Ablation percutanée et nouvelles stratégies ... -...
50
Ablation percutanée et nouvelles stratégies thérapeutiques du CHC : l’avènement des dispositifs micro-ondes de seconde génération sonne t’il le glas de la radiofréquence ? Olivier Seror Radiologie, Hôpital Jean Verdier, Bondy, AP-HP/Paris XIII
-
Upload
duongthien -
Category
Documents
-
view
213 -
download
0
Transcript of Ablation percutanée et nouvelles stratégies ... -...
Ablation percutanée et nouvelles stratégies thérapeutiques du CHC : l’avènement des dispositifs micro-ondes de seconde génération sonne t’il le glas de la radiofréquence ?
Olivier Seror Radiologie, Hôpital Jean Verdier, Bondy, AP-HP/Paris XIII
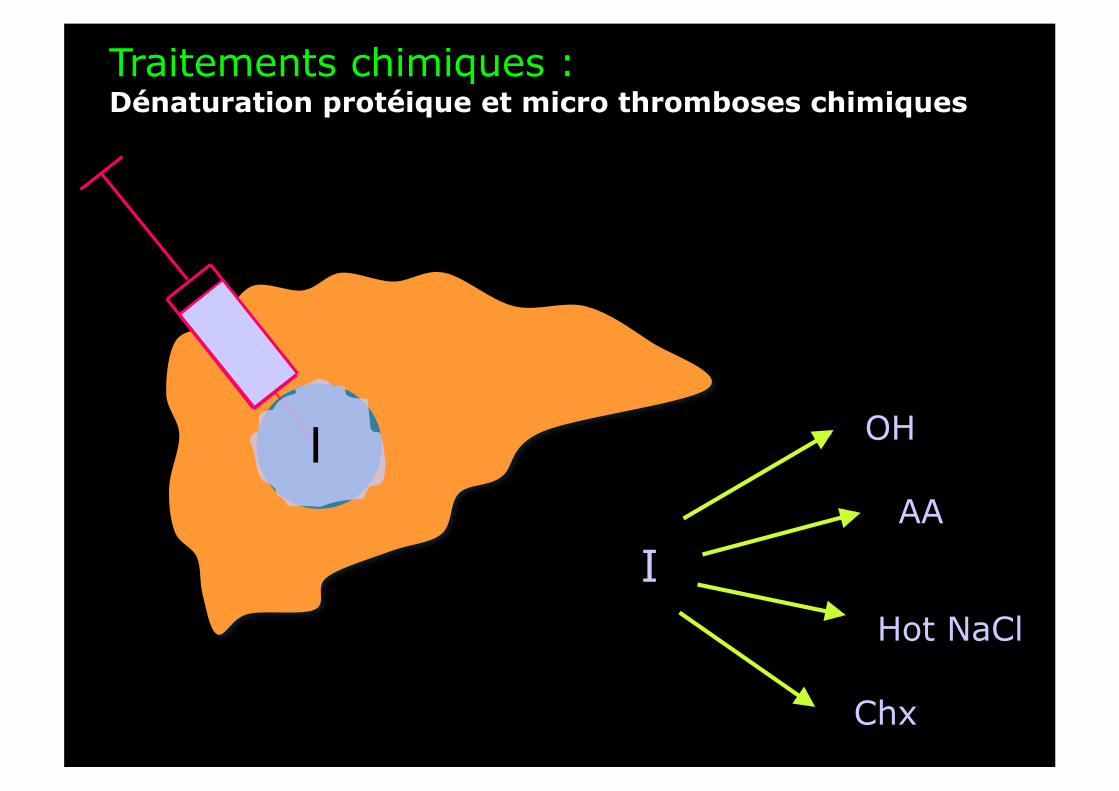
Traitements chimiques : Dénaturation protéique et micro thromboses chimiques
I OH
AA
Hot NaCl
Chx
I
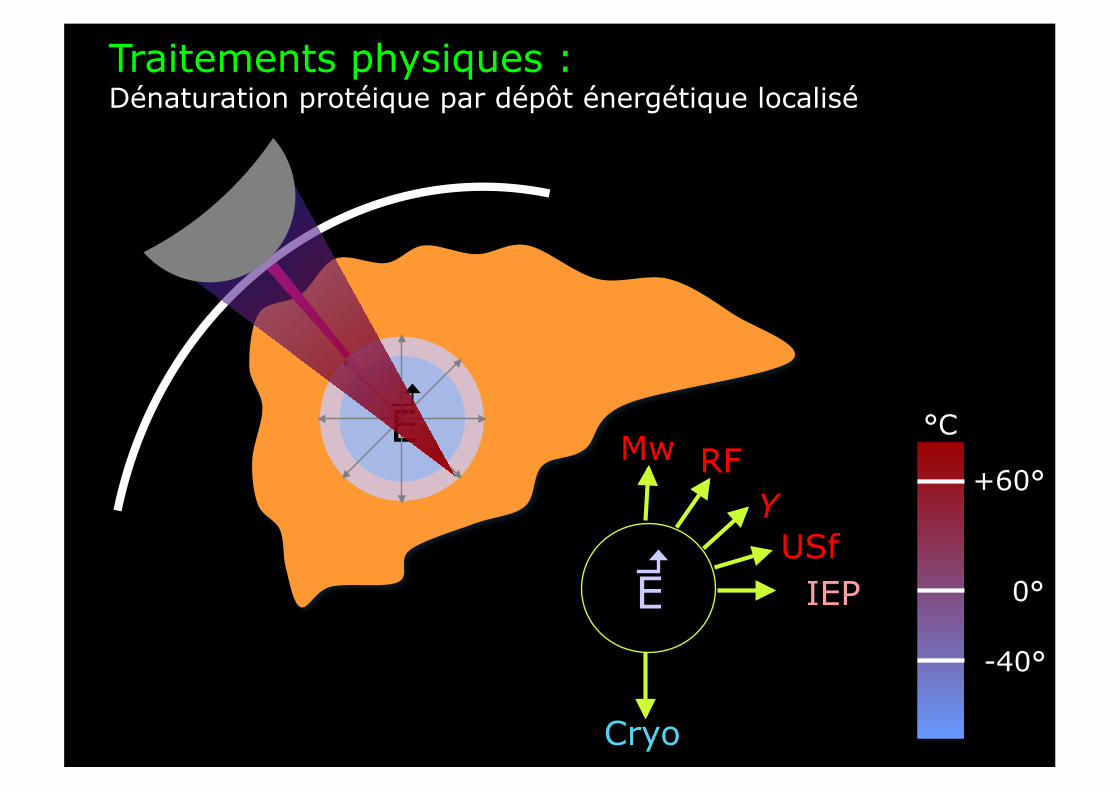
Υ
Cryo
RF Mw
IEP
E
Traitements physiques : Dénaturation protéique par dépôt énergétique localisé
USf E 0°
+60°
-40°
°C
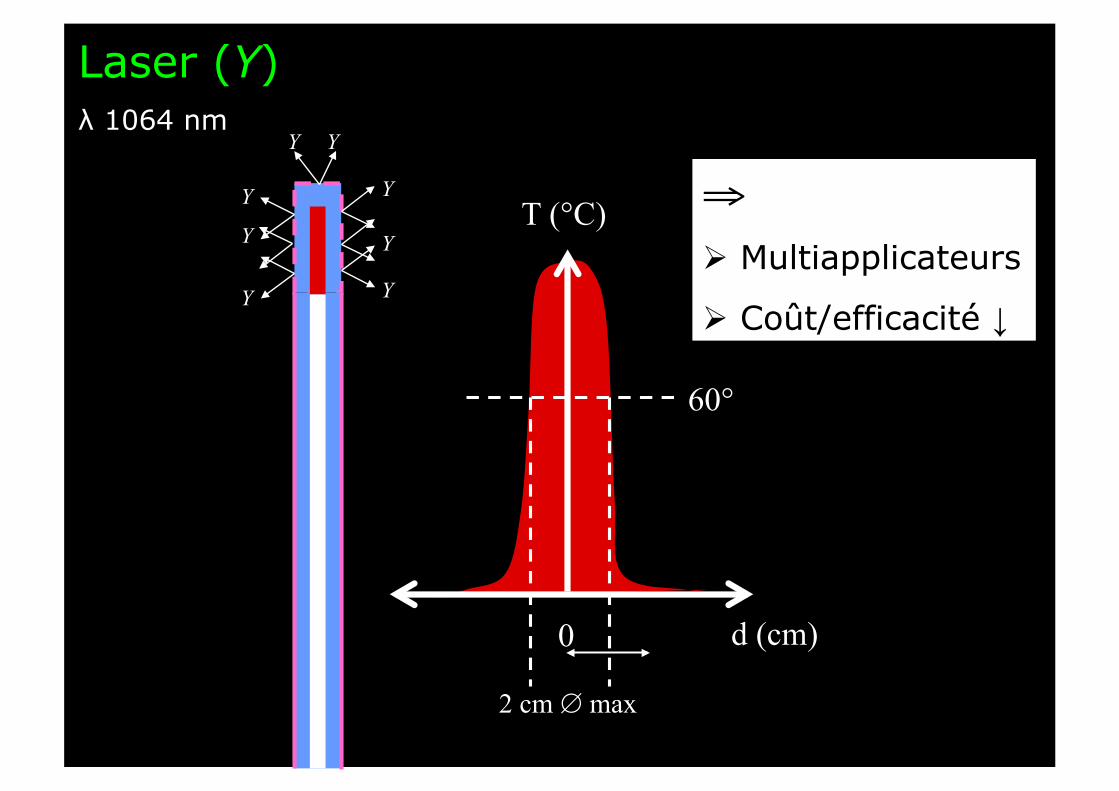
Laser (Υ) λ 1064 nm
Υ
Υ
Υ
Υ
Υ Υ
Υ
Υ
⇒ Multiapplicateurs
Coût/efficacité ↓
0 d (cm)
T (°C)
2 cm ∅ max
60°
- 40°
- 20°
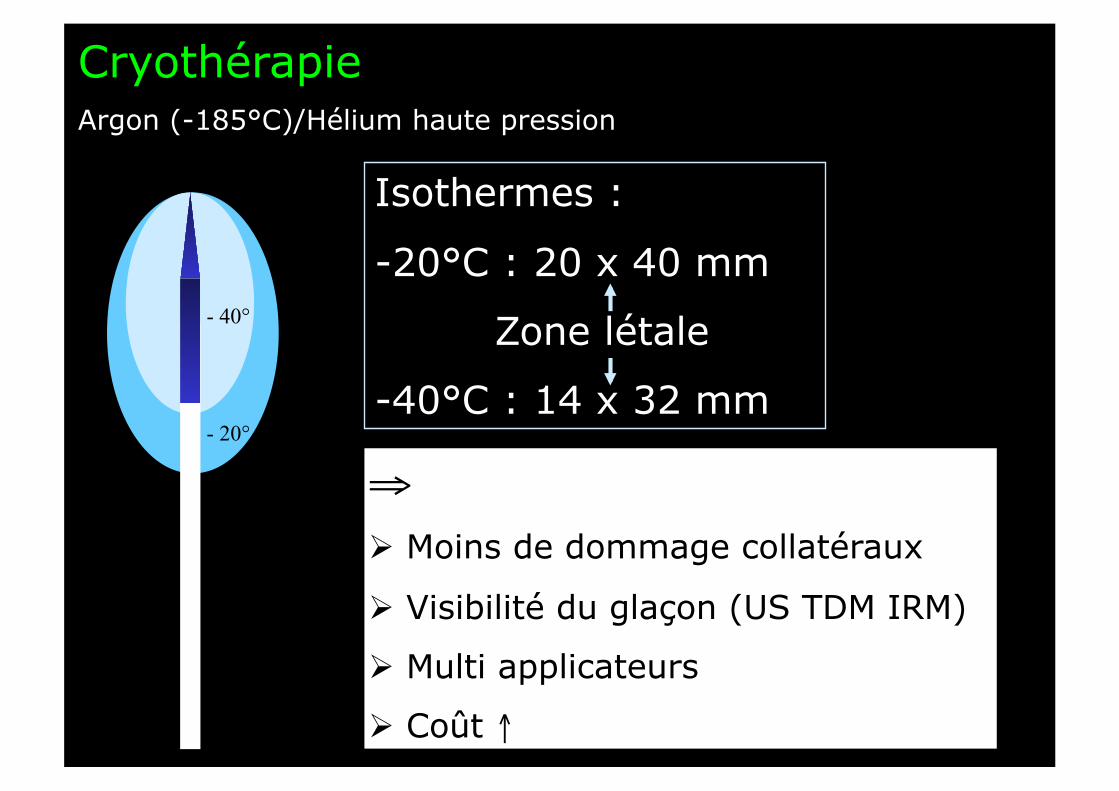
Cryothérapie Argon (-185°C)/Hélium haute pression
⇒ Moins de dommage collatéraux
Visibilité du glaçon (US TDM IRM)
Multi applicateurs
Coût ↑
Isothermes :
- 20°C : 20 x 40 mm
Zone létale
- 40°C : 14 x 32 mm

--
++
++
--
Mw 915/2450MHz
O H H
O H H
O H H
O H H
O H H
O H H
O H H
O H H
⇒ Rapide
Très (trop) efficace
Coût ↑
M
++
--
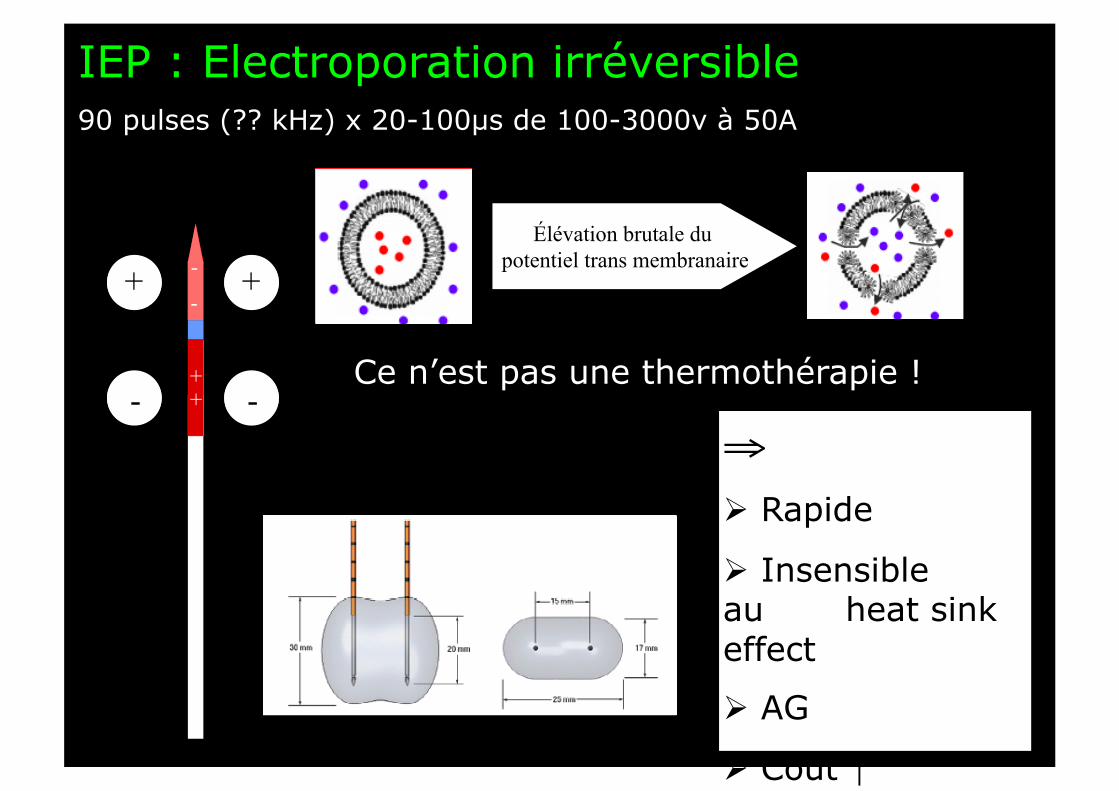
IEP : Electroporation irréversible 90 pulses (?? kHz) x 20-100µs de 100-3000v à 50A
++
--
-
+
-
+ -
+
-
+ Élévation brutale du
potentiel trans membranaire
Ce n’est pas une thermothérapie !
