Τινεώτεροπροτείνειη Συμφωνία Maastricht IV γιατο...
48
Θεόδωοξπ Ρξκκάπ MD, PhD(U.K.), FACG, FEBG, AGAF Δμτής Γαστρεμτερολογικής Κλιμικής Νοσοκομείο ΄΄Ερρίκος Ντυμάμ΄΄ Τι νεώτερο προτείνει η Συμφωνία Maastricht IV για το Ελίκοβακτηρίδιο του πυλωρού;
Transcript of Τινεώτεροπροτείνειη Συμφωνία Maastricht IV γιατο...
Θεόδωοξπ ΡξκκάπMD, PhD(U.K.), FACG, FEBG, AGAF
Δμτής Γαστρεμτερολογικής Κλιμικής
Νοσοκομείο ΄΄Ερρίκος Ντυμάμ΄΄
Τι νεώτερο προτείνει η Συμφωνία Maastricht IV για τοΕλίκοβακτηρίδιο του πυλωρού;
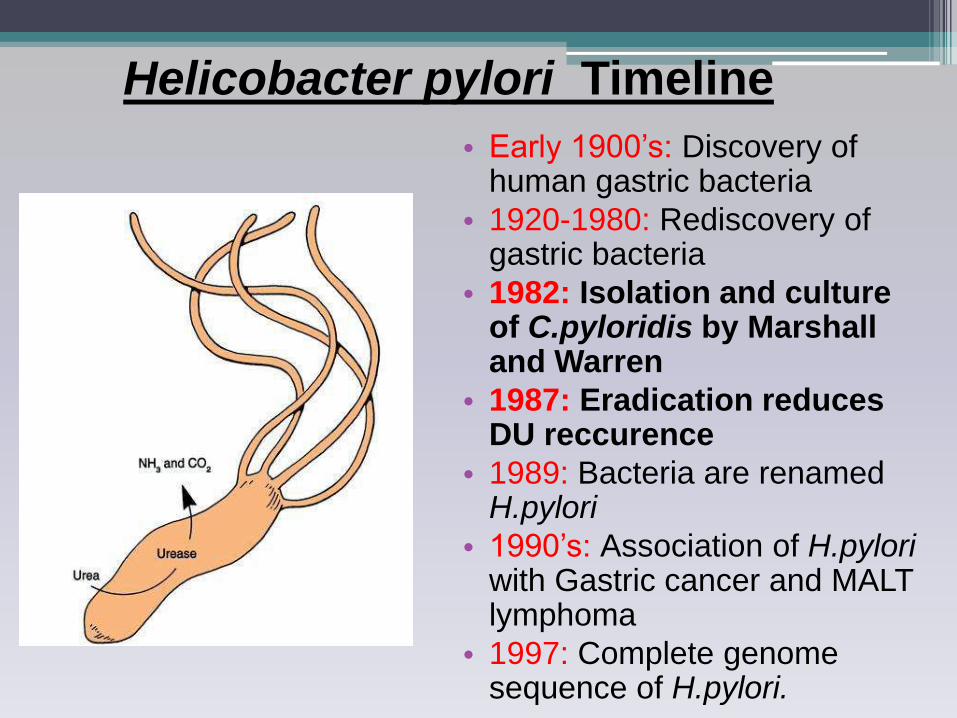
Helicobacter pylori Timeline
• Early 1900’s: Discovery of human gastric bacteria
• 1920-1980: Rediscovery of gastric bacteria
• 1982: Isolation and culture of C.pyloridis by Marshall and Warren
• 1987: Eradication reduces DU reccurence
• 1989: Bacteria are renamed H.pylori
• 1990’s: Association of H.pyloriwith Gastric cancer and MALT lymphoma
• 1997: Complete genome sequence of H.pylori.
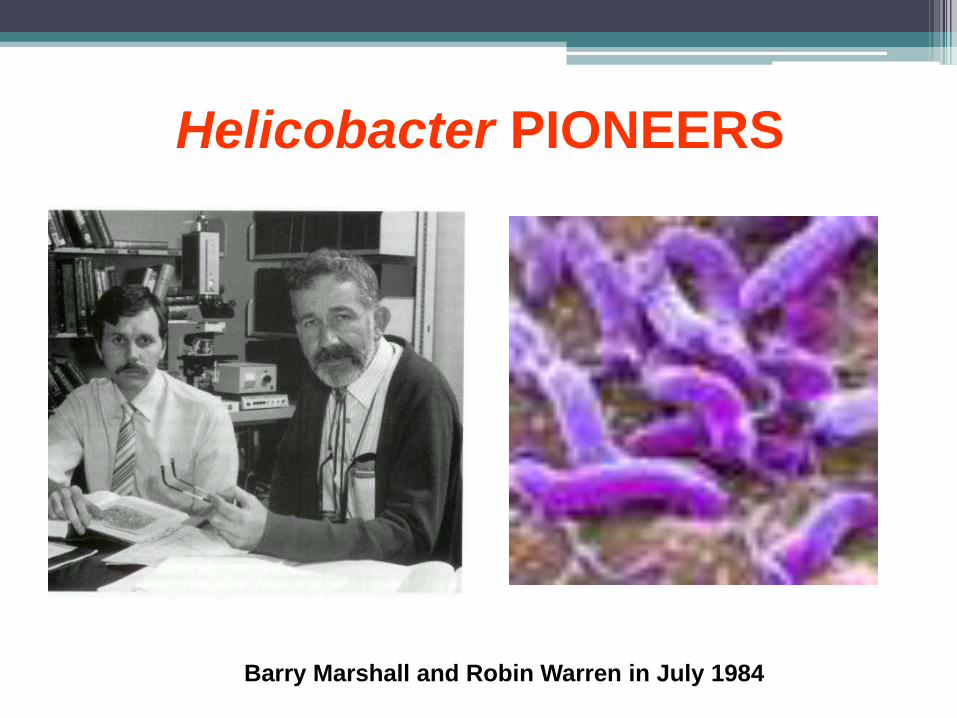
Helicobacter PIONEERS
Barry Marshall and Robin Warren in July 1984
The Nobel Prize in Physiology or Medicine 2005
Press Release: The 2005 Nobel Prize in Physiology or Medicine
3 October 2005
The Nobel Assembly at Karolinska Institute has today decided to award
The Nobel Prize in Physiology or Medicine for 2005
jointly to
Barry J. Marshall and J. Robin Warren
for their discovery of
"the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease"
The three recent major steps in
Gastroenterology
• Strong antisecretory
factors
• Progress in GI endoscopy
• H.pylori isolation
PPI
CH2
O
S
CH3 OCH2CF3
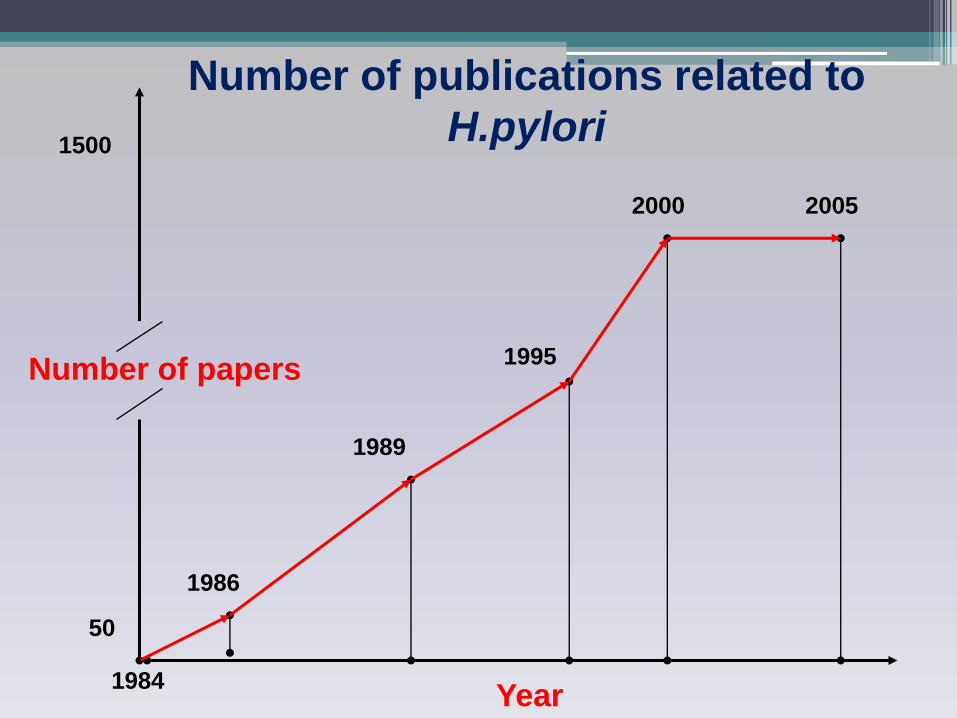
Number of publications related to
H.pylori
