4 ΟΓΚΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ ΡΟΔΟΥ
94
Μεταστατικός Καρκίνος Νεφρού θεραπευτική αντιμετώπιση Nikolaos Tsoukalas MD, MSc, PhD Medical Oncologist, MSc in Bioinformatics Clinical Research Fellow in Oncology Guy’s & St Thomas’ NHS Cancer Centre Queen Elizabeth Hospital London UK
-
Upload
isrodoy-isr -
Category
Health & Medicine
-
view
81 -
download
0
Transcript of 4 ΟΓΚΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ ΡΟΔΟΥ

Μεταστατικός Καρκίνος Νεφρούθεραπευτική αντιμετώπιση
Nikolaos Tsoukalas MD, MSc, PhD
Medical Oncologist, MSc in BioinformaticsClinical Research Fellow in Oncology
Guy’s & St Thomas’ NHS Cancer CentreQueen Elizabeth Hospital
London UK

Disclosure
• No actual or potential conflict of interest in relation to this presentation.
• No real or apparent conflicts of interest to disclose.

Renal cell carcinoma• Renal cell carcinoma (RCC) accounts for 2%–3% of all
adult malignancies, representing the seventh most common cancer in men and the ninth most common cancer in women.
• Worldwide, there are ∼209 000 new cases and 102 000 deaths per year. The incidence of all stages of RCC has increased over the past several years, contributing to a steadily increasing mortality rate per unit population.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

Current targets of therapies for RCC: VEGF and mTOR
Inhibition of some other target pathways are under investigation
Transcriptional activation
VEGF
HIF-1α
VHL
Protein synthesis
Angiogenesis
Bevacizumab
Growth and metabolism
mTOR
Growth factor receptor
PI3K
PIP2PIP3
PTEN
AKT
Temsirolimus, everolimus
Sunitinib, sorafenib, axitinib,
pazopanib
Tumour cell
Endothelial cell
VEGFR
EGF, epidermal growth factor; VHL, von Hippel–Lindau

ESMO Academy 2015

Patient outcomes
Therapeutic options
Median PFS4–5 months
Median PFS9–11 months
Median PFS4–5 months
? ?
~40–60%1,2~100% <20%3–5Eligible patients
SunitinibPazopanib
Bevacizumab + IFN-α
Temsirolimus
Axitinib(post-sunitinib/
cytokine)Everolimus
(post-VEGFR-TKI)Sunitinib
(post-cytokine)Pazopanib
(post-cytokine)Sorafenib
(post-cytokine)
Everolimus(post-VEGFR-TKI
× 2)
Neoadjuvant Adjuvant First-line Second-line Third-line
Progress in advanced kidney cancer, 2007–2014
Adapted from Larkin. ASCO GU 2014IFN-α, interferon-alpha; VEGFR-TKI, vascular endothelial growth factor receptor-tyrosine kinase inhibitor
1. Levy et al. Eur J Cancer 2013; 2. Sonpavde et al. Eur Urol 2012; 3. Iacovelli et al. Eur J Cancer 2013; 4. Pal et al. ASCO GU 2013; 5. Heng et al. ASCO 2013












ESMO Academy 2015


ESMO Academy 2015

ESMO Academy 2015

ESMO Academy 2015





Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
• In the era of immunotherapy, cytoreductive nephrectomy was recommended in patients with good PS [I, A].
• Whether this recommendation will remain with current targeted therapies is currently being investigated in two prospective trials.
• In routine practice, cytoreductive nephrectomy is recommended in patients with good PS and large primary tumours with limited volumes of metastatic disease, and for patients with a symptomatic primary lesion. Cytoreductive nephrectomy is not recommended in patients with poor PS.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
• Metastasectomy can be considered and performed after multidisciplinary review for selected patients with solitary or easily accessible pulmonary metastases, solitary resectable intraabdominal metastases, a long disease-free interval after nephrectomy, or a partial response in metastases to immunotherapy or targeted therapy.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

