4π Noncoplanar Stereotactic Body Radiation Therapy …ksheng.bol.ucla.edu/4piHN.pdf · 4p...
9
Physics Contribution 4p Noncoplanar Stereotactic Body Radiation Therapy for Head-and-Neck Cancer: Potential to Improve Tumor Control and Late Toxicity Jean-Claude M. Rwigema, MD,* Dan Nguyen, BS,* Dwight E. Heron, MD, y Allen M. Chen, MD,* Percy Lee, MD,* Pin-Chieh Wang, PhD,* John A. Vargo, MD, y Daniel A. Low, PhD,* M. Saiful Huq, PhD, y Stephen Tenn, PhD,* Michael L. Steinberg, MD,* Patrick Kupelian, MD,* and Ke Sheng, PhD* *Department of Radiation Oncology, University of California Los Angeles, Los Angeles, California; and y Department of Radiation Oncology, University of Pittsburgh Cancer Institute, Pittsburgh, Pennsylvania Received May 27, 2014, and in revised form Aug 27, 2014. Accepted for publication Sep 30, 2014. Summary Stereotactic body radiation therapy is increasingly used in head-and-neck cancer, mainly for recurrent previ- ously irradiated head-and- neck cancer. Recent data on reirradiation using SBRT suggest the potential to reduce severe late toxicity, while maintaining similar local control relative to conventionally fractionated radiation therapy. We tested 4p radiation therapy in recurrent, primary unresect- able, and metastatic head- and-neck cancer. Our results Purpose: To evaluate the potential benefit of 4p radiation therapy in recurrent, locally advanced, or metastatic head-and-neck cancer treated with stereotactic body radiation therapy (SBRT). Methods and Materials: Twenty-seven patients with 29 tumors who were treated us- ing SBRT were included. In recurrent disease (nZ26), SBRT was delivered with a me- dian 44 Gy (range, 35-44 Gy) in 5 fractions. Three patients with sinonasal mucosal melanoma, metastatic breast cancer, and primary undifferentiated carcinoma received 35 Gy, 22.5 Gy, and 40 Gy in 5 fractions, respectively. Novel 4p treatment plans were created for each patient to meet the objective that 95% of the planning target volume was covered by 100% of the prescription dose. Doses to organs at risk (OARs) and 50% dose spillage volumes were compared against the delivered clinical SBRT plans. Local control (LC), late toxicity, tumor control probability (TCP), and normal tissue complication probability were determined. Results: Using 4p plans, mean/maximum doses to all OARs were reduced by 22% to 89%/10% to 86%. With 4p plans, the 50% dose spillage volume was decreased by 33%. Planning target volume prescription dose escalation by 10 Gy and 20 Gy were achieved while keeping doses to OARs significantly improved or unchanged from clin- ical plans, except for the carotid artery maximum dose at 20-Gy escalation. At a Reprint requests to: Ke Sheng, PhD, Department of Radiation Oncology, 200 Medical Plaza, B265, University of California, Los Angeles, Los Angeles, CA 90095. Tel: (310) 853-1533; E-mail: ksheng@ mednet.ucla.edu Presented at the 56th Annual Meeting of the American Society for Radiation Oncology, September 14-17, 2014, San Francisco, CA. Conflict of interest: none. Supplementary material for this article can be found at www.redjournal.org. AcknowledgmentsdThe study was supported in part by Varian Med- ical Systems. The authors thank Karen Holeva for her support with data management. Int J Radiation Oncol Biol Phys, Vol. -, No. -, pp. 1e9, 2014 0360-3016/$ - see front matter Ó 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ijrobp.2014.09.043 Radiation Oncology International Journal of biology physics www.redjournal.org
Transcript of 4π Noncoplanar Stereotactic Body Radiation Therapy …ksheng.bol.ucla.edu/4piHN.pdf · 4p...

International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Physics Contribution
4p Noncoplanar Stereotactic Body RadiationTherapy for Head-and-Neck Cancer: Potential toImprove Tumor Control and Late ToxicityJean-Claude M. Rwigema, MD,* Dan Nguyen, BS,*Dwight E. Heron, MD,y Allen M. Chen, MD,* Percy Lee, MD,*Pin-Chieh Wang, PhD,* John A. Vargo, MD,y Daniel A. Low, PhD,*M. Saiful Huq, PhD,y Stephen Tenn, PhD,* Michael L. Steinberg, MD,*Patrick Kupelian, MD,* and Ke Sheng, PhD*
*Department of Radiation Oncology, University of California Los Angeles, Los Angeles, California;and yDepartment of Radiation Oncology, University of Pittsburgh Cancer Institute, Pittsburgh,Pennsylvania
Received May 27, 2014, and in revised form Aug 27, 2014. Accepted for publication Sep 30, 2014.
Summary
Stereotactic body radiationtherapy is increasingly usedin head-and-neck cancer,mainly for recurrent previ-ously irradiated head-and-neck cancer. Recent data onreirradiation using SBRTsuggest the potential toreduce severe late toxicity,while maintaining similarlocal control relative toconventionally fractionatedradiation therapy. We tested4p radiation therapy inrecurrent, primary unresect-able, and metastatic head-and-neck cancer. Our results
Reprint requests to: Ke Sheng, PhD, D
Oncology, 200 Medical Plaza, B265, Univ
Angeles, Los Angeles, CA 90095. Tel: (310) 85
mednet.ucla.edu
Presented at the 56th Annual Meeting of
Radiation Oncology, September 14-17, 2014, S
Int J Radiation Oncol Biol Phys, Vol. -, No.
