surgeryfor gastroenterological procedures, to score the 10 videosearlier presented to the anaesthetists. Their k statistic wason average 0.50 indicative of moderate agreement. As
70
60
50
40
30
20Per
cent
age
of s
core
s
10
0
70
60
50
40
30
20Per
cent
age
of s
core
s
10
01 2 3 4 5
Surgical rating scale
1 2 3 4 5
Surgical rating scale
Deep NMB (PTC 1–2)Moderate NMB (TOF 1–2)A B
Fig 3 Distribution of the surgical ratings obtained during standard of care (A) and during deep NMB (B). NMB, neuromuscular block.
Table 4 Measurements after surgery. Values are mean (SD). TOF,train-of-four; PACU, post-anaesthesia care unit; SpO2
, arterialhaemoglobin oxygen saturation
ModerateNMB (TOF 1–2)
Deep NMB(PTC 1–2)
Sugammadex (mg) 380 (101)
Neostigmine (mg) 1 (0)
Time to TOF ratio .0.9 (min) 10.9 (4.9) 5.1 (2.4)
Time in PACU (min) 86 (19) 86 (25)
SpO2(%) 98.6 (1.8) 98.2 (1.4)
Breathing rate (min21) 14.5 (2.2) 14.5 (2.2)
Pain score (10-point scale) 2.6 (1.6) 2.1 (2.2)
Sedation score (five-point scale) 2.0 (0.6) 1.3 (1.0)
Surgical conditions during laparoscopy BJA
503
94

expected, this agreement is substantially greater than thatbetween surgeon and anaesthetists. It further shows that dif-ferent surgeons (in this casewith a different subspecialty) ratethe surgical field differently. The current study was specificallyaimed at scoring urological procedures performed in narrowretroperitoneal space. The results show a clinically relevantbenefit of deep NMB for the surgeon involved in this study.Whether this benefit will also be relevant to other surgeonsperforming similar surgeries and possibly even for otherlaparoscopic procedures, such as for bariatric laparoscopicsurgery is the topic of further research.
Deep neuromuscular block
Our a priori estimation of SRS distributions came close for thedeep NMB but was underestimated for the moderate block.Good and optimal conditions were achieved during standardcare (good 48% and optimal 34%) although at a lower fre-quency than during deep NMB (good 32% and optimal 67%).This indicates that in 82% of measurements during standardcare and in 99% during deep NMB conditions were good tooptimal. However, variability in ratings was high for moderateNMB compared with deep NMB: 26% vs 5%. Still, also in deepNMB, the range of scores (mean ranged from 4 to 5) was con-sidered high and is still open for improvement. Possibly,further improvement may be obtained by (more) strictly con-trolling anaesthetic depth, analgesic state, and arterialcarbon dioxide concentrations. In the current study, respiratorsettings were such that end-tidal carbon dioxide concentra-tions were between 4.4 and 6 kPa (33 and 56mmHg). High ar-terial carbon dioxide concentrations stimulate the respiratoryneuronal pool in the brainstem, which activates the phrenicnerve.12 As a consequence diaphragm contractions maypersist despite a deep NMB. The NMB at the diaphragm is lessintense than at the adductor pollicis muscle.13 14 Indeed,
some of the video images showed movement related to dia-phragm contraction unrelated to the ventilator-induced inspir-ation–expiration sequence or cardiac contractions despite TOFvalues of zero. The surgeon scored such conditions at the lowend of the SRS. In laparoscopic bariatric surgery, the workingspace volume and visibility increased in response to NMB.15 Inthe current study, the retroperitoneal pressure was kept con-stant to 1.3–1.5 kPa (9–11 mm Hg) in both groups and it maybe assumed that the working space volume was greater in thedeep NMB group. However, the scoring by the surgeon is onlyin part based on the perceived volume of the retroperitonealspace. Other factors similarly influence the surgeon’s workingconditions and consequently play an additional role in hisscoring. For example, muscle contractions (including thediaphragm) and resultant movement of other structures areimportant as well. Further studies should address these issues.
We tested deep vs moderate block using two differentdrug regimens. The reason for this was that this approachenabled us to compare our current practice with atracuriumand mivacurium with an approach that not only allows usto induce a deep NMB but also allows rapid reversal of thatdeep block. As our end point was to compare the depth ofthe NMB irrespective of the drugs used to induce that state,we do not believe that this influenced our outcome signifi-cantly. We observed that full reversal after deep NMB oc-curred after 5 min. It is important, however, to realize thatmeasurements were made at 5 min intervals and full reversalwith TOF ratios .0.9 may have occurred earlier (for sugam-madex reversal to TOF ratio .0.9 is expected after 2–3 min).
Scoring by anaesthetists of the surgical field
An important finding in our study is that the agreement ofscores between the anaesthetists and surgeon was poor. Thisindicates that the anaesthetists are less well able to measure
50
40
30
20
Per
cent
age
of s
core
s
10
01 2 3 4 5
Rating
50
40
30
20
Per
cent
age
of s
core
s10
01 2 3 4 5
Rating
4
2
0
–2
Diff
eren
ce b
etw
een
ratin
gs
–4
–61 2 3 4 5
Mean of ratings
Surgeon Anaesthetists Bland–Altman comparisonA B C
Fig 4 (A) Distribution of scorings obtained from a random sample of 10 video snippets scored by the surgeon. (B) Distribution of scorings obtainedfromarandomsampleof10video snippets scoredby the surgeonagroupof12anaesthetists. (C) PopulationBland–Altmananalysis of the scoringsfrom anaesthetists and surgeon. The continuous horizontal line is the bias; the dotted line the limits of agreement. The size of the dots representsthe number of (overlapping) data points, which range from 1 for the smallest dots (1, 0) and (1.5, 20.5), to 16 for the largest dot (4, 22).
BJA Martini et al.
504
95

