Department of Cardiology , Brawijaya Medical School Saiful Anwar General Hospital
2016 Large Clinical Studies in Interventional Cardiology
37ο Π.Κ.Σ «Επεµβατική Καρδιολογία» 22/10/2016, Athens - Greece
Kostopoulos KonstantinosCARDIOLOGIST1st Cardiac Dpt. NIKEA GENERAL HOSPTAL Piraeus – GREECE
PRAGUE-18: Pra vs Tica σε PPCI !έλεγχος αποτελεσµατικότητας & αιµορραγίας ANTARCTIC: Κανονική vs προσαρµοσµένης δόσης Pra σε ACS PCI, >75y.o PEGASUS TIMI 54: (Tica 60 vs 90) vs ASA: CV events σε high risk pts µε >12m x-ACS CHAMPION PHOENIX: STEMI PPCI: “off hours” vs “on hours” DOCTORS: OCT use in ACS BBK II: Culotte vs T-stenting για διχασµικές βλάβες EROSION: Συµβολή OCT σε αποφυγή stenting ασθενών µε ACS NORSTENT: “Real world” σύγκριση BMS & DES
CE-MARC II: Διάγνωση CAD: C. Cath - CMR vs UK NICE guidelines vs MPS-spect P2-S3i TAVR: TAVI σε διάµεσου κινδύνου ασθενείς µε σοβαρή AoS
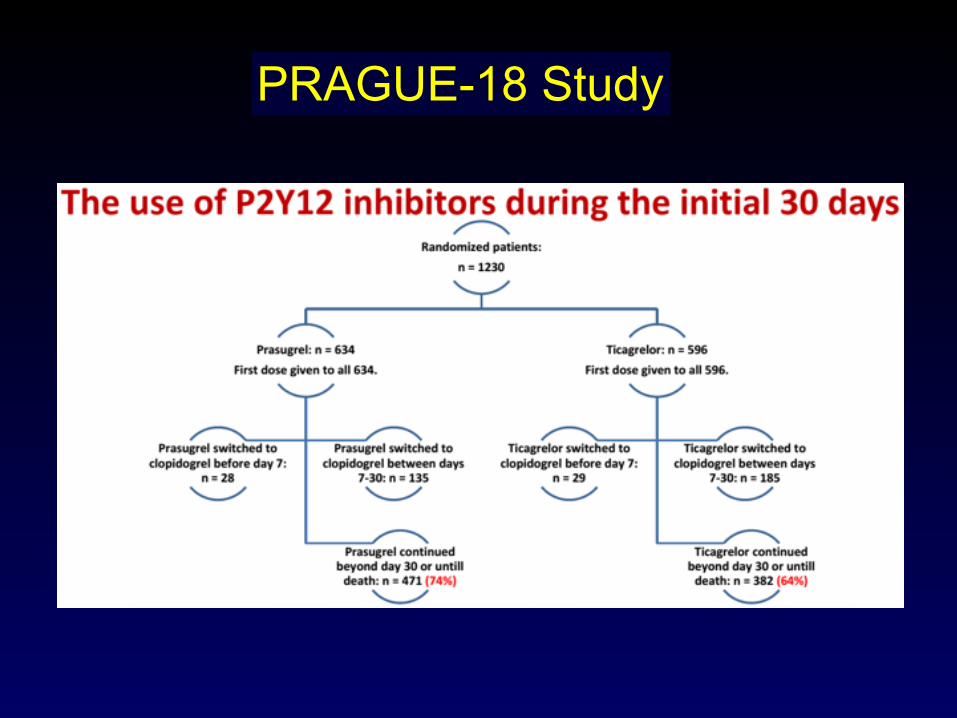
