and Anti Drugs on Vital Signs - Cardiac Safety Research ... · Drugs on Vital Signs Jim Keirns...
28
Differences with Age in Effects of Differences with Age in Effects of Adrenergic and Anti‐Muscarinic l Drugs on Vital Signs Jim Keirns Astellas Pharma Global Astellas Pharma Global Development, Inc 7/18/2012 1 CSRC BP Thinktank
Transcript of and Anti Drugs on Vital Signs - Cardiac Safety Research ... · Drugs on Vital Signs Jim Keirns...

Differences with Age in Effects ofDifferences with Age in Effects of Adrenergic and Anti‐Muscarinic
lDrugs on Vital Signs
Jim KeirnsAstellas Pharma GlobalAstellas Pharma Global
Development, Inc
7/18/2012 1CSRC BP Thinktank

Reason for my interest in the topic: MirabegronSelective β‐3 adrenergic agonist approved in Japan (2011) and US (2012) for treatment of Overactive Bladder (OAB)
Affinity of Mirabegron for Human β‐Adrenoceptor SubtypesAffinity of Mirabegron for Human β Adrenoceptor Subtypes
Ki (nmol/L)
β Β Ββ1 Β2 Β3
4200 ± 900 1300 ± 300 40 ± 20.2
Ki values are expressed as the mean ± SE of 3 runs; receptor binding study using membrane fractions from p ; p g y gChinese hamster ovary (CHO) cells expressing human β‐AR subtypes
2

Changes in response to drugs with age
• The changes in response to drugs with age are summarized in the chapter “Pharmacology across the ageing continuum” (Gronich)continuum (Gronich).
• Particularly notable are changes in the cholinergic and adrenergic systems with aging. Changes in the CV system with age are summarized in the chapter “Effects of aging onwith age are summarized in the chapter Effects of aging on cardiovascular structure and function” (Kitzman).– Gronich N, Abernethy DR, in Waldman SA, Terzic A,
Pharmacology and Therapeutics, 2009, Sanders, Philadelphia.Pharmacology and Therapeutics, 2009, Sanders, Philadelphia.– Kitzman DW, Taffet G. in Hazzard’s Geriatric Medicine and
Gerontology, 6th Ed. 2009, McGraw‐Hill, New York.• There are changes in autonomic tone with age that affectThere are changes in autonomic tone with age that affect
the response to drugs that act on this system.
7/18/2012 CSRC BP Thinktank 3

Cholinergic system• Decreased cholinergic responsiveness in aged rats (Ayyagari )
is the basis for the use of donepezil and other cholinesterase inhibitors to treat Alzheimer’s diseaseinhibitors to treat Alzheimer s disease.– Ayyagari PV, Gerber M, Joseph JA, Crews FT. Uncoupling of muscarinic
cholinergic phosphoinositide signals in senescent cerebral cortical and hippocampal membranes. Neurochem Int 1998; 32:107‐115.
• The PI for Sanctura® trospium reports the following from the TQT study: Also in this study, the immediate‐release formulation of trospium chloride was associated with an increase in heart rate that correlated with increasing plasmaincrease in heart rate that correlated with increasing plasma concentration, with a mean elevation in heart rate compared to placebo of 9 beats per minute for the 20 mg dose and of 18 beats per minute for the 100 mg dose. In the two Phase 3beats per minute for the 100 mg dose. In the two Phase 3 SANCTURA XR® trials the mean increase in heart rate compared to placebo was approximately 3 beats per minute in both studies.
7/18/2012 CSRC BP Thinktank 4