⇒ Rapide
Insensible au . heat sink effect
AG
Coût ↑
CHC : Indication princeps
• Tumeur ≤ 3 cm
• ≤ 3 nodules
• Inopérable (cirrhose)

Randomized controlled trials
PEI/RF
Palliative treatments
New agents Sorafenib
BCLC (AASLD) 2005
Stades 0 et A
Child-Pugh A-B
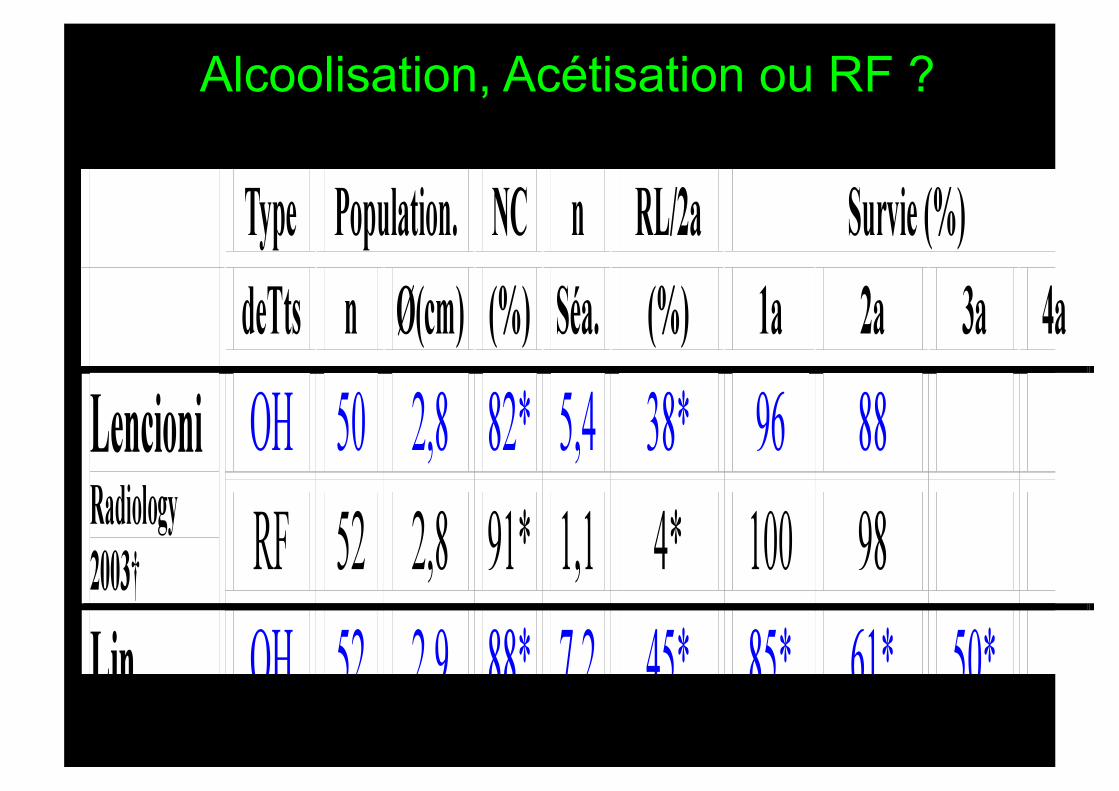
Alcoolisation, Acétisation ou RF ?
Randomized controlled trials
PEI/RF
Palliative treatments
RF New agents Sorafenib
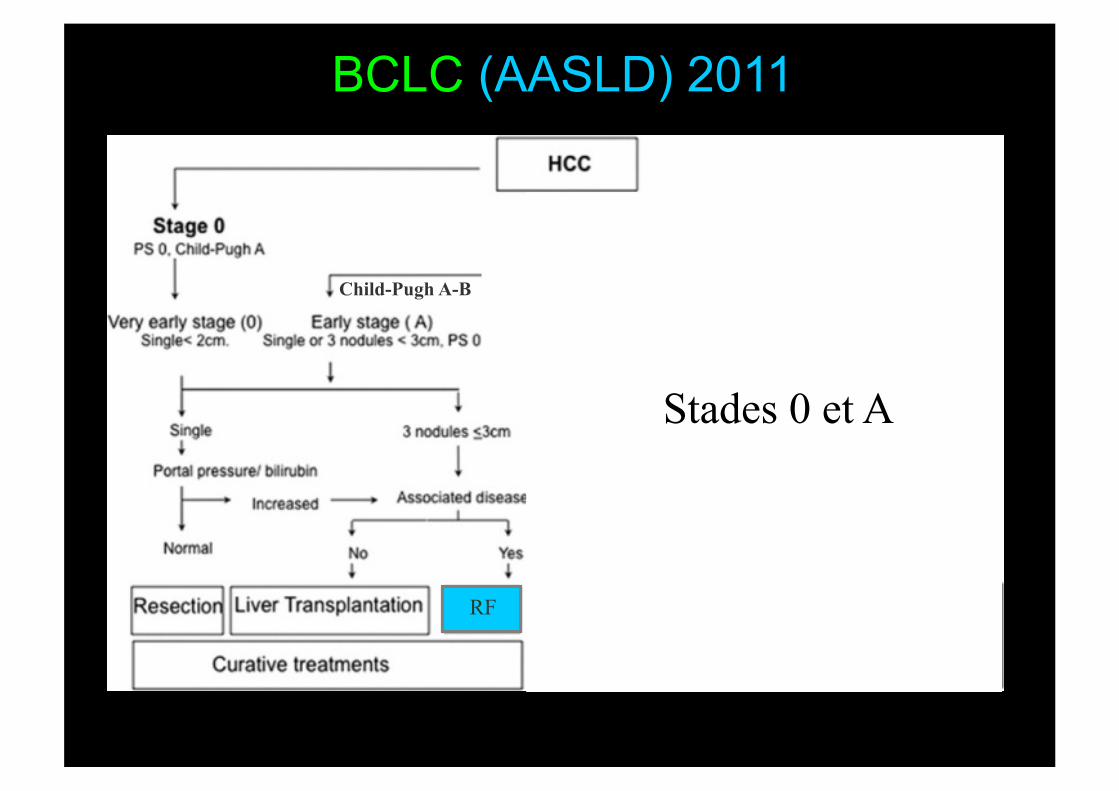
BCLC (AASLD) 2011
Stades 0 et A
Child-Pugh A-B
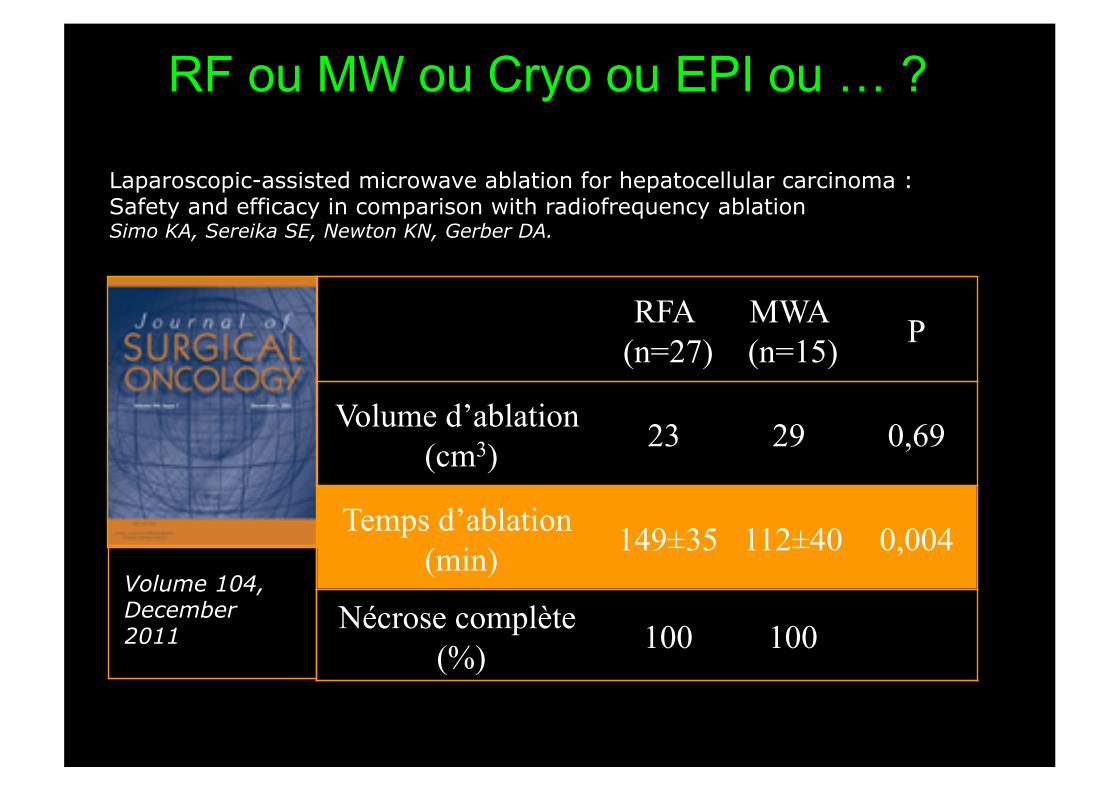
RF ou MW ou Cryo ou EPI ou … ?
Laparoscopic-assisted microwave ablation for hepatocellular carcinoma : Safety and efficacy in comparison with radiofrequency ablation Simo KA, Sereika SE, Newton KN, Gerber DA.
