β1-adrenergic receptor polymorphisms and antihypertensive response to metoprolol
9
PHARMACOGENETICS AND GENOMICS 1 -Adrenergic receptor polymorphisms and antihypertensive response to metoprolol Objectives: Marked interpatient variability exists in blood pressure response to -blocker monotherapy. We tested the hypothesis that 2 common polymorphisms in the gene for 1 -adrenergic receptor are associated with antihypertensive response to metoprolol in patients with uncomplicated hypertension. Methods: Forty hypertensive men and women aged 35 to 65 years were studied. Baseline studies included 24-hour ambulatory blood pressure monitoring. Patients took 50 mg metoprolol twice daily with weekly titration to response or 200 mg twice daily. After a minimum of 4 weeks at stable dose, treatment phase 24-hour ambulatory blood pressure monitoring was repeated. The codon 49 and 389 genotypes for 1 - adrenergic receptor were determined by polymerase chain reaction with restriction fragment length polymor- phism. Multilinear regression was performed to determine the impact of genotype and other variables on blood pressure response to metoprolol. Results: Patients homozygous for Arg at codon 389 had a nearly 3-fold greater reduction in daytime diastolic blood pressure (13.3% 8.4% versus 4.5% 8.2%, P .0018) compared with those who carried the variant allele. The haplotype pair (diplotype) for 1 -adrenergic receptor was also a significant predictor of response, with patients having the Ser49Arg389/Ser49Arg389 diplotype demonstrating a decline in blood pressure of 14.7 mm Hg versus 0.5 mm Hg in patients with the Gly49Arg389/Ser49Gly389 diplotype. In multiregression analysis, baseline daytime diastolic blood pressure, codon 389 genotype, and codon 49 genotype were significant predictors of blood pressure after treatment. Conclusions: Our data suggest that 1 -adrenergic receptor polymorphisms are important determinants of antihypertensive response to metoprolol. In the future, codon 49 and 389 genotypes or 1 -adrenergic receptor haplotypes might be used to predict the diastolic blood pressure response to metoprolol in patients with hypertension. (Clin Pharmacol Ther 2003;74:44-52.) Julie A. Johnson, PharmD, Issam Zineh, PharmD, Brian J. Puckett, PharmD, Susan P. McGorray, PhD, Hossein N. Yarandi, PhD, and Daniel F. Pauly, MD, PhD Gainesville, Fla Affecting approximately 50 million Americans, hy- pertension is the most prevalent chronic disease in the United States and a major contributor to mortality and vascular morbidity. 1 The benefits of antihypertensive drug therapy on curtailing hypertension-related stroke, heart failure, and end-stage renal disease are well rec- ognized. Currently, -blockers are recommended first- line agents in the management of hypertension. 2 How- ever, marked variability in response exists, with adequate blood pressure (BP) control failing to be achieved with -blocker monotherapy in 30% to 60% of patients. 3,4 The factors responsible for this interpatient variabil- ity are not well understood; however, genetic differ- ences in the 1 -adrenergic receptor ( 1 AR) may con- tribute. Two common polymorphisms occur in the gene that encodes the 1 AR. Both are single-nucleotide polymorphisms (SNPs), with an A3 G substitution oc- From the Department of Pharmacy Practice, College of Pharmacy; Division of Biostatistics, Department of Statistics; College of Nursing; and Division of Cardiology, College of Medicine; Univer- sity of Florida. Dr Zineh and Dr Puckett were equal contributors. This study was supported by National Institutes of Health grant HL64691 (Dr Johnson) and by the University of Florida General Clinical Research Center grant RR00082. Received for publication Jan 24, 2003; accepted March 11, 2003. Reprint requests: Julie A. Johnson, PharmD, Department of Phar- macy Practice, College of Pharmacy, University of Florida, PO Box 100486, Gainesville, FL 32610. E-mail: [email protected] Copyright © 2003 by the American Society for Clinical Pharmacol- ogy & Therapeutics. 0009-9236/2003/$30.00 0 doi:10.1016/S0009-9236(03)00068-7 44
Transcript of β1-adrenergic receptor polymorphisms and antihypertensive response to metoprolol
PHARMACOGENETICS ANDGENOMICS
�1-Adrenergic receptor polymorphisms andantihypertensive response to metoprolol
Objectives: Marked interpatient variability exists in blood pressure response to �-blocker monotherapy. Wetested the hypothesis that 2 common polymorphisms in the gene for �1-adrenergic receptor are associatedwith antihypertensive response to metoprolol in patients with uncomplicated hypertension.Methods: Forty hypertensive men and women aged 35 to 65 years were studied. Baseline studies included24-hour ambulatory blood pressure monitoring. Patients took 50 mg metoprolol twice daily with weeklytitration to response or 200 mg twice daily. After a minimum of 4 weeks at stable dose, treatment phase24-hour ambulatory blood pressure monitoring was repeated. The codon 49 and 389 genotypes for �1-adrenergic receptor were determined by polymerase chain reaction with restriction fragment length polymor-phism. Multilinear regression was performed to determine the impact of genotype and other variables onblood pressure response to metoprolol.Results: Patients homozygous for Arg at codon 389 had a nearly 3-fold greater reduction in daytime diastolicblood pressure (�13.3% � 8.4% versus �4.5% � 8.2%, P � .0018) compared with those who carried thevariant allele. The haplotype pair (diplotype) for �1-adrenergic receptor was also a significant predictor ofresponse, with patients having the Ser49Arg389/Ser49Arg389 diplotype demonstrating a decline in bloodpressure of 14.7 mm Hg versus 0.5 mm Hg in patients with the Gly49Arg389/Ser49Gly389 diplotype. Inmultiregression analysis, baseline daytime diastolic blood pressure, codon 389 genotype, and codon 49genotype were significant predictors of blood pressure after treatment.Conclusions: Our data suggest that �1-adrenergic receptor polymorphisms are important determinants ofantihypertensive response to metoprolol. In the future, codon 49 and 389 genotypes or �1-adrenergicreceptor haplotypes might be used to predict the diastolic blood pressure response to metoprolol in patientswith hypertension. (Clin Pharmacol Ther 2003;74:44-52.)
