Μ.Μαδεμλή Επιστημονική Συνεργάτης Β ’ Εργαστήριο...
121
Σκιαγραφικά υλικά – Σκιαγραφικά υλικά – Εναλλακτικά Εναλλακτικά μέσα για νεφροπαθείς μέσα για νεφροπαθείς – Εναλλακτική – Εναλλακτική απεικόνιση για νεφροπαθείς – απεικόνιση για νεφροπαθείς – Αγγειογραφία Αγγειογραφία CO CO 2 Μ.Μαδεμλή Μ.Μαδεμλή Επιστημονική Συνεργάτης Επιστημονική Συνεργάτης Β’ Εργαστήριο Ακτινολογίας Β’ Εργαστήριο Ακτινολογίας
description
Σκιαγραφικά υλικά – Εναλλακτικά μέσα για νεφροπαθείς – Εναλλακτική απεικόνιση για νεφροπαθείς – Αγγειογραφία CO 2. Μ.Μαδεμλή Επιστημονική Συνεργάτης Β ’ Εργαστήριο Ακτινολογίας. Ενδοφλέβια σκιαγραφικά μέσα. - PowerPoint PPT Presentation
Transcript of Μ.Μαδεμλή Επιστημονική Συνεργάτης Β ’ Εργαστήριο...

Σκιαγραφικά υλικά –Σκιαγραφικά υλικά – Εναλλακτικά μέσα για Εναλλακτικά μέσα για νεφροπαθείςνεφροπαθείς – Εναλλακτική απεικόνιση για – Εναλλακτική απεικόνιση για
νεφροπαθείς – Αγγειογραφία νεφροπαθείς – Αγγειογραφία COCO22
Μ.ΜαδεμλήΜ.Μαδεμλή
Επιστημονική ΣυνεργάτηςΕπιστημονική Συνεργάτης
Β’ Εργαστήριο ΑκτινολογίαςΒ’ Εργαστήριο Ακτινολογίας

Ενδοφλέβια σκιαγραφικά μέσαΕνδοφλέβια σκιαγραφικά μέσα
ΙωδιούχαΙωδιούχα : Υπολογιστική Αγγειογραφία (: Υπολογιστική Αγγειογραφία (CTA), CTA), Ψηφιακή Αφαιρετική Αγγειογραφία (Ψηφιακή Αφαιρετική Αγγειογραφία (DSA)DSA)
Χηλικές ενώσεις γαδολινίουΧηλικές ενώσεις γαδολινίου : Μαγνητική : Μαγνητική Αγγειογραφία (Αγγειογραφία (MRAMRA))
Διοξείδιο άνθρακα Διοξείδιο άνθρακα COCO22 : Ψηφιακή Αφαιρετική : Ψηφιακή Αφαιρετική Αγγειογραφία (Αγγειογραφία (DSA)DSA)
ΜικροφυσαλίδεςΜικροφυσαλίδες: Υπερηχοτομογραφία: Υπερηχοτομογραφία (CEUS) (CEUS)

Ιωδιούχα σκιαγραφικά μέσαΙωδιούχα σκιαγραφικά μέσα

Ιωδιούχα ενδοφλέβια σκιαγραφικά μέσαΙωδιούχα ενδοφλέβια σκιαγραφικά μέσα
ΥδατοδιαλυτάΥδατοδιαλυτά, , εξωκυττάρια σκιαγραφικά μέσα με εξωκυττάρια σκιαγραφικά μέσα με βάσηβάση ιώδιοιώδιο
Το ιώδιο λόγω του υψηλού του ατομικού αριθμού Το ιώδιο λόγω του υψηλού του ατομικού αριθμού ((Z=Z=53) 53) απορροφά τις ακτίνες Χαπορροφά τις ακτίνες Χ και εμφανίζει και εμφανίζει σταθερή χημική δομή με το δακτύλιο του βενζολίουσταθερή χημική δομή με το δακτύλιο του βενζολίου
Διαχέονται στον εξωκυττάριο χώροΔιαχέονται στον εξωκυττάριο χώρο Λόγω της τοξικότητάς του, για την ενδοφλέβια Λόγω της τοξικότητάς του, για την ενδοφλέβια
χορήγηση του, χρησιμοποιείται μαζί με μία οργανική χορήγηση του, χρησιμοποιείται μαζί με μία οργανική ένωση πολύ χαμηλής τοξικότηταςένωση πολύ χαμηλής τοξικότητας
Μοριακή δομήΜοριακή δομή: : τρι-ιωδιωμένος δακτύλιος βενζολίουτρι-ιωδιωμένος δακτύλιος βενζολίου Ιονικά, Μη-ιονικάΙονικά, Μη-ιονικά, Μονομερή, Διμερή, Μονομερή, Διμερή

Φυσικοχημικές ιδιότητεςΦυσικοχημικές ιδιότητες
• Φαινόμενο ώσμωσηςΦαινόμενο ώσμωσης
Το φαινόμενο της παθητικής διάχυσης των μορίων του Το φαινόμενο της παθητικής διάχυσης των μορίων του διαλύτη ενός διαλύματος, από μια περιοχή χαμηλής διαλύτη ενός διαλύματος, από μια περιοχή χαμηλής συγκέντρωσης διαλυμένης ουσίας σε περιοχή μεγαλύτερης συγκέντρωσης διαλυμένης ουσίας σε περιοχή μεγαλύτερης συγκέντρωσης, μέσω μιας ημιδιαπερατής μεμβράνηςσυγκέντρωσης, μέσω μιας ημιδιαπερατής μεμβράνης
• Ωσμωτική πίεσηΩσμωτική πίεση
Η υδροστατική πίεση η οποία απαιτείται να εφαρμοσθεί επί Η υδροστατική πίεση η οποία απαιτείται να εφαρμοσθεί επί της πλευράς του πυκνότερου διαλύματος για να της πλευράς του πυκνότερου διαλύματος για να αντισταθμισθεί το φαινόμενο της ώσμωσης αντισταθμισθεί το φαινόμενο της ώσμωσης
• Ωσμωτικότητα (Ωσμωτικότητα (osmolarity)osmolarity)
Ωσμωτικότητα ενός διαλύματος είναι η Ωσμωτικότητα ενός διαλύματος είναι η συγκέντρωση συγκέντρωση ωσμωτικά δραστικών σωματιδίωνωσμωτικά δραστικών σωματιδίων ανεξάρτητα από το είδος ανεξάρτητα από το είδος της ουσίας. Μετράται σε ωσμώλια ανά λίτρο (osm/L). Η της ουσίας. Μετράται σε ωσμώλια ανά λίτρο (osm/L). Η μονάδα αφορά όγκο, και ο όγκος εξαρτάται από τη μονάδα αφορά όγκο, και ο όγκος εξαρτάται από τη θερμοκρασία και από το χώρο που κατέχουν οι διαλυμένες θερμοκρασία και από το χώρο που κατέχουν οι διαλυμένες ουσίες ουσίες

Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής αντίθεσηςυδατοδιαλυτών μέσων σκιαγραφικής αντίθεσης
ΩσμωμοριακότηταΩσμωμοριακότητα (osmola(osmolallity) ity)
Ωσμωμοριακότητα ενός διαλύματος ορίζεται από τον Ωσμωμοριακότητα ενός διαλύματος ορίζεται από τον αριθμό αριθμό των μορίων-σωματιδίων /Kg διαλύτη των μορίων-σωματιδίων /Kg διαλύτη ((mmOsm/kg HOsm/kg H22O)O)
εξαρτάται από τη μάζα του διαλύτηεξαρτάται από τη μάζα του διαλύτη
ελαττώνεται όσο αυξάνει ο αριθμός των ατόμων του ελαττώνεται όσο αυξάνει ο αριθμός των ατόμων του ιωδίου προς τα στοιχεία στο διάλυμαιωδίου προς τα στοιχεία στο διάλυμα
δεν εξαρτάται από την θερμοκρασία (σε αντίθεση με την δεν εξαρτάται από την θερμοκρασία (σε αντίθεση με την ωσμωτικότητα)ωσμωτικότητα)
δεν εξαρτάται από το μοριακό βάρος της διαλυμένης δεν εξαρτάται από το μοριακό βάρος της διαλυμένης ουσίαςουσίας
Ισοωσμωτικό διάλυμαΙσοωσμωτικό διάλυμα
Το διάλυμα που έχει ωσμωμοριακότητα ίση με του Το διάλυμα που έχει ωσμωμοριακότητα ίση με του πλάσματος του αίματος (290πλάσματος του αίματος (290mosm/Kg)mosm/Kg). Αντίστοιχα . Αντίστοιχα υπάρχουν τα υπερ- και υποωσμωτικά διαλύματαυπάρχουν τα υπερ- και υποωσμωτικά διαλύματα
Η ωσμωμοριακότητα των ιωδιωμένων ΣΜ είναι μεγαλύτερη Η ωσμωμοριακότητα των ιωδιωμένων ΣΜ είναι μεγαλύτερη από του πλάσματοςαπό του πλάσματος

Επιδράσεις υψηλής ωσμωμοριακότηταςΕπιδράσεις υψηλής ωσμωμοριακότητας
Παθητική μεταφορά υγρών από ενδοκυττάριο στον Παθητική μεταφορά υγρών από ενδοκυττάριο στον εξωκυττάριο/ ενδαγγειακό χώρο εξωκυττάριο/ ενδαγγειακό χώρο αφυδάτωση αφυδάτωση κυττάρων και αύξηση του εσωτερικού τους ιξώδους κυττάρων και αύξηση του εσωτερικού τους ιξώδους απώλεια το φυσιολογικό του σχήμα και της απώλεια το φυσιολογικό του σχήμα και της φυσιολογικής τους λειτουργίαςφυσιολογικής τους λειτουργίας
αφυδάτωση ερυθρών αιμοσφαιρίων αφυδάτωση ερυθρών αιμοσφαιρίων ανοξία των ανοξία των ιστώνιστών
καταστροφή του ενδοθηλίου των αγγείων καταστροφή του ενδοθηλίου των αγγείων απελευθέρωση αγγειοκινητικών ουσιών απελευθέρωση αγγειοκινητικών ουσιών (λευκοτριένες, ισταμίνη και προσταγλαδίνες, (λευκοτριένες, ισταμίνη και προσταγλαδίνες, βραδυκινίνη, ενεργοποίηση συμπληρώματος και βραδυκινίνη, ενεργοποίηση συμπληρώματος και του παράγοντα πήξης VII) του παράγοντα πήξης VII)

Επιδράσεις υψηλής ωσμωμοριακότηταςΕπιδράσεις υψηλής ωσμωμοριακότητας
αιμοδυναμικές διαταραχές (αύξηση αιμοδυναμικές διαταραχές (αύξηση κυκλοφορούντος όγκου αίματος κυκλοφορούντος όγκου αίματος αγγειοδιαστολή, ελάττωση περιφερικών αγγειοδιαστολή, ελάττωση περιφερικών αντιστάσεων αντιστάσεων ελάττωση Α.Π.) ελάττωση Α.Π.)
διαταραχές καρδιακής λειτουργίας (διαταραχές καρδιακής λειτουργίας ( όγκου όγκου παλμού, αρνητική ινότροπο δράση και παλμού, αρνητική ινότροπο δράση και αρρυθμίες)αρρυθμίες)
βλάβη αιματοεγκεφαλικού φραγμούβλάβη αιματοεγκεφαλικού φραγμού διούρηση, αφυδάτωσηδιούρηση, αφυδάτωση αίσθημα θερμότητας, ερυθρότητααίσθημα θερμότητας, ερυθρότητα πόνοπόνο

Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής αντίθεσηςυδατοδιαλυτών μέσων σκιαγραφικής αντίθεσης
ΓλοιότηταΓλοιότητα το μέτρο της αντίστασης ροής του ΣΜ στο πλάσμα του το μέτρο της αντίστασης ροής του ΣΜ στο πλάσμα του
αίματος. Μετράται σε millipascal x sec (mPa αίματος. Μετράται σε millipascal x sec (mPa XX s) s) εξαρτάται άμεσα από την Θεξαρτάται άμεσα από την Θ00C, από το ΜΒ, το μέγεθος και το C, από το ΜΒ, το μέγεθος και το
σχήμα των μορίων και τον αριθμό των υδροξυλίων στο σχήμα των μορίων και τον αριθμό των υδροξυλίων στο μόριο, σχετίζεται με τη συγκέντρωση του διαλύματοςμόριο, σχετίζεται με τη συγκέντρωση του διαλύματος
Χαμηλή γλοιότηταΧαμηλή γλοιότητα αύξηση ρυθμού χορήγησης αύξηση ρυθμού χορήγησης αποφυγή προβλημάτων από τη μικροκυκλοφορία αποφυγή προβλημάτων από τη μικροκυκλοφορία ελάττωση εμφάνισης αλλεργικών αντιδράσεωνελάττωση εμφάνισης αλλεργικών αντιδράσεων χορηγώντας τα σκιαγραφικά στη θερμοκρασία του σώματος χορηγώντας τα σκιαγραφικά στη θερμοκρασία του σώματος
(37(3700C) η γλοιότητα ελαττώνεται σε ποσοστό > 50%C) η γλοιότητα ελαττώνεται σε ποσοστό > 50% τα διμερή μέσα σκιαγραφικής αντίθεσης έχουν υψηλότερη τα διμερή μέσα σκιαγραφικής αντίθεσης έχουν υψηλότερη
γλοιότητα από τα μονομερή (με μικρότερο μόριο)γλοιότητα από τα μονομερή (με μικρότερο μόριο)

Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής αντίθεσηςυδατοδιαλυτών μέσων σκιαγραφικής αντίθεσης
Υδροφιλία-ΥδατοδιαλυτότηταΥδροφιλία-Υδατοδιαλυτότητα • εξαρτάται άμεσα από τον αριθμό των υδροξυλίων στο εξαρτάται άμεσα από τον αριθμό των υδροξυλίων στο
μόριομόριο
• τα υδροξύλια στο μόριο των μη ιονικών μέσων τα υδροξύλια στο μόριο των μη ιονικών μέσων σκιαγραφικής αντίθεσης ελαττώνουν την ικανότητα σκιαγραφικής αντίθεσης ελαττώνουν την ικανότητα σύνδεσής τους με τις πρωτείνες του πλάσματος, σύνδεσής τους με τις πρωτείνες του πλάσματος, καθιστώντας τα περισσότερο αδρανήκαθιστώντας τα περισσότερο αδρανή
τα ενδοφλεβίως χορηγούμενα μέσα σκιαγραφικής τα ενδοφλεβίως χορηγούμενα μέσα σκιαγραφικής αντίθεσης πρέπει να είναι εξαιρετικά υδατοδιαλυτά, αντίθεσης πρέπει να είναι εξαιρετικά υδατοδιαλυτά, ώστε να αποφεύγεται η κρυσταλλοποίησή τους μέσα στις ώστε να αποφεύγεται η κρυσταλλοποίησή τους μέσα στις σύριγγες ή τα αγγεία του σώματοςσύριγγες ή τα αγγεία του σώματος