RFA (n=27)
MWA (n=15) P
Volume d’ablation (cm3) 23 29 0,69
Temps d’ablation (min) 149±35 112±40 0,004
Nécrose complète (%) 100 100
Volume 104, December 2011
Randomized controlled trials
PEI/RF
Palliative treatments
RF New agents Sorafenib
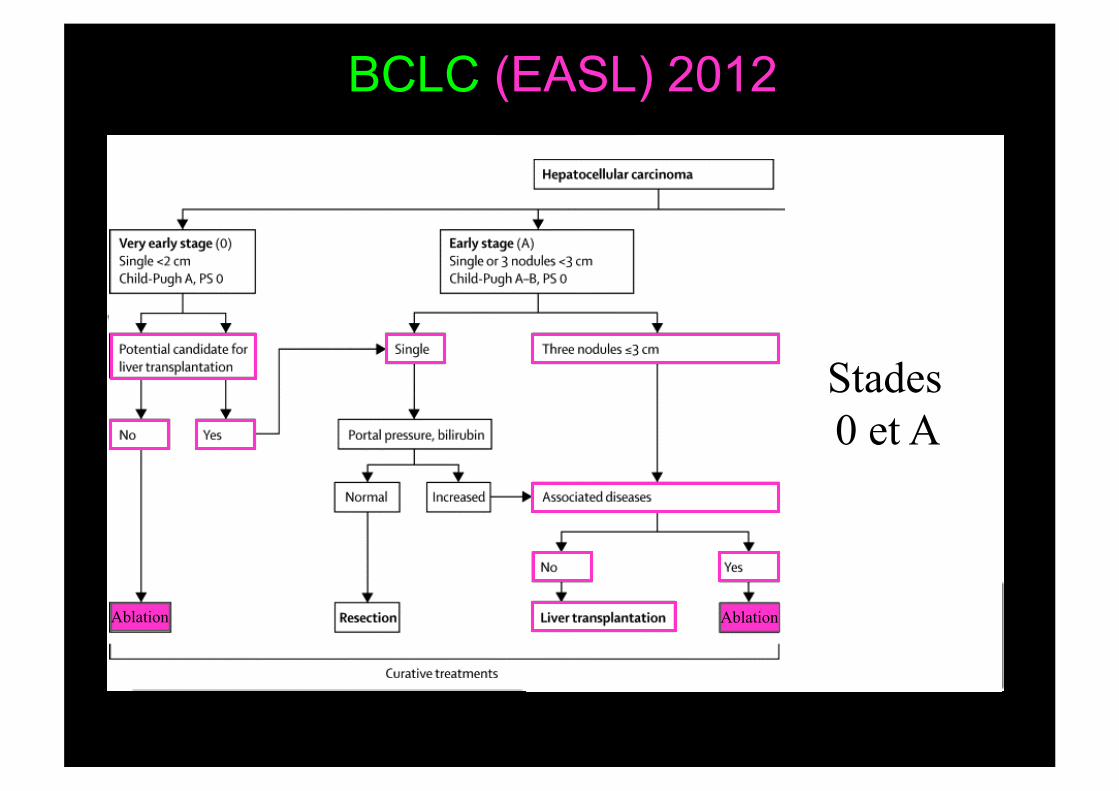
BCLC (EASL) 2012
Stades 0 et A
Child-Pugh A-B
Ablation Ablation
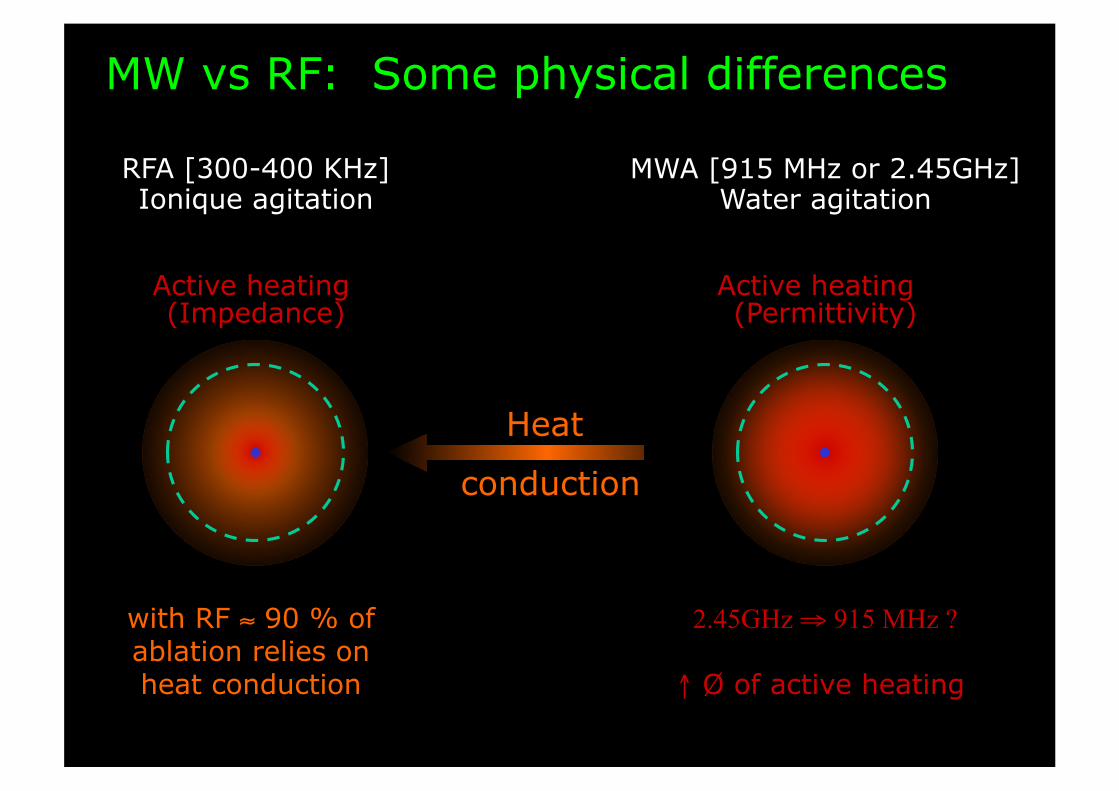
MW vs RF: Some physical differences
RFA [300-400 KHz] Ionique agitation
Active heating (Impedance)
MWA [915 MHz or 2.45GHz] Water agitation
Active heating (Permittivity)
Heat
conduction
2.45GHz ⇒ 915 MHz ?
↑ Ø of active heating
with RF ≈ 90 % of ablation relies on heat conduction
MWA is less controllable on lesion size
Generates detrimental backward heating
…
MWA versus RFA: Some (potential) disadvantages
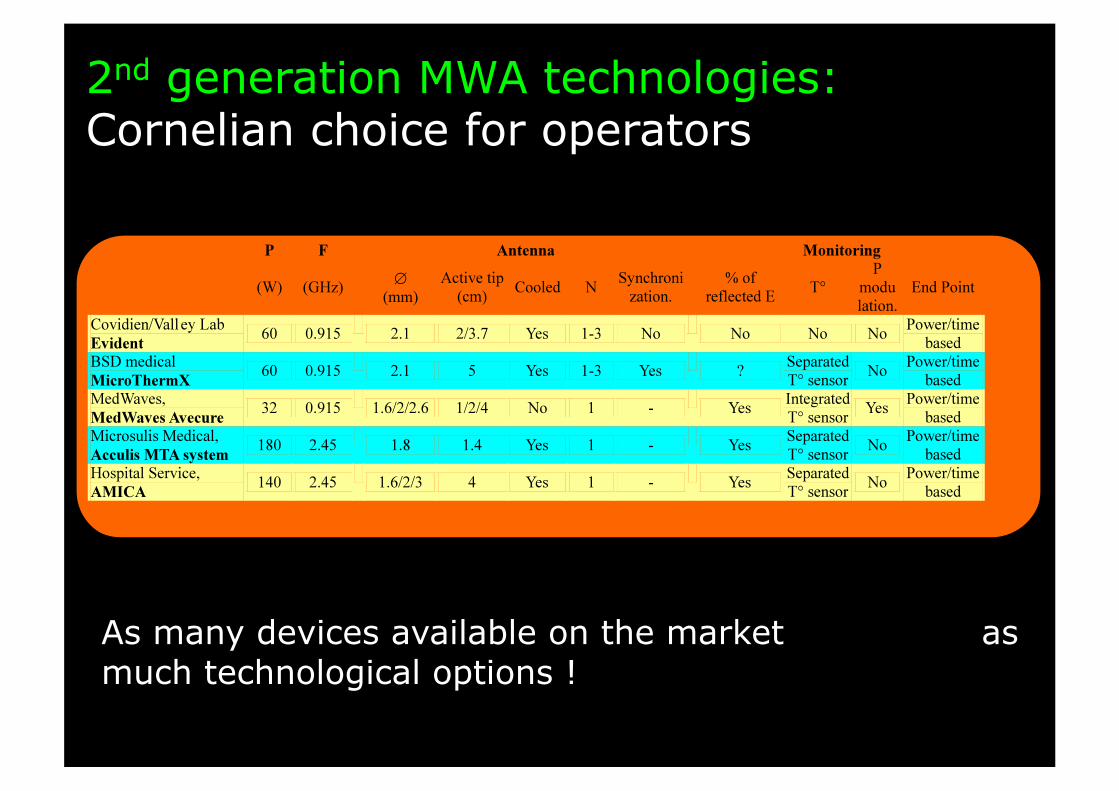
As many devices available on the market as much technological options !
2nd generation MWA technologies: Cornelian choice for operators
Sizes of ablation area Long & small axis
mm
10
20
30
40
50
60
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis Small axis
N = 24 N = 20 N = 29
Long axis along probes’ axis
Retraction (up to 40% !)
