
Negative impact of 5-alpha-reductase inhibitors on male fertility
Upload
hamzahazaliCategory
view
61download
0description
ACE INHIBITORS Drugs : captopril, enalapril Mainly used in CHF and hypertension Basis of use;
Angiotensinogen(α2 globulin) ↓Renin from JG cells of kidney Angiotensin I ACE inhibitor - ↓ACE Decreased Angiotensin II
↓ ↓
Decreased preload and afterload Decreased blood pressure i.e
↓ relieves HTN
Increasd cardiac output
↓
Relieves CHF
Indications HTN CHF MI Angina pectoris Left ventricular hypertrophy
decreased angiotensin II
increased vasodilatation of vascular smooth muscle
decreased Na+ and water retention
Decreased output of sympathetic nervous system
increased bradykinin level
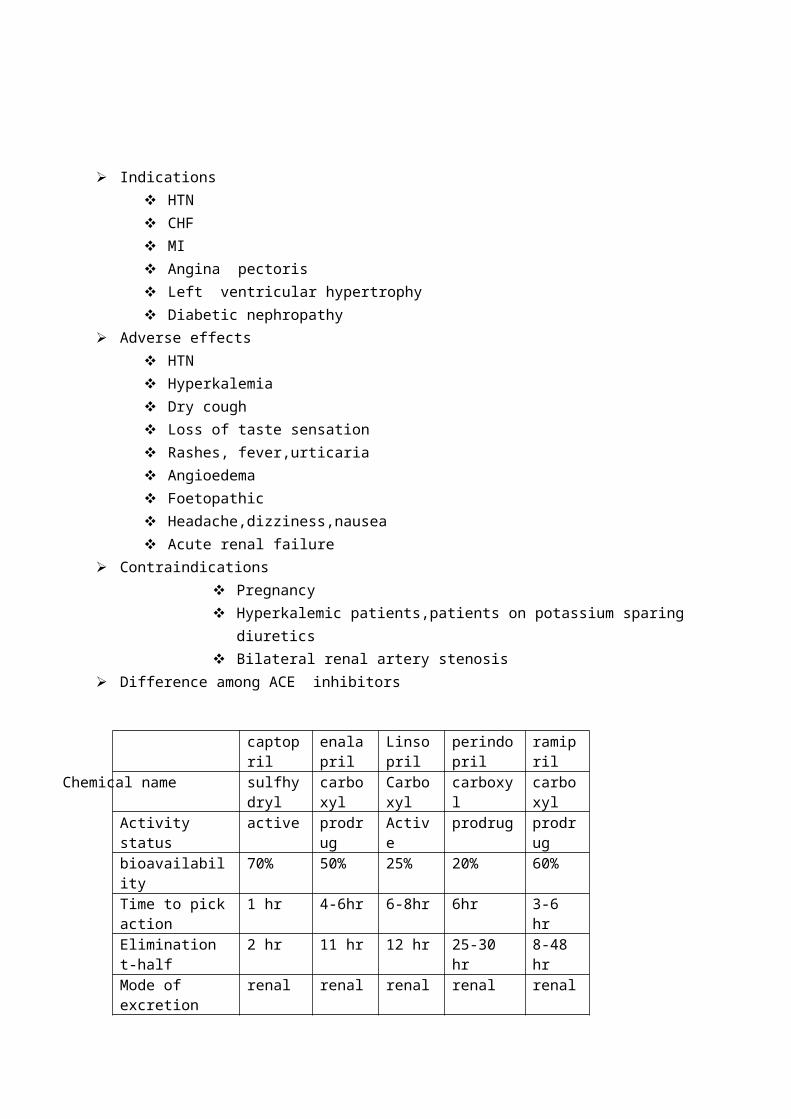
Diabetic nephropathy Adverse effects
HTN Hyperkalemia Dry cough Loss of taste sensation Rashes, fever,urticaria Angioedema Foetopathic Headache,dizziness,nausea Acute renal failure
Contraindications Pregnancy Hyperkalemic patients,patients on potassium sparing diuretics Bilateral renal artery stenosis
Difference among ACE inhibitors
captopril enalapril Linsopril perindopril ramiprilChemical name sulfhydryl carboxyl Carboxy
lcarboxyl carboxyl
Activity status active prodrug Active prodrug prodrugbioavailability 70% 50% 25% 20% 60%Time to pick action 1 hr 4-6hr 6-8hr 6hr 3-6 hrElimination t-half 2 hr 11 hr 12 hr 25-30 hr 8-48 hrMode of excretion renal renal renal renal renalDuration of action 6-12 hr 24 hr ≥24 hr ≥24 hr ≥24 hrDaily dose (mg) 25-150 2.5-40 5-40 2-8 1.25-10
ANGIOTENSIN ANTAGONISTS
Drugs: losartan Uses: HTN and CHF Basis of use:
Acts as competitive antagonists of angiotensin II ↓ Blocks all actions of angiotensin II
1. ↓decreased outflow from sympathetic nervous system2. Increased vasodilatation of vascular smooth muscle3. Decreased sodium and water retention4. Decreasd ADH release and promotion of growth of blood vessels and heart
↓ ↓
Decreases B.P. that lasts
Decreased preload and afterload for 24 hrs ,relieves HTN.

↓Increased cardiac output
Differences between ACE inhibitors and angiotensin II antagonists.