Julie A. Johnson, PharmD, Issam Zineh, PharmD, Brian J. Puckett, PharmD,Susan P. McGorray, PhD, Hossein N. Yarandi, PhD, and Daniel F. Pauly, MD, PhDGainesville, Fla
Affecting approximately 50 million Americans, hy-pertension is the most prevalent chronic disease in the
United States and a major contributor to mortality andvascular morbidity.1 The benefits of antihypertensivedrug therapy on curtailing hypertension-related stroke,heart failure, and end-stage renal disease are well rec-ognized. Currently, �-blockers are recommended first-line agents in the management of hypertension.2 How-ever, marked variability in response exists, withadequate blood pressure (BP) control failing to beachieved with �-blocker monotherapy in 30% to 60%of patients.3,4
The factors responsible for this interpatient variabil-ity are not well understood; however, genetic differ-ences in the �1-adrenergic receptor (�1AR) may con-tribute. Two common polymorphisms occur in the genethat encodes the �1AR. Both are single-nucleotidepolymorphisms (SNPs), with an A3G substitution oc-
From the Department of Pharmacy Practice, College of Pharmacy;Division of Biostatistics, Department of Statistics; College ofNursing; and Division of Cardiology, College of Medicine; Univer-sity of Florida. Dr Zineh and Dr Puckett were equal contributors.
This study was supported by National Institutes of Health grantHL64691 (Dr Johnson) and by the University of Florida GeneralClinical Research Center grant RR00082.
Received for publication Jan 24, 2003; accepted March 11, 2003.Reprint requests: Julie A. Johnson, PharmD, Department of Phar-
macy Practice, College of Pharmacy, University of Florida, POBox 100486, Gainesville, FL 32610.
E-mail: [email protected] © 2003 by the American Society for Clinical Pharmacol-
ogy & Therapeutics.0009-9236/2003/$30.00 � 0doi:10.1016/S0009-9236(03)00068-7
44

curring at nucleotide 145, resulting in a Ser to Glysubstitution at codon 49, and a G3C substitution atnucleotide 1165, resulting in an Arg to Gly substitutionat codon 389. There are racial differences in allelefrequencies for both polymorphisms, with Gly49 fre-quencies of 0.15 and 0.29 and Gly389 frequencies of0.27 and 0.42 in white subjects and black subjects,respectively.5-7 The codon 49 polymorphism is locatedin the extracellular amino terminus. The codon 389polymorphism occurs in an intracellular domain prox-imal to the seventh transmembrane-spanning region ofthe receptor. This area is highly conserved and impor-tant in G-protein coupling.
In vitro studies suggest that both of these polymor-phisms have functional consequences. In vitro mu-tagenesis data demonstrate that the Arg389 form of thereceptor has basal and agonist-stimulated adenylyl cy-clase activities that are approximately 2-fold and 3-foldhigher, respectively, than the activity of the Gly389form.8 Moreover, a recent study suggested that theArg389 homozygous genotype was associated with hy-pertension.9 In addition, a study from our laboratorydemonstrated that in patients undergoing dobutaminestress testing the resting heart rate and diastolic bloodpressure (DBP) were higher in patients with the Arg389homozygous genotype.10 As such, we hypothesizedthat hypertensive patients who are homozygous forArg389 may have hypertension predominantly medi-ated through the adrenergic nervous system and thusmay have the largest antihypertensive response to�-blockers. The primary purpose of this study was totest this hypothesis.
Recent in vitro studies, in which site-directed mu-tagenesis techniques were used, have also suggestedthat the codon 49 polymorphism is functional. Al-though some of the data from these 2 studies are con-flicting, they are consistent in showing that the Gly49form of the receptor is associated with greater agonist-promoted down-regulation.11,12 Therefore we hypothe-sized that the codon 49 genotype might also affect theantihypertensive response to �-blockers. In addition,we sought to determine whether haplotype was moreinformative than either polymorphism alone.
METHODSPatients. The study population included white, Af-
rican American, and Hispanic men and women withhypertension who were between 35 and 65 years old.Hypertension was defined as untreated (for at least 2weeks) sitting (�5 minutes) DBP greater than or equalto 95 mm Hg and less than or equal to 115 mm Hg on2 clinic visits separated by at least 3 days. Systolic
blood pressure (SBP) above a certain threshold was notrequired for entry into the study. Patients could betaking medications for other indications but were ex-cluded if any of these medications could conceivablyaffect BP.
Patients were excluded if they had concomitant con-ditions that were being treated with antihypertensivemedications or had other conditions that are typicallyconsidered exclusion criteria for �-blocker studies.13
All eligible patients provided written informed consent.The protocol was approved by the University of FloridaInstitutional Review Board, Gainesville, Fla. All studyvisits took place in the University of Florida GeneralClinical Research Center.
Study protocol. Once patients were deemed eligible,they underwent 24-hour ambulatory blood pressure(ABP) monitoring by an Accutracker DX device (Sun-Tech Medical Instruments, Inc, Raleigh, NC). Monitorswere validated against a mercury sphygmomanometerand measured 4 random BP readings per hour duringwaking hours (6 AM to 11 PM, “daytime”) and 3 randomBP readings per hour during patient sleep times (11 PM
to 6 AM, “nighttime”). These wake and sleep timeslargely correlated with patients’ active and restingtimes and sleeping habits. In the case of night shiftworkers (n � 3), the waking hours and sleep times wereset at 17 and 7 hours, respectively, and were chosen ona patient-specific basis to coincide with the patient’swake and sleep times. Accurate BP measurementscould not be obtained with the Accutracker DX devicein 2 patients. In these patients the SpaceLabs 90207oscillometric ABP monitor (SpaceLabs, Inc, Redmond,Wash) was used. After placement of the ABP monitor,patients were instructed to go about their usual dailyactivities.