mm
10
20
30
40
50
60
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis Small axis
N = 24 N = 20 N = 29
Sizes of ablation area Long & small axis / Application time
2.45 GHz 180W
915 MHz 32W
2.45 GHz 130W
Average 3.7±1.9min 6.9±4min 7.2±5min
mm
10
20
30
40
50
60
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis/ Applicat° time
Small axis/ Applicat° time
N = 24 N = 20 N = 29
Sizes of ablation area Long & small axis

Sizes of ablation area Long & small axis / antenna repositioning
2.45 GHz 180W
915 MHz 32W
2.45 GHz 130W
Average 1.7±1 1.6±1 1.4±0.7
mm
10
20
30
40
50
60
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis Small axis
N = 24 N = 20 N = 29
mm
10
20
30
40
50
60
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis/ N positioning
Small axis/ N positioning
N = 24 N = 20 N = 29
Sizes of ablation area Long & small axis
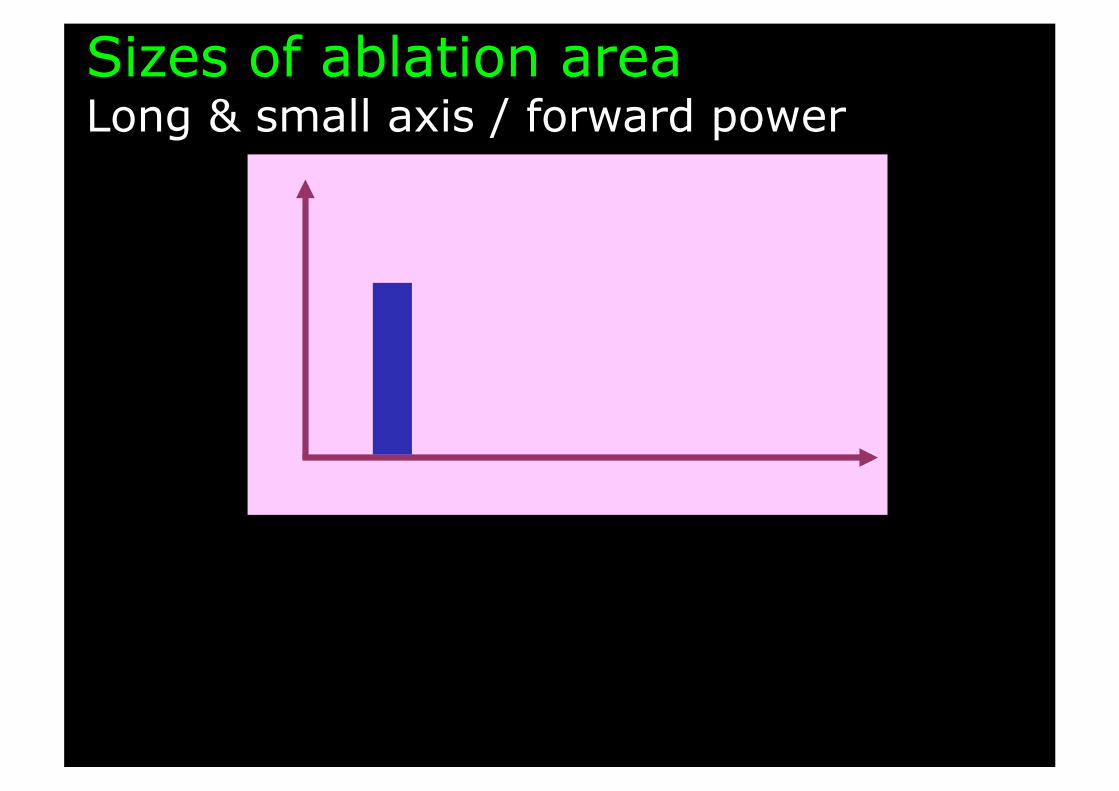
Sizes of ablation area Long & small axis / forward power
mm
10
20
30
40
50
60
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis Small axis
N = 24 N = 20 N = 29
2.45 GHz 180W
915 MHz 32W
2.45 GHz 130W
Average 160±30W 30±1,6W 60±16W
mm.10-2
20 40
60
80
100
120
2.45 GHz 180 W
915 MHz 32 W
2.45 GHz 130 W
Long axis/ Forward power
Small axis/ Forward power
N = 24 N = 20 N = 29 140
Sizes of ablation area Long & small axis
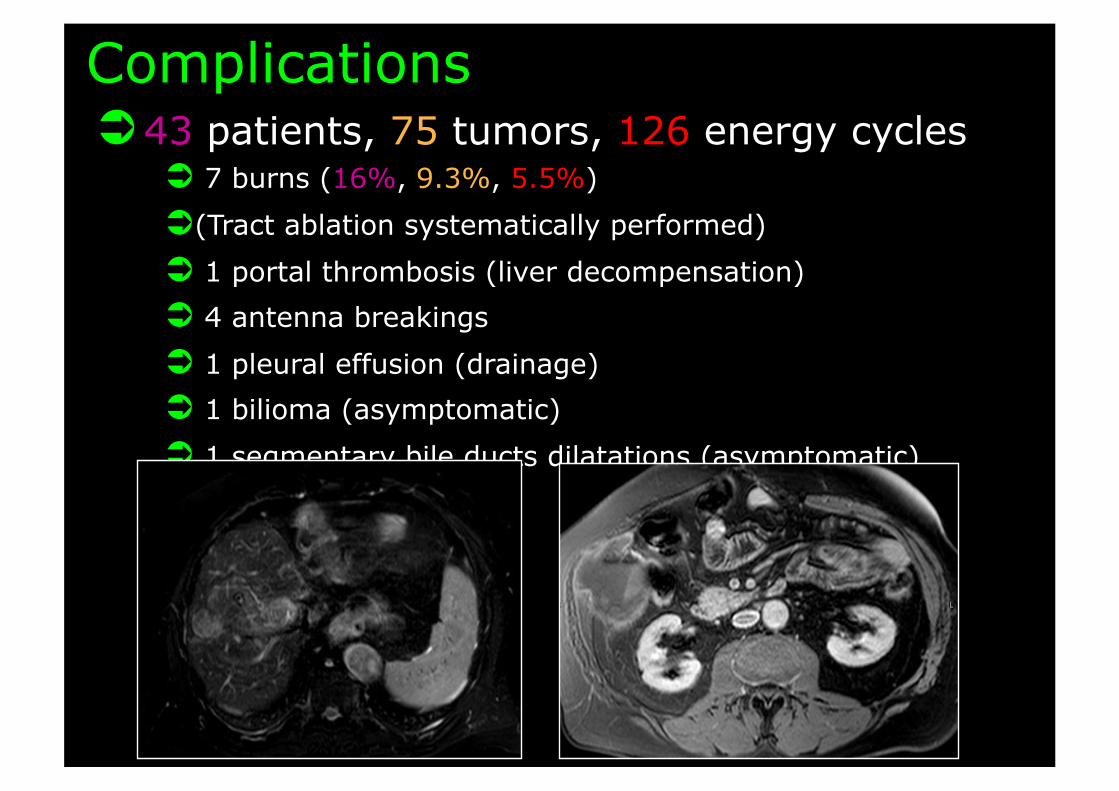
Complications 43 patients, 75 tumors, 126 energy cycles
7 burns (16%, 9.3%, 5.5%)
(Tract ablation systematically performed)
1 portal thrombosis (liver decompensation)
4 antenna breakings
1 pleural effusion (drainage)
1 bilioma (asymptomatic)
1 segmentary bile ducts dilatations (asymptomatic)

A worse safety profile than RFA
Complications : RF vs MW
Mortality Major Morbidity
Minor Morbidity
Thermal damages
Mechanical damages
MWA N = 736 Livraghi, CVIR 2011
0% 2.9% 7.3% 3.8% 1.9%
RFA N = 2320 Livraghi, Radiology 2003
0.3% 2.4% 5% 0.3% 0.5%
3 main causal factors Induction of fast and less controlled ablation area no effective protective procedures inside the 2 cm active heating area!
Burns along transmission line due to backward energy Less protective effect of blood flow
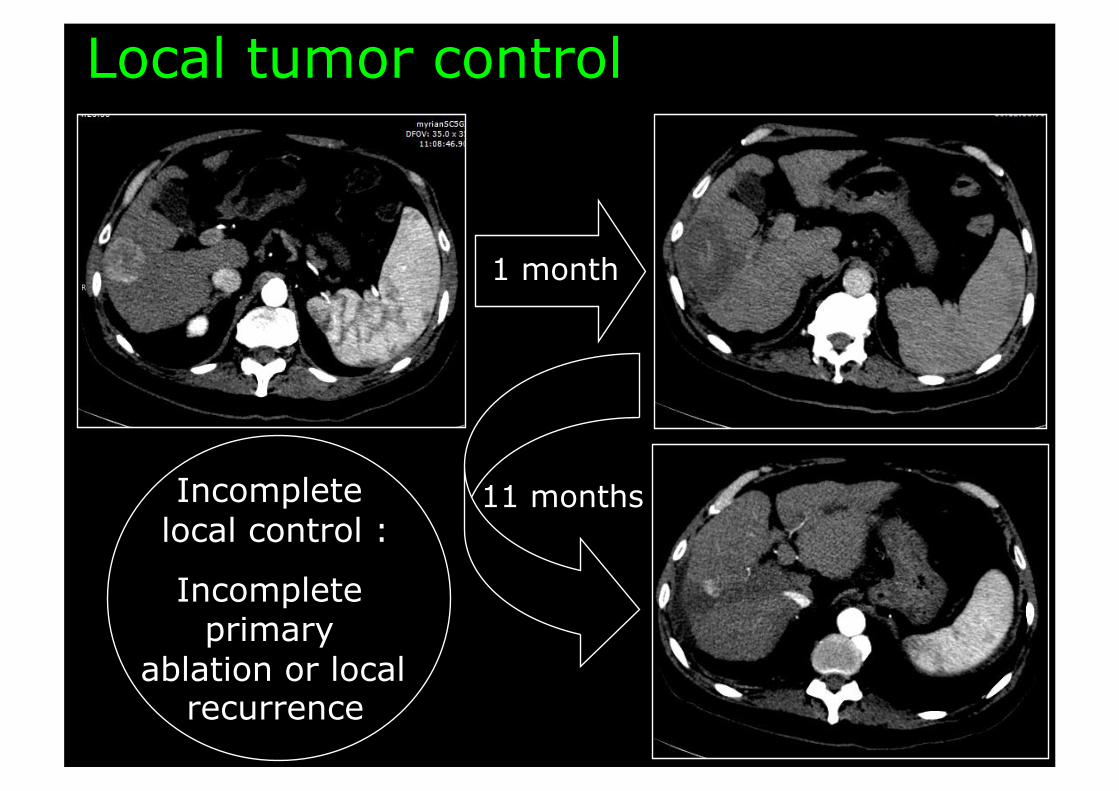
Local tumor control
1 month
11 months Incomplete local control :
Incomplete primary
ablation or local recurrence
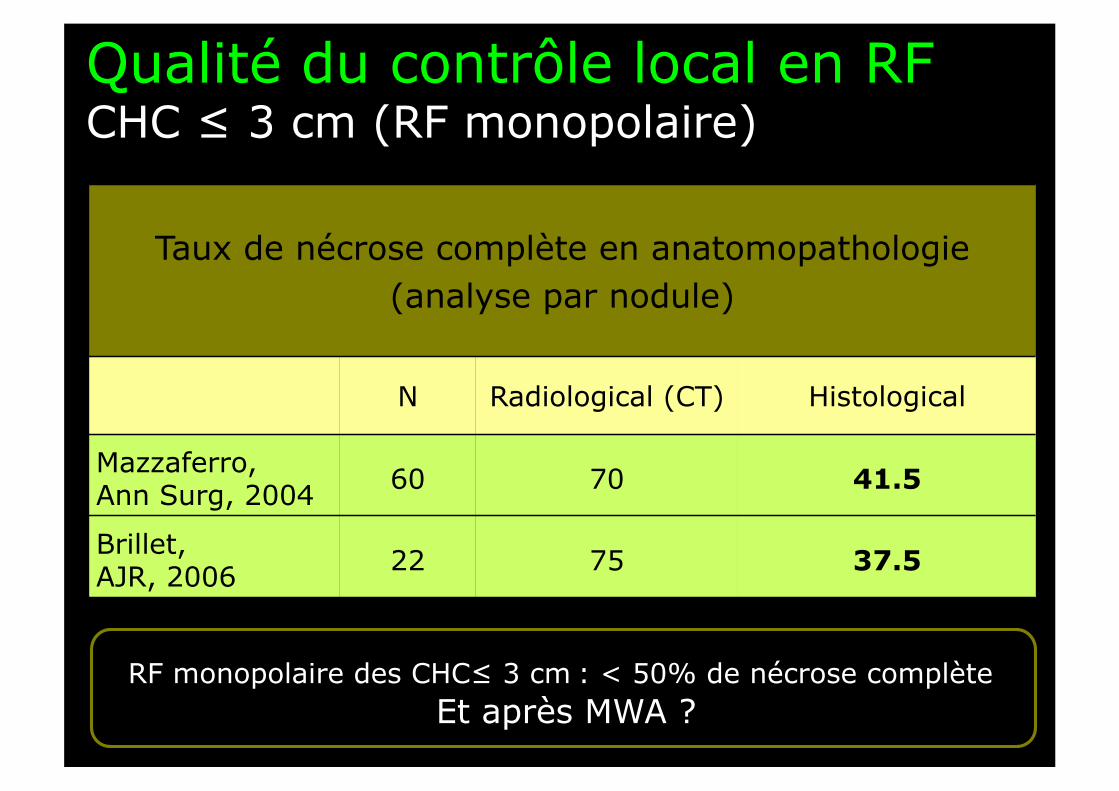
Taux de nécrose complète en anatomopathologie (analyse par nodule)
N Radiological (CT) Histological
Mazzaferro, Ann Surg, 2004 60 70 41.5
Brillet, AJR, 2006 22 75 37.5
RF monopolaire des CHC≤ 3 cm : < 50% de nécrose complète Et après MWA ?