the quality of surgical conditions from the video images andhence derive insufficient information from these imagesregarding the working conditions of the surgeon. It may beargued that in our study observing a 30 s video image doesnotprovidesufficient input toassess thequalityof surgical con-dition in non-surgically skilled personnel. This certainlymay betrue, but in our study, and possibly also in clinical practice, theanaesthetistsbase their impressionof thesurgicalfieldprimar-ilyon thevolumeof theworkingspaceand thevisibilityof retro-peritoneal tissues (most importantly related to the absence orpresence of blood in the image obscuring relevant structures)without addressing muscle contractions and other move-ments visible on the video image. In our hospital, live videoimagesof the laparoscopicfieldarepresentedto theanaesthe-tists during each case and these, together with his/her clinicalexperience and interactionwith the surgeon, form the basis oftheanaesthetic regimen, including theadditionaluseofneuro-muscular blocking agents when surgical conditions aredeemed poor. Some anaesthetists may not be willing toinduce a deep NMB. Thismay be related to their inability to ad-equately judge the operating field from the video screen butadditionally to their fear for suboptimal post-surgical condi-tions. Evidently, this may be the cause of some discussion inthe operating theatre. To prevent such situations, we suggestthat surgeons and anaesthetists communicate their wishesand intentions before the procedure (e.g. during preoperativetime-out) and closely cooperate in obtaining optimal workingconditions. Here, we show that providing a deepNMB improvessurgical conditions.
Authors’ contributionsC.M. was involved in the conception of the study idea anddesignof the study.Heperformedpartof theexperiments, par-ticipated in thedataanalysis, andwritingof thepaper.M.B.par-ticipated in the writing of the protocol, performed part of theexperiments, and participated in the writing of the paper.R.F.B. was involved in the design of the study and participatedin the development of the surgical rating scale, performed allsurgeries, and scored the quality of the surgical field at 15min intervals. L.P.A. was involved in the writing of the protocoland the interpretation of the results, and writing of the paper.A.D. was involved in the inception of the study idea, the designof the study, wrote the protocol, performed part of the experi-ments, analysed the data, interpreted the results, and wrotethe paper.
AcknowledgementWe thank the nurse anaesthetists, surgical nurses, and recov-ery room personnel of the Leiden University Medical Centerfor their help in performing the study.
Declaration of interestL.P.A. and A.D. received speaker fees from Merck BV, Oss, TheNetherlands.
FundingThis study is supported in part by Merck BV, Oss, The Nether-lands and by institutional funds from the Department of An-aesthesiology, Leiden University Medical Centre, Leiden, TheNetherlands. Merck was not involved in the design andconduct of the study, data analysis, and production of themanuscript. Merck’s statistician Hein Fennema did assist withthe sample size analysis.
References1 King M, Sujirattanawimol N, Danielson DR, et al. Requirements for
muscle relaxants during radical retropubic prostatectomy. Anes-thesiology 2000; 93: 1392–7
2 Murphy GS, Szokol JW, Marymont JH, et al. Residual neuromuscularblockade and critical respiratory events in the postanesthesia careunit. Anesth Analg 2008; 107: 130–7
3 Beccaria P, Cabrini L, Garancini MP, Colombo S. Recurarisation in asurgical ward. Anaesth Intensive Care 2008; 36: 917
4 Welliver M, McDonough J, Kalynych N, Redfern R. Discovery, devel-opment, and clinical application of sugammadex sodium, a select-ive relaxant binding agent. Drug Des Devel Ther 2009; 2: 49–59
5 Abrishami A, Ho J,Wong J, Yin L, Chung F. Sugammadex, a selectivereversal medication for preventing postoperative residual neuro-muscular blockade. Cochrane Database Syst Rev 2009; CD007632
6 Boon M, Martini M, Aarts LP, et al. Effect of variations in depth ofneuromuscular blockade on rating of surgical conditions bysurgeon and anesthesiologist in patients undergoing laparoscopicrenal or prostatic surgery (BLISS trial): study protocol for a rando-mized controlled trial. Trials 2013; 14: 63
7 Cohen J. A coefficient of agreement for nominal scales. EducPsychol Meas 1960; 20: 37–46
8 Weijenborg PTM, ter Kuile MM, Jansen FW. Intraobserver and inter-observer reliabilityof videotaped laparoscopyevaluations forendo-metriosis and adhesions. Fert Steril 2007; 87: 373–80
9 NiestersM,MahajanR, Olofsen E, et al.Validation of a novel respira-tory rate monitor based on exhaled humidity. Br J Anaesth 2012;109: 981–9
10 Viera AJ, Garrett JM. Understanding interobserver agreement: thekappa statistic. Fam Med 2005; 37: 360–3
11 Zaider TI, Heimberg RG, Fresco DM, Schneier FR, Liebowitz MR.Evaluationof theclinicalglobal impressionscaleamong individualswith social anxiety disorder. Psychol Med 2003; 33: 611–22
12 DahanA.Generalanesthesiaandcontrolof respiration.SemAnesth1996; 15: 328–34
13 Cantineau JP, Porte F, d’Honneur G, Duvaldestin P. Neuromusculareffects of rocuronium on the diaphragm and adductor pollicismuscles in anesthetized patients. Anesthesiology 1994; 81:585–90
14 Hemmerling TM, Donati F. Neuromuscular block at the larynx, thediaphragm and the corrugator supercilii muscle: a review. Can JAnaesth 2003; 50: 779–94
15 Danneels I, Mulier JP, Dillemans B, Vandebussche D. Effect ofmuscle relaxants on the abdominal pressure-volume relation. EurJ Anaesthesiol 2006; 23: 32
Handling editor: J. P. Thompson
Surgical conditions during laparoscopy BJA
505
96

Five-minute parameter of thromboelastometry is sufficient todetect thrombocytopenia and hypofibrinogenaemia inpatients undergoing liver transplantationJ.-G. Song, S.-M. Jeong, I.-G. Jun, H.-M. Lee and G.-S. Hwang*
Department of Anaesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea
* Corresponding author. E-mail: [email protected]
Editor’s key points
† Rapid diagnosis ofcoagulopathy is critical toappropriate treatment ofperioperative bleeding.
† Early parameters of clotformation measured byrotationalthromboelastometrywere studied in livertransplant patients.
† The clot amplitude at 5min correlated with lowplatelet counts and lowfibrinogen concentration,which might serve as arapid guide to transfusionin these patients.
Background. Early detection of coagulopathy is important to prevent bleeding during livertransplantation (LT). Rotation thromboelastometry (ROTEMw) provides the earliest parameter ofclot amplitudes at 5 min (A5). We evaluated whether A5 correlates with platelet count (PLT) andfibrinogen concentration (Fib) and can predict thrombocytopenia and hypofibrinogenaemia inhypocoagulable patients undergoing living-donor LT (LDLT).
Methods. A total of 3446 retrospective ROTEMw measurements, including 1139 EXTEM, 1182INTEM, and 1125 FIBTEM, with simultaneously measured PLT and Fib, were analysed duringLDLT in 239 patients. The correlations between A5 andmaximum clot firmness (MCF) index, PLT,and Fib were calculated. Receiver operating characteristic analysis with area under the curve(AUC) was used to assess A5 thresholds predictive of PLTand Fib.
Results. Themedian PLTwas 47 000mm23 and themedian Fibwas 100mgdl21 during LDLT. TheA5parametersofEXTEM(A5EXTEM)andINTEM(A5INTEM)werehighlycorrelatedwithMCF(r¼0.96andr¼0.95, respectively), PLT (r¼0.76 and r¼0.77, respectively), and Fib (r¼0.63 and r¼0.64,respectively). A5 of FIBTEM (A5FIBTEM) was also correlated with MCF (r¼0.91) and Fib(r¼0.75). A5EXTEM thresholds of 15 and 19 mm predicted PLT,30 000 mm23 (AUC¼0.90) and,50 000 mm23 (AUC¼0.87), respectively, whereas A5FIBTEM 4 mm predicted Fib,100 mg dl21
(AUC¼0.86). Biases fromA5EXTEM and A5FIBTEM to their MCFswere 16.4 and 1.3mm, respectively.
Conclusions.A5 as an early variable of clot firmness is effective in detecting critically low PLTandFib. A5 can therefore be a reliable fast index guiding transfusion therapy in hypocoagulablepatients undergoing LDLT.
Keywords: blood coagulation; liver transplantation; thromboelastometry
Accepted for publication: 2 July 2013
Patients who undergo liver transplantation (LT) often experi-ence massive bleeding requiring transfusion. The transfusion ofmanyallogeneic blood products, however,without a fast and re-liablemonitoring system, can furtheraggravate thehaemostaticdisordersof thesepatients, resulting inpooroveralloutcomes.1–4
Earlydetection and timely correctionof coagulopathyare crucialin preventing further exacerbation of bleeding diathesis and inbreaking the vicious cycle of coagulopathy during LT, in additionto improving overall patient outcomes.
Rotation thromboelastometry (ROTEMw delta, TEM Inter-national GmbH, Munich, Germany) is a point-of-care coagula-tion monitoring system that evaluates the viscoelasticity ofwhole blood, allowing the entire clotting process, from clot ini-tiation and formation to clot stability, to be assessed.5 6 Incontrast to conventional laboratory tests [e.g. measurementsof platelet count (PLT), prothrombin time (PT), activatedpartial thromboplastin time (aPTT), and fibrinogen concentra-tion (Fib)], ROTEMw can measure early variables, such as clot
amplitude at 5 min (A5) and 10 min (A10) after clotting time(CT) in EXTEM, INTEM, and FIBTEM. Owing to its rapid assess-ment of PLTand Fib, ROTEMw is frequently used to guide transfu-sion therapy.7–10 Moreover, a recent studywith a large databasedemonstrated that earlymeasures of clot firmness, includingA5,A10, and clot amplitude at 15 min (A15), are linearly correlatedwithROTEMwdeterminedmaximumclotfirmness(MCF),allowingthe fast and reliable prediction ofMCF in non-cardiac patients, in-cluding those with subnormal, normal, and supranormal MCFvalues.11
The A10 of EXTEM (A10EXTEM) was shown to be rapid andvaluable in predicting coagulation status, and also being usefulin assessing the need for perioperative transfusion of plateletsand fibringen.8 The correlations of the more rapid A5 with PLTcount and Fib concentration have not been determined, and itremains unclear whether A5 could determine quantitative PLTandFib level inhypocoagulablepatientsundergoing living-donorLT (LDLT) surgery.We thereforeassessedwhetherA5onROTEMw
British Journal of Anaesthesia 112 (2): 290–7 (2014)Advance Access publication 24 September 2013 . doi:10.1093/bja/aet325
& The Author [2013]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
97

