Anticonvulsants Part II
19
-
Upload
brian-piper -
Category
Documents
-
view
959 -
download
3
description
This PPT is part two of two lectures given to second year pharmacy students in a pharmacology & toxicology class.
Transcript of Anticonvulsants Part II

Anticonvulsants IIBrian J. Piper, Ph.D., M.S.
February 8, 2013

Objectives
• Pharmacy students will be able to:– describe the MOA of recently developed AEDs.– identify and contrast the relative frequency of
adverse events for AEDs.

Voltage Sensitive Ion Channels• Composed of multiple subunits (α,β,δ)• α subunit, transmembrane 4 = voltometer• can exist in open, closed, or inactive states
Pore inactivator
Stahl (2008). Essential Psychopharmacology, p. 149, 152.

Carbamazepine
• Structure: similar to TCAs• Indications: generalized & partial seizures• PK: CYP3A4 inducer (↓ Carb t1/2 from 36 to 10!, ↓ birth
control)• Adverse Events: diplopia, ataxia (not sedation)• Pregnancy Category: D• MOA: stabilizes the inactivated state of voltage-gated sodium
channels

MOAs of Carbamazepine (& others)
• Prolong inactive state of voltage sensitive ion channel for Na+, Ca2+, K+
• Bind to α subunit of Na+ channel• Increase inhibitory effects of GABA
Stahl (2008). Essential Psychopharmacology.

Stevens-Johnson Syndrome • Potentially lethal drug induced hypersensitivity • Carbamazepine (1/5,000), phenobarbital,
phenytoin, lamotrigine• Symptoms: fever, sore throat, skin sloughing
(mouth/lips, genitals, anus)• Adults (Han Chinese) > children
Bae et al. (2013). Korean Journal of Pain, 26(1), 80 – 83.
Conjunctivitis in SJS

Oxcarbazepine (& Eslicarbazepine)• Structure: similar to carbamazepine• Indications: generalized & partial seizures• Adverse Events: diplopia, ataxia, hyponatremia• PK: – CYP3A4 inducer– t1/2 = 2 / 10
• AE: SJS (rare)
(Europe only)

Lamotrigine• Indications: – partial & generalized seizures– Lennox-Gastaut syndrome – Bipolar I
• MOA: voltage gated ion channels, ↓ glutamate release
• Adverse Effects: dizziness, headache, somnolence• PK: t1/2 = 24 h• Pregnancy Category: C

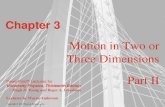
Comparative Efficacy & Tolerability• AED naïve epileptics (age 13-80) randomized to
lamotrigine (150 mg/day) or carbamazepine (600 mg/day)
->
->
Brodie et al. (1995). Lancet, 345, 476-479.

Gabapentin
• MOA: – voltage sensitive Ca2+ channels– ↑ GABA– ↓ glutamate
• Indications: partial seizures, pain, not bipolar
• Adverse Events: somnolence, ataxia, headache• PK:– t1/2 = 6 hours– not CYP inducer, negligible drug interactions
Porter & Meldrum (2011). In Katzung’s Basic & Clinical Pharmacology, p. 413.

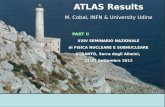
AED Rash• Rashes, commonly minor, are commonly experienced by epileptics (16%).• Comparison of rash rates in practices of 13 epileptologists (N = 1,890 adults)• Average rate of rash = 2.8%• Significantly above average: phenytoin (PHT), lamotrigine (LTG)• Average: oxcarbazepine (OXC), carbamazepine (CBZ)• Significantly below average: gabapentin (GBP), valproate (VPA)
Arif et al. (2007). Neurology, 68, 1701-1709.

AED Rash• Rashes, commonly minor, are commonly experienced by epileptics (16%).• Comparison of rash rates in practices of 13 epileptologists (N = 1,890 adults)• AED discontinuation due to rash = 1.3%• Significantly above average: phenytoin (PHT), lamotrigine (LTG)• Average: oxcarbazepine (OXC), carbamazepine (CBZ)• Significantly below average: gabapentin (GBP), valproate (VPA)
Arif et al. (2007). Neurology, 68, 1701-1709.

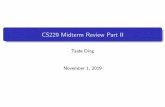
No malformations = safe?• Prospective study of offspring of
epileptics that received:– sodium valproate (VPA,
N=42) – carbamazepine (CBZ, N=48)– lamotrigine (LTG, N=34)– polytherapy (Poly, N=30), – no medications (NoMe,
N=27).
• Offspring of non-epileptics (control, N=230) were also examined
• Neuropsychological test ≈ 1 year• Monotherapy < Control
--------------------------------------------------
Bromley et al. (2010). Epilepsia, 51(10), 2058-2065.
*

Prenatal AEDs & Autism
• Neurodevelopmental disorders (Autism Spectrum Disorders, ADHD & dyspraxia) at age 6 in a prospective study.
Bromley et al. (2013). Journal of Neurology, Neurosurgery, & Psychiatry, in press.

Future Pipeline
15

FDA Approved IndicationsAgent Epilepsy Seizure Type Other
phenobarbital partial & generalized
phenytoin partial & generalized
valproic acid absence & partial manic episodes, migraine
carbamazepine partial & generalized bipolar I, pain (neuralgia)
oxcarbazepine partial
lamotrigine partial & generalized bipolar I
gabapentin partial pain (neuralgia)

AED & Suicide• Suicide rates are 3-fold higher among epileptics relative
to the general population.• The FDA issued an alert that all AEDs “may increase risk
of suicidal thoughts/behavior; monitor for worsening of depression and any unusual changes in mood or behavior.”
• Evidence is currently inconclusive whether increased suicide following AEDs (oxcarbazepine, valproate) occurs only in high risk populations (bipolar, chronic pain) or in epileptics without comorbid conditions.
Patorno et al. (2010), JAMA, 303(14), 1401-1409; Hecimovic et al. (2011). Epilepsy & Behavior, 22, 77-84.

General AED Principles
• At least 50% of epileptics have a substantial reduction in seizure frequency with AEDs.
• If one AED doesn’t work, the likelihood that a second won’t work is greater.
• Seizures are intractable in 30% of epileptics.
Brodie, M. J. (2010). Seizure, 19, 650-655,

Summary
• AEDs target voltage gated channels & GABA.• 2nd generation AED are better tolerated than
older agents but offer limited improvements in efficacy.
• Polytherapy is very common for seizure control which presents opportunities to manage drug interactions.