1984
1986
1989
1995
2000 2005
Year
50
1500
Number of papers
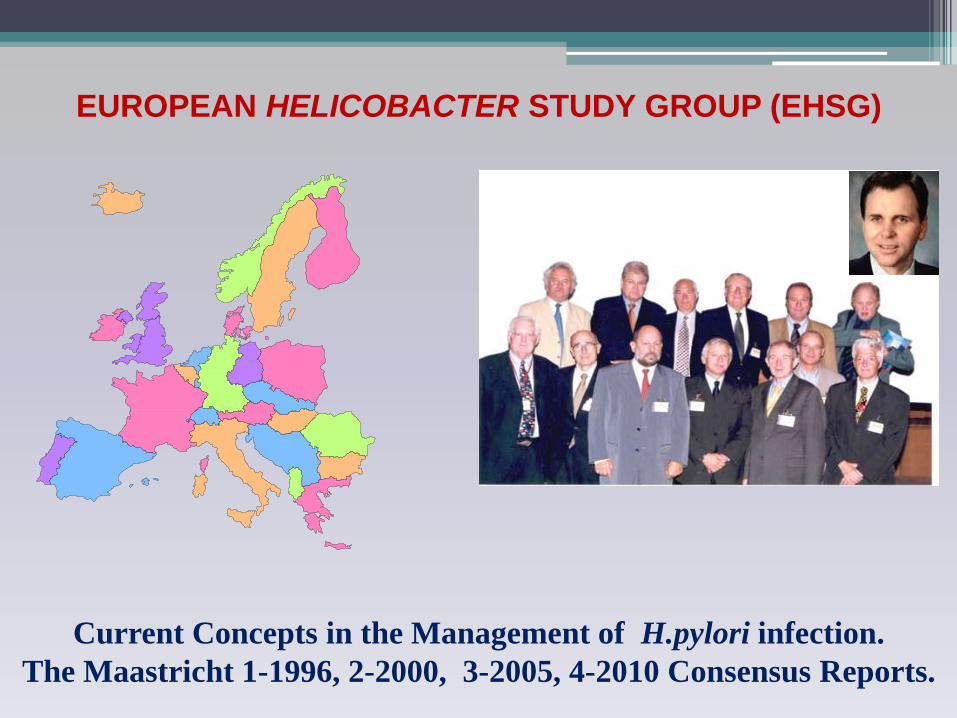
EUROPEAN HELICOBACTER STUDY GROUP (EHSG)
Current Concepts in the Management of H.pylori infection.
The Maastricht 1-1996, 2-2000, 3-2005, 4-2010 Consensus Reports.

MAASTRICHT IVMarch 16-18 2010, Florence, Italy

50 participants
25 countries
Gastroenterologists, GPs, Pathologists, Microbiologists
MAASTRICHT IV Consensus Report
ΔΙΑΔΙΚΑΣΙΑ (Ι)
Aλαζθνπήζεθαλ νη πξόζθαηεο γλώζεηο από
εηδηθνύο ζηνπο ζρεηηθνύο ηνµείο έξεπλαο πξηλ ηεζεί
µία ζεηξά νπζηαζηηθώλ εξσηεκάησλ.
Τα δεηήµαηα κειεηήζεθαλ από ηξεηο νµάδεο
εξγαζίαο.
ΔΙΑΔΙΚΑΣΙΑ (ΙΙ)Η θάζε νµάδα εξγαζίαο:
• κειέηεζε µία εηδηθή έλλνηα, ζέµα ή δήηεµα• δηαηύπσζε ηελ νµόθσλε δήισζε ή ζύζηαζή ηεο • δήισζε ηε βαξύηεηα ηεο δήισζεο ή ζύζηαζεο
(ζπληζηάηαη αλεπηθύιαθηα, ζπληζηάηαη, αβέβαηε) • θαηέηαμε ηε βαξύηεηα ησλ ελδείμεσλ πνπ ππνζηήξηδαλ ηε
δήισζε ή ζύζηαζε (αλαµθίβνιε, ππνζηεξηθηηθή ή αζαθήο)
• πεξηέγξαςε ηελ αηηηνινγία ηεο δήισζεο ή ζύζηαζεο.
Κάθε οµάδα εργαζίας παροσζίαζε ηις ζσζηάζεις ηης ζηην ολομέλεια για ζσζήηηζη και ζηη ζσνέτεια με υηθοθορία ζσμθφνήθηκαν οι ηελικές οµόθφνεςζσζηάζεις.
Timer Votes
1. I agree
2. I don’t agree
Question: Is a period of 4-6 weeks sufficient for follow-up after the end of H. pylori treatment?
Statement: The time for follow-up after the end of eradication therapy should be at least 4 weeks.
Evidence Level: 1 Grade of Recommendation: A
ΔΙΑΔΙΚΑΣΙΑ (ΙΙI)
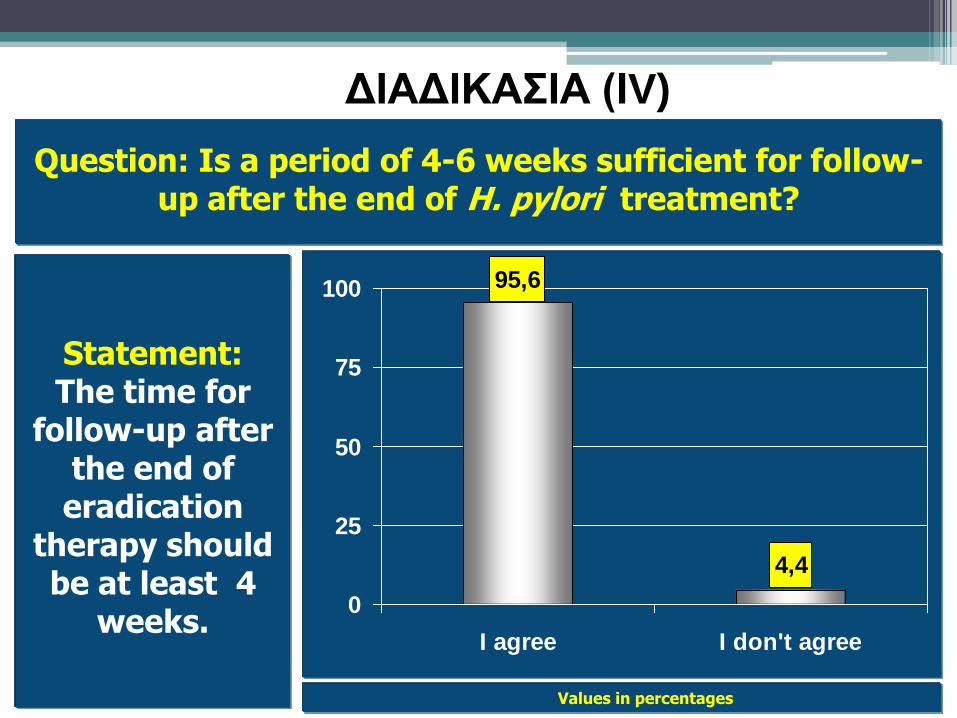
Values in percentages
95,6
4,4
0
25
50
75
100
I agree I don't agree
Question: Is a period of 4-6 weeks sufficient for follow-up after the end of H. pylori treatment?
