36 Πανελλήνιο Καρδιολογικό...
43
36 ο Πανελλήνιο Καρδιολογικό Συνέδριο Λήδα Πιερέττα Παπαβασιλείου M.D., Ph.D Δ .Θ.Κ.Α ΥΓΕΙΑ Ηλεκτροφυσιολογία. Διαστρωμάτωση κινδύνου για αιφνίδιο καρδιακό θάνατο σε ασθενείς που δεν συμπεριλαμβάνονται σε μεγάλες κλινικές μελέτες Σε ασθενείς με συγγενείς καρδιοπάθειες
-
Upload
truongkhanh -
Category
Documents
-
view
230 -
download
0
Transcript of 36 Πανελλήνιο Καρδιολογικό...
36ο Πανελλήνιο Καρδιολογικό Συνέδριο
Λήδα Πιερέττα Παπαβασιλείου M.D., Ph.DΔ .Θ.Κ.Α ΥΓΕΙΑ
Ηλεκτροφυσιολογία. Διαστρωμάτωση κινδύνου γιααιφνίδιο καρδιακό θάνατο σε ασθενείς που δενσυμπεριλαμβάνονται σε μεγάλες κλινικές μελέτες
Σε ασθενείς με συγγενείς καρδιοπάθειες
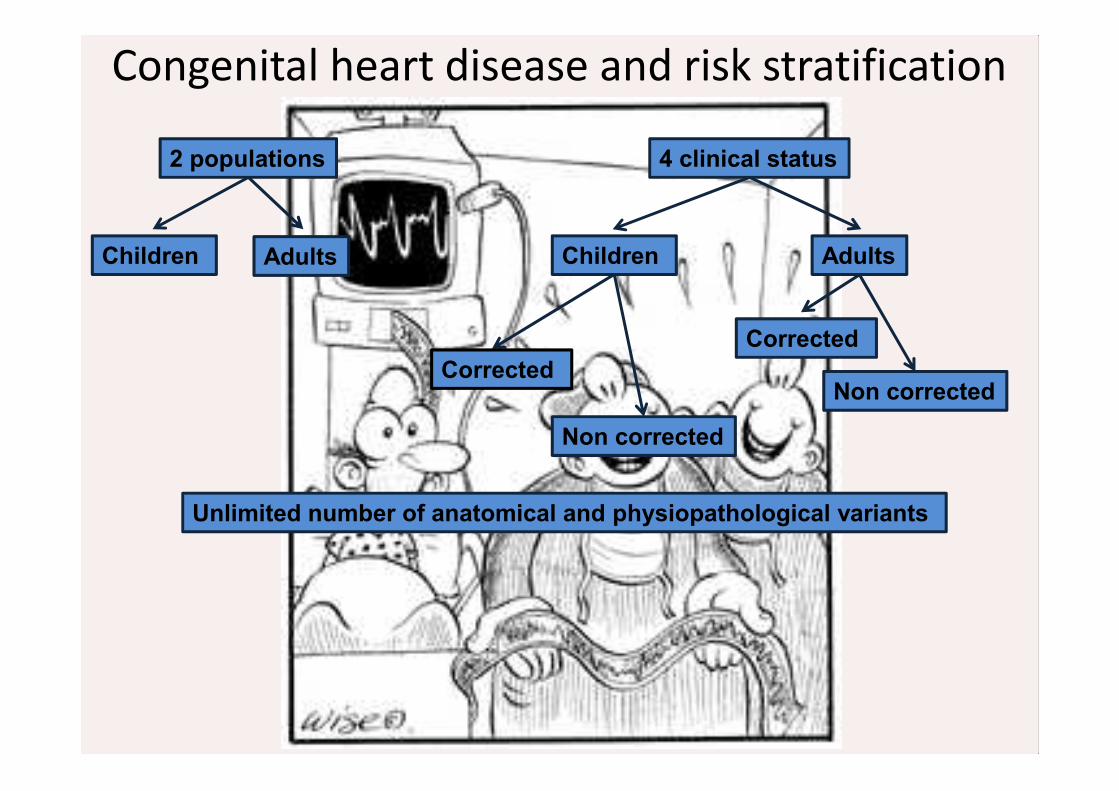
Congenital heart disease and risk stratification
2 populations
Children Adults
4 clinical status
Children Adults
Corrected
Non corrected
Corrected
Non corrected
Unlimited number of anatomical and physiopathological variants
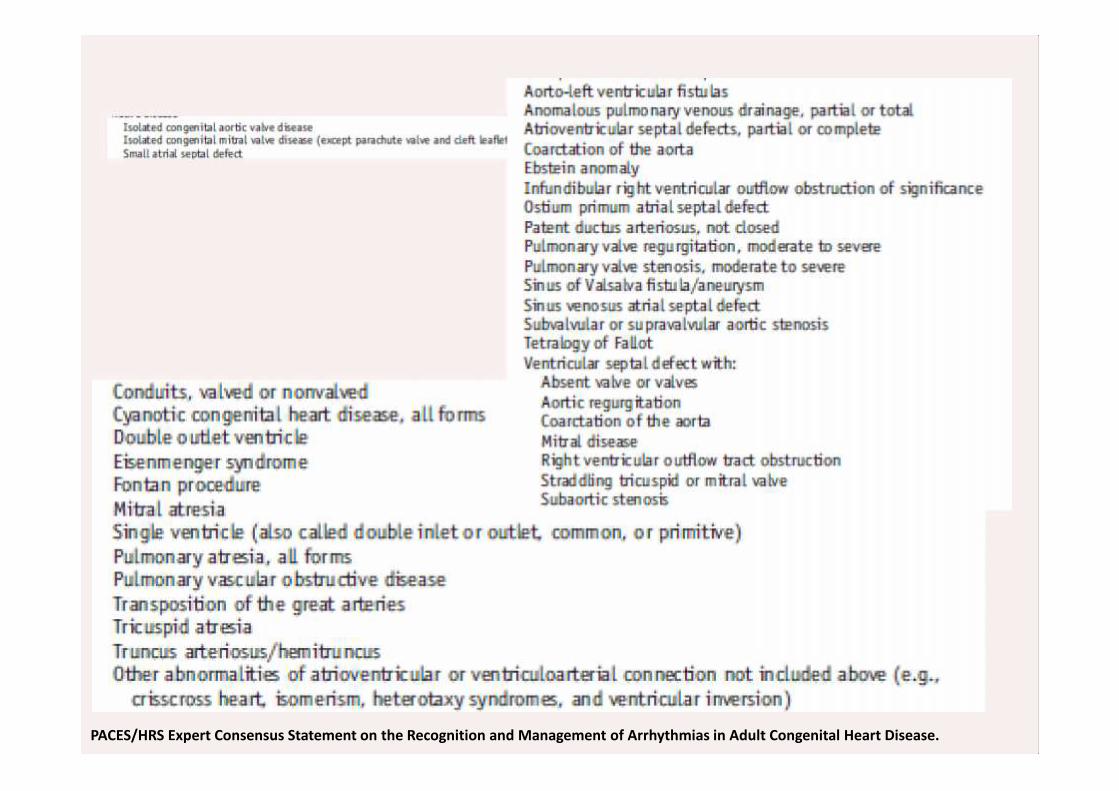
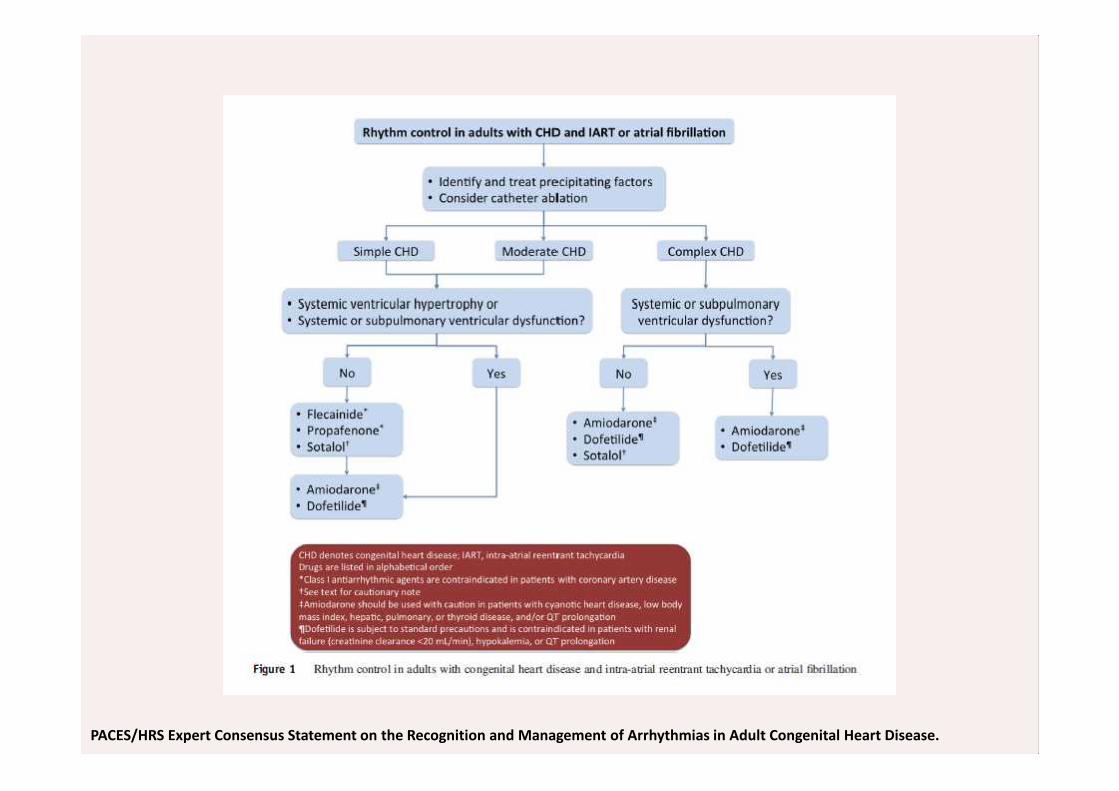
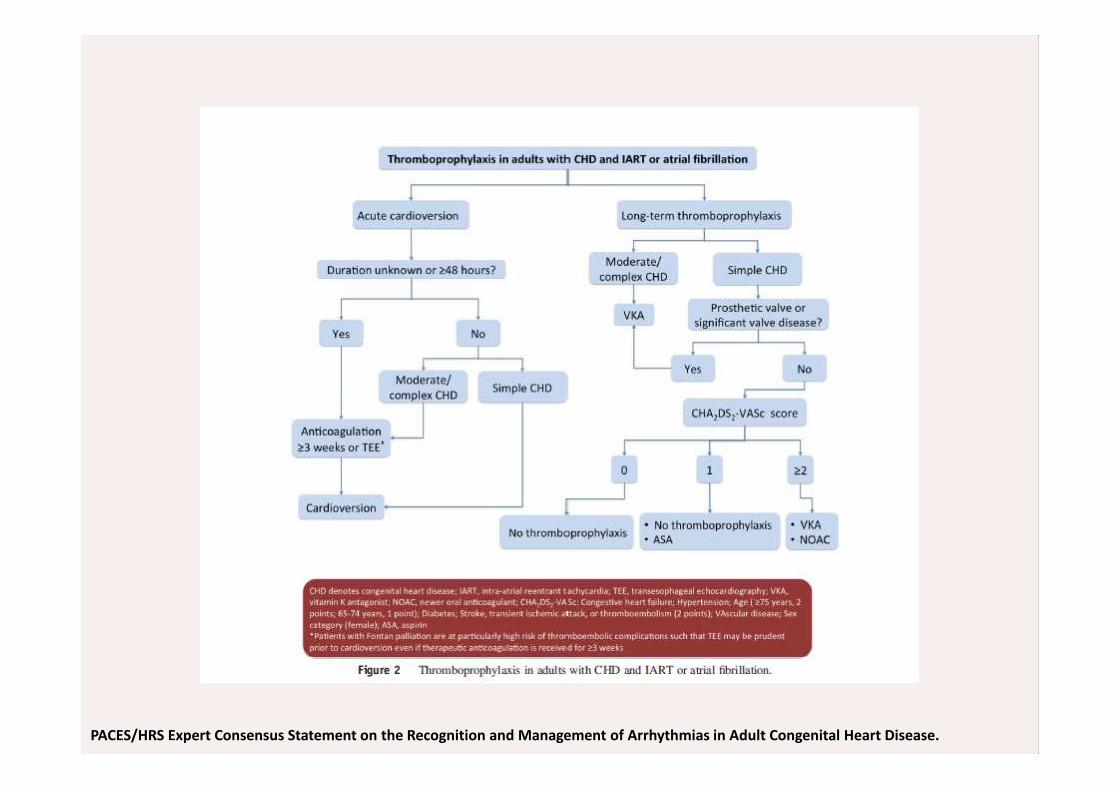
PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease.
