Biochem Exam 2 Review.2
42
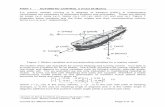
BIOCHEMISTRY 13. THE CONJUGATION OF CARBOHYDRATES TO EACH OTHER & PROTEINS 1. Produces either an α (below) or β-glycoside (above) depending on oxygen position a. Determines if digestion occurs (as beta in cellulose à cant digest) 2. Polymerization involves activated sugar nucleotide intermediates (e.g. UDP-Galactose) 3. Maltose : two glucoses in an α(1à4) linkage 4. Lactose : galactose & glucose in β(1à4) linkage 5. Sucrose : glucose & fructose (α-D-glucosyl-β-D-fructoside)
description
#schoolwork #biochemistry
Transcript of Biochem Exam 2 Review.2

BIOCHEMISTRY
13. THE CONJUGATION OF CARBOHYDRATES TO EACH OTHER & PROTEINS
1. Produces either an α (below) or β-glycoside (above) depending on oxygen positiona. Determines if digestion occurs (as beta in cellulose à cant digest)
2. Polymerization involves activated sugar nucleotide intermediates (e.g. UDP-Galactose)
3. Maltose : two glucoses in an α(1à4) linkage4. Lactose : galactose & glucose in β(1à4) linkage5. Sucrose : glucose & fructose (α-D-glucosyl-β-D-fructoside)

6. Glycogen: homopolymers of glucose; chains of glucose with α(1à4) linkages with closely spaced branching via α(1à6) linkages every 8-10 residues; spherical particles in cytoplasm
7. Starch: homopolymers of glucosea. Amylose : unbranched chain with α(1à4) linkage helical coilb. Amylopectin : α(1à4) linkages but is branches every 12 residues via an
α(1à6) linkage8. Cellulose : Unbranched chain with β(1à4) linkages9. Glycosaminoglycans (GAGs) : long unbranched polysaccharides of repeating anionic
disaccharides that may be sulfated; important part of connective tissuea. Negatively charged (highly hydrated)b. E.g. Chondroitin sulfate; keratin sulfate; heparin; hyaluronic acid
10. Glycation : proteins reacting with sugars; non-enzymatic involving Schiff base formation
between the aldehyde of the sugar and an amino group on the protein to generate a ketoamine; no cofactorsa. Is for secreted proteins or domains facing extracellularly (except for O-GlcNac)b. Can be N-linked (Asn) or O-linked (Ser, Thr)
c. E.g. diabetic Glycated Hemoglobin (HbA1C) gives an integrated average of blood sugar level over the past two months
11. Glycoproteins : critical for biological recognition (e.g. blood types; influenza virus)a. Exported out of the cell or have their glycosylated domains oriented outside
(except for O-GlcNac)b. O-GlcNac glycoproteins are found in the nucleus and cytoplasm; regulate
cellular responses to hormones as well as regulate transcription, cell growth & division
12. O-linked glycoproteins have carbohydrate added to the protein one sugar at a timea. Are glycosylated in the Golgib. E.g. blood group substances; salivary musins
13. N-linked glycoproteins have carbohydrate first added as a preassembled 14 sugar blocka. First stage is formation of a branched oligosaccharide on a lipid carrier molecule (dolichol phosphate)b. Dolichol is phosphorylated by a kinase c. Synthesis is begun by the sequential transfer of a residue from UDP-N-acetylglucosamine to the
phosphate of dolichol-phosphate on the ER membrane
d. Tunicamycin : antibiotic that selectively inhibits the addition of N-acetylglucosamine-phosphate to dolichol phosphate
14. Blood groups are dependent on sugar residues at the ends of carbohydrate chains of glycoproteins or glycolipids

a. Type O individuals are more prone to ulcers because H.Pylori binds specific structures that look like type O sugars
15. Proteoglycans : consists of negatively-charged polysaccharide glycosaminoglycan chains which are attached to a core of protein
a. E.g. Heparin sulfate, collagen, and laminin are interwoven in the basement membrane
16. Selectin- Carbohydrate systema. Recruitment of WBC into areas of infectionb. Leukocyte-adhesion deficiency II
i. Many infections early in life; inability to create pus at wound site; don’t recruit WBCs
ii. Inability to put fucose onto things (to make something the selectins will recognize)
iii. Abnormal blood type (Bombay)17. Congenital diseases of glycosylation (CDGs): patients are defective in one or more
enzymes that break down glycoproteins; different clinical presentations a. Lysosomes have both endo and exoglycosidasesb. Enzyme deficiencies result in accumulation of partially degraded materials in vesicles that impair
function; partial breakdown products are excreted in urine
c. Single cell defects i. Pompe :
1. Glycogen storage disease type II2. Accumulation of glycogen in the lysosome due to deficiency of the lysosomal acid
alpha-glucosidase enzyme. It is the only glycogen storage disease with a defect in lysosomal metabolism
d. Multiple enzyme defects i. I Cell : Failure of the M6P system leads to export of lysosomal
enzymes1. Normally, N-linked glycoproteins can be modified to generate mannose 6-
phosphate, which is recognized by a receptor in the endosomal trafficking system that causes the modified protein to be transported to the lysosome
14. DIGESTION, ABSORPTION, AND CELL UPTAKE OF CARBOHYDRATES

1. Monosaccharides: glucose, fructose2. Disaccharides
a. Maltose (Glu-Glu)b. Lactose (Gal-Glu)c. Sucrose (Fru-Glu)
3. Polysaccharidesa. Starch (Glu)
i. Amylose is the linear polyglucoseii. Amylopectin is the branched polyglucose
4. Carbohydrate digestion starts in the mouth and continues in the intestinea. Salivary α –Amylase is inactivated by low pH of stomach (stomach doesn’t
digest carbohydrates)i. The end products of starch digestion by α –Amylase
are:1. Maltose, maltotriose, and small branched
oligosaccharides (limit dextrins)a. Are cleaved by specific enzymes
present in the brush border membranes of mucosal cells of the small intestine
2. NOT glucose
Name Origin Acts onα -Amylase Salivary glands Glu-α(1à4)-glu
in starchα-Amylase Pancreas Glu-α(1à4)-glu
in starchMaltase Intestinal mucosa Glu-α(1à4)-glu
in maltoseIsomaltose Intestinal mucosa Glu-α(1à6)-glu
in isomaltose and branched dextrins
Sucrase Intestinal mucosa Glu-α(1à2) β-fru in sucrose