analysis is an early and reliable index for the transfusion of PLTand Fib during LDLT.We also assessed A5 cut-off values predict-ing thrombocytopenia and hypofibrinogenaemia in patientsundergoing LDLT.
MethodsPatients
A total of 401 patients who underwent LT at Asan MedicalCenter, Seoul, Republic of Korea, between June 2010 and May2011 were enrolled. Of these, 162 patients were excludedfrom this analysis, including 73 who received orthotopic LT,53 who had incomplete ROTEMw and laboratory test data, and36 patients aged ,18 yr. The remaining 239 LDLT recipientswere included in this retrospective analysis. Records about an-aesthesia, available on computerizeddatabases,were analysedretrospectively. This studyprotocolwas approvedby the Institu-tional Review Board of the Asan Medical Center.
Anaesthetic technique
Generalanaesthesia for LDLTsurgerywasperformedaccordingtoour institutional standardprotocol.12 Briefly, anaesthesiawasinduced with i.v. thiopental, fentanyl, and vecuronium, andmaintainedwith1%sevoflurane,a50%O2/airmixture,andcon-tinuous infusion with fentanyl and vecuronium. Twenty-gaugefemoral and radial arterial catheters were inserted to monitorarterial pressure and to sample blood. A 7.5 French pulmonaryartery catheter (Swan–Ganz CCOmbo V CCO/SvO2/CEDV,Edwards Lifesciences LLC, CA, USA) was inserted to monitorhaemodynamic variables. Body temperature was measuredusing a thermistor in a pulmonary artery catheter. Transfusionsof packed red blood cells, fresh-frozen plasma, and cryoprecipi-tate were based on clinical decisions or guided by standard la-boratory tests or the transfusion algorithm based on ROTEMparameters. According to institutional standards, transfusionswere administered to maintain PT,2.0 INR, Fib.100 mg dl21,and PLT.30 000 mm23. Synthetic colloidal solution was notused, but solutions of 5% albumin with balanced crystalloidwere administered during LDLT.
Blood sampling and thromboelastomery
During LDLT, standard coagulation assays and ROTEMw testswereroutinelyperformed,usingbloodsamplesatpre-establishedtime points, including 1 h after induction of general anaesthe-sia, 1 h after surgical incision, 30 min after hepatectomy, and30min after graft reperfusion and after hepatic artery anasto-mosis. ROTEMw tests were performed according to the manu-facturer’s instructions, using equipment and test reagentsprovided by Tem International GmbH. The ROTEMw devicewas placed in the operating theatre and all tests were per-formed by transplantation anaesthesiologists or anaesthesianurses trained to perform ROTEMw tests. Of the ROTEMw testsperformed, inadequate runtime, patientswho received throm-bin inhibitor or signs of hyperfibrinolysiswere excluded. Finally,1139 EXTEM, 1182 INTEM, and 1125 FIBTEM tests wereincluded in the study. ROTEMw variables recorded included: (i)clotting time (CT), defined as the time (s) from the start of
measurement to the initiation of clotting, defined as a clotfirmness of 2 mm; (ii) clot formation time (CFT), defined asthe time (s) from initiation of clotting until a clot firmness of20 mm; (iii) MCF, defined as the maximal amplitude (mm) ofthe graphical trace of clot firmness; (iv) a-angle (a), definedas the tangent to the graphic trace at an amplitude of 2 mm;and A5 and A10 (mm), which reflect the amplitudes 5 and 10min, respectively, after CT. At each time point, blood sampleswere withdrawn from the radial artery, and haemoglobin, PT,PLT, and Fib were measured.
Standard coagulation assays
PT was assessed using Thromborel S kits (Siemens HealthcareDiagnostics, GmbH, Marburg, Germany), and fibrinogen wasassayed using the Dade Thrombin Reagent (Siemens Health-careDiagnostics). All testswere performedusing anautomaticcoagulation analyser (Sysmex CA-7000, Siemens HealthcareDiagnostics).
Statistical analyses
Continuous variableswereexpressedasmedian (inter-quartilerange) ormean [standarddeviation (SD)]. Between-group com-parisons were evaluated using the x2 test, Fisher’s exact tests,t-tests, and Mann–Whitney U-tests, as appropriate. Correla-tions between standard coagulation test results and those per-formed on ROTEMw were analysed using Spearman’s rankcorrelation coefficient (r). The Bland–Altman analyses13 wereperformed to estimate the mean difference (bias) (SD) betweenearly measures of clot firmness (A5 and A10) and MCF. Receiveroperating characteristic (ROC) curves and the area under the
Table 1 Patient characteristics and laboratory data. Values areexpressed as median (inter-quartile range) or percentage, asappropriate
Variable
Preoperative patient characteristic data
Age (yr) 53 (48–57)
Gender, male (%) 76.0
Body mass index (kg m22) 23.8 (21.7–25.9)
Model for end-stage liver disease score 14 (10–21)
Child–Pugh score 8 (6–10)
Liver disease (%)
Hepatitis B virus-related cirrhosis 67.7
Hepatitis C virus-related cirrhosis 7.0
Alcoholic cirrhosis 12.7
Autoimmune 1.4
Others 11.2
Diabetes (%) 27.9
Hypertension (%) 2.2
Intraoperative laboratory data
Haemoglobin (g dl21) 9.5 (8.6–10.7)
Platelets (×103 mm23) 47 (32–64)
Prothrombin time (INR) 1.8 (1.6–2.2)
Fibrinogen (mg dl21) 100 (77–137)
Early detection of coagulopathy using ROTEM BJA
291
98