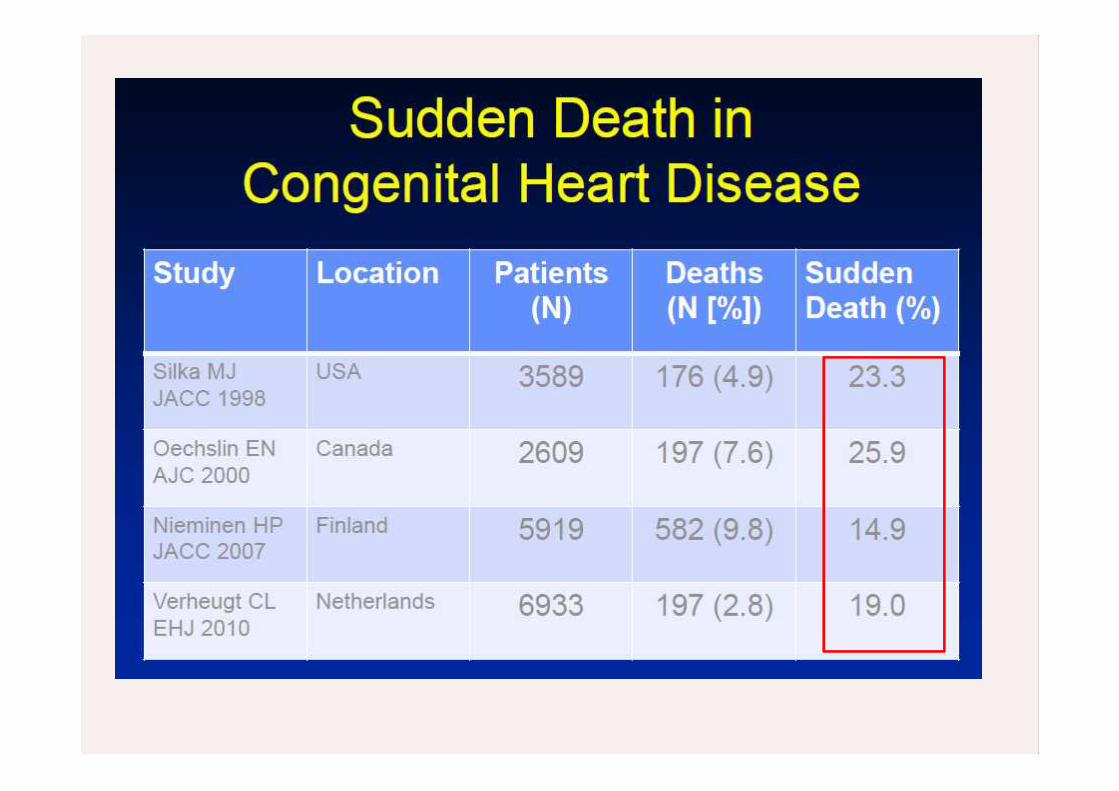
CHD incidence and SCD
• CHD:8/1000 live births• 800.000 adults with CHD in US in 2001 (45% mild, 40%
moderate, 15% severe), over 1.000.000 in 2014• SCD 15-26%• Heart failure 13-27%• Annual incidence 0.1%/y much higher than age
matched controls (100-fold higher than age-matchedcontrols)
• Most infants with CHD will survive adulthood rate willincrease
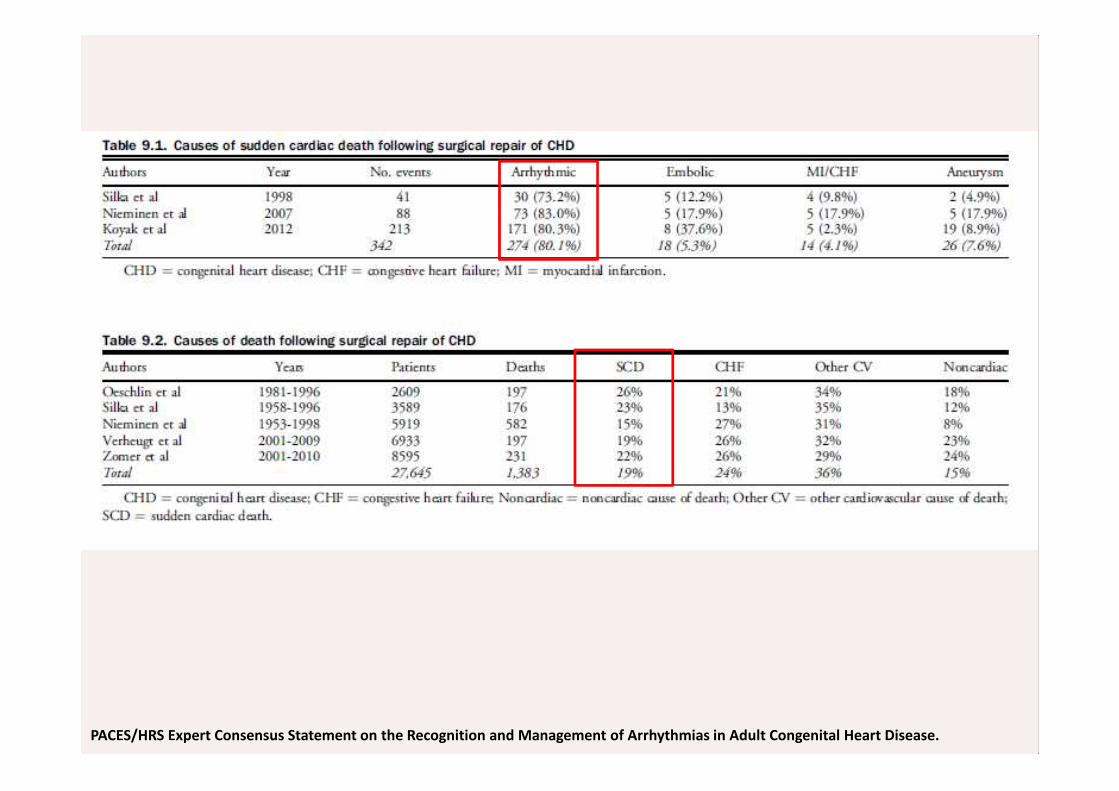
PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease.
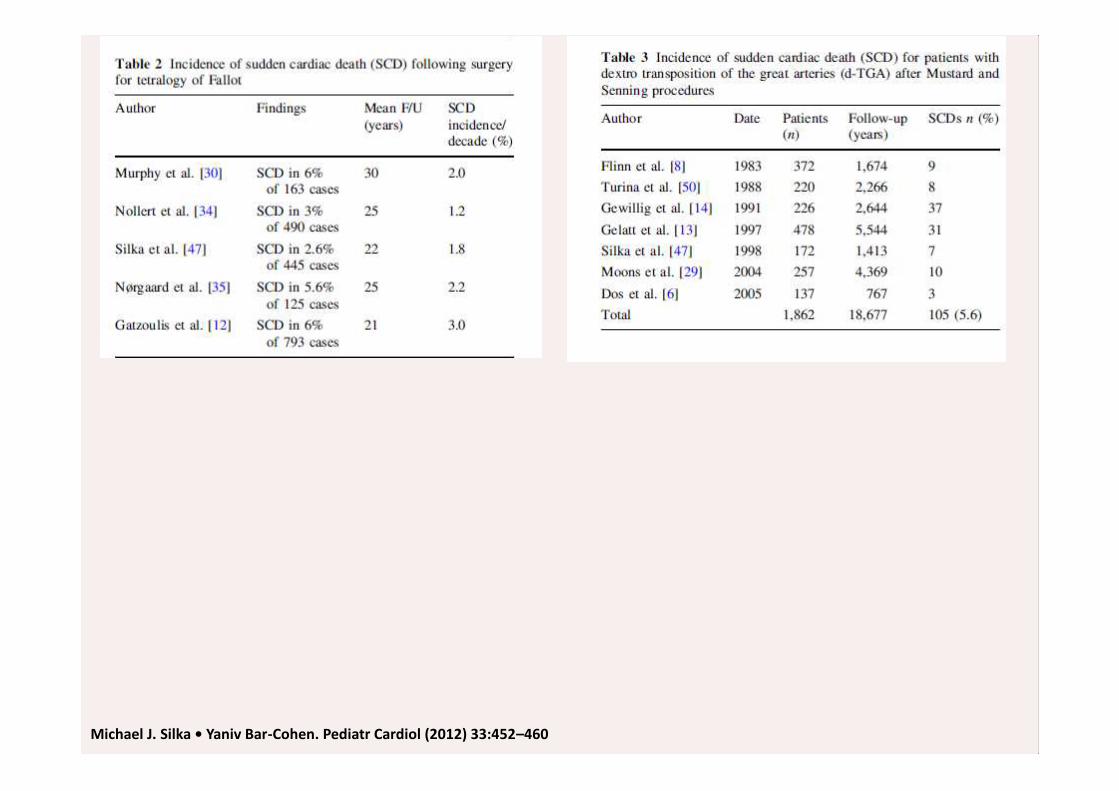
Michael J. Silka • Yaniv Bar-Cohen. Pediatr Cardiol (2012) 33:452–460
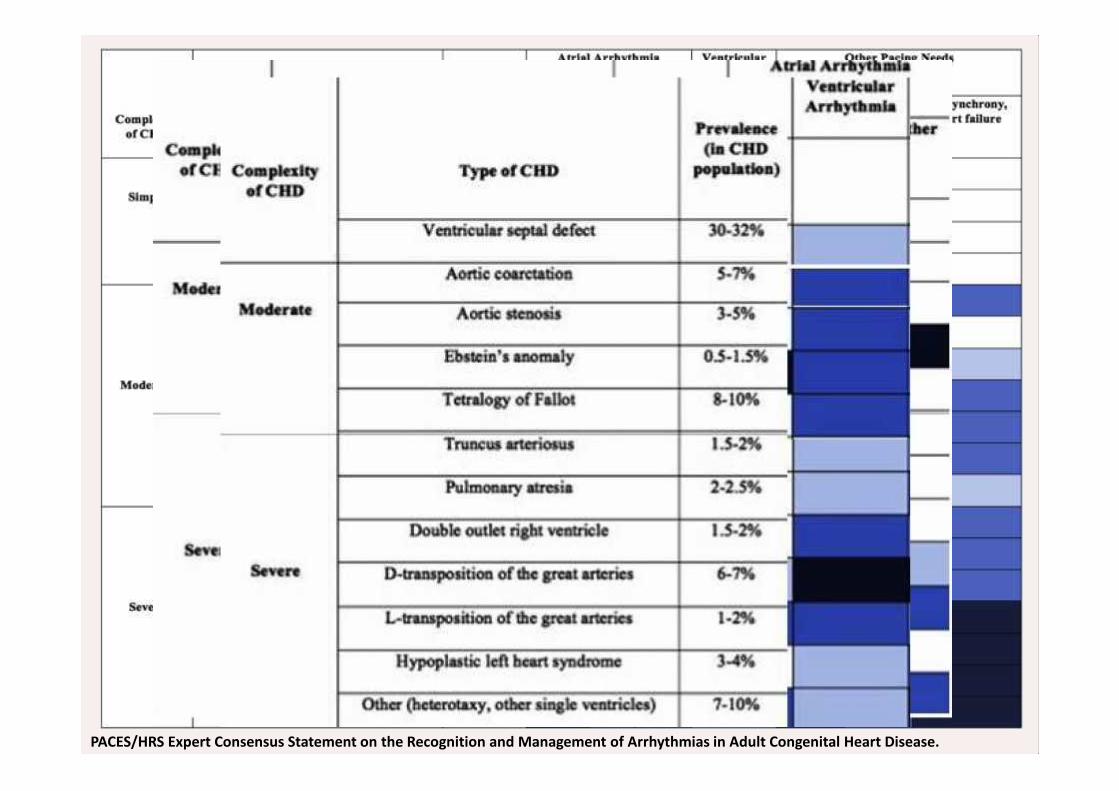
Figure 3.2
PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease.
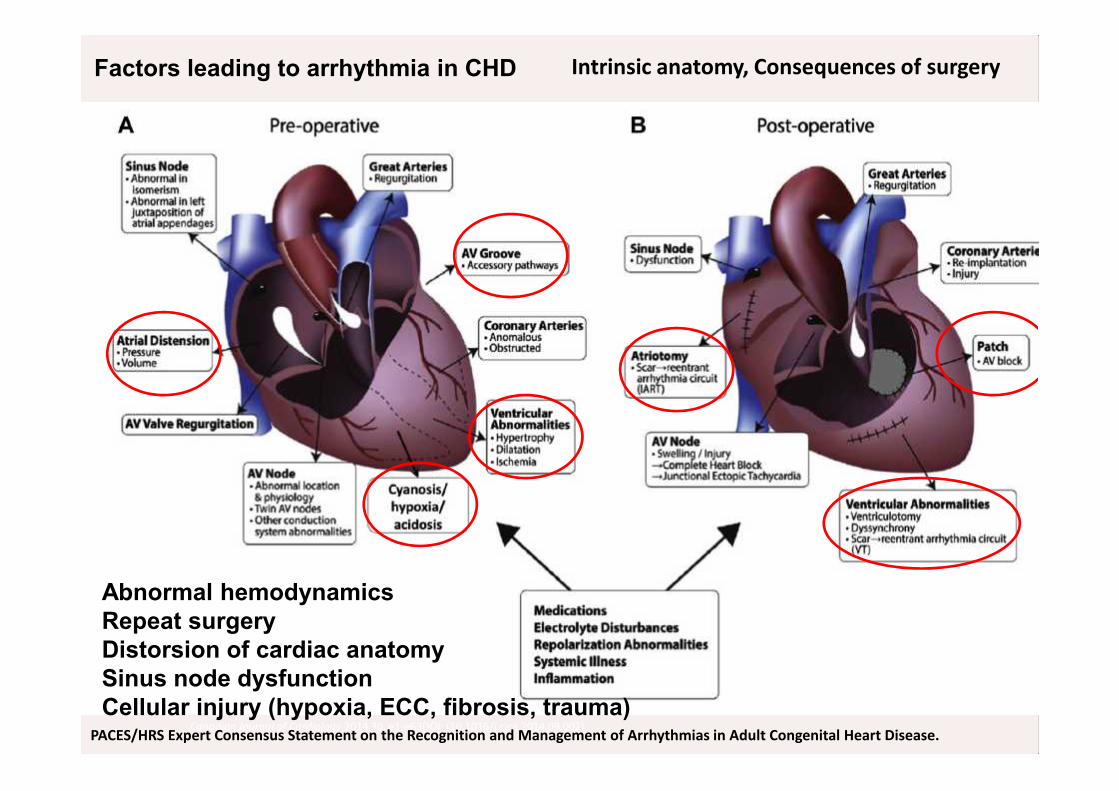
Intrinsic anatomy, Consequences of surgery
Canadian Journal of Cardiology 2014 30, e1-e63DOI: (10.1016/j.cjca.2014.09.002)PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease.