Qualité du contrôle local en RF CHC ≤ 3 cm (RF monopolaire)
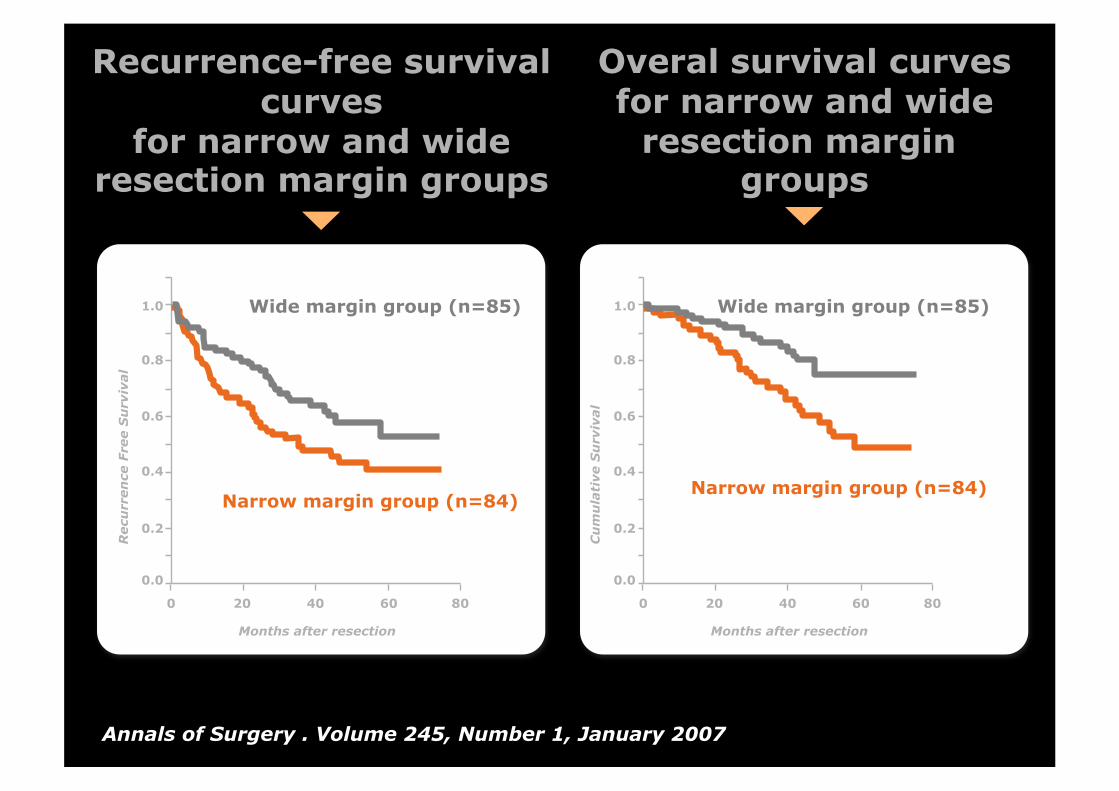
Annals of Surgery . Volume 245, Number 1, January 2007
Recurrence-free survival curves
for narrow and wide resection margin groups
0.0
0.2
0.4
0.6
0.8
1.0
Recu
rren
ce F
ree S
urv
ival
0 20 40 60 80
Months after resection
Wide margin group (n=85)
Narrow margin group (n=84)
Overal survival curves for narrow and wide
resection margin groups
0.0
0.2
0.4
0.6
0.8
1.0
Cu
mu
lati
ve S
urv
ival
0 20 40 60 80
Months after resection
Wide margin group (n=85)
Narrow margin group (n=84)

In your opinion what should be the best way to perform in situ thermal ablation of a malignant liver tumor? First option: from the center to the periphery
Second option: from the periphery to the center
Learn from liver oncologic surgery practice …

Intra tumoral RFA
Technologie RF : mono vs multipolaire
Ablation margins Quite predicable Poorly predicable
Spread of heating Centripetal Centrifugal
No touch RFA
From single to multi applicators and
multipolar devices
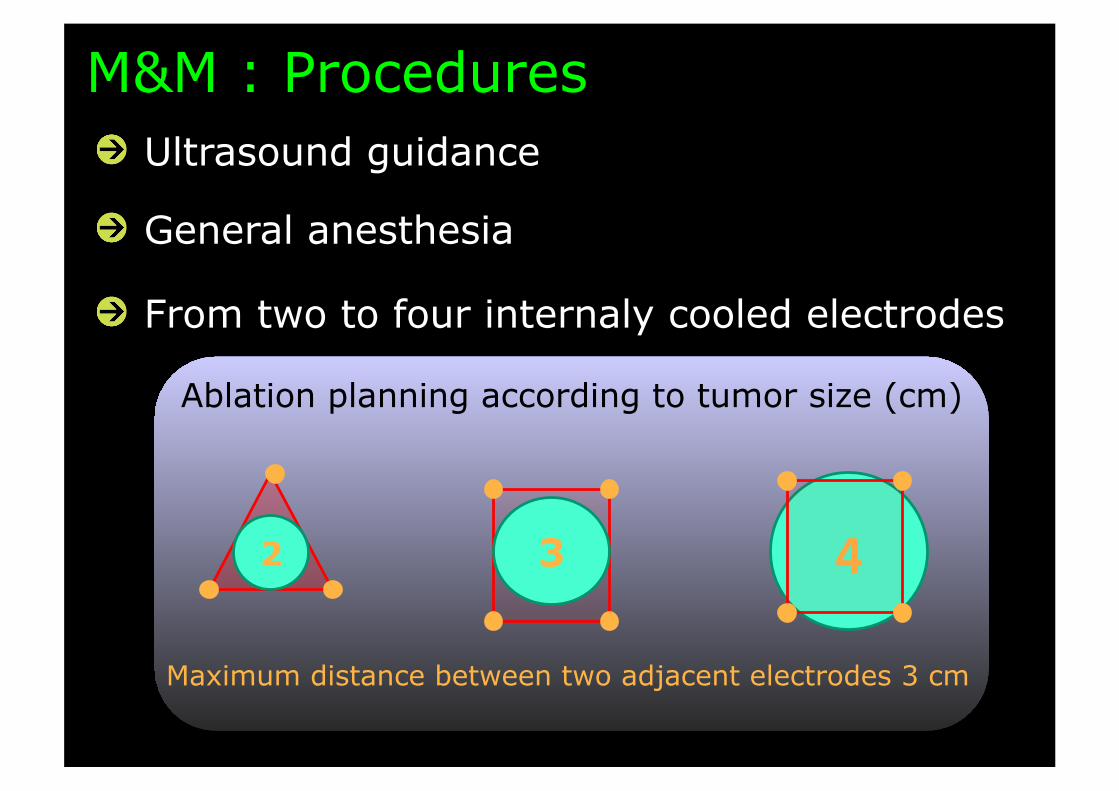
Ablation planning according to tumor size (cm)
M&M : Procedures
" Ultrasound guidance
" General anesthesia
" From two to four internaly cooled electrodes
4 3 2
Maximum distance between two adjacent electrodes 3 cm
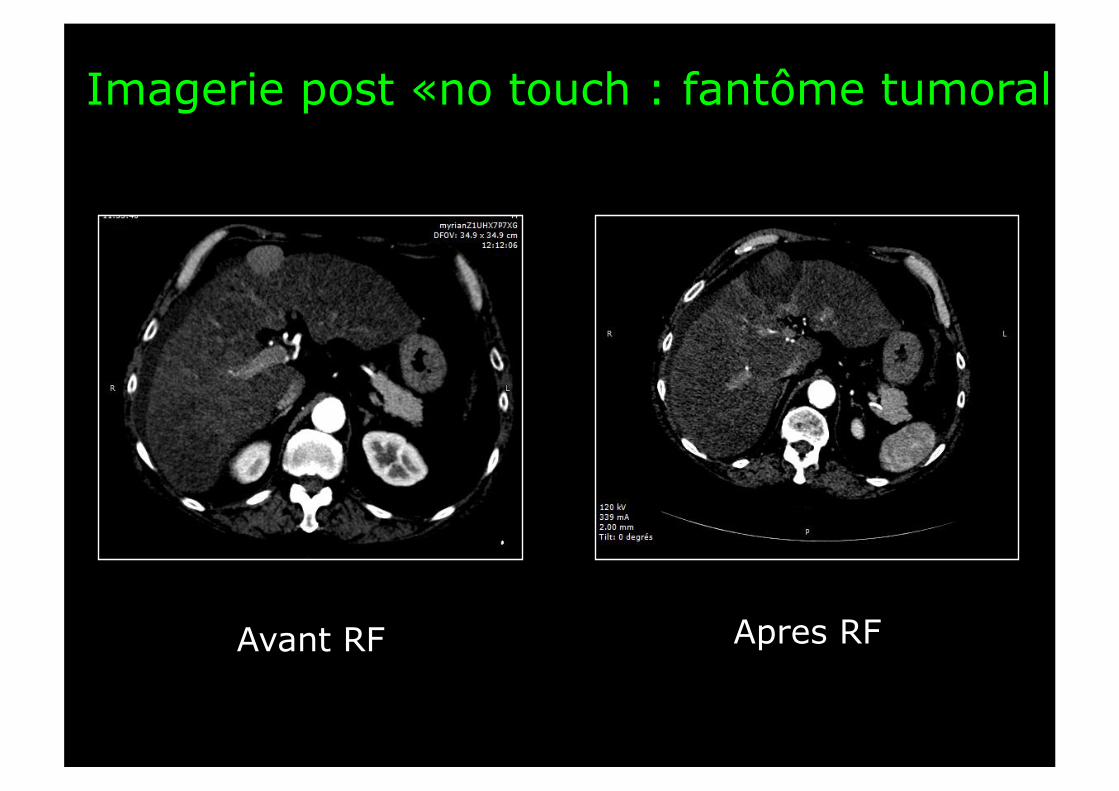
Imagerie post «no touch : fantôme tumoral