ESMO Academy 2015

Targeted agents currently approved for mRCC in Europe
Sorafenib (oral)Advanced RCC after IFN‑α/IL-2 or if unsuitable for IFN-α/IL-22
Bevacizumab (+IFN-α) (IV)
First-line mRCC3
Everolimus (oral)Advanced RCC after
VEGF‑targeted therapy5
Axitinib (oral)Advanced RCC after sunitinib
or a cytokine7
Temsirolimus (IV)Advanced RCC with 3–6 prognostic risk factors4
2006 2007 2008 2009 2010 2011 2012 2013 2014
Pazopanib (oral)Advanced RCC6
Sunitinib (oral)Advanced/mRCC1
1. Sunitinib SmPC, Jan 2014; 2. Sorafenib SmPC, Feb 2013; 3. Bevacizumab SmPC, Feb 2014; 4. Temsirolimus SmPC, Oct 2013; 5. Everolimus SmPC, Nov 2013; 6. Pazopanib SmPC, Dec 2013; 7. Axitinib SmPC, Oct 2013.
IFN-α, interferon-alpha; IL-2, interleukin-2; IV, intravenous










ESMO Academy 2015

ESMO Academy 2015

ESMO Academy 2015

ESMO Academy 2015

ESMO Academy 2015

ESMO Academy 2015

ESMO Academy 2015




Pivotal trials in the 2nd line setting
TRIAL TREATMENTSTARGET Sorafenib vs PlaceboAXIS Axitinib vs SorafenibRECORD-1 Everolimus vs PlaceboINTORSECT Temsirolimus vs SorafenibMETEOR Cabozantinib vs EverolimusCheckMate-025 Nivolumab vs Everolimus

Axitinib: a next-generation TKI
• Binds to VEGFR-1, -2 and -3• Fits tightly into the ‘deep pocket’
conformation of the kinase domain of VEGFRs, resulting in high potency and selectivity in vitro
Hu-Lowe DD, et al. Clin Cancer Res 2008;14:7272–83; Escudier B and Gore M. Drugs R D 2011;11:113–26; INLYTA®. Summary of Product Characteristics. 2012. Available at: www.medicines.org.uk/emc/.

Sorafenib 400 mg BD
Eligibility criteria included: mRCC with clear-cell
histology Failure of one prior first-
line regimen containing:– Sunitinib – Bevacizumab + IFN-α– Temsirolimus– Or cytokines
Stratification by prior regimen and ECOG PS
Phase III study of axitinib versus sorafenib insecond-line treatment of mRCC (AXIS)
Primary endpoints: PFS by independent central reviewSecondary endpoints: OS, ORR, safety and tolerability, duration of response, patient-reported outcomes
Axitinib5 mg BD*
N=723
Treat until PD, unmanageable AE, or withdrawal of consent
Rini BI, et al. Lancet 2011;378:1931–9.Sorafenib Summary of Product Characteristics. 2012. Available at: www.medicines.org.uk/emc/.
*Dose increase (to maximum of 10 mg BD) or reduction (to minimum of 2 mg BD) is recommended based on individual safety and tolerability; The dose could be decreased after initiation. AE=adverse event; ECOG PS=Eastern Cooperative Oncology Group performance status; ORR=objective response rate; OS=overall survival; PFS=progression-free survival; PD=progressive disease.
1:1
RANDOMISATION

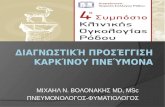
AXIS Trial: PFS results
Rini BI, et al. Lancet. 2011;378:1931-1939.
1.00.90.80.70.60.50.40.30.20.1
00 2 4 6 8 10 12 14 16 18 20
Prob
abili
ty o
f PFS
AxitinibSorafenib
Median PFS, Mos (95% CI)6.7 (6.3-8.6)4.7 (4.6-5.6)
Stratified HR: 0.665(95% CI: 0.544-0.812; P < .0001)
Pts at Risk, nAxitinib
Sorafenib256224
361362
202157
145100
9651
6428
3812
206
103
11
00
Months