Factors leading to arrhythmia in CHD
Abnormal hemodynamicsRepeat surgeryDistorsion of cardiac anatomySinus node dysfunctionCellular injury (hypoxia, ECC, fibrosis, trauma)
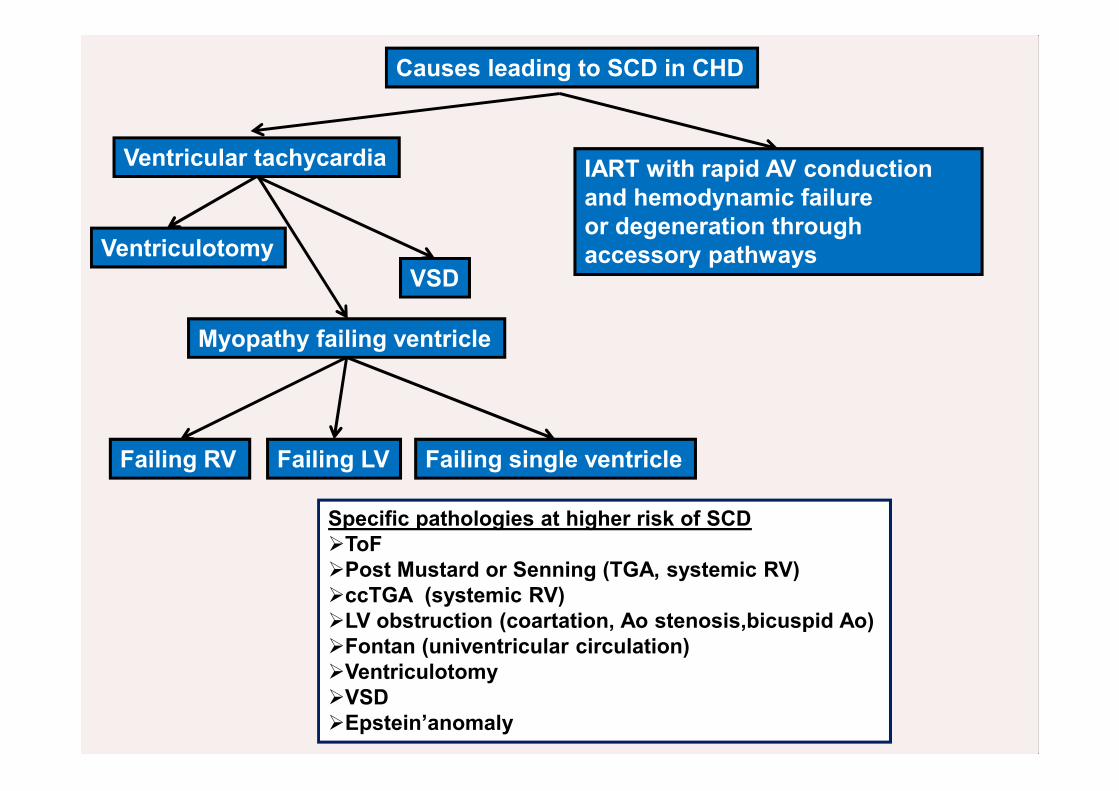
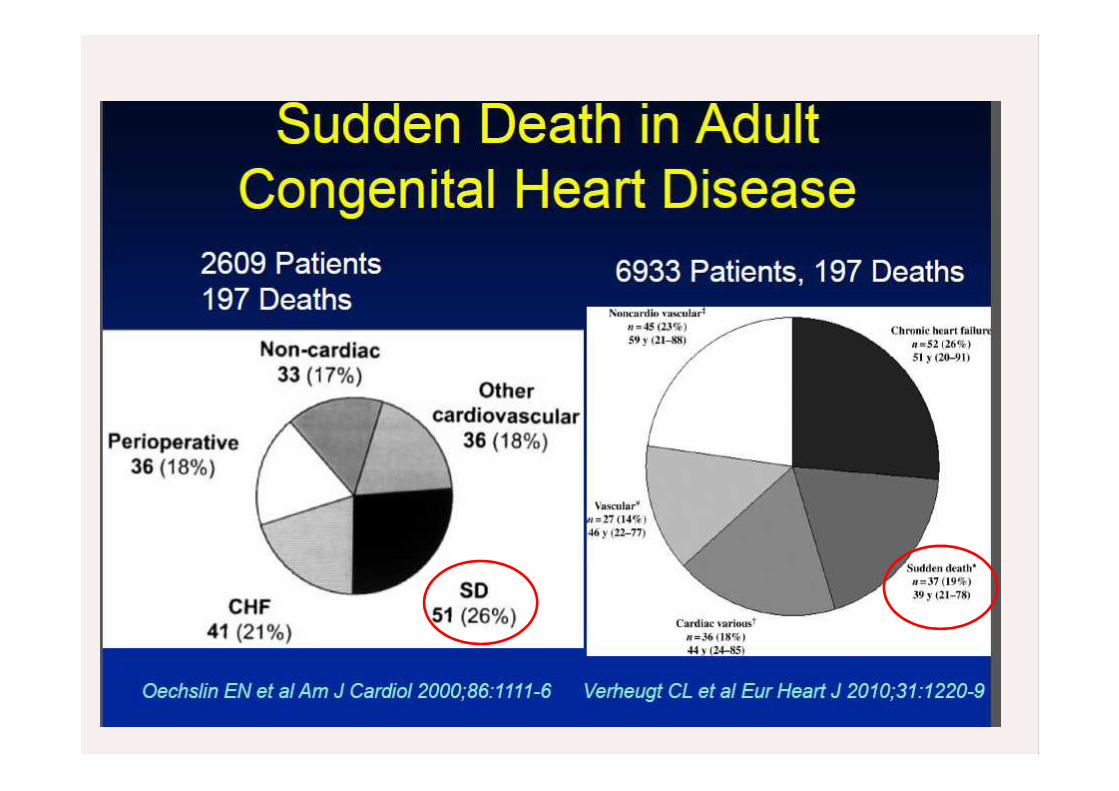
Causes leading to SCD in CHD
Ventricular tachycardia IART with rapid AV conductionand hemodynamic failureor degeneration throughaccessory pathwaysVentriculotomy
VSD
Myopathy failing ventricle
Failing RV Failing LV Failing single ventricle
Specific pathologies at higher risk of SCDToFPost Mustard or Senning (TGA, systemic RV)ccTGA (systemic RV)LV obstruction (coartation, Ao stenosis,bicuspid Ao)Fontan (univentricular circulation)VentriculotomyVSDEpstein’anomaly
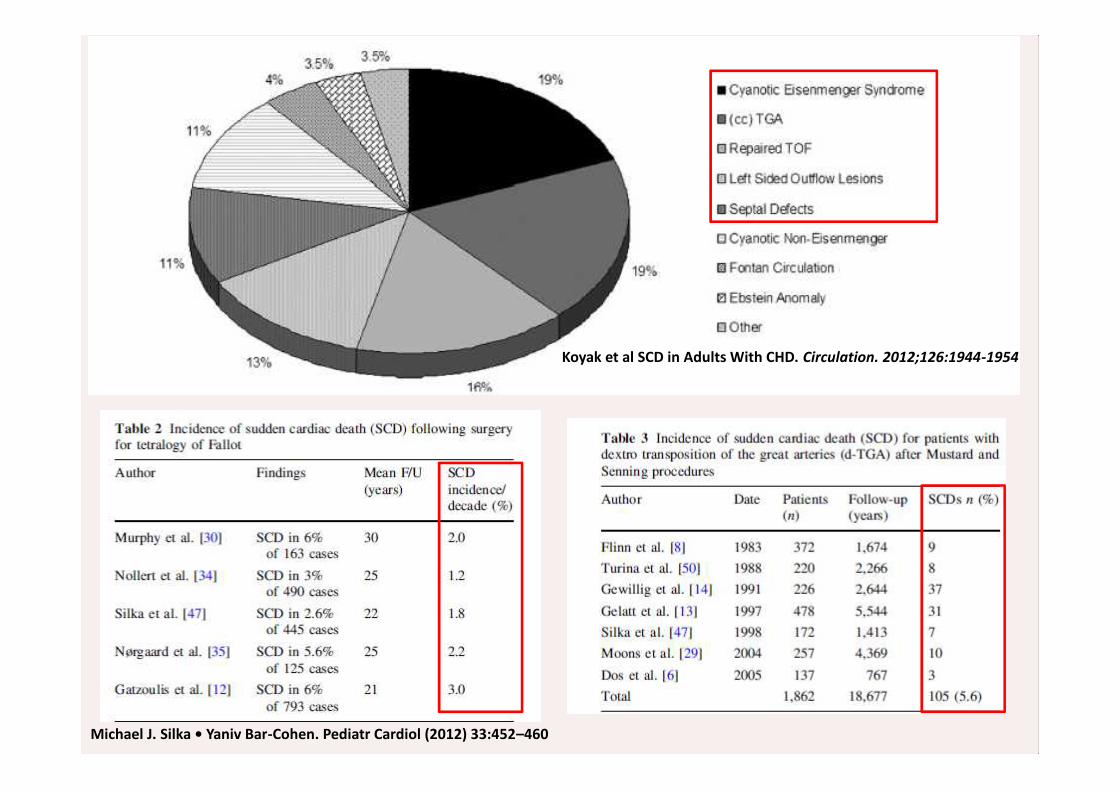
Koyak et al SCD in Adults With CHD. Circulation. 2012;126:1944-1954
Michael J. Silka • Yaniv Bar-Cohen. Pediatr Cardiol (2012) 33:452–460
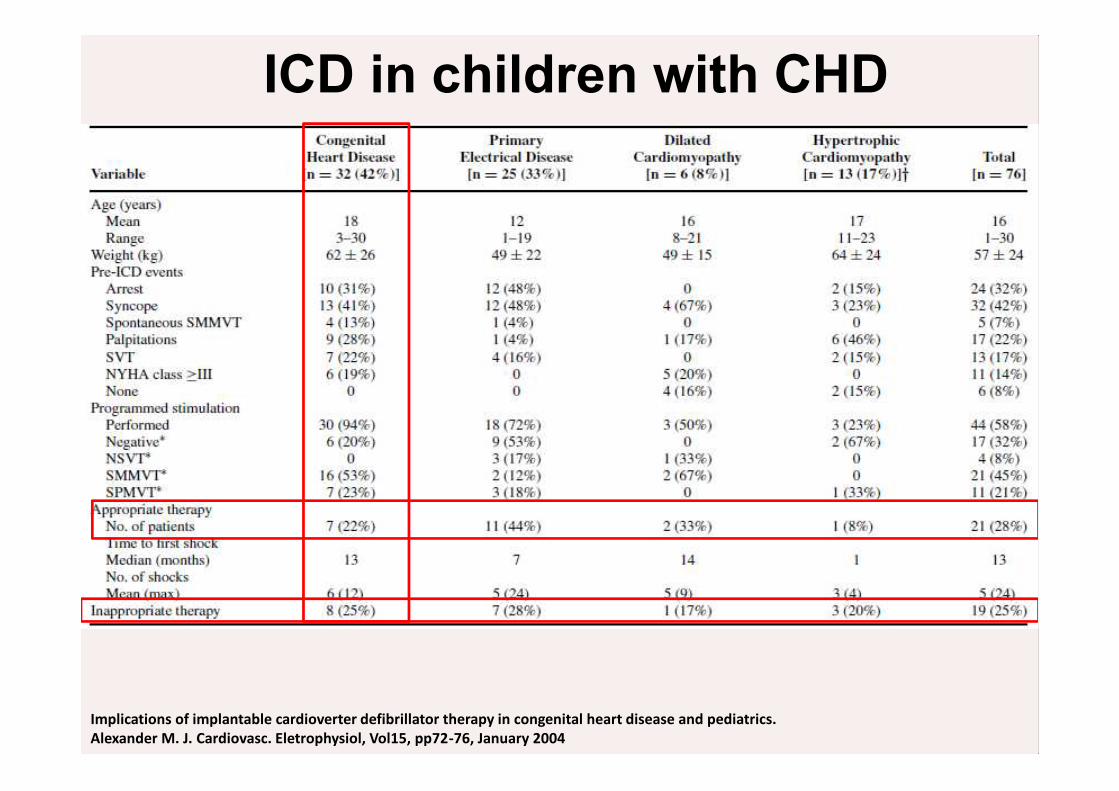
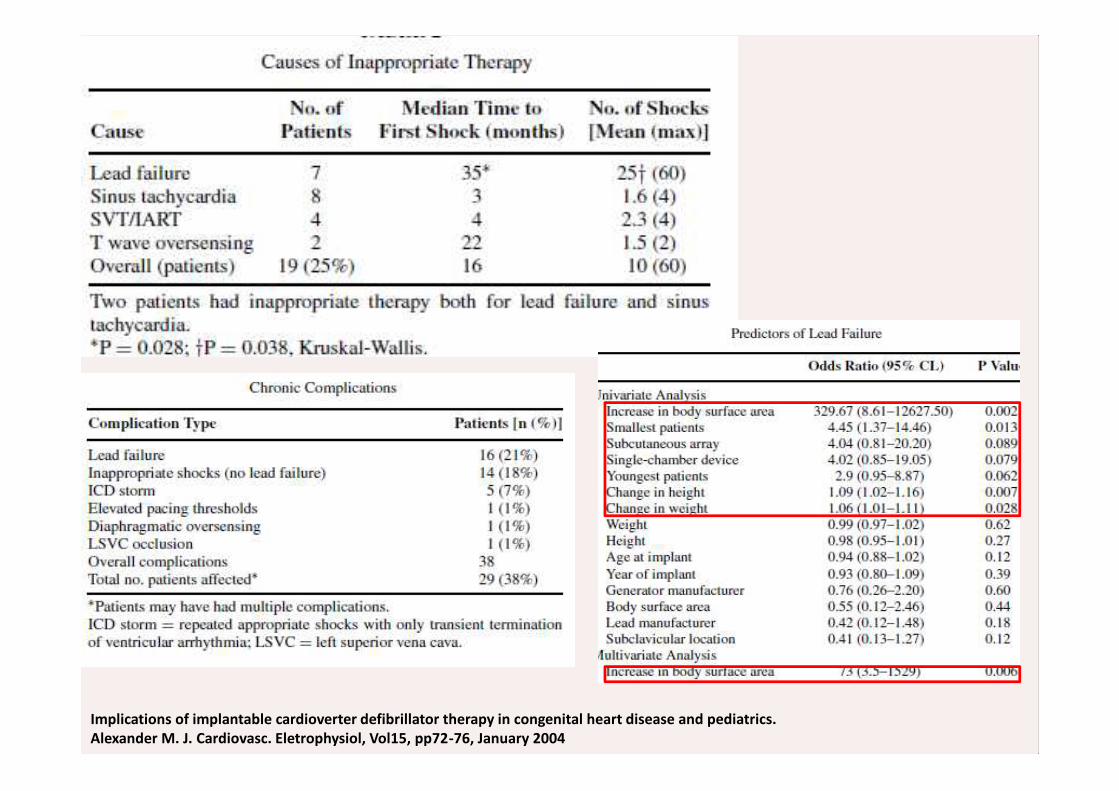
Implications of implantable cardioverter defibrillator therapy in congenital heart disease and pediatrics.Alexander M. J. Cardiovasc. Eletrophysiol, Vol15, pp72-76, January 2004
ICD in children with CHD
Implications of implantable cardioverter defibrillator therapy in congenital heart disease and pediatrics.Alexander M. J. Cardiovasc. Eletrophysiol, Vol15, pp72-76, January 2004