Συγκέντρωση ιωδίουΣυγκέντρωση ιωδίου Η συγκέντρωση του ιωδίου καθορίζεται από τον αριθμό Η συγκέντρωση του ιωδίου καθορίζεται από τον αριθμό
μορίων του ιωδίου σε μορίων του ιωδίου σε mg mg ανά ml του διαλύματοςανά ml του διαλύματος (mg/ml)(mg/ml)
Καθορίζει την ακτινοσκιερότητα του ΣΜ και είναι Καθορίζει την ακτινοσκιερότητα του ΣΜ και είναι ανάλογη αυτήςανάλογη αυτής
Η υψηλή συγκέντρωση του ΣΜ αυξάνει τις πιθανότητες Η υψηλή συγκέντρωση του ΣΜ αυξάνει τις πιθανότητες ανεπιθύμητων ενεργειώνανεπιθύμητων ενεργειών
Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής
αντίθεσηςαντίθεσης

Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων Φυσικοχημικές ιδιότητες ΕΦ χορηγούμενων ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής αντίθεσηςυδατοδιαλυτών μέσων σκιαγραφικής αντίθεσης
• Ιονικά μέσα σκιαγραφικής αντίθεσηςΙονικά μέσα σκιαγραφικής αντίθεσης
Τα ιονικά σύμπλοκα (άλατα) σε διάλυμα διασπώνται σε Τα ιονικά σύμπλοκα (άλατα) σε διάλυμα διασπώνται σε ανιόνταανιόντα-- και κατιόντα και κατιόντα+ + και κάθε διαλυμένο μόριο αποδίδει και κάθε διαλυμένο μόριο αποδίδει δύο σωματίδιαδύο σωματίδια
Υψηλή ωσμομοριακότηταΥψηλή ωσμομοριακότητα
• Μη ιονικά μέσα σκιαγραφικής αντίθεσηςΜη ιονικά μέσα σκιαγραφικής αντίθεσης
Στο μόριο τους υπάρχουν υδροξυλικές ομάδες στις Στο μόριο τους υπάρχουν υδροξυλικές ομάδες στις οργανικές πλευρικές αλυσίδες που βρίσκονται στις θέσεις οργανικές πλευρικές αλυσίδες που βρίσκονται στις θέσεις 1,3,5. 1,3,5.
Δεν διασπώνται σε διάλυμαΔεν διασπώνται σε διάλυμα
Κάθε διαλυμένο μόριο αποδίδει ένα σωματίδιο στο διάλυμαΚάθε διαλυμένο μόριο αποδίδει ένα σωματίδιο στο διάλυμα
Υποδιπλάσια ωσμωμοριακότητα σε σχέση με τα ιονικάΥποδιπλάσια ωσμωμοριακότητα σε σχέση με τα ιονικά

Ιονικά μονομερή ιωδιωμένα μέσαΙονικά μονομερή ιωδιωμένα μέσα
Το πρόβλημαΤο πρόβλημα
Τα ιονικά μονομερή ιωδιωμένα μέσα σκιαγραφικής αντίθεσης ως άλατα Τα ιονικά μονομερή ιωδιωμένα μέσα σκιαγραφικής αντίθεσης ως άλατα αποτελούνταν από ένα ανιόν (COOαποτελούνταν από ένα ανιόν (COO--) και από ένα κατιόν μέρος (Η) και από ένα κατιόν μέρος (Η++ ή Na ή Na++ ή ή MeglMegl++ /μεθυλγλυκαμίνη) /μεθυλγλυκαμίνη).. Η παρουσία ιόντων Η παρουσία ιόντων μεταβάλλει την ηλεκτρολυτικήμεταβάλλει την ηλεκτρολυτική ισορροπία, η οποία με τη σειρά της ισορροπία, η οποία με τη σειρά της επηρεάζει τη διαπερατότητα των κυτταρικών επηρεάζει τη διαπερατότητα των κυτταρικών μεμβρανώνμεμβρανών
• απελευθέρωση ιόντωναπελευθέρωση ιόντων στον εξωκυττάριο χώρο στον εξωκυττάριο χώρο. . Τα ελεύθερα ιόντα των Τα ελεύθερα ιόντα των ιονικών μέσων σκιαγραφικής αντίθεσης προκαλούν: ιονικών μέσων σκιαγραφικής αντίθεσης προκαλούν: • δερματικές εκδηλώσεις• δερματικές εκδηλώσεις• οίδημα της γλωττίδος• οίδημα της γλωττίδος• βρογχόσπασμο και κώμα• βρογχόσπασμο και κώμα
• υψηλή ωσμωμοριακότηταυψηλή ωσμωμοριακότητα, προκειμένου να πραγματοποιηθεί , προκειμένου να πραγματοποιηθεί ικανοποιητική ικανοποιητική συγκέντρωση ιωδίου σε πρακτικά μικρούς όγκουςσυγκέντρωση ιωδίου σε πρακτικά μικρούς όγκους (Conray 300 mg/ml, (Conray 300 mg/ml, ωσμωμοριακότητα 1530 mOsm/kg Hωσμωμοριακότητα 1530 mOsm/kg H220 σε σχέση με εκείνη του πλάσματος, 0 σε σχέση με εκείνη του πλάσματος, του υγρού των ιστών και των κυττάρων του ανθρώπινου οργανισμού που του υγρού των ιστών και των κυττάρων του ανθρώπινου οργανισμού που είναι περίπου 290 mOsm/kg Hείναι περίπου 290 mOsm/kg H220)0)


ΔοσολογίαΔοσολογία Εξαρτάται από τη συγκέντρωση του ΣΜ, τον τύπο (ιονικό, Εξαρτάται από τη συγκέντρωση του ΣΜ, τον τύπο (ιονικό,
μη-ιονικό), το ΣΒ, την ηλικία του εξεταζόμενου μη-ιονικό), το ΣΒ, την ηλικία του εξεταζόμενου
5ml/kg 5ml/kg σωματικού βάρους (μη ιονικά μέσα σκιαγραφικής σωματικού βάρους (μη ιονικά μέσα σκιαγραφικής αντίθεσης συγκέντρωσης 300mg I/mL)αντίθεσης συγκέντρωσης 300mg I/mL)
2-3ml/kg σωματικού βάρους (ιονικά μέσα)2-3ml/kg σωματικού βάρους (ιονικά μέσα)
Η χορήγηση ΣΜ σε αναλογία Η χορήγηση ΣΜ σε αναλογία gram I : GFR gram I : GFR ίση με ίση με 1:11:1 θεωρείται σχετικά ασφαλής αν δεν υφίστανται άλλοι θεωρείται σχετικά ασφαλής αν δεν υφίστανται άλλοι παράγοντες κινδύνουπαράγοντες κινδύνου
Παράγοντες που επηρεάζουν τη δοσολογίαΠαράγοντες που επηρεάζουν τη δοσολογία ηλικία εξεταζομένουηλικία εξεταζομένου νεφρική λειτουργία νεφρική λειτουργία
Παράγοντες χορήγησης ΕΦ χορηγούμενων ιωδιωμένων Παράγοντες χορήγησης ΕΦ χορηγούμενων ιωδιωμένων υδατοδιαλυτών μέσων σκιαγραφικής αντίθεσηςυδατοδιαλυτών μέσων σκιαγραφικής αντίθεσης

Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. ΌψιμεςΌψιμες
3.3. ΚαθυστερημένεςΚαθυστερημένες

Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. ΌψιμεςΌψιμες
3.3. ΚαθυστερημένεςΚαθυστερημένες

Ταξινόμηση άμεσων μη-νεφρικών αντιδράσεωνΤαξινόμηση άμεσων μη-νεφρικών αντιδράσεων
ανεπιθύμητες ενέργειες που εμφανίζονται έως ανεπιθύμητες ενέργειες που εμφανίζονται έως και 1 ώρα μετά την έγχυσηκαι 1 ώρα μετά την έγχυση
• ΉπιεςΉπιες :: ναυτία, ήπιοι έμετοι, κνίδωση, κνησμόςναυτία, ήπιοι έμετοι, κνίδωση, κνησμός
• Ενδιάμεσες Ενδιάμεσες :: έντονοι έμετοι, κνίδωση με έντονοι έμετοι, κνίδωση με στίγματα, βρογχόσπασμος, λαρυγγικό ή προσωπικό στίγματα, βρογχόσπασμος, λαρυγγικό ή προσωπικό οίδημα αντίδραση παρασυμπαθητικούοίδημα αντίδραση παρασυμπαθητικού
• Σοβαρές - απειλητικές για τη ζωήΣοβαρές - απειλητικές για τη ζωή :: υποτασική υποτασική καταπληξία, πνευμονικό οίδημα, αναπνευστική καταπληξία, πνευμονικό οίδημα, αναπνευστική ανακοπή, καρδιακή ανακοπή, σπασμοίανακοπή, καρδιακή ανακοπή, σπασμοί

Κατηγορίες οξέων ανεπιθύμητων αντιδράσεων των Κατηγορίες οξέων ανεπιθύμητων αντιδράσεων των ιωδιωμένων μέσων σκιαγραφικής αντίθεσηςιωδιωμένων μέσων σκιαγραφικής αντίθεσης
1.1. Ιδιοσυγκρασιακές συστηματικές αντιδράσεις Ιδιοσυγκρασιακές συστηματικές αντιδράσεις απρόβλεπτες αντιδράσεις αναφυλακτοειδούς απρόβλεπτες αντιδράσεις αναφυλακτοειδούς
τύπουτύπου Δεν σχετίζονται με την ποσότητα του ΣΜΔεν σχετίζονται με την ποσότητα του ΣΜ υπάρχουν κάποιοι προδιαθεσικοί παράγοντεςυπάρχουν κάποιοι προδιαθεσικοί παράγοντες Αποδίδονται στην έκλυση ισταμίνης, Αποδίδονται στην έκλυση ισταμίνης,
σεροτονίνης, προσταγλαδινών, αδενοσίνης, σεροτονίνης, προσταγλαδινών, αδενοσίνης, λευκοτριενών, κυτοκινών και ενδοθηλίνηςλευκοτριενών, κυτοκινών και ενδοθηλίνης
Εμφανίζονται έως 1 ώρα μετά την έγχυση του Εμφανίζονται έως 1 ώρα μετά την έγχυση του ΣΜ, ενώ οι σοβαρότερες εντός 20ΣΜ, ενώ οι σοβαρότερες εντός 20minmin
εκδηλώνονται με συμπτώματα κνίδωσης, εκδηλώνονται με συμπτώματα κνίδωσης, προσωπικού ή λαρυγγικού οιδήματος, προσωπικού ή λαρυγγικού οιδήματος, βρογχόσπασμου και υπότασηςβρογχόσπασμου και υπότασης

2.2. Χημειοτοξικές αντιδράσειςΧημειοτοξικές αντιδράσεις
εξαρτώμενες από τις φυσικοχημικές ιδιότητες εξαρτώμενες από τις φυσικοχημικές ιδιότητες (ωσμωμοριακότητα, γλοιότητα, υδροφιλία, (ωσμωμοριακότητα, γλοιότητα, υδροφιλία, συγγένεια με πρωτεΐνες, σύνδεση με συγγένεια με πρωτεΐνες, σύνδεση με CaCa+2+2, , περιεκτικότητα περιεκτικότητα NaNa++) και την ταχύτητα ) και την ταχύτητα χορήγησης των σκιαγραφικώνχορήγησης των σκιαγραφικών
Σχετίζονται με τη δοσολογία του ΣΜΣχετίζονται με τη δοσολογία του ΣΜ Πιθανότερες σε εξασθενημένους και ασταθείς Πιθανότερες σε εξασθενημένους και ασταθείς
ασθενείςασθενείς εκδηλώνονται με διαταραχές του εκδηλώνονται με διαταραχές του
καρδιαγγειακού , αναπνευστικού, καρδιαγγειακού , αναπνευστικού, ουροποιητικού, ΓΕΣ, νευρικού συστήματος ουροποιητικού, ΓΕΣ, νευρικού συστήματος (παρασυμπαθητικού) και του δέρματος. (παρασυμπαθητικού) και του δέρματος.
Κατηγορίες οξέων ανεπιθύμητων αντιδράσεων Κατηγορίες οξέων ανεπιθύμητων αντιδράσεων των ιωδιωμένων μέσων σκιαγραφικής των ιωδιωμένων μέσων σκιαγραφικής
αντίθεσηςαντίθεσης

3.3. Τοπική Εξαγγείωση ΣΜΤοπική Εξαγγείωση ΣΜ
μπορεί να συμβεί τόσο μετά ενδαρτηριακή όσο μπορεί να συμβεί τόσο μετά ενδαρτηριακή όσο και μετά ενδοφλέβια χορήγησηκαι μετά ενδοφλέβια χορήγηση
συμβαίνει συνήθως σε ηλικιωμένους, σε συμβαίνει συνήθως σε ηλικιωμένους, σε πάσχοντες από σακχαρώδη διαβήτη, από πάσχοντες από σακχαρώδη διαβήτη, από νοσήματα του συνδετικού ιστού, από νοσήματα του συνδετικού ιστού, από αρτηριοσκλήρυνση, ή μετά από επανειλημμένες αρτηριοσκλήρυνση, ή μετά από επανειλημμένες προσπάθειες παρακέντησης προσπάθειες παρακέντησης
μπορεί να προκληθεί μέχρι και τοπική νέκρωσημπορεί να προκληθεί μέχρι και τοπική νέκρωση
Κατηγορίες οξέων ανεπιθύμητων αντιδράσεων Κατηγορίες οξέων ανεπιθύμητων αντιδράσεων των ιωδιωμένων μέσων σκιαγραφικής των ιωδιωμένων μέσων σκιαγραφικής
αντίθεσηςαντίθεσης

Σχετιζόμενες με τον ασθενήΣχετιζόμενες με τον ασθενή
1.1. Προηγηθείσα μέτρια ή σοβαρή άμεση αντίδραση σε Προηγηθείσα μέτρια ή σοβαρή άμεση αντίδραση σε ιωδιούχο ΣΜ:ιωδιούχο ΣΜ: Ο κίνδυνος εμφάνισης ανεπιθύμητων Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά αντιδράσεων αυξάνει κατά 6 φορές6 φορές σε ασθενείς με σε ασθενείς με γνωστή γνωστή υπερευαισθησίαυπερευαισθησία συγκριτικά με τους ελεύθερους ιστορικού συγκριτικά με τους ελεύθερους ιστορικού
2.2. Άσθμα:Άσθμα: Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά αυξάνει κατά 6-10 6-10 φορές σε ασθενείς με γνωστό άσθμα φορές σε ασθενείς με γνωστό άσθμα συγκριτικά με τους ελεύθερους ιστορικούσυγκριτικά με τους ελεύθερους ιστορικού
3.3. Αλλεργία που χρήζει φαρμακευτικής αγωγής:Αλλεργία που χρήζει φαρμακευτικής αγωγής: Ο κίνδυνος Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά 3 3 φορέςφορές σε ασθενείς με γνωστή αλλεργία (σε σε ασθενείς με γνωστή αλλεργία (σε περιβαλλοντολογικούς παράγοντες ή φαρμακευτικά περιβαλλοντολογικούς παράγοντες ή φαρμακευτικά σκευάσματα) συγκριτικά με τους ελεύθερους ιστορικού σκευάσματα) συγκριτικά με τους ελεύθερους ιστορικού
Σχετιζόμενες με τον τύπο του χορηγούμενου ΣΜΣχετιζόμενες με τον τύπο του χορηγούμενου ΣΜ
• Υψηλής ωσμωμοριακότητας Ιονικό ΣΜ (Υψηλής ωσμωμοριακότητας Ιονικό ΣΜ (HOCM-ionic)HOCM-ionic):: Ο Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά κατά 4-5 φορές4-5 φορές σε σχέση με τα μη-ιονικά ΣΜ σε σχέση με τα μη-ιονικά ΣΜ
Παράγοντες κινδύνου εμφάνισης οξέων Παράγοντες κινδύνου εμφάνισης οξέων ανεπιθύμητων αντιδράσεωνανεπιθύμητων αντιδράσεων