Statement:The time for
follow-up after the end of eradication
therapy should be at least 4
weeks.
ΔΙΑΔΙΚΑΣΙΑ (ΙV)
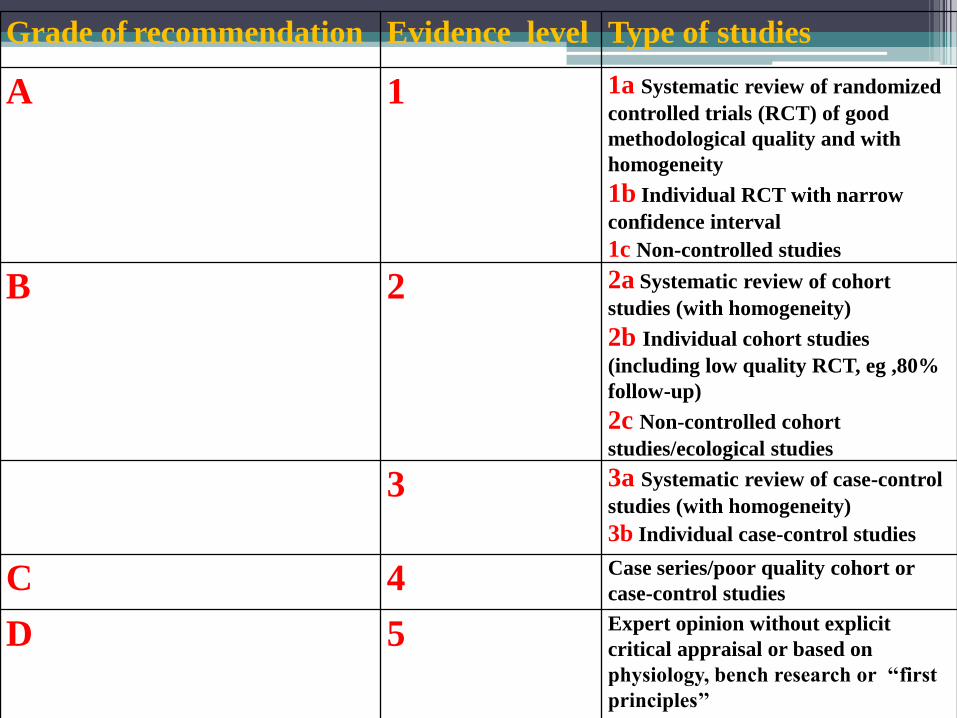
Grade of recommendation Evidence level Type of studies
A 1 1a Systematic review of randomized
controlled trials (RCT) of good
methodological quality and with
homogeneity
1b Individual RCT with narrow
confidence interval
1c Non-controlled studies
B 2 2a Systematic review of cohort
studies (with homogeneity)
2b Individual cohort studies
(including low quality RCT, eg ,80%
follow-up)
2c Non-controlled cohort
studies/ecological studies
3 3a Systematic review of case-control
studies (with homogeneity)
3b Individual case-control studies
C 4 Case series/poor quality cohort or
case-control studies
D 5 Expert opinion without explicit
critical appraisal or based on
physiology, bench research or ‘‘first
principles’’
Gut 2012;61:646
Current concepts in the management of Helicobacter pylori infection –The
Maastricht IV Consensus Report
P. MALFERTHEINER, F. MEGRAUD, C. O'MORAIN, F.
BAZZOLI, E. EL-OMAR, D. GRAHAM, R. HUNT,
T. ROKKAS, N. VAKIL, E. KUIPERS
& THE EUROPEAN HELICOBACTER STUDY GROUP (EHSG)
Current concepts in the management of
Helicobacter pylori infection –The
Maastricht IV Consensus Report
60 Statements on:
• Epidemiology
• Diagnosis
• Pathogenesis
• Management
• Carcinogenesis
Diagnosis
Treatment
Carcinogenesis
Diagnosis
Statement : The diagnostic accuracy of the stool
antigen test is equivalent to Urea Breath Test if a
validated laboratory-based monoclonal test is used.
Evidence level: 1a Grade of Recommendation: A
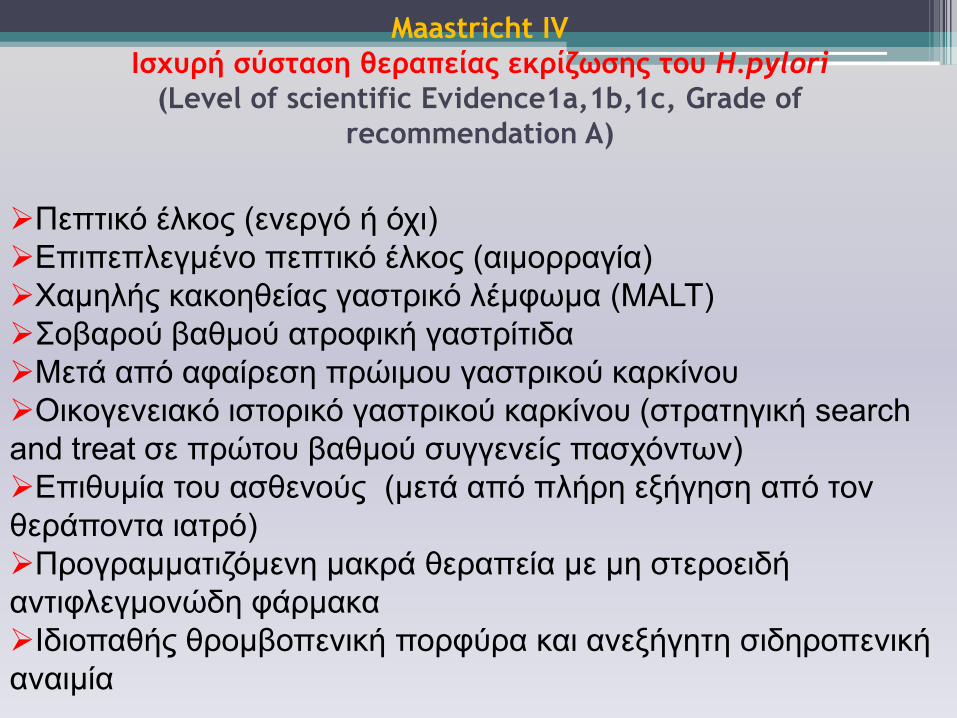
Πεπηηθό έιθνο (ελεξγό ή όρη)
Επηπεπιεγκέλν πεπηηθό έιθνο (αηκνξξαγία)
Χαµειήο θαθνεζείαο γαζηξηθό ιέµθσµα (MALT)
Σνβαξνύ βαζκνύ αηξνθηθή γαζηξίηηδα
Μεηά από αθαίξεζε πξώηµνπ γαζηξηθνύ θαξθίλνπ
Οηθνγελεηαθό ηζηνξηθό γαζηξηθνύ θαξθίλνπ (ζηξαηεγηθή search