Once baseline studies were completed, drug therapywas initiated. Patients took 50 mg metoprolol tartrateevery 12 hours and were seen for weekly titration to100 mg and 200 mg every 12 hours, if needed. Doseswere increased until (1) clinic DBP less than 90 mm Hgwas achieved, (2) a maximum of 200 mg metoprololtwice daily was reached, or (3) the patient had intoler-able side effects. Patients for whom target DBP wasachieved continued therapy for at least 4 more weeks.Those in whom target BP failed to be reached on themaximum metoprolol dose but who had a DBP reduc-tion of 10% or greater were also treated for 4 moreweeks. Patients in whom either of these response cri-teria failed to be met proceeded to the end of studyevaluation. All clinic visits for BP checks took place atthe same time of day to minimize the impact of diurnalvariation on clinic BP.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Johnson et al 45
For treatment phase evaluations, 24-hour ABP mon-itoring was repeated, followed by admission of thepatient to the General Clinical Research Center for apharmacokinetic study. Indwelling venous catheterswere placed, and blood samples were drawn immedi-ately before and at 2, 4, 8, and 12 hours after themetoprolol dose for pharmacokinetic analysis. R- andS-metoprolol plasma concentrations were determinedby chiral HPLC with fluorescence detection as previ-ously described.14 S-metoprolol (active enantiomer)area under the plasma concentration–time curve from 0to 12 hours [AUC(0-12]) was determined in each pa-tient by the mixed log-linear method (Kinetica 4.0.1;InnaPhase Corp, Philadelphia, Pa).
Genotyping. Blood samples were obtained for geno-typing at study entry. Genomic deoxyribonucleic acidwas isolated from whole blood by a commercial kit(Purgene; Gentra Systems, Minneapolis, Minn). Geno-types at codons 49 and 389 were determined by poly-merase chain reaction and subsequent restriction frag-ment length polymorphism with Sau96I and BstNIenzymes, respectively, in accordance with protocolsmodified from previously described methods.6,8 Geno-types were scored by at least 2 blinded investigatorswho were unaware of the subjects’ clinical drug re-sponses. In cases of disagreement, the sample under-went a second restriction fragment length polymor-phism analysis that was blindly scored by 3 persons.Patients were considered to have been officially scoredwhen all investigators agreed that the genotype wasunambiguous.
Haplotype assignment. We have recently shownthat the codon 49 and 389 polymorphisms are in link-age disequilibrium such that the Gly49Gly389 combi-nation rarely, if ever, occurs.15 Thus patients who weredouble heterozygotes were assigned Ser49Gly389 andGly49Arg389 as their 2 haplotypes.
Data analysis. Analysis of ABP data was conductedaccording to usual protocols.13 Hourly BP means werecalculated for the 24-hour time period. These were thenused to calculate daytime (6 AM-11 PM) and nighttime(11 PM-6 AM) means.
On the basis of statistical power analysis, it wascalculated that 20 patients per genotype group wasrequired to provide 80% power to detect a difference inresponse of 4.4 mm Hg between genotypes with a2-tailed � of .05. Because Gly49Gly and Gly389Glygenotypes were expected to occur infrequently in thestudy population, it was planned a priori that thesehomozygotes would be combined with heterozygotesand the groups classified as Gly49 carriers and Gly389carriers for analysis.
Baseline characteristics were compared between ge-notypes by use of the chi square test, Fisher exact test,or Student unpaired t test, as appropriate. Treatmenteffect and S-metoprolol area under the plasma concen-tration–time curve (AUC) by genotype were comparedby Student unpaired t test and Mann-Whitney U test,respectively. Secondary analyses included BP responseby race or ethnicity and categoric BP response (ie,responder versus nonresponder) by genotype. Patientswere classified as responders to metoprolol mono-therapy if they had a decrease in daytime DBP of 10%or greater from baseline.
Linear regression models were used to examine thejoint effects of covariates on treatment daytime DBP.The following variables were analyzed for inclusion inthe model: baseline mean daytime DBP (by ABP mon-itoring), age, sex, race, smoking status, body massindex, exercise (self-reported), codon 389 genotype,codon 49 genotype, and S-metoprolol plasma AUC(0-12). Several of these variables (eg, smoking status)were included for analysis because they have beenassociated with varying rates of BP control in a largepatient population.16 Three different step-type selectionmethods (backward elimination, forward selection, andminimum R2 improvement) were used to determine thebest-fitting regression model from the maximummodel. Given that the goal is reliable prediction offuture observations, the level of significance was set at.10 to avoid missing useful predictors of BP response tometoprolol. Transformation of variables, such as logAUC, was considered, and interactions and model di-agnostics were examined. Parameter estimates of pre-dictors identified as significant in the model were sub-sequently derived.
All statistical analyses were performed with the useof Statistica (version 5.1; StatSoft Inc, Tulsa, Okla) orSAS (version 8; SAS Institute Inc, Cary, NC). Exceptin the step-type regression analyses, a P value of lessthan .05 was considered statistically significant.
RESULTSA total of 40 patients were enrolled in the study.
Allele frequencies were 0.73 for Arg389 and 0.84 forSer49. There were 18 Arg389 homozygotes (45%), 22Gly389 carriers (55%), 27 Ser49 homozygotes(67.5%), and 13 Gly49 carriers (32.5%). There were noGly homozygotes at either codon; thus all Gly carriersat both codons were heterozygotes. Genotype frequen-cies for both polymorphisms were in Hardy-Weinbergequilibrium.