Adrenergic systemd fl b l b lb• CNS adrenergic outflow in subcortical suprabulbar regions is
increased with age, and this has been associated with a state of generalized adrenergic activation (Esler; Seals). Central and peripheral beta‐adrenorecepters are reduced.peripheral beta adrenorecepters are reduced.
– Esler M, Hasting J, Lambert G et al. The influence of aging on the human sympathetic nervous system and brain norepinephrine turnover. Am J Physiol 2002; 282:R909‐R916.
– Seals DR, Dinenno FA. Collateral damage: cardiovascular consequences of chronic sympathetic activation with human aging. Am J Physiol 2004; 287:H1895‐H1905.
• In the CV system both beta1‐ and beta2‐adrenergic responses are decreased with advancing age (Schutzer). The decline in beta1‐adrenergic responsiveness results in decreased tachycardicresponse to sympathetic stimulation The decline in beta ‐response to sympathetic stimulation. The decline in beta2‐adrenergic responsiveness leads to a relative state of peripheral vascular vasoconstriction owing to loss of beta2‐adrenergic vasorelaxation (Pan).
– Schutzer WE, Mader SI. Age‐related changes in vascular adrenergic signaling: clinical and mechanistic Implications. Aging Res Rev 2003; 2:169‐190.
– Pan HYM, Hoffman BB, Porsche RA, Blaschke TF. Decline in beta‐adrenergic receptor‐mediated vascular relaxation with aging in man. J Pharmacol Exp Ther 1986; 239: 802‐807.807.
7/18/2012 CSRC BP Thinktank 5

Adrenergic system (cont.)• α1‐adrenergic vasoconstrictor responses are impaired in older
individuals (Hogikyan). Older patients show less tachycardia than younger patients when exposed to beta adrenergicthan younger patients when exposed to beta2‐adrenergic agonists for treatment of pulmonary diseases (Vestel). An isoproterenol dose that increases heart rate by 25 bpm in healthy young men produces an increase of only 10 bpm inhealthy young men produces an increase of only 10 bpm in older subjects (Kitzman, ref. on slide #3). These different factors contribute to the well‐known reduction with increasing age in maximal heart rate achievable with exercise ( k )(Tanaka).– Hogikyan RV, Supiano MA. Arterial alpha‐adrenergic responsiveness is
decreased and SNS activity is increased in older humans. Am J Physiol 1994; 266:E717‐724.
– Vestal RE, Wood AJJ, Shand DG. Reduced beta‐adrenergic sensitivity in the elderly. Clin Pharmacol Ther 1979; 26: 181‐186.
– Tanaka H, Monahan KD, Seals DR. Age‐predicted maximal heart rate revisited. J Am Coll Cardiol 2001; 37:153‐156.
7/18/2012 CSRC BP Thinktank 6

Qsymia: age‐related differences in vital signsQsymia: age related differences in vital signs
• With a 15 mg dose of phentermine in combination with g ptopiramate (Qsymia, a sympathomimetic antiobesity drug)
VI‐0521 (QNEXA®) Advisory Committee Briefing Document. Endocrinologic and Metabolic Drugs Advisory Committee MeetingEndocrinologic and Metabolic Drugs Advisory Committee Meeting. July 15, 2010. VIVUS, Inc. NDA 022580
7/18/2012 CSRC BP Thinktank 7

Milnacipran: age‐related differences in vital signs
• Another example is milnacipran (serotonin‐norepinephrine re‐t k i hibit f fib l i ) I h 1 H lth V l tuptake inhibitor; for fibromyalgia). In a phase 1 Healthy Volunteer
study (Clinical Pharmacology review. Aug. 29, 2008. NDA 22‐256) conducted to examine cardiovascular safety, doses of 50, 100 and 200 mg/day (administered as 25, 50, 100 mg bid) increased heart g/ y ( , , g )rate (compared to placebo) 5.7, 7.0, and 10.3 bpm on Day 1 and 10.8, 11.5, and 16.2 bpm on Day 3. In Phase 3, increases with milnacipran 100‐200 mg/day were 7‐8 bpm. Si il l i h lth l t il i 50 100 d 200 /d• Similarly, in healthy volunteers milnacipran 50, 100 and 200 mg/day increased SBP (compared to placebo) 5‐7, 4, and 6‐9 mmHg on Days 1‐3 and increased DBP 3‐7, 3‐8, and 5‐8 mmHg on Days 1‐3. In Phase 3, increases with milnacipran 100‐200 mg/day were 3 mmHg, p g/ y gSBP and 2‐3 mmHg DBP (compared to placebo).
7/18/2012 CSRC BP Thinktank 8

