1 Drugs used to treat diabetes mellitus Ján Mojžiš Department of Pharmacology Ján Mojžiš...
38
1 Drugs used to treat diabetes mellitus Ján Mojžiš Department of Pharmacology
-
Upload
benjamin-douglas -
Category
Documents
-
view
234 -
download
1
Transcript of 1 Drugs used to treat diabetes mellitus Ján Mojžiš Department of Pharmacology Ján Mojžiš...

1
Drugs used to treat diabetes mellitus
Ján Mojžiš
Department of Pharmacology
Ján Mojžiš
Department of Pharmacology
2
INSULIN AND ORAL HYPOGLYCEMIC DRUGS
Pancreas - endocrine gland (peptide hormones insulin, glucagon, and somatostatin) and exocrine gland (digestive enzymes). Peptide hormones - from cells Langerhans isletsβ or B-cells -insulinα2 or A-cells – glucagonα1 or D-cells - somatostatin
Hormones play an important role in regulating the metabolic activities of the body, particularly the homeostasis of blood glucose.
3
Metabolic roles of insulin and glucagon:
High serum glucose insulin release from beta cells of the pancreas.
Increased serum insulin lower blood glucose levels by driving carbohydrate into cells.
Low serum glucose in insulin and glucagon.
Elevated serum glucagon mobilization of energy storage forms. Used to fuel gluconeogenesis in the liver, producing glucose.
Somatostatin - regulates the secretion of insulin and glucagon within the islets).
4
DIABETES MELLITUS
Rapidly growing incidence - 135 million people worldwide are afflicted with Type 2
Diabetes is not a single disease - it is a heterogeneous group of syndromes characterized by an elevation of blood glucose caused by a relative or absolute deficiency of insulin.
Insulin-dependent diabetes mellitus (Type 1), and non-insulin-dependent diabetes mellitus (Type 2).
5
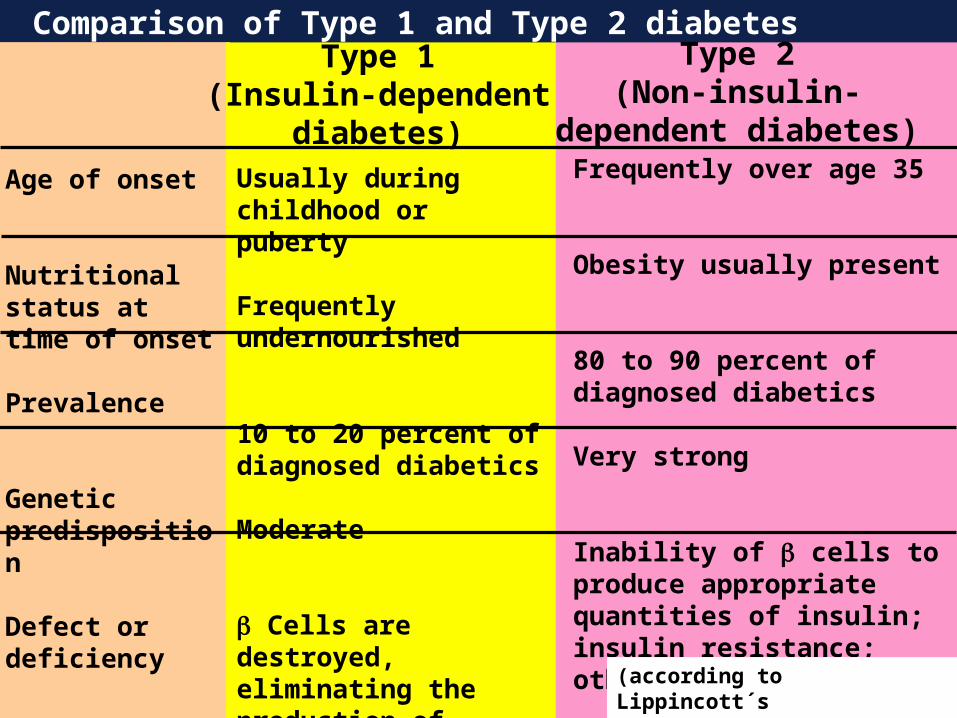
Comparison of Type 1 and Type 2 diabetes
Age of onset
Nutritional status at time of onset
Prevalence
Genetic predisposition
Defect or deficiency
Type 1(Insulin-dependent
diabetes)
Type 2(Non-insulin-
dependent diabetes)
Usually during childhood or puberty
Frequently undernourished
10 to 20 percent of diagnosed diabetics
Moderate
Cells are destroyed, eliminating the production of insulin
Frequently over age 35
Obesity usually present
80 to 90 percent of diagnosed diabetics
Very strong
Inability of cells to produce appropriate quantities of insulin; insulin resistance; other defects
(according to Lippincott´s Pharmacology, 2006