Lenvima

Lenvatinib ± Everolimus in mRCC: Randomized, Open-Label Phase II Study
• Primary endpoint: PFS with lenvatinib ± everolimus vs everolimus alone• Secondary endpoints: PFS with combination vs lenvatinib alone, ORR, OS,
safety/tolerability
Lenvatinib 18 mg QD +Everolimus 5 mg QD
(n = 51)
Measurable metastatic or advanced RCC;
following progression≤ 9 mos after 1 prior
VEGF therapy (N = 153)
Stratified by hemoglobin (low vs normal) and corrected serum calcium
(≥ vs < 10 mg/dL)
Lenvatinib 24 mg QD(n = 52)
Motzer R, et al. ASCO 2015. Abstract 4506. Reprinted with permission.
Everolimus 10 mg QD (n = 50)
Treated until PD or unacceptable toxicity

Lenvatinib ± Everolimus in mRCC: Efficacy
Response Lenvatinib/Everolimus
(n = 51)
Lenvatinib(n = 52)
Everolimus(n = 50)
Median PFS, mos
14.6HR: 0.40; P < .001
vs everolimus
7.4HR: 0.61; P = .048
vs everolimus
5.5
ORR, % 43P < .001 vs everolimus
27P = .007 vs everolimus
6
Median OS,* mos 25.5HR: 0.51; P = .024
vs everolimus
19.1HR: 0.68; P =.118
vs everolimus
15.4
Motzer R, et al. ASCO 2015. Abstract 4506. Reprinted with permission.
*Updated analysis.

Cabozantinib
Cometriq

METEOR phase III study

Basic characteristics
Choueiri et al. NEJM 2015

Choueiri et al. NEJM 2015

Overall survival
Choueiri et al. NEJM 2015
Response rateCabozantinib Everolimus
21% 5%
40/187 9/188
P<0.001

Adverse Effects
Choueiri et al. NEJM 2015

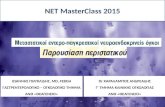
Opdivo

Phase 3 trial of Nivolumab vs Everolimus following VEGF-targeted therapy
Motzer et al. NEJM 2015
Nivolumab produced higher response rates than everolimus (25% vs. 5%) and median overall survival was longer (by 5.4 months), to more than 2 years.

Motzer RJ et al. N Engl J Med 2015;373:1803-1813
Baseline Characteristics (1)

Baseline Characteristics (2)
Motzer RJ et al. N Engl J Med 2015;373:1803-1813

Overall Survival
Motzer RJ et al. N Engl J Med 2015;373:1803-1813
Nivolumab Everolimus
24% 5%
103/410 22/411
P<0.001
Response rate

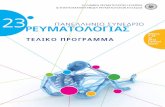
Overall Survival in Subgroup Analyses
Motzer RJ et al. N Engl J Med 2015;373:1803-1813

Progression-free Survival
Motzer RJ et al. N Engl J Med 2015;373:1803-1813

Overall Survival according to PD-L1 Expression Level
Motzer RJ et al. N Engl J Med 2015;373:1803-1813

AEs (≥10%) of treated patients in either group (1)
Motzer RJ et al. N Engl J Med 2015;373:1803-1813

Motzer RJ et al. N Engl J Med 2015;373:1803-1813
AEs (≥10%) of treated patients in either group (2)

2nd line trials (non-immunotherapy)Author Agent Phase RR PFS
Pili et al. Abstr 4549 Aflibercept II 2-3% 8-11mo
McKay et al. Abstr 4559 Buparlisib (PI3K) + Bev I 13% 9mo
Keefe et al, Abstr 4543 CRLX101 (HIF) +Bev Ib/IIa 23% 10mo
Voss et al, Abstr 4567 Dalantercept (ALK) + axitinib
II 25% 8mo
Hainsworth et al, Abstr 4547 LY2510924 (CXCR4) + sunitinib
II rand 39% 12mo
Peterson et al, Abstr TPS4580
RX-0201 (AKT1) + Everolimus
I (ongoing)
Twarowski et al, Abstr 4523 Tivantinib (MET) +/- Erlotinib
II rand 0% 2-5mo
Dorff et al, Abstr 4542
Bevacizumab +/-TRC105 (Endoglin)
II rand 3%
ASCO 2015