curve (AUC) was used to determine the optimal cut-off valuesof A5, A10, and MCF on EXTEM, INTEM, and FIBTEM predictingPLT counts ,30 000 and ,50 000 mm23 and Fib concentra-tions,100mgdl21. Sensitivityand specificitywere also calcu-lated. All statistical analyses were performed using Medcalcw
(Medcalc Software, Mariakerke, Belgium) statistical software.A two-tailed P-value of ,0.05 was considered statisticallysignificant.
ResultsThe patient characteristics, intraoperative laboratory data,and liver transplant results of the 239 included patients areshown in Table 1. During LDLT, the median (inter-quartilerange) PLT was 47 000 (32 000–64 000) mm23, the medianFib was 100 mg dl21 (772137 mg dl21), and the median PTwas 1.8 (1.6–2.2) INR, demonstrating that these patients
0
80
60
40
20
0
80
60
40
20
25
20
15
10
5
0
25
20
15
10
5
00 5 10 15 20 25 30 0 5 10 15 20 25 30
0
80
60
40
20
0
80
60
40
20
0 10 20 30 40 50 50 70 80 0 10 20 30 40 50 50 70 80
0 10 20 30 40 50 50 70 800 10 20 30 40 50 50 70 80
r=0.961
r=0.975 r=0.965
r=0.951r=0.907
r=0.950
EX
TE
M A
5 (m
m)
EXTEM MCF (mm)
EXTEM MCF (mm)
INTEM MCF (mm)
INTEM MCF (mm)
INT
EM
A5
(mm
)
EX
TE
M A
10 (
mm
)F
IBT
EM
A5
(mm
)
FIBTEM MCF (mm) FIBTEM MCF (mm)
FIB
TE
M A
10 (
mm
)IN
TE
M A
10 (
mm
)
Fig 1 Correlations between early ROTEM parameters and MCF. Early ROTEM parameters (A5 and A10) on all ROTEM assays (EXTEM, INTEM, andFIBTEM) demonstrated excellent correlations with MCF.
BJA Song et al.
292
99

were in a hypocoagulable state. We found that 1026 analyses(90.1%) of MCFEXTEM and 1069 (90.4%) of MCFINTEM presentedvalues below the reference range (,50 mm each), whereas inFIBTEM analysis, 823 assays (73.2%) of MCFFIBTEM were belowthe reference range (MCFFIBTEM,9 mm). Correlation analysesbetween ROTEMw parameters (A5, A10, and MCF of EXTEM,INTEM, and FIBTEM) are shown in Figure 1. Among the ROTEMw
parameters, both A5EXTEM (r¼0.961, P,0.0001) and A10EXTEM(r¼0.975, P,0.0001) were highly correlated with MCFEXTEM, andalso with MCFINTEM (r¼0.950 and r¼0.965, respectively;P,0.0001 each). In addition, A5FIBTEM (r¼0.907, P,0.0001) andA10FIBTEM (r¼0.951, P,0.0001) showed high correlation withMCFFIBTEM.
Intraoperative ROTEMwdata andbiases calculated from theBland–Altman analyses of A5 and A10 for EXTEM, INTEM, andFIBTEMparameters are shown in Table 2. Intraoperative trendsof ROTEMw data and laboratory parameters are shown inFigure2. Because thescatterplot seemedto followacurvilinearrelationship betweenROTEMwdataand conventional coagula-tion parameters, we performed both linear and curvilinearfitting (Fig. 3). The curvilinear fits showed better correlationsfor all comparisons. A5EXTEM, A10EXTEM, and MCFEXTEM showedbetter correlations with PLT (r¼0.76, r¼0.76, and r¼0.75, re-spectively, P,0.001 each) than with Fib (r¼0.63, r¼0.65, andr¼0.63, respectively, P,0.0001 each), indicating that MCFparameters areexplainedbetter byPLT thanbyFib. In addition,A5INTEM, A10INTEM, and MCFINTEM showed good correlationswith PLT (r¼0.77, r¼0.77, and r¼0.75, respectively, P,0.001each) and Fib (r¼0.64, r¼0.66, and r¼0.62, respectively,P,0.0001 each), and A5FIBTEM, A10FIBTEM, and MCFFIBTEM werecorrelated with Fib (r¼0.75, r¼0.76, and r¼0.75, respectively,P,0.0001 each) (Fig. 3).
ROCcurveanalysis showedthat thecut-off valuesofA5EXTEMand A10EXTEM predicting PLT,30 000mm23 were 15mm (sen-sitivity: 86%, specificity: 77%) and 22 mm (sensitivity: 85%,specificity: 78%), respectively, and that their cut-off values topredict PLT,50 000 mm23 were 19 mm (sensitivity: 82%,
specificity: 78%) and 27 mm (sensitivity: 82%, specificity: 77%),respectively. AUCs of A5EXTEM and A10EXTEM were 0.90 and0.898, respectively, for PLT,30 000 mm23 and were 0.871 and0.867, respectively, for PLT,50 000mm23 (allP,0.0001) (Fig. 4).
The cut-off values of A5INTEM and A10INTEM were 16 mm(sensitivity: 82%, specificity: 86%) and 22 mm (sensitivity: 85%,specificity: 83%), respectively, for predicting PLT,30 000 mm23,and 19 mm (sensitivity: 82%, specificity: 77%) and 27 mm(sensitivity: 79%, specificity: 79%), respectively, for predictingPLT,50 000 mm23. AUCs of A5INTEM and A10INTEM were 0.914and 0.915, respectively, for PLT,30 000 mm23 and were 0.873and 0.869, respectively, for PLT,50 000 mm23 (all P,0.0001)(Fig. 4).
ROC curve analysis showed that A5FIBTEM and A10FIBTEMpredicting Fib,100 mg dl21 were 4 mm (sensitivity: 81%,specificity: 77%) and 5 mm (sensitivity: 76%, specificity:82%), respectively. The AUCs of A5FIBTEM and A10FIBTEM forFib,100 mg dl21 were 0.86 and 0.87, respectively (allP,0.0001) (Fig. 4).
DiscussionThefirstmajor findingof our studywas thatall correlationsandROC curve analyses, including AUCs, were very similar forA5EXTEM and A10EXTEM and for A5INTEM and A10INTEM, stronglysuggesting that A5 is as precise as A10, but can more rapidlypredict MCF, thrombocytopenia, and hypofibrinogenaemiain patients undergoing LDLT. Secondly, A5EXTEM and A5INTEMwere similar in predicting MCF, with both showing goodcorrelations with PLTand Fib, suggesting that they can be usedinterchangeably, despite INTEM and EXTEM reflecting differentcoagulation pathways. Thirdly, FIBTEM analysis showed thatthe difference (bias) between A5FIBTEM and MCFFIBTEM was small,only 1.3 mm in patients with hypofibrinogenaemia (medianFib¼100 mg dl21). In addition, the ROC curves of A5FIBTEM andA10FIBTEM for Fib,100 mg dl21 yielded almost identicalAUCs, indicating that A5FIBTEM was as useful as A10FIBTEM inconsistently predicting hypofibrinogenaemia. Lastly, althoughreplacement guidelines for thrombocytopenia and hypofibri-nogenaemia during LT surgery vary widely among institutions,the critical PLT triggering transfusion is generally thought torange from30 000 to50 000mm23.14 15Wethereforeanalysedthe correlations between A5 parameters on ROTEMw analysisand the commonly used quantitative cut-off values forPLT,30 000 mm23 and ,50 000 mm23 and Fib,100 mg dl21
during LT.8 15
Because conventional laboratory tests have long turn-around times in clinical settings, determining when to start atransfusion and the amounts of allogeneic blood productstransfused into patients with massive bleeding is difficult.Therefore, early variables assessed by point-of-care ROTEMdevice, which are available within 10–20 min, have beenincreasingly used to trigger transfusion of platelets andfibrinogen-rich products. Trigger values were based on evi-dence that these variables could successfully determinethrombocytopenia and hypofibrinogenaemia in patientsundergoing LT and cardiac surgery and those with severe
Table 2 Intraoperative ROTEMw data and bias for A5 and A10 onthe Bland–Altman analyses. Data were expressed as median(inter-quartile range) or mean (SD). NA, not available. A5, clotamplitude at 5min; A10, clot amplitude at 10min; MCF, maximumclot firmness
Variables EXTEM INTEM FIBTEM
Clot time (s) 71 (52–103) 229 (197–278) 59 (46–95)
Clot formationtime (s)
235 (173–307) 231 (164–309) NA
a-Angle (8) 49 (39–58) 52 (42–61) NA
A5 (mm) 19 (15–25) 20 (15–25) 5 (3–7)
A10 (mm) 27 (22–34) 27 (22–33) 5 (4–8)
MCF (mm) 37 (31–43) 37 (31–43) 6 (4–9)
Bias for A5(mm)
16.4 (3.7) 16.2 (3.6) 1.3 (1.4)
Bias for A10(mm)
8.8 (2.7) 8.8 (2.8) 0.7 (1.0)
Early detection of coagulopathy using ROTEM BJA
293
100