6
Summary of hypoglycemic agents HYPOGLYCEMIC DRUGS
INSULIN
ORAL HYPOGLYCEMIC DRUGS
-GLUCOSIDASE INHIBITORS
GASTROINTESTINALHORMONES
Aspart insulinExtended zinc insulinGlargine insulinGlulisine insulinInsulin zinc suspensionLispro insulinNPH insulin suspensionProtamine zinc insulinSemilente insulinUltralente insulin
GlipizideGlimepirideGlyburideMetforminNateglinidePioglitazoneRepaglinideRosiglitazoneTolbutamideTroglitazone
AcarboseMiglitol
Exenatide
7
Type 1 diabetes
Treatment:
Exogenous (injected) insulin to control hyperglycemia, avoid ketoacidosis, and maintain acceptable levels of glycosylated hemoglobin (HbA1c).
to maintain blood glucose as close to normal as possible, and to avoid wide swings in their levels (that contribute to long-term complications).
Pancreas transplantation; transplantation of islet cells - also under investigation.
8
Type 2 diabetes Treatment:
To maintain blood glucose within normal limits and to prevent the development of complications.
Weight reduction, exercise, dietary modification - decrease insulin resistance and correct the hyperglycemia in some patients.
Mostly dependent on oral hypoglycemic agents. As the disease progresses, b-cell function declines, and insulin therapy is often required to achieve satisfactory serum glucose levels.

9
Major factors contributing to hyperglycemia observed in Type 2 diabetes
1 Insulin resistance in peripheral tissues
2 Inadequate insulin secreation from cells
PANCREAS
Insulin
ADIPOSETISSUE
MUSCLE
Glucose
LIVER
Increased productionof glucose
Decreasedglucose uptake
10
INSULIN AND ITS ANALOGS
polypeptide hormone; two peptide chains connected by disulfide bonds. Synthesized as a precursor (pro-insulin) proteolytic cleavage insulin and peptide C - both are secreted by b-cells.
Sources: Human insulin - replaced I. from beef or pork pancreas. By recombinant DNA technology - special strains of E. coli or yeast
Modifications of amino acid sequence different pharmacokin. properties:lispro, aspart - faster onset and shorter duration of action than regular insulin (they do not aggregate or form complexes). glargine, detimir - long-acting, prolonged, flat levels of the hormone following a single injection.
11
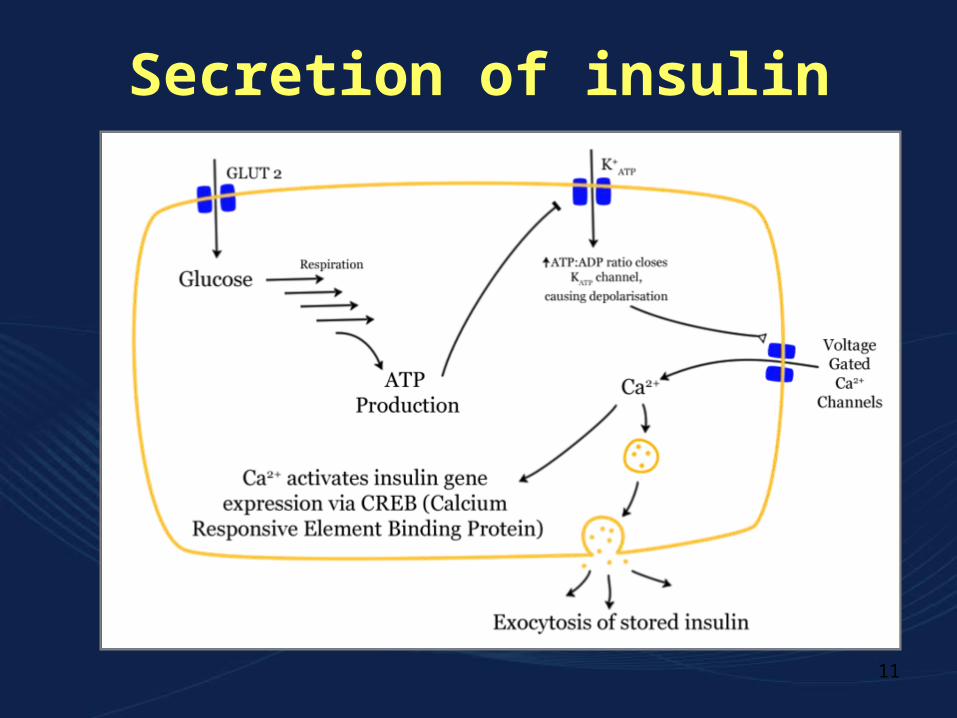
Secretion of insulin