Avant RF Apres RF

Histologie post «no touch : Safety Margin
Avant RF Apres RF
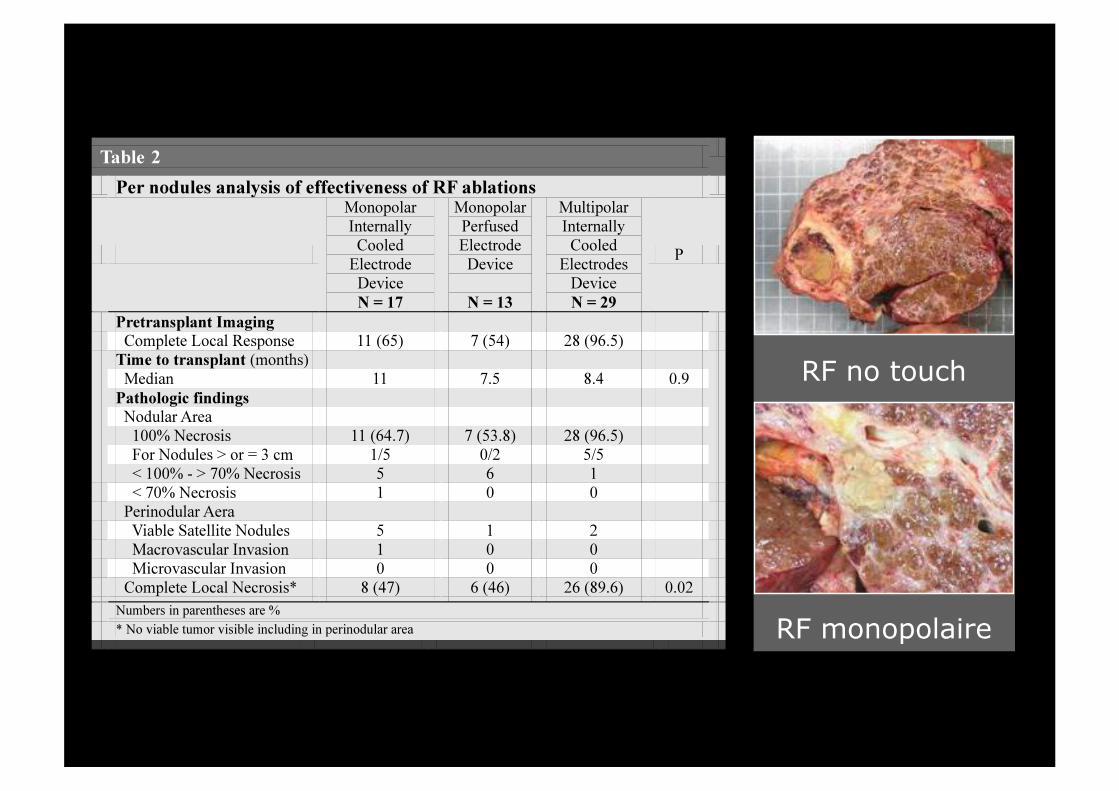
RF no touch
RF monopolaire
BCLC (EASL) 2012
Randomized controlled trials Palliative treatments
New agents Sorafenib
Stades 0 et A
PEI/RF RF
Child-Pugh A-B
Ablation Ablation
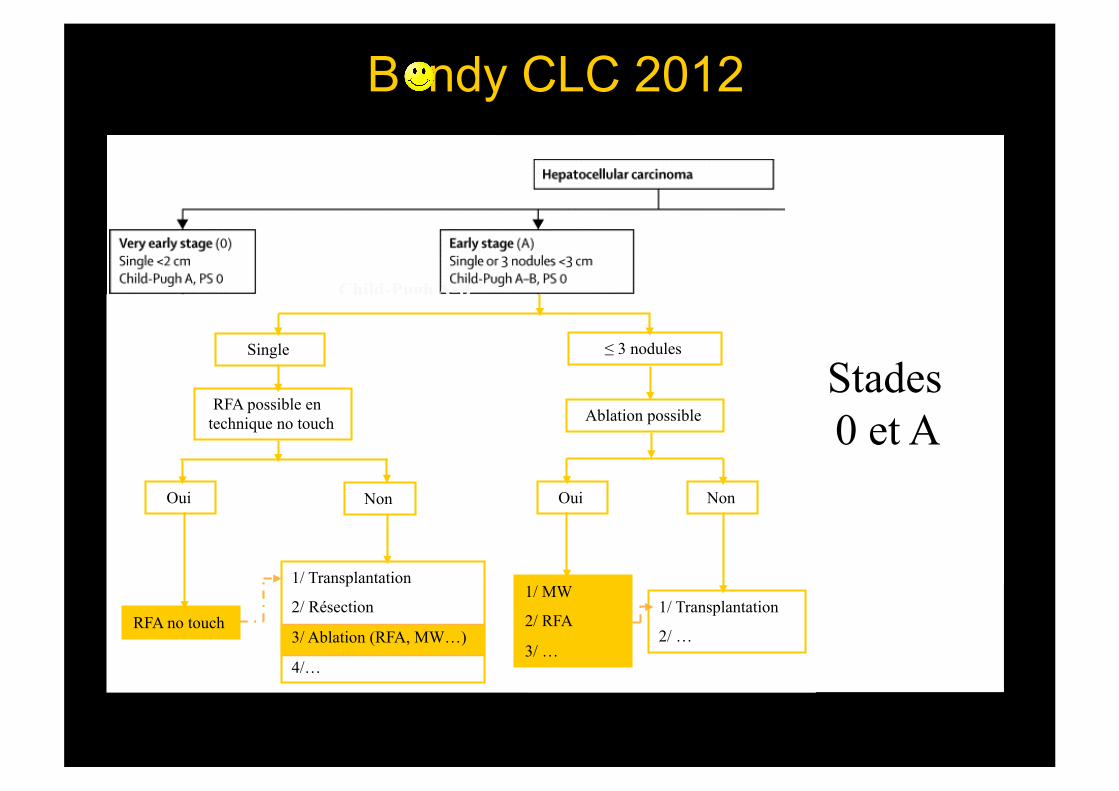
RFA possible en technique no touch
Single
Oui Non
RFA no touch
1/ Transplantation
2/ Résection
3/ Ablation (RFA, MW…)
4/…
Ablation possible
≤ 3 nodules
Oui Non
1/ MW
2/ RFA
3/ …
1/ Transplantation
2/ …
B ndy CLC 2012
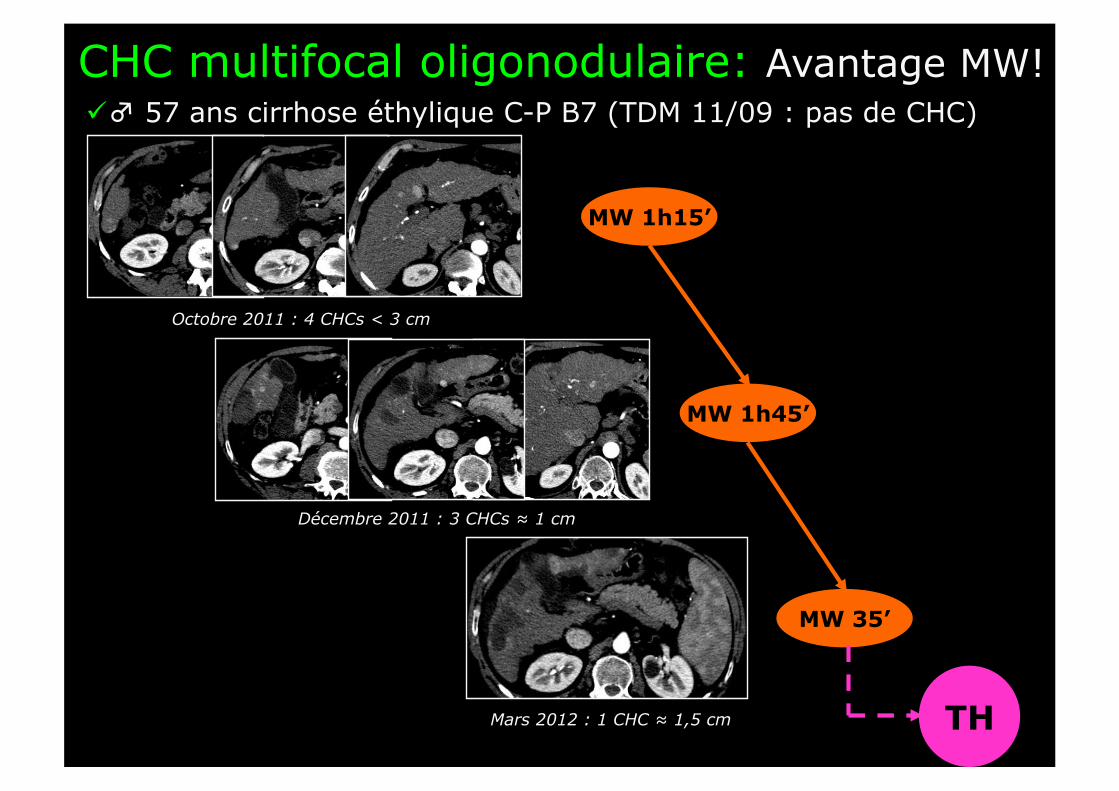
CHC multifocal oligonodulaire: Avantage MW! ♂ 57 ans cirrhose éthylique C-P B7 (TDM 11/09 : pas de CHC)
Octobre 2011 : 4 CHCs < 3 cm
Décembre 2011 : 3 CHCs ≈ 1 cm
Mars 2012 : 1 CHC ≈ 1,5 cm
MW 1h45’
MW 35’
MW 1h15’
TH
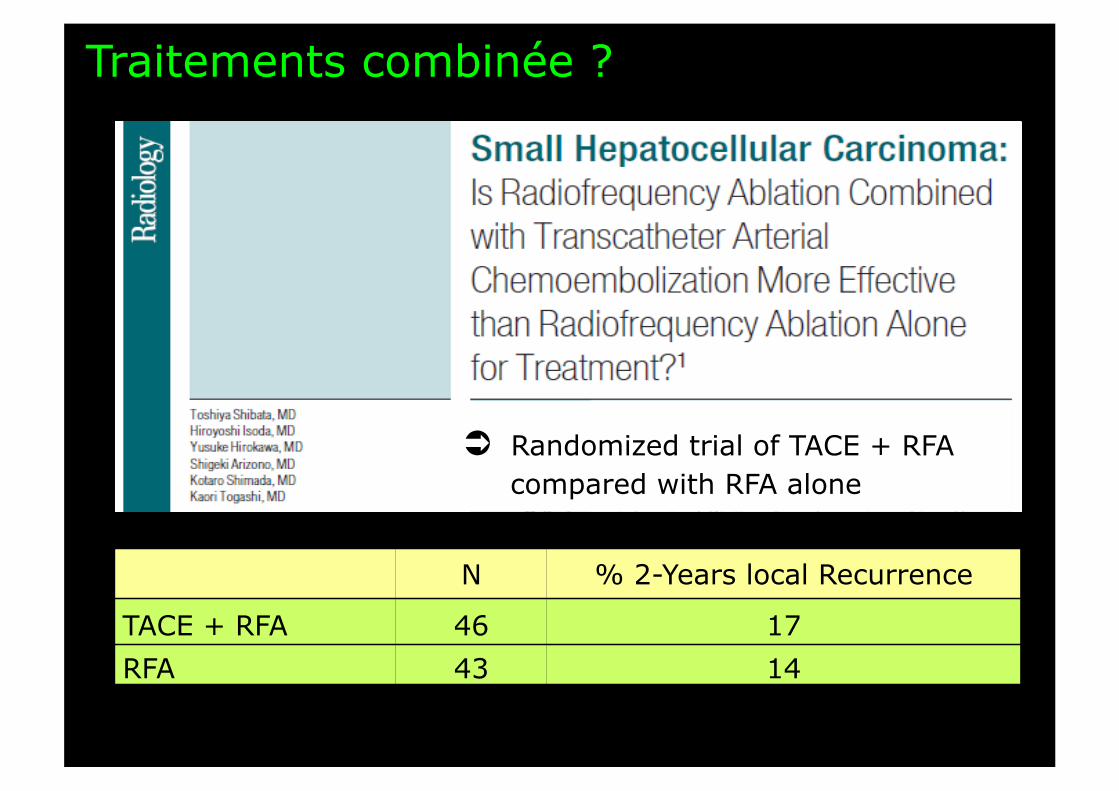
Traitements combinée ?
N % 2-Years local Recurrence
TACE + RFA 46 17 RFA 43 14
Randomized trial of TACE + RFA compared with RFA alone

Combinaison des technologies d’ablation ? ♂ 71 ans cirrhose post HVC C-P B6
Nov. 11 : 3 CHCs < 3,5 cm Dec. 11 : reliquat préportal MW Mar. 12 : 0 CHC actif visible IEP
Et les « gros » CHC ?
• Tumeur ≥ 5 cm
• Tumeur infiltrante
• Extension portale (intra hépatique)
• Inopérables +++
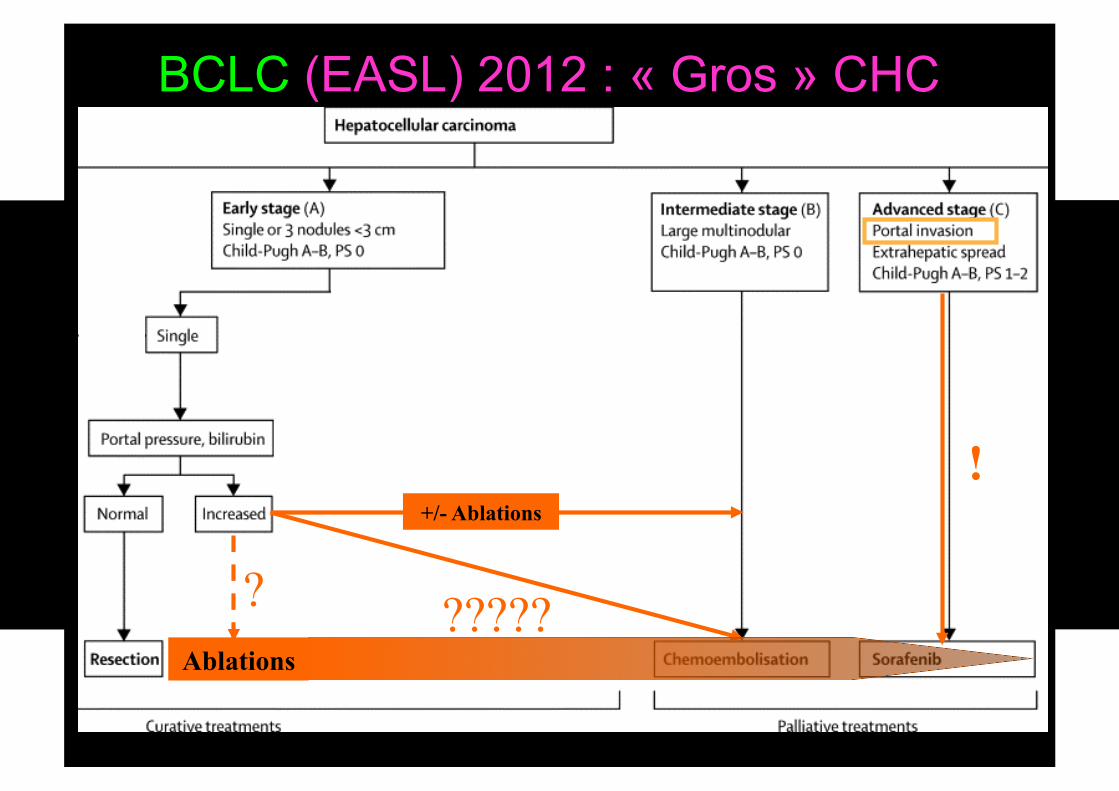
BCLC (EASL) 2012 : « Gros » CHC
+/- Ablations
!
Ablations
? ?????