0360-3016/$ - see front matter � 2014 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2014.09.043
Purpose: To evaluate the potential benefit of 4p radiation therapy in recurrent, locallyadvanced, or metastatic head-and-neck cancer treated with stereotactic body radiationtherapy (SBRT).Methods and Materials: Twenty-seven patients with 29 tumors who were treated us-ing SBRTwere included. In recurrent disease (nZ26), SBRTwas delivered with a me-dian 44 Gy (range, 35-44 Gy) in 5 fractions. Three patients with sinonasal mucosalmelanoma, metastatic breast cancer, and primary undifferentiated carcinoma received35 Gy, 22.5 Gy, and 40 Gy in 5 fractions, respectively. Novel 4p treatment plans werecreated for each patient to meet the objective that 95% of the planning target volumewas covered by 100% of the prescription dose. Doses to organs at risk (OARs) and50% dose spillage volumes were compared against the delivered clinical SBRT plans.Local control (LC), late toxicity, tumor control probability (TCP), and normal tissuecomplication probability were determined.Results: Using 4p plans, mean/maximum doses to all OARs were reduced by 22% to89%/10% to 86%. With 4p plans, the 50% dose spillage volume was decreased by33%. Planning target volume prescription dose escalation by 10 Gy and 20 Gy wereachieved while keeping doses to OARs significantly improved or unchanged from clin-ical plans, except for the carotid artery maximum dose at 20-Gy escalation. At a
epartment of Radiation
ersity of California, Los
3-1533; E-mail: ksheng@
the American Society for
an Francisco, CA.
Conflict of interest: none.
Supplementary material for this article can be found at
www.redjournal.org.
AcknowledgmentsdThe study was supported in part by Varian Med-
ical Systems. The authors thank Karen Holeva for her support with data
management.
-, pp. 1e9, 2014r Inc. All rights reserved.

Rwigema et al. International Journal of Radiation Oncology � Biology � Physics2
show improved organ
sparing and the potential tosafely enhance tumor controlwith dose escalation.median follow-up of 10 months (range, 1-41 months), crude LC was 52%. The 2-yearLC of 39.2% approximated the predicted mean TCP of 42.2%, which increased to45.9% with 4p plans. For 10-Gy and 20-Gy dose escalation, 4p plans increasedTCP from 80.1% and 88.1% to 85.5% and 91.4%, respectively. The 7.4% rate of grade�3 late toxicity was comparable to the predicted 5.6% mean normal tissue complica-tion probability for OARs, which was significantly reduced by 4p planning at the pre-scribed and escalated doses.Conclusions: 4p plans may allow dose escalation with significant and consistent im-provements in critical organ sparing, tumor control, and coverage.� 2014 Elsevier Inc.
Introduction
Despite improvements in the multimodality treatment ofprimary head-and-neck cancer, local recurrence after pri-mary treatment remains significant and accounts for morethan 50% of disease-related mortality (1). Stereotactic bodyradiation therapy (SBRT) has emerged as a salvage treat-ment strategy with many clinical applications in patientswith head-and-neck cancer. In particular, for those withunresectable recurrent previously irradiated head-and-neckcancer, a number of studies, including a single-institutionphase 1 and multi-institution phase 2 trials, have demon-strated the feasibility of SBRT, with efficacy similar to thatof intensity modulated radiation therapy (IMRT) and3-dimensional conformal radiation therapy (2-6). Othershave investigated the use of SBRT in the primary setting oflocally advanced unresectable primary or metastatic head-and-neck cancers, or to overcome radioresistance amongother cancers (7-9).
The rates of severe late toxicities pose a major concernwhen contemplating head-and-neck cancer reirradiation,mainly owing to the poor tolerance of critical structuressurrounding the previously irradiated treatment target.Current SBRT data, although not randomized, suggest thepossibility of reducing severe late complications whencompared with conventionally fractionated radiation ther-apy, owing to the highly precise delivery of radiation dose tothe target volume with minimal dose to surrounding organs-at-risk (OARs) (10). The most common SBRT regimen,consisting of 5 fractions delivered on alternating days(QOD), has been shown to be generally safer than treatmentdelivered on consecutive days (QD). Specifically, the rates ofgrade �3 late toxicities with QOD seem to be on average�10% (4, 5, 7) and seem to increase to approximately 20%with QD (11, 12). Studies have also evaluated radio-sensitization with concurrent cetuximab, image guidance,optimal treatment target definition, and treatment duration,as well as quality of life after SBRT, to further demonstratethe feasibility and improved outcomes of SBRT (3, 13-17).
Although the improved local tumor control and treat-ment safety of SBRT seem promising, the limited 2-yearlocal control (LC) rates of 30 to 52% (4-7) and the potentialfor severe toxicities with SBRT make SBRT a challengingsalvage option for patients who cannot afford a second localfailure coupled with added toxicity. Therefore, in the
present study, we sought to investigate whether 4p planningcould improve the dosimetry and quality of SBRT plansdelivered using a variety of standard techniques, to deter-mine whether the risk of severe late complications can befurther reduced without causing a decline in LC.
The 4p system has already been shown to potentiallyprovide improved dose conformality, reduced dose spillageto normal OARs, and lower integral dose when comparedwith volumetric modulated arc therapy (VMAT) in SBRTfor central lung tumors, liver tumors, and prostate cancer(18-20). For central lung tumors, dose escalation was alsosafely achieved (19). In this work we tested whether doseescalation was feasible in previously irradiated or advancedhead-and-neck cancer.
Methods and Materials
Twenty-seven patients (median age 66 [range, 42-87] years;14 male) with 29 malignant tumors previously treated usingSBRT at the University of California Los Angeles (nZ8)and at the University of Pittsburgh Cancer Institute (nZ19)from February 2007 to October 2013 were included in thestudy. Details of patient and previous treatment character-istics are shown in Table 1.
