Asian HCV With PegIntron
80
Treating hepatitis C virus (HCV) with pegylated interferon (pegIFN) α-2b Overview of efficacy and safety data for pegIFN α-2b, including Asian data
Transcript of Asian HCV With PegIntron

Treating hepatitis C virus (HCV) with pegylated interferon (pegIFN) α-2b
Overview of efficacy and safety data forpegIFN α-2b, including Asian data

Outline
• Epidemiology and disease burden• Definitions of HCV treatment responses• Evolution of HCV treatment and current guidelines• Treatment outcomes with pegIFN α plus ribavirin (RBV)• Durability of response • Predictors of treatment success• Evidence supporting response-guided therapy
– HCV-1: RVR and EVR are important predictors of SVR– HCV-2/3: RVR is an important predictor of SVR
• Adverse events• Difficult-to-treat HCV populations

Epidemiology and disease burden

Global incidence of hepatitis C
1. Sy T et al. Int J Med Sci. 2006;3:41-46; 2. Ghany MG et al. Hepatology. 2009;49:1335-1374.
31.9
13.1
21.3
8.9
32.3
62.2
0
10
20
30
40
50
60
70
Africa Americas Eastern Mediterranean
Europe Southeast Asia
Western Pacific
Pa
tie
nts
(M
illi
on
s)
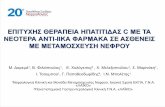
• World Health Organization (WHO) estimates that ~180 million people are infected with hepatitis C worldwide2
Estimated hepatitis C infections, by region1

Prevalence of HCV in Asia Pacific
Sievert W, et al. Liver Int 2011;31 Suppl 2:61-80.

HCV genotype distribution by country in Asia Pacific
Sievert W, et al. Liver Int 2011;31 Suppl 2:61-80.

Burden and impact of HCV• Approximately 55–85% of newly infected HCV cases progress to
chronic HCV (CHC).1
• Of those, 20–30% will develop liver fibrosis, cirrhosis, and liver failure, and 2–5% will progress to HCC.1
• In the WHO EU region (2002):2
– HCV caused more than 86,000 deaths, accounting for 35% of cirrhosis and 32% of liver cancer deaths.
• In the US:1,3
– HCV-related mortality (death from liver failure or HCC) has risen from 3,700 in 1998 and is expected to peak at 13,000 in 2030.
– HCV-related mortality is currently 8,000–10,000 annually.
• In Southeast Asia:4
– HCV caused 14,000 deaths in 2002.
1. El-Kamary SS, et al. Clin Infect Dis 2011;53:150-157; 2. Muhlberger N, et al. BMC Public Health 2009;9:34; 3. Deuffic-Burban, S, et al. J Viral Hepat. 2007;14:107-115; 4. WHO global burden of disease, 2004 update. Available at: http://www.who.int/healthinfo/global_burden_disease/ GBD_report_2004update_full.pdf; accessed November 2011.

Clinical outcomes of HCV: Risk of mortality and HCC increase if HCV is not cured
7918 815 6974248 2089 1097
1. El-Kamary SS, et al. Clin Infect Dis 2011;53:150-157; 2. Cardoso AC, et al. J Hepatol 2010;52:652-657; 3. Backus LI, et al. Clin Gastroenterol Hepatol 2011;9:509-516.
221
HCC and liver-related mortality1,2 5-year mortality3
HCV Ab-negative chronic HCV infection SVR No SVR
General population
Ab, antibody; SVR, sustained virologic response

Definitions of HCV treatment responses

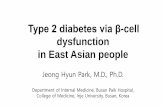
Types of virologic responses to HCV treatment
SVR(24 wk post Tx)
RVR(4 wk)
0
2
4
6
8
EVR(12 wk)
2 log10 decline
Limit of detection
Weeks
0 4 12 24 36 48 72
Vir
al l
oad
: H
CV
RN
A (
log
10 I
U/m
L)
Relapse
cEVR
pegIFN, peginterferon; RBV, ribavirin; RVR, rapid virological response; EVR, early virological response; cEVR, complete early virologic response; SVR, sustained virological response; ETR, end of treatment response; Tx, treatment.
Null response
pEVR
ETR
Treatment: PegIFN α/RBV
Slow response

Evolution of HCV treatment and current guidelines

Progressive improvement in treatment outcomes for chronic HCV-1
1. McHutchison JG, et al. N Engl J Med 1998;339:1485-1492; 2. Poynard T, et al. Lancet 1998;352:1426-1432; 3. Manns MP, et al. Lancet 2001;358:958-965; 4. Lindsay KL, et al. Hepatology 2001;34:395-403; 5. Fried MW, et al. N Engl J Med 2002;347:975-982; 6. McHutchison JG, et al. N Engl J Med 2009;361:580-593; 7. Kwo PY, et al. Lancet 2010;376:705-716; 8. Bacon BR, et al. N Engl J Med 2011;364:1207-1217.
1990–1997 1998–2009 2010–2011
IFN48 Weeks7–11%1,2
IFN/RBV48 Weeks28–37%1,2
PegIFN-α 2b/RBV
48 Weeks~40%3-6
PegIFN-α 2b/RBV/BOCTx-naive
~63–66%7,8
PegIFN-α 2b/RBV/BOCTx-failure~59–66%9
SV
R r
ate
(%
)
IFN, interferon; RBV, ribavirin; BOC, boceprevir; Tx, treatment.

Progress in HCV treatment outcomes in Asia by genotype
Yu ML and Chuang WL. J Gastroenterol Hepatol 2009;24:336-345.
SVR, sustained virological response; IFN, interferon; MU, million units; wks, weeks; RBV, ribavirin; Peg, peginterferon; RVR + ve, subgroup of patients who achieved a rapid virological response, defined as PCR-seronegative for HCV RNA after 4 weeks of therapy.
20091990

EASL recommendations on goals and endpoints of HCV treatment
• PegIFN α plus RBV is the current standard of care.• The goal of therapy is to eradicate HCV infection (A1).• The endpoint of therapy is SVR (A1).
– Once obtained, SVR equates to cure of infection in > 99% of patients.
• Intermediate endpoints to assess the likelihood of an SVR are HCV RNA levels at 4, 12, and 24 weeks of therapy (B2).
• In treatment-naïve patients, strongest baseline predictors of SVR are:– HCV genotype (A1).– Genetic polymorphisms located in chromosome 19
(IL28B), particularly in genotype 1 patients (A1).– Stage of liver fibrosis (A1).
EASL Clinical Practice Guidelines. J Hepatol 2011;55:245-264.
EASL: European Association for the Study of the Liver; RBV, ribavirin

EASL guidelines 2011: Response-guided therapy with pegIFN α/RBV for HCV-1†
EASL Clinical Practice Guidelines. J Hepatol 2011;55:245-264.
EASL: European Association for the Study of the Liver† applies also to HCV genotype 4

EASL guidelines 2011: Response-guided therapy with pegIFN α/RBV for HCV-2/3†
EASL: European Association for the Study of the Liver† applies also to genotypes 5 and 6, excluding 12–16 weeks
* Marginally less effective due to higher relapse rates, especially for G3 with high viral load.
EASL Clinical Practice Guidelines. J Hepatol 2011;55:245-264.