PRAGUE-18 Study Randomized comparison of
Ticagrelor vs Prasugrel in STEMI
1. Head-to-head comparison of PRASUGREL vs TICAGRELOR in STEMI patients treated by P.PCI
2. Safety of (economically motivated) postdischarge switch from PRASU/TICA to CLOPIDOGREL
Circulation Sept 2016
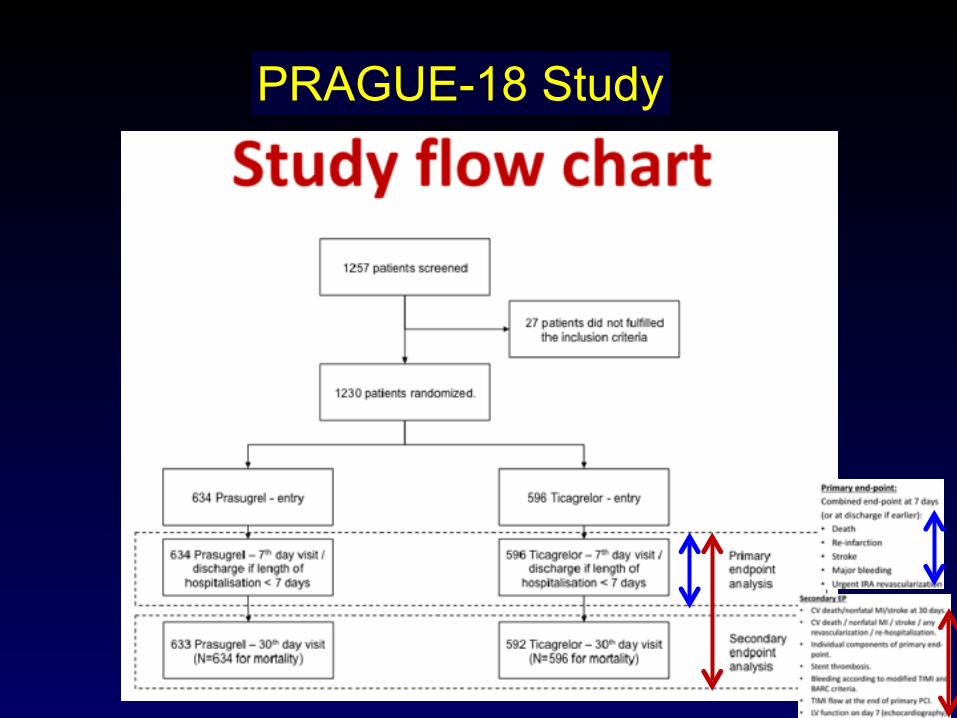
PRAGUE-18 Study
PRAGUE-18 Study
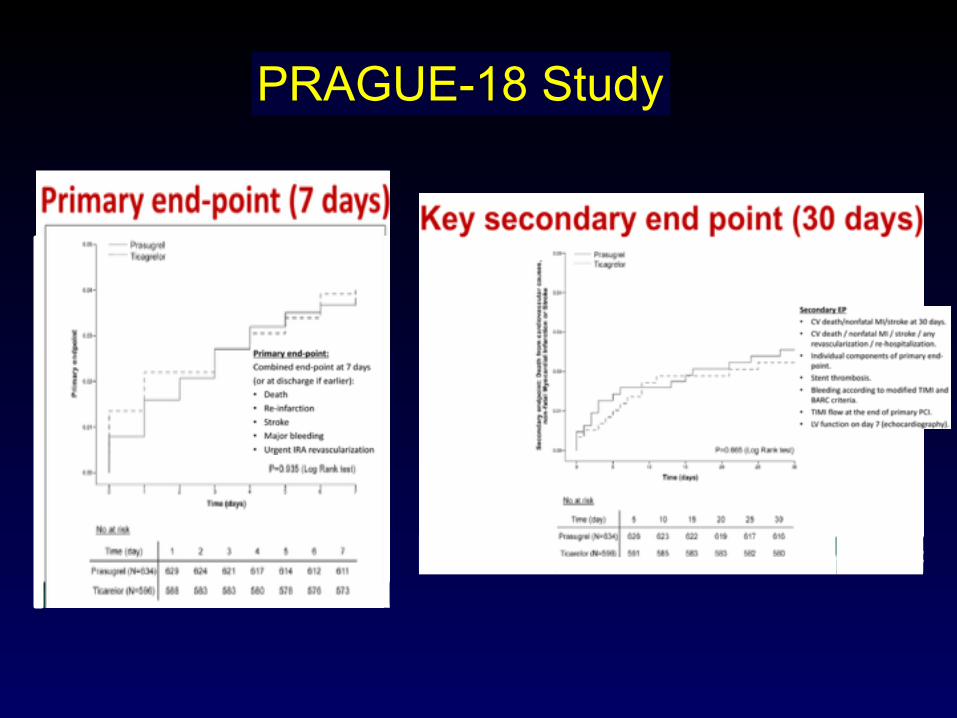
PRAGUE-18 Study
PRAGUE-18 Study
CONCLUSION
No difference between TICA & PRASU in the early phase of AMI treated by PPCI
1y F.U results are expected by May 2017
Lancet Aug 2016
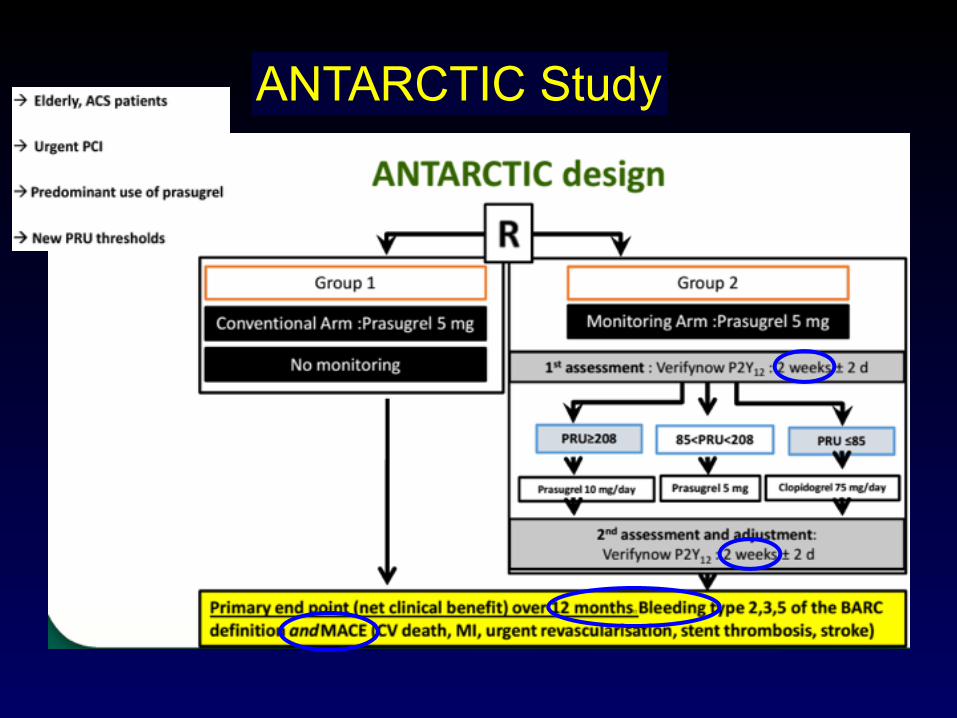
ANTARCTIC Study
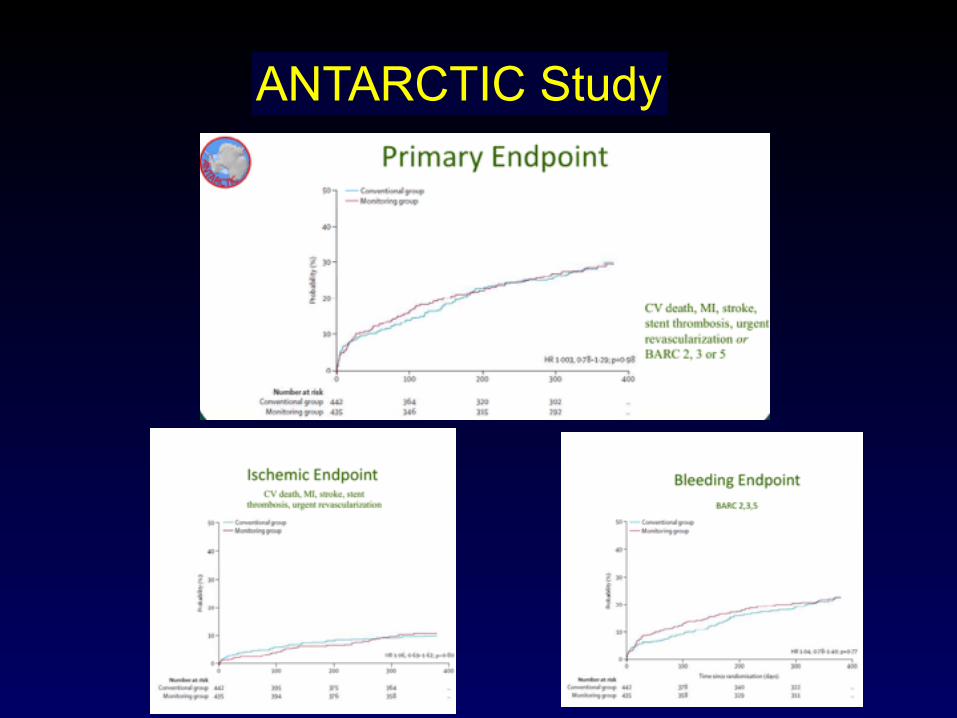
ANTARCTIC Study
ANTARCTIC Study
CONCLUSION
PLT function monitoring ATP therapy adjustment in stented for ACS elderly pts does not improve clinical outcome. This failure in clinical improvement is not related to the risk level of the population or type of P2Y12 antagonist
