Biochem part for ICS

of 25
-
Upload
kate-alyssa-caton -
Category
Documents
-
view
216 -
download
0
description
ICS
Transcript of Biochem part for ICS
1. Describe a globin chain as to: its helices and the relation of the helices to the heme plane
HEMOGLOBIN
A. Structure 4 subunits:o 2 alpha chains o 2 beta chains o Bound mainly by non covalent forces Normal adult hemoglobin content: o Variants:HgbA (22) 95%HgbA2 (22) 4% (minimal)HgbF (22) 1% (very minimal) Heme Plane:o Most closely associated with helix Fo Iron at the center with 6 coordination points: 4 occupied by Pyrrole nitrogen5th bound to proximal histidine or the F8; has direct contact with heme.6th occupied by oxygen (oxyhemoglobin); if empty (deoxyhemoglobin). Has direct contact with E7 (7th amino acid on helix E) or distal histidine.
2. Compare and contrast: proximal and distal histidine as to its relation to the heme plane.
Proximal Histidine F8 or 8th amino acid residue in helix F In direct contact with iron of the heme plane Most closely associated with heme plane (hence the term proximal reference point is heme)
Distal Histidine E7 or 7th amino acid residue in helix E In direct contact with oxygen which is bound to heme plane (not in contact with iron/heme; hence, the term distal)
3. Describe a globin chain as to its: helices and the relation of the helices to the heme plane.
Hemoglobin: 4 polypeptide chains; 4 globin chains of hemoglobin contain 1 heme per globin chain = Hgb contains 4 heme planes per hemoglobin molecule
Myoglobin: consists of eight alpha helical segments which are linked to one another by turns to form a globular structure
Myoglobin can bind only one molecule of oxygen, because it contains only one heme group. In contrast, hemoglobin can bind four oxygen molecules one at each of its four heme groups.
BINDING SITES ON THE HEMOGLOBIN MOLECULE Carboxy terminus: formation of salt bridges Amino terminus: H proton binding and CO2 binding Heme Plane exclusive for Oxygen
4. Define: oxygen saturation curve, partial pressure of oxygen, fraction of inspired oxygen, oxygen affinity.a. How is oxygen affinity measured?
Y axis: Hgb saturation or O2 sat; expressed in % X axis: partial pressure of O2 levels (pO2)
The oxygen dissociation curve for hemo globin is sigmoidal in shape (in contrast to that of myoglobin, which is hyperbolic), indicating that the subunits cooperate in binding oxygen.
Oxygen binding curve plot of fractional saturation (Y axis) versus concentration of oxygen (X axis) o The value of Y range from 0 (all sites empty) to 1 (all sites filled).
Partial Pressure of Oxygen:Diffusion of gases is from areas of high pressure to areas of low pressure Process: Arterialization of venous/deoxygenated blood: CO2 that is rich in venous blood from tissues contact with alveoli diffuse CO2 into alveoli then out to atmosphere CO2 partial pressure barely changed (45 to 40 mmHg) so it becomes a reference value. (This is the reason why CO2 is the true measure of alveolar ventilation and not oxygen.)
Measuring oxygen affinity:
The states can readily depict the oxygen affinity of hemoglobin. o T (tensed) state: Associated with deoxyhemoglobin Shift to the right: low affinity to O2 More stable o R (relaxed state): Associated with oxyhemoglobin Shift to the left: high affinity to O2 (exposes more oxygen binding sites)
5.1 Compare and contrast myoglobin (Mb) and Hemoglobin (Hgb) as to:A. Structure protein structure, helices, and heme planeB. Function
MyoglobinHemoglobin
Structure:One globin chain and one heme plane (O2 binding site), consists of eight alpha helical segments which are linked to one another by turns to form a globular structure.A protein in tertiary structure, single polypeptide chain with domains divided into helices
Function:O2 storage (in times of increased demand) Transports O2, CO2 and H+ = isohydric mechanism
Structure:4 subunits: o 2 alpha chains o 2 beta chains o Bound mainly by non covalent forces
Heme Plane: o Most closely associated with helix F o Iron at the center with 6 coordination points: 4 occupied by Pyrrole nitrogen 5th bound to proximal histidine or the F8; has direct contact with heme. 6th occupied by oxygen (oxyhemoglobin); if empty (deoxyhemoglobin). Has direct contact with E7 (7th amino acid on helix E) or distal histidine.