12
Administration
Polypeptide degraded in GIT if taken orally mostly by subcutaneous injection (in a hyperglycemic emergency, regular insulin intravenously
Continuous s.c. infusion also - it does not require multiple injections.
Aerosol preparation (inhaled and absorbed in the deep lung) or oral spray (absorbed through the buccal mucosa) - in trials
13
Adverse reactions to insulin
-Hypoglycemia - the most serious and common adverse reactions to an overdose
-Lipodystrophy (less common with human insulin)
- Allergic reactions (less common with human insulin)
14
A. Rapid-onset and short-acting preparations
Regular insulin - short-acting, soluble, crystalline zinc insulin. Usually s.c. (i.v. in emergencies); rapidly blood sugar. Safely used in pregnancy
Effect - within 30 min; peaks between 2 - 3 hours after s.c. injection; lasts 5-8 hours. When administered at mealtime, the blood glucose rises faster than the insulin with resultant early postprandial hyperglycemia and an increased risk of late postprandial hypoglycemia should be injected 30-45 or more min before the meal to minimize the mismatching.
15
Rapid-acting insulin
Three injected rapid-acting insulin analogs: lispro, aspart, and glulisine, are commercially available.
- their rapid onset and early peak action more closely mimic normal endogenous prandial insulin secretion than regular insulin- additional benefit: allowing insulin to be taken immediately before the meal without sacrificing glucose control.
Duration of action is rarely more than 3-5 hours

16
B. Intermediate-acting insulin preparations
1. Lente insulin:
Amorphous precipitate of insulin with zinc ion
Onset and peak effect - slower than in regular insulin, but are sustained for a longer period. Not suitable for i.v.
2. Neutral protamine Hagedorn (NPH)
- suspension of crystalline zinc insulin combined with polypeptide, protamine.
Intermediate duration of action
Onset cca 2-5 hours; duration of 4-12 hours
Only s.c. (never i.v.).

17
C. Prolonged-acting insulin preparations
1. Ultralente insulin (extended zinc insulin): Suspension of zinc insulin crystals in acetate buffer large particles that are slow to dissolve slow onset of action and long-Iasting effect
2. Insulin glargine (GLAR geen): Precipitation at the injection site longer action.
Slower onset than NPH insulin; flat, prolonged hypoglycemic effect (i.e., it has no peak ). Slow onset of action (1-1.5 hours); maximum effect after 4-6 hours. This maximum activity is maintained for 11-24 hours or longer.
Must be given s.c.
18
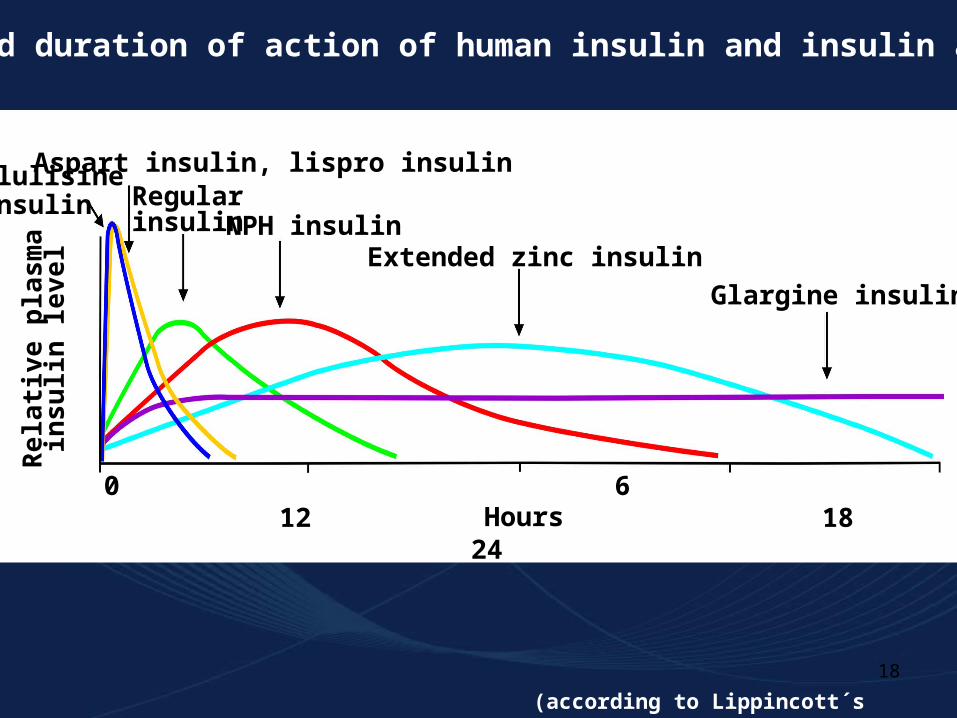
Onset and duration of action of human insulin and insulin analogs.
0 6 12 18 24 Hours
Rel
ativ
e pl
asm
a in
sulin
leve
l
Glulisine insulin
Aspart insulin, lispro insulinRegular insulin NPH insulin
Extended zinc insulin
Glargine insulin
(according to Lippincott´s Pharmacology, 2006)