Για όλους τους ασθενείςΓια όλους τους ασθενείς
1.1. Χρησιμοποίηση Χρησιμοποίηση μη ιονικού ΣΜμη ιονικού ΣΜ
2.2. Κρατήστε τον ασθενή για Κρατήστε τον ασθενή για παρακολούθηση για 30minπαρακολούθηση για 30min μετά τη μετά τη χορήγηση του σκιαγραφικούχορήγηση του σκιαγραφικού
3.3. Έχετε άμεσα διαθέσιμο τον εξοπλισμό και τα φάρμακα για Έχετε άμεσα διαθέσιμο τον εξοπλισμό και τα φάρμακα για ανάνηψηανάνηψη
Για ασθενείς αυξημένου κινδύνουΓια ασθενείς αυξημένου κινδύνου
1.1. Εξετάστε το ενδεχόμενο Εξετάστε το ενδεχόμενο εναλλακτικού τρόπου εξέτασηςεναλλακτικού τρόπου εξέτασης που να μην που να μην απαιτεί χρήση ιωδιούχου ΣΜαπαιτεί χρήση ιωδιούχου ΣΜ
2.2. Χρήση Χρήση διαφορετικού σκευάσματος ιωδιούχου ΣΜδιαφορετικού σκευάσματος ιωδιούχου ΣΜ, σε γνωστή , σε γνωστή προηγούμενη αντίδρασηπροηγούμενη αντίδραση
3.3. Εξετάστε το ενδεχόμενο χορήγησης Εξετάστε το ενδεχόμενο χορήγησης φαρμακευτικής αγωγής πριν φαρμακευτικής αγωγής πριν την εξέτασητην εξέταση : 30mg prednisolone (ή 32mg methylprednisolone) : 30mg prednisolone (ή 32mg methylprednisolone) από του στόματος 12 και 2 ώρες πριν τη χορήγηση του από του στόματος 12 και 2 ώρες πριν τη χορήγηση του σκιαγραφικούσκιαγραφικού
Τρόποι μείωσης της πιθανότητας εμφάνισης Τρόποι μείωσης της πιθανότητας εμφάνισης άμεσων αντιδράσεωνάμεσων αντιδράσεων

Ναυτία / ΈμετοιΝαυτία / Έμετοι
• Παροδικές:Παροδικές: Υποστηρικτική αγωγήΥποστηρικτική αγωγή
• Σοβαρές, εκτεταμένες:Σοβαρές, εκτεταμένες: Χορήγηση κατάλληλων αντιεμετικώνΧορήγηση κατάλληλων αντιεμετικών
ΚνίδωσηΚνίδωση
• Διάσπαρτη / παροδική:Διάσπαρτη / παροδική: Υποστηρικτική αγωγή και Υποστηρικτική αγωγή και παρακολούθησηπαρακολούθηση
• Διάσπαρτη / παρατεινόμενη: Διάσπαρτη / παρατεινόμενη: Ενδεχόμενη χορήγηση Ενδεχόμενη χορήγηση ενδεδειγμένου Η1-αντιισταμινικούενδεδειγμένου Η1-αντιισταμινικού διφαινυδραμίνη(διφαινυδραμίνη(Benadryl)Benadryl) po/im/iv 25-50mgpo/im/iv 25-50mg Πιθανή υπνηλία ή/και υπόταση Πιθανή υπνηλία ή/και υπόταση
• Σοβαρής μορφής:Σοβαρής μορφής: Ενδεχόμενη χορήγηση Ενδεχόμενη χορήγηση Αδρεναλίνης Αδρεναλίνης (1:1000) 0,1-0,3ml(1:1000) 0,1-0,3ml ενδομυϊκά σε ενήλικες ενδομυϊκά σε ενήλικες
παιδιά 6-12ετ 50% δόσης ενηλίκουπαιδιά 6-12ετ 50% δόσης ενηλίκουπαιδιά<6ετ 25% δόσης ενηλίκου. Επανάληψη εφ’όσον παιδιά<6ετ 25% δόσης ενηλίκου. Επανάληψη εφ’όσον χρειάζεταιχρειάζεται
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

ΒρογχόσπασμοΒρογχόσπασμο
1.1. Χορήγηση Χορήγηση ΟΟ22 με μάσκα (6-10 με μάσκα (6-10l/min)l/min)
2.2. B-2 B-2 αγωνιστήςαγωνιστής σε δοσομετρημένο σπρέι εισπνοών (2-3 σε δοσομετρημένο σπρέι εισπνοών (2-3 βαθειές εισπνοές)βαθειές εισπνοές)
3.3. ΑδρεναλίνηΑδρεναλίνη
Φυσιολογική Α.Π.Φυσιολογική Α.Π. : : Ενδομυϊκά 1:1000, 0,1-0,3 Ενδομυϊκά 1:1000, 0,1-0,3ml (mg) ml (mg) ((χρησιμοποιείστε μικρότερη δόση σε ασθενείς με χρησιμοποιείστε μικρότερη δόση σε ασθενείς με στεφανιαία νόσο ή ηλικιωμένους). στεφανιαία νόσο ή ηλικιωμένους). Σε παιδιά: 0,01Σε παιδιά: 0,01mg/kgr – mg/kgr – μέγιστη δόση 0μέγιστη δόση 0,3mg,3mg
Χαμηλή Α.Π.:Χαμηλή Α.Π.: Ενδομυϊκά 1:1000, 0,5Ενδομυϊκά 1:1000, 0,5ml (ml (0,50,5mg)mg)Σε παιδιά 6-12ετ: 0,3Σε παιδιά 6-12ετ: 0,3ml (ml (0,30,3mg)mg) ενδομυϊκά ενδομυϊκά <6ετ: 0,15<6ετ: 0,15ml (ml (0,150,15mg)mg) ενδομυϊκά ενδομυϊκά
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Λαρυγγικό οίδημαΛαρυγγικό οίδημα
1.1. Χορήγηση Χορήγηση ΟΟ22 με μάσκα (6-10 με μάσκα (6-10l/min)l/min)
2.2. Αδρεναλίνη Αδρεναλίνη Ενδομυϊκά 1:1000, 0,5Ενδομυϊκά 1:1000, 0,5ml (ml (0,50,5mg)mg). . Σε παιδιά 6-12ετ: 0,3Σε παιδιά 6-12ετ: 0,3ml (ml (0,30,3mg)mg) ενδομυϊκά ενδομυϊκά <6ετ: 0,15<6ετ: 0,15ml (ml (0,150,15mg)mg) ενδομυϊκά ενδομυϊκά
ΣπασμοίΣπασμοί
1.1. Χορήγηση Χορήγηση ΟΟ22 με μάσκα (6-10 με μάσκα (6-10l/min)l/min)
2.2. Χορήγηση Χορήγηση διαζεπάμης 5διαζεπάμης 5mg mg ΕΦΕΦ ή ή μιδαζολάμη (μιδαζολάμη (DormicumDormicum)0,5-1)0,5-1mgmg
3.3. Σε παρατεινόμενα συμπτώματα καλέστε ειδικό: εξετάστε ενδεχόμενο Σε παρατεινόμενα συμπτώματα καλέστε ειδικό: εξετάστε ενδεχόμενο χορήγησης φαινυντοΐνης 15-18χορήγησης φαινυντοΐνης 15-18mg/Kg mg/Kg σε 50σε 50 mg/min mg/min
4.4. Προσεκτική παρακολούθηση ζωτικών λειτουργιών, ιδιαίτερα Προσεκτική παρακολούθηση ζωτικών λειτουργιών, ιδιαίτερα pOpO22 λόγω του κινδύνου καταστολής του αναπνευστικού κέντρου από τις λόγω του κινδύνου καταστολής του αναπνευστικού κέντρου από τις βενζοδιαζεπίνεςβενζοδιαζεπίνες
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Πνευμονικό οίδημαΠνευμονικό οίδημα
1.1. Χορήγηση Χορήγηση ΟΟ22 με μάσκα (6-10 με μάσκα (6-10l/min)l/min)
2.2. Ανύψωση κορμούΑνύψωση κορμού
3.3. Χορήγηση διουρητικών: Χορήγηση διουρητικών: φουροσεμίδη20-40φουροσεμίδη20-40mgmg ΕΦ αργή ΕΦ αργή έγχυσηέγχυση
4.4. EEξετάστε το ενδεχόμενο χορήγησης ξετάστε το ενδεχόμενο χορήγησης μορφίνης(1-3μορφίνης(1-3mg)mg)
5.5. Μεταφορά σε ΜΕΘ ή ΤΕΠΜεταφορά σε ΜΕΘ ή ΤΕΠ
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Υπόταση Υπόταση
Μόνο Υπόταση (<70Μόνο Υπόταση (<70mmHg)mmHg)
1.1. Ανύψωση ποδιώνΑνύψωση ποδιών ασθενούς ασθενούς
2.2. Χορήγηση Χορήγηση ΟΟ22 με μάσκα (6-10με μάσκα (6-10l/min)l/min)
3.3. Ενδοφλέβια χορήγηση υγρώνΕνδοφλέβια χορήγηση υγρών : ταχέως, φυσιολογικό ορό ή : ταχέως, φυσιολογικό ορό ή γαλακτικό διάλυμα γαλακτικό διάλυμα RingerRinger
4.4. Εάν δεν ανταποκρίνεται : Εάν δεν ανταποκρίνεται : ΑδρεναλίνηΑδρεναλίνη 1:1000, 1:1000, 0,50,5ml (ml (0,50,5mg)mg) ενδομυϊκάενδομυϊκά, επανάληψη εφ’ όσον χρειάζεται , επανάληψη εφ’ όσον χρειάζεται Σε παιδιά 6-12ετ: 0,3Σε παιδιά 6-12ετ: 0,3ml (ml (0,30,3mg)mg) ενδομυϊκά , ενδομυϊκά ,
<6ετ: 0,15<6ετ: 0,15ml (ml (0,150,15mg)mg) ενδομυϊκά ενδομυϊκά
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Υπόταση Υπόταση
Κρίση παρασυμπαθητικού (υπόταση Κρίση παρασυμπαθητικού (υπόταση <70mmHg <70mmHg και βραδυκαρδίακαι βραδυκαρδία <60<60σφ)σφ)
1.1. Ανύψωση ποδιώνΑνύψωση ποδιών ασθενούς ασθενούς
2.2. Χορήγηση Χορήγηση ΟΟ22 με μάσκα (6-10 με μάσκα (6-10l/min)l/min)
3.3. Ατροπίνη 0,6-1,0Ατροπίνη 0,6-1,0mg mg ενδοφλεβίωςενδοφλεβίως επανάληψη εφ’ όσον χρειάζεται επανάληψη εφ’ όσον χρειάζεται μετά 3-5 λεπτά, μέχρι 3μετά 3-5 λεπτά, μέχρι 3mg mg συνολικά (0,04συνολικά (0,04mg/Kg)mg/Kg) στους στους ενηλίκους. Στα ενηλίκους. Στα παιδιάπαιδιά χορηγήστε 0,02 χορηγήστε 0,02mg/kgr mg/kgr ενδοφλεβίως ενδοφλεβίως (μέγιστο 0,6(μέγιστο 0,6mg mg ανά δόση) επανάληψη εφ’ όσον χρειάζεται μέχρι ανά δόση) επανάληψη εφ’ όσον χρειάζεται μέχρι 22mg mg συνολικά συνολικά
4.4. Ενδοφλέβια χορήγηση υγρώνΕνδοφλέβια χορήγηση υγρών : ταχέως, φυσιολογικό ορό ή : ταχέως, φυσιολογικό ορό ή γαλακτικό διάλυμα γαλακτικό διάλυμα RingerRinger
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Σοβαρή υπέρτασηΣοβαρή υπέρταση
1.1. Χορήγηση Χορήγηση Ο2Ο2 με μάσκα (6-10 με μάσκα (6-10l/min)l/min) 2.2. Παρακολούθηση Παρακολούθηση ΗΚΓ, οξυγόνωσης αίματος (οξύμετρο), ΗΚΓ, οξυγόνωσης αίματος (οξύμετρο),
Α.Π.Α.Π.
3.3. ΧορήγησηΧορήγηση νιτρογλυκερίνης 0,4 νιτρογλυκερίνης 0,4mg tb mg tb υπογλώσσια (έως Χ υπογλώσσια (έως Χ 3)3)
4.4. Αν δεν ανταποκρίνεται, χορήγηση Αν δεν ανταποκρίνεται, χορήγηση λαβεταλόληςλαβεταλόλης (Narcan, (Narcan, Trandate)Trandate) 20 20mg mg ΕΦΕΦ, μετά 20-80, μετά 20-80mgmg ανά 10’ έως 300 ανά 10’ έως 300mgmg
5.5. Μεταφορά σε ΜΕΘ ή ΤΕΠΜεταφορά σε ΜΕΘ ή ΤΕΠ
6.6. Για φαιοχρωμοκύττωμα Για φαιοχρωμοκύττωμα φαιντολαμίνη(φαιντολαμίνη(Regitine)Regitine) 5 5mgmg ΕΦ ΕΦ (ή λαβεταλόλη)(ή λαβεταλόλη)
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Γενικευμένη αναφυλακτοειδής αντίδρασηΓενικευμένη αναφυλακτοειδής αντίδραση ((υπόταση <70υπόταση <70mmHg mmHg και ταχυκαρδία >100σφ)και ταχυκαρδία >100σφ)
1.1. ΚαλέστεΚαλέστε ομάδα ανάνηψης ομάδα ανάνηψης
2.2. Αναρρόφηση των αεροφόρων οδώνΑναρρόφηση των αεροφόρων οδών κατά τον ενδεδειγμένο τρόπο κατά τον ενδεδειγμένο τρόπο
3.3. Ανυψώστε τα πόδια του ασθενούςΑνυψώστε τα πόδια του ασθενούς
4.4. Χορήγηση Χορήγηση Ο2Ο2 με μάσκα (6-10 με μάσκα (6-10l/min)l/min)
5.5. ΑδρεναλίνηΑδρεναλίνη 1:1000, 1:1000, 0,50,5ml (mg)ml (mg) ενδομυϊκά ενδομυϊκά, στους ενηλίκους. , στους ενηλίκους. Επανάληψη εφ’ όσον χρειάζεται. Επανάληψη εφ’ όσον χρειάζεται.
Σε παιδιά: 6-12ετ: 0,3Σε παιδιά: 6-12ετ: 0,3ml (ml (0,30,3mg)mg) ενδομυϊκά , ενδομυϊκά , <6ετ: 0,15<6ετ: 0,15ml (ml (0,150,15mg)mg) ενδομυϊκά ενδομυϊκά
6.6. Ενδοφλέβια χορήγηση υγρώνΕνδοφλέβια χορήγηση υγρών (π.χ. φυσιολογικό ορό ή γαλακτικό (π.χ. φυσιολογικό ορό ή γαλακτικό διάλυμα διάλυμα RingerRinger))
7.7. Η1-αναστολέαΗ1-αναστολέα π.χ. διφαινυδραμίνη 25-50 π.χ. διφαινυδραμίνη 25-50mg mg ΕΦΕΦ
Αντιμετώπιση άμεσων ανεπιθύμητων Αντιμετώπιση άμεσων ανεπιθύμητων αντιδράσεωναντιδράσεων

Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. ΌψιμεςΌψιμες
3.3. ΚαθυστερημένεςΚαθυστερημένες

Ανεπιθύμητες ενέργειες που εμφανίζονται 1 ώρα έως 1 εβδ μετά την Ανεπιθύμητες ενέργειες που εμφανίζονται 1 ώρα έως 1 εβδ μετά την ΕΦ χορήγησηΕΦ χορήγηση
Συμπτώματα:Συμπτώματα: κεφαλαλγία, δερματικό εξάνθημα, κνησμός, κνίδωση, κεφαλαλγία, δερματικό εξάνθημα, κνησμός, κνίδωση, ναυτία, έμετοι, πυρετός, μυοσκελετικό άλγος και γαστρεντερικές ναυτία, έμετοι, πυρετός, μυοσκελετικό άλγος και γαστρεντερικές διαταραχές. Κάποια εξ αυτών δεν σχετίζονται με το σκιαγραφικό μέσοδιαταραχές. Κάποια εξ αυτών δεν σχετίζονται με το σκιαγραφικό μέσο
Αληθείς όψιμες παρενέργειες αποτελούν οι Αληθείς όψιμες παρενέργειες αποτελούν οι δερματικές εκδηλώσειςδερματικές εκδηλώσεις. . Συνήθως είναι ήπιες και υποχωρούν μόνες τουςΣυνήθως είναι ήπιες και υποχωρούν μόνες τους
Προδιαθεσικοί παράγοντες δερματικών εκδηλώσεωνΠροδιαθεσικοί παράγοντες δερματικών εκδηλώσεων: :
a)a) προηγούμενη αντίδραση σε ΣΜ , αλλεργία σε άλλα φάρμακαπροηγούμενη αντίδραση σε ΣΜ , αλλεργία σε άλλα φάρμακα
b)b) Ασθενείς λαμβάνοντες θεραπεία με Ασθενείς λαμβάνοντες θεραπεία με ιντερλευκίνη-2ιντερλευκίνη-2
c)c) Χορήγηση μη-ιονικών διμερώνΧορήγηση μη-ιονικών διμερών
Προφυλακτική αγωγήΠροφυλακτική αγωγή με με στεροειδήστεροειδή δίδεται σε ασθενείς με δίδεται σε ασθενείς με αναφερόμενη προηγούμενη σοβαρή αντίδραση σε ΣΜαναφερόμενη προηγούμενη σοβαρή αντίδραση σε ΣΜ
ΣυνιστάταιΣυνιστάται η ενημέρωση ασθενών που με προηγούμενη σοβαρή η ενημέρωση ασθενών που με προηγούμενη σοβαρή αντίδραση και τους λαμβάνοντες ιντερλευκίνη-2 για τις πιθανές αντίδραση και τους λαμβάνοντες ιντερλευκίνη-2 για τις πιθανές δερματικές εκδηλώσεις δερματικές εκδηλώσεις
Όψιμες μη-νεφρικές ανεπιθύμητες αντιδράσειςΌψιμες μη-νεφρικές ανεπιθύμητες αντιδράσεις

Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. ΌψιμεςΌψιμες
3.3. ΚαθυστερημένεςΚαθυστερημένες

Καθυστερημένες αντιδράσειςΚαθυστερημένες αντιδράσεις
Ανεπιθύμητες ενέργειες που εμφανίζονται περισσότερο από 1 εβδ Ανεπιθύμητες ενέργειες που εμφανίζονται περισσότερο από 1 εβδ μετά την έγχυσημετά την έγχυση
ΘυρεοτοξίκωσηΘυρεοτοξίκωση Σε αυξημένο κίνδυνοΣε αυξημένο κίνδυνο
1.1. Πάσχοντες από ν.Πάσχοντες από ν.GraveGrave’’ss που δεν υποβάλλονται σε θεραπεία που δεν υποβάλλονται σε θεραπεία
2.2. Ασθενείς με Ασθενείς με πολυοζώδη βρογχοκήλη και αυτονομία του πολυοζώδη βρογχοκήλη και αυτονομία του θυρεοειδούς θυρεοειδούς ειδικά ηλικιωμένοι και διαμένοντες σε περιοχές ειδικά ηλικιωμένοι και διαμένοντες σε περιοχές ένδειας ιωδίουένδειας ιωδίου
ΣυμπτώματαΣυμπτώματα
• Απώλεια βάρους, ανησυχία, εύκολη κόπωση, δυσανεξία στη Απώλεια βάρους, ανησυχία, εύκολη κόπωση, δυσανεξία στη ζέστη, υπερκινησία, παροδική παράλυση, ταχυκαρδία και ζέστη, υπερκινησία, παροδική παράλυση, ταχυκαρδία και αρρυθμίααρρυθμία
• Σε προϋπάρχουσα καρδιακή νόσο: Κολπική μαρμαρυγή, Σε προϋπάρχουσα καρδιακή νόσο: Κολπική μαρμαρυγή, Συμφορητική ΚΑ, επιδείνωση στηθάγχης, θρομβοεμβολικά Συμφορητική ΚΑ, επιδείνωση στηθάγχης, θρομβοεμβολικά επεισόδια, και σπάνια θάνατοεπεισόδια, και σπάνια θάνατο

Καθυστερημένες αντιδράσειςΚαθυστερημένες αντιδράσεις
ΘυρεοτοξίκωσηΘυρεοτοξίκωση ΣυστάσειςΣυστάσεις
• Ιωδιούχα σκιαγραφικά μέσα Ιωδιούχα σκιαγραφικά μέσα αντενδείκνυνται σε αντενδείκνυνται σε ασθενείς με εκδηλωμένο υπερθυρεοειδισμόασθενείς με εκδηλωμένο υπερθυρεοειδισμό
• Ιδιαίτερες προφυλάξεις συνήθως δεν είναι απαραίτητεςΙδιαίτερες προφυλάξεις συνήθως δεν είναι απαραίτητες• Σε επιλεγμένους ασθενείς υψηλού κινδύνου ακολουθείται Σε επιλεγμένους ασθενείς υψηλού κινδύνου ακολουθείται
προληπτική αγωγή που χορηγείται από ενδοκρινολόγοπροληπτική αγωγή που χορηγείται από ενδοκρινολόγο• Οι ασθενείς υψηλού κινδύνου πρέπει να παρακολουθούνται Οι ασθενείς υψηλού κινδύνου πρέπει να παρακολουθούνται
στενά από ενδοκρινολόγο μετά την χορήγηση ιωδιούχου ΣΜστενά από ενδοκρινολόγο μετά την χορήγηση ιωδιούχου ΣΜ
Αν πρόκειται να ακολουθήσει σπινθηρογράφημα θυρεοειδούς Αν πρόκειται να ακολουθήσει σπινθηρογράφημα θυρεοειδούς πρέπει να μεσολαβήσουν 2μήνεςπρέπει να μεσολαβήσουν 2μήνες
Σε ασθενείς που πρόκειται να υποβληθούν σε θεραπεία με Σε ασθενείς που πρόκειται να υποβληθούν σε θεραπεία με Ραδιενεργό Ιώδιο δεν χορηγείται ιωδιούχο σκιαγραφικό για Ραδιενεργό Ιώδιο δεν χορηγείται ιωδιούχο σκιαγραφικό για τουλάχιστο 2 μήνες πριντουλάχιστο 2 μήνες πριν
Αποφυγή χορήγησης τουλάχιστον 24ώρες πριν από Αποφυγή χορήγησης τουλάχιστον 24ώρες πριν από σπινθηρογράφημα οστών ή σήμανσης ερυθρών αιμοσφαιρίωνσπινθηρογράφημα οστών ή σήμανσης ερυθρών αιμοσφαιρίων

ΙΙ. Νεφρικές ανεπιθύμητες ενέργειεςΙΙ. Νεφρικές ανεπιθύμητες ενέργειες
Νεφροτοξικότητα από σκιαγραφικό μέσο Νεφροτοξικότητα από σκιαγραφικό μέσο (CIN)(CIN)
Κατάσταση κατά την οποία παρουσιάζεται βλάβη Κατάσταση κατά την οποία παρουσιάζεται βλάβη στη νεφρική λειτουργία (αύξηση της κρεατινίνης του στη νεφρική λειτουργία (αύξηση της κρεατινίνης του ορού >25% ή 0,5ορού >25% ή 0,5mg/dl) mg/dl) εντός 3 ημερώνεντός 3 ημερών μετά την μετά την ενδαγγειακή χορήγηση σκιαγραφικού μέσουενδαγγειακή χορήγηση σκιαγραφικού μέσου σε σε απουσία εναλλακτικής αιτιολογίαςαπουσία εναλλακτικής αιτιολογίας

Νεφρικές παρενέργειεςΝεφρικές παρενέργειες
Νεφροτοξικότητα από σκιαγραφικό μέσο Νεφροτοξικότητα από σκιαγραφικό μέσο (CIN)(CIN)
ΠαθοφυσιολογίαΠαθοφυσιολογία
1)1) Αγγειακές μεταβολέςΑγγειακές μεταβολές: :
a)a) το υπερωσμωτικό ΣΜ προκαλεί επαναρρόφηση Ητο υπερωσμωτικό ΣΜ προκαλεί επαναρρόφηση Η22Ο Ο οίδημα οίδημα νεφρικών σωληναρίων και αύξηση ενδονεφρικής πίεσης νεφρικών σωληναρίων και αύξηση ενδονεφρικής πίεσης ελάττωση νεφρικής αιμάτωσηςελάττωση νεφρικής αιμάτωσης και και ρυθμού σπειραματικής ρυθμού σπειραματικής διήθησηςδιήθησης
b)b) Έκκριση αγγειοκινητικών ουσιών : Έκκριση αγγειοκινητικών ουσιών : ενδοθηλίνη και αδενοσίνη ενδοθηλίνη και αδενοσίνη αγγειοσύσπαση, αγγειοσύσπαση, ΝΟ και προστακυκλίνη ΝΟ και προστακυκλίνη αγγειοδιαστολή αγγειοδιαστολή
2)2) Άμεση τοξικότητα στα νεφρικά σωληνάριαΆμεση τοξικότητα στα νεφρικά σωληνάρια: : πρωτεϊνουρία πρωτεϊνουρία3)3) Ενδογενείς βιοχημικές διαταραχέςΕνδογενείς βιοχημικές διαταραχές : αύξηση ελεύθερων ριζών : αύξηση ελεύθερων ριζών
ΟΟ22 ή μείωση των αντιοξειδωτικών πρωτεϊνών ή μείωση των αντιοξειδωτικών πρωτεϊνών
Σε ασθενείς με Σε ασθενείς με προϋπάρχουσα διαταραχή της νεφρικής προϋπάρχουσα διαταραχή της νεφρικής λειτουργίαςλειτουργίας αυξάνεται η πιθανότητα νεφροτοξικής δράσης των αυξάνεται η πιθανότητα νεφροτοξικής δράσης των ΣΜΣΜ

Ελλ Νεφρολογία 2009; 21 (4): 302 - 315

Παράγοντες κινδύνου για Παράγοντες κινδύνου για CINCIN
• Σχετικοί με τον ασθενήΣχετικοί με τον ασθενή
1.1. eGFR <60ml/mineGFR <60ml/min ( (ή αυξημένη κρεατινίνη ορού) πριν από ενδαρτηριακή ή αυξημένη κρεατινίνη ορού) πριν από ενδαρτηριακή έγχυση έγχυση
2.2. eGFR <45ml/mineGFR <45ml/min πριν από ενδοφλέβια έγχυση Ιδιαίτερα αν συνυπάρχειπριν από ενδοφλέβια έγχυση Ιδιαίτερα αν συνυπάρχει1.1. Διαβητική νεφροπάθειαΔιαβητική νεφροπάθεια2.2. ΑφυδάτωσηΑφυδάτωση3.3. Συμφορητική Καρδιακή Ανεπάρκεια (ΣΚΑ) χαμηλού ΚΕΣυμφορητική Καρδιακή Ανεπάρκεια (ΣΚΑ) χαμηλού ΚΕ4.4. Πρόσφατο ΟΕΜ(<24Πρόσφατο ΟΕΜ(<24h)h)5.5. Ενδοαορτική αντλίαΕνδοαορτική αντλία6.6. Περιεπεμβατική υπότασηΠεριεπεμβατική υπόταση7.7. Χαμηλός αιματοκρίτηςΧαμηλός αιματοκρίτης8.8. Ηλικία Ηλικία >70ετ>70ετ
9.9. Ταυτόχρονη χορήγηση Ταυτόχρονη χορήγηση νεφροτοξικών φαρμάκωννεφροτοξικών φαρμάκων, π.χ. μη στεροειδών , π.χ. μη στεροειδών αντιφλεγμονωδώναντιφλεγμονωδών
• Σχετικοί με τη διαδικασίαΣχετικοί με τη διαδικασία
1.1. Ενδαρτηριακή έγχυσηΕνδαρτηριακή έγχυση2.2. ΣΜ υψηλής ωσμωμοριακότηταςΣΜ υψηλής ωσμωμοριακότητας3.3. Μεγάλες δόσεις σκιαγραφικού μέσουΜεγάλες δόσεις σκιαγραφικού μέσου4.4. Πολλαπλές χορηγήσεις σκιαγραφικού εντός ολίγων ημερών.Πολλαπλές χορηγήσεις σκιαγραφικού εντός ολίγων ημερών.