Function:-transport O2 and CO2
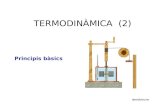
5.2 Compare and contrast the oxygen saturation curve of Mb, Hbf, and Hba, in the peripheral tissue and lungs
Oxygen saturation curves for myoglobin and hemoglobin. The saturation curve for myoglobin shows the typical rapid oxygen concentration-dependent saturation of this monomeric oxygen-binding protein. The other two curves show the typical sigmoidal saturation curves for cooperative oxygen binding exhibited by fetal hemoglobin (HbF) and adult hemoglobin (HbA). Also indicated in the diagram are the typical oxygen concentrations in peripheral tissues and the lungs. Note that whereas, myoglobin can be fully oxygen saturated in the tissues, hemoglobin requires much higher oxygen tension to become fully saturated which only occurs in the lungs. The position of HbF saturation to the left of HbA (i.e. at lower oxygen tension) reflects the fact that fetal hemoglobin binds oxygen with higher affinity than adult hemoglobin and this is so that the fetus can acquire oxygen from the maternal circulation. (from themedicalbiochemistrypage.com)
Lungs: o 96% sat: pO2: 80-100 (normal) located in Plateau o Hemoglobin takes oxygen maximally Lungs to Tissues: Descent of the curve/Steep Curve going Down o Rapid release of oxygen into the tissues/cells/extrapulmonary cells o Rapid effective delivery of O2 into the tissues after its rapid decline in % saturation or arterial O2 tension (from old trans) Tissues to Lungs: Rapid rise of the curve/ Steep Curve going Up o From systemic venous blood (40mmHg), there is a rapid uptake or increase in % saturation and arterial O2 tension
6. Compare and contrast the oxygen saturation curve of Hbf and HbA in the fetal venous blood, fetal arterial blood, and adult venous blood.
(Refer to graph in #5)
Typically, fetal arterial oxygen pressures (for HbF) are lower than adult arterial oxygen pressures (HbA). Hence higher affinity to bind oxygen is required at lower levels of partial pressure in the fetus to allow diffusion of oxygen across the placenta.
Not super sure here, pero ito na closest I could find for #6 :( Wala sa transes.
7. Define cooperativity in oxygen binding of globin proteins.
Cooperativity - activity at one functional site affects the activity at others. As a consequence, a slight change in substrate concentration can produce substantial changes in activity.
Significance of cooperative binding: Oxygen must be transported in the blood from the lungs to the tissues. If there is no cooperativity, only 67% (max.) is saturated with O2, which is not enough to support our metabolic processes (example is in the lungs) For the cells in the tissues, with PO2 at 20 torr level, only 38% is delivered Since the 4 globin chains in Hgb exhibits cooperativity, Hgb becomes nearly saturated with oxygen such that 96% oxygen saturation with PO2 level at 100 torr. When hemoglobin moves to the tissues, the saturation level drops to 32% therefore there is release of oxygen content by around 66%. Since Mgb has only 1 heme plane, can only contribute around 7% delivery to tissues. Binding would require more cooperativity. Because of interface interaction of four globin chains, they are able to maximize uptake of oxygen. But if each globin chain acts separately then there would be no significant conformational changes thus there would be significantly less uptake of oxygen by hemoglobin.
8. Compare and contrast cooperativity in Hb and Mb.
Cooperativity - activity at one functional site affects the activity at others. As a consequence, a slight change in substrate concentration can produce substantial changes in activity.