19
Patients with type 1 DM
Soluble insulin is used (i.v.) in emergency treatment of hyperglycaemic diabetic emergencies (e.g. diabetic ketoacidosis).
Many patients with type 2 DM ultimately require insulin treatment.
Short-term treatment of patients with type 2 DM or impaired glucose tolerance during intercurrent events (e.g. operations, infections, myocardial infarction).
During pregnancy, for gestational diabetes not controlled by diet alone.
Clinical uses of insulin

20
ORAL HYPOGLYCEMIC AGENTS:
INSULIN SECRETAGOGUES
Useful in the treatment of Type 2 diabetes
The patient most likely to respond well to oral hypoglycemic agents is one who develops diabetes after age 40 and has had diabetes less than 5 years.
Patients with long-standing disease may require a combination of hypoglycemic drugs with or without insulin to control their hyperglycemia.

21
A. Sulfonylureas
they promote insulin release from the -cells
1. Mechanisms of action of the sulfonylureas: 1) stimulation of insulin release from the β-cells blocking the ATP-sensitive K+ channels, resulting in depolarization and Ca2+ influx; 2) reduction of serum glucagon levels; and 3) increasing binding of insulin to target tissues and receptors.
2. Pharmacokinetics and fate: Given orally; bind to serum proteins; metabolized by the liver; excreted by the liver or kidney. Tolbutamide has the shortest duration of action (6-12 hours),whereas the second-generation agents last about 24 hours.
1st generation: TOLBUTAMIDE (tole BYOO ta mide), CHLORPROPAMIDE (klor PROE pa mide), TOLAZAMIDE (tole AZ a mide), ACETOHEXAMIDE (a seat oh HEX a mide),
2nd generation: GLIBENCLAMIDE, GLYBURIDE (GLYE byoor ide) ; GLIPIZIDE (GLIP i zide), GLIMEPIRIDE
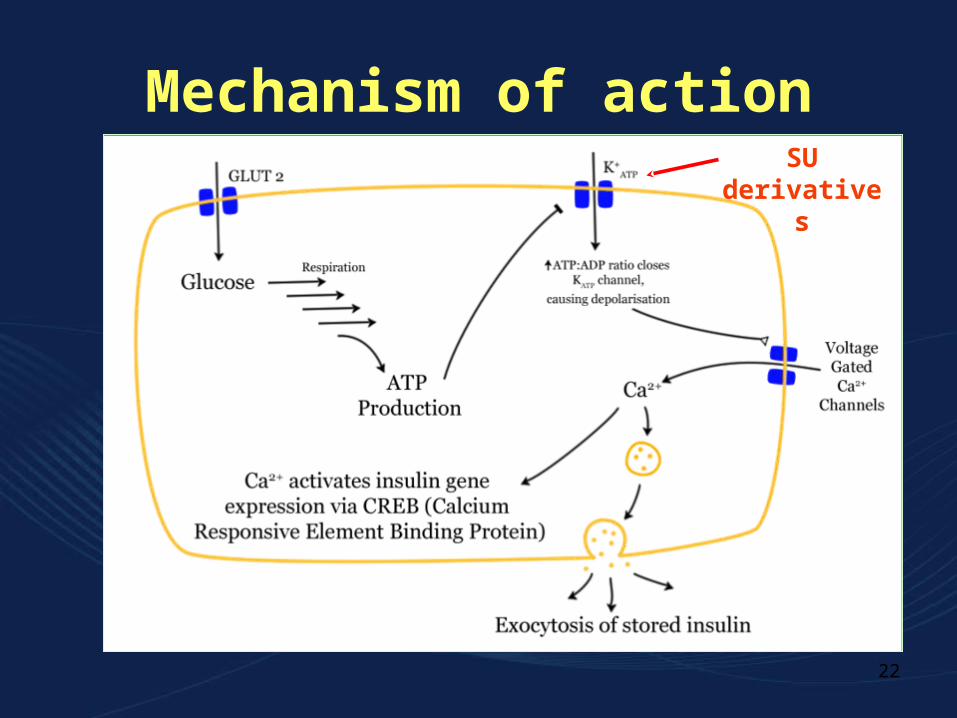
22
Mechanism of actionSU
derivatives
23
Administration, fate: given orally, metabolized by the liver, and excreted by the liver or kidney. Contraindicated in patients with hepatic or renal insuficiency (delayed excretion of the drug may cause hypoglycemia).
All bind strongly to plasma albumins »»» interactions with other drugs (e.g. salicylates, sulfonamides) which compete for binding sites »»» hypoglycaemia
Adverse effects:- hypoglycemia- disulfiram-like reactions (flushing, nausea, headache after alcohol)- allergic reactions- GIT disturbances - weight gain, hyperinsulinemia, and hypoglycemia