Mirabegron: Healthy Volunteers
StudyDose(mg)
Subjects(n)
VS Measurement Condition
VS Measurement
DayMultiple of
Recommended DoseMean* (SD)
↑Pulse (bpm)Mean* (SD)↑BP (mmHg)
Vital Sign (Pulse, BP) in Healthy Volunteers (Median age 31‐32 years)
Study (mg) (n) Condition Day Recommended Dose ↑Pulse (bpm) ↑BP (mmHg)Dose Exposure SBP DBP
PK (031) 50 12 supine Day 13 1x 1x 5.4 (4.85) 2.5 (6.13) 3.1 (4.67)100 12 supine Day 13 2x 2.1x 8.5 (4.07) 5.1 (4.31) 1.9 (3.78)200 12 supine Day 13 4x 5.5x 12.4 (6.70) 9.0 (8.58) 6.2 (2.55)300 12 i D 13 6 10 1 17 2 (5 24) 6 4 (6 30) 4 6 (5 04)300 12 supine Day 13 6x 10.1x 17.2 (5.24) 6.4 (6.30) 4.6 (5.04)
TQT (077) 50 83 supine Day 9 1x 1x 6.3 (6.44) 4.5 (7.98) 0.7 (5.64)100 82 supine Day 9 2x 2.6x 9.3 (7.06) 6.7 (8.12) 3.6 (6.85)200 84 supine Day 9 4x 6.5x 14.4 (7.91) 9.6 (9.17) 5.5 (7.08)
* Mean Area Under the Effective Change Curve over 11.5 hrs for ‐031 and 24 hrs for ‐077
Pulse Rate Changes in Healthy Volunteers and in OAB Patients at Recommended Doses
Mean Area Under the Effective Change Curve over 11.5 hrs for 031 and 24 hrs for 077
Drug Dose Mean Increase in Pulse (bpm)Healthy Volunteers OAB Patients
Mirabegron 50 mg 5.4 1.0
Results from Sanctura (09/2011) Approved US label
Trospium 60 mg 9 3 ‐ 4
.
9

Cardiovascular Safety Assessment of Phase 3 Studies conducted in Europe & North America
12 week phase 3 studies and long‐term (52‐week) controlled study – Vital sign measurements
• Patient diary• Office device• 24 hour ABPM in a subset of patients
Analysis of BP and PulseQ tit ti h t i ti– Quantitative characterization• Central tendency• Exposure response analyses• Categorical analyses
– Clinical assessment• Adverse event reporting using SPA definitions of hypertension andAdverse event reporting using SPA definitions of hypertension and tachycardia
10

Scheme of Values Included in Calculation of Average Vital Sign Values for Each Visit and AM/PM (Diary Data) for 12‐Week Phase 3 Studies:
SPA Recommended ProcedureSPA‐Recommended ProcedureVisit
Baseline Week 4 Week 8 Week 12
Morning/ Afternoon Sequence
Diary Day Diary Day Diary Day Diary Day
1 2 3 4 5 1 2 3 4 5 1 2 3 4 5 1 2 3 4 5
1 ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○The 6 shaded values are averaged to
AM 2 ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ●
3 ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ●
1 ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
averaged to calculate the visit value.
PM
1 ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
2 ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ●
3 ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ● ○ ○ ● ● ●○ – Represents an individual vital sign measurement that was not included in the calculation of a patient’s
average value per visit and time of day
● – Represents an individual vital sign measurement that was included in the calculation of a patient’s average value per visit and time of day
Verberk WJ, Kroon AA, Kessels AGH, et al. The optimal scheme of self blood pressure measurement as determined from ambulatory blood pressure recordings. J Hypertension 2006;24:1541‐1548.
935,961 pulse; 935,950 SBP; 935,745 DBP measurements
11

12‐Week Phase 3 StudiesChange from Baseline to Final Visit SBP/DBP (Patient Diary)Change from Baseline to Final Visit SBP/DBP (Patient Diary)
N BaselineAM SBP
Placebo 1329 125.9
25 mg mirabegron 410 129.2
50 mg mirabegron 1327 126 450 mg mirabegron 1327 126.4
100 mg mirabegron 891 125.0
Tolterodine 476 128.2
AM DBP
Placebo 1329 77.1
25 mg mirabegron 410 78.2
50 mg mirabegron 1327 77.2
100 mg mirabegron 890 77.4
Tolterodine 476 76.8
PM SBP
Placebo 1326 125.0
25 mg mirabegron 410 129.0
50 mg mirabegron 1327 125.6
100 mg mirabegron 890 123.7
Tolterodine 476 127.4
PM DBP
Placebo 1326 75.3
25 mg mirabegron 410 76.1
50 mg mirabegron 1327 75.4
100 mg mirabegron 890 75.3
T l di 476 75 4
‐3.0 ‐2.0 ‐1.0 0.0 1.0 2.0 3.0
Adjusted Mean Change from Baseline (95% CI)
Mean Difference vs Placebo (95% CI)
‐3.0 ‐2.0 ‐1.0 0.0 1.0 2.0 3.0
Tolterodine 476 75.4
12