ACE Inhibitors Angiotensin II antagonists1.interfere with degradation of bradykinin→increases bradykinin level
1.no such interference
2.alternative pathway of A-II production and AT-I receptor activation remain intact with them
2.causes complete inhibition of AT-I receptor
3.causes inactivation of AT-1 and AT-2 receptor 3.causes indirect AT-2 receptor activation
4.has more potential to cause cough and dysguesia 4.has very less potential to cause
“ β BLOCKER”
CLASSIFICATION1)non selective (β1 and β2) a)without intrinsic sympathomimetic action: propranolol , timolol b)with intrinsic sympathomimetic activity: pindolol c)with additional α blocking property:labetalol2)cardioselective (β1) Metoprolol, atenolol3)selective β2 Butonamide
Basis of use of β blocker in1)HTN
long time use of β blocker
decreased activation of β1 receptor on heart
decreased renin release from JG cell of kidney
decreased noradrenalin release and decreased
sympathetic tone
2)Arrythmia Β blockers causes diminision of phase 4 depolarisation
↓
1)Decreased automatic firing of SA node
2)prolongation of AV conduction
3) decreased heart rate and contractility
↓
Helps in the treatment of :
a)tachyarrythmia due to sympathetic overactivity
b)atrial flutter
c)digoxin induced dysrhythmia
d)WPW syndrome
3)Angina pectoris
Bloackade of β1 receptor on heart
↓
Decreased heart rate, force of contraction and cardiac output
↓
Decreased cardiac work and oxygen demand
↓
Relieves stable angina by reducing its frequency and severity
NOTE: Propranolol is used in the chronic management of stable angina and not in an acute attackQ)Why β blockers are contraindicated in variant angina ?Ans) Variant angina is due to spasm of coronary artery. Use of β blockers leads to unopposed α receptor mediated constriction of coronary artery.This leads to the aggravation of variant angina.
Indications of β blocker: Angina pectoris Hypertension Cardiac arrhythmias Acute MI Migraine prophylaxis Anxiety neurosis
Chronic open angle glaucoma
Chronic open angle glaucoma Pheochromocytoma Thyrotoxicosis Tetralogy of fallot Essential tremor
Adverse effects of β blockers: CCF Bradycardia Aggravates AV conduction defects Bronchoconstriction Hypoglycaemia Nausea vomiting and constipation Uterine hypomotility and prolonged labour Fatigue depression and hallucination Cold extremities Nightmares Impotency
Contraindications of β blockers Bronchial asthma CCF Heart block Cardiogenic shock Bradycardia Patients on oral hypoglycaemic agents
NITRATES
Classification:
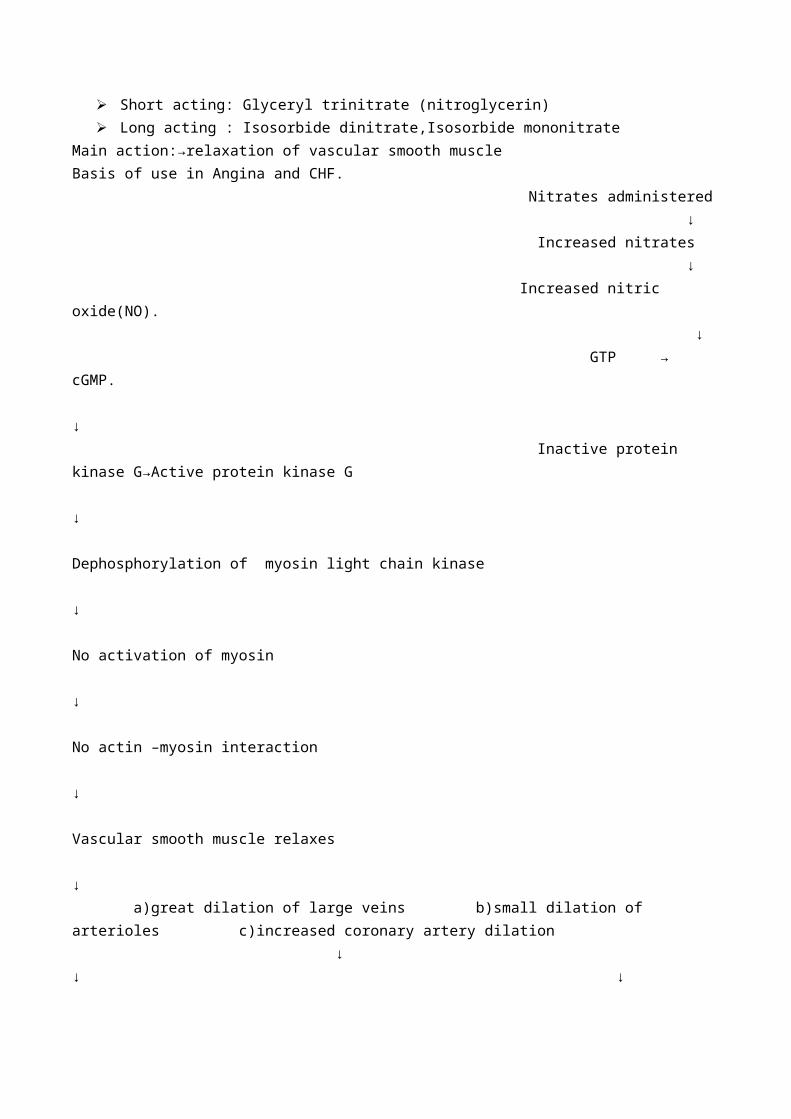
Short acting: Glyceryl trinitrate (nitroglycerin) Long acting : Isosorbide dinitrate,Isosorbide mononitrate
Main action:→relaxation of vascular smooth muscleBasis of use in Angina and CHF. Nitrates administered ↓ Increased nitrates ↓ Increased nitric oxide(NO). ↓ GTP → cGMP. ↓