and treat ζε πξώηνπ βαζκνύ ζπγγελείο παζρόλησλ)
Επηζπµία ηνπ αζζελνύο (κεηά από πιήξε εμήγεζε από ηνλ
ζεξάπνληα ηαηξό)
Πξνγξαµµαηηδόµελε καθξά ζεξαπεία µε µε ζηεξνεηδή
αληηθιεγµνλώδε θάξµαθα
Ιδηνπαζήο ζξνκβνπεληθή πνξθύξα θαη αλεμήγεηε ζηδεξνπεληθή
αλαηκία
Maastricht IV
Ιρυσοή ρύρςαρη θεοαπείαπ εκοίζωρηπ ςξσ H.pylori
(Level of scientific Evidence1a,1b,1c, Grade of
recommendation A)
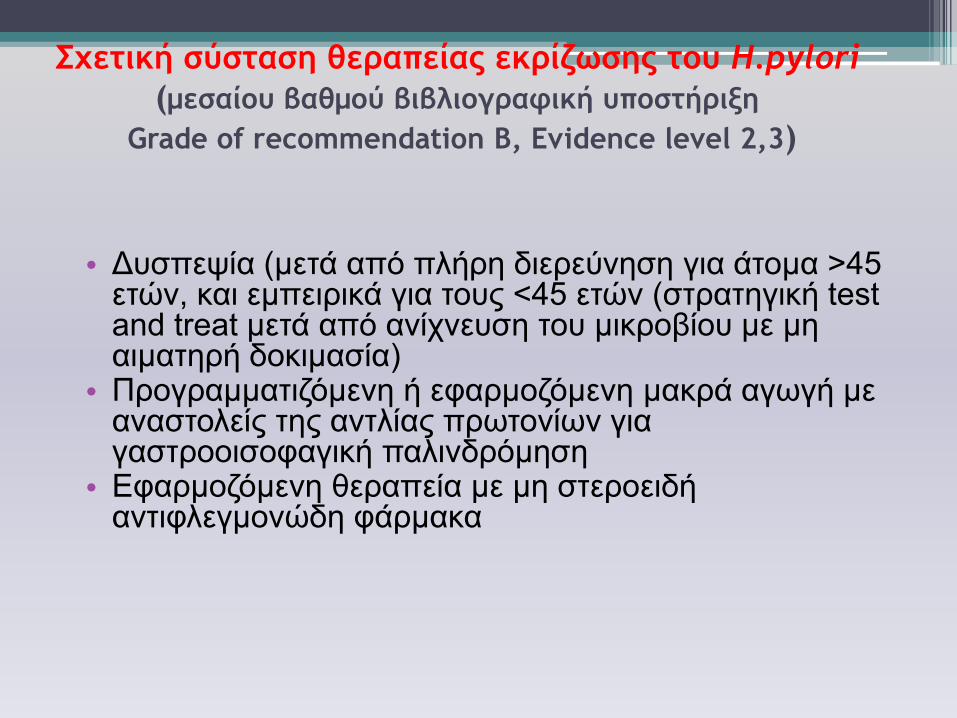
Συεςική ρύρςαρη θεοαπείαπ εκοίζωρηπ ςξσ H.pylori
(μεραίξσ βαθμξύ βιβλιξγοατική σπξρςήοινη
Grade of recommendation Β, Evidence level 2,3)
• Δπζπεςία (µεηά από πιήξε δηεξεύλεζε γηα άηνκα >45 εηώλ, θαη εκπεηξηθά γηα ηνπο <45 εηώλ (ζηξαηεγηθή test and treat κεηά από αλίρλεπζε ηνπ κηθξνβίνπ κε κε αηκαηεξή δνθηκαζία)
• Πξνγξαµµαηηδόµελε ή εθαξµνδόµελε καθξά αγσγή µε αλαζηνιείο ηεο αληιίαο πξσηνλίσλ γηα γαζηξννηζνθαγηθή παιηλδξόµεζε
• Εθαξµνδόµελε ζεξαπεία µε µε ζηεξνεηδή αληηθιεγµνλώδε θάξµαθα
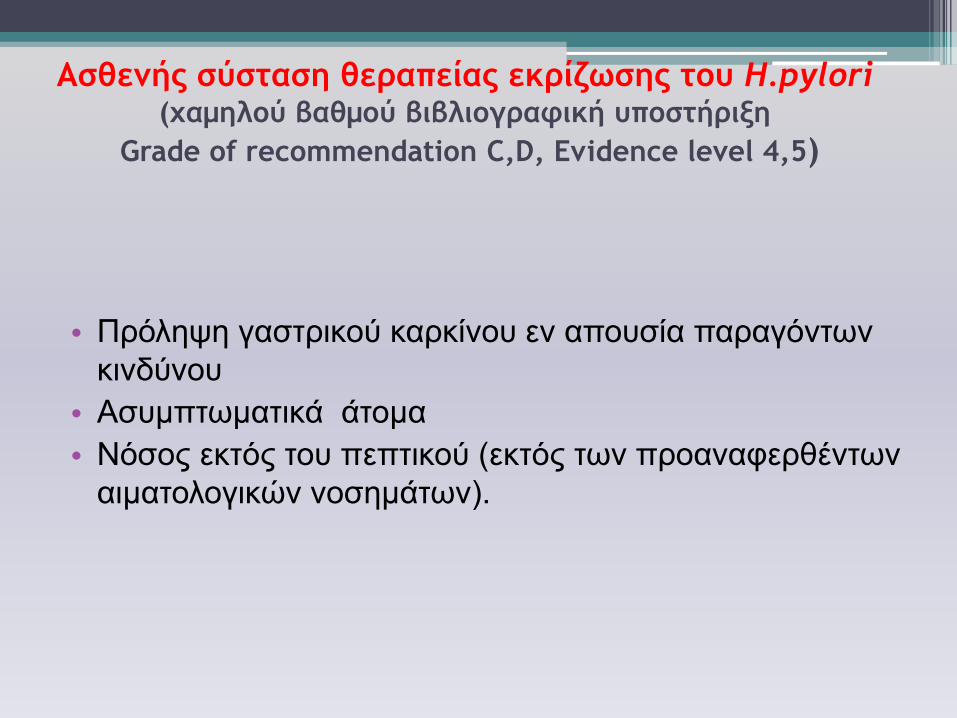
Αρθεμήπ ρύρςαρη θεοαπείαπ εκοίζωρηπ ςξσ H.pylori(υαμηλξύ βαθμξύ βιβλιξγοατική σπξρςήοινη
Grade of recommendation C,D, Evidence level 4,5)
• Πξόιεςε γαζηξηθνύ θαξθίλνπ ελ απνπζία παξαγόλησλ
θηλδύλνπ
• Αζπµπησµαηηθά άηνµα
• Νόζνο εθηόο ηνπ πεπηηθνύ (εθηόο ησλ πξναλαθεξζέλησλ
αηκαηνινγηθώλ λνζεκάησλ).
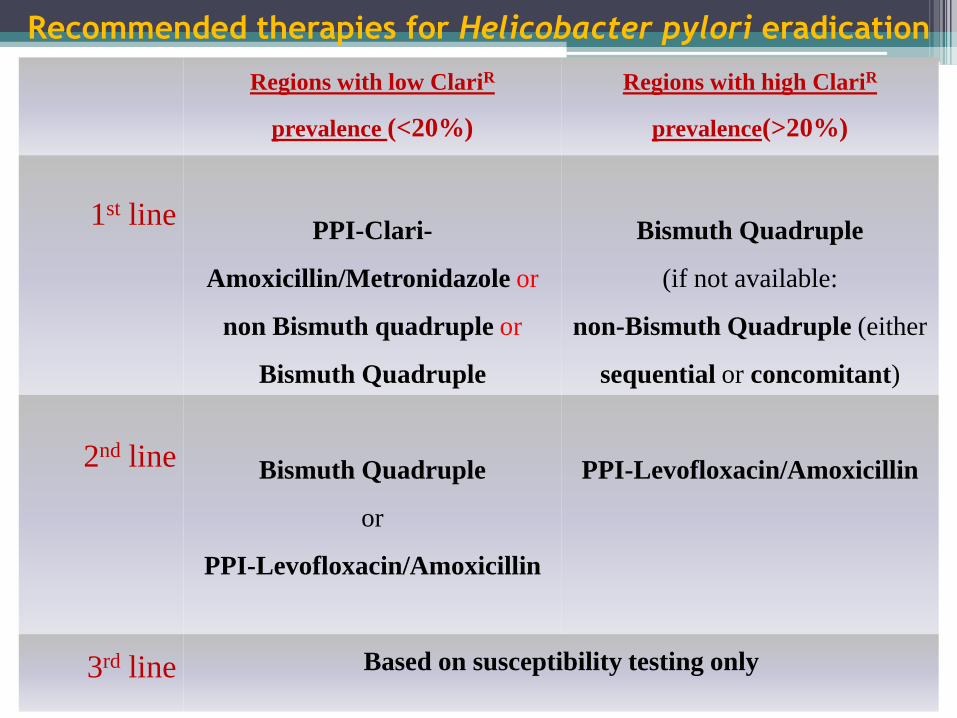
Recommended therapies for Helicobacter pylori eradication
Regions with low ClariR
prevalence (<20%)
Regions with high ClariR
prevalence(>20%)
1st linePPI-Clari-
Amoxicillin/Metronidazole or
non Bismuth quadruple or
Bismuth Quadruple
Bismuth Quadruple
(if not available:
non-Bismuth Quadruple (either
sequential or concomitant)
2nd lineBismuth Quadruple
or
PPI-Levofloxacin/Amoxicillin
PPI-Levofloxacin/Amoxicillin
3rd line Based on susceptibility testing only
H. pylori and MALT lymphoma
Statement : H. pylori eradication is the first line treatment for
low-grade gastric MALT lymphoma.