trauma.8 11 16–18 In traumapatients, anA10FIBTEMof 5mmwasthe threshold that best predicted hypofibrinogenaemia (,100mg dl21), whereas an A15INTEM of 46 mm best predictedthrombocytopenia (,50 000 mm23).18 During LT surgery, ourresults demonstrated that both A10EXTEM and A10INTEM of27mmwere the thresholds best predicting thrombocytopenia(,50 000 mm23), whereas an A10FIBTEM of 5 mm best pre-dicted hypofibrinogenaemia (,100 mg dl21). These findingsare in agreement with previous studies showing that anA10FIBTEM of 5 mmwas optimal in trauma patients18 and thatan A10EXTEM of 29 mm was the optimal cut-off for thrombo-cytopenia (,50 000 mm23) during LT.8
Notably, this study was the first to show that A5 is a reliableearly parameter that can substitute for both A10 and MCF inpatients in a hypocoagulable state observed during LDLT(median MCFEXTEM¼37 mm and median MCFFIBTEM¼6 mm).Among the ROTEMw parameters, the A5 and A10 indices of
both EXTEM and INTEM showed excellent correlations withtheir MCF values, and A5FIBTEM and A10FIBTEM were highly corre-lated with MCFFIBTEM. These results are comparable with theexcellent correlations observed for A5 and A10 with their MCFsin a heterogeneous study population that included individualswith subnormal, normal, and supranormal MCF values.11 Ourfindings also demonstrated that the correlation coefficients ofA5EXTEM and A10EXTEM with PLT, A5INTEM and A10INTEM with PLT,andA5FIBTEMandA10FIBTEMwithFibwerealmost identical. There-fore, these results strongly indicate that A5 is as accurateasA10,allowing earlier parameters to guide PLT transfusion during LT.8
We observed biases between early variables (A5 and A10)and MCF of ROTEMw analyses. Because the median values ofMCFEXTEM, MCFINTEM, and MCFFIBTEM were 37, 37, and 6 mm, re-spectively, our data characterize patientswith subnormalMCF.In EXTEM and INTEM assays, the biases between A5 and A10and MCF were 16 and 9 mm, respectively. Therefore, to
14
12
10
8
650
40
30
20
10
060
50
40
30
20
10
0
60
70
50
40
30
20
10
0T0 T0 T1 T2 T3 T4 T0 T1 T2 T3 T4T1 T2 T3 T4
200 300
250
200
150
100
50
0
14
12
10
8
6
4
2
020
15
10
5
25
20
15
10
5
0
–5
0
150
100
50
0
50
40
30
20
10
060
50
40
30
20
10
070
60
50
40
30
20
10
0
Hae
mog
lobi
n (g
dl–
1 )
Pla
tele
t (10
3 ×m
m–3
)IN
TE
M A
5 (m
m)
INT
EM
A10
(m
m)
INT
EM
MC
F (
mm
)
FIB
TE
M M
CF
(m
m)
FIB
TE
M A
10 (
mm
)F
IBT
EM
A5
(mm
)F
ibrin
ogen
(m
g dl
–1)
EX
TE
M A
5 (m
m)
EX
TE
M A
10 (
mm
)E
XT
EM
MC
F (
mm
)
Fig 2 Intraoperative trends of ROTEMand laboratory parameters. Data aremedian (SD). T0, 1 h after induction of general anaesthesia; T1, 1 h aftersurgical incision; T2, 30 min after hepatectomy; T3, 30 min after graft reperfusion; T4, after hepatic artery anastomosis.
BJA Song et al.
294
101

80 60 40 20 80 60 40 20 80 70 60 50 40 30 20 10 00
5000
010
000
015
000
020
000
000
5000
010
000
015
000
020
000
00
0
80 60 40 20 0
80 60 40 20 00
100
200
300
400
500
010
020
030
040
050
0
0
-20
80 60 40 20 0
80 70 60 50 40 30 20 10 0
80 60 40 20 0
8030 25 20 15 10 5 0 35 30 25 20 15 10 5 0 0
100
200
300
400
500
60 40 20 0
80 60 40 20 0
80 60 40 20
0
8025 20 15 10
5 0
60 40 20 0
EXTEM A5 (mm)
INTEM A5 (mm) INTEM A10 (mm)
INTEM A10 (mm) INTEM MCF (mm)
FIBTEM MCF(mm)FIBTEM A10 (mm)FIBTEM A5 (mm)
INTEM A5 (mm)
INTEMMCF (mm)
EXTEM MCF (mm)
EXTEM A10 (mm)
EXTEM A10 (mm)EXTEM A5 (mm)
EXTEM MCF (mm)
r=0.
764
r=0.
757
r=0.
766
r=0.
648
r=0.
659
r=0.
761
r=0.
769
r=0.
629
r=0.
638
r=0.
750
R2 =
0.49
R2 =
0.49
R2 =
0.67
R2 =
0.66
R2 =
0.65
R2 =
0.64
R2 =
0.65
R2 =
0.49
R2 =
0.49
R2 =
0.69
Y=
7.6+
0.00
03X
–3.7
E–1
0 X2
r=0.
752
r=0.
750
r=0.
628
r=0.
615
r=0.
745
R2 =
0.62
R2 =
0.62
R2 =
0.45
R2 =
0.42
R2 =
0.72
Y=
17.9
+0.
0005
X–1
.3E
–10X
2Y
=11
8+0.
0004
X–1
.3E
–9X
2Y
=17
.5+
0.2X
–0.0
003X
2Y
=18
.4+
0.2X
–0.0
003X
2Y
=1.
5+0.
04X
+6.
6E–5
X2
Y=
11.2
+0.
0004
X–8
E–1
0X2
Y=
10.2
+0.
2X–0
.000
2X2
Y=
10+
0.2 X
–0.0
002 X
2Y
=0.
5+0.
05X
+1.
5E–5
X2
Y=
7.2+
0.00
03X
–4.8
E–1
0X2
Y=
6.4+
0.14
X–0
.000
1 X2
Y=
6.1+
0.15
X–0
.000
1X2
Y=
0.5+
0.04
X+
1.3E
–5X
2
Y=
11.5
+0.
0004
X–8
E–1
0X2
PLT
(m
m–3
)P
LT (
mm
–3)
Fib
rinog
en (
mg
dl–1
)F
ibrin
ogen
(m
g dl
–1)
Fib
rinog
en (
mg
dl–1
)
Fig3
Linea
r(r)an
dcu
rvilinea
r(R2)relationsh
ipbe
twee
nROTE
Mpa
rametersan
dco
nve
ntion
alco
agulation
tests.Notethat
A5,A10
,andMCFon
both
EXTE
Man
dIN
TEMsh
owed
good
correlations
withPLTs
andmod
erateco
rrelationswithfib
rinog
enco
nce
ntration.A
5,A10
,andMCFof
FIBTE
Malso
show
edgo
odco
rrelationswithfib
rinog
enco
nce
ntration.
Early detection of coagulopathy using ROTEM BJA
295
102