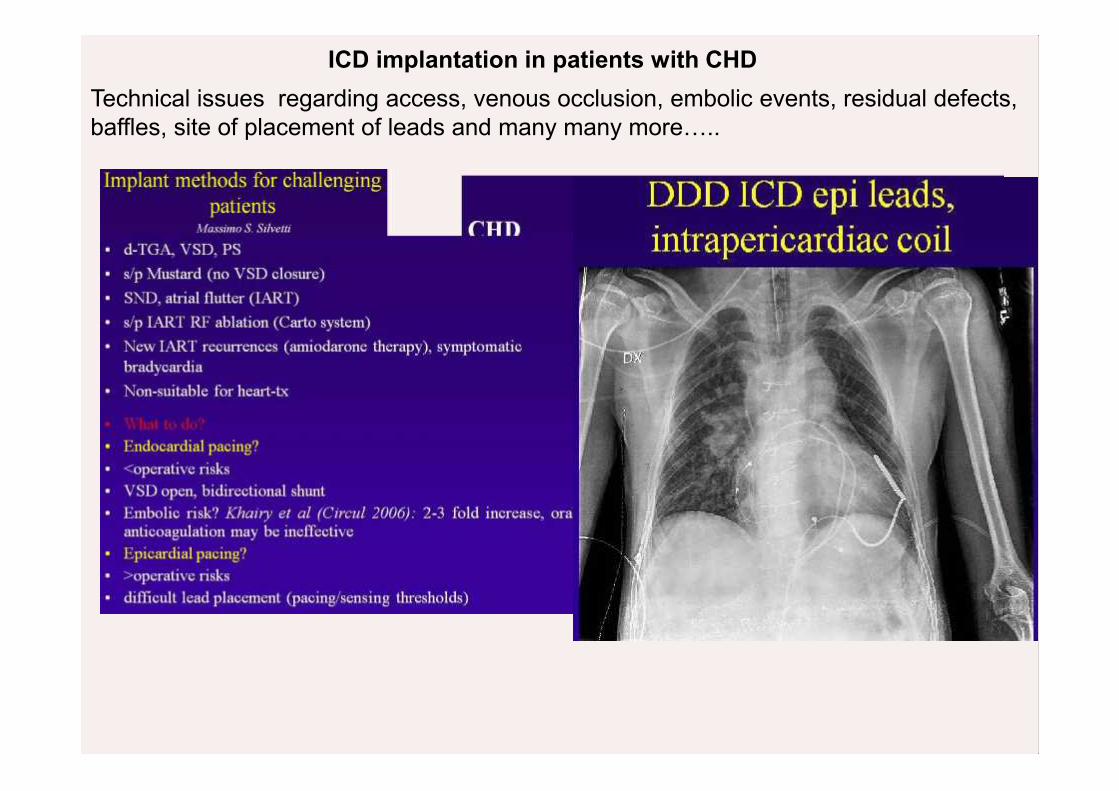
ICD implantation in patients with CHDTechnical issues regarding access, venous occlusion, embolic events, residual defects,baffles, site of placement of leads and many many more…..
Tetralogy of Fallot .The never ending story
Most studied
15-30% Monomorphic VT 2-4% SCD
20-30% IART
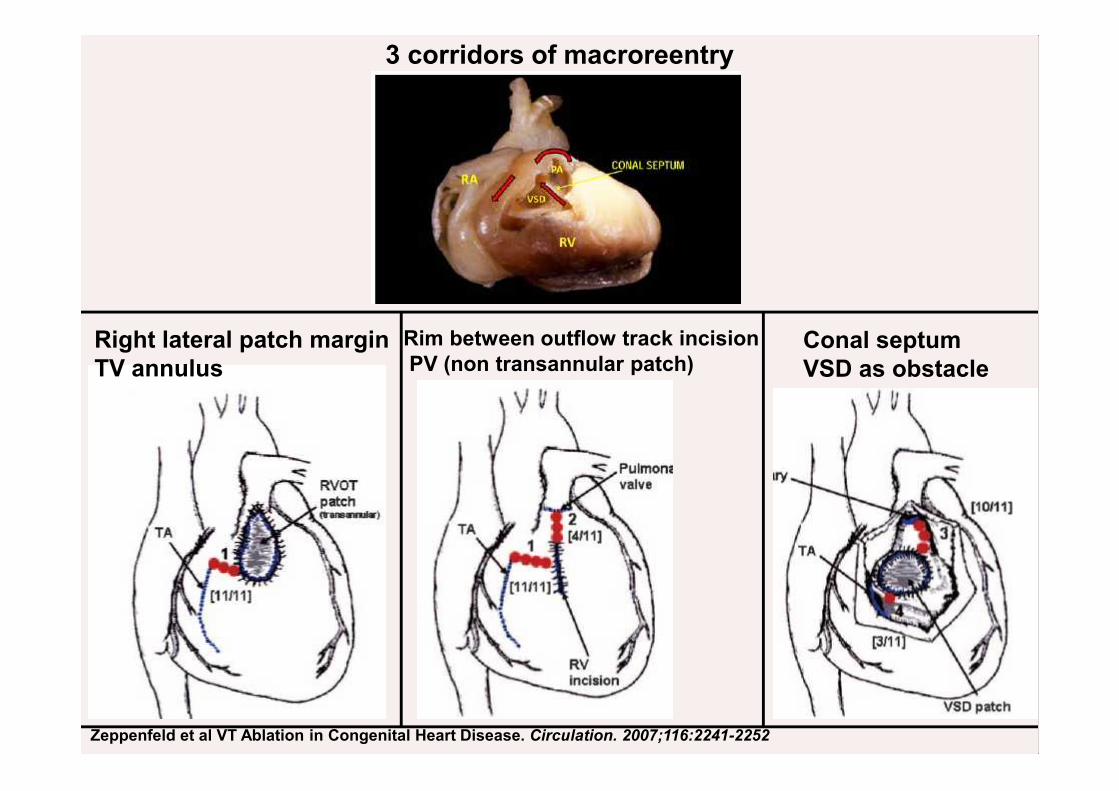
Zeppenfeld et al VT Ablation in Congenital Heart Disease. Circulation. 2007;116:2241-2252
3 corridors of macroreentry
Conal septumVSD as obstacle
Rim between outflow track incisionPV (non transannular patch)
Right lateral patch marginTV annulus
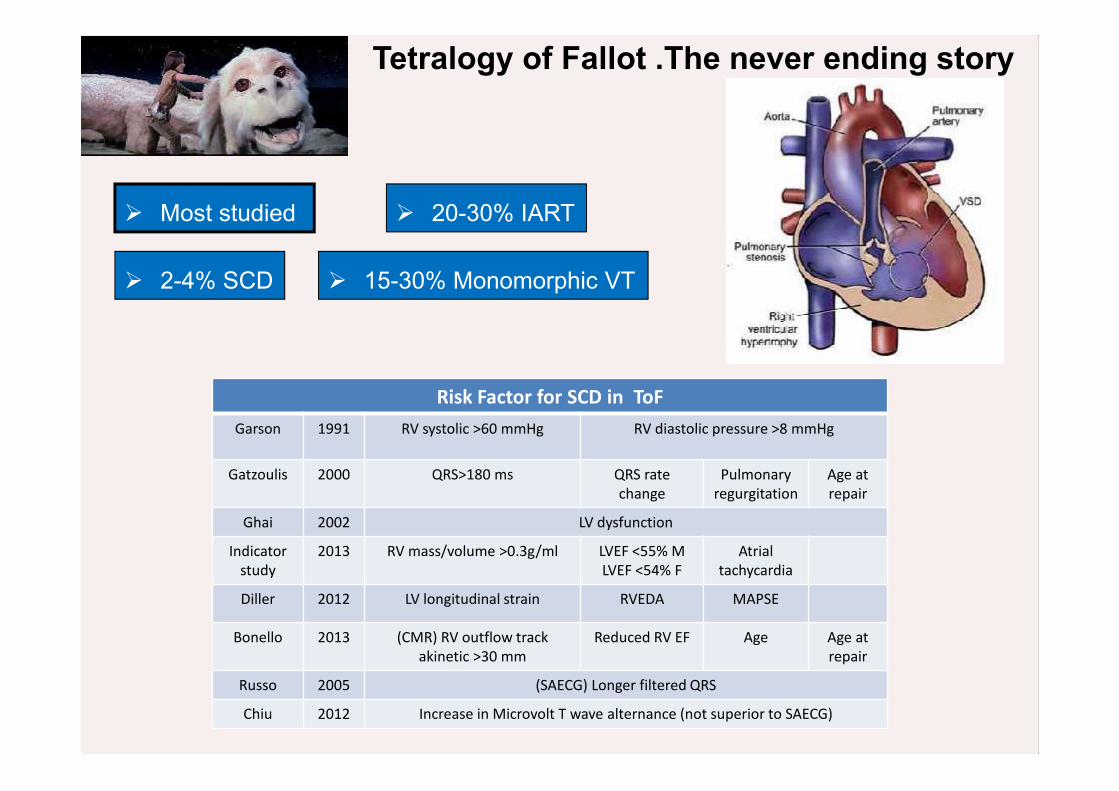
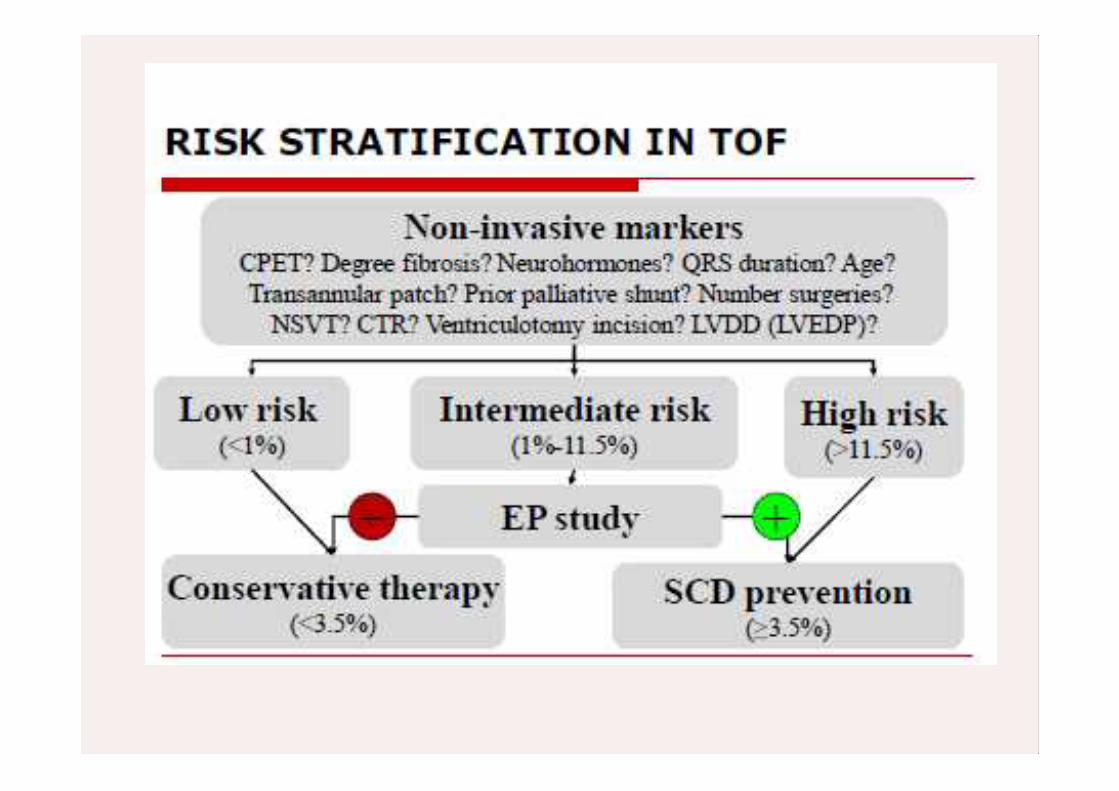
Tetralogy of Fallot .The never ending story
Most studied
Risk Factor for SCD in ToFGarson 1991 RV systolic >60 mmHg RV diastolic pressure >8 mmHg
Gatzoulis 2000 QRS>180 ms QRS ratechange
Pulmonaryregurgitation
Age atrepair
Ghai 2002 LV dysfunction
Indicatorstudy
2013 RV mass/volume >0.3g/ml LVEF <55% MLVEF <54% F
Atrialtachycardia
Diller 2012 LV longitudinal strain RVEDA MAPSE
Bonello 2013 (CMR) RV outflow trackakinetic >30 mm
Reduced RV EF Age Age atrepair
Russo 2005 (SAECG) Longer filtered QRS
Chiu 2012 Increase in Microvolt T wave alternance (not superior to SAECG)
15-30% Monomorphic VT 2-4% SCD
20-30% IART