Inactive protein kinase G→Active protein kinase G ↓ Dephosphorylation of myosin light chain kinase ↓ No activation of myosin ↓ No actin –myosin interaction ↓ Vascular smooth muscle relaxes ↓ a)great dilation of large veins b)small dilation of arterioles c)increased coronary artery dilation ↓ ↓ ↓ Peripheral pooling of blood decreased T.P.R Increased blood and Oxygen supply
↓ ↓ To heart
Decreased venous return decreased afterload
↓
Decreased preload
Indications:
Angina pectoris CHF and acute LVF MI Pulmonary HTN Biliary colic Esophageal spasm Cyanide poisoning
Adverse effects: Fullness of head, throbbing headache Flushing Weakness Sweating Palpitation Dizziness Fainting Methenoglobenemia Rashes
Contraindication: Glaucoma Hypertrophic cardiomyopathyss Hypotension
CALCIUM CHANNEL BLOCKERSDrugs:
Phenylalkylamine: Verapamil Benzothiazepine:Diltiazem Dihydropyridine: Nifedipine, Amlodipine
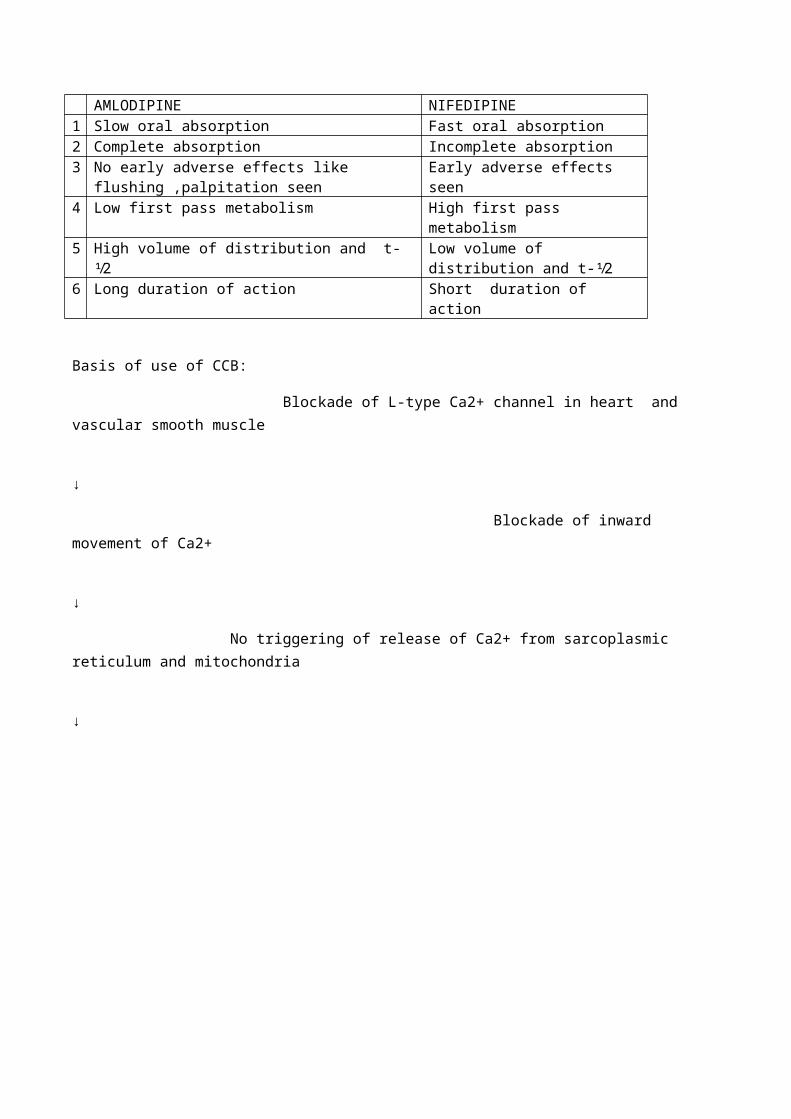
Differences between nifedipine and amlodipine:
AMLODIPINE NIFEDIPINE1 Slow oral absorption Fast oral absorption2 Complete absorption Incomplete absorption3 No early adverse effects like flushing ,palpitation seen Early adverse effects seen4 Low first pass metabolism High first pass metabolism5 High volume of distribution and t-⅟2 Low volume of distribution and t-⅟26 Long duration of action Short duration of action
Basis of use of CCB:
Blockade of L-type Ca2+ channel in heart and vascular smooth muscle
↓
Blockade of inward movement of Ca2+
↓
No triggering of release of Ca2+ from sarcoplasmic reticulum and mitochondria
↓
No/low availability of Ca2+ in cytosol
no/low availability of calcium in the cytosol
VERAPAMIL,DILTIAZEM(acts on heart↓
no seperation of troponin-tropomyosin complex↓
no actin myosin interaction↓
decreased HR ,force of contraction,and conduction velocity
decreased cardiac work and oxygen
requirements↓
releives angina
decreases total peripheral resistance
↓releives HTN
DHPS acts mainly on vascular smooth muscle↓
no phosphorylation of MLCK↓
NO EXITATION-CONTRACTION COUPLING↓
vascular smooth muscle relaxation, mainly a
decreased total peripheral resistance↓
releives HTN

Indications
Angina pectoris HTN Hypertrophic cardiomyopathy Arrhythmias Others: premature labour
Adverse effects: Tachycardia Ankle edema Flushing Hyperplasia of gums Hyperkalemia Headache Constipation Lethargy Bradycardia
Contraindications: Hypotension Cardiogenic shock Acute MI 2nd and 3rd degree heart block
Differences among CCBs
Properties Diltiazem Verapamil Nifedipine1 Channel blocking power + ++ +++2 Frequency dependence of
channel blockade+ ++ _
3 Channel recovery rate delayed Much delayed _4 Cardiac effects
Heart rate ↓,_ ↓ ↑AV conduction velocity ↓ ↓↓ _Contractility ↓,↑ _,↓ ↑Output _,↑ _,↓ ↑
5 Vascular smooth muscle relaxation
+ ++ +++
6 Uses Angina,HTN,(Arrythmia) Angina,arrhythmias,(HTN) Angina,HTN