Κίνδυνος από ιωδιούχα ΣΜ σε ασθενείς που Κίνδυνος από ιωδιούχα ΣΜ σε ασθενείς που λαμβάνουν μεταφορμίνηλαμβάνουν μεταφορμίνη
Γαλακτική οξείδωσηΓαλακτική οξείδωση
Η μεταφορμίνη εκκρίνεται αναλλοίωτη στα ούρα κατά 90% Η μεταφορμίνη εκκρίνεται αναλλοίωτη στα ούρα κατά 90% 24ώρες24ώρες
Επί νεφρικής ανεπάρκειας, είτε προϋπάρχουσας είτε Επί νεφρικής ανεπάρκειας, είτε προϋπάρχουσας είτε προκαλούμενης από το ιωδιούχο ΣΜ, η μεταφορμίνη δεν προκαλούμενης από το ιωδιούχο ΣΜ, η μεταφορμίνη δεν αποβάλλεται μπορεί να προκαλέσει παραγωγή γαλακτικού αποβάλλεται μπορεί να προκαλέσει παραγωγή γαλακτικού οξέος από τον εντερικό σωλήνα σε επαρκείς ποσότητες, ώστε οξέος από τον εντερικό σωλήνα σε επαρκείς ποσότητες, ώστε να προκαλέσει γαλακτική οξείδωσηνα προκαλέσει γαλακτική οξείδωση
Η μεταφορμίνη δεν προκαλεί νεφρική ανεπάρκειαΗ μεταφορμίνη δεν προκαλεί νεφρική ανεπάρκεια

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
• Σε εξέταση εκλογής Σε εξέταση εκλογής κατά την παραπομπήκατά την παραπομπή
1.1. Αναγνώριση ασθενών με Αναγνώριση ασθενών με eGFR <60ml/min/1,73meGFR <60ml/min/1,73m22
• Ασθενείς με γνωστή αύξηση της Ασθενείς με γνωστή αύξηση της SCrSCr• Ασθενείς >70ετΑσθενείς >70ετ• Ασθενείς που θα υποβληθούν σε ενδαρτηριακή έγχυση ΣΜΑσθενείς που θα υποβληθούν σε ενδαρτηριακή έγχυση ΣΜ• Ασθενείς με ιστορικό που ενισχύει την πιθανότητα χαμηλής Ασθενείς με ιστορικό που ενισχύει την πιθανότητα χαμηλής GFRGFR: :
Νεφρικής νόσουΝεφρικής νόσου Χειρουργικής επέμβασης νεφρώνΧειρουργικής επέμβασης νεφρών ΠρωτεϊνουρίαςΠρωτεϊνουρίας ΔιαβήτηΔιαβήτη Υπέρτασης Υπέρτασης Ουρικής αρθρίτιδαςΟυρικής αρθρίτιδας Πρόσφατη λήψη νεφροτοξικών φαρμάκων Πρόσφατη λήψη νεφροτοξικών φαρμάκων
Μέτρηση Μέτρηση SCrSCr εντός 7 ημ από τη χορήγηση του ΣΜ εντός 7 ημ από τη χορήγηση του ΣΜ

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
Σε εξέταση εκλογής Σε εξέταση εκλογής πριν την εξέτασηπριν την εξέταση
1.1. Σε ασθενείς με Σε ασθενείς με eGFR <60ml/min/1,73meGFR <60ml/min/1,73m22 ( ή αυξημένη( ή αυξημένη SCrSCr) και ) και αυτούς με αυξημένο κίνδυνο νεφροτοξικότηταςαυτούς με αυξημένο κίνδυνο νεφροτοξικότητας
• Εξέταση ενδεχομένου Εξέταση ενδεχομένου εναλλακτικής μεθόδουεναλλακτικής μεθόδου απεικόνισης χωρίς απεικόνισης χωρίς χρήση ΕΦ ιωδιούχου ΣΜχρήση ΕΦ ιωδιούχου ΣΜ
• Διακοπή Διακοπή νεφροτοξικών φαρμάκων, μαννιτόλης και διουρητικών νεφροτοξικών φαρμάκων, μαννιτόλης και διουρητικών αγκύληςαγκύλης τουλάχιστον 24ώρες πριν την εξέταση τουλάχιστον 24ώρες πριν την εξέταση
• Έναρξη ενυδάτωσης: Έναρξη ενυδάτωσης: 11ml/KrBW/h NaCl 0,9%ml/KrBW/h NaCl 0,9% για τουλάχιστον για τουλάχιστον 6 ώρες 6 ώρες πριν και μετάπριν και μετά την εξέταση την εξέταση
2.2. Σε διαβητικούς που λαμβάνουν μεταφορμίνηΣε διαβητικούς που λαμβάνουν μεταφορμίνη• Εάν Εάν eGFR > 60ml/min/1,73meGFR > 60ml/min/1,73m22, , συνέχισησυνέχιση της μεταφορμίνης της μεταφορμίνης
• Εάν Εάν eGFR <60 eGFR <60 και και >30 ml/min/1,73m>30 ml/min/1,73m22, , διακοπήδιακοπή μεταφορμίνης για μεταφορμίνης για 4848h h πριν την εξέταση και επανέναρξη μόνο επί φυσιολογικής πριν την εξέταση και επανέναρξη μόνο επί φυσιολογικής SCr SCr μετά 48μετά 48h.h.
• Εάν Εάν eGFR <30 ml/min/1,73meGFR <30 ml/min/1,73m22, , αποφυγή χορήγησης ΕΦ ιωδιούχου αποφυγή χορήγησης ΕΦ ιωδιούχου ΣΜΣΜ

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
• Σε επείγοντα περιστατικά Σε επείγοντα περιστατικά κατά την παραπομπήκατά την παραπομπή
1.1. Αναγνώριση ασθενών με Αναγνώριση ασθενών με eGFR <60ml/min/1,73meGFR <60ml/min/1,73m22 (αν είναι (αν είναι δυνατόν)δυνατόν)
2.2. Αναγνώριση ασθενών που λαμβάνουν μεταφορμίνηΑναγνώριση ασθενών που λαμβάνουν μεταφορμίνη
Μέτρηση Μέτρηση GFR GFR ή ή SCrSCr αν είναι δυνατό να αναβληθεί η αν είναι δυνατό να αναβληθεί η διαδικασία μέχρι τη λήψη των αποτελεσμάτων διαδικασία μέχρι τη λήψη των αποτελεσμάτων χωρίς αυτό χωρίς αυτό να βλάψει τον ασθενήνα βλάψει τον ασθενή
Σε εξαιρετικά επείγον περιστατικό Σε εξαιρετικά επείγον περιστατικό αν δεν μπορεί να αν δεν μπορεί να πραγματοποιηθεί μέτρηση πραγματοποιηθεί μέτρηση SCrSCr, ακολουθείτε το , ακολουθείτε το πρωτόκολλο για ασθενείς με πρωτόκολλο για ασθενείς με eGFR <60ml/min/1,73meGFR <60ml/min/1,73m22, , όσο όσο πιο πιστά επιτρέπουν οι συνθήκεςπιο πιστά επιτρέπουν οι συνθήκες

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
• Σε επείγοντα περιστατικά Σε επείγοντα περιστατικά πριν την εξέτασηπριν την εξέταση
1.1. Σε ασθενείς με αυξημένο κίνδυνο νεφροτοξικότηταςΣε ασθενείς με αυξημένο κίνδυνο νεφροτοξικότητας• Εξέταση ενδεχομένου Εξέταση ενδεχομένου εναλλακτικής μεθόδουεναλλακτικής μεθόδου απεικόνισης χωρίς χρήση απεικόνισης χωρίς χρήση
ΕΦ ιωδιούχου ΣΜΕΦ ιωδιούχου ΣΜ
• Έναρξη ΕΦ ενυδάτωσης όσο το δυνατόν νωρίτερα πριν την εξέταση: Έναρξη ΕΦ ενυδάτωσης όσο το δυνατόν νωρίτερα πριν την εξέταση: 11ml/KrBW/h NaCl 0,9%ml/KrBW/h NaCl 0,9%
2.2. Σε διαβητικούς που λαμβάνουν μεταφορμίνηΣε διαβητικούς που λαμβάνουν μεταφορμίνη• Εάν Εάν eGFR > 60ml/min/1,73meGFR > 60ml/min/1,73m22, , συνέχισησυνέχιση της μεταφορμίνης της μεταφορμίνης
• Εάν Εάν eGFR <60 eGFR <60 και και >30 ml/min/1,73m>30 ml/min/1,73m22, , ή ή άγνωστηάγνωστη, σταθμίζουμε κίνδυνο-, σταθμίζουμε κίνδυνο-όφελος και εξετάζουμε ενδεχόμενο εναλλακτικής μεθόδου. Αν όφελος και εξετάζουμε ενδεχόμενο εναλλακτικής μεθόδου. Αν απαραίτητηαπαραίτητη
Διακοπή μεταμορφίνηςΔιακοπή μεταμορφίνης Ενυδάτωση Ενυδάτωση 11ml/KrBW/h NaCl 0,9%ml/KrBW/h NaCl 0,9% για τουλάχιστον για τουλάχιστον 6 ώρες μετά6 ώρες μετά την την
εξέτασηεξέταση Έλεγχο νεφρικής λειτουργίας, γαλακτικού οξέος και Έλεγχο νεφρικής λειτουργίας, γαλακτικού οξέος και pHpH αίματος αίματος Αναζήτηση συμπτωμάτων Αναζήτηση συμπτωμάτων γαλακτικής οξείδωσης γαλακτικής οξείδωσης (έμετοι, υπνηλία, ναυτία, (έμετοι, υπνηλία, ναυτία,
επιγαστραλγία, ανορεξία,υπέρπνοια, λήθαργο, διάρροια, και δίψα.) επιγαστραλγία, ανορεξία,υπέρπνοια, λήθαργο, διάρροια, και δίψα.) ενδεικτικής αιματολογικές εξετάσεις ενδεικτικής αιματολογικές εξετάσεις pHpH<7,25 με γαλακτικό οξύ >5<7,25 με γαλακτικό οξύ >5mmol/lmmol/l

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
• Κατά την εξέτασηΚατά την εξέταση
1.1. Σε ασθενείς με αυξημένο κίνδυνο εμφάνισης νεφροπάθειας Σε ασθενείς με αυξημένο κίνδυνο εμφάνισης νεφροπάθειας από ΣΜαπό ΣΜ
• Χρήση ιωδιούχου σκιαγραφικού Χρήση ιωδιούχου σκιαγραφικού χαμηλής ωσμωμοριακότητας ή χαμηλής ωσμωμοριακότητας ή ισοωσμωτικό ισοωσμωτικό
• Χορήγηση στη Χορήγηση στη μικρότερη δυνατή δόση μικρότερη δυνατή δόση
2.2. Σε ασθενείς χωρίς αυξημένο κίνδυνο εμφάνισης νεφροπάθειας Σε ασθενείς χωρίς αυξημένο κίνδυνο εμφάνισης νεφροπάθειας από ΣΜαπό ΣΜ
• Χορήγηση στη μικρότερη δυνατή δόση Χορήγηση στη μικρότερη δυνατή δόση

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
• Μετά την εξέτασηΜετά την εξέταση
1.1. Σε ασθενείς με Σε ασθενείς με eGFR <60ml/min/1,73meGFR <60ml/min/1,73m22 ( ή αυξημένη( ή αυξημένη SCrSCr)) • Συνέχιση ΕΦ Συνέχιση ΕΦ ενυδάτωσης ενυδάτωσης για τουλάχιστον 6 ώρεςγια τουλάχιστον 6 ώρες
2.2. Σε διαβητικούς που λαμβάνουν μεταφορμίνη με Σε διαβητικούς που λαμβάνουν μεταφορμίνη με eGFR eGFR <60ml/min/1,73m<60ml/min/1,73m22 ( ή αυξημένη( ή αυξημένη SCrSCr))
• Μέτρηση Μέτρηση eGFR (eGFR (ή ή SCr) 48hSCr) 48h μετά την ΕΦ χορήγηση ΣΜ. μετά την ΕΦ χορήγηση ΣΜ. Σε μη επιδείνωσηΣε μη επιδείνωση συνέχιση μεταφορμίνης συνέχιση μεταφορμίνης Σε Σε επιδείνωσηεπιδείνωση διακοπή μεταφορμίνης διακοπή μεταφορμίνης

Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN
Προφυλακτική φαρμακευτική ΑγωγήΠροφυλακτική φαρμακευτική Αγωγή Νεφρικά αγγειοδιασταλτικάΝεφρικά αγγειοδιασταλτικά
• Αναστολείς διαύλων Αναστολείς διαύλων CaCa+2+2
• ΝτοπαμίνηΝτοπαμίνη
• Κολπικό νατριουρητικό πεπτίδιοΚολπικό νατριουρητικό πεπτίδιο
• Αγωνιστές υποδοχέων ντοπαμίνηςΑγωνιστές υποδοχέων ντοπαμίνης
• Προσταγλαδίνη Ε1Προσταγλαδίνη Ε1 Ανταγωνιστές υποδοχέων ενδογενών αγγειοδραστικών μεσολαβητώνΑνταγωνιστές υποδοχέων ενδογενών αγγειοδραστικών μεσολαβητών
• Ανταγωνιστής υποδοχέων θεοφυλλίνηςΑνταγωνιστής υποδοχέων θεοφυλλίνης
• ΘεοφυλλίνηΘεοφυλλίνη Κυτταροπροστατευτικά φάρμακαΚυτταροπροστατευτικά φάρμακα
• ΑκετυλοκυστεΐνηΑκετυλοκυστεΐνη
• NaNa22CCΟΟ33 ΕΦΕΦ
• ΑκεταζολαμίδηΑκεταζολαμίδη
Ο ρόλος τους Ο ρόλος τους παραμένει παραμένει αμφιλεγόμενοςαμφιλεγόμενος

• Χορήγηση ακετυλοκυστεΐνηςΧορήγηση ακετυλοκυστεΐνης
• Εύκολη χορήγηση, χαμηλό κόστος, περιορισμένες Εύκολη χορήγηση, χαμηλό κόστος, περιορισμένες παρενέργειεςπαρενέργειες
• Δεν έχει καθοριστεί η βέλτιστη δοσολογία Δεν έχει καθοριστεί η βέλτιστη δοσολογία (600mg (600mg ήή 1200mg 1200mg για για 48h)48h)
• Ενεργότητα ποικίλει στα δια του στόματος σκευάσματα Ενεργότητα ποικίλει στα δια του στόματος σκευάσματα • Περίεργη οσμή και γεύση του υγρού παρασκευάσματος Περίεργη οσμή και γεύση του υγρού παρασκευάσματος • άγνωστος ο μηχανισμός πρόληψης της άγνωστος ο μηχανισμός πρόληψης της CINCIN • προκαλεί κρεατινινουρία που προκαλεί ελάττωση της προκαλεί κρεατινινουρία που προκαλεί ελάττωση της
κρεατινίνης ορού ανεξάρτητα από τη μεταβολή του κρεατινίνης ορού ανεξάρτητα από τη μεταβολή του GFRGFR
• Τα αποτελέσματα των κλινικών μελετών είναι Τα αποτελέσματα των κλινικών μελετών είναι αντικρουόμενααντικρουόμενα
• Αβεβαιότητα σχετικά με την αποτελεσματικότητά τηςΑβεβαιότητα σχετικά με την αποτελεσματικότητά της
Τρόποι πρόληψης της Τρόποι πρόληψης της CINCIN

Επίπτωση Επίπτωση CINCIN μετά τη χορήγηση ιωδιούχου ΣΜ μετά τη χορήγηση ιωδιούχου ΣΜ
Η επίπτωση της νεφροπάθειας από ΣΜ είναι Η επίπτωση της νεφροπάθειας από ΣΜ είναι πολύ πολύ χαμηλήχαμηλή σε ασθενείς με σε ασθενείς με GFR >45ml/minGFR >45ml/min (<1%) (<1%)
Η επίπτωση της νεφροπάθειας από ΣΜ σε ασθενείς Η επίπτωση της νεφροπάθειας από ΣΜ σε ασθενείς με με with with GFR <45ml/minGFR <45ml/min ποικίλειποικίλει μεταξύμεταξύ 10-40%10-40%
Katzberg & Barrett, Radiology 2007; 243: 622-628Weisbord SD et al, Clin J Am Soc Nephrol 2008; 3: 1274-1281Thomsen & Morcos, Eur Radiol 2009 Apr;19(4):891-7

