Benjamin S. Brooke, MD
19
Implementing the Leapfrog Standard for β-Blocker Use during AAA Repair in California Hospitals: Translation of Evidence-Based Process Measures to Improve Surgical Outcomes Benjamin S. Brooke, MD Francisca Dominici, PhD; Martin A. Makary, MD MPH; Bruce A. Perler, MD; & Peter J. Pronovost, MD PhD Johns Hopkins School of Medicine and Bloomberg School of Public Health, Baltimore, MD AcademyHealth Annual Research Meeting, June 10, 2008
description
Implementing the Leapfrog Standard for β -Blocker Use during AAA Repair in California Hospitals: Translation of Evidence-Based Process Measures to Improve Surgical Outcomes. Benjamin S. Brooke, MD - PowerPoint PPT Presentation
Transcript of Benjamin S. Brooke, MD

Implementing the Leapfrog Standard for β-Blocker Use during AAA Repair in California Hospitals: Translation of
Evidence-Based Process Measures to Improve Surgical Outcomes
Benjamin S. Brooke, MD
Francisca Dominici, PhD; Martin A. Makary, MD MPH; Bruce A. Perler, MD; & Peter J. Pronovost, MD PhD
Johns Hopkins School of Medicine and Bloomberg School of Public Health, Baltimore, MD
AcademyHealth Annual Research Meeting, June 10, 2008

Translation of Leapfrog Group Evidence-Based Standards
• Purpose• Scope• Implementation• Evaluation• Results• Dissemination • Lessons Learned• Next Steps

Leapfrog Group Hospital Quality & Patient Safety Initiative
Purpose
• Founded in 2000 by consortium of large public and private health care purchasers
• Establish and promote evidence-based standards (“leaps”)– Computerized Physician Order Entry (CPOE)– 24-Hour ICU Physician Staffing– Evidence-Based Hospital Referral (EBHR)
standards for 5 High Risk Operations

Abdominal Aortic Aneurysm (AAA) Repair
• AAA prevalent in 3-9% of U.S. population over the age of 65.
• More than 40,000 prophylactic AAA repairs undertaken each year to prevent rupture & sudden death from occurring.
• 30-day mortality for elective open AAA repair ranges between 4-6%.

Leapfrog Evidence-Based Standards for AAA Repair
1. Hospital AAA Case Volume• Established in 2000 • Minimum of 50 elective cases per year• Supported by observational cohort studies
2. Routine Perioperative Beta-blocker Use• Established in 2003 80% of patients need to be on therapy
during hospitalization & at discharge• Supported by randomized controlled trials

The Leapfrog Group InitiativeScope
• Nationwide - regional “rollout waves”
• Metropolitan and State-wide “lily pads”
• Annual Leapfrog Group Hospital Quality & Patient Safety Survey
• First survey: June 2001 – Atlanta, Tennessee, Minnesota, Seattle, St.
Louis, California
• 1,300 U.S. hospitals participating to date

California
• 337 urban & suburban hospitals targeted
• Diverse/representative patient populations
• California Office of Statewide Health Planning & Development (OSHPD) Discharge Database

Translating Leapfrog Standards into Hospital Policy
Implementation
• Incentives/Rewards:– Public Recognition– Different Financial Incentives– Improvements in Clinical Outcomes– Reduce Health Care Costs
• Potential Barriers– Infrastructure Requirements – Capital Investment – Change in Hospital Culture– Controversial Standards

Implementing Routine β-blocker Use During AAA Repair
• Advantages of Process Measure– Widely used medication in clinical practice– Target population are good candidates– Limited side effects and risks– Inexpensive
• Limitations of Process Measure– Some patients may not tolerate therapy– Requires titration for maximal benefit– Patients may require extra monitoring

Hospital Compliance with Leapfrog β-blocker Standard
Evaluation
• 212 California hospitals returned Leapfrog
Group surveys (63% response rate)
• 140 California hospitals performed elective
AAA repairs – 37 (26%) Met Leapfrog β-blocker Standard– 103 (74%) Did Not Meet β-blocker Standard