Baseline characteristics for Arg389 homozygotesand Gly389 carriers are shown in Table I. African
CLINICAL PHARMACOLOGY & THERAPEUTICS46 Johnson et al JULY 2003
Americans were more likely to be Gly389 carriers thanArg389 homozygotes (composing 36.4% versus 11.1%of each cohort). These differences were of borderlinesignificance (P � .07) and are consistent with thepublished literature on racial differences in codon 389allele frequency.5 No baseline differences in heart rateor BP existed between groups. Baseline characteristicswere also not different between Ser49 homozygotesand Gly49 carriers (data not shown). Adverse effectsfrom metoprolol in this population were minor, and nostudy participants discontinued the study because ofadverse effects.
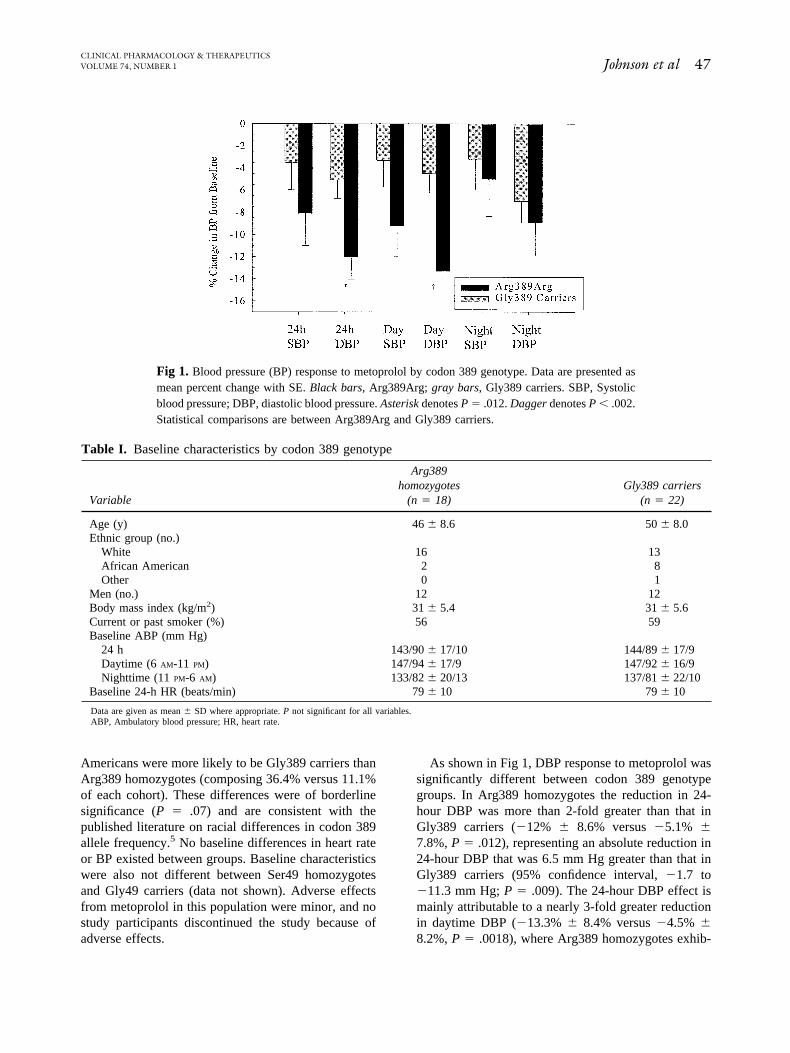
As shown in Fig 1, DBP response to metoprolol wassignificantly different between codon 389 genotypegroups. In Arg389 homozygotes the reduction in 24-hour DBP was more than 2-fold greater than that inGly389 carriers (�12% � 8.6% versus �5.1% �7.8%, P � .012), representing an absolute reduction in24-hour DBP that was 6.5 mm Hg greater than that inGly389 carriers (95% confidence interval, �1.7 to�11.3 mm Hg; P � .009). The 24-hour DBP effect ismainly attributable to a nearly 3-fold greater reductionin daytime DBP (�13.3% � 8.4% versus �4.5% �8.2%, P � .0018), where Arg389 homozygotes exhib-
Table I. Baseline characteristics by codon 389 genotype
Variable
Arg389homozygotes
(n � 18)Gly389 carriers
(n � 22)
Age (y) 46 � 8.6 50 � 8.0Ethnic group (no.)
White 16 13African American 2 8Other 0 1
Men (no.) 12 12Body mass index (kg/m2) 31 � 5.4 31 � 5.6Current or past smoker (%) 56 59Baseline ABP (mm Hg)
24 h 143/90 � 17/10 144/89 � 17/9Daytime (6 AM-11 PM) 147/94 � 17/9 147/92 � 16/9Nighttime (11 PM-6 AM) 133/82 � 20/13 137/81 � 22/10
Baseline 24-h HR (beats/min) 79 � 10 79 � 10
Data are given as mean � SD where appropriate. P not significant for all variables.ABP, Ambulatory blood pressure; HR, heart rate.
Fig 1. Blood pressure (BP) response to metoprolol by codon 389 genotype. Data are presented asmean percent change with SE. Black bars, Arg389Arg; gray bars, Gly389 carriers. SBP, Systolicblood pressure; DBP, diastolic blood pressure. Asterisk denotes P � .012. Dagger denotes P � .002.Statistical comparisons are between Arg389Arg and Gly389 carriers.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Johnson et al 47
ited a reduction in DBP that was 8.6 mm Hg greaterthan that found in Gly389 carriers (95% confidenceinterval, �3.5 to �13.6 mm Hg; P � .0014). There wasalso a trend toward a greater reduction in daytime SBPin the Arg389 homozygotes compared with Gly389carriers (�9.2% � 11.9% versus �3.3% � 11.3%, P� .12). There were no significant differences in night-time SBP or DBP responses to metoprolol on the basisof the codon 389 genotype. Likewise, there were nodifferences in the heart rate response to �-blockade onthe basis of genotype (data not shown).