12‐Week Phase 3 Studies Adjusted Differences versus Placebo for Change from
B li i SBP E h Vi i
2
Baseline in SBP at Each VisitSBP AM
cebo
for
95% CI)
-1
0
1
fferen
ce versus p
lac
m baseline in SBP
(9
0.6 0.5 0.7
-2
1
Adjusted
dif
chan
ge from
Week 4 Week 8 Week 12
Mirabegron 50 mg
2
SBP PMMirabegron 50 mg
placeb
o for
P (95%
CI)
-1
0
1
differen
ce versus p
rom baseline in SBP
0.6 0.4 0.5
-2Week 4 Week 8 Week 12
Source: CVRR 9.3.1.1
Adjusted
chan
ge f r
13

Long‐Term (52‐Week) Controlled Study Change from Baseline to Final Visit SBP/DBP (Patient Diary)Change from Baseline to Final Visit SBP/DBP (Patient Diary)
n Baseline
AM SBP
50 mg mirabegron 791 126.7
100 mg mirabegron 802 125.9
Tolterodine 793 126.8
AM DBP
50 mg mirabegron 791 77.6
100 mg mirabegron 802 77.2
Tolterodine 793 77.6
PM SBP
50 mg mirabegron 789 126.4
100 mg mirabegron 802 125.7
Tolterodine 793 126.3
PM DBP
50 mg mirabegron 789 76.2
100 mg mirabegron 802 75.9
Tolterodine 793 76 1
‐2.0 ‐1.0 0.0 1.0 2.0
Adjusted Mean Change from Baseline (95% CI)
Tolterodine 793 76.1
14

Categorical Analysis of Blood Pressure
n (%) of PatientsPlaceboN = 1380
Mirabegron 50 mgN = 1375
EU/NA 12‐Week Phase 3 Studies
SBP AM (n = 1196) (n = 1202)
3 Consecutive Post-Baseline VisitsChange from baseline ≥ 2 mm Hg 252 (21.1%) 255 (21.2%)g g ( ) ( )Change from baseline ≥ 5 mm Hg 136 (11.4%) 140 (11.6%)
Change from baseline ≥ 10 mm Hg 28 (2.3%) 35 (2.9%)Change from baseline ≥ 15 mm Hg 8 (0.7%) 8 (0.7%)Change from baseline ≥ 20 mm Hg 6 (0.5%) 5 (0.4%)
DBP AM (n = 1196) (n = 1202)
3 C ti P t B li Vi it3 Consecutive Post-Baseline Visits
Change from baseline ≥ 2 mm Hg 170 (14.2%) 219 (18.2%)Change from baseline ≥ 5 mm Hg 62 (5.2%) 80 (6.7%)Change from baseline ≥ 10 mm Hg 11 (0.9%) 10 (0.8%)Change from baseline ≥ 15 mm Hg 0 1 (0.1%)
15

Regression Analysis of Exposure Response for Blood Pressure 0 mg 50 mg 200 mg
25 mg 100 mg
16

Baseline Corrected SBP Versus AUC in Healthy Subjects & OAB Patientsy j
Hg 40
Systolic Blood Pressure Afternoon in Patients / 6h Post‐dose in HV
Hg 40
Systolic Blood Pressure Morning in Patients / Pre‐dose (24h) in HV
baselin
e, m
mH
0
20
baselin
e, m
mH
0
20
Chan
ge from
‐40
‐20
Chan
ge from
‐40
‐20
AUC, ng.h/mL0 1000 2000 3000 4000 5000
AUC, ng.h/mL0 1000 2000 3000 4000 5000
OAB patients; 50mgOAB patients; 25, 100, 200 mgHealthy volunteers; 25, 50, 100, 200, 300 mgOAB patients; all doses (25, 50,100, 200 mg)HV; all doses (25, 50, 100, 200, 300 mg)
178‐PK‐02217