ANTARCTIC Study
PEGASUS TIMI 54 Study (ASA vs ASA+TICA)
NEJM 2015
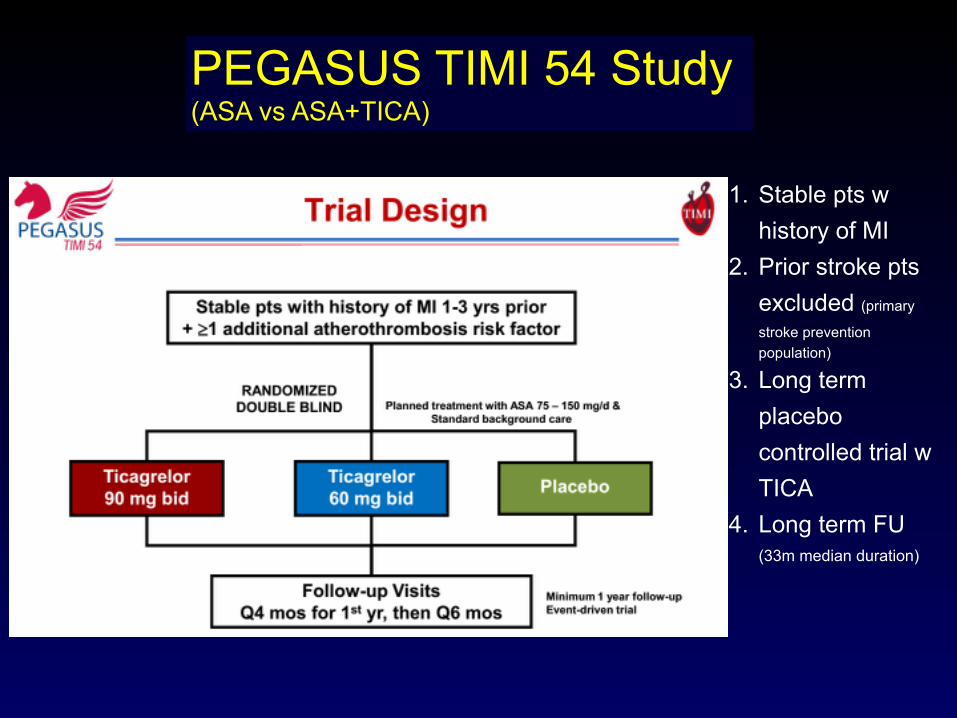
1. Stable pts w history of MI
2. Prior stroke pts excluded (primary
stroke prevention population)
3. Long term placebo controlled trial w TICA
4. Long term FU (33m median duration)
PEGASUS TIMI 54 Study (ASA vs ASA+TICA)
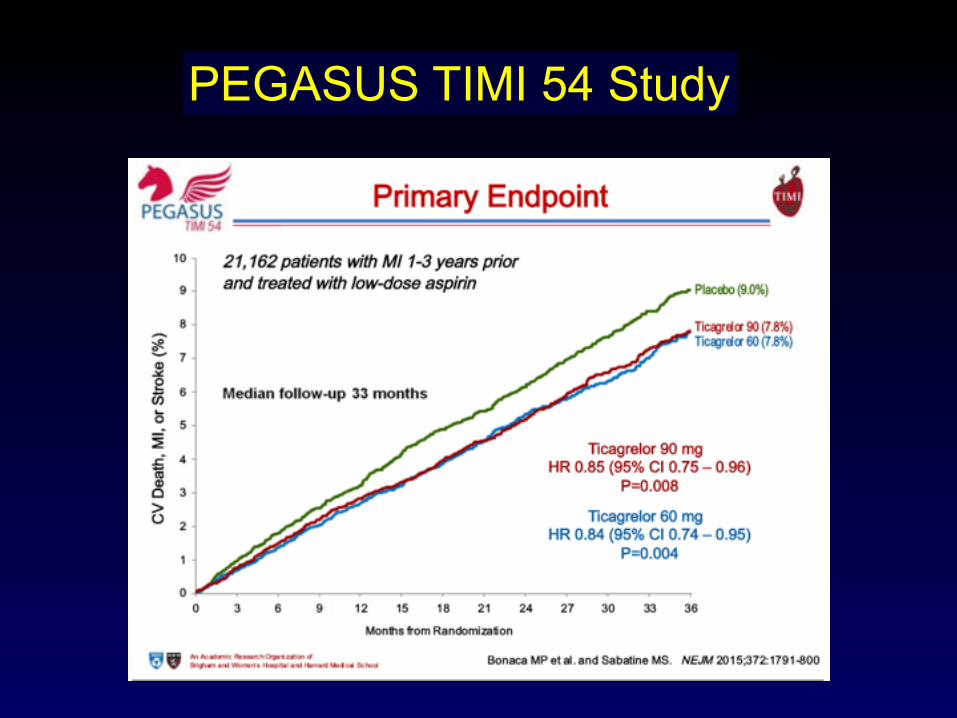
PEGASUS TIMI 54 Study
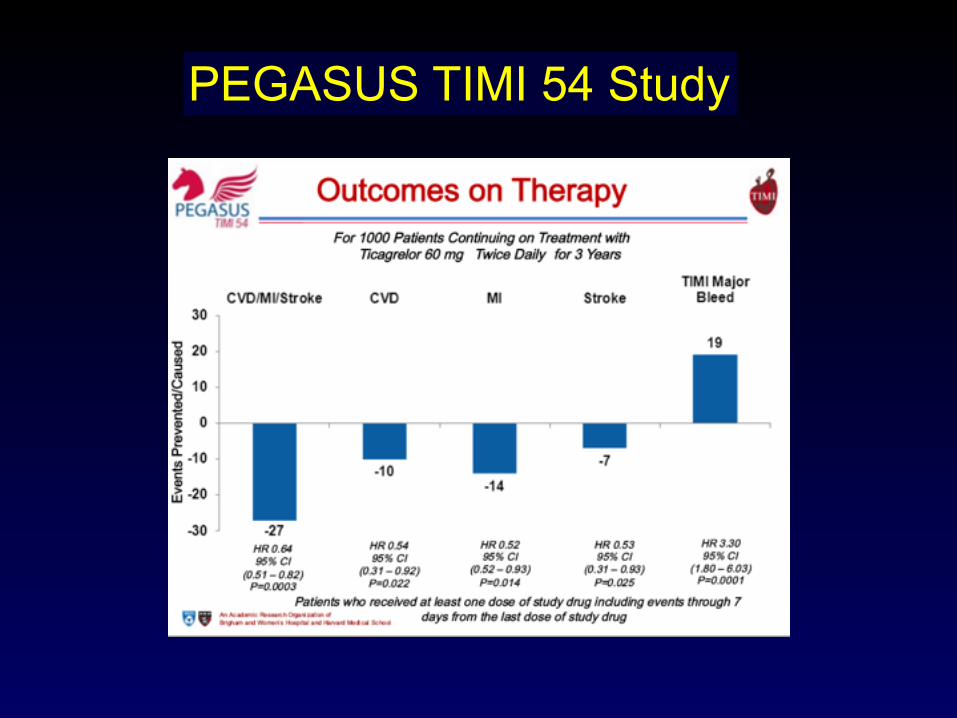
PEGASUS TIMI 54 Study
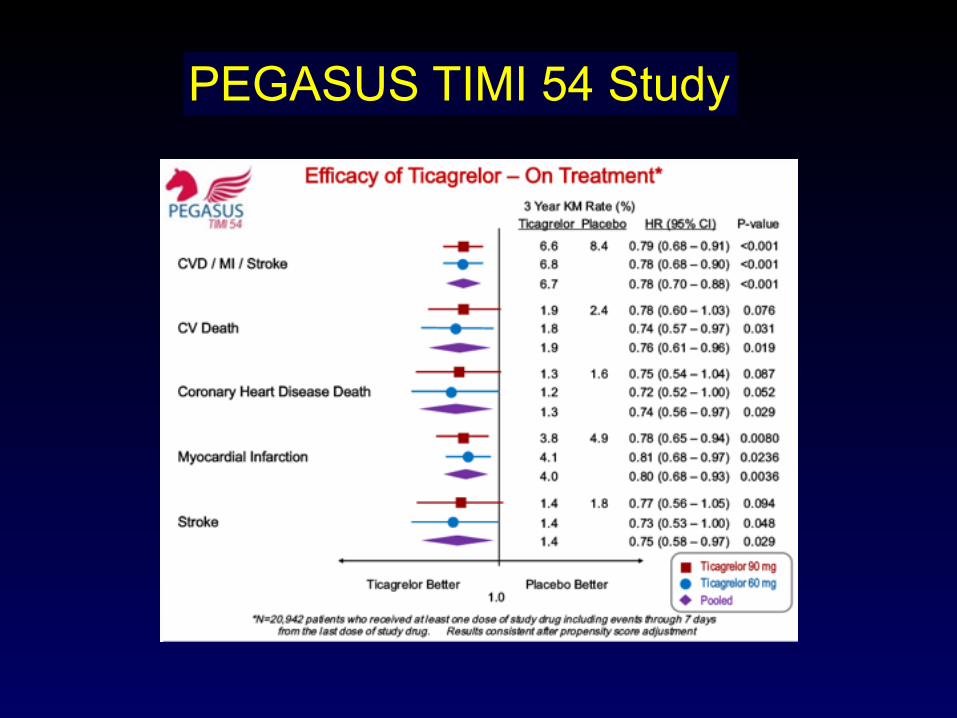
PEGASUS TIMI 54 Study
PEGASUS TIMI 54 Study

PRAGUE-18ANTARCTIC
PEGASUS TIMI 54CHAMPION PHOENIX
DOCTORSBBK II
EROSIONNORSTENTCE-MARC II

STEMI PPCI: on-hours (07.00-19.00) off-hours (19.00-07.00, weekends, holidays)
stent
throm
bosis
, all-c
ause
mor
tality
, isc
hemi
a-dr
iven r
evas
cular
izatio
n at 4
8h
DOCTORS Study
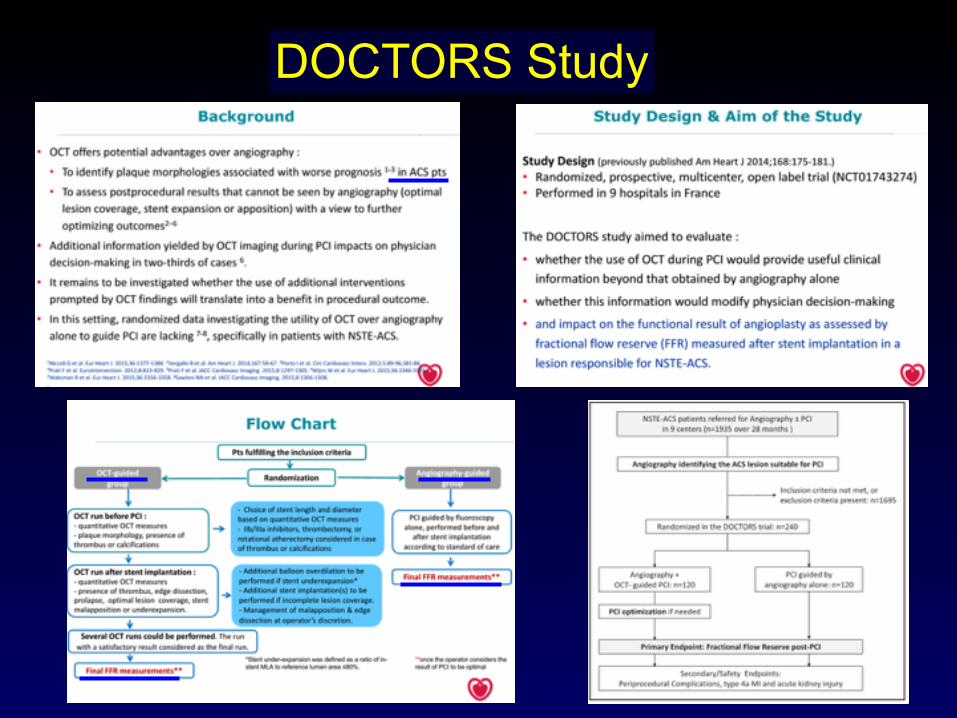
DOCTORS Study
DOCTORS Study