CARDIAC GLYCOSIDES(DIGOXIN)Drugs: Digoxin, DigitoxinUse: Mainly used in CHFBasis of use in CHF: Binds reversibly with Na+K+ATPase enzyme of cardiac cell membrane ↓ Inhibition of Na+K+ATPase pump ↓
Increased intracellular concentration of Na+ ↓ Increased intracellular Na+ leads to increased Ca++ influx via Na+Ca++ exchange pump ↓ Increased contraction of heart ↓ Increased cardiac output of filling pressure that doesnot produce congestive symptoms ↓ Improved circulation decreases sympathetic tone and hence total peripheral resistance ↓ Decreased heart rate and oxygen demand ↓ Provides relief in CHF
Indications:
Congestive cardiac failure Left ventricular failure Atrial fibrillation &flutter Premature beat Supraventricular tachycardia
Contraindication: Hypokalemia Renal&hepatic disease M.I Thyrotoxicosis Myxoedema Ventricular tachycardia Partial A-Vblock Acute myocarditis Wolf-parkinsons white syndrome
Adverse effects:I)Cardiac effects
Premature beats Atrial and ventricular tachycardia Heart block Sinus bradycardia
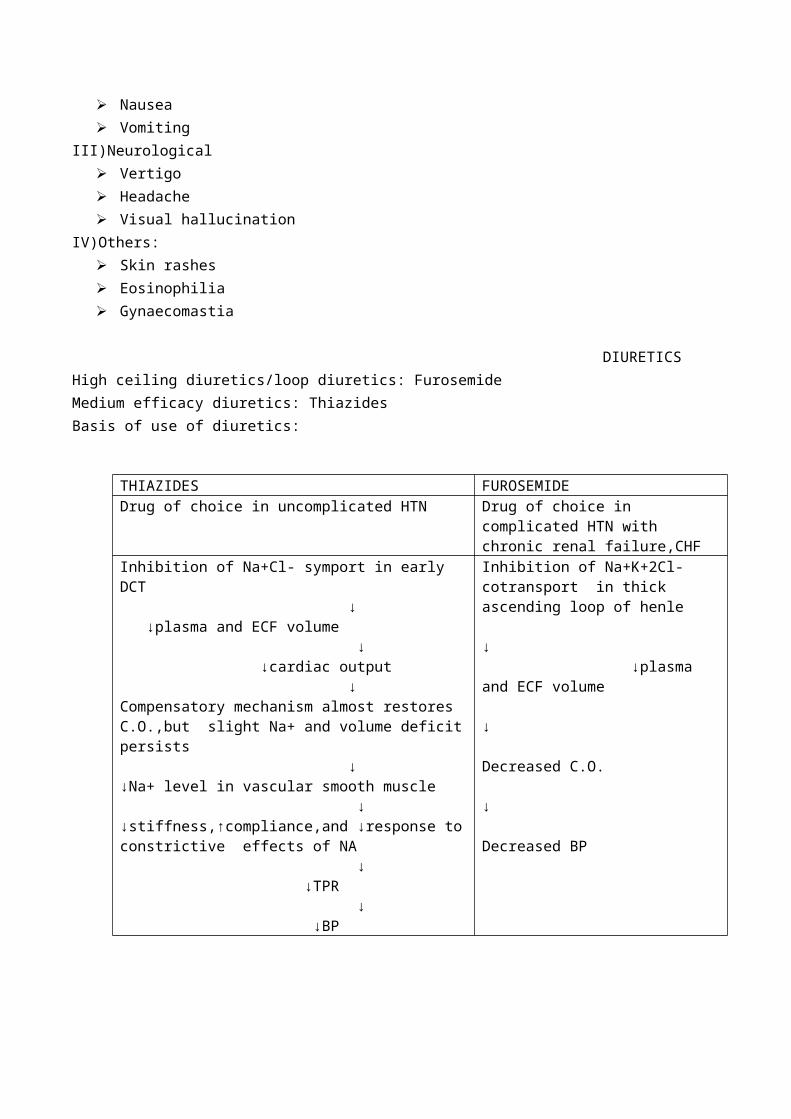
II)GI effects Anorexia Nausea Vomiting
III)Neurological Vertigo Headache Visual hallucination

IV)Others: Skin rashes Eosinophilia Gynaecomastia
DIURETICSHigh ceiling diuretics/loop diuretics: FurosemideMedium efficacy diuretics: ThiazidesBasis of use of diuretics:
THIAZIDES FUROSEMIDEDrug of choice in uncomplicated HTN Drug of choice in complicated HTN with
chronic renal failure,CHFInhibition of Na+Cl- symport in early DCT ↓ ↓plasma and ECF volume ↓ ↓cardiac output ↓Compensatory mechanism almost restores C.O.,but slight Na+ and volume deficit persists ↓↓Na+ level in vascular smooth muscle ↓↓stiffness,↑compliance,and ↓response to constrictive effects of NA ↓ ↓TPR ↓ ↓BP
Inhibition of Na+K+2Cl- cotransport in thick ascending loop of henle ↓ ↓plasma and ECF volume ↓ Decreased C.O. ↓ Decreased BP
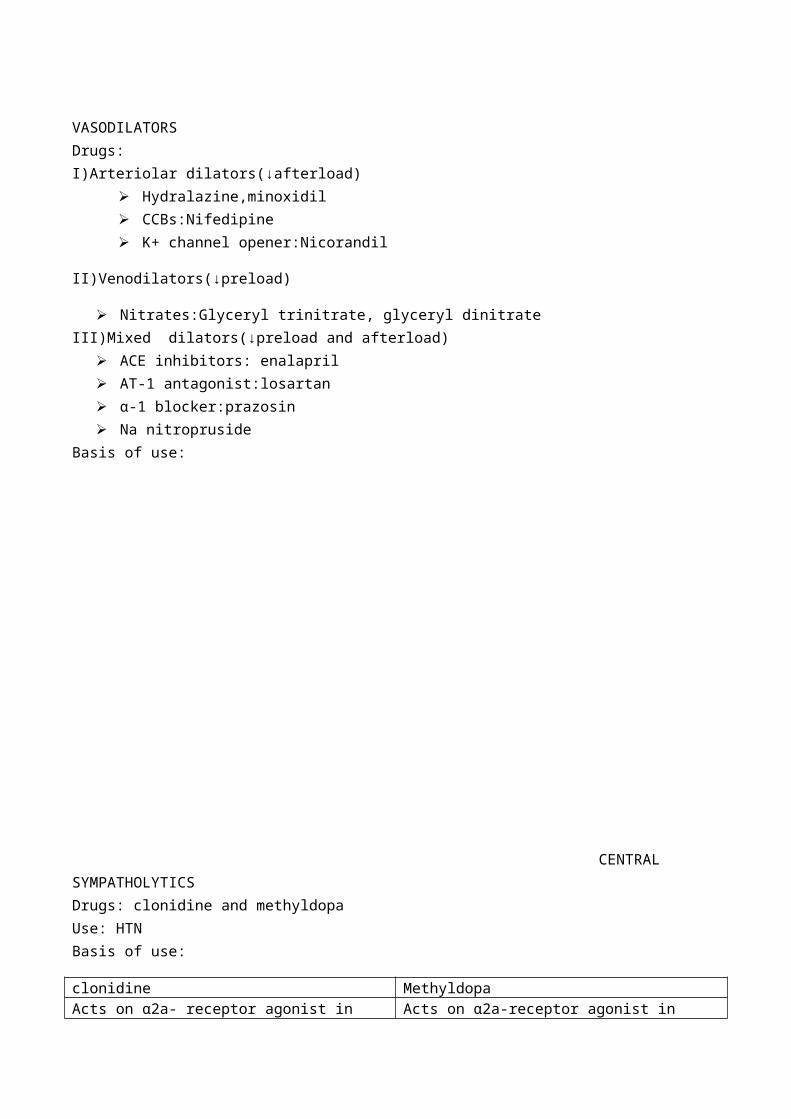
VASODILATORSDrugs:I)Arteriolar dilators(↓afterload)
Hydralazine,minoxidil CCBs:Nifedipine K+ channel opener:Nicorandil
II)Venodilators(↓preload)
Nitrates:Glyceryl trinitrate, glyceryl dinitrateIII)Mixed dilators(↓preload and afterload)
ACE inhibitors: enalapril AT-1 antagonist:losartan α-1 blocker:prazosin

Na nitroprusideBasis of use:
CENTRAL SYMPATHOLYTICS Drugs: clonidine and methyldopaUse: HTNBasis of use:
clonidine MethyldopaActs on α2a- receptor agonist in vasomotor centre in medulla ↓ ↓sympathetic activity ↓ Decrease BP
Acts on α2a-receptor agonist in vasomotor centre in medulla ↓ ↓sympathetic outflow ↓ Decreased TPR ↓ Decreased BP
Dopamine in therapy: cardiogenic shock
vasodilators
dilatation of venous blood vessels↓
↑peripheral pooling of blood↓
↓in preload
provide releif in CHF
decreased TPR and CO↓
Decreased BP
Dilation of arteriolar blood vessels↓
↓ed arteriolar resistance↓
↓in afterload

RESPIRATORY SYSTEMDRUGS FOR COUGHClassification:
Pharyngeal demulcents:logenges, cough drops Expectorants(mucokinetics)