Hypertension Adverse Events Based on SPA Criteria:Prospectively Applied in Phase 3 Protocols
12‐Week Phase 3 Studies
Long‐Term (52‐Week) Controlled Study
Mi b
Placebo(n = 1380)
Mirabegron 50 mg
(n = 1375)
Mirabegron
Tolterodine(n = 812)
50 mg(n = 812)
100 mg(n = 820)
Patients with any 117 (8 5%) 120 (8 7%) 89 (11 0%) 83 (10 1%) 86 (10 6%)
1 Average SBP >140 mm Hg and/or average DBP >90 mm Hg at 2 consecutive
Patients with any hypertension AE 117 (8.5%) 120 (8.7%) 89 (11.0%) 83 (10.1%) 86 (10.6%)
1. Average SBP >140 mm Hg and/or average DBP >90 mm Hg at 2 consecutive post‐baseline visits for patients normotensive at baseline
2. Average increase in SBP >20 mm Hg and/or average increase in DBP >10 mm Hg at 2 consecutive post‐baseline visits for patients hypertensive at baselineg p p yp
3. Initiation of treatment for hypertension or an increase in dose of anti‐hypertensive medication
18

ConclusionsConclusions
• Effects of adrenergic and anti‐muscarinic drugsEffects of adrenergic and anti muscarinic drugs on vital signs are larger in young adults typically used in phase 1 and clinical pharmacology studies p p gythan in older patients.
• To characterize the effects of such drugs inTo characterize the effects of such drugs in patients it is better to make the measurements in patients rather than in younger healthy subjects, p y g y jor if healthy subjects are used age‐match them to the patients.
7/18/2012 CSRC BP Thinktank 19

AcknowledgementsAcknowledgements
• Astellas colleagues: Mike Allen, Mary Beth Blauwet,Astellas colleagues: Mike Allen, Mary Beth Blauwet, Paul de Koning, Leticia Delgado‐Herrera, William Fitzsimmons, Marcel van Gelderen, Virginie Kerbusch‐Herben, Salim Mujais, Steve Ryder
• Reviewers at PMDA, FDA and EMA with whom we interacted during review of the NDA for mirabegron.
7/18/2012 CSRC BP Thinktank 20

Back‐up
7/18/2012 CSRC BP Thinktank 21

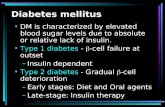
Phase 1 (Healthy Volunteers) Not Representative of Phase 2/3 (OAB Patients) Vital Sign Measurements
MenWomen
220
1A. Maximum heart rate decreases with age
e (bpm
)200
180
ximal Heart Rate 180
160
Max
140
120
Age (year)
10 20 30 40 50 60 70 80 90
1B. Adrenergic responsiveness to Beta‐agonist decreases with age
Tanaka, et al, 2001; Stratton et al. 1992; Kitzman and Taffet 2009
• Cardiovascular responses to isoproterenol were reduced in healthy older men compared to younger men: heart rate, systolic and diastolic blood pressures
22

Phase 1 (Healthy Volunteers) Not Representative of Phase 2/3 (OAB Patients) Vital Sign Measurements
S d Di l Ph d i Eff f Mi b S d SSteady Diurnal Pharmacodynamic Effect of Mirabegron at Steady State Little diurnal fluctuation in vital sign pharmacodynamic effect of mirabegron
PK Study 178‐CL‐031*20
TQT Study 178‐CL‐077*20
m placebo
(mmHg)
n = 12
15
10
5
Q y
n = 83
m placebo
(mmHg)
15
10
SBP Differen
ce from 5
‐5
0
Mirabegron 50 mg
SBP Differen
ce from 5
‐5
0
Mirabegron 50 mg
(mmHg) Long‐Term (52‐Week) Controlled Study (ABPM)
15
20
S 0 5 10Time, h
20 2515 S
Time, h0 5 10 15 20 25
rence from
Baseline
(95%
CI)
‐10
‐5
0
5
10
n = 21
SBP Diffe
0 5 10 15 20 25Dose Hour
‐20
‐15
10
* Adapted from the FDA Background Document Dated 16 March 2012
Mirabegron 50 mg
23