For recurrent previously irradiated tumors (nZ26),SBRTwas delivered with a median 44 Gy (range, 35-44 Gy)in 5 fractions QOD at a median interval of 20 months fromthe initial radiation therapy course of a median 70 Gy(range, 45-131.2 Gy) for primary disease. Four patients hadpreviously received multiple courses of radiation therapywith cumulative doses >110 Gy and required SBRT forfocal recurrences in the neck (nZ3) and maxillary sinus(nZ1) (Table 1). Seven patients (25.9%) had concurrentcetuximab with SBRT reirradiation at 400 mg/m2 on day�7then 250 mg/m2 on day 0 and þ8. Three patients withsinonasal mucosal melanoma, metastatic breast cancer,and unresectable primary undifferentiated carcinoma hadreceived 35 Gy, 22.5 Gy, and 40 Gy in 5 fractions QOD,respectively. Different radiosurgery systems were utilized todeliver SBRT, including CyberKnife (nZ6) (Accuray,Sunnyvale CA), Novalis Tx (nZ9) (Varian Medical Sys-tems, Palo Alto, CA; and BrainLAB, Feldkirchen, Ger-many), Trilogy (nZ8), and TrueBeam STx (nZ6) (VarianMedical Systems). The clinical plans used static IMRT(nZ24), noncoplanar VMAT (nZ1), and coplanar VMAT

Table 1 Patient and treatment characteristics
Patientno.
Age(y) Gender Histology
Prior RTdose (Gy)*
Primarysite
SBRTdose (Gy)y
SBRTsite
TV(cm3) Machine Technique
1 59 M SCC 131 Oropharynx 40 Neck 18.9 Novalis-Tx C-VMAT2 77 F SCC 45 Oral tongue 40 Base of tongue 83.4 Novalis-Tx S-IMRT3 86 M UC NA Pterygoid 40 Pterygoid 32.3 Novalis-Tx S-IMRT4 71 M SCC 45 Base of tongue 40 Base of tongue 209.4 Novalis-Tx C-VMAT5 67 M SCC Unknown Larynx 40 Larynx 5.9 Novalis-Tx S-IMRT6 71 M SCC 86.4 Tongue 35 Neck 202.8 Novalis-Tx S-IMRT7a 78 M AC NA Breast 22.5 Neck 41.6 Novalis-Tx C-VMAT7b 78 M SCC 129 Oropharynx 40 Neck 6.2 Novalis-Tx C-VMAT8 83 F SNMM NA Nasal cavity 35 Nasal cavity 78.5 Novalis-Tx NC-VMAT9 75 M SCC 66.6 Parotid 44 Cervical spine 41.9 Cyberknife S-IMRT10 62 M SCC 71.3 Larynx 35 Neck 15.7 Cyberknife S-IMRT11 54 M UC 70 Nasopharynx 44 Base of skull 83.9 Cyberknife S-IMRT12 80 F PCT 70.2 Thyroid 44 Retrostyloid 75 Cyberknife S-IMRT13 61 F SCC 70 Nasopharynx 44 Base of skull 38 Cyberknife S-IMRT14 85 F AC 68.4 Parotid 44 Parotid 22.4 Cyberknife S-IMRT15 72 M SCC 63 Larynx 44 Hypopharynx 50.6 TrilogyTM S-IMRT16 50 M SCC 70 Base of tongue 40 Oropharynx 12.7 TrilogyTM S-IMRT17a 61 F UC 112 Sinonasal 44 Maxillary sinus 2.8 TrilogyTM S-IMRT17b 61 F UC 112 Sinonasal 44 Neck 3.7 TrilogyTM S-IMRT18 42 F SCC 70 Nasopharynx 44 Nasopharynx 89 TrilogyTM S-IMRT19 54 M AC 64 Oropharynx 44 Oropharynx 25.8 TrilogyTM S-IMRT20 75 F SCC 70 Base of tongue 40 Base of tongue 13.6 TrilogyTM S-IMRT21 79 M SCC 68.8 Larynx 44 Larynx 63.3 TrilogyTM S-IMRT22 70 F MC 61.2 Palate 44 Maxillary sinus 9.7 TrueBeam-STX S-IMRT23 65 F MC Unknown Parotid 44 Parotid 74.4 TrueBeam-STX S-IMRT24 46 M ACC 66 Parotid 44 Submandibular 63.3 TrueBeam-STX S-IMRT25 60 M SCC 70 BOT/FOM 44 Base of tongue 195 TrueBeam-STX S-IMRT26 70 F SCC 70 Oropharynx 40 Oropharynx 16.5 TrueBeam-STX S-IMRT27 70 F SCC 64 Oral cavity 44 Palate 40.5 TrueBeam-STX S-IMRT
Abbreviations: AC Z adenocarcinoma; ACC Z acinic cell carcinoma; BOT/FOM Z base of tongue/floor of mouth; MC Z myeloepithelial carci-
noma; C-VMAT Z coplanar volumetricemodulated arc therapy; NC-VMAT Z noncoplanar volumetricemodulated arc therapy; PCT Z papillary
carcinoma of thyroid; SNMM Z sinonasal mucosal melanoma; SCC Z squamous cell carcinoma; S-IMRT Z static intensity modulated radiation
therapy; TV Z tumor volume; UC Z undifferentiated carcinoma.
a, b denote patients with 2 lesions.
* Total prior prescription dose.y SBRT dose in 5 fractions.
Volume - � Number - � 2014 4p SBRT for head-and-neck cancer 3
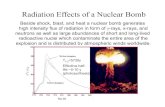
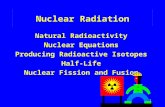
(nZ4). Figure 1a shows typical beam orientation patterns of4p planning compared with static IMRT, coplanar VMAT,and noncoplanar VMAT. All clinical plans were initiallygenerated and optimized using treatment planning systemscorresponding to the different techniques used clinically.All clinical and 4p plans were then imported into CERR(Computational Environment for Radiotherapy Research,Washington University, St. Louis, MO) and dose distribu-tions evaluated using identical settings.