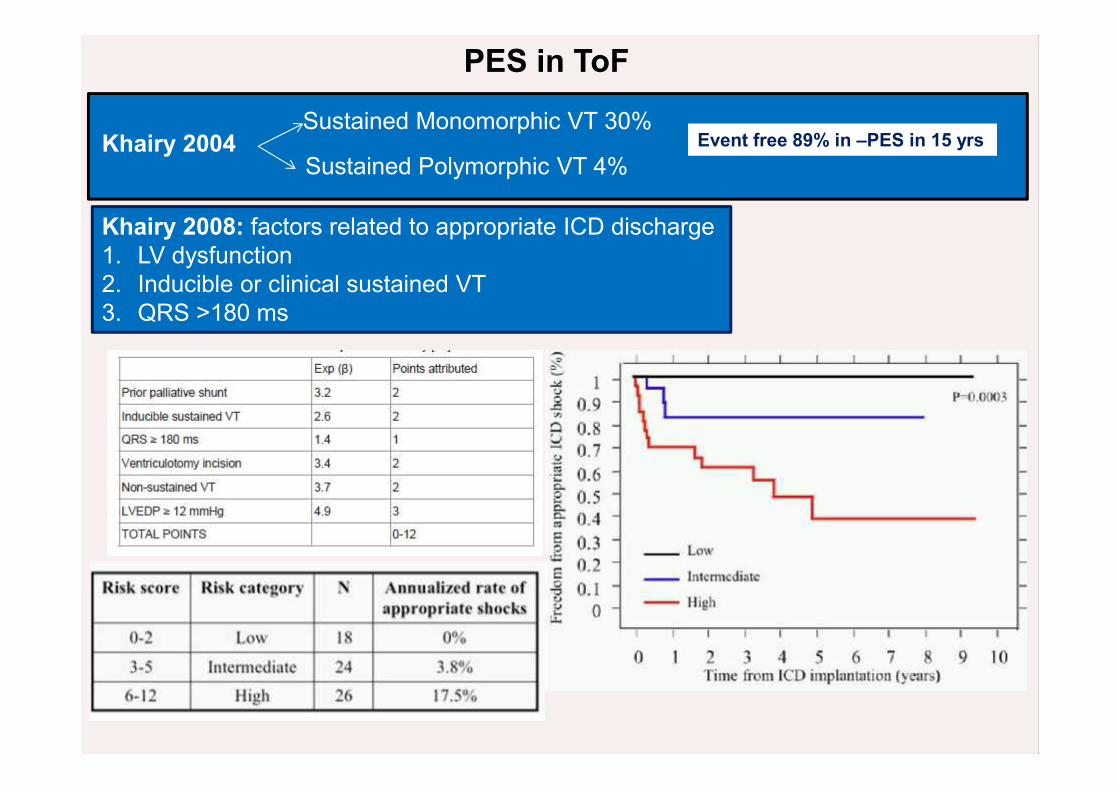
PES in ToF
Khairy 2004Sustained Monomorphic VT 30%
Sustained Polymorphic VT 4%
Khairy 2008: factors related to appropriate ICD discharge1. LV dysfunction2. Inducible or clinical sustained VT3. QRS >180 ms
Event free 89% in –PES in 15 yrs
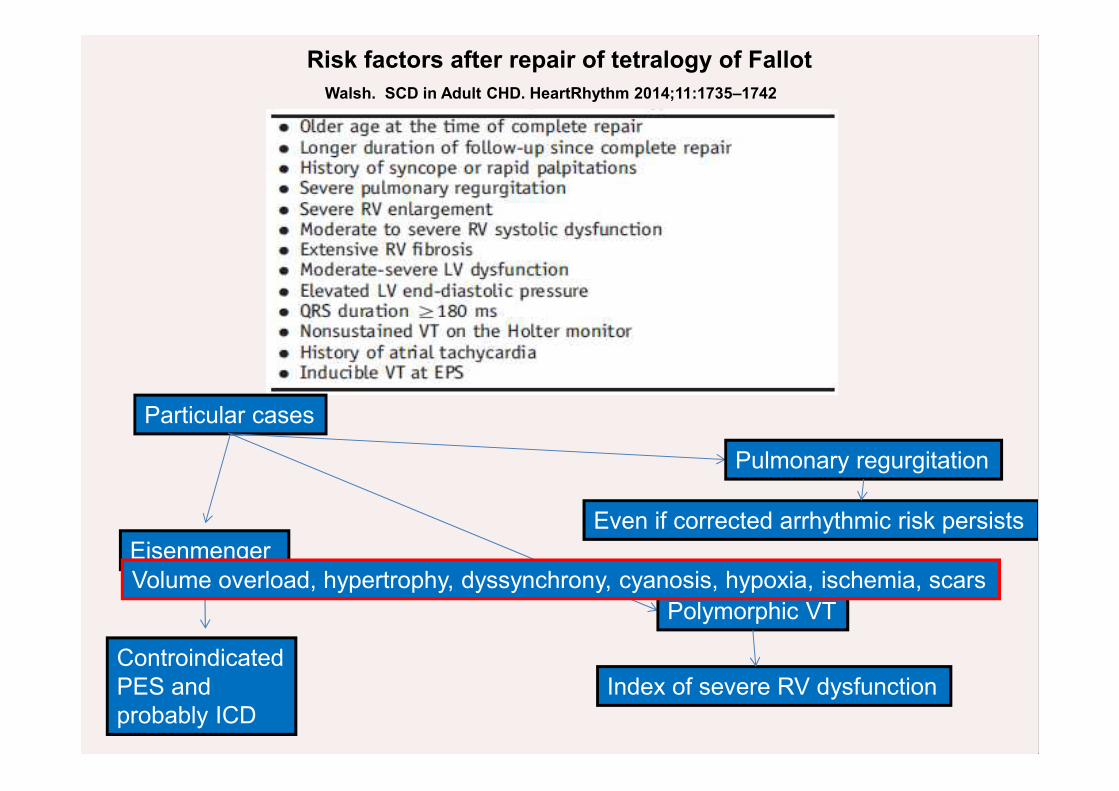
Walsh. SCD in Adult CHD. HeartRhythm 2014;11:1735–1742
Risk factors after repair of tetralogy of Fallot
Particular cases
Eisenmenger
Polymorphic VT
Pulmonary regurgitation
ControindicatedPES andprobably ICD
Index of severe RV dysfunction
Even if corrected arrhythmic risk persists
Volume overload, hypertrophy, dyssynchrony, cyanosis, hypoxia, ischemia, scars

TGA
Higher risk of SCD compared with ToF 5-10%SCD is the leading cause of death after atrial baffle surgeryWilson 1998:SCD in Mustard- Senning 10%Koyak 2012: 10,5% in D-TGA (84% in Mustard-Senning 7% in ccTGA3-5% CAV at birth and 20% for ccTGA
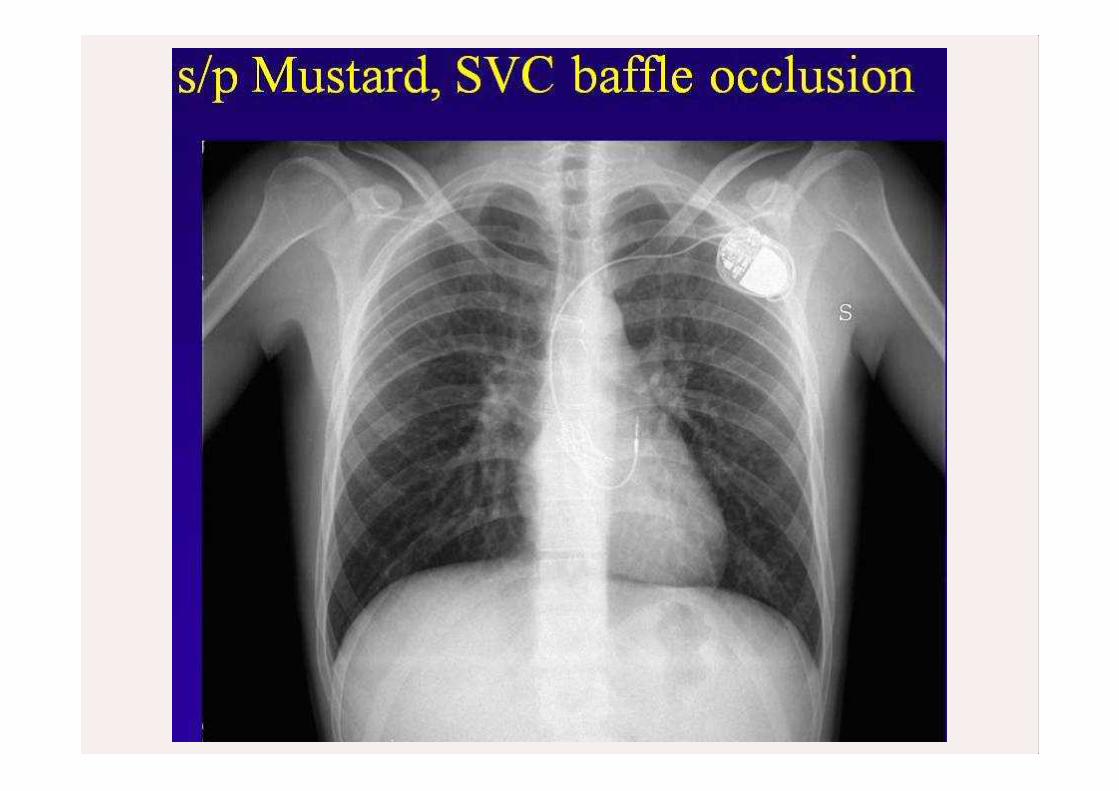
S/P Mustard o SenningTill early 80’s
S/P arterial switchSince 1980
ccTGA
S/P Rastelli
Atrial bafflesextensive atrial scarSystemic RV
Systemic LV
Systemic RV
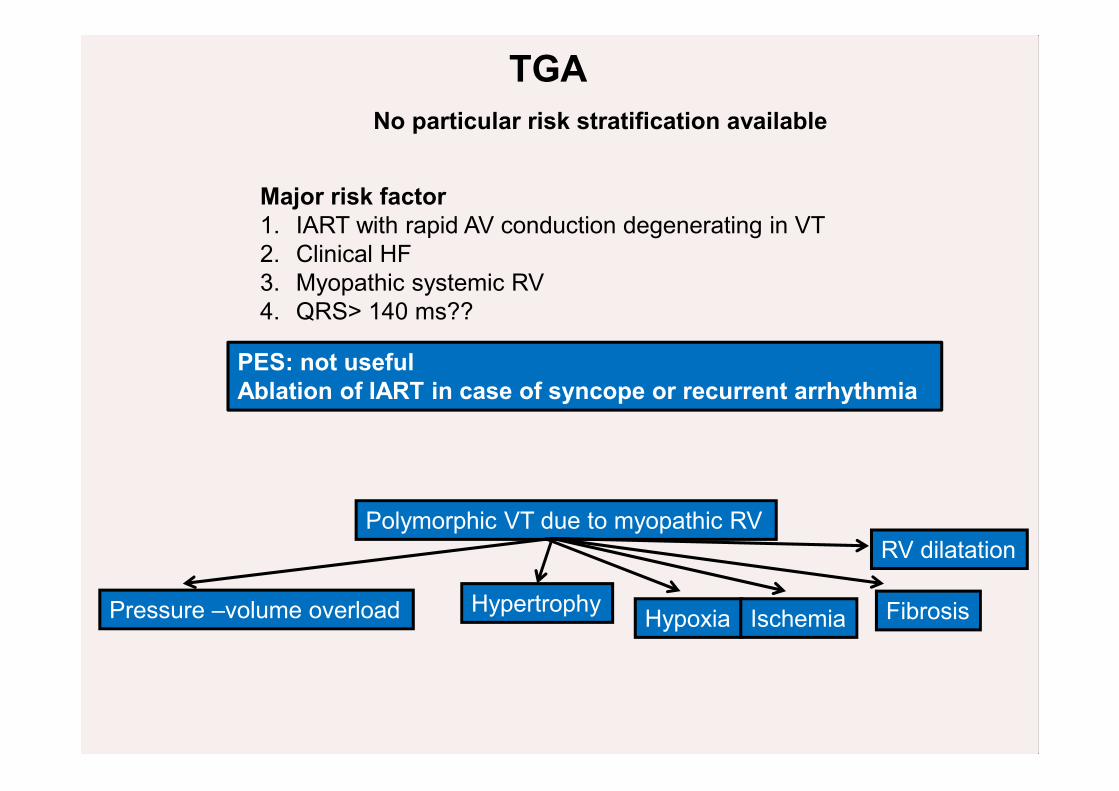
TGANo particular risk stratification available
Major risk factor1. IART with rapid AV conduction degenerating in VT2. Clinical HF3. Myopathic systemic RV4. QRS> 140 ms??