12‐Week Phase 3 StudiesChange from Baseline to Final Visit Pulse (Patient Diary)
AM BPMn Baseline
Placebo 1329 70.5
25 mg mirabegron 410 71.0
50 mg mirabegron 1327 70.4
100 mg mirabegron 891 70.4
Tolterodine 476 69.8
PM BPMn Baseline
Placebo 1326 75.3
25 mg mirabegron 410 75.5
50 mg mirabegron 1327 74.9
100 mg mirabegron 890 74.4
Tolterodine 476 73.9
Adjusted Mean Changefrom Baseline (95% CI)
‐1.0 0.0 1.0 2.0 3.0
Mean Differencevs Placebo (95% CI)
‐1.0 0.0 1.0 2.0 3.0
24

Long‐Term (52‐Week) Controlled StudyChange from Baseline to Final Visit Pulse (Patient Diary)
AM BPMn Baseline
50 mg mirabegron 791 71.0
100 mg mirabegron 802 70.2
Tolterodine 792 70.1
PM BPMPM BPM
50 mg mirabegron 789 74.2
100 mg mirabegron 802 74.1
Tolterodine 792 73.8
1 0 0 0 1 0 2 0 3 0
Adjusted Mean Change from Baseline (95% CI)
‐1.0 0.0 1.0 2.0 3.0
25

Regression Analysis of Exposure Response for Pulse
0 mg
25 mg
50 mg 200 mg
100 mg
26

Categorical Analysis of Pulse12‐Week Phase 3 Studies
n (%) of PatientsPlaceboN = 1380
Mirabegron 50 mgN = 1375
Pulse AM (n =1196) (n = 1202)3 Consecutive Post-Baseline Visits
Change from baseline ≥ 2 BPM 171 (14.3%) 247 (20.5%)Change from baseline ≥ 5 BPM 77 (6.4%) 87 (7.2%)Change from baseline ≥ 10 BPM 13 (1.1%) 13 (1.1%)Change from baseline ≥ 15 BPM 4 (0 3%) 2 (0 2%)Change from baseline ≥ 15 BPM 4 (0.3%) 2 (0.2%)
Long‐term (52‐Week) Controlled Study
n (%) of Patients
MirabegronTolterodine
N = 81250 mg
N = 812100 mgN = 820
Pulse AM (n = 686) (n = 704) (n = 683)( ) ( ) ( )3 Consecutive Post-Baseline Visits
Change from baseline ≥ 2 BPM 179 (26.1%) 268 (38.1%) 217 (31.8%)Change from baseline ≥ 5 BPM 69 (10.1%) 112 (15.9%) 87 (12.7%)Change from baseline ≥ 10 BPM 14 (2 0%) 20 (2 8%) 19 (2 8%)Change from baseline ≥ 10 BPM 14 (2.0%) 20 (2.8%) 19 (2.8%)Change from baseline ≥ 15 BPM 6 (0.9%) 1 (0.1%) 2 (0.3%)
27

Tachycardia (AE and Pulse)
12 W k Ph 3 St di L t (52 W k) C t ll d St d12‐Week Phase 3 Studies Long‐term (52‐Week) Controlled Study
n (%) of PatientsPlacebo(n = 1380)
Mirabegron Mirabegron
Tolterodine(n = 812)
50 mg(n = 1375)
50 mg(n = 812)
100 mg(n = 820)
Any occurrence of tachycardia 43 (3.1%) 52 (3.8%) 25 (3.1%) 49 (6.0%) 53 (6.5%)
Tachycardia as AE 9 (0.7%) 18 (1.3%) 10 (1.2%) 19 (2.3%) 26 (3.2%)
T h diTachycardia as pulse ≥ 100 bpm 36 (2.6%) 39 (2.8%) 19 (2.3%) 35 (4.3%) 32 (3.9%)
Tachycardia as AE and pulse ≥ 100 bpm
2 (0.1%) 5 (0.4%) 4 (0.5%) 5 (0.6%) 5 (0.6%)bpm
28