a)Directly acting:citrate of Na+/K+,KIb)Reflexly acting:ammonium chloride/carbonate,KIc)Mucolytics:bromhexine
Antitussives (cough suppressants)a)opiods:codeine,morphineb)non opiods:Noscapine,dextromethorphanc)antihistaminics:promethzine,chlorpheniramine
Basis of use of mucolytics in therapy: Bromhexine ↓ a)by direct action b)by liberation of lysosomal enzymes ↓ Dissolves the mucopolysaccaride fibers ↓ Liquefaction of tenacious sputum occurs
↓Liquid sputum is easily removed out of tract
Short note :cough supressant/antitussives Mention classification from above
dopamine
stimulates β1 receptors on heart↓
↑ed heart rate and force of contraction↓
increased BP
stimulation of D1and D2 receptor↓
dilation of renal and visceral arterioles↓
↑ed blood flow to kidney and viscera
provides quick relief in shock
Mode of action: Cough suppressants
↓1) Acts on CNS to raise threshold of cough centre2) Acts on respiratory tract to reduce production of cough impulse
↓Controles cough of types1)dry ,unproductive2)tiring and sleep disturbing
DRUGS FOR BRONCHIAL ASTHMA
I)Bronchodilators a)sympathomimetics:salbutamol,terbutalin b)methylxanthines:aminophylline,theophylline c)anticholinergics:ipratropium bromideII)leukotriene antagonists:monteleukast,zafirleukastIII)Mast cell stabilisers:sodium cromoglycateIV)Corticosteroids: a)systemic:hydrocortisone,prednisolone b)inhalational:beclomethasone dipropionateV)Anti IgE-Antibody:omalizumab a)sympathomimeticsDrugs: salbutamol, terbutalin(selective β2 agonists)Basis for use in bronchial asthma:
Note:when inhaled produce bronchodilation within 5 min. And action lasts for 2-4 hrs only.so it is used for terminating an attack of asthma instead of round the clock prophylaxisAdverse effects of salbutamol MARcH PANT
Muscle tremor Ankle edema Restlessness Hypokalemia Palpitation Arrhythmia Nervousness Tachycardia
b)methylxanthinesdrugs:aminophylline,theophyllineBasis of use: Adverse effects of aminophylline ,theophylline:(µg/ml)
acts as selective β2 agonist↓
↑cAMP level in
bronchial muscle cell↓
bronchodilation occurs
mast cell and other inflammatory cell↓
↓ed response of inflammatory mediators
improves the airway obstruction, releives asthma
c)anticholinergics
drug:ipratropium bromidebasis of use in asthma: blockage of cholinergic receptor in large airways ↓ Bronchodilation occurs ↓ Provides relieve in asthmaNote:more suitable for regular prophylactic use,not for acute symptomatic relief Preferred because it has no effect on mucociliary clearance and respiratory secretions II)Mast cell stabilisersDrug: sodium cromoglycate,ketotifen
ABOVE
35:DEATH
AT35:CONVULSIONS,ARRYTHMIAS SHOCK
AT30:DELIRIUM,INCRE
ASED
MUSCLE
TONE, EXTRASYSTOLE
AT25:FLUSHING,AGITATION ,TACHYPNOE
AAT20:PALPITATION,VOMITING,RESTLESSNESS,TREMOUR,DIURESI
SAT15:HEADACHE,INSO
MNIA,NERVOUSNESS,DYSPEPSIA
AT10:MINI
MAL SIDE
EFFECTAT5:NO SIDE
EFFECT

Basis of use:
Mainly used for prophylactic purpose.