Κλινική σημασία της Κλινική σημασία της CINCIN
Η νεφροπάθεια από ΣΜ αυξάνει την επίπτωση Η νεφροπάθεια από ΣΜ αυξάνει την επίπτωση των των μη-νεφρικών επιπλοκώνμη-νεφρικών επιπλοκών και αυξάνει τη και αυξάνει τη νοσοκομειακή παραμονήνοσοκομειακή παραμονή
Η νεφροπάθεια από ΣΜ αυξάνει τη νοσοκομειακή Η νεφροπάθεια από ΣΜ αυξάνει τη νοσοκομειακή θνησιμότηταθνησιμότητα
Rihal et al; Circulation 2002; 105: 2259-2265.Bartholemew et al, Am J Cardiol 2004; 93: 1515-1519Marenzi et al, JACC 2004; 44:1780-1785Solomon R, Clin J Am Soc Nephrol 2008; 3: 1242-1243Weisbord SD et al, Clin J Am Soc Nephrol 2008; 3: 1274-1281From AM et al, Mayo Clin Proc 2008; 83: 1095-1100

Αιμοκάθαρση και ιωδιούχα ΣΜΑιμοκάθαρση και ιωδιούχα ΣΜ
Όλα τα σκιαγραφικά μέσα μπορούν να απομακρυνθούν Όλα τα σκιαγραφικά μέσα μπορούν να απομακρυνθούν από τον οργανισμό με την αιμοκάθαρση και την περιτοναϊκή από τον οργανισμό με την αιμοκάθαρση και την περιτοναϊκή διύλιση. Ωστόσο διύλιση. Ωστόσο δεν υπάρχει απόδειξη ότι η αιμοκάθαρση δεν υπάρχει απόδειξη ότι η αιμοκάθαρση προστατεύει τον ασθενή με νεφρική ανεπάρκεια από την προστατεύει τον ασθενή με νεφρική ανεπάρκεια από την πρόκληση νεφροπάθειας από σκιαγραφικόπρόκληση νεφροπάθειας από σκιαγραφικό
Συστάσεις για αιμοκαθαιρόμενους ή ασθενείς σε Συστάσεις για αιμοκαθαιρόμενους ή ασθενείς σε περιτοναϊκή κάθαρσηπεριτοναϊκή κάθαρση
1.1. Αποφυγή υπερβολικού φορτίουΑποφυγή υπερβολικού φορτίου ωσμωτικών και υγρών ωσμωτικών και υγρών2.2. Δεν είναι απαραίτητος ο συσχετισμός του χρόνου Δεν είναι απαραίτητος ο συσχετισμός του χρόνου
χορήγησης του σκιαγραφικού και του χρόνου συνεδρίας χορήγησης του σκιαγραφικού και του χρόνου συνεδρίας αιμοκάθαρσηςαιμοκάθαρσης
3.3. Δεν είναι απαραίτητη η επιπλέον συνεδρία αιμοκάθαρσης Δεν είναι απαραίτητη η επιπλέον συνεδρία αιμοκάθαρσης για την απομάκρυνση του ΣΜ (ισχύει και για ασθενείς σε για την απομάκρυνση του ΣΜ (ισχύει και για ασθενείς σε περιτοναϊκή κάθαρση)περιτοναϊκή κάθαρση)

ESUR Guidelines on ESUR Guidelines on Contrast Media Contrast Media European Society of European Society of UUrogenital Radiologyrogenital Radiology

Σκιαγραφικά μέσα Σκιαγραφικά μέσα Μαγνητικού ΣυντονισμούΜαγνητικού Συντονισμού

Σκιαγραφικά μέσα Μαγνητικού ΣυντονισμούΣκιαγραφικά μέσα Μαγνητικού Συντονισμού
Σκιαγραφικά μέσα που περιέχουν παραμαγνητικά ή υπερπαραμαγνητικά Σκιαγραφικά μέσα που περιέχουν παραμαγνητικά ή υπερπαραμαγνητικά μεταλλικά ιόντα και επηρεάζουν τις μαγνητικές ιδιότητες των μεταλλικά ιόντα και επηρεάζουν τις μαγνητικές ιδιότητες των περιβαλλόντων ιστώνπεριβαλλόντων ιστών
1.1. Παραμαγνητικά σκιαγραφικά μέσαΠαραμαγνητικά σκιαγραφικά μέσα:: Θετικά σκιαγραφικά μέσα που Θετικά σκιαγραφικά μέσα που προκαλούν ελάττωση του Τ1 και Τ2 χρόνου χαλάρωσης και αύξηση της προκαλούν ελάττωση του Τ1 και Τ2 χρόνου χαλάρωσης και αύξηση της έντασης σήματος σε Τ1 προσανατολισμένες ακολουθίες. έντασης σήματος σε Τ1 προσανατολισμένες ακολουθίες. Χρησιμοποιούνται για την ενίσχυση αντίθεσης των ιστών, χαρακτηρισμό Χρησιμοποιούνται για την ενίσχυση αντίθεσης των ιστών, χαρακτηρισμό βλαβών, εκτίμηση αιμάτωσης και διαταραχές ροήςβλαβών, εκτίμηση αιμάτωσης και διαταραχές ροής
• Χηλικές ενώσεις ΓαδολινίουΧηλικές ενώσεις Γαδολινίου• Χηλικές ενώσεις ΜαγγανίουΧηλικές ενώσεις Μαγγανίου• Παράγοντες ηπατοκυτταρικής ειδικότηταςΠαράγοντες ηπατοκυτταρικής ειδικότητας
2.2. Υπερπαραμαγνητικά σκιαγραφικά μέσα (Υπερπαραμαγνητικά σκιαγραφικά μέσα (SPIO)SPIO):: Περιέχουν Περιέχουν υπερπαραμαγνητικά οξείδια σιδήρου (υπερπαραμαγνητικά οξείδια σιδήρου (SPIOsSPIOs και και USPIOs)USPIOs). Προκαλούν . Προκαλούν ελάττωση του χρόνου χαλάρωσης σε Τ2 και Τ2* προσανατολισμένες ελάττωση του χρόνου χαλάρωσης σε Τ2 και Τ2* προσανατολισμένες ακολουθίες με πολύ μικρότερη επίδραση στον Τ1 χρόνο χαλάρωσης. Η ακολουθίες με πολύ μικρότερη επίδραση στον Τ1 χρόνο χαλάρωσης. Η πτώση σήματος εμφανίζεται σε φυσιολογικό ιστό , όπου το ΔΕΣ πτώση σήματος εμφανίζεται σε φυσιολογικό ιστό , όπου το ΔΕΣ προσλαμβάνει τα οξείδια σιδήρου σε αντίθεση με περιοχές μεταστατικής προσλαμβάνει τα οξείδια σιδήρου σε αντίθεση με περιοχές μεταστατικής προσβολήςπροσβολής

ΧηλικέςΧηλικές ενώσειςενώσεις γαδολινίουγαδολινίου
A.A. ΜηΜη ειδικάειδικά εξωκυττάριαεξωκυττάρια
1. 1. ΙονικάΙονικά γραμμικάγραμμικά:: τοτο Gd+3 Gd+3 συνδέεταισυνδέεται μεμε 5 5 καρβοξυλικέςκαρβοξυλικές ομάδεςομάδες καικαι 3 3 αμινοομάδεςαμινοομάδες. . ΗΗ ελεύθερηελεύθερη θέσηθέση συνδέεταισυνδέεται μεμε μόριομόριο νερούνερού σημαντικόσημαντικό γιαγια τηντην ενίσχυσηενίσχυση τουτου σήματοςσήματος σεσε ΤΤ1WI. 1WI. ΟιΟι δύοδύο καρβοξυλικέςκαρβοξυλικές ομάδεςομάδες εξουδετερώνονταιεξουδετερώνονται απόαπό δύοδύο κατιόντακατιόντα μεγλουμίνηςμεγλουμίνης ήή Na+ Na+
ππ..χχ.Gadopentetate dimeglumine (Magnevist.Gadopentetate dimeglumine (Magnevist))
2. 2. ΜηΜη ιονικάιονικά γραμμικάγραμμικά:: τοτο Gd+3 Gd+3 συνδέεταισυνδέεται μεμε 3 3 καρβοξυλικέςκαρβοξυλικές ομάδεςομάδες καικαι 2 2 μεθυλαμίδιαμεθυλαμίδια. . ΟιΟι δεσμοίδεσμοί τουτου μορίουμορίου είναιείναι πιοπιο χαλαροίχαλαροί σεσε σχέσησχέση μεμε τατα ιονικάιονικά γραμμικάγραμμικά καικαι μειώνεταιμειώνεται ηη σταθερότητασταθερότητα τουτου μορίουμορίου
ππ..χχ. Gadodiamide (Omniscan), Gadoversetamide (Optimark). Gadodiamide (Omniscan), Gadoversetamide (Optimark) ΣταΣτα μακροκυκλικάμακροκυκλικά μόριαμόρια τουτου Gd+3 Gd+3 οιοι προσχηματισμένοιπροσχηματισμένοι πολυκαρβοξυλικοίπολυκαρβοξυλικοί (12 (12
θέσειςθέσεις) ) άκαμπτοιάκαμπτοι δακτύλιοιδακτύλιοι πουπου περιλαμβάνουνπεριλαμβάνουν τοτο Gd+3 Gd+3 στοστο κέντροκέντρο τουςτους (ligands) (ligands) προσφέρουνπροσφέρουν σημαντικήσημαντική σταθερότητασταθερότητα στοστο μόριομόριο. . ΣυνδέεταιΣυνδέεται μεμε τουλάχιστοτουλάχιστο 3 3 καρβοξυλικέςκαρβοξυλικές ομάδεςομάδες στιςστις περιφερικέςπεριφερικές θέσειςθέσεις
3. 3. ΙονικάΙονικά κυκλικάκυκλικά: : ππ..χχ. Gadoterate dimeglumine (Dotarem) . Gadoterate dimeglumine (Dotarem)
4. 4. ΜηΜη ιονικάιονικά κυκλικάκυκλικά ππ..χχ. . Gadobutrol (Gadovist), Gadoteridol (Prohance)Gadobutrol (Gadovist), Gadoteridol (Prohance)
ΔενΔεν συνδέονταισυνδέονται μεμε πρωτεΐνεςπρωτεΐνες καικαι αποβάλλονταιαποβάλλονται μόνομόνο απόαπό τουςτους νεφρούςνεφρούς
1. Παραμαγνητικά μέσα ΣΑ1. Παραμαγνητικά μέσα ΣΑ

ΧηλικέςΧηλικές ενώσειςενώσεις γαδολινίουγαδολινίου
B. B. ΠαράγοντεςΠαράγοντες υψηλήςυψηλής χαλάρωσηςχαλάρωσης
• ΙονικάΙονικά γραμμικάγραμμικά:: λόγωλόγω τηςτης ικανότηταςικανότητας σύνδεσηςσύνδεσης μεμε πρωτεΐνεςπρωτεΐνες, , έκκρισηςέκκρισης διαδια τηςτης χολήςχολής καικαι τηςτης καθυστερημένηςκαθυστερημένης φάσηςφάσης ηπατοκυτταρικήςηπατοκυτταρικής πρόσληψηςπρόσληψης χρησιμοποιούνταιχρησιμοποιούνται στηνστην απεικόνισηαπεικόνιση τουτου ήπατοςήπατος
ππ..χχ. Gadobenate dimeglumine (MultiHance), Gadofosveset trisodium (Vasovist), . Gadobenate dimeglumine (MultiHance), Gadofosveset trisodium (Vasovist), gadoxetate disodium (Primovist)gadoxetate disodium (Primovist)
ΣυνδέονταιΣυνδέονται μεμε πρωτεΐνεςπρωτεΐνες καικαι αποβάλλονταιαποβάλλονται απόαπό τουςτους νεφρούςνεφρούς καικαι τοτο ήπαρήπαρ διαδια τηςτης χολήςχολής
ΠαράγοντεςΠαράγοντες ηπατοκυτταρικήςηπατοκυτταρικής ειδικότηταςειδικότητας
• ΠεριλαμβάνουνΠεριλαμβάνουν σύμπλοκεςσύμπλοκες ενώσειςενώσεις μαγγανίουμαγγανίου. . ΦέρειΦέρει 5 5 αδέσμευτααδέσμευτα e- e- καικαι είναιείναι 3 3 φορέςφορές ισχυρότεροιισχυρότεροι παράγοντεςπαράγοντες ΤΤ1 1 χαλάρωσηςχαλάρωσης απόαπό τοτο Gd Gd καικαι υψηλότερηυψηλότερη πρόσληψηπρόσληψη απόαπό τατα ηπατοκύτταραηπατοκύτταρα
• Mangafodipir trisodium (Teslascan): Mangafodipir trisodium (Teslascan): ΑποδίδειΑποδίδει ιόνταιόντα μαγγανίουμαγγανίου πουπου συνδέονταισυνδέονται μεμε αα2-2-μακρογλοβουλίνημακρογλοβουλίνη καικαι μεταφέρονταιμεταφέρονται στοστο ήπαρήπαρ
• Manganese chloride CMC-001 (LumenHance): Manganese chloride CMC-001 (LumenHance): χορηγείταιχορηγείται απόαπό τουτου στόματοςστόματος καικαι φτάνειφτάνει στοστο ήπαρήπαρ μέσωμέσω τηςτης πυλαίαςπυλαίας κυκλοφορίαςκυκλοφορίας
1. Παραμαγνητικά μέσα ΣΑ1. Παραμαγνητικά μέσα ΣΑ


Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. Όψιμες - ΚαθυστερημένεςΌψιμες - Καθυστερημένες

Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. Όψιμες - ΚαθυστερημένεςΌψιμες - Καθυστερημένες

Ταξινόμηση άμεσων μη-νεφρικών αντιδράσεωνΤαξινόμηση άμεσων μη-νεφρικών αντιδράσεων
Ο κίνδυνος εμφάνισης είναι σημαντικά μικρότερος συγκριτικά Ο κίνδυνος εμφάνισης είναι σημαντικά μικρότερος συγκριτικά με τα ιωδιούχα ΣΜμε τα ιωδιούχα ΣΜ
• Ήπιες:Ήπιες: ναυτία, ήπιοι έμετοι, κνίδωση, έμετος, κνησμός ναυτία, ήπιοι έμετοι, κνίδωση, έμετος, κνησμός
• Ενδιάμεσες:Ενδιάμεσες: έντονοι έμετοι, κνίδωση με στίγματα, έντονοι έμετοι, κνίδωση με στίγματα, βρογχόσπασμος, λαρυγγικό ή προσωπικό οίδημα αντίδραση βρογχόσπασμος, λαρυγγικό ή προσωπικό οίδημα αντίδραση παρασυμπαθητικούπαρασυμπαθητικού
• Σοβαρές - απειλητικές για τη ζωή:Σοβαρές - απειλητικές για τη ζωή: υποτασική καταπληξία, υποτασική καταπληξία, πνευμονικό οίδημα, αναπνευστική ανακοπή, καρδιακή πνευμονικό οίδημα, αναπνευστική ανακοπή, καρδιακή ανακοπή, σπασμοίανακοπή, σπασμοί