A secondary analysis included determination of al-lele frequencies for the �1AR polymorphisms amongDBP responders and nonresponders to metoprolol. Theallele frequencies for Arg389 and Gly389 were signif-icantly different between responders and nonre-sponders (Table II). There were more nonwhite sub-jects among nonresponders than among responders (9versus 2, P � .006). However, consideration of BPreduction by genotype within white subjects alone re-vealed data similar to those in the entire population(daytime DBP response in Arg389Arg versus Gly389carriers, �14.3% � 8.06% versus �4.4% � 7.9%; P �.003), suggesting that race was not confounding thefinding. Because there were only 2 nonwhite subjects inthe Arg389Arg group, meaningful analyses of BP re-duction by genotype within this group could not beperformed.
BP response to metoprolol was not significantly as-sociated with codon 49 genotype. However, there didappear to be a consistently larger magnitude of BPreduction across all ABP parameters in Ser49 homozy-gotes compared with Gly49 carriers, with a trend to-ward significance for 24-hour and daytime DBP reduc-tion (P � .08 for both parameters).
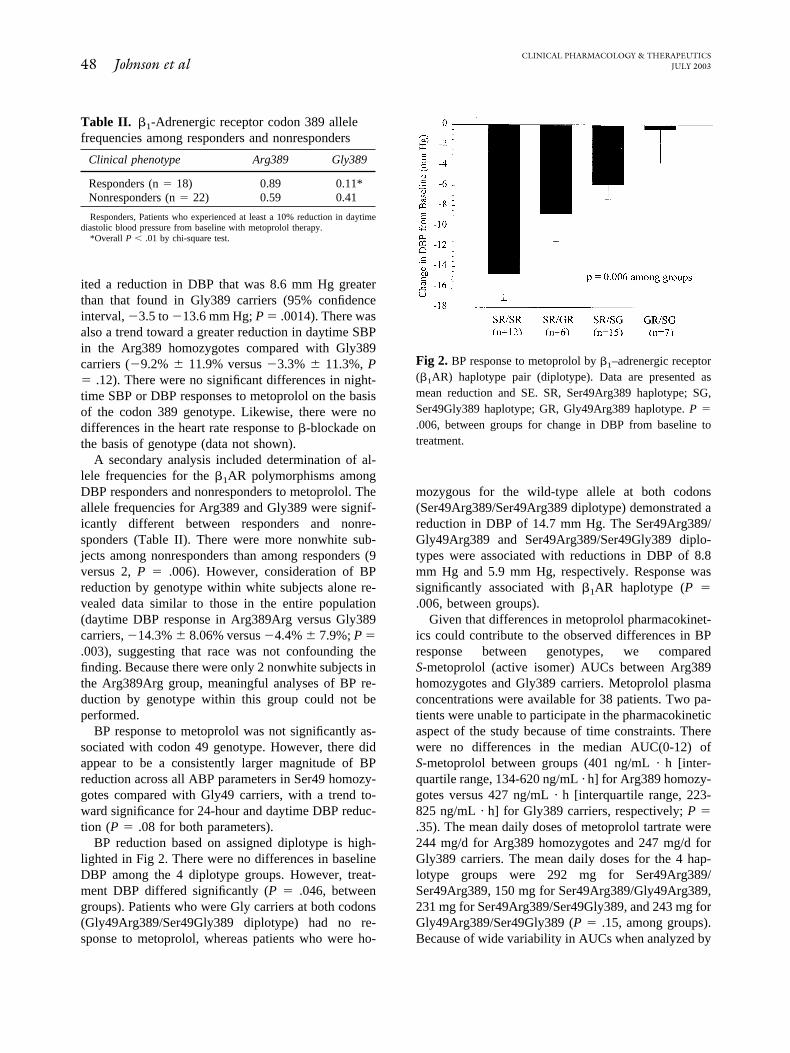
BP reduction based on assigned diplotype is high-lighted in Fig 2. There were no differences in baselineDBP among the 4 diplotype groups. However, treat-ment DBP differed significantly (P � .046, betweengroups). Patients who were Gly carriers at both codons(Gly49Arg389/Ser49Gly389 diplotype) had no re-sponse to metoprolol, whereas patients who were ho-
mozygous for the wild-type allele at both codons(Ser49Arg389/Ser49Arg389 diplotype) demonstrated areduction in DBP of 14.7 mm Hg. The Ser49Arg389/Gly49Arg389 and Ser49Arg389/Ser49Gly389 diplo-types were associated with reductions in DBP of 8.8mm Hg and 5.9 mm Hg, respectively. Response wassignificantly associated with �1AR haplotype (P �.006, between groups).
Given that differences in metoprolol pharmacokinet-ics could contribute to the observed differences in BPresponse between genotypes, we comparedS-metoprolol (active isomer) AUCs between Arg389homozygotes and Gly389 carriers. Metoprolol plasmaconcentrations were available for 38 patients. Two pa-tients were unable to participate in the pharmacokineticaspect of the study because of time constraints. Therewere no differences in the median AUC(0-12) ofS-metoprolol between groups (401 ng/mL · h [inter-quartile range, 134-620 ng/mL · h] for Arg389 homozy-gotes versus 427 ng/mL · h [interquartile range, 223-825 ng/mL · h] for Gly389 carriers, respectively; P �.35). The mean daily doses of metoprolol tartrate were244 mg/d for Arg389 homozygotes and 247 mg/d forGly389 carriers. The mean daily doses for the 4 hap-lotype groups were 292 mg for Ser49Arg389/Ser49Arg389, 150 mg for Ser49Arg389/Gly49Arg389,231 mg for Ser49Arg389/Ser49Gly389, and 243 mg forGly49Arg389/Ser49Gly389 (P � .15, among groups).Because of wide variability in AUCs when analyzed by
Table II. �1-Adrenergic receptor codon 389 allelefrequencies among responders and nonresponders
Clinical phenotype Arg389 Gly389
Responders (n � 18) 0.89 0.11*Nonresponders (n � 22) 0.59 0.41
Responders, Patients who experienced at least a 10% reduction in daytimediastolic blood pressure from baseline with metoprolol therapy.