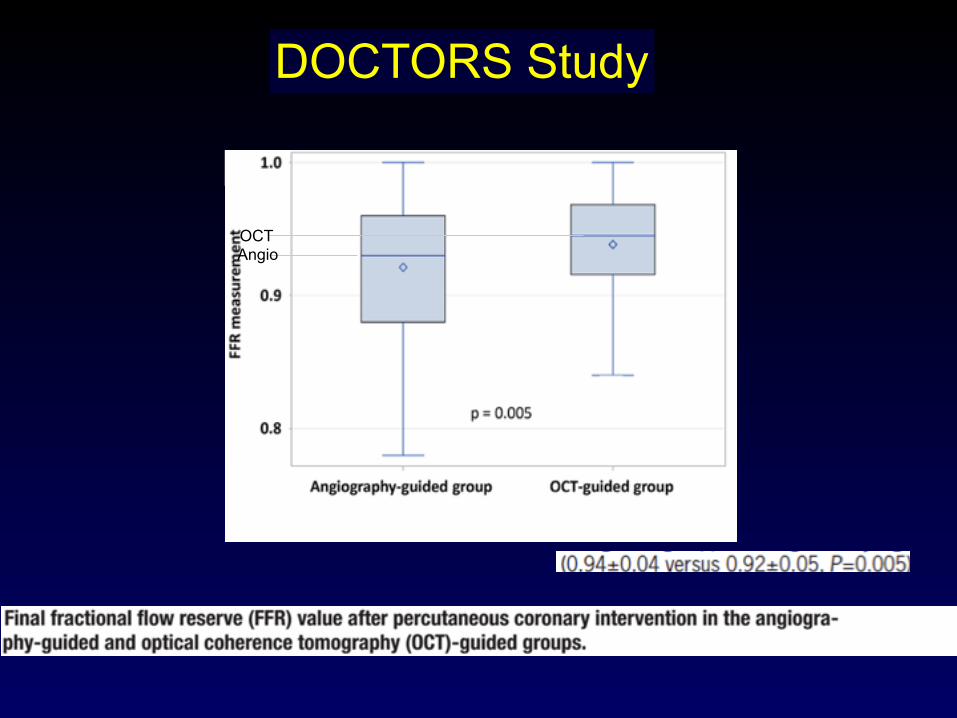
OCTAngio
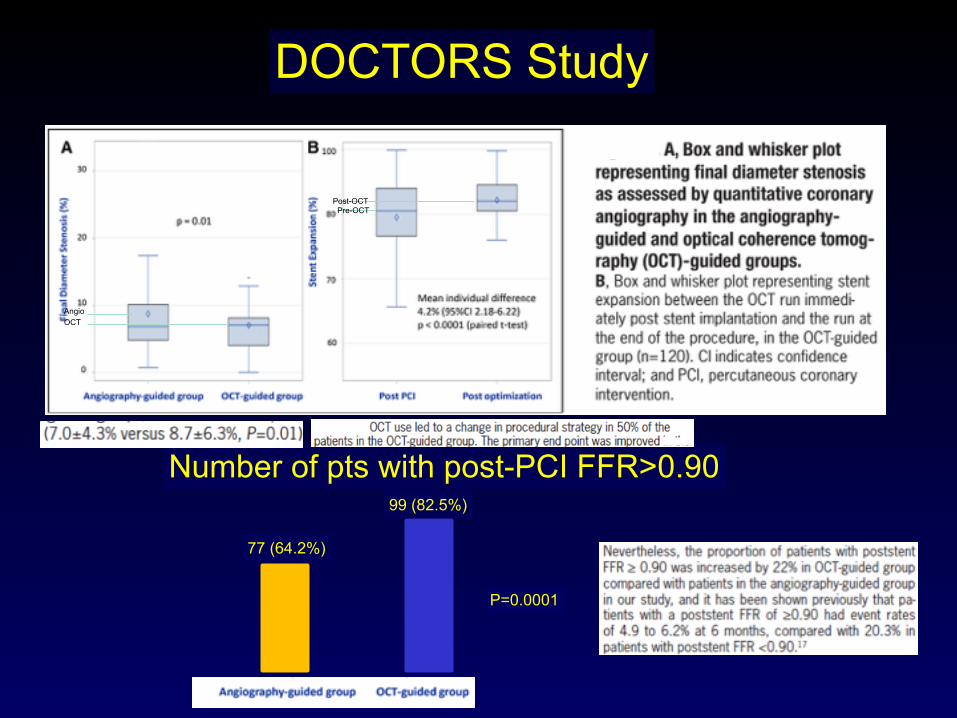
DOCTORS Study
Number of pts with post-PCI FFR>0.90
77 (64.2%)
99 (82.5%)
P=0.0001
OCTAngio
Post-OCTPre-OCT
DOCTORS Study
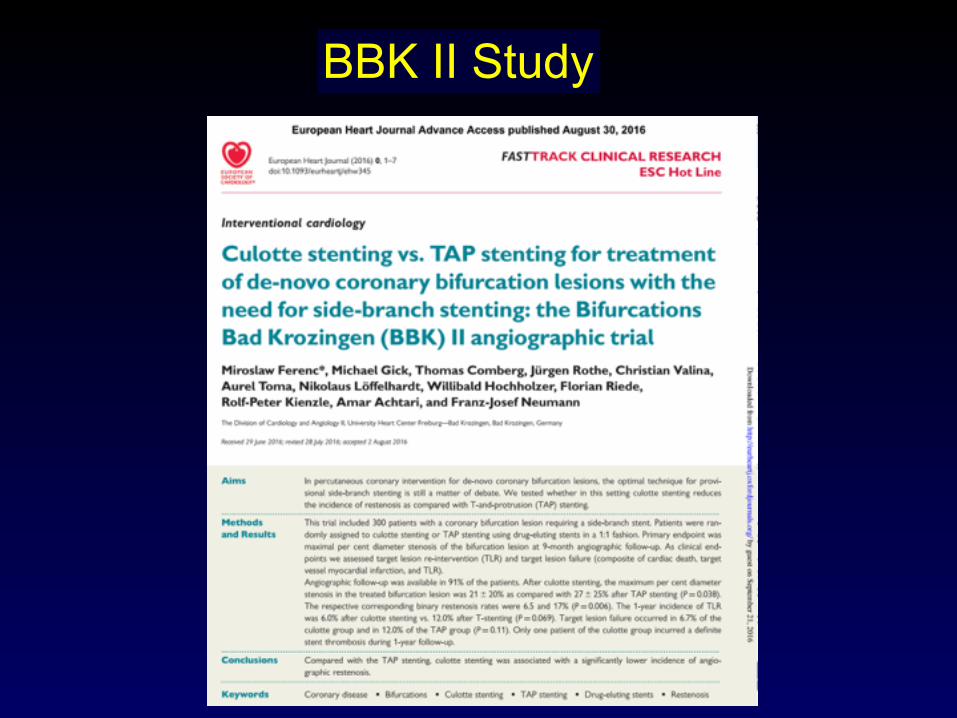
BBK II Study
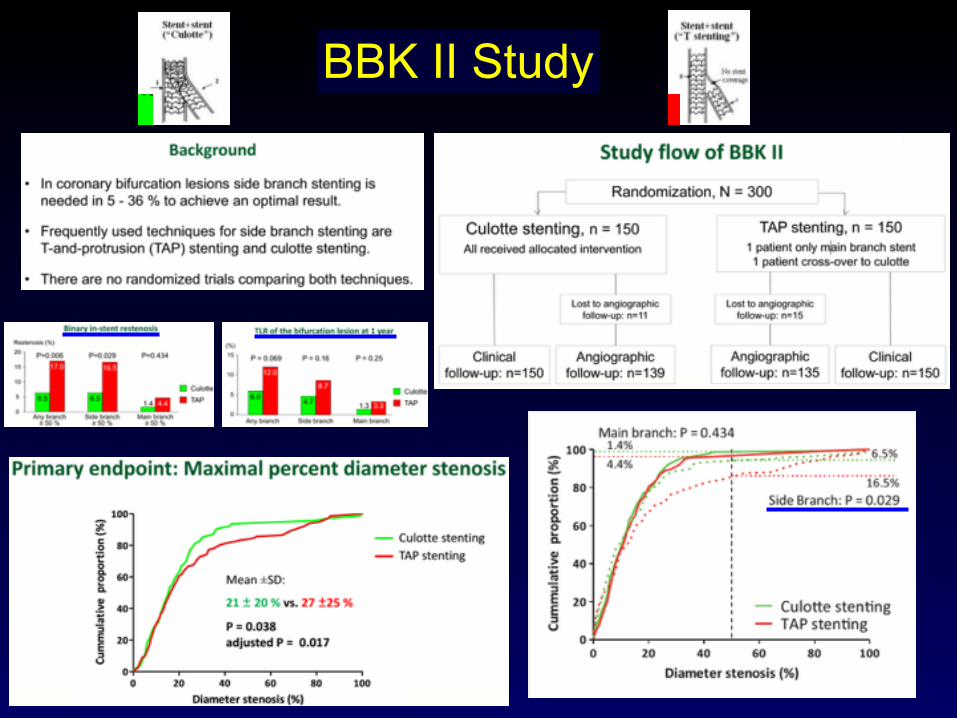
BBK II Study
BBK II Study
EROSION Study
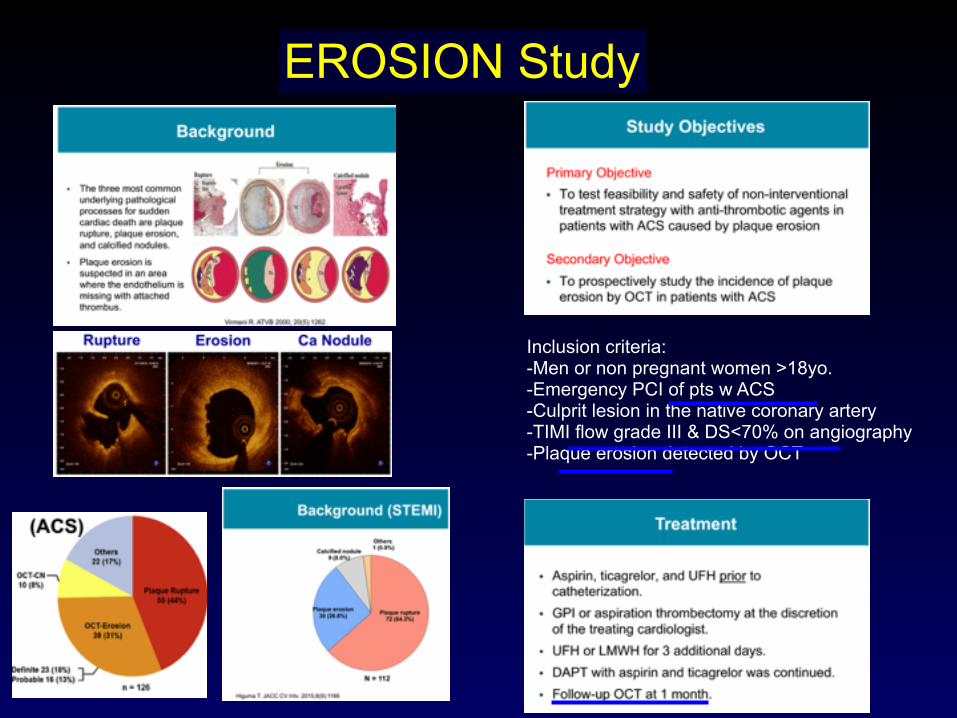
EROSION Study
Inclusion criteria: -Men or non pregnant women >18yo. -Emergency PCI of pts w ACS -Culprit lesion in the native coronary artery -TIMI flow grade III & DS<70% on angiography -Plaque erosion detected by OCT
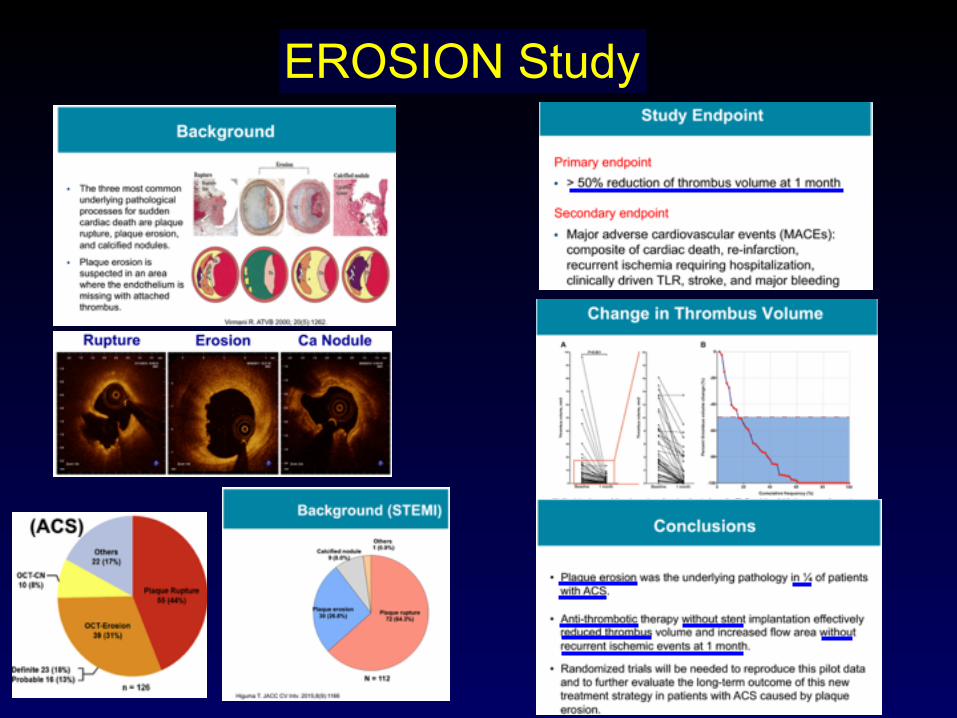
EROSION Study
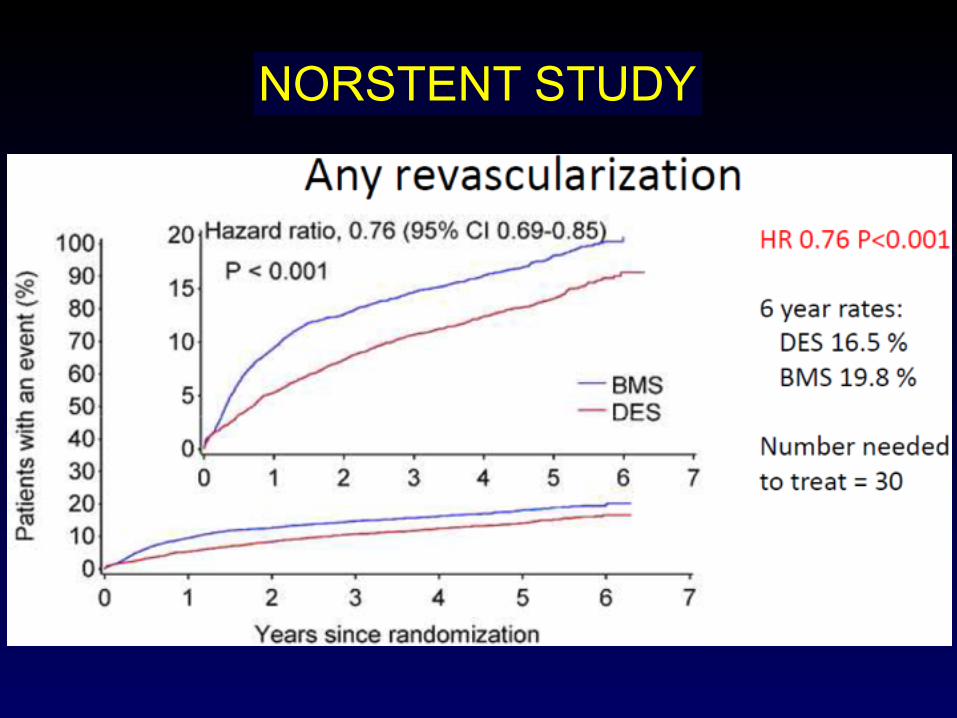
NORSTENT STUDY
NORSTENT STUDY
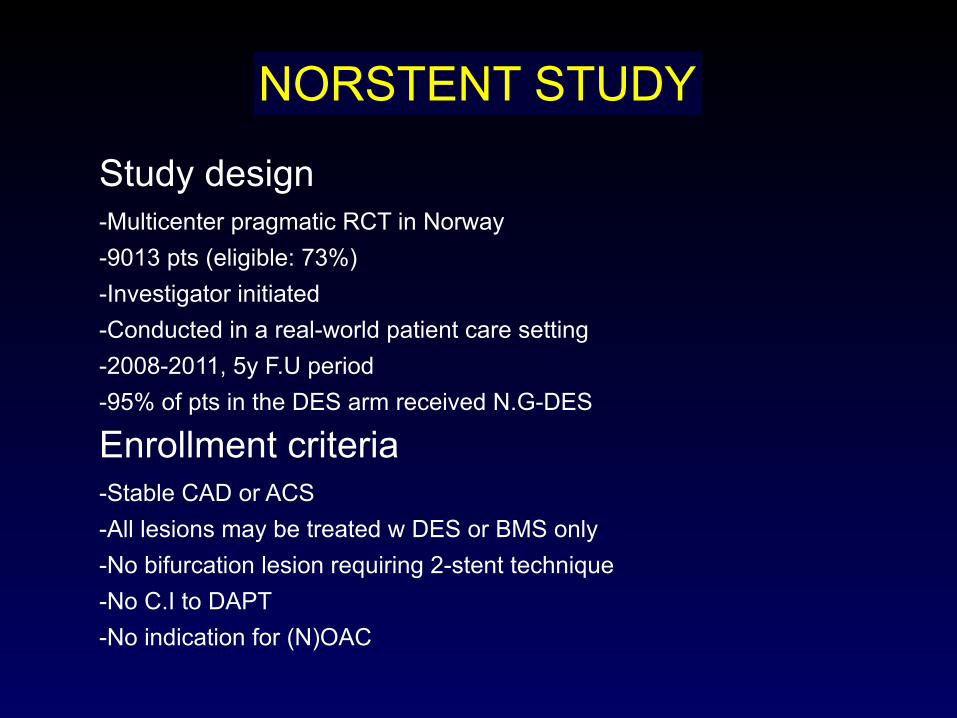
Study design -Multicenter pragmatic RCT in Norway -9013 pts (eligible: 73%) -Investigator initiated -Conducted in a real-world patient care setting -2008-2011, 5y F.U period -95% of pts in the DES arm received N.G-DES