Lactase Intestinal mucosa Gal- β(1à4)glu in lactose
5. Lactose intolerance : Failure to digest lactose; lactase insufficiency
a. Can be diagnosed by failure to observe glucose increase after lactose challenge; can observe H2 in the breath
b. Normally: Lumen of intestine: lactose à glucose and galactose
c. Intolerance : lactose passes further down GI tract and its metabolism by bacteria in colon à formation of gas
i. These compounds have an osmotic effect of sucking water out from intestinal cells
6. Mammals lack enzymes to digest cellulose (has glu-β(1à4)glu bonds) and many other plant polysaccharides of dietary fiber
a. Mammalian enzymes that cleave starch and glycosidic bonds of galactose, mannose, pentoses, or sugar acids (from pectin, gum, agar)
b. E.g. xylose; arabinose7. Facilitated diffusion
a. Mediated by specific membrane carrier proteins and is saturable (the number of carrier protein molecules limits the rate transport as solute concentration increases)
b. Does not require metabolic energyc. Requires a concentration gradient maintained by rapid removal of the transported sugar from inside
the cell to the capillaries
d. E.g. fructose; mannose; also glucose absorption into intestinal cells (in addition to active transport in intestine) à glucose release is facilitated transport, first stop is the liver
8. Active transport a. For glucose & galactose in intestineb. Allows absorption against a concentration gradientc. The entry of sugar is coupled to the entry of Na+ (for which there is always
a gradient of concentration from the outside [high] to the inside)d. Sugar & Na+ are carried by the same carrier protein e. At a different site on the cell membrane, energy is expended (via hydrolysis of
ATP) by the cell to maintain the Na+ concentration gradient (to pump Na+ out)
i. Membrane moves K+ into the cell while moving Na+ out

Lumen Cell Blood Other cells[glucose] Medium High Medium Low
Transport Active àCell FacilitatedàBlood
FacilitatedàCell
9. Transportersa. SGLT (Sodium-linked)/ active transport
i. Intestinal mucosa; Kidney brush border b. Facilitative
i. Responsive to insulin (GluT4)1. Skeletal muscle, fat, WBC
ii. Not responsive to insulin1. GluT 2: liver, pancreas, intestine
10. Liver, RBC, and brain cells : carrier-mediated transport is not stimulated by insulin11. Muscle, fat, and WBC : glucose absorption is stimulated by insulin which acts by
mobilizing the transporters from stores on the membranes of the ERa. Insulin reduces circulating
blood glucose by stimulating uptake
i. Promotes generation of fat & storage of glucose as glycogen, and decrease of PGL
b. Unstimulated cells have an increased ability to transport glucose in the presence of insulin
12. Diabetics &Blood Glucose Levela. The rise in concentration reflects:
i. Absorption into the bloodii. Removal from the blood by all tissues
iii. Conversion of glucose to lactate, glycogen, and fat in the liver
iv. Conversion of non-glucose substrates to glucose in liver
v. Return of glucose to blood from liverb. Doubling of glucose after a meal; return
within 2 hours
c. Diabetes: start higher, go higher, come down slower13. Lack of an increase in BGL after ingestion of meal with free glucose would indicate a
a. Defect in absorption of glucose from intestine 14. Lack of an increase after ingestion of maltose could reflect defect in either
a. Digestion of the disaccharide to free glucose

b. Or absorption of the glucose
15. Glucose is phosphorylated quickly when it is absorbed by isoenzymes (glucokinase or hexokinase)
a. G6P is charged and cannot exit the cell
Enzymes Distribution Km for glucose
Effect Regulation
Hexokinases All tissues <0.2 mM
Low Km (high affinity; essentially always on)
Feedback inhibition by
product (G6P)Glucokinase Liver,
pancreatic islet β-cells
10-20 mM
High Km; High Vmax à high capacity but low
affinity
Substrate concentration and
amount of enzyme; Most active when BGL is high
16. Hexokinase a. Can phosphorylate other hexoses (e.g. fructose)b. High affinity for glucose (km=.1mM vs 5mM glucose concentration)
i. Enzymes are always fully on; most tissues always need steady supply of G6P to remain onc. If cell has enough G6P, it doesn’t need more (product inhibition)
17. Glucokinase a. Found in liver (first look at high glucose after a meal; makes even more
glucokinase in a high carb diet) & pancreasb. High Vmax allows liver to effectively remove excess glucose, and minimize
hyperglycemia after eating

c. High BGL àIncreases glucose uptake by the liver; allows glucose to be stored as glycogen; BGL exiting liver is lower than entering
i. In liver, insulin stimulates gene transcription and synthesis of glucokinase
d. Not inhibited by G6P (don’t want it to be product inhibited); want liver to be able to continue in high glucose conditions
e.
e. Acts as part of glucose sensor system in pancreatic islet β-cells (which secrete insulin in response to high BGL to regulate glucose metabolism in liver & other tissues by mechanisms that will lower the BGL)
i. High BGLà high ATP à shuts off potassium channel à insulin release
1. High BGL 2. Activate glucokinase3. Beta cell make more ATP
a. Which regulates the ATP-K channel that maintains cell polarity
4. Depolarizes the cell5. Calcium influx6. Release of insulin
18. Diabetesa. Type I diabetic
i. Higher resting glucose concentrationii. Higher peaks in plasma glucose after meal
iii. Return to baseline sloweriv. Not producing insulin necessary to control blood sugar
b. Type II i. Have the pancreatic islet β-cells to make insulin
ii. Maturity onset diabetes of the young (MODY) : glucokinase gene or transcriptional regulation factor mutation;
1. Is based on a single mutation in one of several genes, so this class of type II is also called autosomal dominant type II diabetes
2. Not enough glucokinase causes β-cells to not respond normally to ingested glucose, so they do not secrete insulin normally
3. Mild to moderate hyperglycemia4. Is not associated with obesity or high blood lipid levels