Significance of cooperative binding: Oxygen must be transported in the blood from the lungs to the tissues. If there is no cooperativity, only 67% (max.) is saturated with O2, which is not enough to support our metabolic processes (example is in the lungs) For the cells in the tissues, with PO2 at 20 torr level, only 38% is delivered Since the 4 globin chains in Hgb exhibits cooperativity, Hgb becomes nearly saturated with oxygen such that 96% oxygen saturation with PO2 level at 100 torr. When hemoglobin moves to the tissues, the saturation level drops to 32% therefore there is release of oxygen content by around 66%. Since Mgb has only 1 heme plane, can only contribute around 7% delivery to tissues. Binding would require more cooperativity. Because of interface interaction of four globin chains, they are able to maximize uptake of oxygen. But if each globin chain acts separately then there would be no significant conformational changes thus there would be significantly less uptake of oxygen by hemoglobin.
9.) Compare and contrast T and R state of Hb as to: Relation of Fe to the heme plane Presence of salt bridges Heme pocketsT (tensed) state: Associated with deoxyhemoglobin Shift to the right: low affinity to O2 More stableDinagdag ko lang to kahit wag na isulat haha R (relaxed state): Associated with oxyhemoglobin Shift to the left: high affinity to O2 (exposesmore oxygen binding sites)
10.) Compare and contrast the affinity of Hb and Mb to carbon monoxide CO has higher affinity to Hgb compared to O2. CO prefers to bind to the heme plane of hemoglobin in a perpendicular manner. Myoglobin, having only a single binding site at heme plane, insists that oxygen should bind at a slightly oblique angle. This is due to the effect of distal histidine. Myoglobin is more protective of its heme plane, hence, it has slight resistance to the harmful effects of CO.
12.) Describe the biochemical basis of Bohr effect.
11. Enumerate the allosteric effectors of Hb and their relevance on oxygen delivery to tissues.
1. The Bohr Effect The binding of protons by Hgb which lowers its affinity for oxygen High hydrogen concentration, w/c is measured by low pH, would favor a more extensive combination, more salt bridges of the T state, hence it would favor oxygen release. The more tense Hgb is, the higher the tendency for O2 release Acidity enhances the release of oxygen. Advantageous because O2 cannot stay bound to Hgb. It must be released to the tissues. T state is more stable Lungs Actively metabolizing tissues
pH pH due to H+ secretion
Hgb binds O2 Hgb releases O2
Hgb releases H+ Hgb binds H+
2. pH Low pH: positive allosteric effector High pH: negative allosteric effectorShifted to the right Slightly low pH Less affinity of O2 to Hgb more release of O2
Shifted to the left High pH More affinity of O2 to Hgb less O2 release into tissues
3. Temperature
Increased Temperature Positive allosteric effector Advantages: a) Support Oxygen demand in fever b) Support Oxygen demand in exercise Increase in core body temperature will require more oxygen Hypothermia Compensatory Mechanisms a) O2 utilization b) O2 solubility in plasma (from 2.3 to 4 or 5 mL O2/L) c) CO2 solubility Because of the effect of temperature, there is an added 21% higher release of O2 into the tissues Positive allosteric effect
4. Effect of BPG (Bisphosphoglycerate) BPG: mild tissue hypoxia a) Mild Anemia (Hgb , 12g/dL) b) Mild CP (cardiopulmonary) insufficiency (e.g. smoking) c) altitude
If there is no BPG on RBCs: o Sigmoidal dissociation curve becomes more hyperbolic o This means there is a significant 8% of O2 which will not be released into the tissues readily.
5. CO2
Most of the CO2 produced in metabolism ishydrated and transported as bicarbonate ion. However,some CO2 is carried as carbamate bound to the N-terminal aminogroups of hemoglobin (forming carbaminohemoglobin), which can be represented schematically as follows:Hb NH2 + CO2 Hb NH COO + H+
The binding of CO2 stabilizes the T (taut) or deoxy form ofhemoglobin, resulting in a decrease in its affinity for oxygen and a right shift in the oxygen dissociation. In the lungs, CO2 dissociates from the hemoglobin, and is released in thebreath.