The novel 4p treatment planning process has beenpreviously described (17-19). Briefly, the 4p method is ahighly noncoplanar and nonisocentric planning systemdeveloped on C-arm gantry linear accelerators. For eachpatient a candidate pool was created consisting of 1162beams evenly distributed throughout the 4p solid sphereangle space, with approximately 6� of separation betweenadjacent beams. A beam geometry solution space wasinitially created using the 3-dimensional surface images ofa human subject and the treatment machine to determine
the minimal distances between the x-ray source and thetumor for each beam angle. A collision buffer of 4 cm wasadded to the distances. If the resultant distance was>100 cm, extended source-to-tumor distances were used.Beams that still resulted in collision of the gantry andcouch or patient due to reaching the couch movementlimits were excluded. Of the remaining candidate beams,30 intensity modulated beams were automatically selectedto meet the objective of 95% of the planning target volume(PTV) covered by 100% of the prescription dose. Thecandidate beams were segmented into 5 � 5-mm2 beam-lets. This was followed by the calculation of2.5 � 2.5 � 2.5-mm3 resolution dose matrices using an in-house convolution/superposition code with 6-MV poly-energetic kernels. A column generation algorithm (21)was used to iteratively select and optimize the beamsuntil the desired number of 30 beams was reached.
In addition to the plans adhering to their original pre-scription doses, dose escalation plans of 10 Gy and 20 Gy

Fig. 1. (a) Typical entrance patterns of 4p beams versusvolumetric modulated arc therapy (VMAT) (coplanar andnoncoplanar) beams and static intensity modulated radia-tion therapy (IMRT) beams. (b) Axial, coronal, and sagittalCT views with dose wash of the clinical case and the 4pplans at prescription and escalated planning target volumedoses for a single patient. The color bar was adjusted to beuniform between all cases. All 4p plans spare the carotidartery (axial view) compared with the clinical plan. A colorversion of this figure is available at www.redjournal.org.
Rwigema et al. International Journal of Radiation Oncology � Biology � Physics4
additional dose to the PTV were also created on the clinicaland 4p planning systems and evaluated using CERR. Dosesto OARs and 50% dose spillage volume index (R50) werecompared against the delivered clinical SBRT plans. R50
was used as a measure of the high dose gradient outside thePTV. R50 was defined as:
R50ZV50
VPTV
ð1Þ
where V50 is the total volume receiving 50% or more of theprescription dose, and VPTV is the volume of the PTV. To
maintain a consistent correlation between R50 and normaltissue toxicity, V50 was defined according to the originalprescription dose in the dose-escalated plans.
Planning target volume coverage was determined andcompared with the clinical plans by evaluating the dose thatcovered 95%, 98%, and 99% of the PTV, as well as the PTVminimum and maximum doses (ie lowest and highest pointdoses in the PTV corresponding to the volume of 1 voxel).Crude and actuarial LC and late toxicity rates, aswell as tumorcontrol probability (TCP) and normal tissue complicationprobability (NTCP) were determined. Local control wasdefined as any reduction in tumor volume and/or metabolicactivity as assessed with follow-up positron emission to-mography/CT and/or MRI as well as clinical examination.Kaplan-Meier analysis was used to determine actuarial LCrates. Toxicity was graded according to the Common Termi-nology Criteria for Adverse Events, version 3 (22).
TCP was calculated as:
TCPZexpð �DcV expð�aBEDÞÞ ð2Þwhere Dc is the clonogens density Z 107/cm3, V is thetumor GTV volume, and BED is the biological equivalentdose calculated assuming a/b Z 10 Gy for the tumor (22).The TCP was determined at tumor radiosensitivities (a) of0.15/Gy, 0.25/Gy, and 0.35/Gy (23, 24).
NTCP was calculated according to the Lyman model(23), defined as:
NTCPZ1ffiffiffiffiffiffi2p
pZ t
�N
exp
��x2
2
�dx ð3Þ
where
tZ½D� TD50ðvÞ�½m TD50ðvÞ� ð4Þ
vZV
Vref
ð5Þ
TD�v�ZTD
�1�)v�n ð6Þ
and TD50 is the dose that led to a 50% complication rate, nis the volume dependence parameter, m is the slope of thecomplication probability dose curve, Vref is the referencevolume, V is the actual volume irradiated, and v is thefractional volume irradiated (25). Statistical comparisonsfor between groups were performed with a paired t test fordata with a normal distribution, otherwise a nonparametricWilcoxon rank test was used to compare means all with astatistical significance of PZ.05 (2-tailed).
Results
At the same prescription dose (4pPD), the mean andmaximum (Dmax) doses to OARs were reduced with 4pplans compared with clinical plans. Significant reductions(P<.05) were observed for the spinal cord, the brainstem,pharyngeal constrictor muscles, parotid glands, the larynx,the mandible, the cochlea, and the optic apparatus (iechiasm, eye, lens, and optic nerves), whereas statisticallynonsignificant (P>.05) reductions were obtained for the

Volume - � Number - � 2014 4p SBRT for head-and-neck cancer 5
brachial plexus, the carotid artery, and the cervical esoph-agus (Table 2). Dose spillage outside the PTV, as measuredby R50, was reduced by 33% (P<.001) (Table 3). Coverageof the PTV was improved according to respective increasesin PTV maximum and mean doses, D95, D98, and D99 by4.4%, 5.5%, 2.4%, 4.7%, and 6.5%, respectively (P<.01).The 1.7% increase in PTV minimum dose was not statis-tically significant (PZ.69). Planning target volume pre-scription dose escalations by 10 Gy (4pPD þ 10 Gy) in 5fractions were achieved with a simultaneous reduction inR50 by 5.7% (PZ.07, Table 3), and doses to OARssignificantly improved or were unchanged from clinicalplans (Table 2). For 20-Gy escalation (4pPD þ 20 Gy) in 5fractions, R50 was increased by 24.2% (PZ.001, Table 3);however, doses to OARs were still significantly improvedor unchanged from clinical plans, except for a significantincrease in Dmax for the carotid artery (Table 2). Whenpatients with tumors partially or completely wrapping thecarotid artery were excluded (nZ9), the reductions incarotid artery mean dose and Dmax were maintained withdose escalation at both levels (Table 2).