INsulIN stimulates 2 things to go IN 2 cells: Potassium and Glucose."In the Phasted State, Phosphorylate":
The phosphorylation cascade becomes active when blood glucose is low
15. THE METABOLISM OF GLUCOSE: GLYCOLYSIS
a. Glucose to Pyruvate (aerobic) or Lactate (anaerobic) yielding 2ATP/mole glucoseb. Eleven enzymatic reactions; all the enzymes are present in the soluble cytoplasm of the cell
i. Hexokinase 1. Input: 2 ATP/ 1 mole glucose 2. Product: Glucose-6-Phosphate + ADP3. Irreversible
ii. Phosphohexose isomerase1. Input: Glucose-6-Phosphate2. Product: Fructose-6-Phosphate
iii. Phosphofructokinase 1 (PFK 1)1. Input: Fructose-6-Phosphate + ATP2. Output: Fructose-1,6-bisP
3. Inhibited by excess ATP, PEP, Citrate, glucagona. Glucagon shuts off the kinase activity of PFK2. This reverses any synthesis of F-2,6-BP
from F6P and thus inhibits PFK1 activity
4. Relieved by AMP, ADP, Pia. Fructose-2,6-bisphosphate is an allosteric activator of PFK1 b. When PFK-2/F-2,6-bisphosphatase is phosphorylated (P*) by Protein kinase A in
muscle, PFK-2 is activated and F-2,6-bisphosphatase is inhibited. The concentration of Fructose-2,6-bisphosphate is raised so glycolysis is activated
c. Dephosphorylation of PFK-2 drives glycolysis5. *First step committed uniquely to glycolysis 6. PFK1 deficiency : exercise intolerance in skeletal muscle
iv. Aldolase 1. Input: Fructose-1,6-bisP2. Product: two triose-phosphate units
a. Glyceraldehyde-3-P à substrate for next step of glycolysisb. Dihydroxyacetone-P
3. Possible next step: Triose phosphate isomerase (TIM)a. Input: dihydroxyacetone-P b. Product: glyceraldehyde-3-P
c. Pathway only favored when product is removedv. Glyceraldehyde 3-Phosphate Dehydrogenase (GAPDH)
1. Input: glyceraldehyde-3-P + NAD+ + Pi2. Process: oxidation
a. Electrons are accepted by NAD+ coenzymeb. Reaction requires Pi for formation of high energy phosphate bond (at C1) which allows
transfer of the phosphate to ADP3. Product: 1,3-bisphosphoglycerate + NADH + H +
4. Enzyme displays negative cooperativity

a. Binds 4 molecules NAD+ but it becomes harder to add each successive moleculeb. Buffers the enzyme activity from changes in substrate
concentration; enzyme resists the loss of NAD+ that occurs when glycolysis is happening at high rates as in anaerobic muscle
c. Enzyme is sensitive to a much wider range of [S] since it doesn’t get saturated immediately
vi. Phosphoglycerate Kinase (PGK)1. Input: 1,2-bisphosphoglyerate + ADP2. Product: 3-phosphoglycerate + ATP
vii. Phosphoglycerate Mutase (PGM)1. Input: 3-phosphoglycerate2. Product: 2-phosphoglycerate
viii. Enolase 1. Input: 2-phosphoglycerate2. Process: removal of water with creation of high energy phosphate bond
a. Strongly inhibited by fluoride3. Product: Phosphoenolpyruvate
ix. Pyruvate Kinase 1. Input: Phosphoenolpyruvate + ADP
2. Irreversible reaction 3. Stimulated by fructose-1,6-bisphosphate (feed forward stimulation)
4. Inhibited by: alanine, NADH, ATP, fatty acids, and succinyl-CoA5. Product: Pyruvate + ATP
6. PK deficiency causes hemolytic anemiax. Next step happens under anaerobic conditions: Lactate dehydrogenase
1. Input: Pyruvate + NADH + H+
2. Product: Lactate + NAD +
3. This step is required for regeneration of NAD+
2. There is a net yield of 2ATP in the conversion of one glucose to 2 lactatesa. One ATP is used in each of the hexokinase and phosphofructokinase reactionsb. 2ATPs per glucose are generated in each of the 3-phosphoglycerate kinase & pyruvate kinase reactions
3. Poisons can affect glycolysisa. 2-F-Deoxyglucose at hexokinase
i. Allows you to use PET to detect places where a lot of glycolysis is going on à tumors
b. Arsenate affects G3PDH i. Pentavalent arsenate
1. Prevents a net gain of ATP from glycolysis but does not stop the process ii. Mercury compounds & trivalent arsenicals
1. React with sulfhydral group and block the glycolytic process
c. Fluoride inhibits enolase 4. Nicotinamide Adenine Dinucleotide (NAD+) is derived from B-vitamin niacin
a. Pellagra disease i. Niacin deficiency
ii. Poor growth, weight loss, dermatitis, diarrhea, mental disturbances (“3 D’s”)
5. The reduced coenzyme (NADH) is generated by glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and must be recycled (reduced) to NAD+ via lactate dehydrogenase for glycolysis to continue
6. Irreversible steps are sites of regulation and are inhibited under resting conditionsa. Hexokinase b. Pyruvate Kinase
i. Shut off in liver under starvation conditions

c. Phosphofructokinase i. Actual rate of PFK-1 is determined by the amount of a positive
regulator that relieves allosteric inhibition (Fructose-2,6-bisphosphate)
1. F-2,6-BP is made from F6P by PFK-IIii. PFK2 can be regulated by hormones such as insulin & glucagon
1. Phosphatase (Phosphorylated form)
2. PFK2 Synthetase (dephosphorylated form)a. Insulin drives dephosphorylation of PFK2 à activated
PFK2 makes more F2,6BP to positively regulate PFKI to go through the cycle and increase glycolysis
7. Connecting glycolysis with metabolism of pentoses, lipids and amino acids
Allosteric Regulation Phosphorylation Regulation
Induced Enzyme
RegulationRegulated Enzyme Activator Inhibitor Functional State Induced
byHexokinase Glucose-6-P
Phosphofructokinase I Fructose-2,6-bisP
ADP, AMP
Pi
ATPCitrate
Fatty AcidsPEP
GlucagonPyruvate Kinase Fructose-
1,6-bisP (fructose-2,6-bisP)
ATP, NADHAlanine
Fatty acidsSuccinylCoA
Inactive when phosphorylated
High carb & insulin
Glucokinase High BGL
High carb & insulin