Evidence Level: 1a Grade of Recommendation: A
H. pylori and Atrophy / Intestinal
Metaplasia
Statement 11: There is accumulating evidence that following H. pylori eradication, corpus function may improve. However, whether this is associated with regression of atrophic gastritis remains equivocal.
Evidence Level: 2a Grade of Recommendation: B
Statement 11b: There is no evidence that H. pylori eradication can lead to regression of intestinal metaplasia.
Evidence Level: 2a Grade of Recommendation: B
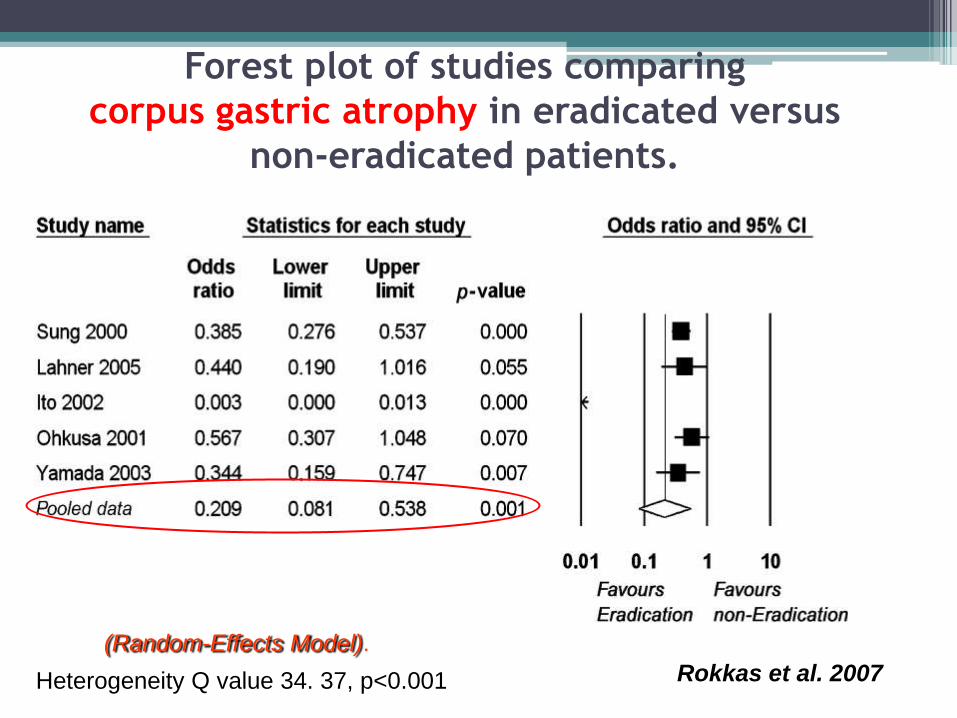
Forest plot of studies comparing
corpus gastric atrophy in eradicated versus
non-eradicated patients.
Rokkas et al. 2007Heterogeneity Q value 34. 37, p<0.001
(Random-Effects Model).
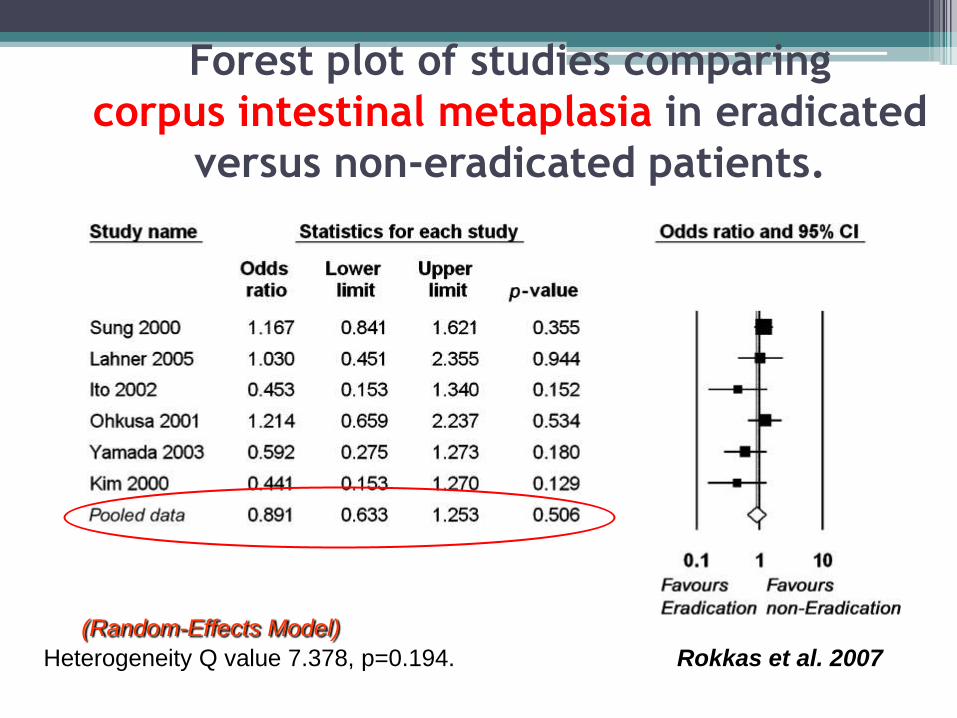
Forest plot of studies comparing
corpus intestinal metaplasia in eradicated
versus non-eradicated patients.
Rokkas et al. 2007
(Random-Effects Model)
Heterogeneity Q value 7.378, p=0.194.
Conclusion:
Compared with no eradication, the long-term
eradication histology results showed significant
improvement for GA for both antrum and corpus,
whereas such an improvement was not shown for IM at
both anatomical sites.
It seems that the development of IM in the stomach is
not reversible by H.pylori eradication and represents the
“point of no return”.
Therefore efforts should be directed at preventing the
development of such a lesion by treating the infection
early in life. Rokkas et al. 2007
Gastric cancer
• Statement : The risk of gastric cancer can be
reduced more effectively by employing
eradication therapy before the development of
preneoplastic conditions.