AASLD practice guidelines
• HCV-1:– Optimal therapy for treatment-naïve patients and
treatment failure is boceprevir or telaprevir combined with pegIFN α and weight-based RBV (Class 1, Level A).1
• HCV-4: – Treatment with pegIFN α plus weight-based RBV (800–
1,400 mg) for 48 weeks (Class I, Level A).1,2
• HCV-2/3: – Treatment with pegIFN α plus RBV for 24 weeks, using a
RBV dose of 800 mg (Class I, Level A). 2
1. Ghany MG, et al. Hepatology 2011;54:1433-1444; 2. Ghany MG, et al. Hepatology 2009;49:1335-1374.
AASLD, American Association for the Study of Liver Diseases

Treatment outcomes with pegIFN α/RBV in CHC

0
10
20
30
40
50
60
70
SVR in HCV-1 patients: 2001–2010
*SVR of non-Hispanic white patient cohort with 98% of them having genotype 1.†99% of patients had HCV-1. ‡Estimated SVR analysis: intended to account for patients with undetectable HCV RNA at the end of treatment and who lacked follow-up data and were considered nonresponders in the primary analysis. SVR, sustained virologic response, i.e. negative HCV RNA 24 weeks after completion of therapy. Yenice N, et al. Turk J Gastroenterol. 2006;17:94-98; Muir AJ, et al. N Engl J Med. 2004;350:2265-2271; Lee S, et al. Intervirology. 2010;53:146-153; Cozzolongo R, et al. Abstract presented at: 41st Annual EASL; April 26-30, 2006; Vienna, Austria. No. 563; Ascione A, et al. Gastroenterology. 2010;138:116-122; Rumi MG et al. Gastroenterology. 2010;138:108-115; Almasio PL et al. Poster presented at: 56th Annual AASLD; November 11-15, 2005; San Francisco, CA. No. LB03; Manns MP, et al. Lancet. 2001;358:958-965; Witthoeft T, et al. J Viral Hepat. 2010;17:459-468; McHutchison JG, et al. N Engl J Med. 2009;361:580-593; Cooper C, et al. Poster presented at: 60th Annual AASLD; October 30-November 3, 2009; Boston, MA. No. 820; Jacobson IM, et al. Hepatology. 2007;46:971-981.
PegIFN α-2b plus RBV
SV
R r
ate
(%)
35
63
52*
33
40†
32
49
423940
4439‡
Yenice2006
Lee2010
Ascione2010
Almasio2005
Cooper2009
Witthoeft2010
Muir2004
Cozzolongo2006
Rumi2010
Manns2001
McHutchison2009
Jacobson2007
37 100 16 52 93 87 338 348 951 1019 1161 1313
Smaller trials (< 1,000)
Larger trials (> 1,000)Korean study
N = 5,515

HCV-1: Consistent SVR in five largest Western trials
PegIFN α-2b plus RBV
SV
R r
ate
(%)
Manns2001
Jacobson2007
Cooper2009
McHutchison2009
Witthoeft2010
348 951 1019 1161 1313
42 4440 39 39*
*Estimated SVR analysis: intended to account for patients with undetectable HCV RNA at the end of treatment who lacked follow-up data and were considered non-responders in the primary analysis. †Patients treated with standard dose and schedule of PegIFN α-2b combination therapy. SVR, sustained virologic response, i.e. negative HCV RNA 24 weeks after completion of therapy.
Manns MP, et al. Lancet. 2001;358:958-965. Witthoeft T, et al. J Viral Hepat. 2010;17:459-468; McHutchison JG, et al. N Engl J Med. 2009;361:580-593; Cooper C, et al. Poster presented at: 60th Annual AASLD; October 30-November 3, 2009; Boston, MA. No. 820. 5. Jacobson IM, et al. Hepatology. 2007;46:971-981.
• These trials included 10,291 HCV-1 patients, of which 7,862 were treated with pegIFN α-2b plus RBV.
• Of these, 4,792 were treated with the standard dose and schedule of pegIFN α-2b (1.5 μg/ kg/wk for 48 weeks).
N = 4,792†

IDEAL study: PegIFN α-2b compared with pegIFN α-2a in HCV-1, treatment-naïve, US patients
N = 1,019 PegIFN -2b 1.5 µg/kg/wk
+ RBV 800–1,400 mg/d x 48 weeks
N=1,035PegIFN -2a 180 µg/wk
+ RBV 1000–1,200 mg/d x 48 weeks
N = 1,016 PegIFN -2b 1.0 µg/kg/wk
+ RBV 800–1,400 mg/d x 48 weeksScreeningScreeningScreeningScreening
Follow-up24 weeks
Follow-up24 weeks
Follow-up24 weeks
4 12 24 48 4 12 24
Stratified by baseline viral load (> or ≤ 600,000 IU/mL) and race (African American)
Standard response stop criteria applied at Weeks 12 (no EVR) and 24 (HCV-RNA +)
Sulkowski M et al. EASL 2008. Abstract 991; Oral Presentation. Available at: http://www.hcv.pl/galeria/popularnonaukowe/Sulkowski_IDEAL.pdf.
Weeks

Time course of response: Proportion of patients with undetectable HCV-RNA (ITT)
11
40
51 53
40
8
36
48 49
38
12
45
6264
41
0
20
40
60
80
TW4 TW12 TW24 EOT SVR
Pat
ien
ts w
ith
u
nd
etec
tab
le H
CV
RN
A (
%)
PegIFN α-2b 1.5 + RBVN = 1,019
PegIFN α-2b 1.0 + RBVN = 1,016
PegIFN α-2a 180 + RBVN = 1,035
Sulkowski M et al. EASL 2008. Abstract 991; Oral Presentation. Available at: http://www.hcv.pl/galeria/popularnonaukowe/Sulkowski_IDEAL.pdf.
ITT, intention-to-treat; TW, treatment week; EOT, end of treatment, SVR, sustained virologic response
P = 0.57