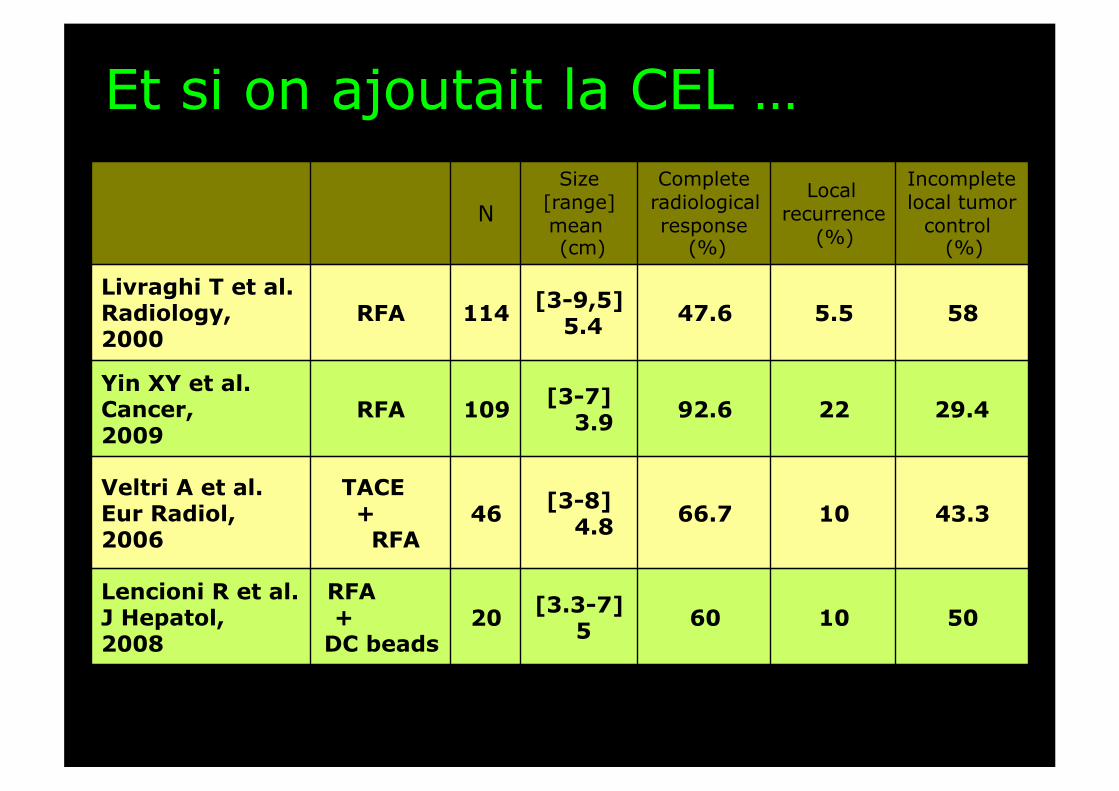
RF monopolaire du gros CHC
N Size
[range] mean (cm)
Complete radiological response
(%)
Local recurrence
(%)
Incomplete local tumor
control (%)
Livraghi T et al. Radiology, 2000
RFA 114 [3-9,5] 5.4 47.6 5.5 58
Yin XY et al. Cancer, 2009
RFA 109 [3-7] 3.9 92.6 22 29.4
N Size
[range] mean (cm)
Complete radiological response
(%)
Local recurrence
(%)
Incomplete local tumor
control (%)
Livraghi T et al. Radiology, 2000
RFA 114 [3-9,5] 5.4 47.6 5.5 58
Yin XY et al. Cancer, 2009
RFA 109 [3-7] 3.9 92.6 22 29.4
Veltri A et al. Eur Radiol, 2006
TACE +
RFA 46 [3-8]
4.8 66.7 10 43.3
Lencioni R et al. J Hepatol, 2008
RFA +
DC beads 20 [3.3-7]
5 60 10 50
Et si on ajoutait la CEL …
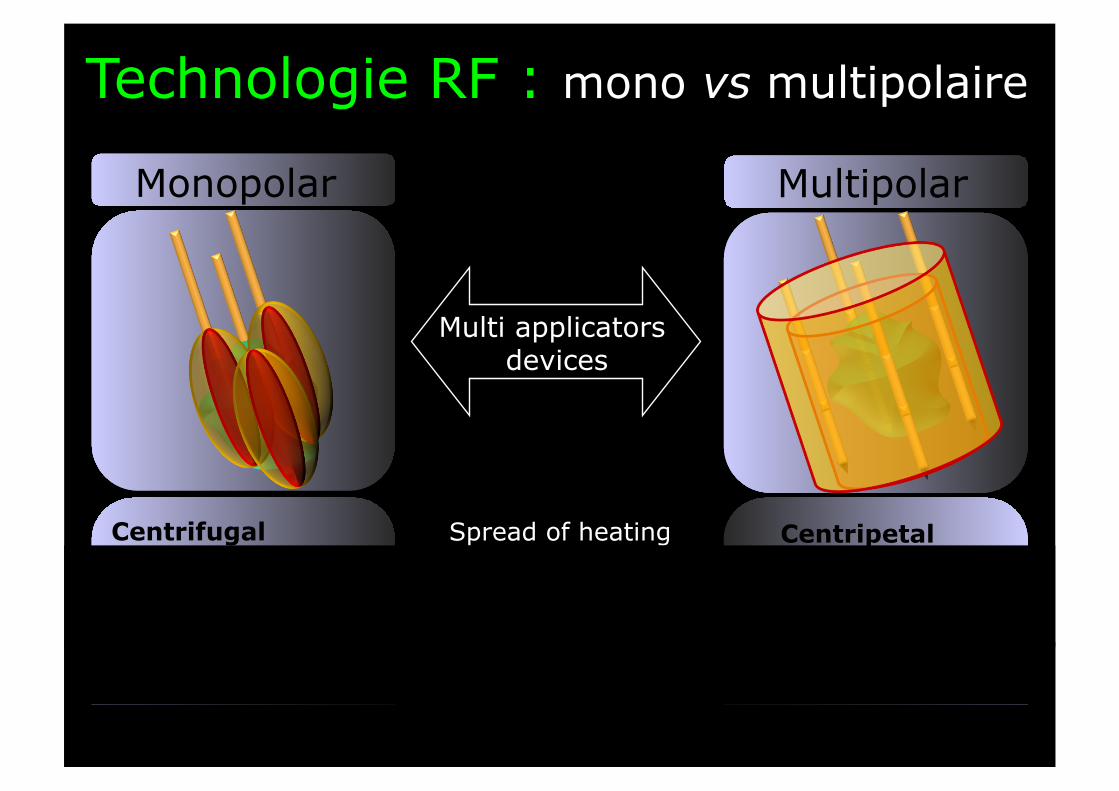
Monopolar Multipolar
Resort to overlapping ablations Limited Mandatory
Ablation margins Quite predicable Poorly predicable
Ablation volume Summation of all inter applicators ablation areas
Summation of all surrounding applicator ablation areas
Spread of heating Centripetal Centrifugal
Multi applicators devices
Technologie RF : mono vs multipolaire
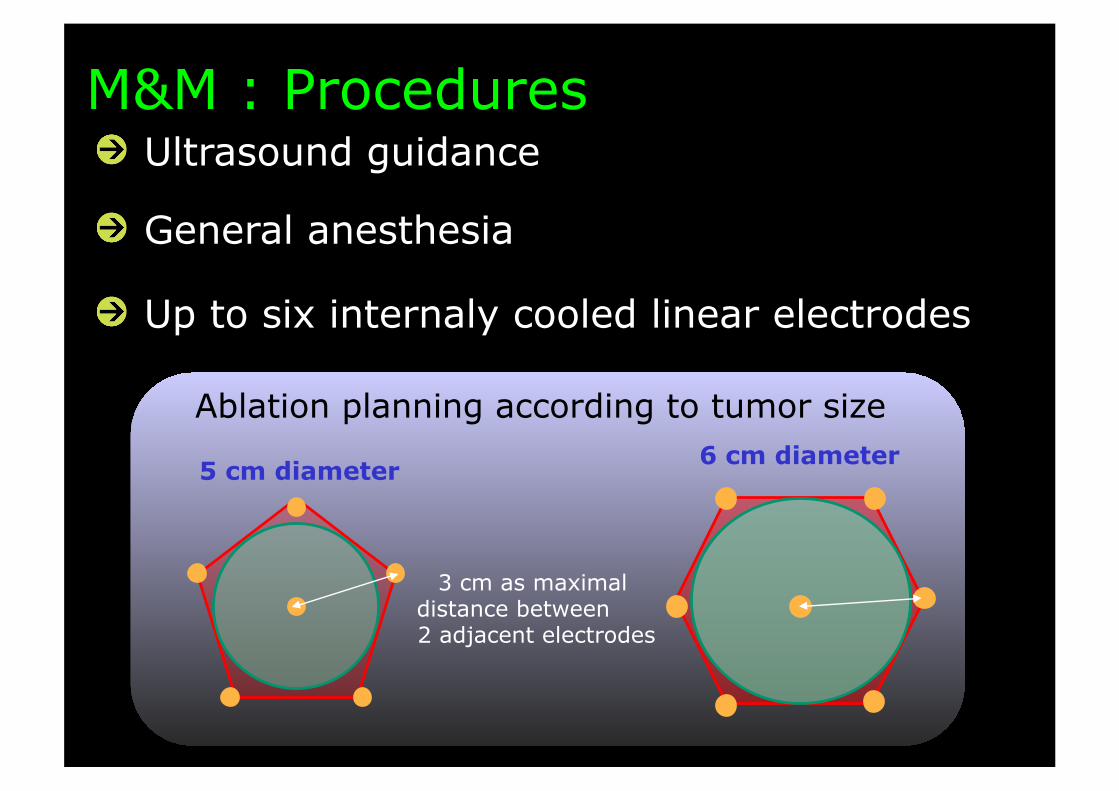
Ablation planning according to tumor size
" Ultrasound guidance
" General anesthesia
" Up to six internaly cooled linear electrodes
3 cm as maximal distance between 2 adjacent electrodes
5 cm diameter 6 cm diameter
M&M : Procedures
" 87% de réponse complète (47/54)
" 6/7 des échecs étaient des formes infiltrantes
Résultats: Réponse précoce
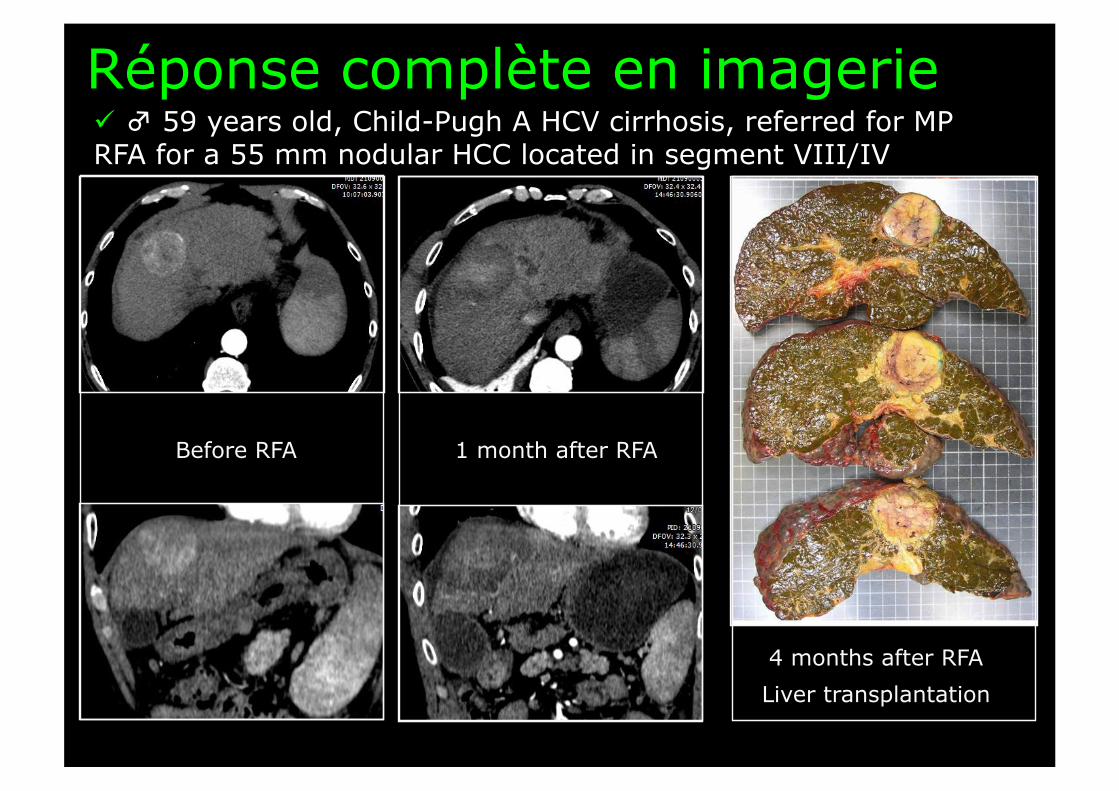