III)corticosteroids Systemic:hydrocortisone,prednisolone Inhalational:beclomethasone dipropionateBasis of use:
NASAL DECONGESTANTS:These are α agonists which when applied as a dilute solution produce local vasoconstrictionDrugs:naphazoline,xylometazoline,oxymetazoline,phenylephrine,pseudoephedrineMOA: Acts as α agonist ↓ Produce vasoconstriction and shrinkage of nasal mucosa ↓ Provides relief from nasal obstructionAdverse effectsSAARC
Stinging sensation Atrophic rhinitis Anosmia CNS depression Rise in BP
Uses:common cold ,allergic rhinitis
provides relief in asthma
inhibit degranulation of mass cells caused by triggering stimulus
↓inhibit release of inflammatory
mediators like LTs,PAF,from mast and other inflammatory cells.
decreased inflammatory response of bronchial muscle.
↓↓ed bronchospasm caused by allergens ,cold,irritants
Contraindication:HTN,patients on MAO inhibitors
DRUGS FOR TUBERCULOSIS:
First line drugs Second line drug Newer drugsIsoniazid(H) Thiacetazone CiprofloxacinRifampin(R) PAS OfloxacinPyrazinamide(Z)
Ethionamide Clarithromycin
Ethambutol(E) Cycloserine azithromycinStreptomycin(S) Kanamycin
Amikacin
Basis for use of Isoniazid: Sensitive bacteria concentrates isoniazid and convert it into active metabolite by catalase peroxidise enzyme. ↓Active metabolites binds with INH-A gene and inhibit synthesis of fatty acid synthase enzyme ↓ Inhibition of mycolic acid synthesis responsible for cell wall formation ↓ Produce bacteriocidal effect both extracellularly and intracellularlyBasis for use of rifampicin: Inhibits DNA dependent RNA polymerase ↓ Stoppage of expression of bacterial gene ↓ Tuberculocidal effect is exertedAdverse effects of anti-tubercular drug
ISONIAZID RIFAMPIN PYRAZINAMIDE ETHAMBUTOL STREPTOMYCINPeripheral neuritis Liver damage Hepatitis Optic nerve damage OtotoxicityPsychosis Influenza like rxn Hyperuricemia,gout Anaphylactic rxn NephrotoxicityHepatitis Orange –red
urineArthralgia Nausea,vomiting Anaphylaxis
Rashes,fever Fever,skin rash photosensitivity Confusion,headache eosinophilia DOTS regimen for TBDOTS strategy:emphasize on the use of all first line anti-tubercular drugs in single daily dosingBasis of combination of anti-tubercular drugs:
To prevent the emergence of resistant organisms and relapse of TB Use of H and R reduces duration from more than 12 months to less than 9 months whereas
addition of Z reduces it to 6 months
GASTRO INTESTINAL SYSTEM
DRUGS USED FOR PEPTIC ULCER
I)H2 antihistaminics:cimetidine, ranitidine
II)proton pump inhibitor:omeprazole ,pantoprazole, lansoprazole
Basis for use in peptic ulcer:
At acidic pH of canaliculi of parietal cell it get converted into active cationic forms
↓
Binds to cysteine residue of H+K+ATPase by stable covalent bond
↓
Inhibits H+K+ATPase pump irreversibly
↓
Inhibition of secretion of H+ ion into lumen
↓
No gastric acid secretion
Note: both basal and stimulated gastric acid secretion are inhibited
Also inhibit gastric mucosal case enzyme.
III)Basis for use of sucralfate in peptic ulcer
Acquire -ve charge at acidic pH due to seperstion of Al
↓
Binds to protein molecule tranducing from damage to ulcer base
↓
A viscous paste is formed that adheres to the ulcer base
↓
Protects ulcer base from actions of HCl ,pepsin and bile salts
Note: acts by inactivating bile acids and pepsin
Activate mucosal PG synthesis
IV) basis for use of bismuth chelate in peptic ulcer
↑es PG synthesis leads to ↑ed mucous and bicarbonate secretion Forms glycoprotein –bi complex with mucous which coats ulcer and prevent action of HCl Removes H.pylori from mucosal surface and kills it .so it prevents cause and relapse of ulcer Heals 60% ulcer in 4 wks and 90% ulcer in 8 wks.