• Σχετιζόμενες με τον ασθενήΣχετιζόμενες με τον ασθενή
1.1. Προηγηθείσα μέτρια ή σοβαρή άμεση αντίδραση σε ΣΜ Προηγηθείσα μέτρια ή σοβαρή άμεση αντίδραση σε ΣΜ γαδολινίου:γαδολινίου: Ο κίνδυνος εμφάνισης ανεπιθύμητων Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά αντιδράσεων αυξάνει κατά 8 φορές8 φορές σε ασθενείς με σε ασθενείς με γνωστή γνωστή υπερευαισθησίαυπερευαισθησία. Η αντίδραση μπορεί να είναι πιο σοβαρή. Η αντίδραση μπορεί να είναι πιο σοβαρή
2.2. Άσθμα:Άσθμα: Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων ανέρχεται σε 3,7%.ανέρχεται σε 3,7%.
3.3. Αλλεργία που χρήζει φαρμακευτικής αγωγής:Αλλεργία που χρήζει φαρμακευτικής αγωγής: Ο κίνδυνος Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά εμφάνισης ανεπιθύμητων αντιδράσεων αυξάνει κατά 3 φορές3 φορές σε ασθενείς με γνωστή αλλεργία (σε περιβαλλοντολογικούς σε ασθενείς με γνωστή αλλεργία (σε περιβαλλοντολογικούς παράγοντες ή φαρμακευτικά σκευάσματα) συγκριτικά με τους παράγοντες ή φαρμακευτικά σκευάσματα) συγκριτικά με τους ελεύθερους ιστορικού ελεύθερους ιστορικού
• Σχετιζόμενες με τον τύπο του χορηγούμενου ΣΜΣχετιζόμενες με τον τύπο του χορηγούμενου ΣΜ
• Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων δεν Ο κίνδυνος εμφάνισης ανεπιθύμητων αντιδράσεων δεν σχετίζεται με την ωσμωμοριακότητα του ΣΜ: μικρές σχετίζεται με την ωσμωμοριακότητα του ΣΜ: μικρές χορηγούμενες δόσεις χορηγούμενες δόσεις ωσμωτικό φορτίο πολύ μικρό ωσμωτικό φορτίο πολύ μικρό
Παράγοντες κινδύνου εμφάνισης οξέων ανεπιθύμητων Παράγοντες κινδύνου εμφάνισης οξέων ανεπιθύμητων αντιδράσεωναντιδράσεων

Ελάττωση Οξέων Παρενεργειών σκιαγραφικών με βάση το Ελάττωση Οξέων Παρενεργειών σκιαγραφικών με βάση το γαδολίνιογαδολίνιο
• Για όλους τους ασθενείς:Για όλους τους ασθενείς: • Κρατήστε τον ασθενή για Κρατήστε τον ασθενή για παρακολούθηση για 30παρακολούθηση για 30minmin μετά τη μετά τη
χορήγηση του σκιαγραφικούχορήγηση του σκιαγραφικού• Έχετε άμεσα διαθέσιμο τον εξοπλισμό και τα φάρμακα για Έχετε άμεσα διαθέσιμο τον εξοπλισμό και τα φάρμακα για
ανάνηψηανάνηψη• Για ασθενείς αυξημένου κινδύνουΓια ασθενείς αυξημένου κινδύνου
• Εξετάστε το ενδεχόμενο Εξετάστε το ενδεχόμενο εναλλακτικού τρόπου εξέτασηςεναλλακτικού τρόπου εξέτασης που να που να μην απαιτεί χρήση γαδολινίουμην απαιτεί χρήση γαδολινίου
• Χρήση Χρήση διαφορετικού σκευάσματος γαδολινίουδιαφορετικού σκευάσματος γαδολινίου, σε γνωστή , σε γνωστή προηγούμενη αντίδρασηπροηγούμενη αντίδραση
• Εξετάστε το ενδεχόμενο χορήγησης φαρμακευτικής αγωγής Εξετάστε το ενδεχόμενο χορήγησης φαρμακευτικής αγωγής προηγηθείσης της εξέτασης: προηγηθείσης της εξέτασης: 3030mg prednisolonemg prednisolone ( (ή ή 32mg 32mg methylprednisolone)methylprednisolone) από του στόματος από του στόματος 12 και 2 ώρες πριν12 και 2 ώρες πριν τη τη χορήγηση του σκιαγραφικούχορήγηση του σκιαγραφικού

Ι. Μη νεφρικές ανεπιθύμητες ενέργειεςΙ. Μη νεφρικές ανεπιθύμητες ενέργειες
1.1. ΆμεσεςΆμεσες
2.2. Όψιμες - ΚαθυστερημένεςΌψιμες - Καθυστερημένες

Όψιμες παρενέργειες σκιαγραφικών με βάση το Όψιμες παρενέργειες σκιαγραφικών με βάση το γαδολίνιογαδολίνιο
Νεφρογενής Συστηματική Σκλήρυνση (Νεφρογενής Συστηματική Σκλήρυνση (NSF)NSF)
• Ινωτική νόσος που προσβάλει αρχικά το δέρμα και τον Ινωτική νόσος που προσβάλει αρχικά το δέρμα και τον υποδόριο ιστό, αλλά και τους πνεύμονες, οισοφάγο, υποδόριο ιστό, αλλά και τους πνεύμονες, οισοφάγο, καρδιά και σκελετικούς μύες.καρδιά και σκελετικούς μύες.
• Άρχεται από τη μέρα της χορήγησης έως 6 μήνες ή και Άρχεται από τη μέρα της χορήγησης έως 6 μήνες ή και χρόνια μετάχρόνια μετά
• Η σχέση μεταξύ Νεφρογενούς Συστηματικής Η σχέση μεταξύ Νεφρογενούς Συστηματικής Σκλήρυνσης (Σκλήρυνσης (NSF) NSF) και σκιαγραφικών μέσων και σκιαγραφικών μέσων γαδολινίου αναγνωρίστηκε το 2006γαδολινίου αναγνωρίστηκε το 2006
• Συνολική επίπτωση σε ασθενείς με νεφρική Συνολική επίπτωση σε ασθενείς με νεφρική ανεπάρκεια (ΧΝΑ σταδίου 4 και 5) ανεπάρκεια (ΧΝΑ σταδίου 4 και 5) 1-7%1-7%

ΠαθοφυσιολογίαΠαθοφυσιολογία
• Σε ασθενείς με Σε ασθενείς με έκπτωση της νεφρικής λειτουργίαςέκπτωση της νεφρικής λειτουργίας επιμηκύνεται ο επιμηκύνεται ο χρόνος ημίσειας ζωής (από 90 χρόνος ημίσειας ζωής (από 90 min min σε 30σε 30h h ή και περισσότερο)ή και περισσότερο) αυξάνοντας την πιθανότητα αυξάνοντας την πιθανότητα απομετάλλωσης και αποσύνδεσης απομετάλλωσης και αποσύνδεσης μορίου μορίου Gd-ligandGd-ligand οδηγώντας στην απόδοση ελεύθερου οδηγώντας στην απόδοση ελεύθερου GdGd+3+3
• To To ελεύθερο ελεύθερο GdGd+3+3 ενώνεται με ενδογενή ανιόντα ιδίως φωσφορικά ενώνεται με ενδογενή ανιόντα ιδίως φωσφορικά και σχηματίζουν αδιάλυτα άλατα που εναποτίθενται στους ιστούς και σχηματίζουν αδιάλυτα άλατα που εναποτίθενται στους ιστούς φαγοκυτταρώνονται από μακροφάγα φαγοκυτταρώνονται από μακροφάγα απελευθρώνονται κυτοκίνες απελευθρώνονται κυτοκίνες προσελκύονται ινοκύτταραπροσελκύονται ινοκύτταρα
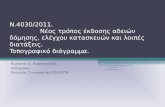
Νεφρογενής Συστηματική ΣκλήρυνσηΝεφρογενής Συστηματική Σκλήρυνση
ΊνωσηΊνωση

Νεφρογενής Συστηματική ΣκλήρυνσηΝεφρογενής Συστηματική Σκλήρυνση
Κλινική εικόναΚλινική εικόνα• Αρχικά Αρχικά
• Άλγος, κνίδωση, οίδημα, ερύθημα, συνήθως Άλγος, κνίδωση, οίδημα, ερύθημα, συνήθως άρχεται στα κάτω άκραάρχεται στα κάτω άκρα
• ΑργότεραΑργότερα• Πάχυνση του δέρματος και του υποδορίου ιστού – Πάχυνση του δέρματος και του υποδορίου ιστού –
«ξυλώδης» υφή και υπόφαιες πλάκες «ξυλώδης» υφή και υπόφαιες πλάκες • Ίνωση των εσωτερικών οργάνων, π.χ. μυών, Ίνωση των εσωτερικών οργάνων, π.χ. μυών,
διαφράγματος, καρδιάς, ήπατος, πνευμόνωνδιαφράγματος, καρδιάς, ήπατος, πνευμόνων• ΑποτέλεσμαΑποτέλεσμα
• Μόνιμη σύσπαση μυώνΜόνιμη σύσπαση μυών• ΚαχεξίαΚαχεξία• Θάνατος σε κάποιο ποσοστό ασθενώνΘάνατος σε κάποιο ποσοστό ασθενών

Severity gradeSeverity grade
• 0: no symptoms,0: no symptoms,• 1: mild physical,1: mild physical, cosmetic or neuropathic symptoms not cosmetic or neuropathic symptoms not
causing any kind of disabilitycausing any kind of disability• 2: moderate physical and/or neuropathic symptoms 2: moderate physical and/or neuropathic symptoms
limiting physicallimiting physical performance to some extentperformance to some extent• 3: severe symptoms limiting daily physical activities 3: severe symptoms limiting daily physical activities
(walking, bathing, shopping etc.(walking, bathing, shopping etc.• 4: severely disabling symptoms causing dependence on 4: severely disabling symptoms causing dependence on
aid or devices for common, daily activitiesaid or devices for common, daily activities
American College of Radiology. Manual of Contrast Media Version 7 2010


Νεφρογενής Συστηματική ΣκλήρυνσηΝεφρογενής Συστηματική Σκλήρυνση
Παράγοντες κινδύνουΠαράγοντες κινδύνου• Υψηλού κινδύνου :Υψηλού κινδύνου :
• Ασθενείς με Ασθενείς με ΧΝΑ σταδίου 4 και 5ΧΝΑ σταδίου 4 και 5 ((GFR<30ml/min)GFR<30ml/min)• Ασθενείς σε Ασθενείς σε περιτοναϊκή κάθαρσηπεριτοναϊκή κάθαρση• Ασθενείς με μειωμένη νεφρική λειτουργία που έχουν ή πρόκειται Ασθενείς με μειωμένη νεφρική λειτουργία που έχουν ή πρόκειται
να υποβληθούν σε να υποβληθούν σε μεταμόσχευση ήπατοςμεταμόσχευση ήπατος
• Χαμηλού κινδύνουΧαμηλού κινδύνου• Ασθενείς με ΧΝΑ σταδίου 3 Ασθενείς με ΧΝΑ σταδίου 3 ((GFRGFR 3030-59-59ml/min)ml/min)• Παιδιά <1έτουςΠαιδιά <1έτους, λόγω μη ωρίμανσης της νεφρικής λειτουργίας, λόγω μη ωρίμανσης της νεφρικής λειτουργίας
• Χωρίς κίνδυνοΧωρίς κίνδυνο• Ασθενείς με φυσιολογική νεφρική λειτουργίαΑσθενείς με φυσιολογική νεφρική λειτουργία
** ΟΝΑ δεν αντικατοπτρίζεται πάντα σε ΟΝΑ δεν αντικατοπτρίζεται πάντα σε SCrSCr ή ή GFRGFR

Δυνητικοί επιβαρυντικοί παράγοντεςΔυνητικοί επιβαρυντικοί παράγοντες
• Υψηλές δόσεις έκθεσης σε Υψηλές δόσεις έκθεσης σε GdGd σε μία ή σε μία ή επαναλαμβανόμενες χορηγήσειςεπαναλαμβανόμενες χορηγήσεις
• Υψηλές δόσεις ερυθροποιητίνηςΥψηλές δόσεις ερυθροποιητίνης• Μεταβολική οξέωσηΜεταβολική οξέωση• Σίδηρος και φερριτίνηΣίδηρος και φερριτίνη• Υπερφωσφαταιμία, υπερασβεστιαιμία Υπερφωσφαταιμία, υπερασβεστιαιμία • Ανοσοκαταστολή / ΑγγειοπάθειαΑνοσοκαταστολή / Αγγειοπάθεια• Χρόνια φλεγμονήΧρόνια φλεγμονή• ΥπερπηκτικότηταΥπερπηκτικότητα• Θρομβωτικά επεισόδιαΘρομβωτικά επεισόδια• Πρόσφατο χειρουργείο αγγειακό ή μηΠρόσφατο χειρουργείο αγγειακό ή μη• Πρόσφατη ανεπάρκεια νεφρικού μοσχεύματοςΠρόσφατη ανεπάρκεια νεφρικού μοσχεύματος
Νεφρογενής Συστηματική ΣκλήρυνσηΝεφρογενής Συστηματική Σκλήρυνση

Σκιαγραφικά μέσα: Ταξινόμηση και συστάσειςΣκιαγραφικά μέσα: Ταξινόμηση και συστάσεις• Υψηλού κινδύνου σκιαγραφικά μέσα για Υψηλού κινδύνου σκιαγραφικά μέσα για NSFNSF
• Gadodiamide Gadodiamide (Ο(Οmniscanmniscan):): Επίπτωση Επίπτωση NSF NSF σε ασθενείς υψηλού κινδύνου 3-7%σε ασθενείς υψηλού κινδύνου 3-7%• Gadopentetate dimeglumine Gadopentetate dimeglumine (Magnevist)(Magnevist):: Επίπτωση Επίπτωση NSF NSF σε ασθενείς υψηλού σε ασθενείς υψηλού
κινδύνου 0,1-1%κινδύνου 0,1-1%• Gadoversetamide Gadoversetamide (Optimark) (Optimark) :: Άγνωστη επίπτωση Άγνωστη επίπτωση NSFNSF
ΣυστάσειςΣυστάσεις• Η χρήση τους Η χρήση τους ΑΝΤΕΝΔΕΙΚΝΥΤΑΙ ΑΝΤΕΝΔΕΙΚΝΥΤΑΙ σεσε
Ασθενείς με ΧΝΑ σταδίου 4 και 5 (Ασθενείς με ΧΝΑ σταδίου 4 και 5 (eGFR<30ml/min), eGFR<30ml/min), αιμοκαθαιρόμενουςαιμοκαθαιρόμενους και ασθενείς με ΟΝΑκαι ασθενείς με ΟΝΑ
Νεογνά και εγκυμονούσεςΝεογνά και εγκυμονούσες Ασθενείς με μειωμένη νεφρική λειτουργία είναι μεταμοσχευμένοι ή Ασθενείς με μειωμένη νεφρική λειτουργία είναι μεταμοσχευμένοι ή
πρόκειται να υποβληθούν σε μεταμόσχευση ήπατοςπρόκειται να υποβληθούν σε μεταμόσχευση ήπατος
• Χορήγηση Χορήγηση μεμε προσοχήπροσοχή σε σε Ασθενείς με ΧΝΑ σταδίου 3 (Ασθενείς με ΧΝΑ σταδίου 3 (eGFReGFR 3030-60-60ml/min), ml/min), τουλάχιστον 7ημ τουλάχιστον 7ημ
μεταξύ των χορηγήσεωνμεταξύ των χορηγήσεων Παιδιά <1 έτουςΠαιδιά <1 έτους
Ποτέ σε δοση >0,1Ποτέ σε δοση >0,1mmol/Kgr mmol/Kgr σε κάθε ασθενήσε κάθε ασθενή
ΑΠΑΡΑΙΤΗΤΗ η μέτρηση κρεατινίνης ορού πριν τη χορήγησηΑΠΑΡΑΙΤΗΤΗ η μέτρηση κρεατινίνης ορού πριν τη χορήγηση