Enrollment criteria -Stable CAD or ACS -All lesions may be treated w DES or BMS only -No bifurcation lesion requiring 2-stent technique -No C.I to DAPT -No indication for (N)OAC
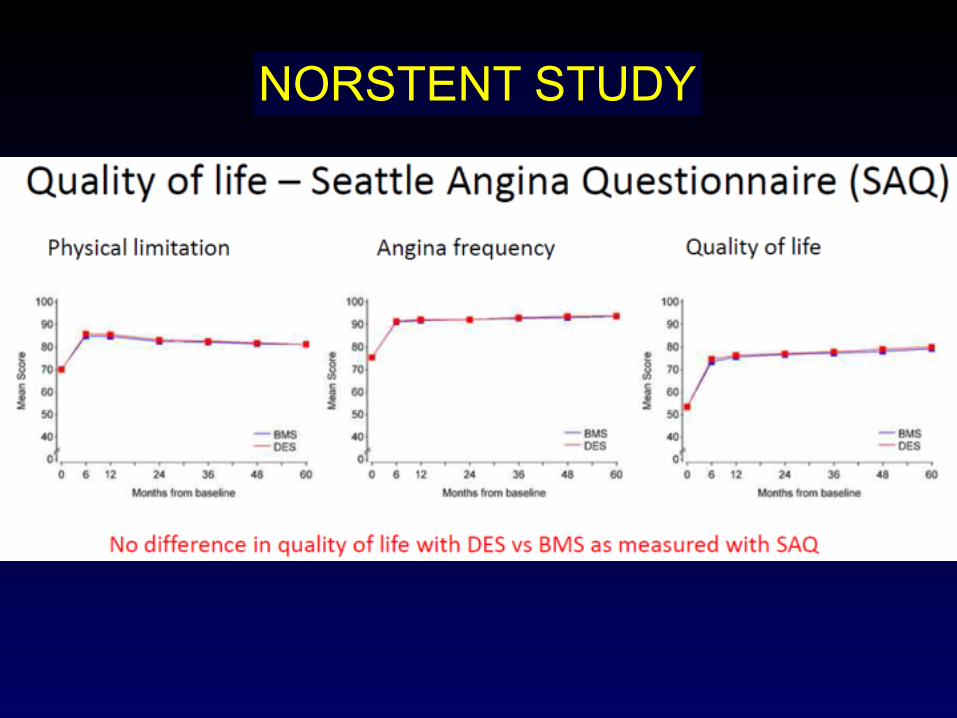
NORSTENT STUDY
NORSTENT STUDY
NORSTENT STUDY
NORSTENT STUDY
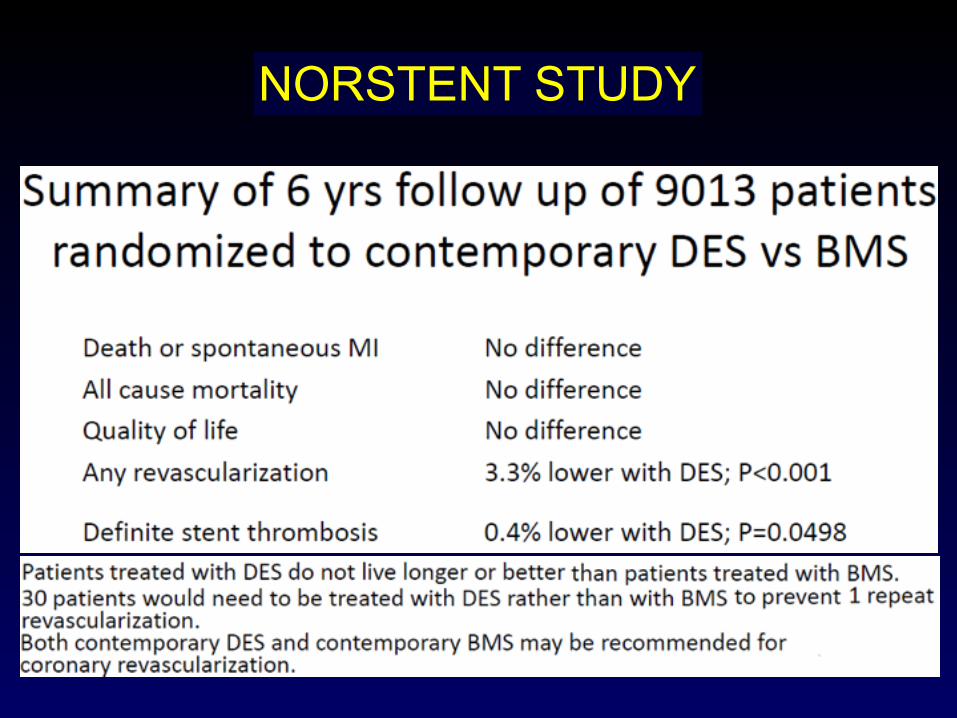
NORSTENT STUDY
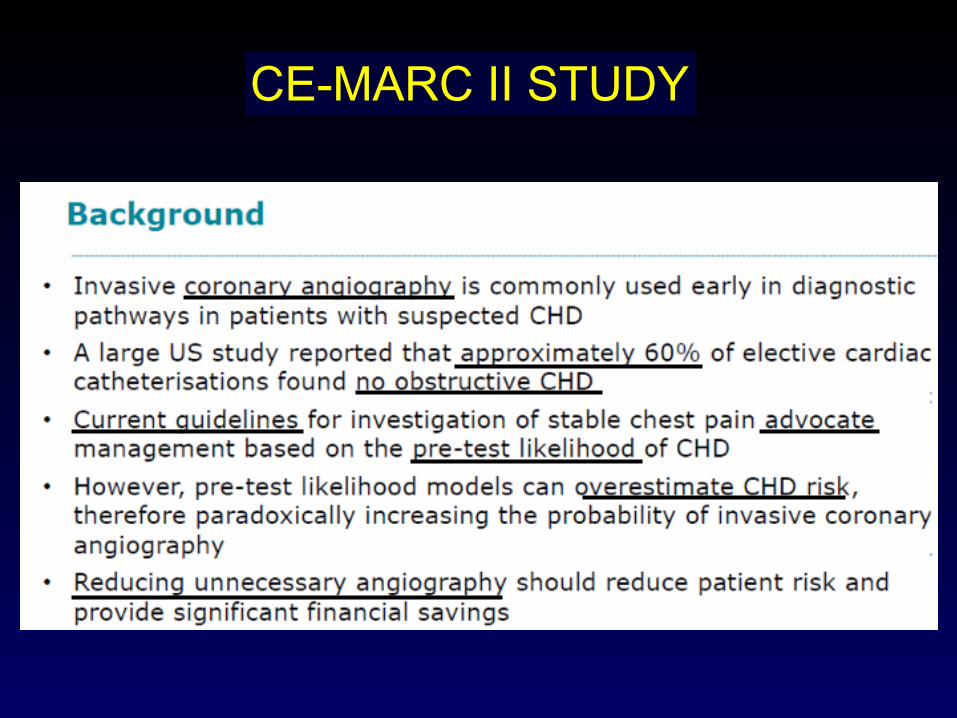
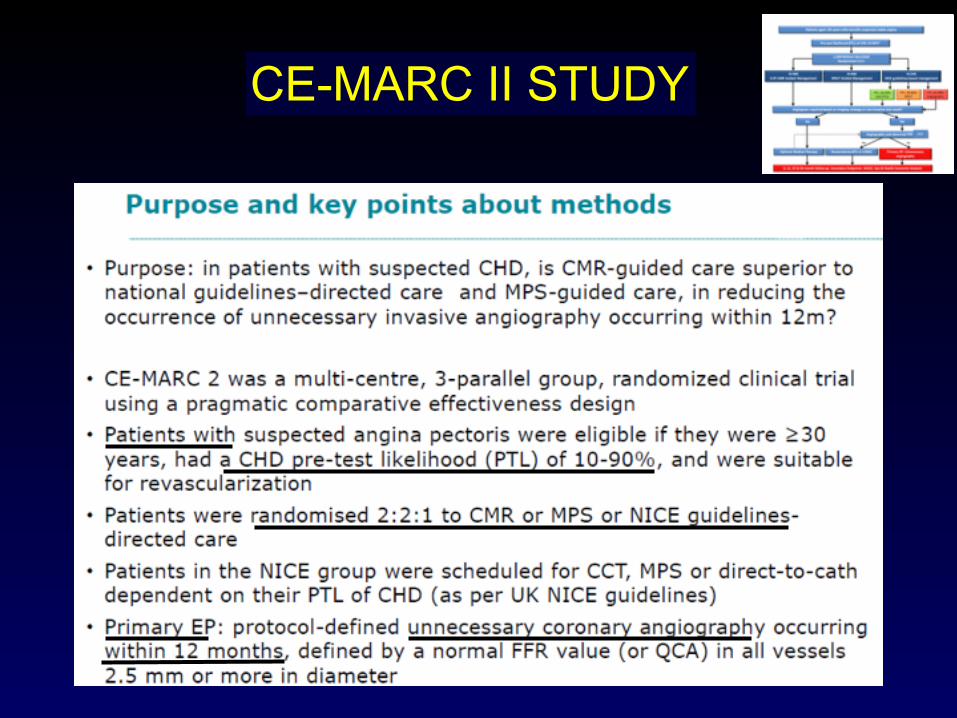
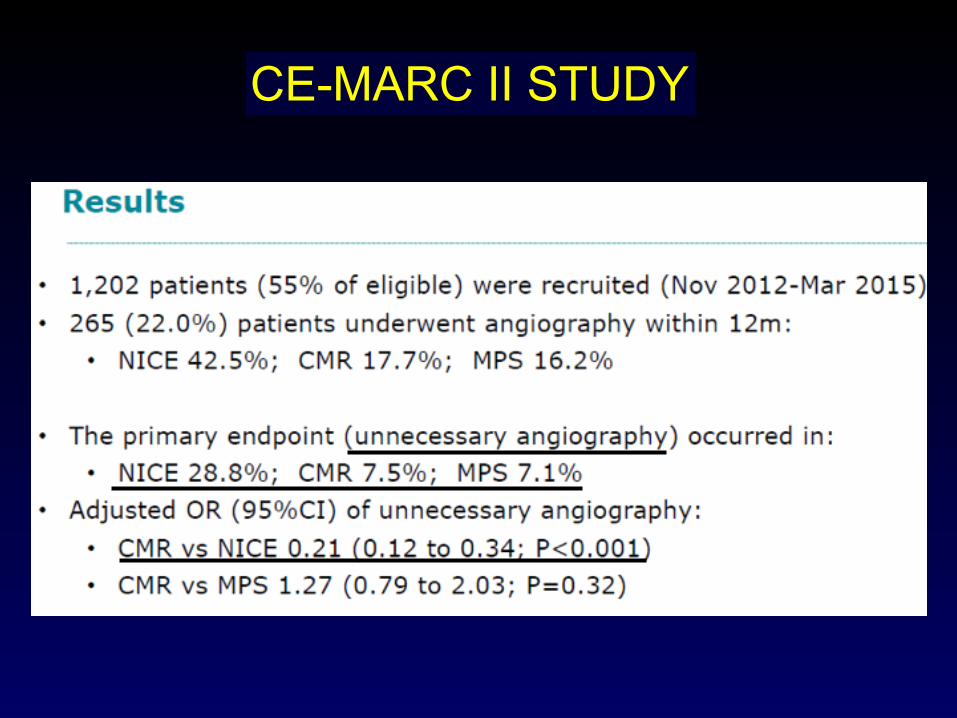
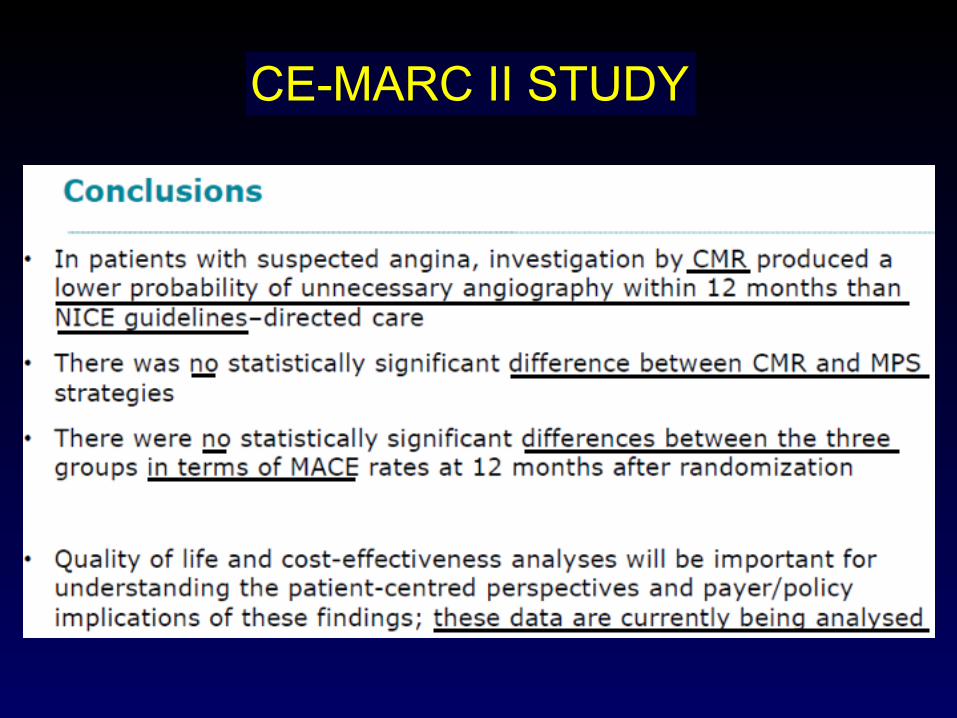
CE-MARC II STUDY
JAMA. 2016;316(10):1051-1060
CMR: Cardiovascular Magnetic Resonance NICE: National Institute for health & Care Excellence MPS: Myocardial Perfusion Scintigraphy
CE-MARC II STUDY
CE-MARC II STUDY
CE-MARC II STUDY

CE-MARC II STUDY
CE-MARC II STUDY
TAVI in Intermediate-Risk Patients
Lancet 2016;387:2218-25 N Engl J Med 2016;374:1609-20
