A Novel Hyaluronate-Atelocollagen / b-TCP-Hydroxyapatite … · 2017-01-30 · dissolved in 1N HCl...
1
A Novel Hyaluronate-Atelocollagen/-TCP-Hydroxyapatite Biphasic Scaffold for the Repair of Osteochondral Defect 1 Lee, T H; 1 An, J H; 1 Oh, J S; 2 Kim, H-J; 2 Park, I K; 2 Choi, B S; + 1 Im, G-I + 1 Dongguk University International Hospital, 2 BIOPOL Co. Ltd. Head of R&D Center Senior author [email protected] INTRODUCTION The authors devised a novel biphasic scaffold which combined hyaluronic acid and atelocollagen for the chondral phase, and hydroxyapatite and -TCP for osseous phase. The purpose of this paper was to introduce the fabrication and physicochemical characteristics of this novel hybrid scaffold, and assess the in-vivo and in-vitro results of this scaffold for osteochondral repair. METHODS 1) Fabrication of hyaluronate/atelocollagen scaffold (chondral phase): Hyaluronates in dried powder form and bovine atelocollagen dried powder form was used for fabrication of scaffold. Ethylene glycol diglycidyl ether was used as the cross-linking agent. Atelocollagen was dissolved in 1N HCl to 0.5% (w/v), then hyaluronate powder was added to 1.5% (w/v) to the solution. The mixture was then vigorously stirred using mechanical stirrer. EGDGE was added to above mixture, poured into a mold (diameter 6mm, height 2mm), reacted for 30 minutes at 30 oC , then freeze-dried for 24 hours at -40 oC . 2) Fabrication of HA/-TCP scaffold (osseous phase): Urethane foaming method was used to fabricate porous ceramic scaffold. Hydroxyapatite and tricalcium phosphate were mixed in the proportion of 6 to 4 (w/w). 3) Fabrication of biphasic scaffold:Fabricated osseous phase was prewetted with hyaluronate /atelocollagen solution. Freeze-dried hyaluronate /atelocollagen scaffold was placed over the HA/-TCP scaffold, then freeze-dried again at -40 o C. The fabricated hybrid scaffold was washed with ultrapure water several times, freeze-dried for 24 hours, and sterilized by gamma radiation. 4) In-vitro and in-vivo chondrogenesis: Chondrocytes were isolated 28 rabbits, cultured, suspended in DMEM/F-12 solution at a concentration of 1 x 10 6 cell/50μl and injected using 1cc syringe inside the chondral phase of biphasic scaffold. Cells were allowed to adhere to the scaffold for 2h at 37 and cultured in chondrogenic medium containing 10 ng/ml of TGF-1 for 2weeks. We made a large osteochondral defect (diameter 6mm, depth 5 mm) on the patellar groove of the right distal femur using OATS trephine (Fig.1B). The defects were managed in one of the following methods: the defects were filled with cell-biphasic scaffold composite (Group I, Fig.1C); only biphasic scaffold was implanted (Group II, Fig.1D): the removed osteochondral fragments were placed back to the defect (Group III, positive control, Fig.1E): the defects were left empty (Group IV, negative control, Fig.1F). Seven rabbits were allocated to each group. RESULTS 1) Scaffold characterization: SEM findings demonstrated that chondral phase had loose, well-interconnected honeycomb-like structure with large pore (diameter 100-150μm), the mean porosity being 93±1.4% (Fig. 2A). Osseous phase also showed well-interconnected porous structures. The diameter was 500-650 μm and the mean porosity was 74±2.2% (Fig. 2B). Biphasic scaffold showed that chondral phase interdigitated into osseous phase (Fig.2C). The compressive strength of biphasic scaffold was 3.2±0.18 MPa. Three dimensional microtomography also showed fine porous structure of osseous phase (Fig.2D). Fig.1 Experimental designs and surgical procedures Fig.2 Scaffold characterization 2)In-vitro chondrogenesis: After 2 weeks of in-vitro culture, chondral phase of chondrocytes/biphasic scaffold became firmer, suggesting production of extracellular matrix (Fig.3A,B) From HE and Safranin-O staining, chondrocytes evenly infiltrated inside the chondral phase, and produced extracelluar matrix. They were located in the center of chondral phase as well as in the periphery (Fig.3 C, D). Their close association with chondral phase was also demonstrated in SEM findings (Fig.3E). Fig.3 In-vitro chondrogenesis model 3) In-vivo chondrogenesis: Gross grading score was highest in group III followed by Group I, Group II and lastly Group IV (negative control). Depression of defect was greatest in Group IV while osteochondral autograft in Group III had least depression, sitting proud of adjacent cartilage in two rabbits. There were three rabbit, two in Group I and one in Group II, which were complete denuded of chondral phase, and osseous phase exposed. The junction to adjacent native cartilage was distinct in rabbits of all groups (Fig. 4). ICRS Visual Histological Score was highest in Group III, followed by Group I, II. Group I and Group II had almost equal scores (Fig.5). Fig.4 Gross & histological finding of osteochondral defects after 3 months Fig.5 ICRS macroscore (A), Visual Histological Score (B) DISCUSSION In conclusion, results obtained using a rabbit osteochondral defect model suggests that biphasic osteochondral composite using chondral phase consisting of hyaluronate and atelocollagen and osseous phase comprising HA and TCP hold promise for the repair of osteochondral defect although denudation of chondral phase is a potential caveat that should be addressed. ACKNOWLEDGEMENT This work was supported by a grant from Ministry of Commerce, Industry and Energy(00013064) Poster No. 1284 • 55th Annual Meeting of the Orthopaedic Research Society
Transcript of A Novel Hyaluronate-Atelocollagen / b-TCP-Hydroxyapatite … · 2017-01-30 · dissolved in 1N HCl...