Rates of relapse with pegIFN α-2b vs. pegIFN α-2a
Almasio PL et al. Poster presented at: 56th Annual AASLD; November 11-15, 2005; San Francisco, CA. No. LB03; Cozzolongo R, et al. Abstract presented at: 41st Annual EASL; April 26-30, 2006; Vienna, Austria. No. 563; McHutchison JG, et al. N Engl J Med. 2009;361:580-593; Lee S, et al. Intervirology. 2010;53:146-153; Witthoeft T, et al. J Viral Hepat. 2010;17:459-468; Ascione A, et al. Gastroenterology. 2010;138:116-122; Rumi MG et al. Gastroenterology. 2010;138:108-115.
PegIFN α-2b PegIFN α-2a
Rat
e o
f re
lap
se (
%)

SVR in Asian studies of HCV-1 patients
133 65 21 107 38 70 4750
†
† Patients all achieved EVR and received 48 weeks' therapy
Chu CJ, et al. Aliment Pharmacol Ther 2009;29:46-54; Chu CJ, et al. Hepatogastroenterology 2007;54:866-870; Fung J, et al. J Infect Dis 2008;198:808-812; Hung CH, et al. Liver Int 2006;26:1079-1086; Lee SD, et al. J Viral Hepat 2005;12:283-291; Tsang OT, et al. J Gastroenterol Hepatol 2010;25:766-771; Kim MN, et al. Korean J Hepatol 2009;15:496-503, Lee S, et al. Intervirology 2010;53:146-153.
PegIFN α plus RBV

60
70
80
90
PegIFN α-2b plus RBV
SVR in Western studies of HCV-2/3 patients S
VR
rat
e (%
)
Manns20011
Zeuzem20042
Mangia20053
Jacobson20074
Manns20115
147 224 775 180
82 81
76
72†
82‡
283
†Estimated SVR analysis: intended to account for patients with undetectable HCV RNA at the end of treatment and who lacked follow-up data and were considered non-responders in the primary analysis. ‡Completers’ analysis, i.e. had both end-of-treatment and 24-week follow-up results.SVR, sustained virologic response, i.e. negative HCV RNA 24 weeks after completion of therapy.
1. Manns MP, et al. Lancet. 2001;358:958-965; 2. Zeuzem S, et al. J Hepatol. 2004;40:993-999; 3. Mangia A, et al. N Engl J Med. 2005;352:2609-2617; 4. Jacobson IM, et al. Hepatology. 2007;46:971-981; 5. Manns M, et al. J Hepatol 2011;55:554-563.
• Patients were treated with pegIFN α-2b (1.5 μg/kg/wk) plus RBV for 481 or 242–5 weeks.
• Patients with HCV-2/3 often respond more readily to pegIFN α-2b and RBV than do patients with HCV-1.

A: PegIFN α-2b 1.5/RBV (24 weeks)
B: PegIFN α-2b 1.0/RBV (24 weeks)
C: PegIFN α-2b 1.5/RBV (16 weeks)
REDD 2/3: Reduced dose and duration of pegIFN α-2b and weight-based RBV in European
and Asian HCV-2/3 patients
Manns M, et al. J Hepatol 2011;55:554-563.
Treatment differences (one-sided 95% CI): aGrp A – Grp B: -0.02 (-0.09); P = 0.024; bGrp A – Grp C: -0.14 (-0.21); P = 0.798. Non-inferiority not achieved for all patients and individual cohorts. Tx, treatment.
SVR in completers
13
6/1
67
13
9/1
74
12
1/1
79
56
/70
66
/82
48
/81
80
/97
73
/92
73
/98
82 80a
68b
80 81
59
83 7975
0
25
50
75
100
SV
R r
ate
(%)
All patients(N = 520)
HepNet cohort(N = 233)
International cohort (N = 287)
SVR in patients with RVR
A (24 weeks): 75.3%B (24 weeks): 75.9%C (16 weeks): 72.4%
In patients who achieved RVR, 16 weeks Tx may be considered, as SVR was similar to that with24 weeks Tx.

REDD 2/3: SVR by genotype
Manns M, et al. J Hepatol 2011;55:554-563.
78
6154
7367
73
5360
46
7570
64
0
25
50
75
100
HepNet cohort(N = 84)
Internationalcohort (N = 51)
HepNet cohort(N = 263)
Internationalcohort (N = 284)
SV
R r
ate
(%)
HCV-2 HCV-3
21
/27
19
/31
14
/26
8/1
1
12
/18
16
/22
47
/89
50
/84
41
/90
77
/10
3
63
/91
58
/90
A: PegIFN α-2b 1.5/RBV (24 weeks)
B: PegIFN α-2b 1.0/RBV (24 weeks)
C: PegIFN α-2b 1.5/RBV (16 weeks)

7670
6659 60
47
7468 66
0
25
50
75
100
Internationalcohort (N = 177)
HepNet cohort(N = 347)
Internationalcohort (N = 158)
REDD 2/3: SVR according to ethnicity
Asian Caucasian
SV
R r
ate
(%)
43
/57
41
/59
40
/61
69
/11
5
68
/11
6
55
/11
6
42
/57
34
/50
34
/51
Manns M, et al. J Hepatol 2011;55:554-563.
A: PegIFN α-2b 1.5/RBV (24 weeks)
B: PegIFN α-2b 1.0/RBV (24 weeks)
C: PegIFN α-2b 1.5/RBV (16 weeks)

SVR in Asian studies of non-HCV-1 genotype patients
65 21 242 7038
†
†
† HCV-6 only; ‡ 237/242 were HCV-2Chu CJ, et al. Hepatogastroenterology 2007;54:866-870; Fung J, et al. J Infect Dis 2008;198:808-812; Hung CH, et al. Liver Int 2006;26:1079-1086; Lee SD, et al. J Viral Hepat 2005;12:283-291; Tsang OT, et al. J Gastroenterol Hepatol 2010;25:766-771.
PegIFN α plus RBV
‡

