Analytical Challenges Developing an Ultrasensitive …...2020/06/20 · Analytical Challenges...
1
Analytical Challenges Developing an Ultrasensitive Simoa Immunoassay for IL-1β as a Biomarker for NASH S. Kar, S. Jaycox, S. Paglialunga, and R. Islam Bioanalytical Sciences, Celerion, Lincoln, NE USA IL-1 β concentrations in 62 incurred samples measured by the Simoa assay did not increase with increased hepatic steatosis or fibrosis as measured by Fibroscan suggesting it cannot be used for trial inclusion/exclusion criteria. Novel Aspect This is the first reported use of an ultrasensitive technology to accurately measure IL-1 β in NASH. While IL-1 β did not correlate with NASH severity for trial inclusion, it may be a useful biomarker for other COUs like target engagement. The challenges of sensitivity, lipemia, and incurred sample analysis are applicable to other NASH biomarker studies. For example, extraction of lipemia is necessary when using the Simoa platform to improve reproducibility and LipoClear did not decrease IL-1 β recovery. Finally, this study demonstrates the need for fit-for-purpose validation based on COU to drive biomarker bioanalytical validation. The decision to measure incurred NASH samples during bioanalytical validation allowed early recognition that IL-1 β did not fit a prognostic biomarker COU before study sample analysis. Introduction There is imperative need for non-invasive biomarkers for non-alcoholic steatohepatitis (NASH). Proinflammatory cytokines promote progression of NASH and are potential biomarkers. IL-1 β , a cytokine produced by inflammasome mediated cell death, induces hepatic inflammation. Antagonists of IL-1 β and inflammasome are under development. Thus, IL-1 β could be a prognostic and target engagement biomarker for NASH drug development. We hypothesized serum IL-1 β increases with disease severity and developed an immunoassay for IL-1 β for a context-of-use (COU) of a prognostic biomarker for patient stratification during NASH trial enrollment. Lipids, Diet, Oxidative Stress Kupffer Cell/ macrophage Inflammation and NASH Inflammasome Activation IL-1β and Inflammasome antagonists IL-1β IL-1β Methods We developed a biomarker work plan for an IL-1 β immunoassay for this COU. Table 1. Biomarker Work Plan for IL-1 β Parameter Requirements Analyte IL-1 β Context of Use Determine if IL-1 β is a biomarker of patient selection, I/E criteria, or prognostic enrichment of steatosis and fibrosis and thus appropriate for inclusion in NASH drug development clinical trials. De Novo or Commercial Kit Kit preferred if enough sensitivity Reference Material Kit material Concentration Range (Normal –> Disease) Below 1 pg/mL expected based on extrapolated ECL values and literature with increase in NASH. Ultrasensitive immunoassay needed. Sample Matrix and Volume Serum Sample Number and Study Length 100-200 samples over 2 years Biological Considerations and Variability Lipemia expected in NASH serum. Measure incurred NASH samples in validation. Commercial Kit Adaptations Test sensitivity, lipemia, endogenous lipemic QC M SD ECL Simo a 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 Extrapolated values. Several values below detection range LLOQ (2.56 pg/mL) LLOQ (0.11 pg/mL) Challenge #1: Sensitivity Lipemic NASH Serum Clear Serum Challenge #2: Precision and Lipemic Sample Interference IL-1 (pg/mL) IL-1 (pg/mL) Challenge #3: Performance of Biomarker for Patient Selection COU In our previous measurements of IL-1 β in human serum with electrochemiluminescence (ECL), 69% of clinical samples were below the limit of quantification (LLOQ). The limited clinical studies which measured IL-1 β reported values below the LLOQ. Therefore, we developed an ultrasensitive immunoassay by converting an IL-1 β commercial kit for the Quanterix Simoa SRX benchtop platform. We optimized buffers to lower noise and determined a minimum required dilution (MRD) of 1:2 minimized matrix interference while maintaining assay sensitivity. Since NASH patients typically have metabolic syndrome, we anticipated challenges with lipemia during sample collection and handling and challenges with reproducibility from experience with bead-based assays. Finally, we assayed incurred samples during validation from an enrollment study which screened patients for NASH by non-invasive Fibroscan transient elastography imaging to determine if our assay fit the COU. Results The Simoa IL-1 β assay demonstrated low background and 25-fold increased sensitivity (LLOQ of 0.110 pg/mL vs. 2.56 pg/mL with ECL after accounting for MRD). 