*Overall P � .01 by chi-square test.
Fig 2. BP response to metoprolol by �1–adrenergic receptor(�1AR) haplotype pair (diplotype). Data are presented asmean reduction and SE. SR, Ser49Arg389 haplotype; SG,Ser49Gly389 haplotype; GR, Gly49Arg389 haplotype. P �
.006, between groups for change in DBP from baseline totreatment.
CLINICAL PHARMACOLOGY & THERAPEUTICS48 Johnson et al JULY 2003

haplotype, nonparametric analysis was performed. Themedian S-metoprolol AUCs for the 4 groups were 497ng/mL · h for Ser49Arg389/Ser49Arg389, 246 ng/mL ·h for Ser49Arg389/Gly49Arg389, 501 ng/mL · h forSer49Arg389/Ser49Gly389, and 417 ng/mL · h forGly49Arg389/Ser49Gly389 (P � .56, among groups).
Linear regression modeling was used to examine theeffects of multiple variables on treatment daytime DBP.Race was the first variable to be removed in the back-ward elimination procedure. Other variables that didnot contribute to variability in antihypertensive re-sponse to metoprolol included sex, smoking status,exercise, and age. Of the 10 variables considered forinclusion in the model by the stepwise selection proce-dure, only baseline mean daytime DBP, codon 389genotype, and codon 49 genotype were significant pre-dictors of treatment daytime DBP (R2 � 0.57, P �.0001) (Table III). The model suggests significant in-dependent DBP-lowering contributions of �8.3 mmHg and �5.1 mm Hg associated with the Arg389 andSer49 homozygous genotypes, respectively. There wasno indication of interaction that would increase or di-minish the joint impact of these 2 variables.
Finally, the minimum R2 improvement method con-firmed the significance of these 3 variables. In addition,this method provided an additional regression modelthat consisted of 5 statistically significant predictors ofBP response (R2 � 0.63). The predictor variables in thismodel included baseline mean daytime DBP, an inter-action term incorporating codon 389 and codon 49genotypes, age, BMI, and AUC. However, the calcu-lated ratio of the model error to the overall error of themaximum model, known as the C(p) statistic, indicatedthat the 5-variable model had too many parametersgiven the number of subjects. Codon 49 and 389 geno-types remained important predictors of BP response inall models analyzed.
DISCUSSIONThat some patients respond better than others to
�-blockers is well accepted by clinicians. In this studywe found that the Arg389 homozygous genotype was
strongly associated with the DBP response to metopro-lol. This finding was consistent across every type ofanalysis conducted. Specifically, we found that theArg389Arg genotype was associated with a signifi-cantly greater reduction in 24-hour and daytime DBPthan was found in carriers of a Gly389 allele. When thepopulation was segregated into clinical responders andnonresponders, we found that the Arg389 allele fre-quency was substantially higher in responders than innonresponders. In addition, the Arg389Arg genotypewas a significant predictor of response in multivariateanalysis. Finally, consideration of haplotypes revealedthat the 2 groups with the largest DBP reduction werethose that included the Arg389Arg genotype. Thus eachanalysis approach indicated that the Arg389Arg geno-type was an important predictor of DBP lowering withmetoprolol. The threshold for statistical significancewas not reached for SBP, most likely because clinicaleffect was titrated to DBP response with change in SBPas a secondary end point. In addition, the study waspowered on the basis of DBP response variability, andgiven that there is greater variability in the SBP re-sponse, we likely had inadequate power to detect sig-nificant differences in SBP response by genotype. Thedata suggest that with additional study subjects signif-icant differences in SBP response by genotype might beobserved.
In addition to codon 389, we evaluated the impact ofcodon 49 genotype and the codon 49/389 haplotype onantihypertensive response to metoprolol. Althoughthere were only trends of an association between codon49 genotype and response when considered in isolation,codon 49 was a significant factor in response variabilityin multiple regression analysis. It is important thathaplotype was more informative than codon 389 geno-type alone. For example, the response in Arg389 ho-mozygotes was modified by the codon 49 genotype, asis evident from the responses of those with theSer49Arg389/Ser49Arg389 diplotype compared withthe Ser49Arg389/Gly49Arg389 diplotype (Fig 2).
The importance of haplotype was well described forthe �2-agonist response relative to �2AR haplotype in
Table III. Factors influencing blood pressure response to metoprolol in multivariate analysis
PredictorParameterestimate
Partial R2
(%) P value
Baseline daytime DBP 0.79 35.6 �.0001Arg389Arg genotype –8.33 15.8 .001Ser49Ser genotype –5.05 4.6 .05
Intercept for the model is 18.82. Expected DBPT (millimeters of mercury) is calculated as DBPT � 18.82 � 0.79(Baseline daytime DBP) – 8.3 (if Arg389Arg) – 5.1(if Ser49Ser), in which DBPT is treatment mean daytime DBP by 24-hour ambulatory blood pressure monitor.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Johnson et al 49

patients with asthma.17 In contrast to the �2ARhaplotype–�2-agonist example, we found both a singleSNP and haplotype to be significantly associated withdrug response. However, it is consistent with the pre-vious study in asthma in which haplotype was used thatwe found haplotype to be a more informative methodfor discerning the genetic contribution to response vari-ability than single genotype alone. Thus these datarepresent another good example of the value of haplo-type analysis over a single SNP analysis approach.However, given that the effects of the 2 �1AR SNPs areadditive, the multiple regression analysis approach withcodon 49 and 389 genotypes seems to be similarlyinformative to the haplotype analysis.