Durability of response

Durability of SVR:Long-term follow-up data (5 years)
99% of patients who attained SVR maintained long-term viral clearance3
SVR after treatment with pegIFN α-2b ± RBV predicts
long-term clearance of HCV3
Phase 3b, multicenter, long-term, follow-up study of 567 patients previously treated for CHC in 2 large, international clinical trials.1, 2
Du
rab
ilit
y o
f S
VR
(%
)
100
95
90
85
80
604020
0
1. Manns MP et al. Lancet. 2001; 358:958-965; 2. Lindsay KL et al. Hepatology. 2001; 34:395-403; 3. Manns, M, et al. Presented at 43rd Annual Meeting of the European Association for the Study of the Liver, April 23-27, 2008, Milan, Italy.
Year

Durability of response to Peg IFN α-2b/RBV in children: 5-year follow-up
• Multicenter study of 97 pediatric patients (3–16 years) treated with pegIFN α-2b (3 MIU/m2) three times per week plus RBV (8–15 mg/kg/day) for 24 weeks, who were followed up for 5 years.
– Overall SVR was 58%: SVR in HCV-1: 47%; SVR in HCV-2/3: 95%).
– Only one patient had virologic relapse during long-term 5-year follow-up (98% durability of response).
• Mean height percentile (44th percentile) at the end of the long-term follow-up was slightly below the mean pre-treatment baseline height percentile (48th percentile).
Kelly DA, et al. J Viral Hepat 2011:doi:10.1111/j.1365-2893.2011.01544.x.

Predictors of treatment success

Predictors of treatment success
• Genotype• Viral load at
baseline
Viral factors
RVR, rapid virological response; EVR, early virological response; cEVR, complete early virological response
On-treatment responses
• RVR (Week 4)• EVR (Week 12)• cEVR
• Age• Ethnicity• Genomics• Immune status• Weight• Severity of liver
disease• Hepatic steatosis• Insulin resistance
Host factors

Patient IL28B SNP genotype confers a higher chance of achieving SVR
1. Thompson AJ, et al. Gastroenterology 2010;139:120-129; 2. Li S, et al. Hepat Mon. 2011;11:163-172 .
0
20
40
60
80
100
SV
R r
ate
(%
)
33
Caucasians
(N = 1,171)
African Americans(N = 300)
Hispanics
(N = 116)
27
69
1513
48
38
27
56
P < 0.0001
P < 0.0001 P = 0.02
• IL28B encodes IFN-λ3, and SNP found near this gene can predict SVR.
• Patients homozygous for the CC allele at SNP rs12979860 have the best chance of achieving SVR, compared to those with the TT or TC genotypes.1
• SNPs rs12979860 and rs8099917 can be used as independent predictors of Tx response.2
TT CT CC
SNP rs12979860
SNP, single nucleotide polymorphism

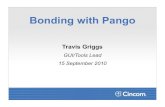
IL28B C allele varies in frequency among geographically distinct ethnic groups
Reprinted with permission from Macmillan Publishers Ltd: Nature. 2009;461:798-801.
rs12979860: High
proportion of CC allele
in Asia

0 5 10
IL28B: CC vs. non-CC
VL<600,000 IU/mL
Caucasian vs. Black
Metavir F0/F1
Hispanic vs. Black
Fasting serum glucose <5.6 mmol/L
IL28B polymorphism is strongest baseline predictor of SVR using pegIFN/RBV
Covariates: rs12979860 (2-level), ethnicity (4-level), age (≤ 40), gender, BMI (< 30), VL (≤ 600,000), ALT (≤ ULN), fasting glucose (< 5.6), hepatic steatosis (N/Y[> 0%]), fibrosis (METAVIR F012), RBV (> 13 mg/kg/d)
P < 0.0001
P < 0.0001
P < 0.0001
P < 0.0001
P < 0.0001
P = 0.004
Thompson AJ, et al. Gastroenterology 2010;139:120-129.
Odds ratio (95% CI)
N = 1,604

RVR is strongest predictor of SVR when treatment is pegIFN/RBV
0 2 4 6 8 10 12 14
All RVR
IL28B CC non-RVR
Metavir F0/F1
VL<600,000 IU/mL
Caucasian vs. Black
Hispanic vs. Black
Fasting serum glucose <5.6 mmol/L
P < 0.001
P < 0.001
P = 0.0001
P = 0.0361
P < 0.001
P < 0.001
P < 0.001
Comparison of RVR vs. no RVR + non-CC genotype; Comparison of no-RVR + CC genotype vs. no-RVR + non-CC genotype; Covariates: RVR vs. no RVR + CC genotype vs. no RVR + non-CC genotype (3-level), ethnicity (4-level), age (≤ 40), gender, BMI (< 30), VL (≤ 600,000), ALT (≤ ULN), fasting glucose (< 5.6), hepatic steatosis (N/Y[> 0%]), fibrosis (METAVIR F012), RBV (> 13 mg/kg/d)Thompson AJ, et al. Gastroenterology 2010;139:120-129.
Odds ratio (95% CI)

IL28B genotype associated with RVR but not SVR in Taiwanese HCV-2 patients
Yu ML, Huang CF, Huang JF, et al. Hepatology 2011;53:7-13.
0
20
40
60
80
100
SV
R r
ate
(%)
RVR SVR
89 86
P = 0.017 P > 0.05
72
85
non-TT TT
• In Asian HCV-2 patients, the rs8099917 TT genotype near IL28B is significantly independently predictive of RVR, which is in turn the single best predictor of SVR.
N = 482

Predictors of SVR in Asian studies of pegIFN α-2b therapy
• Genotype (Fung 2008; Lee 2005, Tsang 2010, Chu 2007; Lee 2010)
• Insulin resistance (Chu 2009)
• Degree of hepatic fibrosis (Chu 2007; Tsang 2010)
• Mutations in interferon sensitivity-determining region (ISDR) (Yen 2008)
• IL28B single nucleotide polymorphism (SNP) rs12979860 (Lin 2011)
• EVR (Chu 2007; Lee 2005)
• Adherence to treatment (Jeong 2009, Kim 2009)
• Age < 50–55 years (Kim 2009; Tsang 2010)
• Baseline HCV RNA ≤ 200,000 IU/mL (Tsang 2010)