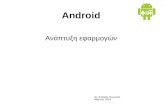
14. Review the formation of BPG in the cell
SOURCE: MARKS MEDICAL BIOCHEMISTRY
2,3-Bisphosphoglycerate (2,3-BPG) is formed in red blood cells from the glycolytic intermediate 1,3-bisphosphoglycerate, as indicated in Figure. 2,3-BPG binds to hemoglobin in the central cavity formed by the four subunits, increasing the energy required for the conformational changes that facilitate the binding of oxy- gen. Thus, 2,3-BPG lowers the affinity of hemoglobin for oxygen. Therefore, oxy- gen is less readily bound (i.e., more readily released in tissues) when hemoglobin contains 2,3-BPG.
15. Compare and contrast:a. Binding of BPG to HBa and HBf
Hgb dissociation curve: HgbF vs HgbAo His143 is replaced by serine (uncharged) 2 less (+) charged siteso Resistant to BPG because of absence of His143o Hyperbolic curve: O2 is extracted from maternal blood to fetal RBC
HgbF binds to BPG less than HgbA because of serine residue in HgbF; this optimizes the transfer of O2 from maternal to fetal circulation The fetal red blood cells have a higher oxygen affinity than maternal red blood cells because fetal hgb does not bind 2,3-BPG, theres a substitution of a serine residue of His 143 in the chain, part of 2,3-BPG binding site. (Stryer)NOTE: At 3 months old, infant will have HgbA
b. the effect on oxygen affinity and its delivery to tissues
Figure 10. BPG/2,3-DPG competitively binds with O2; Hgb becomes T state2,3-BPG lowers the affinity of hemoglobin for oxygen. Therefore, oxy- gen is less readily bound (i.e., more readily released in tissues) when hemoglobin contains 2,3-BPG.
(+) allosteric effector BPG can occur in cases of mild tissue hypoxia(i.e. mild anemia, mild cardiopulmonary insufficiency, high altitude) Relatively high BPG concentrations in RBC (Lehninger) BPG greatly reduces the affinity of hemoglobin for oxygen (inverse relationship between binding of O2 and binding of BPG). (Lehninger) Compensatory mechanism = BPG (which will lead to O2 release) High O2 affinity = better CO2 unloading Increases cooperativity Favors T state o -chains of Hgb form cavity for BPG- generated from alignment of multiple (+) charges o With no BPG, hemoglobin is easily converted to the R state (Lehninger) 16.) Describe the role of the lungs and the kidneys and RBC in the excretion of CO2 from the body.
RBC and lungs
KidneysCO2 levels in the blood are affected by kidney and lung function. The kidneys help maintain the normal bicarbonate levels17.) Enumerate the forms by which CO2 exists in the body and describe how each contribute to the excretion of CO2 Describe Haldane effect; Chlorate shift; isohydride mechanism Describe the mechanism of action of carbonic anhydrase.Haldane EffectIncrease in the concentration of carbon dioxide will displace oxygen from hemoglobin and binding of Oxygen with Hemoglobin in turn will displace Carbon dioxide from blood.Isohydride mechanism and Chlorate shift
MOA of Carbonic anhydrase His will catalyze the release of one hydrogen, so there will be available binding site for its substrate (CO2). In the process, CO2 is converted to bicarbonate and is released. To regenerate the binding site, it has to bind to another molecule of water.
18. Describe the role of the lungs in the maintenance of acid-base balance in the body:
The respiratory system has an important role in the maintenance of acid base balance this is through the regulation of carbon dioxide and it is important because the major blood buffer is the carbon dioxide - bicarbonate buffer system and it has an important role in the maintenance of normal body pH and acid-base balance and then the body, in normal condition would always maintain normal oxygenation status to ensure adequate oxygen to supply our metabolic processes. (Magat, 2013)
a. Enumerate and define the body buffer system
A buffer is a solution that resists change in pH following the addition of an acid or base.
Body Buffer System:Buffers in blood maintain the pH at about 7.40. Cellular production of acids leads to an acidification of blood where the H+ is buffered by several different bases including HCO3, hemoglobin, and HPO4 (Devlin, 7th ed.) Mainly by formation of carbaminohemoglobin
HEMOGLOBIN (50%) Acts as a buffer of blood pH by binding the hydrogen ions produced by the metabolizing cells and preventing the blood pH from becoming too acidic. (Devlin, 7th ed.) Transports about 40% of the total H+ and 15 20% of the CO2 formed in the tissues in the tissues to the lungs and kidneys. The remainder of the H+ is absorbed by the plasmas HCO3 buffer; remainder of CO2 is transported as dissolved HCO3 and CO2.