Intermediate Can be used for:Glucose-6-phosphate Glycogen, polysaccharides, glycoproteins,
pentoses, NADPHFructose-6-phosphate &
glyceradldehyde-3-phosphatePentoses
Dihydroxyacetone-phosphate Glycerol phosphate à phosphatidic acid à neural fat & phospholipids
3-phosphoglycerate Serine1,3-bisphosphoglycerate 2,3-bisphosphoglycerate (BPG)
Pyruvate Amino Acids (Alanine)Acetyl CoA à fatty acids, cholesterol,
steroid hormones
8. Tissue-Specific DifferencesCell/ Tissue Major ATP Source
Erythrocytes Glycolysis onlyHeart muscle, Brain Oxidative metabolism, under all conditions
Skeletal muscle Oxidative metabolism, at rest;both oxidative metabolism & glycolysis during exercise
a. RBCs lack mitochondria and depend entirely on anaerobic glycolysis for energy
i. Converts pyruvate to lactate which is transported to liver for resynthesis to glucose
1. Provides the cell with a mechanism for the oxidation of NADH (produced during the G3PDH reaction) to NAD+ which occurs during the LDH catalyzed reaction so glycolysis can continue
ii. Hemolytic anemia results from genetic enzyme defectsb. Skeletal muscle
i. Pyruvate formed enters mitochondria for oxidative metabolismii. During hard exercise, the rate of glycolysis in skeletal muscle increases greatly and more
pyruvate is produced than can be oxidized in mitochondria
iii. Pyruvate is converted to lactate, regenerating NAD+ in cytoplasm

and ATP for the working muscleiv. Lactate is transported to the liver for resynthesis
c. Cardiac muscle i. Lactate dehydrogenase is inhibited as pyruvate concentration
increases à inhibits conversion of pyruvate to lactate; helps direct pyruvate into oxidative metabolism
1. The electrons of cytoplasmic NADH are transferred to mitochondrial carriers of the oxidative phosphorylation pathway generating a continuous pool of cytoplasmic NAD+
Regulation of glycolysis in RBCEnzyme Stimulating Regulator (indicative of low energy state)
Hexokinase Low G6PPhosphofructokinase I Low ATP
High AMPPyruvate kinase High F-1,6-BP
16. OTHER SUGARS (FRUCTOSE, MANNOSE & GALACTOSE) & ALCOHOL
a. Sorbitol: can interconvert fructose & glucosei. Aldol reductase
1. Input: glucose + NADPH2. Product: Sorbitol + NADP
ii. Sorbitol dehydrogenase 1. Input: sorbitol + NADP
2. Product: fructose + NADPH
b. Fructose:i. Fructokinase
1. Input: fructose + ATP2. Product: fructose-1-phosphate
a. Hexokinase can act on fructose to make fructose-6-phosphate but normally the enzyme has a much higher affinity for glucose
3. Essential fructosuria a. Deficient fructokinase b. Fructose levels elevated in blood & fructose appears in urinec. Hexokinases can phosphorylate fructose when the
concentrations get too high (back up system)d. Not associated with clinical abnormalities because there is no accumulation of F1P

or ATP depletion
ii. Aldolase type B : cleaves F1P (and also F-1,6-bP) into two trioses1. One is phosphorylated (dihydroxyacetone-phosphate)
a. Triosephosphate isomerse : DHAP à G3P à glycolysis2. Glyceraldehyde kinase : glyceraldehyde à G3P à glycolysis3. Hereditary Fructose Intolerance
a. Aldolase B deficiency i. Sensitivity to dietary fructose, sucrose, sorbitol
1. eating a large bowl of fructose can give temporary symptoms
ii. Accumulate fructose-1-phosphate à prevent glycogen breakdown & glucose synthesis
iii. Major medical problem; Sweating, trembling, dizziness, nausea, coma; Infants: abdominal distension, poor growth, liver enlargement
iv. Does not affect aldolase A or C
c. Toxicity of fructose-1-phosphatei. Accumulation is associated with depletion of ATP and Pi
ii. Changes in blood concentrations of metabolites1. Fall in glucose: F1P inhibits release of glucose from glycogen2. Fall in free phosphorus: Pi is used in re-synthesis of ATP; phosphorus
becomes trapped in F1P3. Rise in uric acid : from increased synthesis & breakdown of purine
nucleotides
d. Mannose:i. Hexokinase
1. Input: Mannose2. Product: Mannose-6-phosphate
ii. Phosphomannose isomerase 1. Input: Mannose-6-phosphate2. Product: fructose-6-phosphate à glycolysis
e. Galactose: (lactose = glucose + galactose)i. (1 st ) Galactokinase
1. Input: galactose2. Product: galactose-1-phosphate
a. Cell must make Uridine diphosphoglucose to use this3. Galactokinase Deficiency
1. High levels of blood galactose2. Some is reduced to galactitol (via aldol reductase) which can
lead to development of cataractsii. UDP-glucose pyrophosphorylase
1. Input: glucose-1-phosphate + uridine triphosphate (UTP) + Pi2. Product: uridine diphosphoglucose (UDP-glucose)
iii. (2 nd ) Galactose-1-phosphate uridyltransferase (UDP-Glc) a. Input: UDP-glucose + galactose-1-phosphateb. Product: UDP-galactose + glucose-1-phosphate
iv. Galactose-1-phosphate uridyltransferase deficiency