PES: not usefulAblation of IART in case of syncope or recurrent arrhythmia
Polymorphic VT due to myopathic RV
Pressure –volume overload Hypertrophy Hypoxia Ischemia Fibrosis
RV dilatation
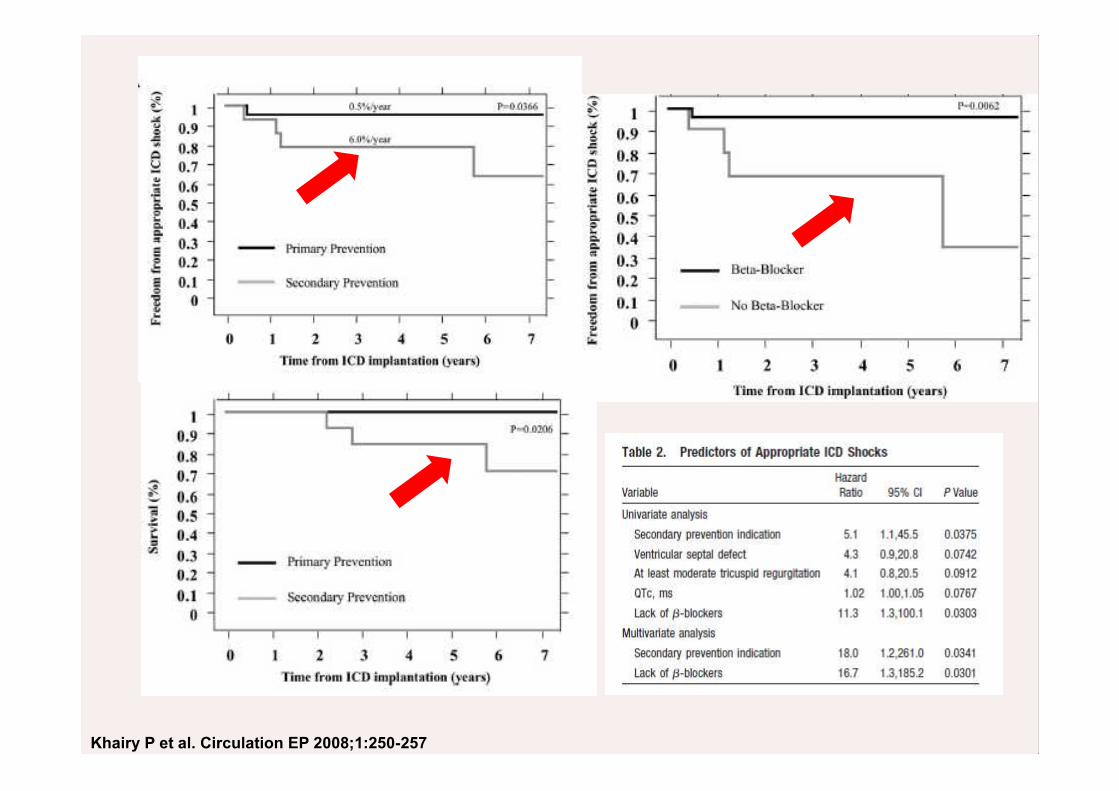
Khairy P et al. Circulation EP 2008;1:250-257
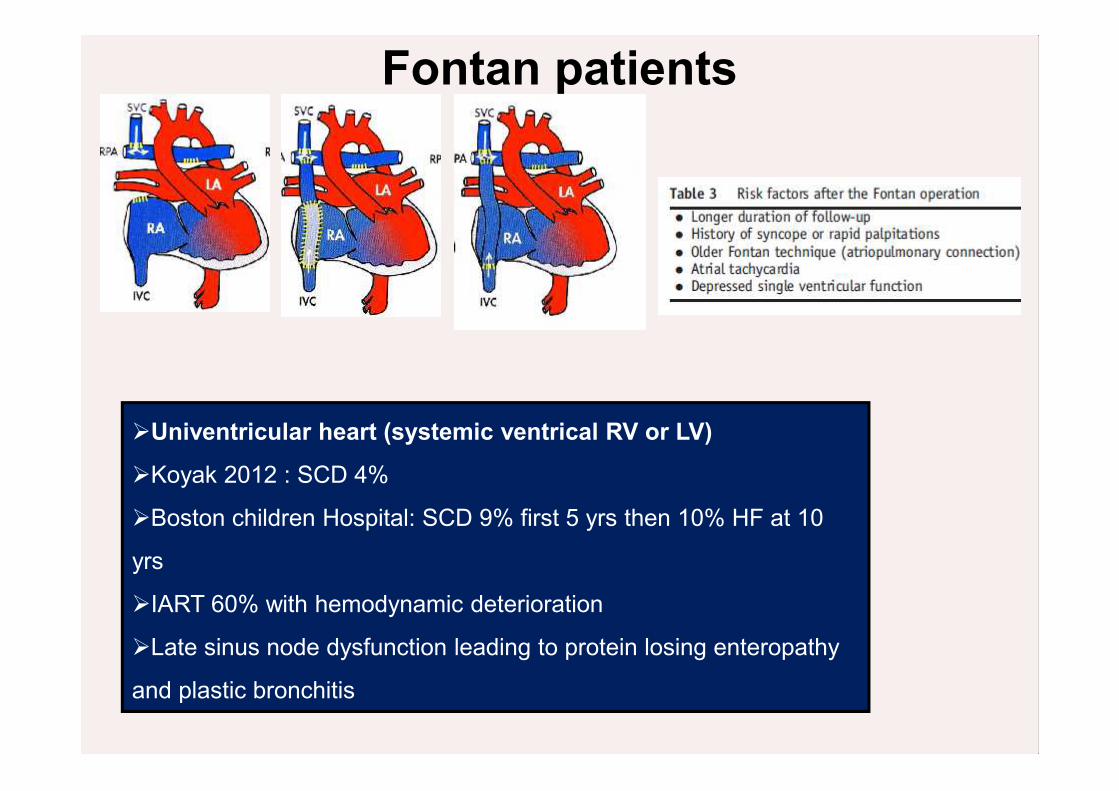
Univentricular heart (systemic ventrical RV or LV)
Koyak 2012 : SCD 4%
Boston children Hospital: SCD 9% first 5 yrs then 10% HF at 10
yrs
IART 60% with hemodynamic deterioration
Late sinus node dysfunction leading to protein losing enteropathy
and plastic bronchitis
Fontan patients
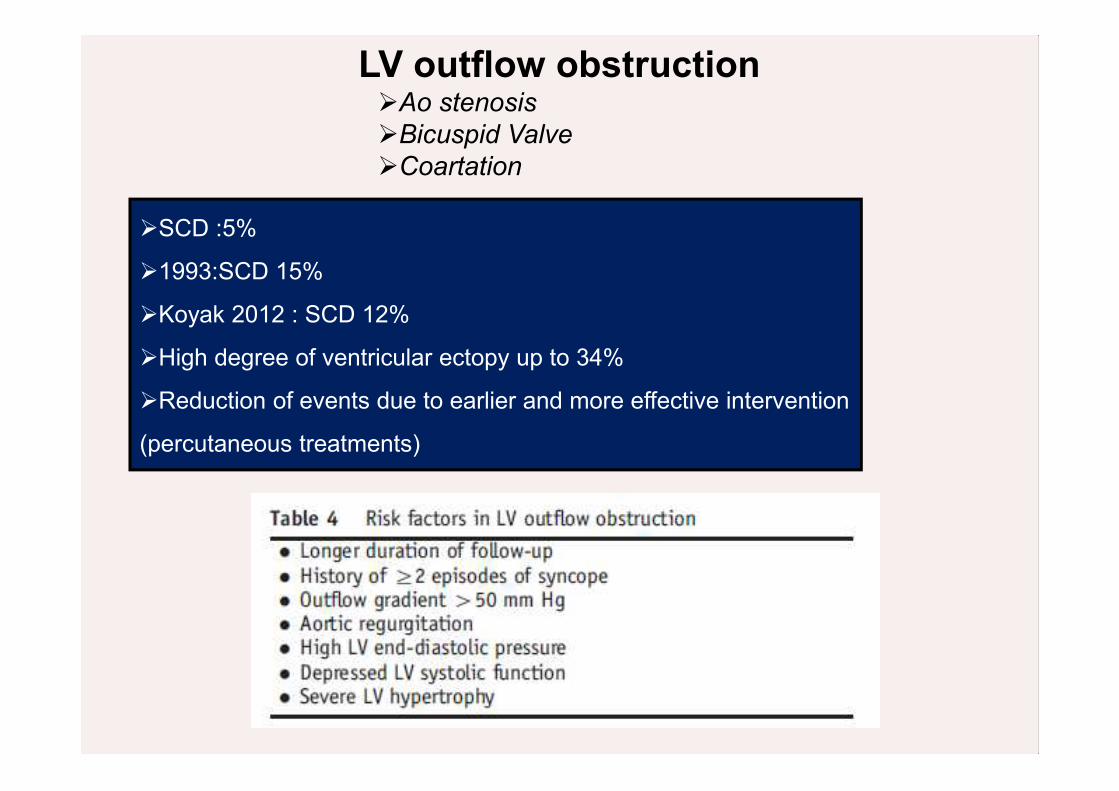
LV outflow obstructionAo stenosisBicuspid ValveCoartation
SCD :5%
1993:SCD 15%
Koyak 2012 : SCD 12%
High degree of ventricular ectopy up to 34%
Reduction of events due to earlier and more effective intervention
(percutaneous treatments)
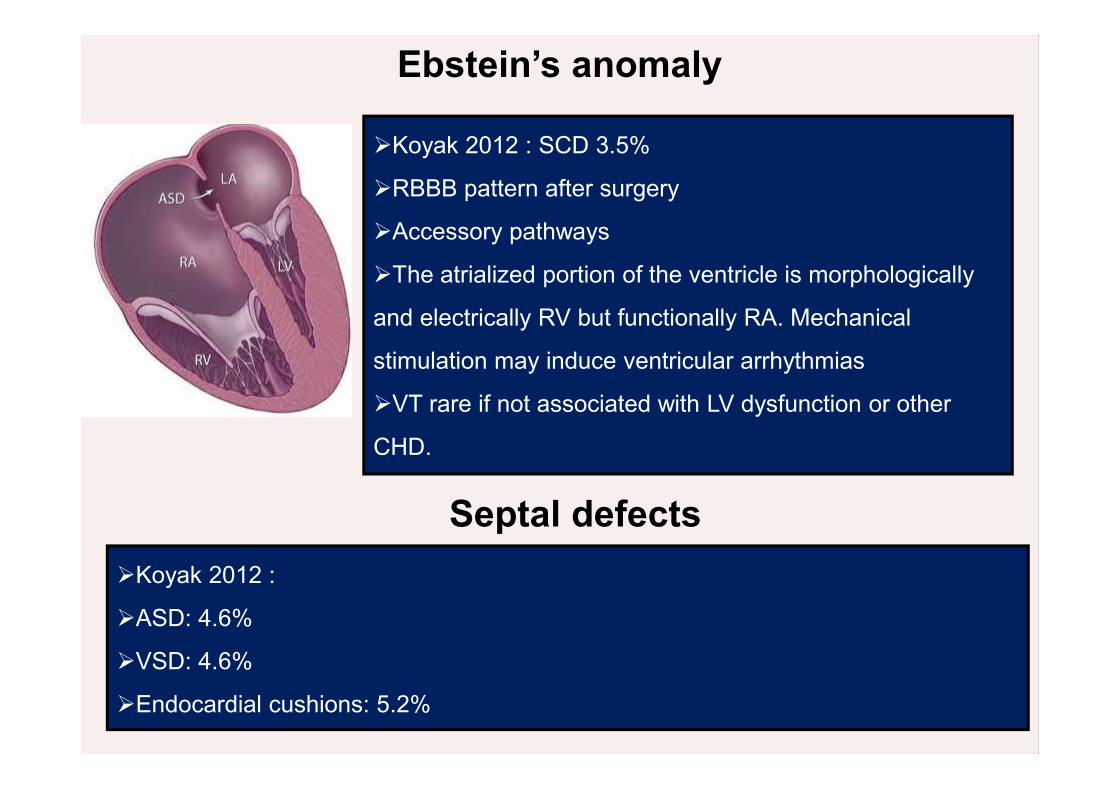
Ebstein’s anomaly
Koyak 2012 : SCD 3.5%
RBBB pattern after surgery
Accessory pathways
The atrialized portion of the ventricle is morphologically
and electrically RV but functionally RA. Mechanical
stimulation may induce ventricular arrhythmias
VT rare if not associated with LV dysfunction or other
CHD.