Evidence Level: 1a Grade of Recommendation: A
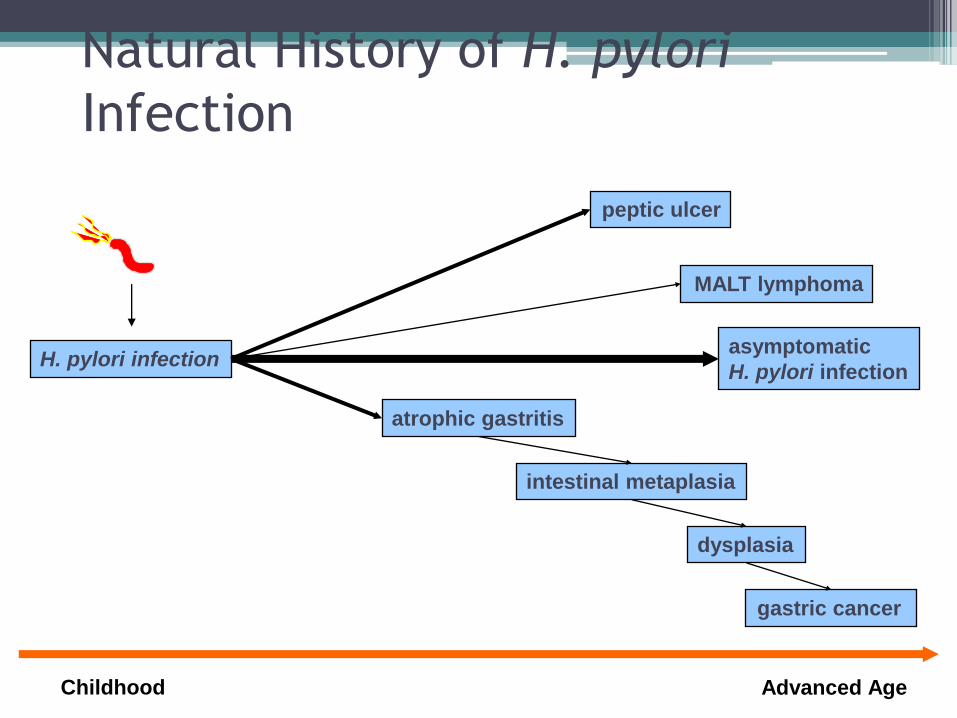
Natural History of H. pylori
Infection
intestinal metaplasia
dysplasia
gastric cancer
peptic ulcer
MALT lymphoma
Childhood Advanced Age
H. pylori infectionasymptomatic
H. pylori infection
atrophic gastritis
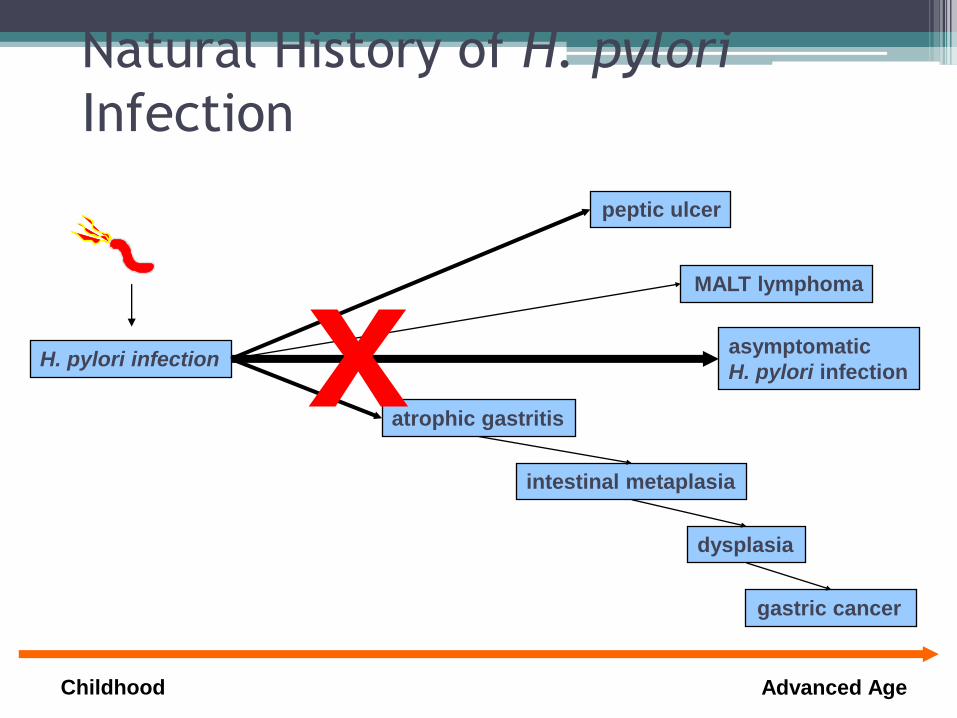
Natural History of H. pylori
Infection
intestinal metaplasia
dysplasia
gastric cancer
peptic ulcer
MALT lymphoma
Childhood Advanced Age
H. pylori infectionasymptomatic
H. pylori infection
atrophic gastritisx
Prevention of gastric cancer
• Statement
a) Preneoplastic high risk conditions require
endoscopic follow up.
b) Prospective studies are needed to determine
the correct timing of follow-up .
• Evidence Level: Grade of Recommendation:
Gastric cancer
• Statement : The risk of gastric cancer is influenced
by host genetic factors (IL-1ß, TNF-, IL-10, IFN-γ,
IL-8) but in clinical practice no specific marker can
be recommended for genetic testing at present.
Evidence Level: 1b Grade of Recommendation: A
Gastric cancer
• Statement : The influence of environmental
factors is subordinate to the effect of H. pylori
infection.
Evidence Level: 1a Grade of Recommendation: A
Gastric
CANCER
Host Genetics
H. pylori infection
Diet
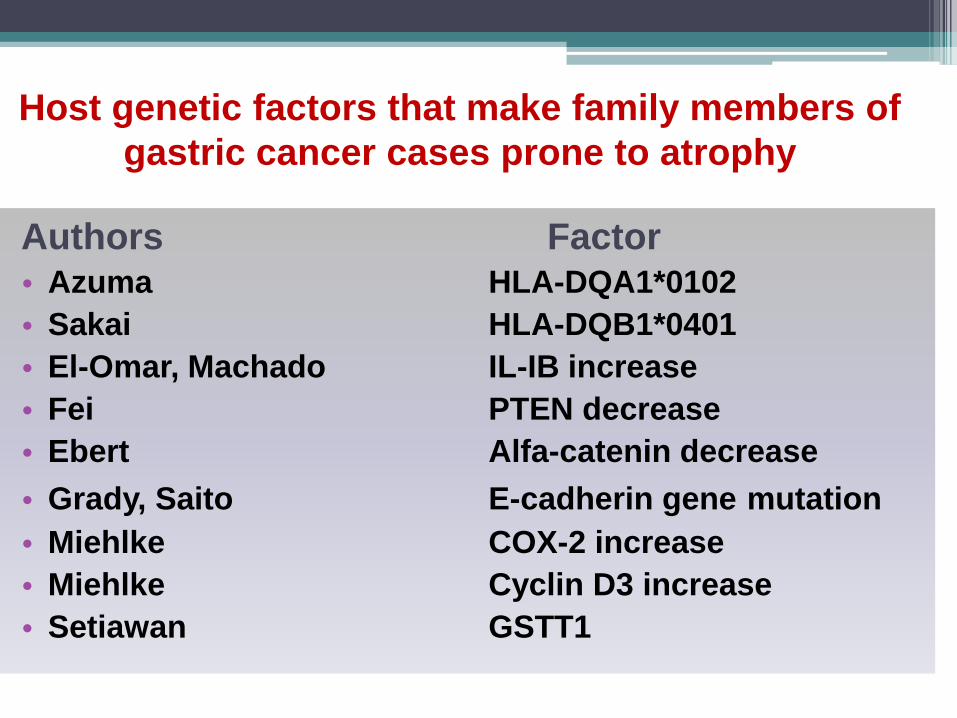
Host genetic factors that make family members of
gastric cancer cases prone to atrophy
Authors Factor• Azuma HLA-DQA1*0102
• Sakai HLA-DQB1*0401
• El-Omar, Machado IL-IB increase
• Fei PTEN decrease
• Ebert Alfa-catenin decrease
• Grady, Saito E-cadherin gene mutation
• Miehlke COX-2 increase
• Miehlke Cyclin D3 increase
• Setiawan GSTT1
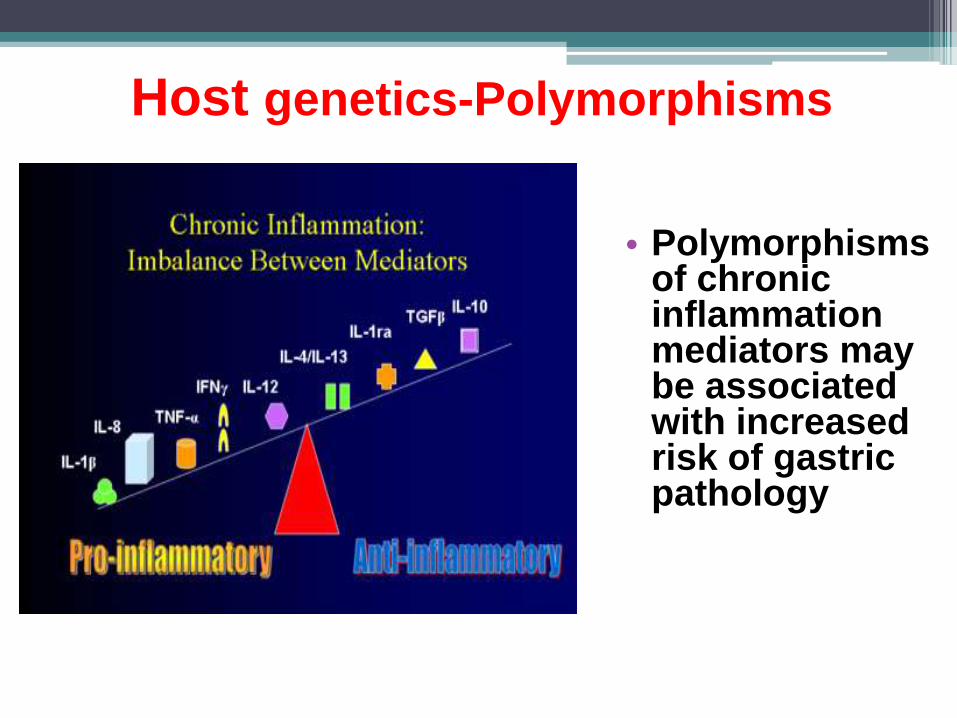
Host genetics-Polymorphisms
• Polymorphisms of chronic inflammation mediators may be associated with increased risk of gastric pathology
Diet and Gastric Cancer
• Summarised evidence suggests that raw vegetables and fruits containing vitamins C and E, beta-carotene and some minerals such as selenium, protect against stomach cancer.