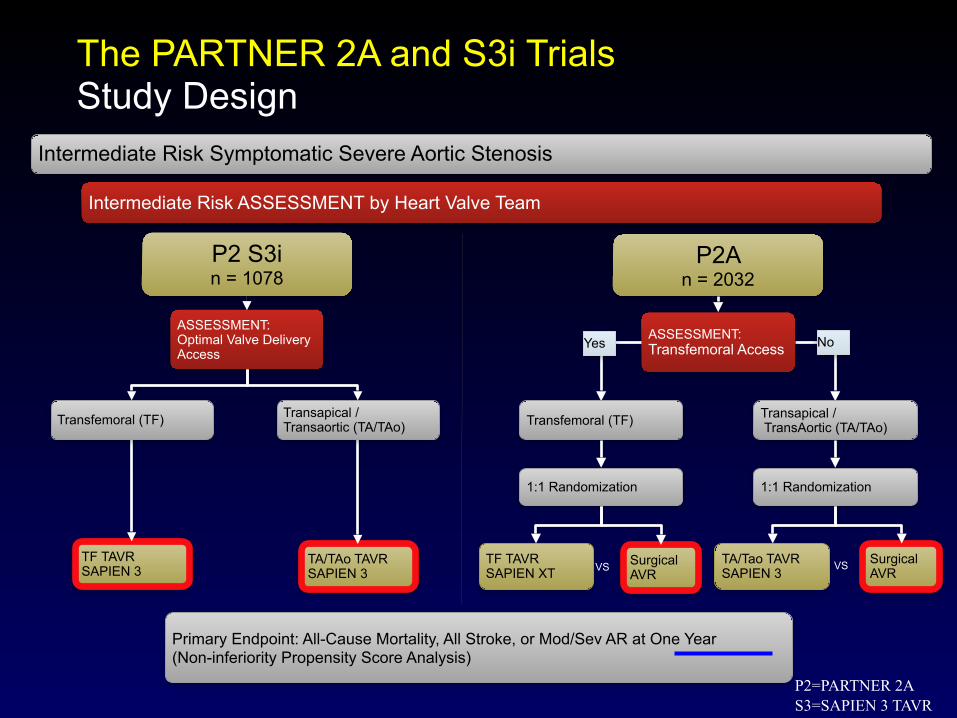
Intermediate Risk Symptomatic Severe Aortic Stenosis
Intermediate Risk ASSESSMENT by Heart Valve Team
TF TAVR SAPIEN 3
TA/TAo TAVR SAPIEN 3
P2 S3i n = 1078
ASSESSMENT: Optimal Valve Delivery Access
Transapical / Transaortic (TA/TAo)Transfemoral (TF)
Surgical AVR
Surgical AVR
P2A n = 2032
ASSESSMENT: Transfemoral Access
Transapical / TransAortic (TA/TAo)Transfemoral (TF)
1:1 Randomization1:1 Randomization
Yes No
TF TAVR SAPIEN XT VS VSTA/Tao TAVR
SAPIEN 3
Primary Endpoint: All-Cause Mortality, All Stroke, or Mod/Sev AR at One Year (Non-inferiority Propensity Score Analysis)
The PARTNER 2A and S3i TrialsStudy Design
P2=PARTNER 2A S3=SAPIEN 3 TAVR
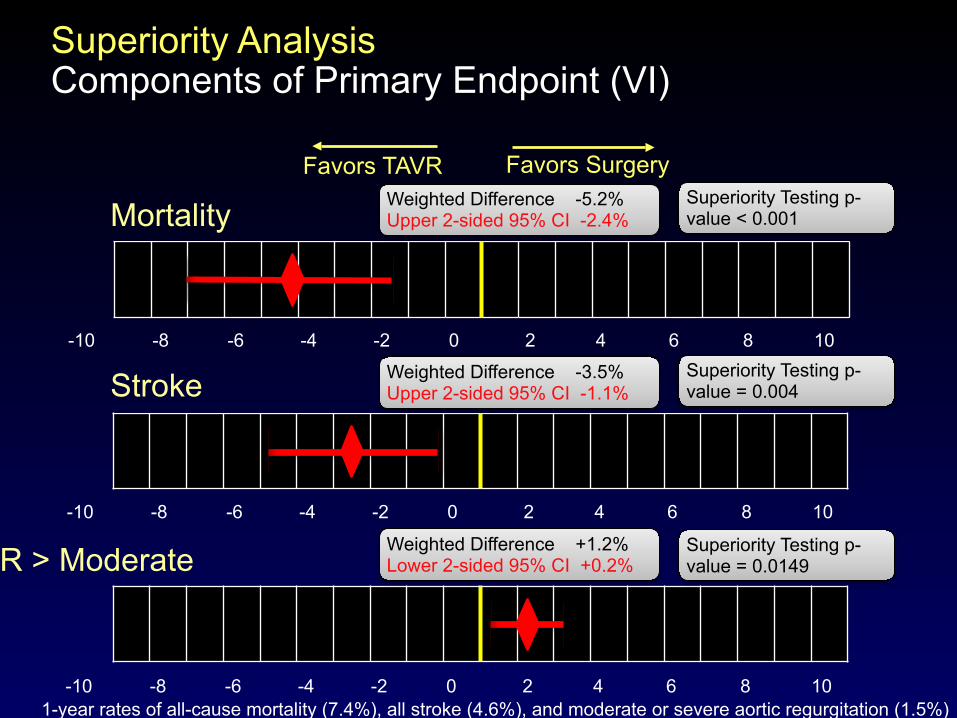
-10 -8 -6 -4 -2 0 2 4 6 8 10
Favors TAVR Favors Surgery
Superiority AnalysisComponents of Primary Endpoint (VI)
-10 -8 -6 -4 -2 0 2 4 6 8 10
-10 -8 -6 -4 -2 0 2 4 6 8 10