Réponse complète en imagerie
Before RFA 1 month after RFA
4 months after RFA
Liver transplantation
♂ 59 years old, Child-Pugh A HCV cirrhosis, referred for MP RFA for a 55 mm nodular HCC located in segment VIII/IV
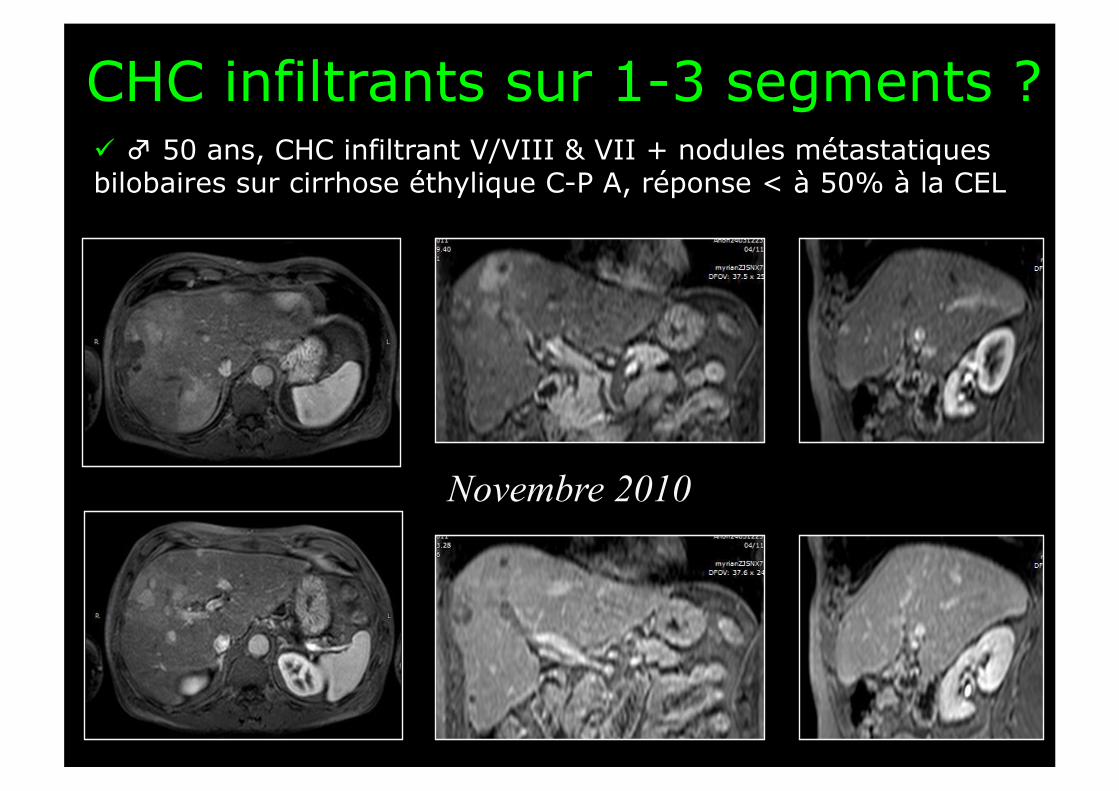
CHC infiltrants sur 1-3 segments ? ♂ 50 ans, CHC infiltrant V/VIII & VII + nodules métastatiques bilobaires sur cirrhose éthylique C-P A, réponse < à 50% à la CEL
Novembre 2010
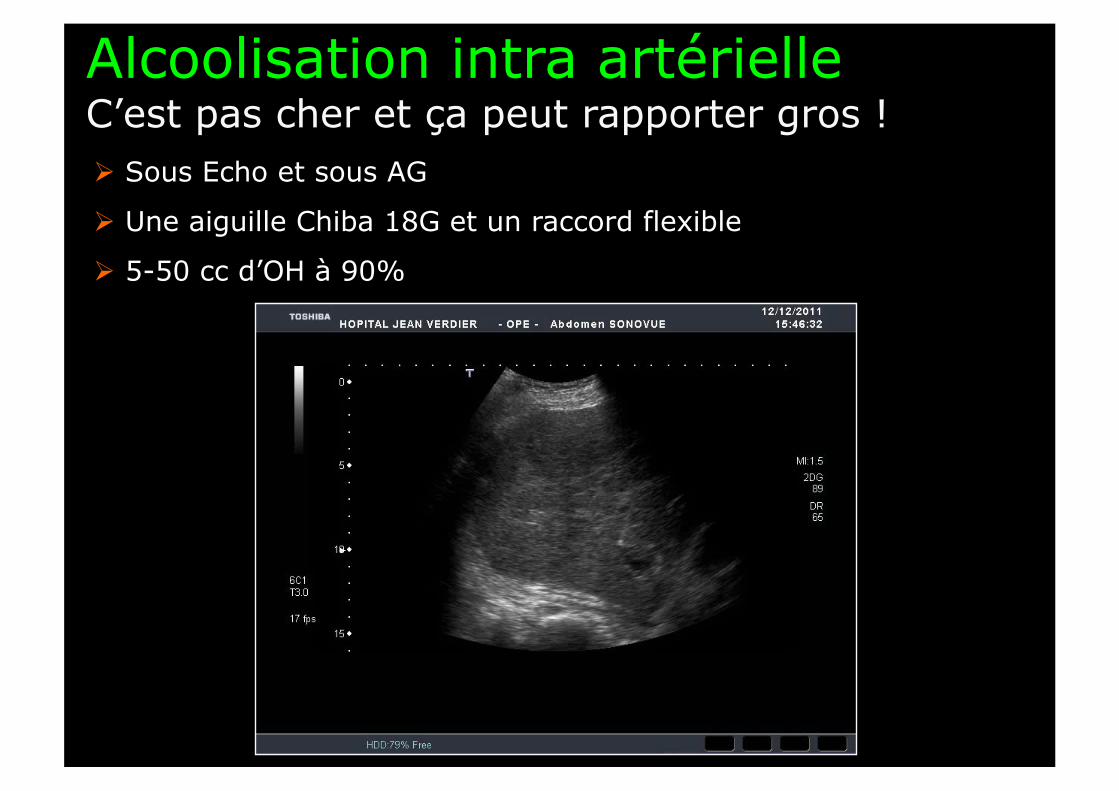
Alcoolisation intra artérielle C’est pas cher et ça peut rapporter gros ! Sous Echo et sous AG
Une aiguille Chiba 18G et un raccord flexible
5-50 cc d’OH à 90%
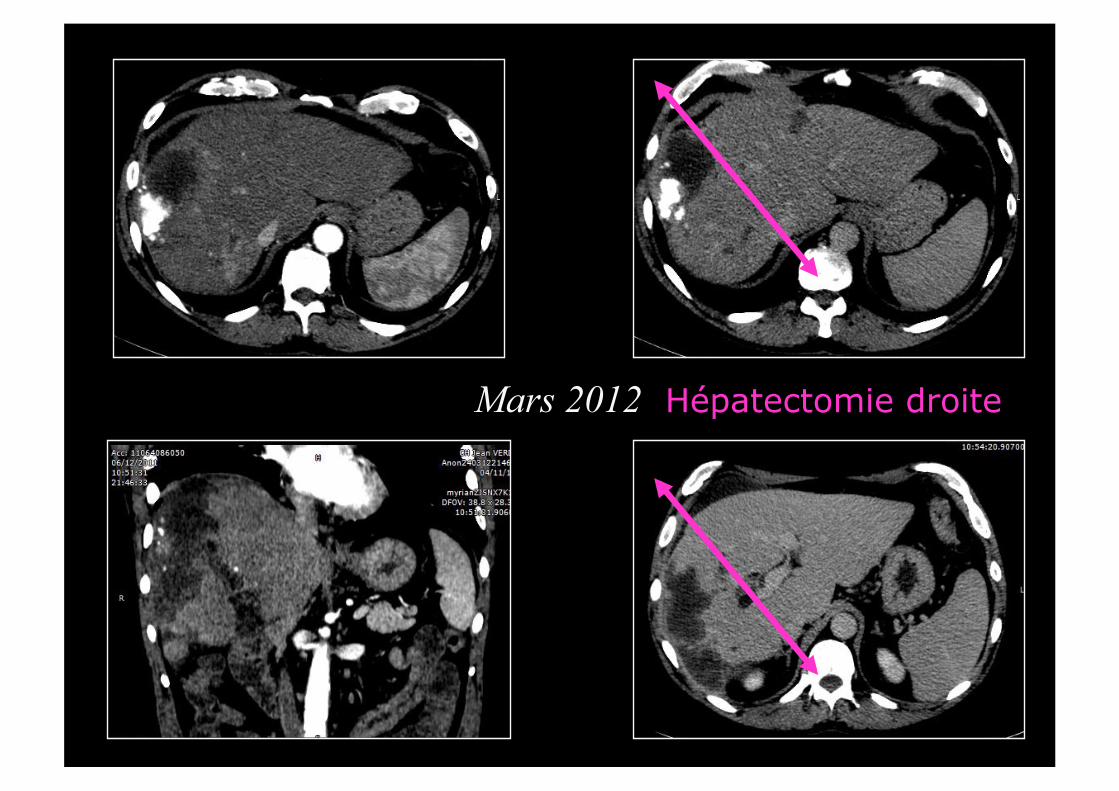
Mars 2012 Hépatectomie droite

Radiofréquence multipolare A tenter si AIA impossible ou en échec ♂ 83 ans, présentant une quadruple récidive de CHC dont une volumineuse lésion infiltrante du III 5 ans après une RFA initiale pour CHC bifocal (rupture de surveillance, cirrhose OH C-P B6)
Aout 2011
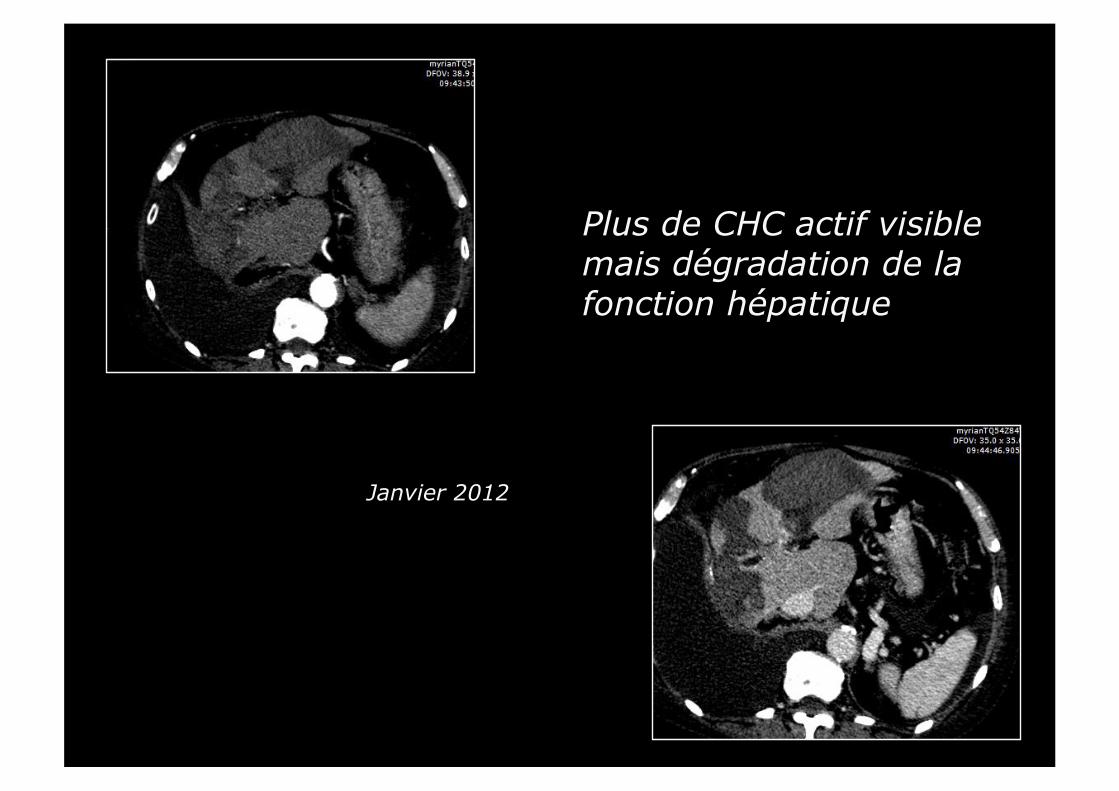
Janvier 2012
Plus de CHC actif visible mais dégradation de la fonction hépatique
Méthode 1
Technique ancienne = Technique obsolète ?
Spectre des indications en intention « curative »
Méthode 2 Méthode 3
Pas de méthode omnipotente ⇒ Pas de substitution ad integratum
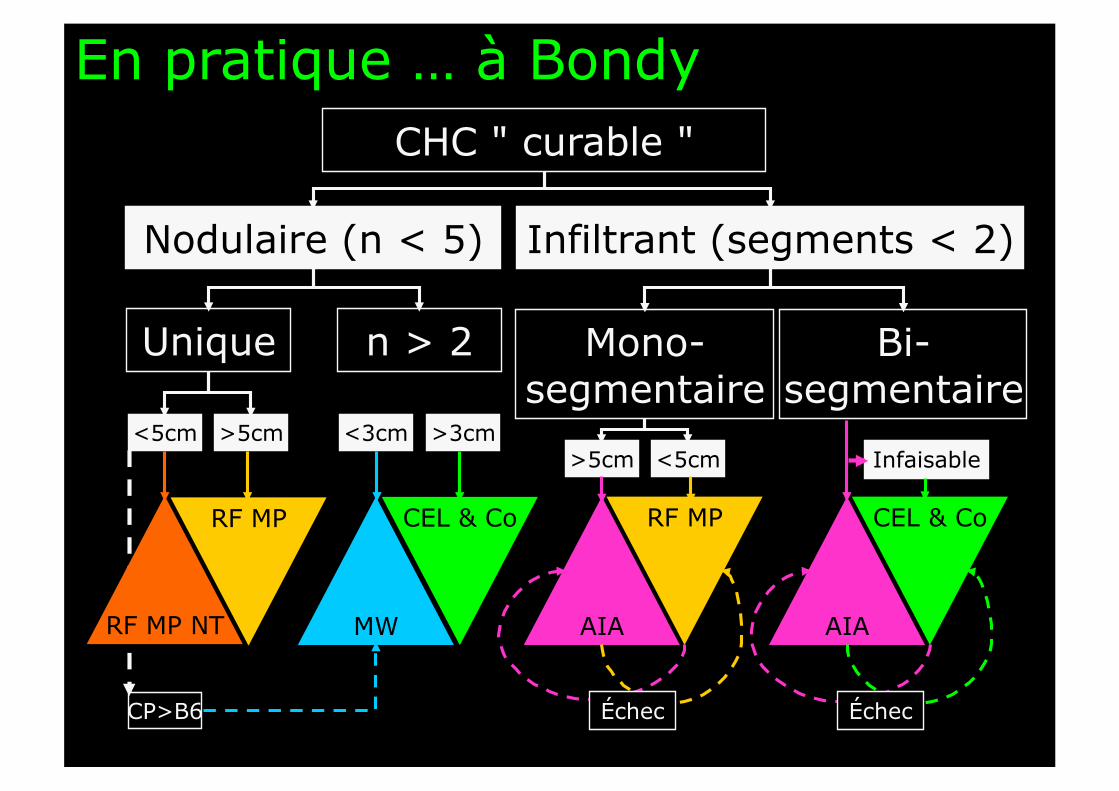
Mono-segmentaire
En pratique … à Bondy CHC " curable "
<5cm
RF MP NT
Infiltrant (segments < 2) Nodulaire (n < 5)
Unique n > 2
>5cm
MW
RF MP
CP>B6
Bi-segmentaire
AIA
RF MP
<3cm >3cm
CEL & Co
AIA
CEL & Co
>5cm <5cm Infaisable
Échec Échec