Evaluating the Impact of Adopting β-blocker Policy
• Survey response data linked to the
OSHPD patient discharge database
• In-hospital mortality compared over 2
periods:– 2000-2002: Pre β-blocker– 2003-2005: Post β-blocker
• Poisson regression rate ratio estimates
for in-hospital mortality

Hospital CharacteristicsResults
Hospitals without β-Blocker Policy (n=103)
Hospitals with β-Blocker Policy (n=37)
Characteristics 2000-2002 2003-2005 2000-2002 2003-2005
Total Admissions, mean (±SD) 15.4 (7.3) 14.0 (6.6) 14.6 (7.3) 14.3 (8.0)
ICU Admissions, mean (±SD) 1.8 (1.7) 1.7 (2.1) 2.1 (2.0) 1.8 (1.6)
Floor Beds, mean (±SD) 216 (120) 231 (103) 205 (147) 254 (150)
ICU Beds, mean (±SD) 26.7 (18.6) 25.7 (14.6) 28.5 (27.8) 30.6 (27.1)
AAA volume, mean (±SD) 23.7 (21.3) 26.7 (31.1) 20.5 (18.3) 24.8 (24.7)
ACGME Surg. Training, % 12 12 14 14
Health System Member, % 81 83 82 84
* Admissions reported in units of thousands

Characteristics of PatientsHospitals without β-blocker (n=6,403 pts)
Hospitals with β-blocker Policy (n=2,167 pts)
Pt. Characteristics 2000-2002 2003-2005 2000-2002 2003-2005Men, % 79 79 80 77Age, % 35-64 65
1783
1783
1585
1783
Race, % White Black Asian
8924
8924
8834
8636
Insurance, % Medicare/Medicaid Private Insurance
7722
7920
8019
8018
Charlson Index, % 1 2 3
423424
38 *3328
433225
36 *
3628
* P<0.05 for comparison within groups over time

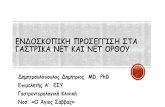
Mean In-Hospital Death Rate
0
1
2
3
4
5
6
1998-99 2000-01 2002-03 2004-05
Hospitals withoutBeta-blockerPolicyHospitals withBeta-blockerPolicy
Mea
n D
eath
s P
er 1
00 A
AA
Rep
airs
Years
Source: California OSHPD dataset between years 1998 to 2005

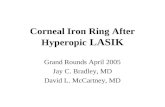
Poisson Regression Rate Ratio Estimates for In-Hospital Mortality
Ratio of Rate Ratios
Hospitals RRR (95% CI) P-value
Hospitals without β-Blocker (n=103) 1.00 (Reference)
Hospitals with β-Blocker Policy (n=37)
Random Effects Unadjusted 0.69 (0.42 to 1.45) 0.153
Random Effects Adjusted * 0.50 (0.26 to 0.96) 0.038
Fixed Effects Unadjusted 0.67 (0.40 to 1.12) 0.129
Fixed Effects Adjusted * 0.43 (0.20 to 0.92) 0.030
* Adjusted for race, insurance, gender, age, Charlson index, AAA volume & ICU admissions.

Bridging the Gap in TranslationDissemination
• Leapfrog Group Strategy– Centers of Excellence– Pay for Participation – Pay for Performance
• Regional Collaboratives– Regional networks of hospitals with
robust evaluation of compliance & outcomes
– e.g. Michigan Keystone initiative

β-blocker Use in California Hospitals Lessons Learned
• Hospitals may achieve significant improvements in patient outcomes by adopting a single evidence-based measure
• There is still low overall compliance with adopting process measures
• More efforts are needed to optimize the compliance and dissemination of proven evidence-based practices

Translation of Leapfrog Evidence-Based Standards
Next Steps
• CMS MEDPAR dataset
• Evaluate Impact of Hospital Compliance
with Other Leapfrog Standards
• Identify other Evidence-Based Process
Measures

Acknowledgments
• Aidan McDermott– JHSPH Dept of Biostatistics
• Sarah Collins – Leapfrog Group
• Dennis Bush– Thompson Healthcare