Stroke
Mortality
AR > Moderate
Weighted Difference -5.2% Upper 2-sided 95% CI -2.4%
Superiority Testing p-value < 0.001
Weighted Difference +1.2% Lower 2-sided 95% CI +0.2%
Superiority Testing p-value = 0.0149
Weighted Difference -3.5% Upper 2-sided 95% CI -1.1%
Superiority Testing p-value = 0.004
1-year rates of all-cause mortality (7.4%), all stroke (4.6%), and moderate or severe aortic regurgitation (1.5%)
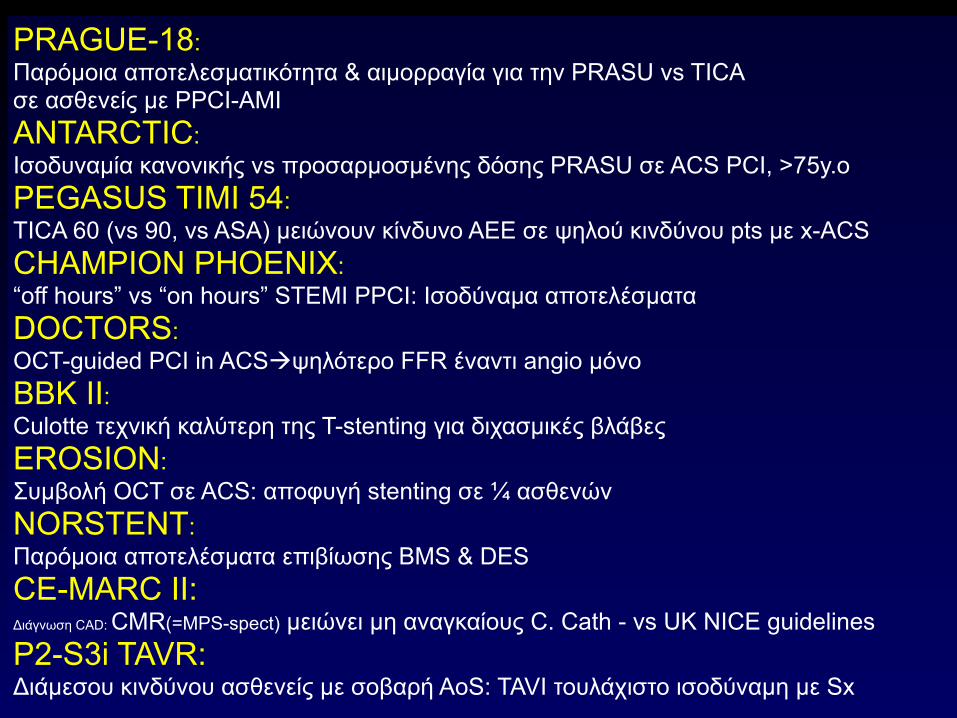
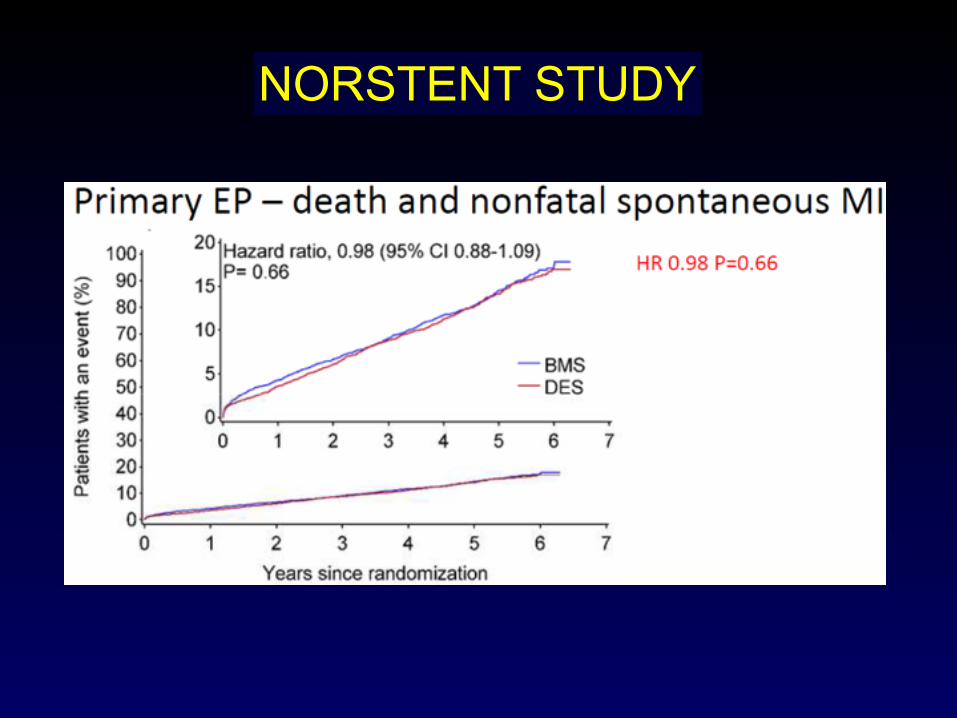
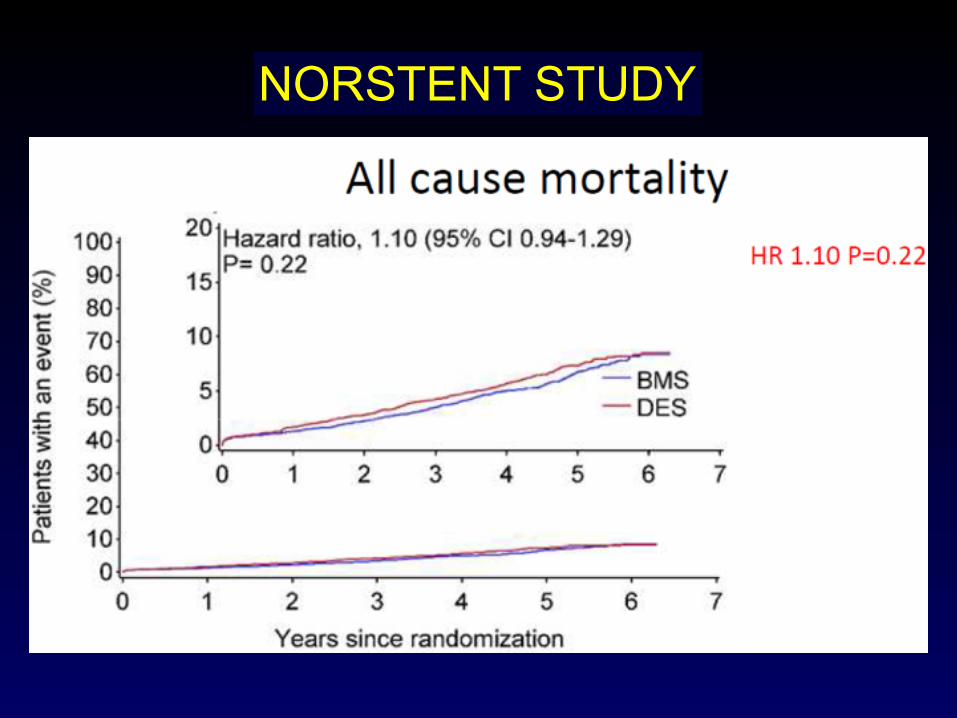
PRAGUE-18: Παρόµοια αποτελεσµατικότητα & αιµορραγία για την PRASU vs TICA σε ασθενείς µε PPCI-AMI ANTARCTIC: Ισοδυναµία κανονικής vs προσαρµοσµένης δόσης PRASU σε ACS PCI, >75y.o PEGASUS TIMI 54: TICA 60 (vs 90, vs ASA) µειώνουν κίνδυνο ΑΕΕ σε ψηλού κινδύνου pts µε x-ACS CHAMPION PHOENIX: “off hours” vs “on hours” STEMI PPCI: Ισοδύναµα αποτελέσµατα DOCTORS: OCT-guided PCI in ACS!