The findings in this study relative to codon 389 andcodon 49 genotypes are also consistent with publisheddata on these polymorphisms. For codon 389, our dataare consistent with recently published data from a pro-spective study in healthy volunteers of �-blocker re-sponse by genotype,18 as well as the existing literatureon the functional effects of this polymorphism and thesympathetic control of BP.8 Furthermore, nighttime BPwas not associated with codon 389 genotype in thisstudy. Because sympathetic tone is substantially re-duced during the nighttime, the nighttime BP is onlyminimally regulated by the sympathetic nervous sys-tem.19 As such, the associations seen between �1ARpolymorphisms and antihypertensive response to�-blockers during the day would not necessarily beexpected to carry over to the nighttime, as was ob-served in our study. The functional data for codon 49suggest that the effect of this polymorphism is primar-ily on receptor regulation, with the Gly49 allele under-going greater agonist-mediated receptor down-regulation.11,12 These in vitro data are also consistentwith our finding of greater antihypertensive response tometoprolol in the Ser49 homozygotes.
In this study we also evaluated another potentiallyimportant source of variable drug response, namely,pharmacokinetics. We measured steady-stateS-metoprolol concentrations and determined the AUC.Metoprolol is metabolized by the genetically polymor-phic cytochrome P450 (CYP) 2D6 enzyme. We did notexamine CYP2D6 genotype as a predictor of BP re-sponse because there is no suggestion that CYP2D6genotype would be a better predictor of response thanthe actual plasma concentrations that result from thosegenotypes. In fact, there is a 5- to 7-fold interpatientvariability in S-metoprolol plasma concentrationsamong CYP2D6 extensive metabolizers14; thus plasmaconcentration is much more informative than CYP2D6genotype or metabolizer phenotype. The S-metoprolol
AUCs were not different between Arg389Arg andGly389 carriers, documenting that the differences inobserved response between these 2 groups were not aresult of differences in drug metabolism or plasma drugconcentrations. These data highlight that the observeddifference in BP response to metoprolol is not one thatcan be addressed through differential doses or plasmaconcentrations. Specifically, data from numerous stud-ies, including this one, indicate that certain patients willhave a negligible antihypertensive response to�-blockade, irrespective of the plasma concentration of�-blocker that is achieved. Our data suggest that �1ARgenotype contributes in an important way to response to�-blockade in hypertension, and for those with a poorresponse, increases in plasma drug concentration willnot change responsiveness. Furthermore, our data indi-cate that those who possess the “responsive” genotypesare not more sensitive (ie, need lower drug concentra-tions) but in many cases will need to be titrated torelatively high doses or concentrations to achieve aresponse. This highlights that achieving adequate dosesor plasma concentrations remains important, even inthose with “responsive” genotypes.
A potential confounder in our study is the inclusionof patients from different racial and ethnic groups. Thiscould be particularly problematic because it is recog-nized that African American subjects tend to havepoorer responses to �-blockers than white subjects3,4
and because the allele frequencies of the �1AR poly-morphisms differ by race.5 Although this could be apossible confounder, we do not believe it is so forseveral reasons. First, race was the first variable re-moved during the backward elimination procedure, in-dicating that it did not account for any of the variabilityin DBP response to metoprolol that was not accountedfor by other variables in the model. In addition, sub-group analysis of response by genotype in white sub-jects alone revealed data essentially identical to those ofthe population as a whole. As such, we do not believeour data are confounded by inclusion of different racialgroups. On the contrary, we believe these data provideinitial evidence that the observed clinical difference inresponse to �-blockers by race might be explainedlargely by the �1AR genetic polymorphisms. Specifi-cally, data from our laboratory on another population ofmore than 600 individuals suggest that the frequency ofthe diplotype associated with the best response in thisstudy (Ser49Arg389/Ser49Arg389) is 42% in whitesubjects and 18% in African American subjects.15 Inaddition, the Arg389 homozygous genotype occurs inapproximately 52% of white subjects and 37% of Af-rican American subjects. Thus the genotype and hap-
CLINICAL PHARMACOLOGY & THERAPEUTICS50 Johnson et al JULY 2003

lotype associated with the best response to �-blockersoccur significantly less often in African American sub-jects than in white subjects and may well provide agenetic or mechanistic explanation for the observedclinical differences in response in these 2 groups.
This primacy of genotype over race as a predictor ofdrug response has also been demonstrated with thiazidediuretics, an antihypertensive drug class historicallythought to be more effective in African American sub-jects than in white subjects. In this study G-protein �3
genotype and race were significant predictors of BPresponse in univariate analysis, but in multivariate anal-ysis, genotype remained in the model whereas race didnot.20 Thus it is our belief that in the future the commonclinical practice of using a patient’s skin color to de-termine initial antihypertensive treatment might be re-placed by using the patient’s genetic profile.
One of the ultimate goals of pharmacogenetics is toallow for individualized therapy, on the basis of geneticinformation.21,22 In the setting of hypertension, thiscould be beneficial from several perspectives. First, theapproach used at present is one of empiric trial anderror, and it is not uncommon for the initial one or twodrug choices prescribed to be ineffective at reducing thepatient’s BP. In addition, because hypertension is asilent disease, it is easy for patients to become dissat-isfied with the drug treatment process, particularly ifthe first prescribed drug is ineffective. This is evident,in part, from National Health and Nutrition Examina-tion Survey (NHANES) III data, which suggest thatonly 27% of hypertensive subjects have adequatelycontrolled BP.1 If antihypertensive response can bepredicted on the basis of genotype, this would increasethe likelihood of finding an effective drug the first timeand thus would potentially increase the number ofpatients in whom hypertension is controlled. The datapresented in this report provide evidence that such aprediction might be possible with �-blockers. Althoughthese data need to be confirmed in a different and largerpopulation, they provide encouraging initial data on thepotential for genetically guided, individualized therapyfor the management of hypertension.