determine the approximate value of their MCFs, 16mmshouldbeadded to theA5valueand 9mmto theA10value inpatientsundergoingLT.Aprevious study, however, reported that19mmshould be added to A5 and 10mm to A10 (11mm for patientswith MCFEXTEM,50 mm) to obtain rough estimates of theirMCFs.11 These discrepancies were more pronounced in FIBTEMassays, in that 4.5 mm was added to A5 and 3.4 mm toA10 mm (1.95 mm in patients with MCFFIBTEM,9 mm)to obtain rough estimates of MCFFIBTEM.
11 In contrast, wefound that only �1 mm (1.3 and 0.7 mm, respectively) had tobe added to the A5 and A10 values of MCFFIBTEM in patients
undergoingLT. Thereare several possible reasons for thediffer-ences between our study and previous studies.11 19 First, thecharacteristics of the patient populations in the previousstudy included all non-cardiac patients, regardless of MCFvalues. A comparison of study populations showed that 73%and 90% in our study were below the reference ranges on theFIBTEM (MCFFIBTEM,9 mm) and EXTEM (MCFEXTEM,50 mm)assays, compared with 14.3% and 49.1%, respectively, in theearlier study.11 Secondly, preexisting differences inconventional laboratory parameters between studies mighthave an effect on ROTEMw analyses. Tripodi and colleagues19
100 60(mm)
50403020100
Sen
sitiv
ity 806040200
0 40 80
A5EXTEM
A10EXTEMA10EXTEM A10EXTEM
A10EXTEM
A5INTEM
A10INTEM A10INTEM A10INTEM A10INTEM
A5INTEM A5INTEMA5INTEM
A5EXTEM A5EXTEM A5EXTEM60
(mm)
50403020100
60(mm)
(mm)
50403020100
6070
50403020100
100
Sen
sitiv
ity 806040200
0 40 80
100
Sen
sitiv
ity
806040200
0 40 80
100
Sen
sitiv
ity 806040200
0 40 80
A5FIBTEM A5FIBTEM A10FIBTEM A10FIBTEM
AUC=0.915
AUC=0.866
AUC=0.898
AUC=0.914
AUC=0.857
100
Sen
sitiv
ity 806040200
0 40 80
100
Sen
sitiv
ity 806040200
0 40 80
AUC=0.9
100
Sen
sitiv
ity 806040200
0 40 80
AUC=0.871
100
Sen
sitiv
ity806040200
0 40 80
AUC=0.867
100806040200
0 40 80
AUC=0.869
100
Sen
sitiv
ity
80604020
00 40 80
AUC=0.873
>15Sens:86.3Spec:76.5
60(mm)
(mm)
(mm)
(mm) (mm)
(mg dl–1)(mg dl–1)
(%) (%)
50403020100
>16Sens:82.0Spec:86.0
>22Sens:84.8Spec:77.9
>22Sens:85.4Spec:82.6
>27Sens:88.9Spec:79.3
>27Sens:82.1Spec:76.7
>19Sens:82.3Spec:77.3
>19Sens:82.1Spec:77.5
>5Sens:76.2Spec:82.0
>4Sens:81.3Spec:76.5
PLT<30x103 PLT>30x103(mm–3) PLT<50x103 PLT>50x103(mm–3)
70
60
40
20
20 2520
15
10
5
0
15
10
5
0Fib<100 FIB>100 Fib<100 FIB>100
0
(mm)
60
40
20
0100-Specificity 100-Specificity
100-Specificity
6050403020100
Fig 4 ROC curves of A5 andA10 on EXTEM, INTEM, and FIBTEMpredicting thrombocytopenia and hypofibrinogenaemia. AUCvalues of A5 andA10on both EXTEM and INTEM were good predictors of PLTs ,30×103 and ,50×103 mm23. AUC values of A5, A10, and MCF on FIBTEM were goodpredictors of fibrinogen ,100 mg dl21.
BJA Song et al.
296
103