Figure 1b shows a planning CT with a dose color washfor a typical 4p case in axial, coronal, and sagittal pro-jections. The dose spillage reduction with 4p plans, asdemonstrated with improved R50, was consistent with theobserved steep dose fall-off outside the PTV that resulted inreduced volume receiving 50% of the original prescription
Table 2 Reductions in mean and maximum doses to organs at risk
Organ at risk
4pPD
Mean (%) P* Dmax (%) P* Mean
Spinal cord 60 <.001 53 <.001 50Brainstem 53 .017 46 .006 40Mandible 45 <.001 22 .001 33Ipsilateral parotid 66 .002 60 <.001 54Contralateral parotid 66 .004 60 <.001 57Pharyngeal constrictor
muscles55 <.001 40 <.001 40
Larynx 57 .004 35 .038 47Cervical esophagus 74 .067 49 .336 66Ipsilateral carotid 22 .014 10 .096 2Ipsilateral carotidz 58 .080 41 .121 49Contralateral carotid 55 .003 57 .001 41Brachial plexus 48 .203 32 .383 33Ipsilateral cochlea 82 .002 65 .004 78Contralateral cochlea 86 .004 77 .005 82Ipsilateral lens 82 .090 74 .064 76Contralateral lens 89 .126 86 .106 78Ipsilateral eye 72 .041 43 .051 56Contralateral eye 70 .023 41 .028 60Ipsilateral optic nerve 68 .006 28 .220 54Contralateral optic nerve 77 .015 56 .014 70Chiasm 81 .010 67 .017 74
Abbreviation: PD Z prescription dose.
* Paired t test P values.y Negative values reflect increased doses to organs at risk.z With patients with tumors partially or completely wrapping the carotid ex
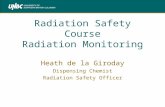
dose even in the 10-Gy dose-escalated plan. Figure 2a and bshow example doseevolume histograms, which demon-strate the improved dosimetry with 4p plans compared withclinical plans. At escalated doses, doseevolume histogramsstill indicated OAR doses lower with 4p plans than wasobserved in nonescalated clinical plans (Fig. 2b).
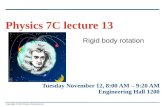
At a median follow-up of 10 months (range, 1-41 months), the crude LC of our cohort was 52%. Themedian overall survival (OS) was 12 months with a cor-responding 2-year LC of 39.2% (actuarial data not shown).The calculated individual patient TCP for clinical plansand 4p plans is shown in Table E1 (available online atwww.redjournal.com). Figure 3 shows the mean TCPcurves for both clinical and 4p plans at a of 0.35. Theclinical TCP of 42.2% at initial prescription dose approx-imated the patient cohort’s LC at 39.2%, suggesting that theradiosensitivity of tumors in the study cohort is closer to0.35. Predicted TCP results using a of 0.25 and 0.15 were<10%, significantly different from the clinical observation,thus not shown here. Using 4p planning, clinical TCPincreased to 45.9% (PZ.02). The slight increase was due toreduced cold spots by 4p as seen in Figure 2a. At 10-Gyand 20-Gy escalation, the clinical TCP was respectivelyincreased from 80.5% and 88.1% to 85.5% (PZ.24) and91.4% (PZ.32) with 4p plans.
There were 3 late toxicities (11.1%), consisting of grade2 dysphagia, grade 3 dysphagia, and grade 3
from clinical plans in comparison with 4p planning
4pPD þ 10 Gy 4pPD þ 20 Gy
(%) P* Dmax (%) P* Mean (%) P* Dmax (%) P*
<.001 40 <.001 40 .001 30 .008.066 34 .022 30 .164 5 .827.001 4 .714 26 .016 �9y .289.007 48 .001 42 .030 36 .014.009 48 .001 45 .025 38 .014
<.001 24 .010 33 .001 14 .187
.006 18 .404 43 .042 7 .953
.110 31 .570 61 .141 26 .684
.845 �11y .230 �19y .086 �26y .041
.163 26 .431 41 .272 14 .786
.008 33 .006 28 .020 18 .040
.401 13 .877 19 .619 �6y .772
.003 56 .011 65 .004 39 .041
.004 72 .005 59 .008 52 .009
.081 70 .060 53 .030 48 .061
.117 71 .106 67 .228 64 .113
.025 38 .048 33 .061 23 .373
.016 24 .268 50 .033 15 .442
.007 9 .748 39 .009 2 .954
.015 48 .027 67 .014 41 .068
.013 59 .034 67 .023 57 .055
cluded.

Table 3 Planning target volume (PTV) statistics for clinical planning as compared with 4p planning at different dose levels
Parameter Clinical, mean SD
4pPD 4pPD þ 10 Gy 4pPD þ 20 Gy
Mean SD P* Mean SD P* Mean SD P*
PTV mean dose (Gy) 41.5 5.3 43.9 5.4 .005 54.6 5.5 <.001 63.4 4.4 <.001PTV max dose (Gy) 45.8 6.6 47.9 6.6 .003 59.1 6.7 <.001 68.0 5.5 <.001PTV min dose (Gy) 29.7 10.3 30.2 10.1 .69 42.1 14.7 <.001 40.6 15 <.001D95 (Gy) 40.3 5.0 41.3 5.1 <.001 51.4 5.2 <.001 60.1 3.9 <.001D98 (Gy) 38.8 5.3 40.7 5.1 .001 50.5 5.3 <.001 58.9 4.2 <.001D99 (Gy) 37.2 6.2 39.8 5.4 .006 49.2 5.9 <.001 57.1 5.7 <.001R50 5.3 2.1 3.5 1.6 <.001 5.0 1.9 .07 6.6 2.9 .001
Abbreviation as in Table 2.