We thank Kathleen Eberst for her expert HPLC analytic assis-tance; Tara Andrisin for her laboratory assistance and aid in genotypescoring; and Steven Terra, John Lima, and Larisa Humma for theirthoughtful comments regarding the manuscript.
The University of Florida has filed a patent application (althoughno ruling has been made by the patent office), with Dr Johnson as theinventor, for the discovery of the association between �1AR poly-morphisms and the �-blocker response. There are no conflicts ofinterest for any of the other 4 authors
References
1. Burt VL, Whelton P, Roccella EJ, Brown C, Cutler JA,Higgins M, et al. Prevalence of hypertension in the USadult population. Results from the Third National Healthand Nutrition Examination Survey, 1988-1991. Hyper-tension 1995;25:305-13.
2. The sixth report of the Joint National Committee onprevention, detection, evaluation, and treatment of highblood pressure. Arch Intern Med 1997;157:2413-46.
3. Comparison of propranolol and hydrochlorothiazide forthe initial treatment of hypertension. II. Results of long-term therapy. Veterans Administration CooperativeStudy Group on Antihypertensive Agents. JAMA 1982;248:2004-11.
4. Materson BJ, Reda DJ, Cushman WC, Massie BM, FreisED, Kochar MS, et al. Single-drug therapy for hyperten-sion in men. A comparison of six antihypertensive agentswith placebo. The Department of Veterans Affairs Co-operative Study Group on Antihypertensive Agents.N Engl J Med 1993;328:914-21.
5. Moore JD, Mason DA, Green SA, Hsu J, Liggett SB.Racial differences in the frequencies of cardiac �1-adrenergic receptor polymorphisms: analysis ofc145A�G and c1165G�C. Hum Mutat 1999;14:271.
6. Maqbool A, Hall AS, Ball SG, Balmforth AJ. Commonpolymorphisms of �1-adrenoceptor: identification andrapid screening assay [letter]. Lancet 1999;353:897.
7. Johnson JA, Terra SG. Beta-adrenergic receptor poly-morphisms: cardiovascular disease associations andpharmacogenetics. Pharm Res 2002;19:1779-87.
8. Mason DA, Moore JD, Green SA, Liggett SB. A gain-of-function polymorphism in a G-protein coupling do-main of the human �1-adrenergic receptor. J Biol Chem1999;274:12670-4.
9. Bengtsson K, Melander O, Orho-Melander M, LindbladU, Ranstam J, Rastam L, et al. Polymorphism in the�1-adrenergic receptor gene and hypertension. Circula-tion 2001;104:187-90.
10. Humma LM, Puckett BJ, Richardson HE, Terra SG,Andrisin TE, Lejeune BL, et al. Effects of beta1-adrenoceptor genetic polymorphisms on resting hemody-namics in patients undergoing diagnostic testing for isch-emia. Am J Cardiol 2001;88:1034-7.
11. Rathz DA, Brown KM, Kramer LA, Liggett SB. Aminoacid 49 polymorphisms of the human �1-adrenergic re-ceptor affect agonist-promoted trafficking. J CardiovascPharmacol 2002;39:155-60.
12. Levin MC, Marullo S, Muntaner O, Andersson B, Mag-nusson Y. The myocardium-protective Gly-49 variant ofthe �1-adrenergic receptor exhibits constitutive activityand increased desensitization and down-regulation. J BiolChem 2002;277:30429-35.
13. Johnson JA, Akers WS, Miller ST, Applegate WB. Meto-prolol minimizes nighttime blood pressure dip in hyper-tensive black males. Am J Hypertens 1995;8:254-9.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 74, NUMBER 1 Johnson et al 51

14. Johnson JA, Burlew BS. Metoprolol metabolism via cy-tochrome P4502D6 in ethnic populations. Drug MetabDispos 1996;24:350-5.
15. Terra SG, McGorray SP, Wallace MR, Picoult-NewbergL, Pepine CJ, Johnson JA. Beta1-adrenergic receptorpolymorphisms and linkage disequilibrium [abstract].Clin Pharmacol Ther 2002;71:P70.
16. Wassertheil-Smoller S, Anderson G, Psaty BM, BlackHR, Manson J, Wong N, et al. Hypertension and itstreatment in postmenopausal women: baseline data fromthe Women’s Health Initiative. Hypertension 2000;36:780-9.
17. Drysdale CM, McGraw DW, Stack CB, Stephens JC,Judson RS, Nandabalan K, et al. Complex promoter andcoding region �2-adrenergic receptor haplotypes alterreceptor expression and predict in vivo responsiveness.Proc Natl Acad Sci U S A 2000;97:10483-8.
18. Sofowora GG, Dishy V, Muszkat M, Xie HG, Kim RB,Harris PA, et al. A common �1-adrenergic receptor poly-morphism (Arg389Gly) affects blood pressure responseto �-blockade. Clin Pharmacol Ther 2003;73:366-71.
19. Imai Y, Abe K, Munakata M, Sakuma H, Hashimoto J,Imai K, et al. Circadian blood pressure variations underdifferent pathophysiological conditions. J Hypertens1990;8:S125-32.
20. Turner ST, Schwartz GL, Chapman AB, Boerwinkle E.C825T polymorphism of the G protein �3-subunit andantihypertensive response to a thiazide diuretic. Hyper-tension 2001;37(2 Pt 2):739-43.
21. Roses AD. Pharmacogenetics and the practice of medi-cine. Nature 2000;405:857-65.
22. Mancinelli L, Cronin M, Sadee W. Pharmacogenomics:the promise of personalized medicine. AAPS PharmSci2000;2:E4.
CLINICAL PHARMACOLOGY & THERAPEUTICS52 Johnson et al JULY 2003