demonstrated that PLT was the most important determinant inMCF in patients with stable cirrhosis, in which the study popula-tionshowedlowPLTwithnearlynormalFib. Incontrast,ourstudypopulation showed both low PLT [47 000 (32 000–64 000) vs65 000 (24 000–178 000) mm23] and Fib [100 (772137) vs199 (108–423) mg dl21], respectively, compared with thatstudy.19 Thirdly, differences in the use of colloids might haveaneffecton theobservedbias,particularly for FIBTEM.Synthet-ic colloids such as hydroxyethyl starch solutions are known tohavean impact onfibrinpolymerization, resulting indecreasedMCF.20 21 However, asweused onlyalbumin for colloid solutionduring LDLT, our data would not be affected by synthetic col-loids in the bias between early variables of clot firmness (A5and A10) and MCF. This difference might result in increasedbias between A5 (A10) and MCF, in particular in FIBTEM,between our study and the earlier study.11 Taken together,because of the potentials for selection and observationbiases among different studies (e.g. differences in gender, eth-nicity, clinical conditions, types of fluid replacement, etc.), careshould be taken when interpreting the results of bias betweenearly variables (A5 and A10) and MCF of ROTEMw analyses.
Our studyhad several limitations. First, itwasa retrospective,single-centre study, suggesting caution in interpreting ourresults as there might have been observation bias and bias inpatient selection. Secondly, we did not assess the predictabilityof transfusionrequirementsbasedonROTEMwanalysisor stand-ard coagulation tests. Further studies are needed to evaluatewhether threshold levels of ROTEMw parameters can estimateclinical bleedingandguide transfusion therapy to improve treat-ment of haemostatic derangements associated with LDLT.
In conclusion, our findings indicate that A5 as an early vari-able of clot firmness in thromboelastometry is effective todetect thrombocytopenia and hypofibrinogenaemia in hypo-coagulable patients undergoing LT. A5 on ROTEMw analysismight be the earliest, most reliable index in selecting transfu-sion guidelines based on PLTand Fib during LDLT.
Authors’ contributionsJ.-G.S.: study design, study data analysis, manuscript prepar-ation, and revision; S.-M.J.: study design and data analysis;I.-G.J.: data collection and analysis; H.-M.L.: data analysis;G.-S.H.: study design, study conduct, data analysis, manuscriptpreparation, and revision.
Declaration of interestNone declared.
FundingNo financial support was received from any funding agency.
References1 de Boer MT, Christensen MC, Asmussen M, et al. The impact of
intraoperative transfusion of platelets and red blood cells on sur-vival after liver transplantation. Anesth Analg 2008; 106: 32–44
2 Nacoti M, Cazzaniga S, Lorusso F, et al. The impact of perioperativetransfusion of blood products on survival after pediatric liver trans-plantation. Pediatr Transplant 2012; 16: 357–66
3 Benson AB, Burton JR Jr, Austin GL, et al. Differential effects ofplasma and red blood cell transfusions on acute lung injury and in-fection risk following liver transplantation. Liver Transpl 2011; 17:149–58
4 Massicotte L, Sassine MP, Lenis S, Seal RF, Roy A. Survival ratechangeswith transfusion of blood products during liver transplant-ation. Can J Anaesth 2005; 52: 148–55
5 McCluskeySA, Karkouti K,WijeysunderaDN,etal.Derivationof a riskindex for the prediction of massive blood transfusion in liver trans-plantation. Liver Transpl 2006; 12: 1584–93
6 Ganter MT, Hofer CK. Coagulation monitoring: current techniquesand clinical use of viscoelastic point-of-care coagulation devices.Anesth Analg 2008; 106: 1366–75
7 Ebinger T, Ruland A, Lakner M, Schwaiger M. Validity, regulatoryregistration and approval of ROTEM thromboelastometry. BloodCoagul Fibrinolysis 2010; 21: 106–7
8 Roullet S, Pillot J, Freyburger G, et al. Rotation thromboelastometrydetects thrombocytopeniaandhypofibrinogenaemiaduringortho-topic liver transplantation. Br J Anaesth 2010; 104: 422–8
9 Davenport R, Manson J, De’Ath H, et al. Functional definition andcharacterization of acute traumatic coagulopathy. Crit Care Med2011; 39: 2652–8
10 Schochl H, Cotton B, Inaba K, et al. FIBTEMprovides early predictionof massive transfusion in trauma. Crit Care 2011; 15: R265
11 Gorlinger K, Dirkmann D, Solomon C, Hanke AA. Fast interpretationof thromboelastometry in non-cardiac surgery: reliability inpatients with hypo-, normo-, and hypercoagulability. Br J Anaesth2013; 110: 222–30
12 Kim YK, Shin WJ, Song JG, et al. Comparison of stroke volumevariations derived from radial and femoral arterial pressure wave-forms during liver transplantation. Transplant Proc 2009; 41:4220–8
13 Bland JM, Altman DG. Statisticalmethods for assessing agreementbetween two methods of clinical measurement. Lancet 1986; 1:307–10
14 Slichter SJ. Evidence-based platelet transfusion guidelines. Hema-tology Am Soc Hematol Educ Program 2007: 172–8
15 Kang Y, Audu P. Coagulation and liver transplantation. Int Anesthe-siol Clin 2006; 44: 17–36
16 Blasi A, Beltran J, Pereira A, et al.An assessment of thromboelasto-metry tomonitor blood coagulation and guide transfusion supportin liver transplantation. Transfusion 2012; 52: 1989–98
17 Dirkmann D, Gorlinger K, Dusse F, Kottenberg E, Peters J. Earlythromboelastometric variables reliablypredictmaximumclotfirm-ness in patients undergoing cardiac surgery: a step towards earlierdecision making. Acta Anaesthesiol Scand 2013; 57: 594–603
18 Rugeri L, Levrat A, David JS, et al.Diagnosis of early coagulation ab-normalities in trauma patients by rotation thrombelastography.J Thromb Haemost 2007; 5: 289–95
19 TripodiA, PrimignaniM, ChantarangkulV,et al.Thecoagulopathyofcirrhosis assessed by thromboelastometry and its correlation withconventional coagulation parameters. Thromb Res 2009; 124:132–6
20 Winstedt D, Hanna J, Schott U. Albumin-induced coagulopathy isless severe and more effectively reversed with fibrinogen concen-trate than is synthetic colloid-induced coagulopathy. Scand J ClinLab Invest 2013; 73: 161–9
21 SchramkoA, Suojaranta-Ylinen R, KuitunenA, Raivio P, Kukkonen S,Niemi T. Hydroxyethylstarch and gelatin solutions impair blood co-agulation after cardiac surgery: a prospective randomized trial. Br JAnaesth 2010; 104: 691–7
Handling editor: H. C. Hemmings
Early detection of coagulopathy using ROTEM BJA
297
104

International Journal of AnaesthesiaVolume 112 Number 2 February 2014
IN THIS ISSUE
In the February BJA. . . viii
EDITORIALS
Peripheral endothelial dysfunction after subarachnoid haemorrhage: what the fingertips can tell usN. Scherbakov and W. Doehner 205
b-Blockers and cardiac protection: 5 yr on from POISEP. Foex and J. W. Sear 206
Perioperative immunity: is there an anaesthetic hangover?R. D. Sanders 210
EDITORIAL SERIES ON METHODOLOGY 5
Radioimmunoassay, enzyme and non-enzyme-based immunoassaysR. D. Grange, J. P. Thompson and D. G. Lambert 213
REVIEW ARTICLES
Impact of anaesthetic drugs and adjuvants on ECG markers of torsadogenicityC. Staikou, M. Stamelos and E. Stavroulakis 217
Simulation-based training in anaesthesiology: a systematic review and meta-analysisG. R. Lorello, D. A. Cook, R. L. Johnson and R. Brydges 231
Perioperative management of severe anorexia nervosaK. Hirose, M. Hirose, K. Tanaka, S. Kawahito, T. Tamaki and S. Oshita 246
CARDIOVASCULAR
Comparison of the effects of albumin 5%, hydroxyethyl starch 130/0.4 6%, and Ringer’s lactate on blood lossand coagulation after cardiac surgeryK. Skhirtladze, E. M. Base, A. Lassnigg, A. Kaider, S. Linke, M. Dworschak and M. J. Hiesmayr 255
Topographic analysis and evaluation of anatomical landmarks for placement of central venous cathetersbased on conventional chest X-ray and computed tomographyM. Dulce, I. G. Steffen, A. Preuss, D. M. Renz, B. Hamm and T. Elgeti 265
CLINICAL PRACTICE
Comparison of the effects of xenon and sevoflurane anaesthesia on leucocyte function in surgical patients: arandomized trialA. V. Fahlenkamp, M. Coburn, R. Rossaint, C. Stoppe and H. Haase 272
Crystalloid or colloid for goal-directed fluid therapy in colorectal surgeryD. R. A. Yates, S. J. Davies, H. E. Milner and R. J. T. Wilson 281
Five-minute parameter of thromboelastometry is sufficient to detect thrombocytopenia andhypofibrinogenaemia in patients undergoing liver transplantationJ.-G. Song, S.-M. Jeong, I.-G. Jun, H.-M. Lee and G.-S. Hwang 290
CRITICAL CARE
Liver function test abnormalities after traumatic brain injury: is hepato-biliary ultrasound a sensitivediagnostic tool?F. Sanfilippo, T. Veenith, C. Santonocito, C. S. Vrettou and B. F. Matta 298
Vecuronium pharmacokinetics in patients with major burnsK. R. Vega-Villa, K. Kaneda, S. Yamashita, S. Woo and T. H. Han 304
105