* Paired t test P values.
Rwigema et al. International Journal of Radiation Oncology � Biology � Physics6
osteoradionecrosis. Individual OAR NTCP data are shownin Table E2 (available online at www.redjournal.com). TheNTCP for structures corresponding to observed late toxic-ities, namely pharyngeal constrictor muscles, cervicalesophagus, and larynx and the mandible, were respectivelyreduced by 14.6%, 3.8%, 4.9%, and 17.6% from clinicalplans to 4p plans at the original prescription dose (TableE2). Overall, 4p planning reduced the mean NTCP at theall dose levels by approximately a factor of 3 at all doselevels (P<.0001) (Fig. 3b, Table E2).
Fig. 2. Doseevolume histogram with fractional volumeplotted against dose, with a clinical plan compared with (a)4pPD plan, and (b) 4pPDþ 10 Gy plan and 4pPDþ 20 Gyplan. PCM Z pharyngeal constrictor muscles; PD Zprescription dose; PTV Z planning target volume.
Discussion
The prognosis of recurrent head-and-neck cancer aftersalvage reirradiation is poor, and management of these pa-tients remains challenging. The Radiation TherapyOncologyGroup (RTOG) 96-10 and RTOG 99-11 prospective trialsand others reported 2-year LC of 11%-37% and median OSat 8.2-12.5 months (26-32) in patients reirradiated using3-dimensional techniques with concurrent chemotherapy.Grade �3 late toxicities ranged from 8% to 33% (26-32).With the advent of IMRT, reirradiation with chemotherapysaw further improvements in LC, with 2-year rates of19%-67%, which translated into a median OS benefit of 15-27.6 months (33-35). Yet the observed severe late complica-tions rate of 12%-32% remained largely unchanged (33-35),and notably treatment-related deaths occurred in approxi-mately 10% of patients with either IMRT or 3-dimensionalconformal radiation therapy (26, 35). Emerging SBRT datasuggested an opportunity to preserve LCgains registeredwithIMRT, while potentially reducing severe late toxicities (36).The 2-year LC of 39.2%, a median OS of 12 months, and a7.4% rate of grade 3 late complications were consistent withresults from other SBRT series (4-7, 10-12).
Whereas a randomized, phase 3 trial is ultimately war-ranted to compare results of SBRT and conventionallyfractionated radiation therapy, efforts are clearly needed tocarefully augment LC in the salvage of recurrent head-and-neck cancer to improve patient survival. Herein, we purposedto ameliorate SBRT outcomes with 4p planning, with thegoal to reduce late toxicities while attempting to improvelocal tumor control. We demonstrated that better dosimetry isachievable with reduction in doses to OARs obtained (Fig. 2,Table 2) and dose spillage outside the PTV, while improvingPTV coverage (Fig. 1b, Table 3). Improvements wereobserved in all previously treated patients regardless of plan-ning technique and treatment machine selection. We alsofound that even with a 10-Gy total PTV dose escalation, thereduction in dose spillage was maintained with a corre-sponding reduction inOARdoses.Although dose spillagewasincreased for 4pPDþ 20Gy, doses toOARswere still reducedor unchanged, except for the carotid artery when patients withtumors wrapping the carotid artery were included.

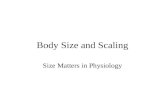
Fig. 3. (a) Mean tumor control probability (TCP) and (b) mean normal tissue control probability (NTCP) for the entirepatient cohort for both clinical (dashed) and 4p plans; (c) 4p planning may enhance the therapeutic index by increasing theseparation between TCP and NTCP curves. PD Z prescription dose.
Volume - � Number - � 2014 4p SBRT for head-and-neck cancer 7
Carotid artery blowout syndrome (CBS) is a serious andoften fatal complication in reirradiation. Published datareveal that CBS rates can be high in reirradiation withSBRT, especially in patients with tumors wrapping thecarotid artery, nearby skin involvement, or necrosis at timeof recurrence (37, 38). Cengiz et al (12) reported a 17.8%rate CBS in patients with tumors wrapping around thecarotid artery among 46 patients reirradiated with Cyber-Knife. They found that CBS occurred when the tumorencompassed �180� of the carotid artery while receiving100% of the prescription dose under a QD regimen, butwhen they adopted QOD, CBS rates were significantlyreduced (12, 39). Our results suggest that 4p SBRT canadd to the benefit of a QOD regimen and render patientswho were otherwise relatively contraindicated suitable forreirradiation with SBRT.
The optimized noncoplanar SBRT (4p) allowed forimprovement in TCP at all dose levels, while simulta-neously keeping NTCP lower when compared with clinicalplans. Thus, our results suggest that 4p may enhance thetherapeutic ratio, because TCP and NTCP curves areseparated further relative to clinical planning (Fig. 3c).Patients with radioresistant, previously irradiated tumors orprimary radioresistant tumors, such as sinonasal mucosalmelanoma (8) as in this study, might benefit from the higherprescription dose. Conversely, 2 patients had a decrement inTCP when the dose was further increased from 10 Gy to20 Gy with 4p planning (Table E1). This finding may be
explained by the fact that during 4p optimization, PTVcoverage may be compromised to preserve high-priorityOAR constraints. Thus, dose escalation should be consid-ered within the context of an individual patient’s anatomicand clinical factors.