• Ascorbic acid protective effect against gastric carcinogenesis is due to its ability to inactivate οxygen free radicals as well as its nitrite scavenging effects.
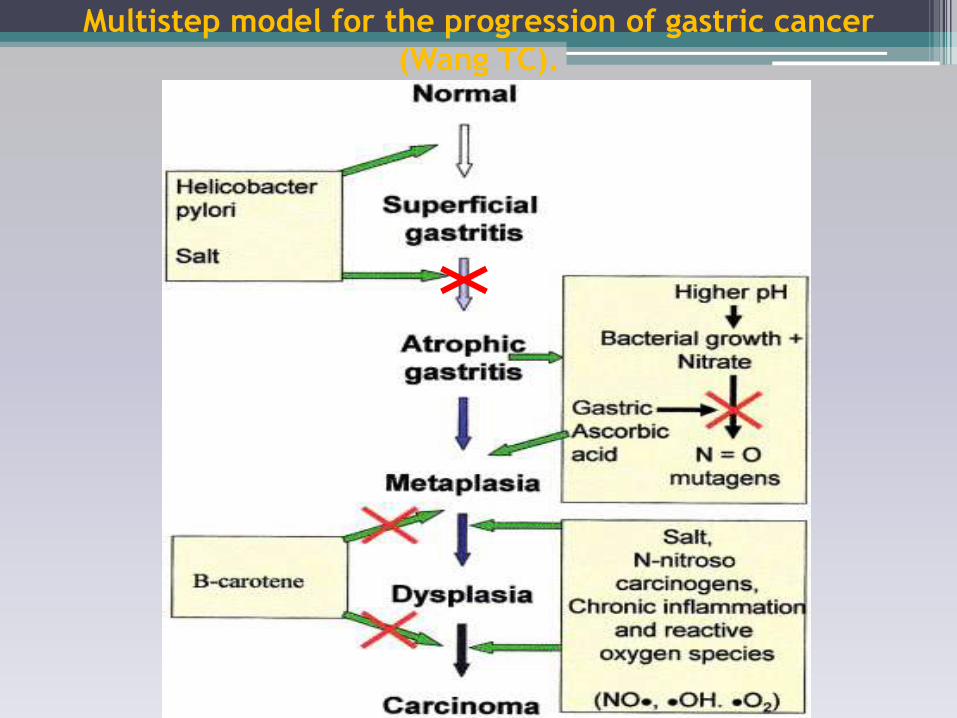
Multistep model for the progression of gastric cancer
(Wang TC).
Gastric cancer
• Statement : Validated serological tests for H. pylori
and markers of atrophy (i.e.pepsinogens) are the
best available non invasive tests to identify
subjects at high risk of gastric cancer.
Evidence level: 2b Grade of Recommendation: B
Prevention of gastric cancer
• Statement : H. pylori eradication to prevent gastric cancer should be
considered in the following individuals:
-First degree relatives of family members with a diagnosis of gastric
cancer
-Previous gastric neoplasia already treated by endoscopic or subtotal
gastric resection
-Patients with risk gastritis: severe pangastritis, corpus predominant
gastritis, severe atrophy
-Chronic gastric acid inhibition for more than one year
-Strong environmental risk factors for gastric cancer (heavy smoking,
work high exposure to dust, coal, quartz, cement, and/or work in
quarries)
-H. pylori positive patients with fear of gastric cancer
Evidence Level: 1c Grade of Recommendation: A
Σε κίνδσνο οι ζσγγενείς
αζθενών με γαζηρικό
καρκίνο;
Rokkas et al.,EJGH 2010
Meta-analysis
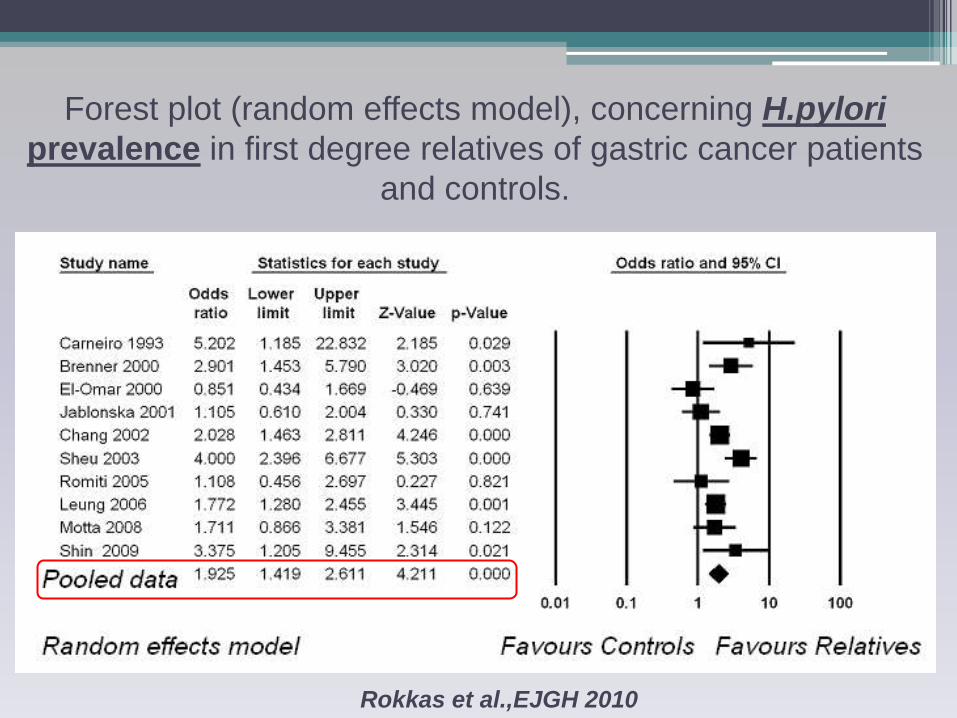
Forest plot (random effects model), concerning H.pylori
prevalence in first degree relatives of gastric cancer patients
and controls.