24
Drugs interacting with sulfonylurea drugs
Sulfonylureas
Sulfonylureas
Increased hypoglycemic actionof sulfonylurea drugs
Reduce hepatic metabolism of sulfonylureas
DicumarolChloramphenicol
Monoamine oxidase inhibitorsPnehylbutazone
ClofibratePhenylbutazone
SalicylatesSulfonamides
AllopurinolProbenecid
PhenylbutazoneSalicylates
Sulfonamides
Displace sulfonyl-ureas from plasma
protein
Decrease urinaryexcretion of
sulfonylureas ortheir metabolites
25
B. Meglitinide analogs
repaglinide - Although they are not sulfonylureas, they have common actions.
1. Mechanism of action: Action is dependent on functioning b-cells. They bind to a distinct site on the sulfonylurea receptor of ATP-sensitive K channels series of reactions culminating release of insulin.
In contrast to the sulfonylureas - they have a rapid onset and short duration of action.
Combined therapy with metformin or the glitazones - better than monotherapy with either agent in improving glycemic control.

26
3. Adverse effects:
- Hypoglycemia (incidence lower than with the sulfonylureas)
- Drugs that inhibit CYP3A4 (e.g., ketoconazole, itraconazole, fluconazole, erythromycin, and clarithromycin) may the glucose-lowering effect of repaglinide
- Drugs that increase levels of this enzyme (e.g., barbiturates, carbamazepine, rifampin) may have the opposite effect.
- Weight gain (less problem than with sulfonylureas)
- Use with caution in patients with hepatic impairment.
27
VI. ORAL HYPOGLYCEMIC AGENTS:
INSULIN SENSITIZERS
the biguanides and thiazolidinediones -improve insulin action. They lower blood sugar by improving target-cell response to insulin without increasing pancreatic insulin secretion.
28
A. BIGUANIDES (METFORMIN )
Orally acting, not influencing beta-cells or affecting insulin production.
It requires insulin for its action, but differs from the sulfonylureas in that it does not promote insulin secretion.
Hyperinsulinemia is not a problem the risk of hypoglycemia is far less than with sulfonylurea agents (it may occur if caloric intake is not adequate or exercise is not compensated for calorically).
29
1. Mechanism of action:
- Inhibition of hepatic gluconeogenesis
-Decrease of intestinal absorption of sugars.
- Increase sensitivity of peripheral tissues to insulin
Very important - ability to modestly reduce hyperlipidemia (LDL and VLDL cholesterol , and HDL ). These effects may not be apparent until 4-6 weeks of use. The patient often loses weight because of loss of appetite.
The only oral hypoglycemic agent proven to decrease cardiovascular mortality.
May be used alone or in combination with other agents, as well as with insulin. Hypoglycemia occurred when taken in combination.
not bound to serum proteins, and it is not metabolized

30
Adverse effects:
Largely GIT.
Contraindicated in diabetics with renal and/or hepatic disease, cardiac or respiratory insufficiency, a history of alcohol abuse, severe infection, or pregnancy.
Long-term use may interfere with vitamin B12 absorption.
A number of drug interactions (effects of metformin may be by cimetidine, furosemide, nifedipine, and oth'er agents).