ψηλότερο FFR έναντι angio µόνο BBK II: Culotte τεχνική καλύτερη της T-stenting για διχασµικές βλάβες EROSION: Συµβολή OCT σε ACS: αποφυγή stenting σε ¼ ασθενών NORSTENT: Παρόµοια αποτελέσµατα επιβίωσης BMS & DES
CE-MARC II: Διάγνωση CAD: CMR(=MPS-spect) µειώνει µη αναγκαίους C. Cath - vs UK NICE guidelines P2-S3i TAVR: Διάµεσου κινδύνου ασθενείς µε σοβαρή AoS: TAVI τουλάχιστο ισοδύναµη µε Sx
TCT 2016 Late-breaking Trials First Reports
• SENTINEL • PARTNER II QUALITY OF LIFE • PARTNER I FIVE-YEAR ECHO • RESPECT• COLOR• PLATINUM DIVERSITY • ReACT • ILLUMENATE U.S• WATCHMAN US POST-APPROVAL STUDY• AMULET OBSERVATIONAL STUD • PRISON IV • TOSCA-5 • TRANSFORM-OCT • RIBS VI
(Oct. 29 – Nov. 2, 2016 - Washington, D.C)
• ILUMIEN III (OPTIMIZE PCI) • BIO-RESORT (TWENTE III) • BIONICS • ABSORB China • ABSORB II • LEADERS FREE • EXCEL • NOBLE • REVELUTION • FANTOM II• MeRes-1 • FORTITUDE• FUTURE-I

Thank U!