1. Classic Galactosemia ; Autosomal recessive2. Infant: cannot utilize galactose; must exclude from diet
a. galactose-1-phosphate accumulates; some is made into galactitol-1-phosphate à both toxic
b. Lack of growth, vomiting, dehydration, jaundice, eventually developmental retardation and cataracts
3. Can still synthesize galactose containing glycoproteins & glycolipids from glucose via UDP-glucose formation and epimerase activity to form UDP-galactose
GALIPUT : Gal actose 1 P hosphate U ridyl T ransferase .4. UDP-galactose-4-epimerase
a. Input: UDP-galactose + NAD+
b. Product: UDP-glucose + NADHc. Allows galactose and N-acetylgalactosamine containing
glycoproteins and glycolipids to be synthesized from glucose even when no galactose is provided in the diet
d. UDP-galactose-4-epimerase deficiency i. Rare, recessive
ii. High levels of blood galactose-1-phosphate
v. (3 rd ) Phosphoglucomutase 1. Input: glucose-1-phosphate2. Process: isomerization (~phosphoglycerate mutase reaction of
glycolysis)3. Product: glucose-6-phosphate à glycolysis
1. Alcohol Metabolismf. Oxidation of ethanol to acetaldehyde:
three different pathways:i. Cytosol
1. Alcohol dehydrogenase (ADH) &

NAD+
2. ADH has broad specificity3. There are 5 different ADH genes whose polymorphisms contribute to the ability of people to
oxidize ethyl alcoholii. Smooth ER
1. Microsomal ethanol oxidizing system (MEOS)2. Becomes important in high alcohol intake3. Alcohol can also interfere with cytochrome P450
iii. Peroxisomes1. Catalase
g. Acetaldehydei. Reacts with amino groups & proteins (cross-linking)
ii. Inhibits mitochondrial functions 1. Feedback loop: high acetaldehyde impairs mito function
leading to accumulation of more acetaldehydeiii. Aldehyde dehydrogenase (ALDH)
1. Input: acetaldehyde + NAD+
2. Product: acetate + NADH + H+ 3. Two forms of the enzyme; ALDH2 is most important & gene occurs in two
polymorphic formsa. Wild type: active enzymeb. Second form: inactive
i. Dominant allele; reduced ability to oxidize acetaldehyde à vasodilation, facial flushing
iv. AcetylCoA Synthetase 1. Input: acetate + ATP + CoA2. Product: acetylCoA + AMP + PPi3. Allows recovery of small amount of energy
h. Acidosisi. Excess acetate appears in the blood
ii. Deficiency of NAD+ leads to increased conversion of pyruvate to lactate by lactate dehydrogenase
i. Gluconeogenesisi. Demand for pyruvate reduces its availability for gluconeogenesis
ii. Ratio of NADH : NAD+ goes up; reduces amount of pyruvate; shut downs down gluconeogenesis
iii. Lack of gluconeogenesis combined with poor nutrition can lead to hypoglycemia
j. Triglycerides/ Fat production

i. Excess NADH supports production of glycerol-3-phosphate from dihydroxyacetone phosphate
ii. Depletion of NAD + impairs the ability to oxidize fatty acids iii. Results in increased triglycerides that can be either secreted into the
plasma or deposited into the liverk. Vitamin deficiency
i. Pyridoxine or folate deficiencies à hemoatologic problems; neurological problems
ii. Wernicke-Korsakoff syndrome (ataxia, mental disturbance, uncoordinated eye movements)
1. An alcoholic can present with these symptoms due to a thiamine deficiency
l. Poisonsi. Methanol (Moonshine)
1. Metabolized by same enzymes that metabolize ethanol2. Alcohol dehydrogenase activity on it produces formaldehyde and formic acid à
death3. Supplementing with ethanol can reverse condition
ii. Antifreeze1. Ethylene glycol is metabolized to glycoaldehyde by alcohol dehydrogenase
a. Then to glycolic acid by aldehyde dehydrogenase
b. Results in severe acidosis
17. OXIDATIVE METABOLISM - THE TRICARBOXYLIC ACID CYCLE
1. TCA: Mitochondria Matrixa. Inner membrane contains a carrier protein that allows pyruvate to enter the
matrix2. Citrate is exported from the mitochondria to allow fat synthesis & inhibit glycolysis
a. Acetyl-CoA is converted to citratei. There is no way to get acetyl-CoA directly out of mitochondria; must
convert to citrate first3. CAN cross mitochondrial membrane
a. Pyruvate; citrate; isocitrate; α-ketoglutarate; succinate; fumarate; malate; ATP, ADP, Pi
4. CAN NOT cross mitochondrial membrane a. Acetyl CoA; Oxaloacetate; NAD+, NADH

5. Pyruvate Dehydrogenase a. Substrate: Pyruvate (3C) + CoA + NAD+
b. Product: Acetyl(2C)-CoA + NADH + H+ + CO2
c. Regulation:i. Not reversible
ii. Inhibited by1. Acetyl CoA; NADH, ATP
a. Activates the kinase which phosphorylates pyruvate dehydrogenase into its INACTIVE form
b. Kinase: Phosphorylated = ACTIVE à PDH INACTIVE
c. Kinase Inhibited by products (pyruvate, NAD+, CoASH); dichloroacetate
iii. Activated by1. Insulin, Mg2+, Ca2+, pyruvate, NAD+, CoASH,
Dichloroacetatea. Phosphatase activated by Ca2
+ (in exercising muscle) & insulin (well-fed state) à means you want to do a lot of glycolysis & TCA cycle
b. Phosphatase: Dephosphosphorylated = ACTIVE à PDH ACTIVE