Drugs Uses Adverse effectsH2 antihistaminics
Duodenal ulcer,gastric ulcer, stress ulcer,gastritis,ZEsyndrome,GERD,Prophylaxis of aspiration pneumonia
Dry mouth, headache, dizziness,bowel upset,rashes;CNS effects like confusional state ,convulsion coma
PPI Peptic ulcer,bleeding peptic ulcer,stress ulcer,GERD,ZE syndrome
Abdominal pain, muscle and joint pain,atrophic gastritis
sucralfate Peptic ulcer constipationANTIEMETICS
5HT-3 ANTAGONISTS( ondansetron)
Basis of use:
Prokinetic drug (metoclopramide,domperidone,cisapride)
-----------
Bisacodyl in laxative.
Note: bisacodyl is an stimulant purgative
Dose:5-15 mg :one to two semiformed motionafter 6-8 hrs
Given as suppository it irritates rectal and anal mucosa
↓
Reflex increase in GI motility
net accumulation of water and
elecrolyte in lumen
inhibition of Na+K+ATPase at basolateral membrane of
villous cells↓
↓reabsorption of water and eletrolytes
stimulation of adenyl cyclase
↓↓secretion of water and
elecrolytes
↑motility↓
↓reabsorption
↓
Evacuation in 20-40 hrs
LACTULOSE IN THERAPY:
Semisynthetic dissaccaride of fructose and lactose Neither digested nor absorbed in small intestine ,so retains water Changes to more osmotically active substance in colon and absorbs water due to bacterial action Dose:10mg BD with plenty of water produces soft stool ↓ ammonia level in hepatic encephalopathy patients
ALBENDAZOLE IN THERAPY
DIFFERERENCES AMONG/BETWEEN:
I)ACE inhibitors and Ang-II antagonists
ACE INHIBITORS ANG-II ANTAGONIST Interfere with the degradation of bradykinin
which leads to ↑ed bradykinin level Has no any such interference
Alternative path of A-II production and AT-1 receptor activation remains intact
Causes complete inhibition of AT-1 receptor
Causes inactivation of AT-1 and AT-2 receptor
Causes indirect AT-2 receptor activation
Has more potential to cause cough and dysguesia
Has very less potential to cause cough and dysguesia
II) Amlodipine and Nifedipine
AMLODIPINE NIFEDIPINE Slow oral absorption Fast oral absorption Complete absorption Incomplete absorption No early adverse effects flushing ,palpitation Early adverse effects seen Low 1st pass metabolism High 1st pass metabolism High volume of distribution and t⅟2 value low long duration of action short duration of action
immobilization and death
of worms
Binds with β tubulin protein in susceptible
worms↓
no microtubule synthesis in worms

III) TETRACYCLINES
Tetracycline Domecycline Doxycycline Potency Low Intermediate High Plasma protein binding Low High High t⅟2 6-10hr 16-18hr 18-24hrAlteration of normal flora
Marked Moderate Least
Diarrhoea High Intermediate Low Phototoxicity Low Highest High
IV)Proton punp inhibitors
Omeprazole Lansoprazole Pantoprazole Esmoprazole Inhibition of H+K+ATPase pump
irreversible Partly reversible Irreversible Irreversible
Effect on H.pylori infection
Less More Less Less
Oral bioavailability and t⅟2
↓ ↑ ↓ ↓
Onset and duration of action
Relatively slow Fast Slow Slow
Route Oral Oral i.v Oral
V)β BLOCKERS
Propranolol Timolol Metoprolol Atenolol
Labetalol
Drug type β 1+β2 β 1+β2 β 1 β 1 β +αPotency on β1 1 6 1 1 ⅓Partial agonists - - - - -Membrane stabilising action ++ +- +- - +Lipid solubility ++ + + - +1st pass metabolism Yes Partial Yes No Yes Route of excretion Hepatic Hepatic +renal hepatic renal HepaticOral bioavailability 30 50-75 40-50 50-60 20
VI)CEPHALOSPORINS
1st generation 2nd generation 3rd generation 4th generationparenteral: cefazoline,cephalothin.Oral:cephalexin
Parenteral :cefuroxime,cefoxitin.Oral:cefaclor
Parenteral :ceftriaxoneOral : cefixime
Parenteral:cefepime
Gram +ve /gm-ve cocci except E.coli, proteus,K.pneumoniae
Gm-ve coverage with some anaerobes
Gm+ve/gm-ve cocci with gm-ve rods
Broad spectrum
None enters CNS Only cefuroxime enters CNS
None None
VII)Macrolides
Erythromycin Clarithromycin Azithromycin 1 Metabolised by liver,excreted through
bileMetabolised by liver, excreted through bile
Excreted by kidney
2 Inhibits cytochrome P450 inhibits No inhibition3 Unsafe in pregnancy unsafe Safe4 Destroyed by gastric acid so tab. Is
coatedNot effected Not effected
5 Food interfere with absorption ↓es absorption interferesVIII)Aminoglycosides
Streptomycin Gentamycin Tobramycin Amikacin Neomycin narrow spectrum:gm-ve bacilli and few gm+ve cocci
broad spectrum like gentamycin but 2-4 times more potent against pseudomonas and proteus
wide spectrum due to resistance to bacterial aminoglycoside inactivating enzyme
Wide
ineffective against pseudomonas and proteus and effective against only only few strains of E.coli,klebsiella and enterobacter
effective against pseudomonas,and proteus and also against most strains of E.coli,klebsiella,enterobacter
lownephrotoxicity and ototoxicity than gentamycin
Use like gentamycin but less potent against pseudomonas and proteus
Not effective against pseudomonas and streptococcal pyogenes
effective against M.TB.,staphylococcus pneumonia,strept.pyogenes
not effective Mainly in hospital infection
Systemic toxicity is high ,used topically
less potent more potent
low nephrotoxicityhigh nephrotoxicity
IX)FLUROQUINOLONES/QUINOLONES
Oral bioavailability%
PPB% Route Indications
1st generationCiprofloxacin 60-80 20-
35Oral/i.v
UTI,gonorrhoea,chanchoroid,MDRTB
Norfloxacin 35-45 15 Oral UTI,GI InfectionOfloxacin 85-95 25 Oral/iv Alternate drug for NSV,cervicitisPefloxacin 90-100 20-30 Oral/
i.vMeningitis,UTI,GI INFECTION
2nd generation
Lomefloxacin 90 10 Oral Like ciprofloxacin but increases activity of gm –ve bacteria
sparfloxacin 90 40 oral Pneumonia,exacerbation of acute bronchitis,sinusitis
X)Cough suppressant drugs:
Pharyngeal demulcents Opoids Non opoids Antihistaminics Acts peripherally,soothes the throat and reduce afferent impulse from pharyngeal mucosa
1)acts on CNS to raise threshold of cough centre2)has abuse liability3)more constipating effect.4)action blocked by naloxone.