OTHER BUFFERS (10%) Organic phosphate (RBC) o Mainly intracellular o Concentration of phosphate is low in the extracellular fluid but the phosphate buffer system is an important urinary buffer Plasma proteins o Absolute amount is small compared to intracellular protein
ISOHYDRIC MECHANISM (40%) Transport of CO2 from tissues to lung in plasma as HCO3 Bicarbonate (HCO3) Maintain a relatively constant plasma pH
b. Review Henderson-Hasselback reaction
The quantitative relationship between the pH of the solution and concentration of a weak acid (HA) and its conjugate base (A) is described by the Henderson-Hasselbach equation. (Lippincott)
The relationship between the pH of a solution, the Ka of an acid, and the extent of its dissociation are given by the Henderson-Hasselbalch equation. (Marks)
In the Henderson-Hasselbalch equation, the formula for the dissociation constantof a weak acid is converted to a convenient logarithmic equation (Equation 4.5).The term pKa represents the negative log of Ka. If the pKa for a weak acid is known,this equation can be used to calculate the ratio of the unprotonated to the protonatedform at any pH. From this equation, you can see that a weak acid is 50% dissociatedat a pH equal to its pKa.Equation 4.5. The Henderson-Hasselbalch equation.For the weak acid HA,
c. Know the formula of the HCO3 buffer system, review how the body handles CO2
CO2 Excretion:In periphery: o Passive diffusion of CO2 into the RBC o Catalytic effect of carbonic anhydrase (enzymatic action) o Facilitated diffusion of bicarbonate from the RBC into the plasma (includes Chloride shift)
In lungs: o Facilitated diffusion of bicarbonate from the plasma into the RBC o Catalytic effect of carbonic anhydrase forming CO2 and H2O o Excretion of CO2 into the atmosphere
In this system, carbon dioxide (CO2) combines with water (H2O) to form carbonic acid (H2CO3), which in turn rapidly dissociates to form hydrogen ions (H+) and bicarbonate (HCO3- ) as shown in the reactions below:
19.) What are arterial blood gases? What is measured by ABGs? How are the concentration of gases expressed? What is the clinical relevance of ABG?An arterial blood gas (ABG) test measures the acidity (pH) and the levels of oxygen and carbon dioxide in the blood from an artery. This test is used to check how well your lungs are able to move oxygen into the blood and remove carbon dioxide from the blood.What is measured by ABGs and How are the concentration of gases expressed?Partial pressure of oxygen (PaO2). This measures the pressure of oxygen dissolved in the blood and how well oxygen is able to move from the airspace of the lungs into the blood.Partial pressure of carbon dioxide (PaCO2). This measures the pressure of carbon dioxide dissolved in the blood and how well carbon dioxide is able to move out of the body.pH. The pH measures hydrogen ions (H+) in blood. The pH of blood is usually between 7.35 and 7.45. A pH of less than 7.0 is called acid and a pH greater than 7.0 is called basic (alkaline). So blood is slightly basic.Bicarbonate (HCO3). Bicarbonate is a chemical (buffer) that keeps the pH of blood from becoming too acidic or too basic.Oxygen content (O2CT) and oxygen saturation (O2Sat) values. O2 content measures the amount of oxygen in the blood. Oxygen saturation measures how much of the hemoglobin in the red blood cells is carrying oxygen (O2).Clinical relevanceAn arterial blood gas (ABG) test is done to: Check for severe breathing problems and lung diseases, such as asthma, cystic fibrosis, or chronic obstructive pulmonary disease (COPD). See how well treatment for lung diseases is working. Find out if you need extra oxygen or help with breathing (mechanical ventilation). Find out if you are receiving the right amount of oxygen when you are using oxygen in the hospital. Measure the acid-base level in the blood of people who have heart failure, kidney failure, uncontrolled diabetes, sleep disorders, severe infections, or after a drug overdose.