d. Pyruvate dehydrogenase i. Thiamine Pyrophosphate (TPP): coenzyme on E1
1. Derived from Vitamin B1 (thiamine)2. Bings pyruvate on thiazole ring; then CO2 is released, leaved 2 Carbons on the ring
3. Deficiency leads to confusion, irritability, weight loss, edema, heart failure: Wernicke’s Encepalopathy (Wernicke-Korsakoff), beri-beri (wet or dry)
ii. Lipoate : active arm on E21. Transfers acetyl group to CoA, and electrons to a coenzyme (FAD) on E3
2. Target for Trivalent arsenic (AsO2-) (arsenic poisoning)iii. FAD : Flavin Adenine Dinucleotide: Coenzyme on E3
1. Derived from Vitamin B2 (riboflavin) iv. Coenzyme A/ Acetyl Coenzyme Av. NAD+
e. Leigh’s Disease i. Deficiency in PDHii. Degeneration of CNS; Neurological affects: loss of head control, motor skills, seizures;
Lactic acidosis can lead to impairment of respiratory & kidney functioniii. Prognosis: poor
iv. Treatment: thiamine or Vitamin B1; high fat, low carb diet; oral sodium bicarbonate/citrate
1. Experimental protocols: using dichloroacetate (reduces inhibitory phosphorylation of PDH)
f. Succinate dehydrogenase and fumarase catalyze sequential steps in the TCA cycle. Homozygous mutations in either gene can result in severe neurological impairment. Germline heterozygous mutations of succinate dehydrogenase are
phaeochromocytoma and paraganglioma. Mutations in fumarase cause a predisposition to cutaneous and uterine leiomyomas, as well as to kidney cancers.
6. TCA Cycle : Generates reduced coenzymes (FADH2 & NADH) that can be treated by ox-phos to generate energy; also generate one GTP
a. Citrate synthase i. OAA + Acetyl CoA à citrate
ii. Irreversible; Regulatediii. Inhibited by: NADH; succinyl CoAiv. Rate increases as [OAA] & [Acetyl CoA] increase
b. Aconitase i. Citrate à isocitrateii. Although citrate appears to be a symmetrical molecule, its two ends are handled
asymmetrically because it can bind on only one way in the asymmetric binding site of the enzyme
c. Isocitrate dehydrogenase i. Isocitrate + NAD+ à α-ketoglutarate + NADH + H+ + CO2
d. α-ketoglutarate dehydrogenase i. α-ketoglutarate + NAD+ à Succinyl-CoA + NADH + H+
ii. Five coenzymes: TPP, lipoate, CoASH, FAH, NAD+
1. ~pyruvate dehydrogenaseiii. Inhibited by: NADH; ATP; succinyl CoAiv. Lipoate is the target of arsenic
e. Succinyl CoA synthetase i. Succinyl-CoA + GDP + Pi à Succinate + GTPii. Succinate is symmetrical

f. Succinic acid dehydrogenase i. Succinate + FAD à Fumarate + FADH2
ii. Inhibited by: OAAiii. Activated by: ATP; Pi; succinate
g. Fumarase i. Fumarate à L-Malate
h. Malate dehydrogenase i. L-Malate + NAD+ à Oxaloacetate (OAA) + NADH
Regulated Enzyme Activator (‘low energy state’) Inhibitor(‘high energy state’)
Citrate synthase NADHATP
Succinyl CoA

Isocitrate dehydrogenase Isocitrate (insulin regulation results in citrate buildup)
ADP, AMPNAD+
Ca++
NADHATP
α-ketoglutarate dehydrogenase
Ca++ NADHSuccinyl CoA
7. Reduced coenzymes come from:a. NADH : Pyruvate dehydrogenase; Isocitrate dehydrogenase; α-ketoglutarate
dehydrogenase; Malate dehydrogenaseb. FADH2 : Succinate dehydrogenase
8. GTP comes from: Succinyl-CoA synthase9. Anaplerotic pathways
a. Need to replenish the intermediatesi. Glutamate dehydrogenase: à α-ketoglutarate
ii. Malic enzyme: Pyruvate à Malateiii. PEP carboxykinase: PEP à OAAiv. Pyruvate carboxylase: Pyruvate à OAAv. Transminase: Amino acids à OAA
10. TCA Cycle Intermediate linksa. All intermediates except malate, isocitrate, and citrate
(M.I.C.) can be turned into amino acidsb. Acetyl CoA à fatty acids & steroid biosynthesisc. Citrate à fatty acids/ sterol synthesis (cytoplasm)d. α-ketoglutarate à glutamate à amino acid purinese. Succinyl-CoA à hemef. Malate à glucose synthesis (cytoplasm)g. Fumarate urea cycle (tyrosine & phenylalanine breakdown)
h. Oxaloacetate ài. OAA formed by pyruvate carboxylase
pyruvateii. à asparate à amino acid purines/ pyrimidines
iii. à Interconverted with malate & exported to cytoplasm to act as substrates for gluconeogenesis
1. Convert to malate à generate NADH in cytoplasm2. Or can convert to asparate

18. THE PENTOSE PHOSPHATE PATHWAY
1. Using G6P for the biosynthesis of pentoses or formation of NADPHa. Ribose-5-phosphate is needed for nucleotide synthesis.b. NADPH is need to reduce glutathione, to synthesize fatty acids, Nitrous Oxide, and steroids/sterols, to
detoxify (cytochrome P450)c. In most tissues 80-90% of glucose oxidation is by Glycolysis the rest 10-20% is by PPP
i. 5-10% of liver glucose metabolism; More in adipocytes
2. Two stages:a. Oxidation
i. Glucose-6-phosphate dehydrogenase 1. G6P + NADP+ à 6-phosphoglucono-δ-lactone + NADPH + H+
2. Committed step; rate limiting3. Coenzyme: NADP+
4. Activated by: Insulin5. Inhibited: Allosterically by NADPH (potent competitive inhibitor)
a. Has a lower Ki than Km of NADP+ when present at higher concentrations
b. As NADPH is depleted more NADP+ is formed
c. High NADP+ stimulates Glucose 6-P dehydrogenase and NADPH production
6. G6PDH deficiency a. Precipitation of hemoglobin occurs due to disulfide
bond formation between Hb moleculesb. Extremely common; May present with: Dark colored urine; Low RBC
count; RBC with inclusion bodies; Elevated reticulocyte count; Low

hemoglobin; Elevated serum bilirubin
c. Clinical disease is related to degree of defecti. Class I: <2% enzyme activity à very severe
ii. Class III (A-): 10-50% enzyme activity à modest1. Patient with 10% of normal activity have enough to
generate NADPH under normal conditions.ii. Lactonase
1. 6-phosphoglucono-δ-lactone + H2Oà 6-phosphogluconate
iii. 6-phosphogluconate dehydrogenase 1. 6-phosphogluconate + NADP+ à Ribulose-5-P + NADPH2. 2nd formation of NADPH molecule
b. Isomerization & Epimerization i. Ribulose-5-Isomerase (“phosphopentose isomerase”)
1. Ribulose-5-P à Ribose-5-Pii. Ribulose-5-Epimerase (“phosphopentose epimerase”)
1. Ribulose-5-P à Xylulose-5-P
3. Transketolase a. Xylulose-5-P à Ribose-5-Pb. Transfers 2 Carbon Units Using
Thiamine (TPP)c. Wernicke-Korsakoff Syndrome
4. Transaldolase a. Transfers 3 carbon units
5. Four Modes of the PP Pathway:a. Balanced need for NADPH and R5P b. Need R5P (more than NADPH)
i. Rapidly dividing cellsc. Much more NADPH than R5P is needed
i. Synthesis of fatty acids in adipose tissued. Both NADPH and ATP are required; R5P can be converted to pyruvate which can be oxidized to