48 of 62 incurred samples were above the LLOQ compared to only 20 with ECL. While Simoa improved sensitivity, most of our incurred samples were grossly lipemic which had higher coefficient of variation (%CV >50%) between replicates compared to non-lipemic serum. Sample dilution to overcome lipemia could not be used due to loss of sensitivity. We extracted lipids from NASH serum with LipoClear, a non-ionic polymer that binds and precipitates lipids. Addition of the buffer reduced %CV to less than 30% for incurred samples without impacting recovery. We also increased acceptance criteria for %CV to 30% which was acceptable for our COU. Sample %CV Before Treatment %CV After Treatment 1 (Non-Lipemic) 9.90 9.30 2 (Non-Lipemic) 5.88 4.78 3 (Lipemic) 39.9 15.2 4 (Lipemic) 57.4 10.2 IL-1β Sensitivity in Human Serum Immunoassay Platform % Recovery High QC Low QC Lipemia level High Mid Low High Mid Low Sample 1 59 82 92 68 77 89 Sample 2 88 85 93 79 87 91 NASH Serum IL-1β Liver Fat Liver Fibrosis NASH Serum IL-1β Table 2. Lipemic Sample Treatment Improves Precision with Simoa Platform Table 3. Lipemic Sample Treatment Maintains Analyte Recovery
Transcript of Analytical Challenges Developing an Ultrasensitive …...2020/06/20 · Analytical Challenges...

Analytical Challenges Developing an Ultrasensitive Simoa Immunoassay for IL-1β as a Biomarker for NASHS. Kar, S. Jaycox, S. Paglialunga, and R. IslamBioanalytical Sciences, Celerion, Lincoln, NE USA
IL-1β concentrations in 62 incurred samples measured by the Simoa assay did not increase with increased hepatic steatosis or fibrosis as measured by Fibroscan suggesting it cannot be used for trial inclusion/exclusion criteria.
Novel AspectThis is the first reported use of an ultrasensitive technology to accurately measure IL-1β in NASH. While IL-1β did not correlate with NASH severity for trial inclusion, it may be a useful biomarker for other COUs like target engagement.
The challenges of sensitivity, lipemia, and incurred sample analysis are applicable to other NASH biomarker studies. For example, extraction of lipemia is necessary when using the Simoa platform to improve reproducibility and LipoClear did not decrease IL-1β recovery.
Finally, this study demonstrates the need for fit-for-purpose validation based on COU to drive biomarker bioanalytical validation. The decision to measure incurred NASH samples during bioanalytical validation allowed early recognition that IL-1β did not fit a prognostic biomarker COU before study sample analysis.
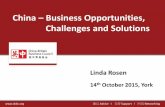
IntroductionThere is imperative need for non-invasive biomarkers for non-alcoholic steatohepatitis (NASH). Proinflammatory cytokines promote progression of NASH and are potential biomarkers.
IL-1β, a cytokine produced by inflammasome mediated cell death, induces hepatic inflammation. Antagonists of IL-1β and inflammasome are under development. Thus, IL-1β could be a prognostic and target engagement biomarker for NASH drug development.
We hypothesized serum IL-1β increases with disease severity and developed an immunoassay for IL-1β for a context-of-use (COU) of a prognostic biomarker for patient stratification during NASH trial enrollment.
Lipids, Diet, Oxidative Stress
Kupffer Cell/ macrophageInflammation and
NASH
Inflammasome Activation
IL-1β and Inflammasome antagonists
IL-1β
IL-1β
MethodsWe developed a biomarker work plan for an IL-1β immunoassay for this COU.