1)acts on CNS to raise threshold of cough centre2)no abuse 3)no constipating effect4)no such blockade occurs
Suppresses cough by sedative and anticholinergic action
SHORT NOTE
1)bioavailability measure of fraction of administered dose of drug that reaches systemic circulation in unchanged
form bioavailability of different routes:
i.v.=100%s.c/i.m =less than 100% due to local PPBoral=much less due to first pass metabolism
factors affecting bioavailability are:a)route of administrationb)physical properties of drugsc)chemical properties of drugsd)individual variation
e)first pass metabolism
2)first pass metabolism refers to the metabolism of drug during its passage from site of absorption into the systemic
circulation all orally administered drugs are expsosed to metabolising enzymes in liver and intestine. Occurs even in skin and lungs Different for different drugs and it determines oral bioavailability Degree of first pass metabolism ;
a)low:phenobarbitoneb)intermediate:aspirinc)high:propranolol
3)metabolism of drugs(biotransformation) Chemical alteration of drug in the body Lipid soluble drug is converted into lipid insoluble drug which is not reabsorbed and is excreted Sites:mainly liver,also in kidney ,intestine,lung It leads to
a)inactivation of drugs;morphineb)activation of inactive drug:levodopa is converted into dopaminec)active metabolite production from active drug:digitoxin is converted to digoxin
Classification of metabolism
Nonsynthetic/phase I/Functionalization rxn
Synthetic/conjugation/Phase II reactions
1.oxidation 1.glucuronide conjugation2.reduction 2.acetylation3.hydrolysis 3.methylation4.cyclization 4.sulfate conjugation5.decyclization 5.glycine conjugation
6.glutathione conjugation 4)phase II metabolism/synthetic rxn Involves conjugation of drug or phase I metabolite with endogeneous substance to form highly ionised
organic acid so that it is excreted in urine or bile It requires very high energy Involves following reactions
a)glucuronide conjugation:conjugated by glucoronic acid eg:aspirin ,morphineb)glutathione conjugation eg:paracetamolc)glycine conjugation:conjugated by glycine eg:salicylatesd)methylation:conjugated by methionine eg:adrenalinee)acetylation:conjugated by acetyl coAf)ribonucleoside synthesis:for purine and pyrimidine antimetabolite used in cancer therapyg)sulphate conjugation: conjugated by sulfokinase eg:sex steroids
5)criterias for essential drug selections Adequate data regarding efficacy and safety of drug should be available through clinical studies In case of two or more similar drug choice should be based on their relative efficacy,safety,
quality,price and availability Choice should be based on pharmacokinetic properties Should be single compound
6)disadvantages of antimicrobial combination therapy It prevents proper diagonis of infection and choice of AMA Increased incidence of side effects as toxicity of one agent can be enhanced by another Increased chances of superinfection Inadequate dose of drug may lead to emergence of resistance Increases cost of therapy
7)low dose aspirin
Balance between the above two helps in the maintainance of circulation When low dose aspirin is used ↓ Inhibition of cycloxygenase enzyme occurs in platelets by acetylation to great extent as compared to endothelial cells ↓ Failure of platelet to resynthesize cox enzyme results in decreased TXA2 and ↑ed PGI2 level ↓ No platelet sticking and thrombus formation occurs ↓ Helps in prevantion of attack of MI
8)drugs used to decrease platelet aggregation NSAIDs:aspirin Dipyridamole Clopidogrel Ticlopidine Abciximab
9)uses of vitamin K preparations Adult vitamin K deficiency(malabsorption,obstruction,jaundice) Vitamin K deficiency in infant following acute diarrhoea Neonatal vitamin K deficiency Bleeding state during oral coagulant therapy
10)oral rehydration solution Used for mild (5-7%BW) or moderate (7.5-10%BW) type of dehydration Composition of ORS(WHO)
OLD NEWNaCl 3.5g 2.6gKCl 1.5g 1.5gTrisodium citrate 2.9g 2.9gGlucose 20g 13.5gWater 1litre 1litre
arachidonic acid↓cycloxygenase
in platelets↓
TX-A2 formation↓
promote platelet aggregation and thrombi formation
in endothelial cells↓
PGI2 formation↓
inhibit platelet aggregation

310mosm/i 245mosm/l
The old ORS formulation was mainly effective for cholera diarrhoea,but when used in non cholera diarrhoea it causes periorbital edema due to excess Na+ reabsorption
So in new ORS formulation the concentration of sodium and glucose is reduced but it has the disadvantage of causing hyponatremia if used in cholera diarrhoea in adults
Rational of components useda)Na and water facilitates each others absorption in GITb)KCl :to compensate acute diarrhoeal K+ loss
c)bicarbonate,citrate, lactate:to correct acidosis Uses:
a)diarrhoeab)non diarrhoeal reasons: heat stroke,post burn/post surgical maintainance of hydration and nutrition.


