generate more ATPi. Biosynthesis
6. Net result: Oxidation of G6P, a 6 carbon sugar, into a 5 carbon sugari. In turn, 3 moles of 5 carbon sugar are converted back into two moles of 6 carbon sugars and
one mole of 3 carbon sugar
1. The 6 carbon sugars can be recycled into the pathway in the form of G6P, generating more NADPH.
2. The 3 carbon sugar generated is glyceraldehyde-3-phsphate which can be shunted to glycolysis and oxidized to pyruvate .
a. Alternatively, it can be utilized by the gluconeogenic enzymes to generate more 6 carbon sugars (fructose-6-phosphate or glucose-6-phosphate).
7. Cells have a high NADPH versus NAD+ (opposite of NAD & NADH); Two oxidation-reduction systems exist side by side with opposite polarities; both systems utilize the same active site
a. NAD+ : coenzyme of oxidation in mitochondria & nucleusi. Gets reduced to NADH
ii. Glycolysis oxidation reactions (usually have with dehydrogenase enzyme reactions)
iii. Want cell to have high NAD and low NADHb. NAPH : coenzyme of reduction in cytosol
i. Gets oxidized to NADPii. Making fat (unsaturated to saturated double bone)
iii. Want high NADPH, low NADP (would drive reactions the opposite way)

8. Oxidative Damagea. superoxide dismutase converts superoxide to hydrogen peroxideb. Glutathione (GSH) is required for reduction of peroxides by peroxidase
(selenium containing enzyme) i. Also responsible for maintaining the intracellular environment in a reduced state so that
disulfide bonds in proteins stay reduced
c. NADPH produced by glucose-6-P dehydrogenase maintains the supply of reduced glutathione needed to destroy peroxide by regenerating the reduced form of GSH
d. Defect means you cant detoxify peroxide and damages RBCsi. RBCs are more dependent on G6PDH than other cells that have alternative pathways to
produce NADPH, such as malic enzyme
19. GLUCONEOGENESIS
1. Liver provides 80-90% of glucose; two sources:a. Glycogen breakdown
i. Sustains BGL for a few hours after a mealb. Gluconeogenesis
i. Sustains BGL for many days in absence of carbohydrate intake2. Kidneys produce 10-20%, but more on fasting
3. Use 2 pyruvate, 4 ATP, 2 GTP, 2 NADH à get ONE molecule of glucose4. Substrates:
a. Lactate (via oxidation of pyruvate)b. Amino acids/ Alanine (via pyruvate, TCA intermediates)c. Glycerol (via glycolysis intermediates; use glycerol backbone of triglycerides
to make glucose) i. Glycerol enters the pathway much later down (at level of DHAP) versus
lactate/ pyruvate à inhibition of earlier enzymes don’t affect as severely
5. Gluconeogenesis goes through multiple (three different) cellular compartmentsa. Mitochondria à cytoplasm à ERb. G6P (end product) is hydrolyzed in ER
i. Hexokinase and glucose-6-phosphatase are localized differently
c. OAA needs a transporter to get out of mitochondriai. Conversion to PEP (through the action of the mitochondrial PEPCK)
ii. Transamination to aspartateiii. Reduction to malate
1. Requires use of an NADH (will be accumulating in the mitochondrion as

the energy charge increase); gets regenerated in cytoplasm when converted back to OAA
6. The four steps that occur in gluconeogenesis but not in glycolysis
a. Pyruvate Carboxylase i. Pyruvate + ATP + CO2-Biotin-Enzyme à OAA ii. Carboxylases add HCO3
- (i.e. CO2) to substrate
iii. Coenzyme: Biotin1. Biotin problems:
a. Tremendous injection of egg white (abatin binds biotin)b. Biotinidase deficiency : Biotinidase recovers biotin from proteins being
degraded
b. PEP Carboxykinase (PEPCK)i. OAA + GTP à P-enolpyruvate (PEP) + CO2 + GTP
ii. Cofactor: GTPiii. Can occur in either cytosol or mitochondriaiv. Regulated by glucocorticoids such as cortisol
c. Fructose-1,6-Bisphosphatase i. F-1,6-BP à F6P
ii. Activated by: Citrateiii. Inhibited by: AMP; F-2,6-BP (low energy levels)iv. *Regulation is the opposite of PFK1
d. Glucose-6-Phosphatase
e. Regulation

i. PFK2: enzyme that synthesized F2,6BP which is a potent activator of glycolysis (PFK1) & inhibitor of gluconeogensis (FBPase)
ii. Insulin promotes the dephosphorylationà Stimulates phosphataseiii. Glucagon stimulates cyclic AMP & phosphorylation of PFK2 àF2,6BP hydrolyzed to
F6P1. Glycolysis decreases/ Gluconeogenesis increases (Fbase not inhibited)
7. Glucagon a. Liver: Stimulates gluconeogenesis and glycogenolysisb. No effect on muscle (no receptor)
8. Insulin a. Muscle: stimulates glucose uptakeb. Liver: Stimulates glycogenesis
Metabolic Actions of Insulin and Glucagon
Fatty acid uptake and release in fat.
InsulinStimulates synthesis of triglycerides (TG) from free fatty acids (FFA); inhibits
release of FFA from TG.
Glucagon Stimulates release of FFA from TG.
Liver glycogen
Insulin Increases synthesis and thereby glucose uptake and storage.
Glucagon Stimulates glycogenolysis and glucose release.
Liver gluconeogenesis
Insulin Inhibits, saves amino acids.
Glucagon Stimulates, glucose synthesized and released.
Glucose uptake, skeletal muscle
Insulin Stimulates uptake, storage as glycogen and use in energy metabolism.
Glucagon No receptors, no effect.
Glycogen, skeletal muscle Insulin Stimulates synthesis.
Glucagon No receptors, no effect.