Septal defectsKoyak 2012 :
ASD: 4.6%
VSD: 4.6%
Endocardial cushions: 5.2%
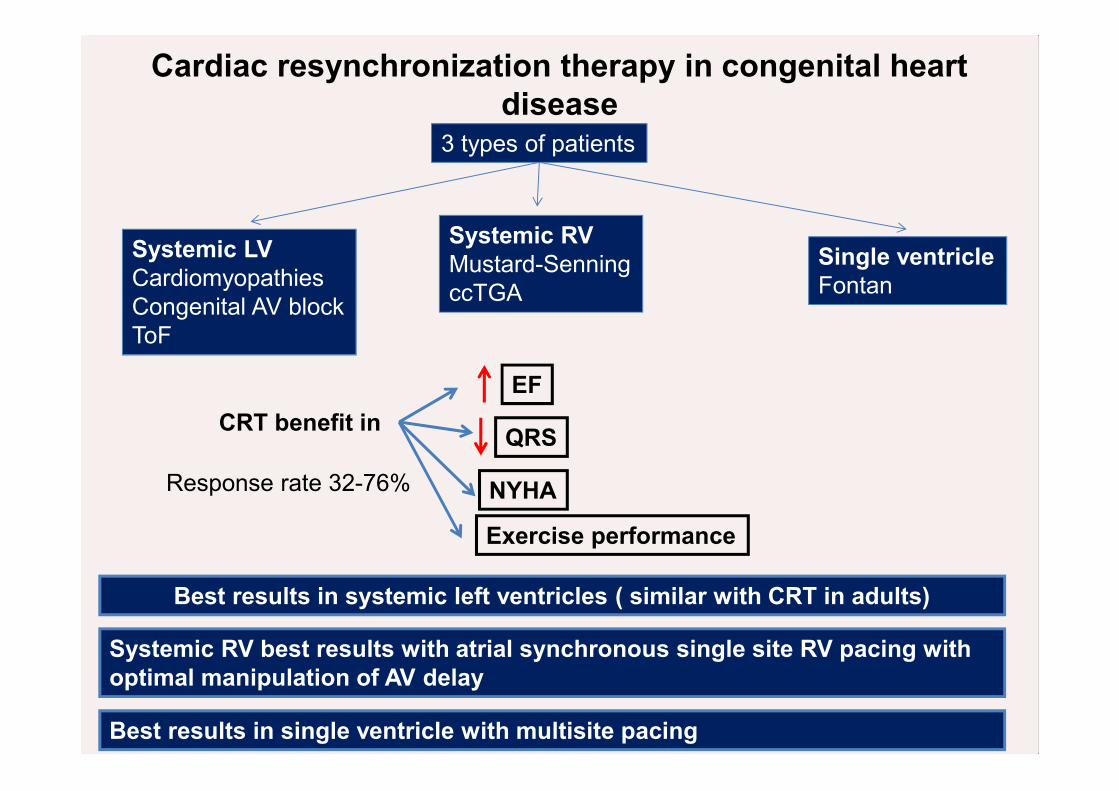
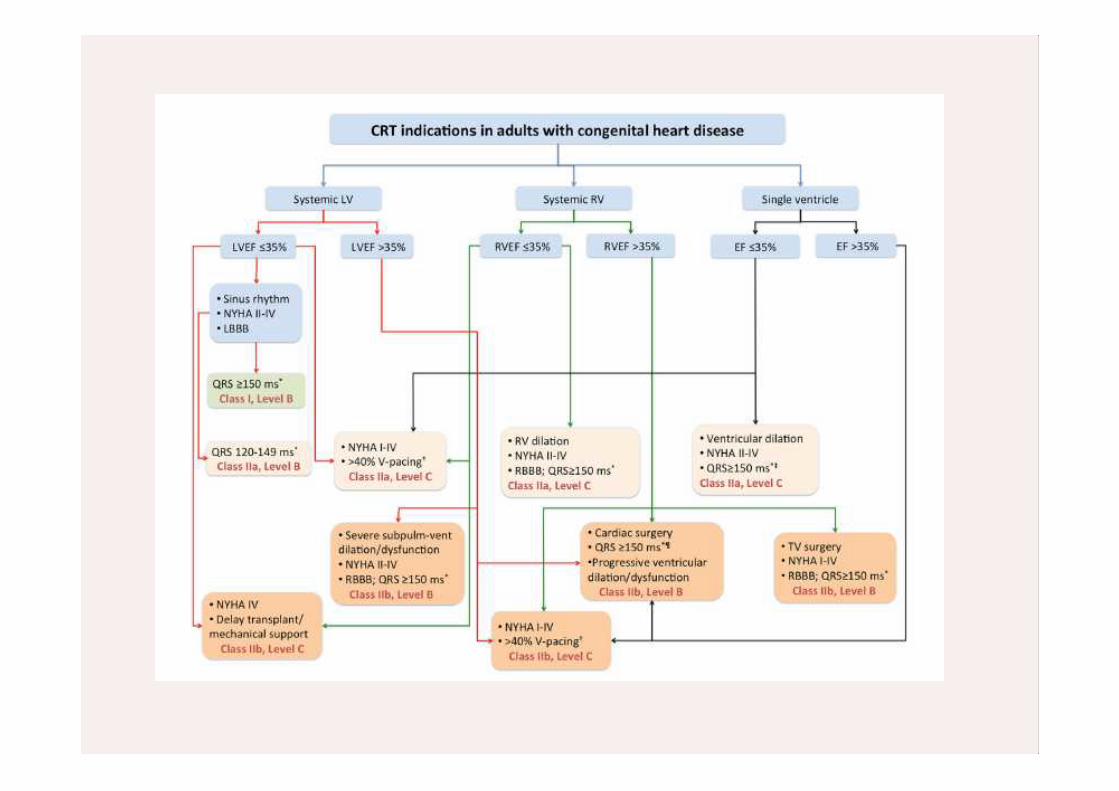
Cardiac resynchronization therapy in congenital heartdisease
3 types of patients
Systemic LVCardiomyopathiesCongenital AV blockToF
Systemic RVMustard-SenningccTGA
Single ventricleFontan
CRT benefit inEF
QRS
NYHA
Exercise performance
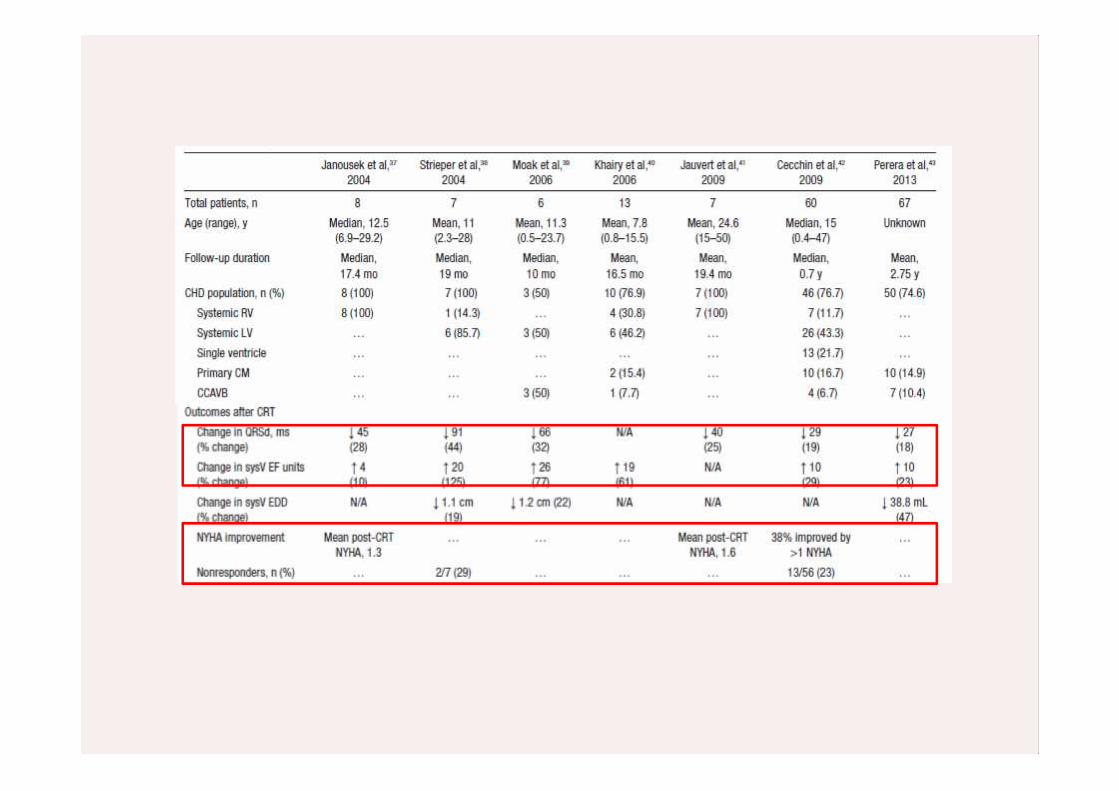
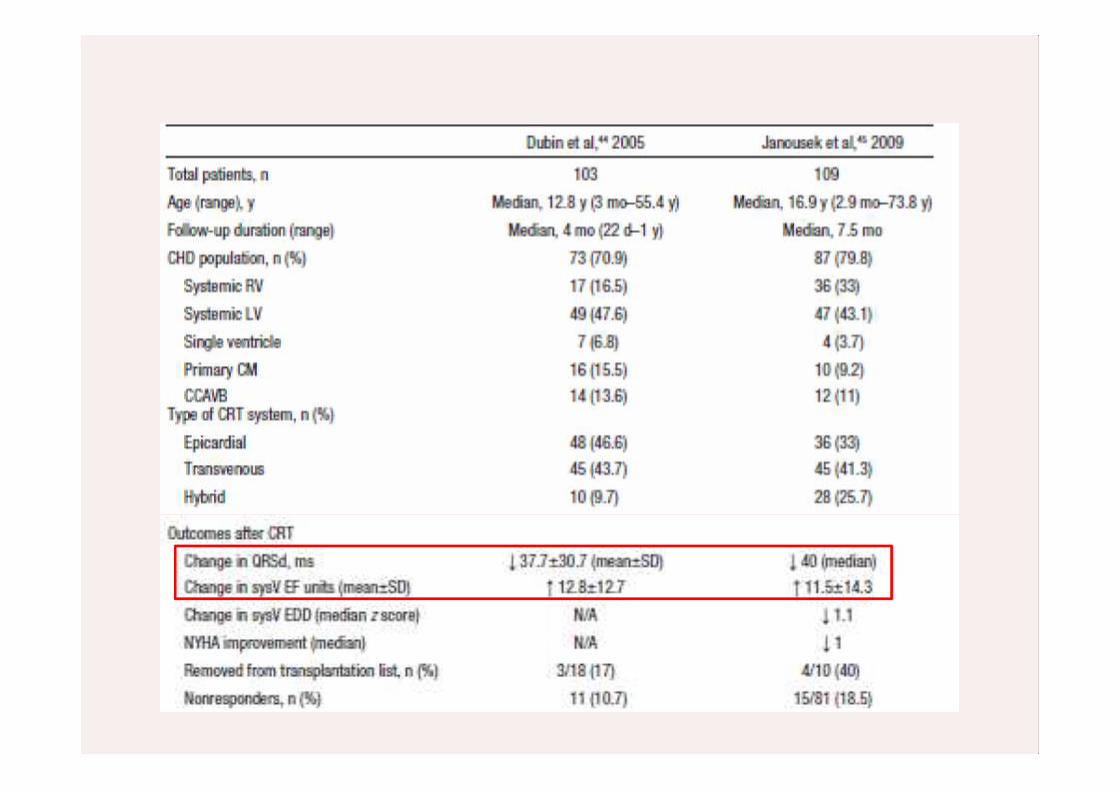
Response rate 32-76%
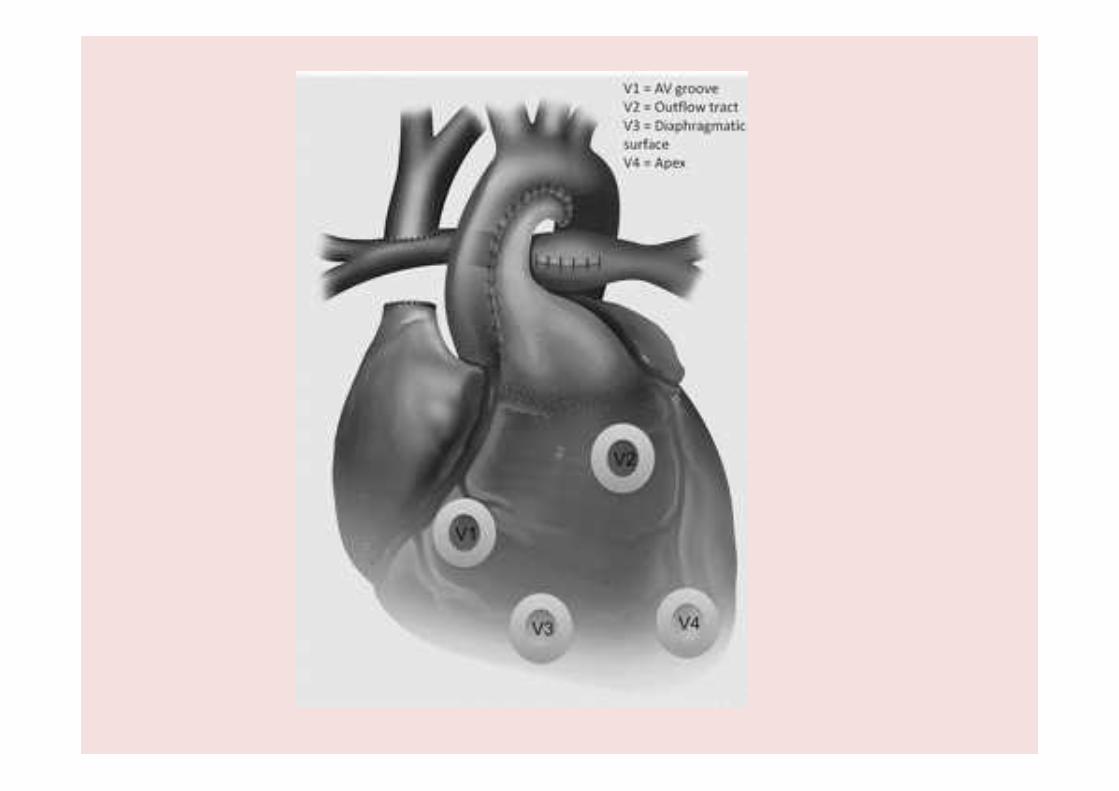
Best results in single ventricle with multisite pacing
Best results in systemic left ventricles ( similar with CRT in adults)
Systemic RV best results with atrial synchronous single site RV pacing withoptimal manipulation of AV delay
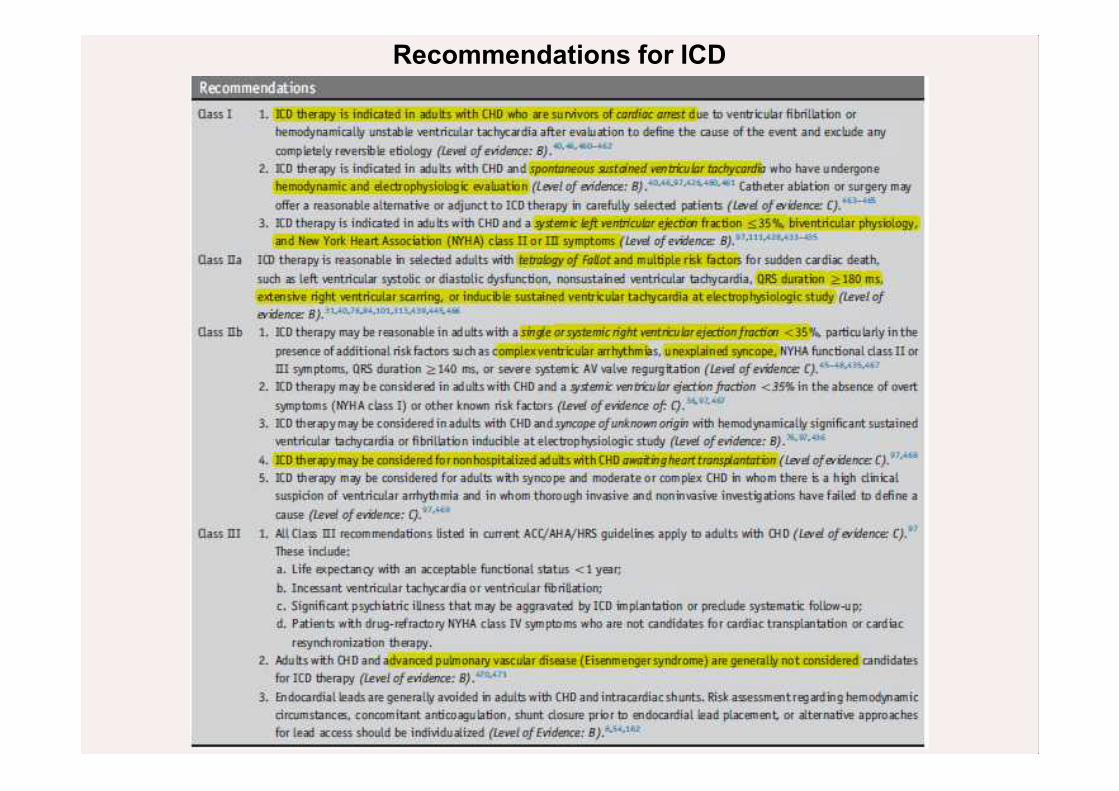
Recommendations for ICD
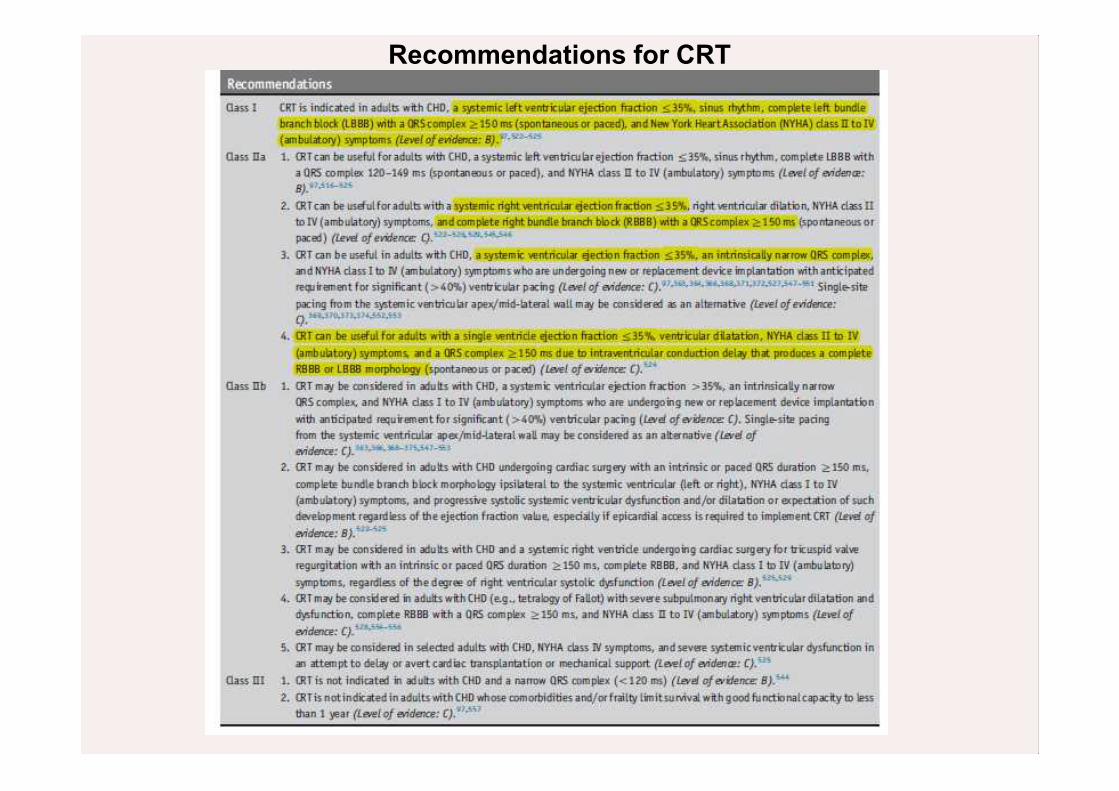
Recommendations for CRT
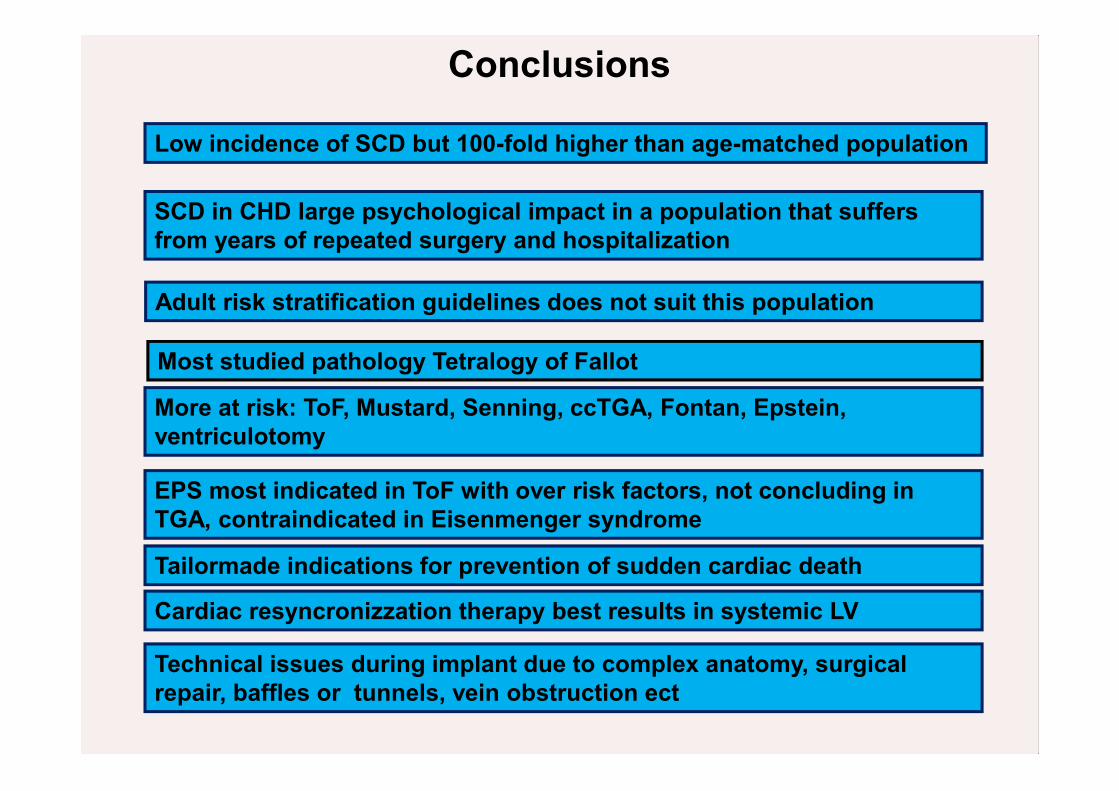
Conclusions
Low incidence of SCD but 100-fold higher than age-matched population
SCD in CHD large psychological impact in a population that suffersfrom years of repeated surgery and hospitalization