Rokkas et al.,EJGH 2010
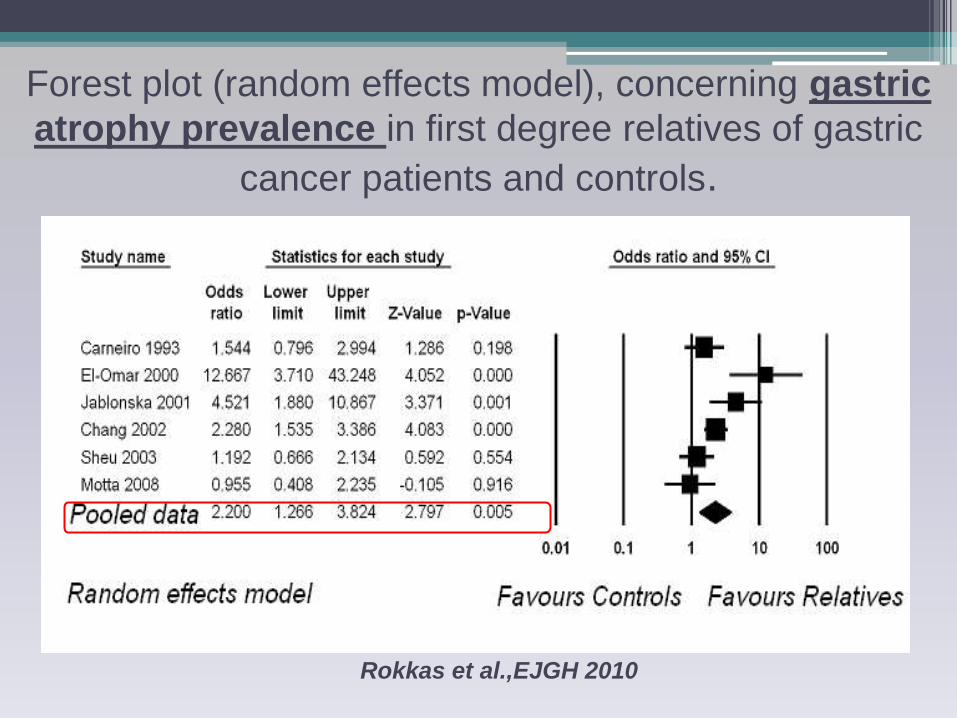
Forest plot (random effects model), concerning gastric
atrophy prevalence in first degree relatives of gastric
cancer patients and controls.
Rokkas et al.,EJGH 2010
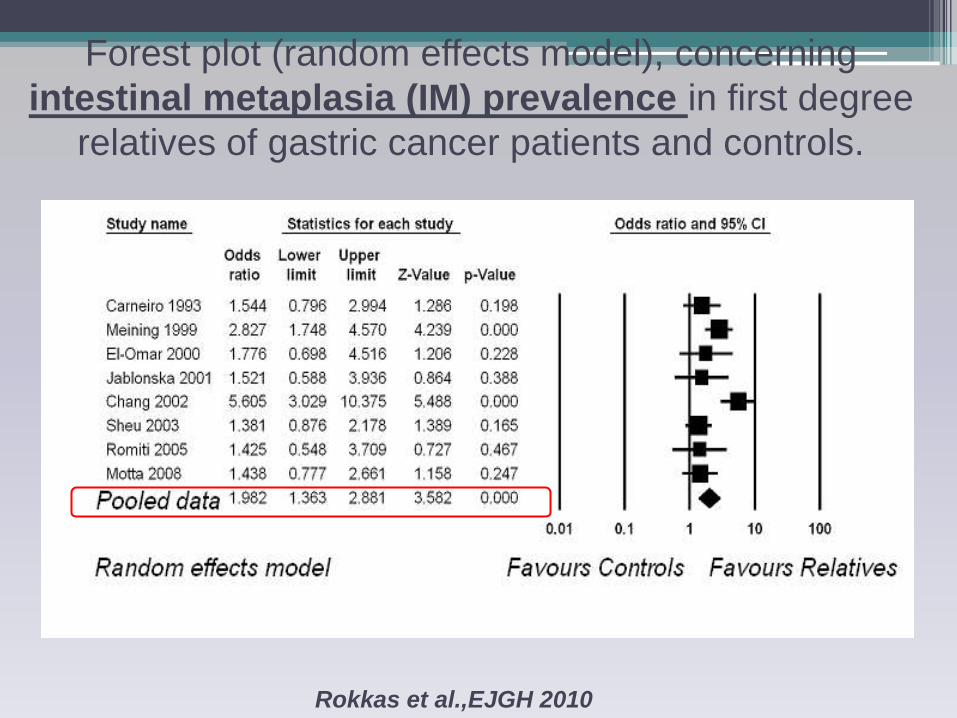
Forest plot (random effects model), concerning
intestinal metaplasia (IM) prevalence in first degree
relatives of gastric cancer patients and controls.
Rokkas et al.,EJGH 2010
Prevention of gastric cancer
Statement : H. pylori infection is the most consistent
risk factor for gastric cancer. Its elimination is
therefore the most promising strategy to reduce the
incidence of gastric cancer.
Evidence Level: 1a Grade of Recommendation: A
Gastric cancer
• Statement : H. pylori eradication for gastric
cancer prevention is cost effective in certain
communities with a high risk for gastric cancer.
• Evidence Level: 3b Grade of Recommendation: B
H. pylori Vaccine
Proof of Principle in Animals
Prophylactic
Therapeutic
Prevention of gastric cancer
• Statement : Vaccine would be the best option
for eliminating H. pylori infection in the
population. A major effort to develop one should
be made.
Evidence Level:1b Grade of Recommendation: A
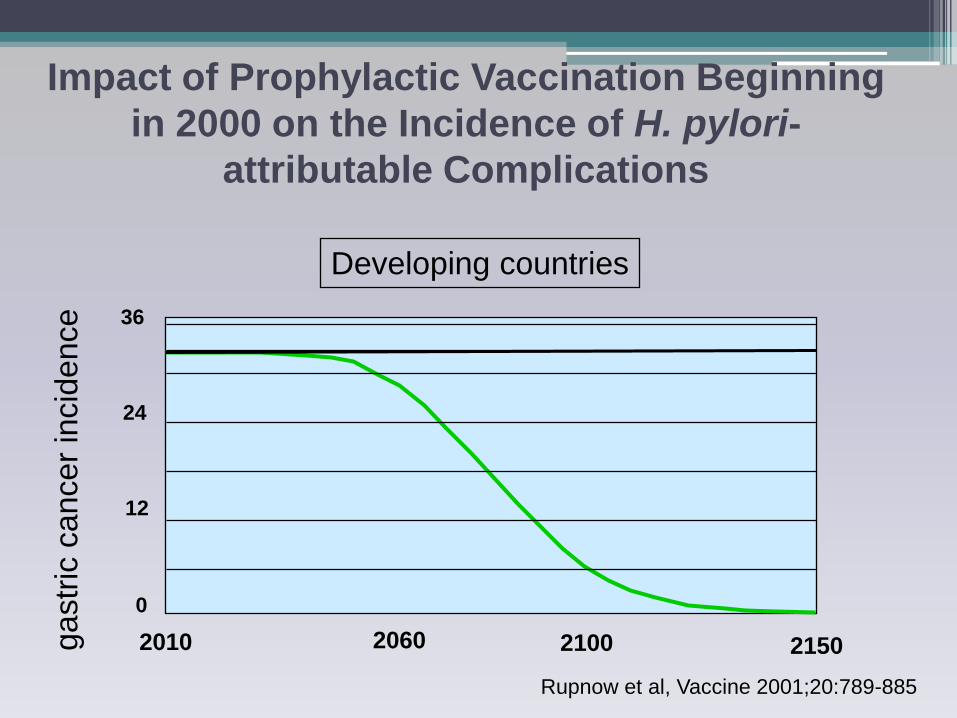
Impact of Prophylactic Vaccination Beginning
in 2000 on the Incidence of H. pylori-
attributable Complications
Rupnow et al, Vaccine 2001;20:789-885
ga
str
ic c
ancer
incid
ence
Developing countries
2010 2060 2150
0
2100
12
24
36



![Lecture Notes · Lecture Notes Heidelberg, ... Leon M. Lederman Melvin Schwartz Jack Steinberger [Nobel prize 1988] Discovery of the ... The Standard Model](https://static.fdocument.org/doc/165x107/5b8ae5ca7f8b9a9b7c8d4b35/lecture-notes-lecture-notes-heidelberg-leon-m-lederman-melvin-schwartz.jpg)