NEUROSCIENCES AND NEUROANAESTHESIA
Impaired endothelial function after aneurysmal subarachnoid haemorrhage correlates witharginine:asymmetric dimethylarginine ratioA. Bergstrom, J. M. Staalsø, B. Romner and N. V. Olsen 311
PAEDIATRICS
Augmentation of thrombin generation in neonates undergoing cardiopulmonary bypassN. A. Guzzetta, F. Szlam, A. S. Kiser, J. D. Fernandez, A. D. Szlam, T. Leong and K. A. Tanaka 319
PAIN
Postoperative pain after abdominal hysterectomy: a randomized, double-blind, controlled trial comparingcontinuous infusion vs patient-controlled intraperitoneal injection of local anaestheticA. Perniola, F. Fant, A. Magnuson, K. Axelsson and A. Gupta 328
Capsaicin 8% patch for treprostinil subcutaneous infusion site pain in pulmonary hypertension patientsV. Libri, J. S. R. Gibbs, D. J. Pinato, T. Iddamalgoda, R. H. Khengar, W. Gin-Sing, L. Huson and P. Anand 337
RESPIRATION AND THE AIRWAY
Tracheal intubation in patients with odentogenous abscesses and reduced mouth openingM. Schumann, I. Biesler, A. Borgers, R. Pfortner, C. Mohr and H. Groeben 348
Flow dynamics using high-frequency jet ventilation in a model of bronchopleural fistulaM. J. Wood, E. S. Lin and J. P. Thompson 355
TRANSLATIONAL RESEARCH
Voltage changes in the lithium dilution cardiac output sensor after exposure to blood from horses givenxylazineT. D. Ambrisko and Y. Moens 367
Time-dependent modulation of muscarinic m1/m3 receptor signalling by local anaestheticsS. Picardi, M. F. Stevens, K. Hahnenkamp, M. E. Durieux, P. Lirk and M. W. Hollmann 370
CORRESPONDENCE
Correspondence 380
BOOK REVIEWS
Book Reviews 395
RETRACTION
Notice of formal retraction of an article by Dr Joachim Boldt 397
Please visit the journal web site: http://bja.oxfordjournals.org
Scan to view this journal on your mobile device
106

International Journal of AnaesthesiaVolume 112 Number 3 March 2014
IN THIS ISSUE
In the March BJA . . . viii
EDITORIALS
I. Improving teamwork in anaesthesia and critical care: many lessons still to learnP. G. Brindley 399
II. Retrograde cerebral venous gas embolism: are we missing too many cases?P. A. Bothma and C. J. Schlimp 401
III. Fluid management in association with neonatal surgery: even tiny guys need their saltP.-A. Lonnqvist 404
IV. History of anaesthesia in Colombia: periods of developmentB. O. Trujillo and J. E. P. Baquero 406
REVIEW ARTICLES
Does anaesthesia with nitrous oxide affect mortality or cardiovascular morbidity? A systematic review withmeta-analysis and trial sequential analysisG. Imberger, A. Orr, K. Thorlund, J. Wetterslev, P. Myles and A. M. Møller 410
Effects of dexamethasone as a local anaesthetic adjuvant for brachial plexus block: a systematic review andmeta-analysis of randomized trialsS. Choi, R. Rodseth and C. J. L. McCartney 427
Perioperative cognitive trajectory in adultsM. R. Nadelson, R. D. Sanders and M. S. Avidan 440
SPECIAL ARTICLE
Pelvic pain: a pathway for care developed for both men and women by the British Pain SocietyA. P. Baranowski, J. Lee, C. Price and J. Hughes 452
CARDIOVASCULAR
Effect of palonosetron on the QTc interval in patients undergoing sevoflurane anaesthesiaH. J. Kim, H.-C. Lee, Y. S. Jung, J. Lee, J. J. Min, D.-M. Hong, E.-K. Choi, S. Oh and Y. Jeon 460
Determination of cardiac output by ultrasound dilution technique in infants and children: a validation studyagainst direct Fick principleM. Boehne, M. Baustert, V. Paetzel, H. Koditz, S. Schoof, C. M. Happel and H. Bertram 469
b2-Adrenoceptor gene variants affect vasopressor requirements in patients after thoracic epiduralanaesthesiaU. H. Frey, J. Karlik, F. Herbstreit and J. Peters 477
CLINICAL PRACTICE
Efficacy of palonosetron for the prevention of postoperative nausea and vomiting: a randomized,double-blinded, placebo-controlled trialH. R. Chun, I. S. Jeon, S. Y. Park, S. J. Lee, S. H. Kang and S. I. Kim 485
Comparison of the prognostic accuracy of scoring systems, cardiopulmonary exercise testing, and plasmabiomarkers: a single-centre observational pilot studyS. James, S. Jhanji, A. Smith, G. O’Brien, M. Fitzgibbon and R. M. Pearse 491
Evaluation of surgical conditions during laparoscopic surgery in patients with moderate vs deepneuromuscular blockC. H. Martini, M. Boon, R. F. Bevers, L. P. Aarts and A. Dahan 498
107

Propofol EC50 for inducing loss of consciousness is lower in the luteal phase of the menstrual cycleF. Fu, X. Chen, Y. Feng, Y. Shen, Z. Feng and B. Bein 506
CRITICAL CARE
Limits of agreement between measures obtained from standard laboratory and the point-of-care deviceHemochron Signature Elitew during acute haemorrhageT. Gauss, S. Hamada, I. Jurcisin, S. Dahmani, L. Boudaoud, J. Mantz and C. Paugam-Burtz 514
Radial artery applanation tonometry for continuous non-invasive arterial pressure monitoring in intensivecare unit patients: comparison with invasively assessed radial arterial pressureA. S. Meidert, W. Huber, J. N. Muller, M. Schofthaler, A. Hapfelmeier, N. Langwieser, J. Y. Wagner, F. Eyer,R. M. Schmid and B. Saugel 521
NEUROSCIENCES AND NEUROANAESTHESIA
Global field synchrony during general anaesthesiaN. Nicolaou and J. Georgiou 529
PAEDIATRICS
Postoperative decrease in plasma sodium concentration after infusion of hypotonic intravenous solutions inneonatal surgeryG. Edjo Nkilly, D. Michelet, J. Hilly, T. Diallo, B. Greff, N. Mangalsuren, E. Lira, I. Bounadja, C. Brasher,A. Bonnard, S. Malbezin, Y. Nivoche and S. Dahmani 540
QUALITY AND PATIENT SAFETY
National critical incident reporting systems relevant to anaesthesia: a European surveyS. Reed, D. Arnal, O. Frank, J. I. Gomez-Arnau, J. Hansen, O. Lester, K. L. Mikkelsen, T. Rhaiem, P. H. Rosenberg,M. St. Pierre, A. Schleppers, S. Staender and A. F. Smith 546
REGIONAL ANAESTHESIA
Flexion-rotation manoeuvre increases dimension of the acoustic target window for paramedian thoracicepidural accessN. Ramsay, J. Walker, R. Tang, H. Vaghadia and A. Sawka 556
RESPIRATION AND THE AIRWAY
Upper limb muscular activity and perceived workload during laryngoscopy: comparison of Glidescopew andMacintosh laryngoscopy in manikin: an observational studyD. Caldiroli, F. Molteni, A. Sommariva, S. Frittoli, E. Guanziroli, P. Cortellazzi and E. F. Orena 563
TRANSLATIONAL RESEARCH
Effects of ex vivo platelet supplementation on platelet aggregability in blood samples from patients treatedwith acetylsalicylic acid, clopidogrel, or ticagrelorE. C. Hansson, C. Shams Hakimi, K. Astrom-Olsson, C. Hesse, H. Wallen, M. Dellborg, P. Albertsson andA. Jeppsson 570
CORRESPONDENCE
Correspondence 576
BOOK REVIEW
Book Review 601
ABSTRACTS
Abstracts of the Chinese Society of Anesthesiology 603P
Please visit the journal web site: http://bja.oxfordjournals.org
Scan to view this journal on your mobile device
108





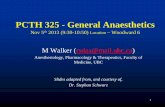





![JAK2/STAT3 Pathway is Required for α7nAChR-Dependent ... · anaesthesia with isoflurane (induction 5%, 2% maintenance) [19], and all efforts were made to minimise animal suffering.](https://static.fdocument.org/doc/165x107/602fd315e0e02e760b543cee/jak2stat3-pathway-is-required-for-7nachr-dependent-anaesthesia-with-isoflurane.jpg)