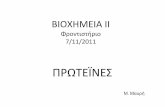
20. Compare/Contrast partial pressures of CO2, & O2 in the atmospheric air, alveoli and blood
Fig 1. Comparison between partial pressure of O2 and CO2Diffusion of gases is from areas of high pressure to areas of low pressure Process: Arterialization of venous/deoxygenated blood: From atmosphere (150mmHg), alveolar O2 is obtained and no CO2From the atmosphere, pAO2 = 150 mmHg and pCO2 = 0 are taken up by alveoli (pCO2 = 0 since we are not supposed to inhale carbon dioxide) Because of gas exchange, venous blood (40 mmHg) will become arterialized/oxygenated (100 mmHg) O2 from high pressure alveoli (150 mmHg from the atmosphere) venous blood arterial CO2 that is rich in venous blood from tissues contact with alveoli diffuse CO2 into alveoli then out to atmosphere CO2 partial pressure barely changed (45 to 40 mmHg) so it becomes a reference value. (This is the reason why CO2 is the true measure of alveolar ventilation and not oxygen.) 21.) Compare the role of the lungs, kidney and RBC in the maintenance of acid-base balance in the body. Pulmonary regulation: CO2 concentration is finely regulated by changes in tidal volume and respiratory rate (minute ventilation). A decrease in pH is sensed by arterial chemoreceptors and leads to increases in tidal volume or respiratory rate; CO2 is exhaled and blood pH increases. In contrast to chemical buffering, which is immediate, pulmonary regulation occurs over minutes to hours. It is about 50 to 75% effective and does not completely normalize pH. Renal regulation: The kidneys control pH by adjusting the amount of HCO3 that is excreted or reabsorbed. Reabsorption of HCO3 is equivalent to removing free H+. Changes in renal acid-base handling occur hours to days after changes in acid-base status. RBC: Red blood cell contains hemoglobin which acts as an important buffer.
22. Compare/Contrast how the RBC handles carbon dioxide in the tissue and in the lungs
(ENOUGH NA ACTUALLY YUNG DIAGRAM ITSELF PERO HERES OTHER INFO NA LANG)
Buffers in blood maintain the pH at about 7.40. Cellular production of acids leads to an acidification of blood where the H+ is buffered by several different bases including HCO3, hemoglobin, and HPO4 (Devlin, 7th ed.) Mainly by formation of carbaminohemoglobin 4 amino terminal groups the binding sites of hydrogen protons In less frequency, hydrogen can also bind to histidine residues. In each globin, chain there are 30. HEMOGLOBIN (50%) Acts as a buffer of blood pH by binding the hydrogen ions produced by the metabolizing cells and preventing the blood pH from becoming too acidic. (Devlin, 7th ed.) Transports about 40% of the total H+ and 15 20% of the CO2 formed in the tissues in the tissues to the lungs and kidneys. The remainder of the H+ is absorbed by the plasmas HCO3 buffer; remainder of CO2 is transported as dissolved HCO3 and CO2. Ionizable groups with pK values close to RBC pH Contains 4 N terminal groups and imidazole side chains of histidine residues (#38) OTHER BUFFERS (10%) Organic phosphate (RBC)o Mainly intracellularo Concentration of phosphate is low in the extracellular fluid but the phosphate buffer system is an important urinary buffer Plasmaproteins o Absolute amount is small compared to intracellular protein ISOHYDRIC MECHANISM (40%) Transport of CO2 from tissues to lung in plasma as HCO3 Bicarbonate(HCO3) - Maintain a relatively constant plasma pH B. Carbon Dioxide Excretion In periphery: o Passive diffusion of CO2 into the RBC o Catalytic effect of carbonic anhydrase (enzymatic action) o Facilitated diffusion of bicarbonate from the RBC into the plasma (includes Chloride shift) Inlungs: o Facilitated diffusion of bicarbonate from the plasma into the RBC o Catalytic effect of carbonic anhydrase forming CO2 and H2O o Excretion of CO2 into the atmosphere
23. Describe intracellular buffering in acidosis
Respiratory CompensationIn metabolic acidosis: The rate and depth of breathing are elevated Blood pH is below 7.35 and bicarbonate level is low As carbon dioxide is eliminated by the respiratory system, PCO2 falls below normalRenal CompensationAcidosis has high PCO2 and high bicarbonate levels The high PCO2 s the cause of acidosis The high bicarbonate levels indicate the kidneys are retaining bicarbonate to offset the acidosis
A. Describe the role of proteins and phospholipids
Phosphate Buffer System Nearly identical to the bicarbonate system Its components are: Sodium salts of dihydrogen phosphate (H2PO4), a weak acid Monohydrogen phosphate (HPO42), a weak base This system is an effective buffer in urine and intracellular fluidProtein Buffer System Plasma and intracellular proteins are the body's most plentiful and powerful buffers Some amino acids of proteins have: Free organic acid groups (weak acids) Groups that act as weak bases (e.g., amino groups) Amphoteric molecules are protein molecules that can function as both a weak acid and a weak base
24.) Describe the role of the kidney in acid-base balance.