Table 1. Biomarker Work Plan for IL-1β
Parameter Requirements
Analyte IL-1β
Context of Use Determine if IL-1β is a biomarker of patient selection, I/E criteria, or prognostic enrichment of steatosis and fibrosis and thus appropriate for inclusion in NASH drug development clinical trials.
De Novo or Commercial Kit Kit preferred if enough sensitivity
Reference Material Kit material
Concentration Range (Normal –> Disease) Below 1 pg/mL expected based on extrapolated ECL values and literature with increase in NASH. Ultrasensitive immunoassay needed.
Sample Matrix and Volume Serum
Sample Number and Study Length 100-200 samples over 2 years
Biological Considerations and Variability Lipemia expected in NASH serum. Measure incurred NASH samples in validation.
Commercial Kit Adaptations Test sensitivity, lipemia, endogenous lipemic QC
MSD E
CL
Simoa
0.0
0.5
1.0
1.52.02.53.03.54.0
Extrapolatedvalues. Severalvalues belowdetection range
LLOQ(2.56 pg/mL)
LLOQ(0.11 pg/mL)
Challenge #1: Sensitivity
Lipemic NASH Serum Clear Serum
Challenge #2: Precision and Lipemic Sample Interference
IL-1
(p
g/m
L)
IL-1
(p
g/m
L)
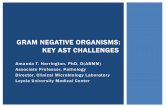
Challenge #3: Performance of Biomarker for Patient Selection COUIn our previous measurements of IL-1β in human serum with electrochemiluminescence (ECL), 69% of clinical samples were below the limit of quantification (LLOQ). The limited clinical studies which measured IL-1β reported values below the LLOQ. Therefore, we developed an ultrasensitive immunoassay by converting an IL-1β commercial kit for the Quanterix Simoa SRX benchtop platform. We optimized buffers to lower noise and determined a minimum required dilution (MRD) of 1:2 minimized matrix interference while maintaining assay sensitivity.
Since NASH patients typically have metabolic syndrome, we anticipated challenges with lipemia during sample collection and handling and challenges with reproducibility from experience with bead-based assays. Finally, we assayed incurred samples during validation from an enrollment study which screened patients for NASH by non-invasive Fibroscan transient elastography imaging to determine if our assay fit the COU.
Results
The Simoa IL-1β assay demonstrated low background and 25-fold increased sensitivity (LLOQ of 0.110 pg/mL vs. 2.56 pg/mL with ECL after accounting for MRD). 48 of 62 incurred samples were above the LLOQ compared to only 20 with ECL.
While Simoa improved sensitivity, most of our incurred samples were grossly lipemic which had higher coefficient of variation (%CV >50%) between replicates compared to non-lipemic serum. Sample dilution to overcome lipemia could not be used due to loss of sensitivity. We extracted lipids from NASH serum with LipoClear, a non-ionic polymer that binds and precipitates lipids. Addition of the buffer reduced %CV to less than 30% for incurred samples without impacting recovery. We also increased acceptance criteria for %CV to 30% which was acceptable for our COU.
Sample %CV Before Treatment %CV After Treatment
1 (Non-Lipemic) 9.90 9.30
2 (Non-Lipemic) 5.88 4.78
3 (Lipemic) 39.9 15.2
4 (Lipemic) 57.4 10.2
IL-1β Sensitivity in Human Serum
Immunoassay Platform
% Recovery
High QC Low QC
Lipemia level High Mid Low High Mid Low
Sample 1 59 82 92 68 77 89
Sample 2 88 85 93 79 87 91
NASH Serum IL-1β
Liver Fat Liver Fibrosis
NASH Serum IL-1β
Table 2. Lipemic Sample Treatment Improves Precision with Simoa Platform
Table 3. Lipemic Sample Treatment Maintains Analyte Recovery