To implement 4p delivery in the clinic using C-arm linearaccelerators, practical considerations such as avoidance ofcouch and gantry collision, as well as achieving optimaltreatment delivery time, must be evaluated. We created abeam geometry solution space based on the computer-aideddesign (CAD) model of the machine and patients. Collisionswere predicted and prevented using this model. To eliminatethe risk of collision and maintain targeting accuracy, thepatients would need to be well immobilized. Increasingthe collision buffer might further improve the safety, butit would lead to an increased number of beams usingextended source-to-tumor distances, slightly degrading themultileaf collimator resolution and dosimetry. Positioningthe couch and gantry manually for such a large number ofnoncoplanar, nonisocentric beams would be impractical andlikely unsafe. However, this task would be feasible withrobotized couch and gantry maneuvering. According to ourmeasurement of a delivered 4p plan, the total time used forcouch and gantry traversing through 30 static beams wouldbe <200 seconds.
As with all studies involving TCP and NTCP modeling,there can be significant uncertainties stemming from inac-curacies in estimated radiobiological parameter values. The

Rwigema et al. International Journal of Radiation Oncology � Biology � Physics8
LC rate predicted by the TCP model is close to theobservation (42.2% vs 39.2%), indicating that the estimatedtumor radiobiological parameters are reasonable. Similarly,the predicted mean NTCP rate of 5.6% approximated theactual 7.4% rate of severe (grade �3) late toxicities. Thevalidity of linear quadratic cell survival in the SBRT doserange has also been questioned, particularly for fractionaldose over 10 Gy, which would be the upper limit of thedose escalated plans. Nevertheless, this uncertainty is un-likely to influence the significant changes in TCP andNTCP observed in this study and overall conclusions.
Conclusions
Using C-arm linear accelerators, 4p radiation therapy mayallow head-and-neck cancer SBRT dose escalation, withsignificant and consistent improvements in tumor control,tumor coverage, and critical organ sparing. These findingsshould be evaluated in a prospective feasibility trial tovalidate whether 4p radiation therapy can enhance LCwhile reducing late toxicity.
References
1. Specenier PM, Vermorken JB. Recurrent head and neck cancer:
Current treatment and future prospects. Expert Rev Anticancer Ther
2008;8:375-391.
2. Heron DE, Ferris RL, Karamouzis M, et al. Stereotactic body radio-
therapy for recurrent squamous cell carcinoma of the head and neck:
Results of a phase I dose-escalation trial. Int J Radiat Oncol Biol Phys
2009;75:1493-1500.
3. Lartigau EF, Tresch E, Thariat J, et al. Multi institutional phase II
study of concomitant stereotactic reirradiation and cetuximab for
recurrent head and neck cancer. Radiother Oncol 2013;109:281-285.
4. Roh KW, Jang JS, Kim MS, et al. Fractionated stereotactic radio-
therapy as reirradiation for locally recurrent head and neck cancer. Int
J Radiat Oncol Biol Phys 2009;74:1348-1355.
5. Unger KR, Lominska CE, Deeken JF, et al. Fractionated stereotactic
radiosurgery forreirradiation of head-and-neck cancer. Int J Radiat
Oncol Biol Phys 2010;77:1411-1419.
6. Rwigema JC, Heron DE, Ferris RL, et al. The impact of tumor volume
and radiotherapy dose on outcome in previously irradiated recurrent
squamous cell carcinoma of the head and neck treated with stereo-
tactic body radiation therapy. Am J Clin Oncol 2011;34:372-379.
7. Siddiqui F, Patel M, Khan M, et al. Stereotactic body radiation therapy
for primary, recurrent, and metastatic tumors in the head-and-neck
region. Int J Radiat Oncol Biol Phys 2009;74:1047-1053.
8. Ozyigit G, Cenzig M, Yazici G, et al. Robotic stereotactic body
radiotherapy in the treatment of sinonasal mucosal melanoma: Report
of four cases. Head Neck 2013;35:E69-E73.
9. Kim JH, Kim MS, Yoo SY, et al. Stereotactic body radiotherapy for
refractory cervical lymph node recurrence of nonanaplastic thyroid
cancer. Otolaryngol Head Neck Surg 2010;142:338-343.
10. Rwigema JC, Heron DE, Ferris RL, et al. Fractionated stereotactic
body radiation therapy in the treatment of previously-irradiated
recurrent head and neck carcinoma: Updated report of the University
of Pittsburgh experience. Am J Clin Oncol 2010;33:286-293.
11. Kodani N, Yamazaki H, Tsubokura T, et al. Stereotactic body radiation
therapy for head and neck tumor: Disease control and morbidity
outcomes. J Radiat Res 2011;52:24-31.
12. Cengiz M, Ozyi�git G, Yazici G, et al. Salvage reirradiaton with
stereotactic body radiotherapy for locally recurrent head-and-neck
tumors. Int J Radiat Oncol Biol Phys 2011;81:104-109.
13. Heron DE, Rwigema JC, Gibson MK, et al. Concurrent cetuximab
with stereotactic body radiotherapy for recurrent squamous cell car-
cinoma of the head and neck: A single institution matched case-con-
trol study. Am J Clin Oncol 2011;34:165-172.
14. Wang K, Heron DE, Flickinger JC, et al. A retrospective, deformable
registration analysis of the impact of PET-CT planning on patterns of
failure in stereotactic body radiation therapy for recurrent head and
neck cancer. Head Neck Oncol 2012;4:12.
15. Wang K, Heron DE, Clump DA, et al. Target delineation in stereo-
tactic body radiation therapy for recurrent head and neck cancer: A
retrospective analysis of the impact of margins and automated PET-CT
segmentation. Radiother Oncol 2013;106:90-95.