31
B. Thiazolidinediones (or glitazones)
Insulin sensitizers - although insulin is required for their action, these drugs do not promote its release from the pancreatic b cells hyperinsulinemia does not result.
Troglitazone [TROE glit a zone] was the first,but was withdrawn after a number of deaths due to hepatotoxicity.
Presently, two members of this class are available, pioglitazone [pye oh GLI ta zone] and rosiglitazone [roe si GLI ta zone].
1. Mechanism of action: exact mechanism remains to be elucidated;
32
2. Pharmacokinetics: Both are absorbed well after oral administration; extensively bound to serum albumin (99,8%) .
Both undergo extensive metabolism by CYP450 isozymes.
Some metabolites of pioglitazone have activity. The metabolites are primarily excreted in the urine, but the parent agent leaves via the bile.
No dosage adjustment is required in renal impairment.
33
3. Adverse effects:
- deaths from hepatotoxicity after troglitazone liver enzyme levels be measured initially, then every 2 months for a year, and periodically thereafter.
- weight increase (possibly through the ability of TZDs to increase subcutaneous fat or due to fluid retention - it can lead to or worsen heart failure)
- headache and anemia
- Women taking oral contraceptives and TZDs may become pregnant, because the TZDs reduce plasma concentrations of the estrogen-containing contraceptives.

34
VII. ORAL HYPOGLYCEMIC AGENTS: a-GLUCOSIDASE INHIBITORS
A. Acarbose
1. Mechanism of action: Taken at the beginning of meals. They act by delaying the
digestion of carbohydrates glucose absorption. Effects by reversibly inhibiting membrane-bound a-glucosidase in the intestinal brush border.
This enzyme is responsible for the hydrolysis of oligosaccharides to glucose and other sugars (Acarbose also inhibits pancreatic a-amylase).
the postprandial rise of blood glucose is blunted.

35
2. Pharmacokinetics:
Acarbose is poorly absorbed; metabolized primarily by intestinal bacteria, some of the metabolites are absorbed and excreted into the urine.
3. Adverse effects:
- flatulence, diarrhea, and abdominal cramping.

36
Duration of action of some oral hypoglycemicagents
Tolbutamide
Glyburide
Glipizide
Glyburide
Nateglinide
Repaglinide
Metformin
Pioglitazone
Rosiglitazone
Acarbose
8 hrs
18 hrs
20 hrs
24 hrs
2 hrs
2 hrs
6 hrs
>24 hrs
>24 hrs
6 hrs
37
Type 2 DM, as a supplement to diet and exercise to reduce symptoms from hyperglycaemia (e.g. thirst, excessive urination).
Metformin is preferred for obese patients unless contraindicated by factor(s) that predispose to lactic acidosis (renal or liver failure, heart failure, hypoxaemia).
Acarbose reduces carbohydrate absorption; it causes flatulence and diarrhoea.
Drugs that act on the sulfonylurea receptor (e.g. tolbutamide, glibenclamide) - well tolerated but often promote weight gain.
Clinical uses of oral hypoglycaemic drugs
38
VIII. GASTROINTESTINAL HORMONES Oral glucose results in a higher secretion of insulin than occurs when an equal load of glucose is given intravenously. This effect is referred to as the "incretin effect," and is apparently reduced in Type 2 diabetes.
important role of GI hormones-notably glucagon-like peptide-1 (GLIP-1) and gastric inhibitory polypeptide-in the digestion and absorption of nutrients including glucose.
A new drug, exenatide – homolog of GLIP-1. It apparently mediates its effect through the GLIP-1 receptor, and it not only improves insulin secretion but also slows gastric emptying time, food intake, glucose suppression of glucagon secretion, and promotes b cell regeneration or decreased apoptosis. weight gain, postprandial hyperglycemia, and loss of b cells are reduced,