Renal system1. Reabsorption of bicarbonate
Carbonic acid formed in the RBC moves to the glomerulus, the tubular cell and tubular lumen. Carbonic acid will get into the tubular cell where it will dissociate into acid and bicarbonate. Bicarbonate will be reabsorbed. Acid is excreted through the buffer system. The proton excreted to the lumen will be exchanged for another cation, Na+. This process is limited by the fact that it requires exchanging with a cation, Na+. The amount of Na+ in the body is limited. This process is also limited by the dissociation constant of the blood buffer system.
2. Excretion of titrable acidity
During illness, the dissociation constant of the blood buffer system is exceeded. As a result, another process is needed for excretion of acids. This is achieved through the phosphate buffer system, excretion of titrable acidity. The excretion starts through the CO2-HCO3- buffer system, then once its dissociation constant has been exceeded, acid will then be excreted through the phosphate buffer system. The amount of H+ in the urine can be measure by determining the amount of alkali required to neutralize the urine. This is called titrable acidity. It is called titrable acidity, since the condition in the tubular cell would be maintained within normal by the same buffer system. The amount of acid excreted requires that the same amount of acid would be replaced within the system to minimize pH change.
3. Excretion as ammonia
Sometimes, during severe illness, even the phosphate buffer systems dissociation constant is exceeded. Therefore, excretion of acid by ammonia then is needed. Ammonium is produced through the degradation of amino acids. During illness, a lot of cells are destroyed. This results to the degradation of more amino acids, producing a lot of ammonia. Acid can now be excreted as ammonia. This explains how the kidneys compensate for acidosis completely, but this requires time since it has to wait for amino acids to be degraded. The kidneys can respond in three (3) days, but the compensation is complete. Within minutes to six (6) hours, the lungs can respond more quickly, although the response is incomplete. In the liver, ammonia is converted to urea and is eliminated from the body through the urine. The remaining ammonia combines with H+ to form the ammonium ion (NH4+) in the renal tubules. NH4+ also displaces Na+ and is eliminated in the urine.
25. Name, describe and compare the different acid-base disorders
Acidosis O Respiratory - alveolar hypoventilation (ex. Heavily sedated, heavily intoxicated, with head injury)O Metabolic H+ overproduction (ex. Severe dehydration, renal problems, diabetic ketoacidosis, lactic acidosis)- HCO3 over excretion (in cases of renal tubular acidosis give patient bicarbonate tablets as replacement)AlkalosisO Respiratory Alveolar hyperventilation (ex. Hysteria)O Metabolic Alkali ingestion (iatrogenic, doctor-induced)
26. Describe how compensatory mechanisms take place in cases of acid-base disorders.
DISORDERCompensatory MechanismsOnset of Compensation
Metabolic AcidosisDECREASE pCO2Minutes/Hours
Metabolic AlkalosisINCREASE pCO2Minutes/Hours
Respiratory AcidosisINCREASE Renal HCO3, re absorption & plasma HCO2- concentrationDays
Respiratory AlkalosisDECREASE Renal HCO3 reabsorption & plasma HCO3 concentrationDays