16. Vargo JA, Heron DE, Ferris RL, et al. Prospective evaluation of pa-
tient-reported quality-of-life outcomes following SBRT cetuximab
for locally-recurrent, previously-irradiated head and neck cancer.
Radiother Oncol 2012;104:91-95.
17. Vargo JA, Heron DE, Ferris RL, et al. Examining tumor control and
toxicity following stereotactic body radiotherapy in locally-recurrent,
previously-irradiated head-and-neck cancers: Implications of treat-
ment duration and tumor volume. Head Neck 2014;36:1349-1355.
18. Dong P, Lee P, Ruan D, et al. 4p non-coplanar liver SBRT: A
novel delivery technique. Int J Radiat Oncol Biol Phys 2013;85:1360-
1366.
19. Dong P, Lee P, Ruan D, et al. 4p noncoplanar stereotactic body ra-
diation therapy for centrally located or larger lung tumors. Int J Radiat
Oncol Biol Phys 2013;86:407-413.
20. Dong P, Nguyen D, Ruan D, et al. Feasibility of prostate robotic ra-
diation therapy on conventional C-arm linacs. Pract Radiat Oncol
2014;4:254-260.
21. Romeijn H, Ahuja R, Dempsey J, et al. A column generation approach
to radiation therapy treatment planning using aperture modulation.
SIAM J Optim 2005;15:838-862.
22. Trotti A, Colevas AD, Setser A, et al. CTCAE v3.0: Development of a
comprehensive grading system for the adverse effects of cancer
treatment. Semin Radiat Oncol 2003;13:176-181.
23. Webb S. Optimum parameters in a model for tumour-control proba-
bility including interpatient heterogeneity. Phys Med Biol 1994;39:
1895-1914.
24. Girinsky T, Lubin R, Pignon JP, et al. Predictive value of in vitro
radiosensitivity parameters in head and neck cancers and cervical
carcinomas: Preliminary correlations with local control and overall
survival. Int J Radiat Oncol Biol Phys 1993;25:3-7.
25. Burman C, Kutcher GJ, Emami B, et al. Fitting of normal tissue
tolerance data to an analytic function. Int J Radiat Oncol Biol Phys
1991;21:123-135.
26. Spencer SA, Harris J, Wheeler RH, et al. RTOG 96-10: Reirradiation
with concurrent hydroxyurea and 5-fluorouracil in patients with
squamous cell cancer of the head and neck. Int J Radiat Oncol Biol
Phys 2001;51:1299-1304.
27. Langer CJ, Harris J, Horwitz EM, et al. Phase II study of low dose
paclitaxel and cisplatin in combination with split-course concomitant
twice-daily reirradiation in recurrent squamous cell carcinoma of the
head and neck: Results of Radiation Therapy Oncology Group Pro-
tocol 99-11. J Clin Oncol 2007;25:4800-4805.
28. Dawson LA, Myers LL, Bradford CR, et al. Conformal re-irradiation
of recurrent and new primary head-and-neck cancer. Int J Radiat
Oncol Biol Phys 2001;50:377-385.
29. De Crevoisier R, Bourhis J, Domenge C, et al. Full-dose reirradiation
for unresectable head and neck carcinoma: Experience at the Gustave-
Roussy Institute in a series of 169 patients. J Clin Oncol 1998;16:
3556-3562.
30. Salama JK, Vokes EE, Chmura SJ, et al. Long-term outcome of
concurrent chemotherapy and reirradiation for recurrent and second
primary head-and-neck squamous cell carcinoma. Int J Radiat Oncol
Biol Phys 2006;64:382-391.

Volume - � Number - � 2014 4p SBRT for head-and-neck cancer 9
31. Kramer NM, Horwitz EM, Cheng J, et al. Toxicity and outcome
analysis of patients with recurrent head and neck cancer treated with
hyperfractionated split-course reirradiation and concurrent cisplatin
and paclitaxel chemotherapy from two prospective phase I and II
studies. Head Neck 2005;27:406-414.
32. Spencer S, Wheeler R, Peters G, et al. Phase 1 trial of combined
chemotherapy and reirradiation for recurrent unresectable head and
neck cancer. Head Neck 2003;25:118-122.
33. Lee N, Chan K, Bekelman JE, et al. Salvage re-irradiation for recurrent
head and neck cancer. Int J Radiat Oncol Biol Phys 2007;68:731-740.
34. Sulman EP, Schwartz DL, Le TT, et al. IMRT reirradiation of head and
neck cancerddisease control and morbidity outcomes. Int J Radiat
Oncol Biol Phys 2009;73:399-409.
35. Sher DJ, Haddad RI, Norris CM Jr, et al. Efficacy and toxicity
of reirradiation using intensity-modulated radiotherapy for recurrent
or second primary head and neck cancer. Cancer 2010;116:4761-
4768.
36. Rwigema JC, Vargo JA, Clump DA, Ferris RL, Ohr J, Heron DE.
Stereotactic body radiotherapy in the management of head and neck
malignancies. Curr Cancer Ther Rev, in press.
37. Yamazaki H, Ogita M, Kodani N, et al. Frequency, outcome and
prognostic factors of carotid blowout syndrome after hypofractionated
re-irradiation of head and neck cancer using CyberKnife: A multi-
institutional study. Radiother Oncol 2013;107:305-309.
38. McDonald MW, Moore MG, Johnstone PA. Risk of carotid blowout
after reirradiation of the head and neck: A systemic review. Int J
Radiat Oncol Biol Phys 2012;82:1083-1089.
39. Yazici G, Sanl TY, Cengiz M, et al. A simple strategy to decrease fatal
carotid blowout syndrome after stereotactic body reirradiaton for
recurrent head and neck cancers. Radiat Oncol 2013;8:242.