Insulin resistance, fibrosis and SVR in Chinese HCV-1 patients on pegIFN α-2b/RBV
0
20
40
60
80
100
SV
R r
ate
(%)
F1-F2 fibrosis(N = 86)
F3-F4 fibrosis(N = 47)
75*
Chu CJ, et al. Aliment Pharmacol Ther 2009;29:46-54.
HOMA-IR < 2 2 < HOMA-IR < 4 HOMA-IR > 4
HOMA-IR, homeostasis model assessment of insulin resistance; **P < 0.004; *P = 0.325
• Insulin resistance increased with the severity of hepatic fibrosis.
• Insulin resistance was a major determinant of SVR in HCV-1 patients who received 24 weeks of pegIFN α combination therapy – the greater the insulin resistance, the lower the SVR rates.
75
95**
54
3935

Evidence supporting response-guided therapy
Virological response to treatment predicts outcome (i.e. SVR)

Predictors of treatment success
• Genotype• Viral load at
baseline
Viral factors
RVR, rapid virological response; EVR, early virological response; cEVR, complete early virological response
On-treatment responses
• RVR (Week 4)• EVR (Week 12)• cEVR
• Age• Genomics• Ethnicity• Immune status• Severity of liver
disease• Hepatic steatosis• Insulin resistance
Host factors

HCV-1: RVR and EVR are important predictors of SVR

IDEAL: Week 4 and Week 12 viral response are key predictors of SVR for HCV-1
1. McHutchison JG, et al. N Engl J Med 2009;361:580-593; 2. Sulkowski M, et al. EASL 2008. Abstract 991.
SV
R
rate
(%
) 1
PPV of SVR
Week 4 Week 12PegIFN α-
2b/RBVPegIFN α-
2a/RBVPegIFN
α-2b/RBVPegIFN α-
2a/RBV
94% 89% 82% 76%
Predictability of treatment response is greater with pegIFN α-2b than with pegIFN α-2a at Weeks 4 and 12.PPV, positive predictive value
2
10
7/1
16
98
/12
3
32
8/4
07
34
4/4
66
68
/15
6
72
/20
3

IDEAL: High correlation between Week 4 and Week 12 as definition for null response
• High positive correlation between HCV-RNA decline at Weeks 4 and 12 (P < 0.001 for each treatment arm):– PegIFN α-2b 1.5 µg/kg/wk + RBV: r = 0.76 (see graph)– PegIFN α-2a 180 µg/wk + RBV: r = 0.73
• High concordance (89%) for both treatment arms between:
– <1-log10 decline at Week 4 and null response at Week 12, or
– ≥1-log10 decline at Week 4 and non-null response at Week 12.
Treatment Week 4 logTreatment Week 4 log1010 drop dropTre
atm
en
t W
ee
k 1
2 l
og
10 d
rop
Poordad F, Poordad F, et alet al. Asian Pacific Digestive Week. Singapore, October 2011.. Asian Pacific Digestive Week. Singapore, October 2011.
Patients with ≤3-log10 decline in HCV-RNA at Week 4 (N = 1,862)
Conclusions: •Week 4 viral load decline of < 1-log10 approximates < 2-log10 decline at Week 12.•Correlation between low Week 4 viral load decline and Week 12 null response may aid early treatment decisions.

IDEAL: Summary of predictors of SVR
• Earlier time to first undetectable HCV RNA level was associated with a greater likelihood of achieving SVR.1
• Predictability of treatment response is greater with pegIFN α-2b than with pegIFN α-2a at Weeks 4 and 12.2
• Correlation between low Week 4 viral load decline and Week 12 null response may aid early treatment decisions.3
• A polymorphism upstream of IL28B (CC vs. CT or TT) is also associated with increased on-treatment and sustained virologic response and effectively predicts treatment outcome.4
1. McHutchison JG, et al. N Engl J Med 2009;361:580-593.2. Sulkowski M, et al. EASL 2008. Abstract 991; 3. Poordad F, et al. Asian Pacific Digestive Week. Singapore, October 2011; 4. Thompson AJ, et al. Gastroenterology 2010;139:120-129 e118.

Mangia A, et al. Hepatology. 2008;47:43-50.
24 weeks
48 weeks
7787 84 83
73
87
SV
R r
ate
(%)
< 400,000 IU/mL ≥ 400,000 IU/mL
P = 0.14P = 0.83
20
40
60
80
100
All LVL HVL
123 62 45 24 78 38
PegIFN α-2a or -2b + RBV 1000–1200 mg
P = 0.12
HVL, high viral load; LVL, low viral load
HCV-1 patients with RVR: Six months treatment sufficient if viral load is low

Six months' pegIFN α-2b sufficient for HCV-1 patients with low viral load who attain RVR
1. Craxi A, et al. J Viral Hepat 2011:doi:10.1111/j.1365-2893.2011.01515.x; 2. Zeuzem S, et al. J Hepatol 2006;44:97-103; 3. Manns MP, et al. Lancet 2001;358:958-965.
Treatment-naïve HCV-1 patients with baseline viral load < 600,000 IU/mL
1 2 3
16/165149/170 98/110 9/106 11/13 1/12

1. Zeuzem S, et al. J Hepatol 2006;44:97-103; 2. Craxi A, et al. J Viral Hepat 2011:doi:10.1111/j.1365-2893.2011.01515.x; 3. Mangia A, et al. Hepatology, 2008; 47:43-50; 4. Pearlman BL, et al. Hepatology. 2007;46:1688-94; 5. Buti M, et al. Hepatology 2010;52:1201-1207.
89
0
20
40
60
SV
R r
ate
(%)
Patients with RVR at Wk 4
80
100
24 wk pegIFN + RBV 48 wk pegIFN + RBV
77
87
PegIFN α-2b 1.5 μg + RBV 800–1,400 mg1,2
PegIFN α-2b 1.5 μg/
PegIFN α-2a 180 μg/+ RBV 1,000–1,200 mg3
PegIFN α-2b 1.5 μg+ RBV 800–1,400 mg4
18
38
49 52
pEVR
38
64
PegIFN α-2b 1.5 μg/ PegIFN α-2a 180 μg/
+ RBV 1,000–1,200 mg3
21 52
No RVR,cEVR
72 wk pegIFN + RBV
PegIFN α-2b 1.5 μg/ + RBV 800–1,400 mg5
25
47
16 15
Slower responders
2–3-log10 decline in HCV RNA at
Week 12
123 62110
88
170
HCV-1: Using response to determine duration of therapy

INDIV2: Relapse rates in HCV-1 according to treatment response and viral load
Baseline viral load
Wiegand J, et al. Clin Infect Dis 2011. doi 10.1093/cid/cir670.
N = 225
TMA, transcription-mediated amplification. *P < 0.0005
*