Amino acid uptake Insulin Stimulates and is necessary for protein synthesis.
Glucagon No receptors, no effect.
Brain (hypothalamus) Insulin Reduces hunger through hypothalamic regulation.
Glucagon No effect.
9. Cori Cycle a. RBC or Muscle: Glucose àLactate put into circulation and travels to liver
where it is made into glucose and put back into circulation to be used in RBC & muscle cell
b. Is an energy loosing deali. Get 2 ATP in muscle and costs 6 ATP
in liver
10. Cahill Cycle a. Muscle: Conversion of pyruvate to alanineb. Converted back to pyruvate and then to glucose
in liver11. Oxidizing alcohol generates excess NADH, depriving liver of gluconeogenic
substratesa. Production of NADH by alcohol metabolism blocks gluconeogenesis by
converting pyruvate back to OAA rather than lactate; also blocks conversion of malate
20. GLYCOGEN METABOLISM
1. Glycogen metabolism is a story of muscle and liver:a. Muscle (up to ~400g) uses glycogen for its own
energy (lacks glucose-6-phosphatase)b. Liver (up to ~100g) exports glucose to the system
(brain). 2. Short term fix; rapid metabolism
a. Amount of glycogen stored is limited b. Long term is gluconeogenesis & fat burning
3. Glucose-6-phosphate a. Stimulates glycogen synthesis & decreases breakdown
4. Fructose-1-phosphate a. Inhibits glycogen breakdown.

5. Insulin leads to a decrease in BGLa. Stimulates glycogen synthase b. Decreases phosphorylase activities
6. Glucagon & epinephrine a. Promote glycogen breakdown and inhibit synthesis.
7. Neuromuscular stimulation a. Activates phosphorylase kinase via acetylcholine receptor and Ca++ to promote
breakdown.
8. Breakdown of Glycogen: a. Glycogen phosphorylase cleaves one glucose residue at a time by
phosphorolysis from the end of the chain. i. This is the regulated step (McArdle’s Disease).
ii. Product is glucose-1-phosphateb. Debranching enzyme transfers three residues of a branching chain to a
different chain and then cleaves the remaining glucose by hydrolysis. i. Product is free glucose
c. Ratio of 12:1 of G1P : free glucosed. Glycogen phosphorylase two distinct conformational states: a T (for tense,
less active) and R (for relaxed, more active) state; i. Low BGL à glucagon à Phosphorylate Glycogen
phosphorylase-a (R/ active state) à MORE ACTIVE à Breakdown Glycogen
1. Also enhanced by binding of AMP2. Inhibited by ATP; G6P; Insulin
9. Synthesis of Glycogen:a. Glycogen synthase elongates the chain by one glucose residue at a time from
UDPglucose to the 4’OH of a glucose at the end of the chaini. Requires a primer which can be made by glycogenin
ii. This is the regulated stepb. Branching Enzyme transfers a terminal segment of growing chain to form a
branch linked a1-6 to a different chain.i. Synthesis slows down as the particle gets bigger; the amount of glycogen we store is limited
c. Glycogen synthase

i. High BGL à Insulin à activate protein phosphatate à Dephosphorylate Glycogen synthase à MORE ACTIVE à Synthesize Glycogen
ii. Low BGL à glucagon à activate protein kinase à Phosphorylate Glycogen synthase à Less active
10. Glycogen Storage Diseases
Enzyme Location Glycogen Features Presentation Treatment
Type IVon
Gierke
Glucose-6-Phosphatase LiverKidney
Increased amountNormal structure
Severe hypoglycemiaHepatomegaly
Lactic acidosisHypoglycemiaHyperuricemiaHyperlipidemia
Constant Glucose infusion
Type IIPompe
α-1,4 glucosidase (lysosomal)
Everywhere Large increaseNormal structure
Cardiorespiratory Failure
HepatomegalyHypotonia Muscular weakness
Enzyme replacement
therapy
Type IIICori
Debranching Enzyme MuscleLiver
Increased amount
Similar to but milder than Type I Heptomegaly
High CarbHigh Protein

Short outer
branches
(enlarged liver)Hypoglycemia, Hyperlipidemia
Short statureType IVAndersons
Branching Enzyme Liver Normal amountLong outer
branches
HepatomegalyFatal
Type VMcArdle
Phosphorylase Muscle Increased amountNormal structure
Exercise problemsCramps
Burgundy colored urine
Type VIHers
Phosphorylase Liver Increased amountNormal structure
Similar to but milder than Type I
Hypoglycemia, Hepatomegaly Lactic acidosis
Carb Supplements
Type VIITauri’s
Phosphofructokinase1 Muscle Increased amountNormal structure
Like Type VExercise
intolerance
Muscle cramps Blood lactate not elevated hemolytic
anemia
Andersons is only disease of glycogen synthesis
Glycogen storage: names of types I through VI"V iagra P ills C ause A M ajor H ardon ":
Von Gierke'sPompe's
Cori'sAnderson'sMcArdle's
Her's
Very Poor Carbohydrate Metabolism (V,P,C,M) of Hers (H) HEpatic glycogen phosphorylase deficiency
ABCD:Anderson's=Branching enzyme.
Cori's=Debranching enzyme.
Pompe's disease: type "Police = Po + lys":lysosomal storage disease (alpha 1,4 glucosidase)
11. Glucose-6-Phosphatase deficiency (glycogen storage disease type I)a. Blood sugar concentration
i. [BGL] low à G6P cant convert to free glucose to be releasedb. Rate of glycolysis
i. High rate of glycolysis due to high [G1P] from glycogen breakdown

c. Rate of glycogen synthesisi. Decreased
d. Source of free blood glucosei. Break down glycogenà
1. Release free glucose2. Rest of G1P (10:1) goes through glycolysis
e. Rate of pentose synthesisi. Increase [G6P] à Increase PPS
ii. Breaking down nucleotides à increase uric acid in blood1. High level of glycolysis & lactic acid
f. Accumulation of lipids in liver and bloodi. NADPH & substrates (DHAP, citrate, acetyl-CoA, G6P) are still
available for FA synthesisg. Development of gout and approaches to control of the consequences of the
diseasei. Constant supply of glucose