2nd (+/- 1st) line trials (immunotherapy)
Author Agent Phase
RR PFS
Amin et al. ASCO 2014 Nivolumab+Pazopanib I 45% 55% (6m)
Amin et al. ASCO 2014 Nivolumab+Sunitinib I 52% 78% (6m)
NCT02423954 Nivolumab+Temsirolimus I
NCT01668784 Nivolumab vs Everolimus III
Rini et al, Cancer 2011 Tremelimumab+Sunitinib I 43% Toxic
Plimack et al, ASCO 2015 CheckMate-010
Nivolumab II OS=25m
Choueiri et al. ASCO 2015 CheckMate-009
Nivolumab II Association with biomarkers
Hammers et al. ASCO 2015 CheckMate-016
Nivolumab+Ipilimumab III ~40% ≥13m

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
• Radiotherapy has a limited role in the primary management of renal cancer. However, it is used in many different clinical situations particularly for unresectable local recurrences and metastatic disease.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
• Bisphosphonate therapy with zoledronic acid has been shown to reduce skeletal-related events in patients with bone metastasis due to mRCC and they should be considered for zoledronic acid treatment, weighting the potential benefits of the treatment (supposed benefit in terms of OS) with the potential harms (risk of osteonecrosis of the jaw) [II, A].
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014
1 Lipton A et al Zoledronic acid delays the onset of skeletal-relatedevents and progression of skeletal disease in patients with advanced renal cellcarcinoma. Cancer 2003.2 Aapro M et al. Guidance on the use ofbisphosphonates in solid tumours: recommendations of an international expertpanel. Ann Oncol 2008.

RCC systemic treatments
1st lineSunitinib
PazopanibIFN-α + Bev
TemsirolimusHD IL-2
mPFS= 9 mo
2nd lineEverolimus
AxitinibSorafenibSunitinib
mPFS= 4-5 mo
3rd lineEverolimusSorafenib
mPFS= 4-5 mo

RCC systemic treatments
1st lineSunitinib
PazopanibIFN-α + Bev
TemsirolimusHD IL-2
mPFS= 9 mo
2nd lineEverolimus
AxitinibSorafenibSunitinib
CabozantinibNivolumab
Lenvatinib+Eve?
mPFS= 4-5 mo
3rd lineEverolimusSorafenib
mPFS= 4-5 mo

2nd line treatment after…1st line 2nd line
Cytokine
SorafenibSunitinibPazopanibAxitinibTivozanibBavacizumab
Anti-angiogenic agent
EverolimusTemsirolimusAxitinibSunitinibSorafenibCabozantinibNivolumabLenvatinib+Everolimus
mTOR inhibitor Sunitinib

Treatment decisions in the clinic
Efficacy is the key factor used to select treatments Safety profiles of individual drugs may also impact on treatment decisions
HypertensionDysphonia
Hand–foot syndromeWeight lossConstipation
Axitinib2Everolimus1
StomatitisInfections
CoughRash
Peripheral oedemaDyspnoea
Pyrexia
FatigueDiarrhoea
NauseaAnorexiaVomiting
Frequent all-causality AEs (≥20%)*
1. Escudier B, et al. Cancer 2010:4256–65; 2. Rini BI, et al. Lancet 2011;378:1931–9
*Outcomes from different clinical trials should not be compared directly due to differences in trial design and patient populations


Turning mRCC into a chronic disease
Larkin and Gore. Lancet 2010.
Time
Tum
our
volu
me
Untreated tumour
cells
Treated tumour cells