INDIV-2: Relapse rates greater in HCV-1 patients with residual viremia
TMA, transcription-mediated amplification. †Defined as negative branched DNA assay, positive TMA assay
†
• Many patients who achieve undetectable HCV RNA levels by quantitative assays still have detectable viremia by highly sensitive assays (e.g. TMA).
• These patients have an increased risk for relapse.
• Baseline viral load and early viral kinetics should be included in treatment algorithms to further individualize treatment strategies and prevent relapse.
Wiegand J, et al. Clin Infect Dis 2011. doi 10.1093/cid/cir670.
6/2
9
14
/44
16
/29
0/29 3/71 9/101

HCV-2/3: RVR is an important predictor of SVR

HCV-2/3: Role of RVR in determining treatment duration
• RVR had a high PPV for SVR regardless of treatment duration.• NPV was clearly related to treatment duration.• HCV-2/3 patients with detectable HCV RNA at Week 4 should have
a minimum of 24 weeks of treatment.RVR, rapid virologic response; SVR, sustained virologic response; PPV, positive predictive value; NPV, negative predictive valuePoordad FF. Aliment Pharmacol Ther. 2010;31:1251-1267.
RVR Treatment duration PPV for SVR NPV for No SVR
HCV-2
Yes14–16 wks 83.2%
24 wks 89.3%
No14–16 wks 71.8%
24 wks 44.3%
HCV-3
Yes14–16 wks 82.4%
24 wks 86.4%
No14–16 wks 73.5%
24 wks 58.2%

HCV-2/3: Short-course therapy effective in patients with RVR
1. Mangia A, et al. N Engl J Med 2005;352:2609-2617; 2. Manns M, et al. J Hepatol 2011;55:554-563.
Short duration of treatment (121 or 162 weeks)
Standard duration of treatment (24 weeks)
72 7585
91
PegIFN α-2b 1.0 μg/kg/wk + RBV 1,000–1,200 mg1
PegIFN α-2b 1.5 μg/kg/wk + RBV 800–1,200 mg2
20
40
60
80
100
SV
R r
ate
(%
)
133 97 8745
0
P = 0.938

Relapse rates in HCV-2/3 patients with RVR treated for 12–16 weeks
Multivariate analysisof predictors of relapse
BMI ≥ 30 (P = 0.036)Platelets ≤ 140,000 (P = 0.001)1
476 374 102 277 35 242
1. Mangia A, et al. Hepatology. 2009;49:358-63; 2. Manns M, et al. J Hepatol 2011;55:554-563.
• Relapse rates higher in Asians than in Caucasians.2
• Relapse rates lower with HCV-2 (0%) than HCV-3 (18%) in patients treated for 24 weeks.2
1 2
BMI, body mass index; Tx, treatment.

Independent predictors for relapse in patients with HCV-3
Patients who achieved RVR (albinterferon α-2b or pegIFN α-2a plus fixed-dose RBV)
• Hepatic steatosis was the strongest predictor of relapse (OR 3.0; 95%CI 1.5–6.1; P < 0.003), irrespective of viral load, in HCV-3 patients who achieved RVR.
• High baseline HCV RNA level was the strongest predictor of steatosis (OR 6.3; 95% CI 3.6–10.8; P < 0.001).
Shah SR, et al. Clin Gastroenterol Hepatol 2011;9:688-693.
23 148 118 113

SVR also depends on RBV dose
Manns MP, et al. Lancet 2001;358:958-965.
• SVR likelihood can be increased if RBV dosage is weight-based.
• SVR rates were higher in all groups where RBV dose was > 10.6 mg/kg bodyweight (lower end of optimum dose range).
• For an average 75 kg man, doses of 10.6 mg/kg, 13.2 mg/kg, and 15 mg/kg represent daily doses of 800 mg, 1000 mg, and 1200 mg RBV, respectively.

Early termination of pegIFN/RBV therapy: Taiwanese study
• Of 617 patients assigned 24 weeks of pegIFN α/RBV,
29 (4.7%) terminated treatment at < 20 weeks.
– Five (17.2%) patients achieved SVR, comprising:
• 0/16 HCV-1 (0%)
• 5/13 HCV-2 (38.5%; P = 0.001).
– All sustained responders were HCV RNA seronegative at week 4 of treatment (i.e. achieved RVR) and received > 8 weeks' treatment.
– Most common reasons for early termination were flu-like symptoms/signs (n = 9).
Yu ML, et al. Antivir Ther 2006;11:1015-1019.

Adherence to therapy regimen results in optimal SVR (Korean study)
Jeong SW, et al. Korean J Hepatol 2009;15:338-349.

Adverse events

IDEAL: Most common adverse events
Adverse event, (%)
PegIFN α-2b/RBVPegIFN α-2a/RBV
N = 1,035(1.0 μg) N = 1,016 (1.5 μg) N = 1,019
Fatigue 66.5 65.9 63.4
Headache 47.8 49.9 42.3
Nausea 37.1 42.5 36.4
Insomnia 38.3 39.4 41.4
Pyrexia 32.6 34.9 22.9
Anemia 28.8 33.9 33.6
Myalgia 26.6 26.9 22.5
Neutropenia 18.5 25.8 31.5
Depression 19.4 25.5 21.0
Irritability 25.8 25.1 25.3
Rash 21.9 22.1 28.0
McHutchison JG, et al. N Engl J Med 2009;361:580-593.

Common adverse events associated with pegIFN/RBV therapy
• Influenza-like (fatigue, headache, fever, and rigors): > 50%
• Psychiatric (depression, irritability, and insomnia): 22–31%
• Neutropenia (ANC < 1500/mm3): 18–20%1,2
– Severe neutropenia* (ANC < 500/mm3): 4%
– Serious infections are uncommon and G-CSF is rarely necessary.3
• Anemia (Hb < 12 g/dL): ~ 30%1,2
– Nadir occurs within 6–8 weeks.
– Anemia requiring action† (Hb < 10 g/dL): 9–15%
• Laboratory abnormalities are the most common reasons for HCV therapy dose reduction.
1. Manns MP, et al. Lancet. 2001;358:958-965.; 2. Fried MW, et al. N Engl J Med. 2002;347:975-982; 3. Soza A, et al. Hepatology. 2002;36:1273-1279.
ANC, absolute neutrophil count; G-CSF, granulocyte-specific colony-stimulating factor; Hb, hemoglobin. *And treatment discontinuation. †And dose modification.