A Novel Hyaluronate-Atelocollagen/β-TCP-Hydroxyapatite Biphasic Scaffold for the Repair of Osteochondral Defect1Lee, T H; 1An, J H; 1Oh, J S; 2Kim, H-J; 2Park, I K; 2Choi, B S; +1Im, G-I
+1Dongguk University International Hospital, 2BIOPOL Co. Ltd. Head of R&D CenterSenior author [email protected]
INTRODUCTIONThe authors devised a novel biphasic scaffold which combined
hyaluronic acid and atelocollagen for the chondral phase, and hydroxyapatite and β-TCP for osseous phase. The purpose of this paper was to introduce the fabrication and physicochemical characteristics of this novel hybrid scaffold, and assess the in-vivo and in-vitro results of this scaffold for osteochondral repair.
METHODS1) Fabrication of hyaluronate/atelocollagen scaffold (chondral phase):
Hyaluronates in dried powder form and bovine atelocollagen dried powder form was used for fabrication of scaffold. Ethylene glycol diglycidyl ether was used as the cross-linking agent. Atelocollagen was dissolved in 1N HCl to 0.5% (w/v), then hyaluronate powder was added to 1.5% (w/v) to the solution. The mixture was then vigorously stirred using mechanical stirrer. EGDGE was added to above mixture, poured into a mold (diameter 6mm, height 2mm), reacted for 30 minutes at 30oC, then freeze-dried for 24 hours at -40oC. 2) Fabrication of HA/β-TCP scaffold (osseous phase): Urethane
foaming method was used to fabricate porous ceramic scaffold. Hydroxyapatite and β−tricalcium phosphate were mixed in the proportion of 6 to 4 (w/w). 3) Fabrication of biphasic scaffold:Fabricated osseous phase was
prewetted with hyaluronate /atelocollagen solution. Freeze-dried hyaluronate /atelocollagen scaffold was placed over the HA/β-TCP scaffold, then freeze-dried again at -40oC. The fabricated hybrid scaffold was washed with ultrapure water several times, freeze-dried for 24 hours, and sterilized by gamma radiation.4) In-vitro and in-vivo chondrogenesis: Chondrocytes were isolated 28
rabbits, cultured, suspended in DMEM/F-12 solution at a concentration of 1 x 106 cell/50µl and injected using 1cc syringe inside the chondral phase of biphasic scaffold. Cells were allowed to adhere to the scaffoldfor 2h at 37� and cultured in chondrogenic medium containing 10 ng/ml of TGF-β1 for 2weeks. We made a large osteochondral defect (diameter 6mm, depth 5 mm) on the patellar groove of the right distal femur using OATS trephine (Fig.1B). The defects were managed in one of the following methods: the defects were filled with cell-biphasic scaffold composite (Group I, Fig.1C); only biphasic scaffold was implanted (Group II, Fig.1D): the removed osteochondral fragments were placed back to the defect (Group III, positive control, Fig.1E): the defects were left empty (Group IV, negative control, Fig.1F). Seven rabbits were allocated to each group.
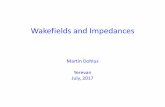
RESULTS1) Scaffold characterization: SEM findings demonstrated that chondral
phase had loose, well-interconnected honeycomb-like structure with large pore (diameter 100-150µm), the mean porosity being 93±1.4% (Fig. 2A). Osseous phase also showed well-interconnected porous structures. The diameter was 500-650 µm and the mean porosity was 74±2.2% (Fig. 2B). Biphasic scaffold showed that chondral phase interdigitated into osseous phase (Fig.2C). The compressive strength of biphasic scaffold was 3.2±0.18 MPa. Three dimensional microtomography also showed fine porous structure of osseous phase (Fig.2D).
Fig.1 Experimental designs and surgical procedures
Fig.2 Scaffold characterization
2)In-vitro chondrogenesis: After 2 weeks of in-vitro culture, chondral phase of chondrocytes/biphasic scaffold became firmer, suggesting production of extracellular matrix (Fig.3A,B) From HE and Safranin-O staining, chondrocytes evenly infiltrated inside the chondral phase, and produced extracelluar matrix. They were located in the center of chondral phase as well as in the periphery (Fig.3 C, D). Their close association with chondral phase was also demonstrated in SEM findings (Fig.3E).
Fig.3 In-vitro chondrogenesis model
3) In-vivo chondrogenesis: Gross grading score was highest in group III followed by Group I, Group II and lastly Group IV (negative control). Depression of defect was greatest in Group IV while osteochondral autograft in Group III had least depression, sitting proud of adjacent cartilage in two rabbits. There were three rabbit, two in Group I and one in Group II, which were complete denuded of chondral phase, and osseous phase exposed. The junction to adjacent native cartilage was distinct in rabbits of all groups (Fig. 4). ICRS Visual Histological Score was highest in Group III, followed by Group I, II. Group I and Group II had almost equal scores (Fig.5).
Fig.4 Gross & histological finding of osteochondral defects after 3 months
Fig.5 ICRS macroscore (A), Visual Histological Score (B)
DISCUSSIONIn conclusion, results obtained using a rabbit osteochondral defect
model suggests that biphasic osteochondral composite using chondral phase consisting of hyaluronate and atelocollagen and osseous phase comprising HA and TCP hold promise for the repair of osteochondral defect although denudation of chondral phase is a potential caveat that should be addressed.
ACKNOWLEDGEMENTThis work was supported by a grant from Ministry of Commerce,
Industry and Energy(00013064)
Poster No. 1284 • 55th Annual Meeting of the Orthopaedic Research Society