Back up slides

ESMO Academy 2015

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
• Recommendations mainly relate to clear-cell histology, since most of the pivotal trials have been done in this common histological subtype.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
• Patients are stratified according to the presence of six risk factors [International Metastatic RCC Database Consortium (IMDC) criteria] 0, 1-2, 3-6:
• Karnofsky performance status (PS) <80%• Haemoglobin <lower limit of normal• Time from diagnosis to treatment of <1 year• Corrected calcium above the upper limit of normal• Platelets greater than the upper limit of normal• Neutrophils greater than the upper limit of normal
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
first-line treatment of patients with good or intermediate prognosis
• Because some RCC have a very indolent course, a period of observation before starting treatment should be considered, especially in patients with limited tumour burden and few symptoms.
• 3 treatments have demonstrated efficacy in pivotal phase 3: bevacizumab (IFN-α), sunitinib and pazopanib [I, A].
• Improvement of PFS over either IFN-α or placebo.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014
1 Escudier B et al. Bevacizumab plus interferon alfa-2afor treatment of metastatic renal cell carcinoma: a randomised, double-blind phaseIII trial. Lancet 2007.2 Motzer R et al. Sunitinib versus interferon alfa inmetastatic renal-cell carcinoma. N Engl J Med 2007.3 Sternberg CN et al. Pazopanib in locally advanced ormetastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol2010.4 Motzer RJ et al. Pazopanib versus sunitinib in metastatic renalcellcarcinoma. N Engl J Med 2013.

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
first-line treatment of patients with good or intermediate prognosis
• Sorafenib [II, B], high-dose interleukin-2 [III, C] and low-dose IFN-α combined with bevacizumab [III, A] are options.
• Single agent IFN-α, the losing arm of three randomised, controlled trials, should no longer be regarded as a standard option [I, D].
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
first-line treatment of patients with poor prognosis
• Temsirolimus is currently the only drug with level I evidence of activity in this patient population [II, A]. The pivotal trial demonstrated improvement of OS compared with IFN-α or combination of temsirolimus and IFN-α.
• Based on subgroup analysis from the pivotal trial as well as expanded access programmes, sunitinib is another reasonable option in this setting [II, B]. Sorafenib based on expanded access programmes is another possible alternative [III, B]. It is clear that, for some poor prognosis patients, best supportive care remains the only suitable treatment option.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014Hudes G et al. Temsirolimus, interferon alfa, or both foradvanced renal-cell carcinoma. N Engl J Med 2007.

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
second-line treatment• Evidence that TKIs are active after cytokines has been
demonstrated with sorafenib [I, A], pazopanib [II, A] and recently axitinib [I, A]. Sunitinib also has activity in this setting [III, A].
• However, since VEGF-targeted therapy is now the first-line standard of care, the number of patients treated with cytokines is decreasing.
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014
1 Sternberg CN et al. Pazopanib in locally advanced ormetastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol2010.2 Escudier B et al. Sorafenib in advanced clear-cell renal-cellcarcinoma. N Engl J Med 2007.3 Rini BI et al. Comparative effectiveness of axitinib versussorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial.Lancet 2011.

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
second-line treatment• After first-line treatment with VEGF-targeted therapy○ Both axitinib [I, B] and everolimus [II, A] are active. Both
drugs have shown significantly improved PFS over placebo (everolimus) or sorafenib (axitinib), but not OS.
○ Based on recent phase III trials, sorafenib can be used as an option [II, A].
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014
1 Rini BI et al. Comparative effectiveness of axitinib versussorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial.Lancet 2011.2 Motzer RJ et al. Efficacy of everolimus in advanced renalcell carcinoma: a double-blind, randomised, placebo-controlled phase III trial.Lancet 2008.3 Hutson TE et al. Randomized phase III trial of temsirolimusversus sorafenib as second-line therapy after sunitinib in patients with metastaticrenal cell carcinoma. J Clin Oncol 2014.

Metastatic Renal Cell Carcinoma: ESMO Clinical Practice Guidelines
third-line treatment • Beyond second-line treatment, enrolment into
clinical trials is recommended where possible. However, some recent trials have been reported, helping to define two different scenarios:
• In patients already treated with two TKIs (or a TKI and bevacizumab), everolimus is recommended [II, A].
• In patients previously treated with VEGF-targeted therapy and mTOR inhibitor, sorafenib [I, B] has shown activity. Another TKI or rechallenge with the same TKI is considered as an option [IV, B].
Annals of Oncology 25 (Supplement 3): iii49–iii56, 2014
Motzer RJ et al. Dovitinib versus sorafenib for third-linetargeted treatment of patients with metastatic renal cell carcinoma: an open-label,randomised phase 3 trial. Lancet Oncol 2014.