Months
Depression
Fatigue
Flu-like symptoms
Time course of major treatment-associated adverse events
Anxiety
1 2 3 40
Incr
ease
in
in
cid
ence
/ s
ever
ity
Dan A, et al. J Hepatol. 2006;44:491-498; Constant A, et al. J Clin Psychiatry. 2005;66:1050-1057.

Adverse events leading to early termination of therapy: Japanese study
• In 2,871 Japanese patients treated with pegIFN α-2b + RBV, the most common reasons for withdrawal were:
– neurovegetative symptoms (30.8%), depression-related syndromes (18.4%), hematologic effects (6.4%) and dermatologic effects (10.8%).
• Withdrawal rates were 13% in patients aged ≥ 65 years and 7% of those aged <65 years.
• Rates of withdrawal due to neurovegetative symptoms, depression-related syndrome, and hematologic effects was significantly higher in men aged ≥ 65 years than in those aged < 65 years (P = 0.0001, P = 0.0016, and P = 0.0170, respectively); this was not observed in women.
Ogawa E, et al. J Gastroenterol Hepatol. 2011 (http://onlinelibrary.wiley.com/doi/10.1111/j.1440-1746.2011.06965.x/pdf)

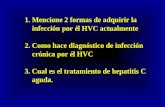
IDEAL: Early onset anemia and SVR
• A higher magnitude of hemoglobin decline was associated with a higher likelihood of SVR.
Sulkowski M, et al. EASL 2009. Copenhagen, Denmark. Abstract 126.
P < 0.0001P < 0.001
P < 0.0001
Hemoglobin decline
(N = 773)
(N = 2,250)

IDEAL: Anemia and erythropoietin (EPO): Impact on relapse rates
Sulkowski M, et al. EASL 2009. Copenhagen, Denmark. Abstract 126.
• Patients with anemia who received PegIFN α-2b and were not treated with EPO had lower relapse rates than those who did not have anemia.
(N = 2,158) (N = 416) (N = 449)

Correlation between SVR and anemia in Taiwanese HCV-1 patients
• In 466 CHC patients treated with pegIFN α/RBV for 24 weeks, a correlation was found between SVR rate and period of anemia during treatment in HCV-1 patients.
Hung CH, et al. Liver Int 2006;26:1079-1086.
HCV-1: N = 205Non-HCV-1: N = 261
r = 0.774, P = 0.003
r = 0.960, P < 0.001
r = 0.107, P = 0.754

IDEAL : Neutropenia, anemia, and thrombocytopenia
Mean (SD) Nadir Hematologic Values
Poordad F, et al. Presented at the 59th AASLD, October 31-November 4, 2008, San Francisco, CA.
PegIFN α-2b 1.5/RBV(N=1,019)
PegIFN α-2a/RBV(N=1,035)
P-value
Neutrophil count, x 109/L 1.15 (0.55) 1.09 (0.56) < 0.001
Platelet count, x 109/L 145 (53) 130 (51) < 0.001
Hemoglobin conc., g/L 10.9 (1.5) 10.9 (1.5) 0.43
• Treatment with pegIFN α-2a/RBV caused significantly more neutropenia and thrombocytopenia than either of the pegIFN α-2b/RBV regimens, particularly in patients with low body weight.
– May reflect increased bone marrow exposure to IFN α based on body weight in the pegIFN α-2a arm in the lower weight groups, and possible inherent differences among the different pegIFN α molecules.

IDEAL: Grade 3–4 neutropenia by treatment arm and baseline weight
• Neutropenia was related to body weight in the pegIFN α-2a arm– Patients with lower body weights had higher rates of dose reduction and
discontinuation than did those with higher body weights
Poordad F, et al. Presented at the 59th AASLD, October 31-November 4, 2008, San Francisco, CA

Thyroid dysfunction in Taiwanese patients treated with IFNα-2b or PegIFN α-2b/RBV
• In 461 CHC patients with normal baseline thyroid functions, incidence of thyroid dysfunction (TSH < 0.1 or > 5 mU/L) was 12.6% after 24–48 weeks of treatment.
• Female gender was significantly associated with thyroid dysfunction (P < 0.001).
• No difference in incidence of thyroid dysfunction for standard IFN vs. pegIFN-treated patients (49/391 vs. 9/70; P=1.00).
• Significant association between higher positive rates of pre-treatment TMA and patients who developed thyroid dysfunction (OR: 5.8, 95% CI: 1.2–27.9).
• ~ 2% remained thyroid dysfunctional at the end of follow up (median, 26.5 months), no risk factors were found.
Kee KM, et al. J Gastroenterol Hepatol 2006;21:319-326.
TSH, thyroid stimulating hormone; TMA, thyroid microsomal antibody

Difficult-to-treat HCV populations

PROTECT: PegIFN α-2b/RBV for HCV recurrence after orthotopic liver
transplantation (OLT)
5550
69
0
10
20
30
40
50
60
70
80
All Patients HCV-1 HCV-2/3
SV
R r
ate
(%)
36/66 25/50 11/16
ITT: 29% ITT:
24%
ITT: 55%
Study completion analysis*
*Patients who completed 48 weeks of treatment and 24 weeks of follow-up. ITT, intention-to-treat.
Gordon FD, et al. Presented at 45th EASL, April 2010 , Vienna, Austria.
• SVR rates were higher among patients who completed treatment.
• RVR, cEVR, and EOT response were predictive of SVR.
• Rejection rate was low.

Patients with HCV-related cirrhosis
• Meta-analysis of 11 studies of 1,133 patients with HCV-related cirrhosis treated with pegIFN/RBV for 48 weeks:1
– Overall SVR rate 33.8% (HCV-1/4: 21.6%;HCV-2/3: 37.8%).
• Korean study (N = 86) of pegIFN/RBV in HCV-related cirrhosis patients:2
– Overall SVR rate 34.9% (HCV-1: 20.8%; non-HCV-1: 2.6%).
– Independent predictors of treatment failure were HCV-1 (P = 0.003), high baseline viral load (> 8.0×105 IU/mL, P = 0.012).
– AEs leading to withdrawal were thrombocytopenia (2 patients), and depression, anxiety disorder and cerebral vascular hemorrhage (each 1 patient).
1. Bota S, et al. 19th United European Gastroenterology Week of the United European Gastroenterology Federation, Stockholm, Sweden, October 2011, Abstract P1213; 2. Kim KH, et al. Korean J Hepatol 2011;17:220-225.