Adult risk stratification guidelines does not suit this population
Most studied pathology Tetralogy of Fallot
Cardiac resyncronizzation therapy best results in systemic LV
Tailormade indications for prevention of sudden cardiac death
More at risk: ToF, Mustard, Senning, ccTGA, Fontan, Epstein,ventriculotomy
EPS most indicated in ToF with over risk factors, not concluding inTGA, contraindicated in Eisenmenger syndrome
Technical issues during implant due to complex anatomy, surgicalrepair, baffles or tunnels, vein obstruction ect
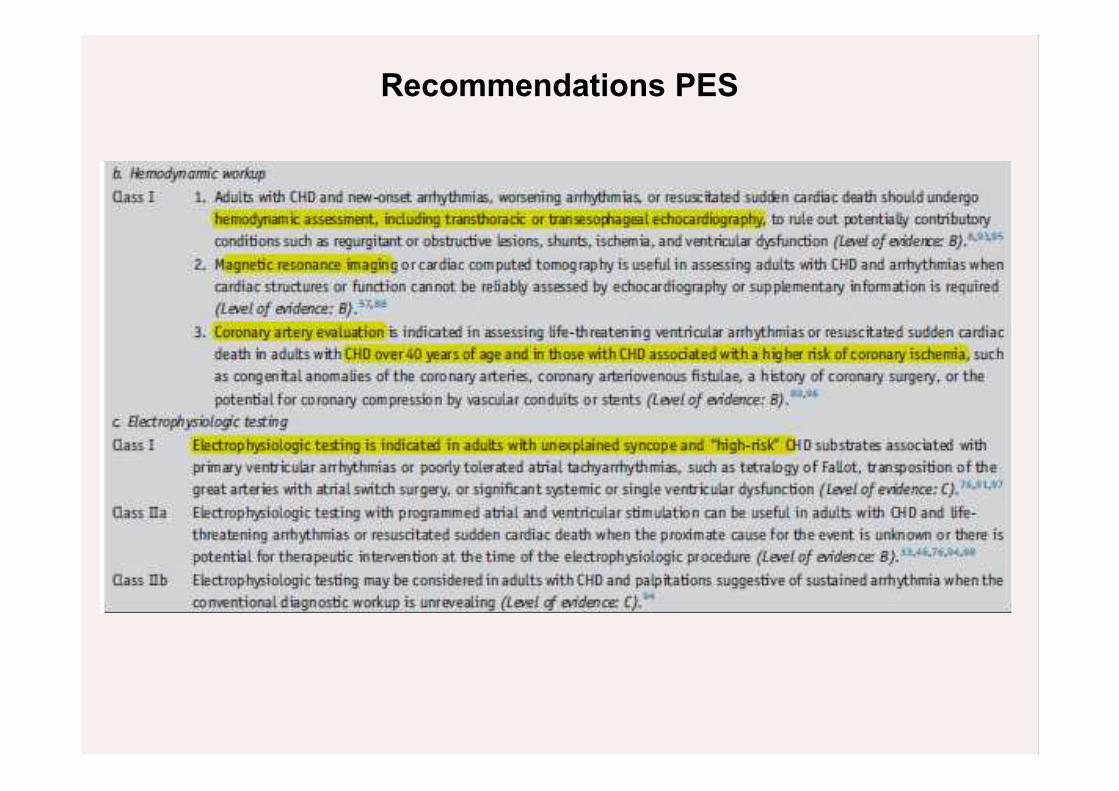
Recommendations PES
PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease.
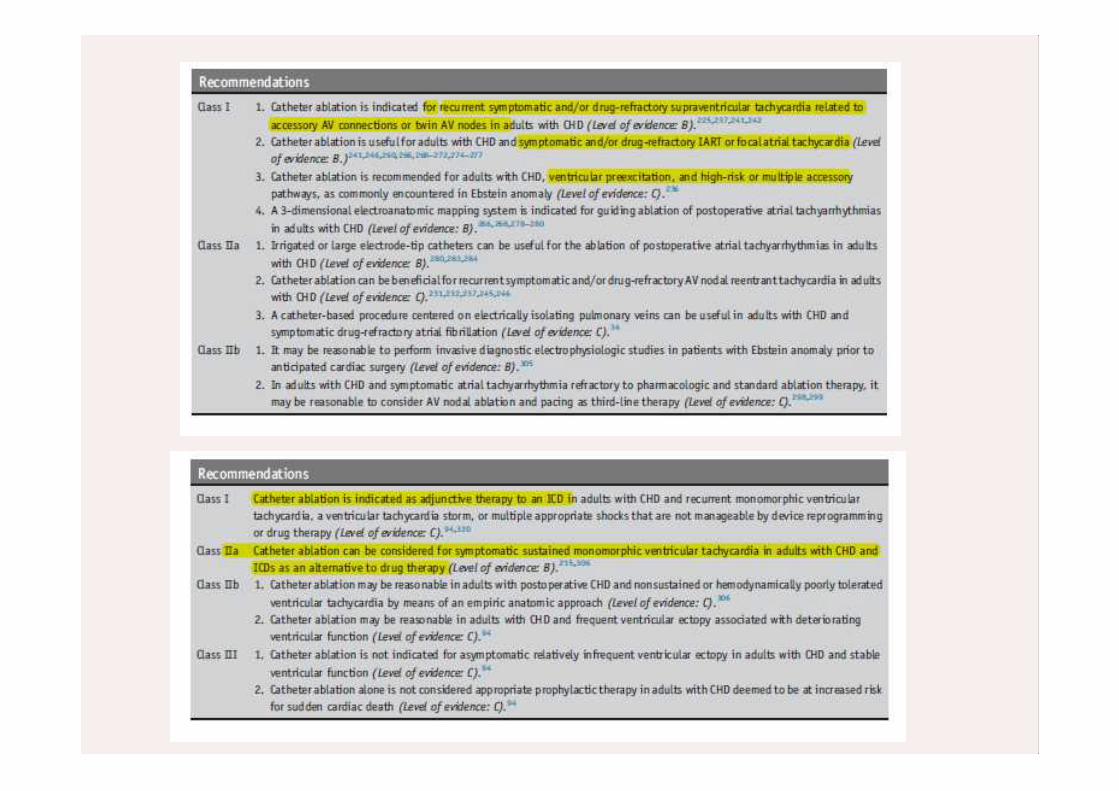
PACES/HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in Adult Congenital Heart Disease.

![HC - Sodeca Worldwide · 2018-05-14 · 17 hc modelo mc ec vsd sr ηe [%] n [kw] [m3/h] [mmh 2 o] [rpm] hc-25-4t/h - - - - - - 0,099 707 5,15 1407 hc-25-4m/h - - - - - - 0,102 693](https://static.fdocument.org/doc/165x107/5bbc90d409d3f2ee168bfb8b/hc-sodeca-2018-05-14-17-hc-modelo-mc-ec-vsd-sr-e-n-kw-m3h-mmh.jpg)