HCV patients co-infected with HIV
• SVR rates following pegIFN α/RBV therapy in HCV/HIV co-infected patients are 15–20% lower than in patients with HCV alone.1
• Predictors of treatment response are largely hepatitis C factors: genotype, HCV viral load, and liver disease stage. 1
• Recommended HCV treatment is pegIFN/RBV for 48 weeks; weight-based RBV dosing should be considered for HCV-1 patients.
1
• Meta-analysis2 of 6 studies of IFN vs. pegIFN in 1,717 patients co-infected with HCV and HIV showed that:
– For HCV-1/4 and HIV-co-infected patients, both types of pegIFN, α-2a and α-2b, achieved higher SVRs than IFN.
– SVRs achieved in patients infected with HCV-1/4 treated with pegIFN and RBV were lower than in those infected with HCV-2/3 (26% vs. 55%).
1. McCaughan GW, et al. J Gastroenterol Hepatol 2007;22:615-633; 2. Zhao S, et al. Eur J Clin Microbiol Infect Dis 2008;27:1183-1192.

HCV patients with ESRD on hemodialysis
• Management of CHC is more complicated in hemodialysis patients due to altered pharmacokinetics and drug-related toxicity, particularly RBV-induced anemia.1
• Malaysian study2 of escalating pegIFN α-2b monotherapy (N = 46; 0.5 μg/kg/week 4 weeks, then 1.0 μg/kg/week 20–44 weeks) showed SVR rates for HCV-1: 37.5%; HCV-3: 80%.
• In Indian study (N = 6), pegIFN α-2b (1.0 μg/kg/week for 24 weeks) was safe and effective (SVR rate 50%).3
• Meta-analyses show that ~33% of ESRD patients with CHC achieve SVR after IFN or pegIFN monotherapy.4
• PegIFN or IFN plus low-dose RBV can increase SVR rates, but close monitoring of hemoglobin levels and high-dose EPO needed to prevent severe anemia.4
1. Berenguer M. Hepatology 2008;48:1690-1699; 2. Tan SS, et al. J Viral Hepat 2010;17:410-418; 3. Amarapurkar DN, Patel ND and Kirpalani AL. Trop Gastroenterol 2007;28:16-18; 4. Liu CH and Kao JH. J Gastroenterol Hepatol 2011;26:228-239.
ESRD, end-stage renal disease; EPO, erythropoietin

Additional slides
Details of Asian studies

Summary of treatment responses to pegIFN α-2b/RBV for CHC in Asia
Reference, country
N Regimen Genotype SVR Comment/findings
Chu 20091
Chinese pts133
pegIFN α-2b + RBV 24 wks
HCV- 1 66%Insulin resistance is major determinant of SVR
Chu 20072
Chinese pts65
1.5 μg/kg/wk + RBV 24 wks
HCV-1non-HCV-1
69%93%
EVR predictor of response: 24wks may be adequate for HCV-1 early responders
Fung 20083
Hong Kong42
pegIFN α-2a or pegIFN α-2b + RBV 48 wks
HCV-1HCV-6
52%86%
48 weeks' treatment with pegIFN α-2a or -2b resulted in significantly higher SVR for HCV-6 patients (P = 0.019)
Hung 20064
Taiwan466
pegIFN α-2a or 1-1.5 μg/kg/wk pegIFN α-2b + RBV 48 wks
HCV-1non-HCV-1 (98% were HCV-2)
52%93%
Significant correlation between SVR rate and time of anemia during therapy

Summary of treatment responses to pegIFN α-2b/RBV for CHC in Asia
Reference, country
N Regimen Genotype SVR Comment/findings
Jeong 20095
Korea92 180 μg pegIFN
α-2a or 1.5 μg/kg/wk pegIFN α-2b + RBV 48 wks (HCV-1) or 24 wks (non-1)
HCV-1non-HCV-1
In those who received ≥ 80% therapy:
86.7%100%
SVR rates differed significantly with degree of adherence to the treatment. Adherence to therapy is a key factor in achieving SVR.Supportive strategies toimprove adherence will increase overall SVR rates.
Lee 20056
Taiwan153 3MU IFN α-2b
t.i.w. + RBVor 1.5 μg/kg/wk pegIFN α-2b + RBV 24 wks
HCV-1non-HCV-1
HCV-1non-HCV-1
41.0%86.8%
65.8%68.4%
HCV-1 relapse was greater in IFN group (52.9% vs. 28.6% with pegIFN α).EVR at week 12 and non-HCV-1 genotype were significant predictors of SVR.
Tsang 20107
Hong Kong70 180 μg pegIFN
α-2a or 1.5 μg/kg/wk pegIFN α-2b + RBV 48 wks
HCV-1HCV-6
57.1%75.7%
Age ≤ 55 years, HCV genotype, liver biopsy staging and baseline hepatitis C virus RNA (≤ 200,000 IU/mL) were independent predictors of SVR.

Summary of treatment responses to pegIFN α-2b/RBV for CHC in Asia
Reference, country
N Regimen Genotype SVR Comment/findings
Yu 20068
Taiwan60 80–100
μg/kg/wk pegIFN α-2b + RBV 24 or 48 wks
HCV-1b 24wks: 48.9%
48wks: 80.0%
In 19 patients without an unfavorable predictor, SVR rate was comparable in the 24-week (78.6%) and 48-week (75.0%) groups.
Kim 20099
Korea130 180 μg pegIFN
α-2a or 1.5 μg/kg/wk pegIFN α-2b + RBV 24 or 48 wks
HCV-1 24 wks: 52.9%
48wks:74.0%
Patients who relapsed after 24 weeks of treatment were treated for further 24 weeks and 42.9% achieved SVR. The 24-week + additional split 24-week therapy following failure is useful treatment strategy for HCV-1 patients.
Lee 201010
Korea126 180 μg pegIFN
α-2a or 1.5 μg/kg/wk pegIFN α-2b + RBV 48 wks (HCV-1) or 24 wks (non-1)
HCV-1 pegIFN α-2a:70.9 %
pegIFN α-2b:72.3%
Whether patients had HCV genotype 1 or non-1, treatment responses were not significantly different for pegIFN α treatments. HCV genotype was the only independent factor that affected SVR (P = 0.048).