Σκιαγραφικά μέσα: Ταξινόμηση και συστάσειςΣκιαγραφικά μέσα: Ταξινόμηση και συστάσεις
• Ενδιάμεσου κινδύνου σκιαγραφικά μέσα για Ενδιάμεσου κινδύνου σκιαγραφικά μέσα για NSFNSF• Gadobenate dimeglumineGadobenate dimeglumine ((MultihanceMultihance):): Ιονικό Ιονικό γραμμικόγραμμικό μόριο ( μόριο (BOPTA)BOPTA)
Επίπτωση Επίπτωση NSF NSF δεν έχει διευκρινιστεί. Δυνατή η δεν έχει διευκρινιστεί. Δυνατή η χρήση 50% χαμηλότερων χρήση 50% χαμηλότερων δόσεωνδόσεων με ικανοποιητικό απεικονιστικό αποτέλεσμα με ικανοποιητικό απεικονιστικό αποτέλεσμα
• Gadofosveset trisodium (Gadofosveset trisodium (VasovistVasovist)): : Ιονικό Ιονικό γραμμικόγραμμικό μόριο ( μόριο (DTPA-DPCP)DTPA-DPCP) Επίπτωση Επίπτωση NSF NSF δεν έχει διευκρινιστεί. Παράγοντας που παραμένει στο αίμα με δεν έχει διευκρινιστεί. Παράγοντας που παραμένει στο αίμα με
συνάφεια στην αλβουμίνη. Διαγνωστικά αποτελέσματα επιτυγχάνονται με το συνάφεια στην αλβουμίνη. Διαγνωστικά αποτελέσματα επιτυγχάνονται με το 50% της δόσης50% της δόσης των εξωκυττάριων των εξωκυττάριων Gd-CM, Gd-CM, αλλά 12πλάσιος ημίσειας ζωήςαλλά 12πλάσιος ημίσειας ζωής
• Gadoxetate disodium (Gadoxetate disodium (Primovist, EovistPrimovist, Eovist) :) : ιονικό ιονικό γραμμικόγραμμικό μόριο ( μόριο (EOB-EOB-DTPA)DTPA)
Επίπτωση Επίπτωση NSF NSF δεν έχει διευκρινιστεί, αλλά με περιορισμένα δεδομέναδεν έχει διευκρινιστεί, αλλά με περιορισμένα δεδομένα. . Δυνατή Δυνατή η χρήση χαμηλότερων δόσεων με ικανοποιητικό απεικονιστικό αποτέλεσμαη χρήση χαμηλότερων δόσεων με ικανοποιητικό απεικονιστικό αποτέλεσμα
ΣυστάσειςΣυστάσεις• Η χρήση τους Η χρήση τους ΜΕ ΠΡΟΣΟΧΗ ΜΕ ΠΡΟΣΟΧΗ σεσε
Ασθενείς με ΧΝΑ σταδίου 4 και 5 (Ασθενείς με ΧΝΑ σταδίου 4 και 5 (eGFR<30ml/min), eGFR<30ml/min), αιμοκαθαιρόμενουςαιμοκαθαιρόμενους και ασθενείς με ΟΝΑκαι ασθενείς με ΟΝΑ
Η μέτρηση κρεατινίνης ορού πριν τη χορήγηση ΔΕΝ ΕΙΝΑΙ ΑΠΑΡΑΙΤΗΤΗΗ μέτρηση κρεατινίνης ορού πριν τη χορήγηση ΔΕΝ ΕΙΝΑΙ ΑΠΑΡΑΙΤΗΤΗ

Σκιαγραφικά μέσα: Ταξινόμηση και συστάσειςΣκιαγραφικά μέσα: Ταξινόμηση και συστάσεις
Χαμηλού κινδύνου σκιαγραφικά μέσα για Χαμηλού κινδύνου σκιαγραφικά μέσα για NSFNSF• Gadobutrol (Gadobutrol (Gadovist, GadavistGadovist, Gadavist):): Μη ιονικό Μη ιονικό κυκλικό κυκλικό μόριο (μόριο (BT-BT-
DO3A) DO3A) Δεν έχουν αναφερθεί περιστατικά Δεν έχουν αναφερθεί περιστατικά NSFNSF. .
• Gadoterate meglumine (Gadoterate meglumine (Dotarem, MagnescopeDotarem, Magnescope)):: Ιονικό Ιονικό κυκλικόκυκλικό μόριο μόριο ((DOTA)DOTA)
Δεν έχουν αναφερθεί περιστατικά Δεν έχουν αναφερθεί περιστατικά NSFNSF. . • Gadoteridol (Prohance) :Gadoteridol (Prohance) : Μη ιονικό Μη ιονικό κυκλικό κυκλικό μόριο (μόριο (HP-DO3A) HP-DO3A)
Δεν έχουν αναφερθεί περιστατικά Δεν έχουν αναφερθεί περιστατικά NSFNSF. .
Η μέτρηση κρεατινίνης ορού πριν τη χορήγηση ΔΕΝ ΕΙΝΑΙ Η μέτρηση κρεατινίνης ορού πριν τη χορήγηση ΔΕΝ ΕΙΝΑΙ ΑΠΑΡΑΙΤΗΤΗΑΠΑΡΑΙΤΗΤΗ
Προτεινόμενη ΔοσολογίαΠροτεινόμενη Δοσολογία
• 00,1,1mmol/Kgr mmol/Kgr ΒΣΒΣ
• Μέγιστη δόση 0,3Μέγιστη δόση 0,3mmol/Kgr mmol/Kgr ΒΣΒΣ

ΙΙ. Νεφρικές ανεπιθύμητες ενέργειεςΙΙ. Νεφρικές ανεπιθύμητες ενέργειες
Νεφροτοξικότητα Νεφροτοξικότητα
• Οξεία νεφρική ανεπάρκεια (ΟΝΑ) σε ασθενείς με προηγούμενη Οξεία νεφρική ανεπάρκεια (ΟΝΑ) σε ασθενείς με προηγούμενη σοβαρή έκπτωση νεφρικής λειτουργίαςσοβαρή έκπτωση νεφρικής λειτουργίας
Παράγοντες κινδύνουΠαράγοντες κινδύνου Μεγάλη ηλικίαΜεγάλη ηλικία Χαμηλή Χαμηλή SCr SCr αναφοράςαναφοράς Διαβητική νεφροπάθειαΔιαβητική νεφροπάθεια Χαμηλή αιμοσφαιρίνη και αλβουμίνηΧαμηλή αιμοσφαιρίνη και αλβουμίνη ΔοσολογίαΔοσολογία
ΠαθοφυσιολογίαΠαθοφυσιολογία
1.1. Υπερωσμωτικότητα χηλικών ενώσεων γαδολινίουΥπερωσμωτικότητα χηλικών ενώσεων γαδολινίου
2.2. Άμεση βλάβη των νεφρικών σωληναρίων λόγω τοξικότηταςΆμεση βλάβη των νεφρικών σωληναρίων λόγω τοξικότητας Περιορισμένα δεδομένα όσον αφορά το μηχανισμό πρόκλησης Περιορισμένα δεδομένα όσον αφορά το μηχανισμό πρόκλησης

Νεφρικές παρενέργειες σκιαγραφικών με βάση το Νεφρικές παρενέργειες σκιαγραφικών με βάση το γαδολίνιογαδολίνιο
Εξετάσεις Μαγνητικής Τομογραφίας Εξετάσεις Μαγνητικής Τομογραφίας Ο κίνδυνος νεφροτοξικότητας είναι Ο κίνδυνος νεφροτοξικότητας είναι πολύ χαμηλόςπολύ χαμηλός όταν όταν
χρησιμοποιούνται σκιαγραφικά μέσα γαδολινίου στις χρησιμοποιούνται σκιαγραφικά μέσα γαδολινίου στις επιτρεπόμενες δόσεις επιτρεπόμενες δόσεις ((μέγιστη επιτρεπόμενη δόση μέγιστη επιτρεπόμενη δόση 0,30,3mmol/kgmmol/kgΣ.Β)Σ.Β)
Ακτινολογικές εξετάσειςΑκτινολογικές εξετάσεις Τα σκιαγραφικά μέσα γαδολινίου Τα σκιαγραφικά μέσα γαδολινίου δενδεν θα πρέπει να θα πρέπει να
χρησιμοποιούνται για ακτινολογικές εξετάσεις σε ασθενείς χρησιμοποιούνται για ακτινολογικές εξετάσεις σε ασθενείς με με νεφρική ανεπάρκειανεφρική ανεπάρκεια
Τα σκιαγραφικά μέσα γαδολινίου είναι Τα σκιαγραφικά μέσα γαδολινίου είναι πιο νεφροτοξικάπιο νεφροτοξικά από τα από τα ιωδιωμένα σκιαγραφικά μέσα σε ισοδύναμες δόσεις ακτινοβολίας ιωδιωμένα σκιαγραφικά μέσα σε ισοδύναμες δόσεις ακτινοβολίας ΧΧ

Αιμοκάθαρση και χορήγηση σκιαγραφικών μέσωνΑιμοκάθαρση και χορήγηση σκιαγραφικών μέσων
Τα σκιαγραφικά μέσα μπορούν να απομακρυνθούν με την Τα σκιαγραφικά μέσα μπορούν να απομακρυνθούν με την αιμοκάθαρση ή την περιτοναϊκή διύλιση. αιμοκάθαρση ή την περιτοναϊκή διύλιση. Δεν έχει αποδειχθεί πως η Δεν έχει αποδειχθεί πως η αιμοκάθαρση προστατεύει τους ασθενείς με έκπτωση της νεφρικής αιμοκάθαρση προστατεύει τους ασθενείς με έκπτωση της νεφρικής τους λειτουργίας από την ανάπτυξη νεφροτοξικότητας από τα τους λειτουργίας από την ανάπτυξη νεφροτοξικότητας από τα σκιαγραφικά μέσα (σκιαγραφικά μέσα (CIN) CIN) ή νεφροτοξικότητας από τα σκιαγραφικά ή νεφροτοξικότητας από τα σκιαγραφικά μέσα (μέσα (CIN) CIN) ή νεφρογενούς συστηματικής σκλήρυνσηςή νεφρογενούς συστηματικής σκλήρυνσης ((NSF)NSF)
Συστάσεις για αιμοκαθαιρόμενους ή ασθενείς σε περιτοναϊκή κάθαρσηΣυστάσεις για αιμοκαθαιρόμενους ή ασθενείς σε περιτοναϊκή κάθαρση• Αποφυγή υπερβολικού φορτίου ωσμωτικών και υγρώνΑποφυγή υπερβολικού φορτίου ωσμωτικών και υγρών• Συσχετισμός χρόνου χορήγησης του σκιαγραφικού και του χρόνου Συσχετισμός χρόνου χορήγησης του σκιαγραφικού και του χρόνου
συνεδρίας αιμοκάθαρσης πρέπει να συζητηθεί με τον συνεδρίας αιμοκάθαρσης πρέπει να συζητηθεί με τον παραπέμπονταπαραπέμποντα

ESUR Guidelines on ESUR Guidelines on Contrast Media Contrast Media European Society of European Society of UUrogenital Radiologyrogenital Radiology

Υπολογιστική & Ψηφιακή Υπολογιστική & Ψηφιακή Αφαιρετική Αγγειογραφία με χρήση Αφαιρετική Αγγειογραφία με χρήση
σκιαγραφικού μέσου με βάση το σκιαγραφικού μέσου με βάση το γαδολίνιογαδολίνιο

CTA CTA ήή DSA DSA με χρήση γαδολινίουμε χρήση γαδολινίου
• Το γαδολίνιο λόγω του υψηλού ατομικού του αριθμού Το γαδολίνιο λόγω του υψηλού ατομικού του αριθμού ((Gd=64) Gd=64) έχει την ιδιότητα να εξασθενεί τις ακτίνες Χ έχει την ιδιότητα να εξασθενεί τις ακτίνες Χ
• Μπορεί να χρησιμοποιηθεί ως σκιαγραφικό μέσο σε Μπορεί να χρησιμοποιηθεί ως σκιαγραφικό μέσο σε CTA CTA ή DSA και να δώσει ποιοτικές εικόνες για αγγειογραφικές ή DSA και να δώσει ποιοτικές εικόνες για αγγειογραφικές και επεμβατικές εξετάσεις και επεμβατικές εξετάσεις
• Αποτελεί εναλλακτική λύση σε ασθενείς Αποτελεί εναλλακτική λύση σε ασθενείς αλλεργικούςαλλεργικούς σε σε ιωδιούχα σκιαγραφικά μέσα, σε ασθενείς με ιωδιούχα σκιαγραφικά μέσα, σε ασθενείς με σοβαρή σοβαρή νεφρική ανεπάρκεια ή αιμοκαθαιρόμενουςνεφρική ανεπάρκεια ή αιμοκαθαιρόμενους και όταν και όταν αντενδείκνυται η χρήση αντενδείκνυται η χρήση COCO22

ΜειονεκτήματαΜειονεκτήματα
• Χαμηλότερη ποιότητα εικόνων συγκριτικά με τη χρήση Χαμηλότερη ποιότητα εικόνων συγκριτικά με τη χρήση ιωδιούχων σκιαγραφικών μέσων, λόγω ιωδιούχων σκιαγραφικών μέσων, λόγω χαμηλότερης χαμηλότερης μοριακής συγκέντρωσηςμοριακής συγκέντρωσης
• Η χορηγούμενη δόση δεν πρέπει να ξεπερνά το Η χορηγούμενη δόση δεν πρέπει να ξεπερνά το μέγιστο μέγιστο επιτρεπτό όριο των 0,3επιτρεπτό όριο των 0,3 mmol/Kg mmol/KgΣ.Β.Σ.Β., ειδικά αν πρόκειται , ειδικά αν πρόκειται για νεφροπαθείς (ασθενής 70για νεφροπαθείς (ασθενής 70KgKg – 50 – 50ml ml ΣΜ γαδολινίου)ΣΜ γαδολινίου)

Αναφερόμενες ανεπιθύμητες ενέργειεςΑναφερόμενες ανεπιθύμητες ενέργειες
• Δυσανεξία στην εκλεκτική αγγειογραφία Δυσανεξία στην εκλεκτική αγγειογραφία άκρων, πιθανόν λόγω υψηλής άκρων, πιθανόν λόγω υψηλής ωσμομοριακότητας – διάλυση του ωσμομοριακότητας – διάλυση του σκιαγραφικού με φυσιολογικό ορόσκιαγραφικού με φυσιολογικό ορό
• Οι αναφερόμενες ανεπιθύμητες ενέργειες του Οι αναφερόμενες ανεπιθύμητες ενέργειες του γαδολινίου όπως και στη διενέργεια γαδολινίου όπως και στη διενέργεια μαγνητικής τομογραφίαςμαγνητικής τομογραφίας

Αντικρουόμενα δεδομέναΑντικρουόμενα δεδομένα
• «Οι μελέτες έως σήμερα υποδεικνύουν ως «Οι μελέτες έως σήμερα υποδεικνύουν ως ασφαλέστερη την αγγειογραφία με γαδολίνιο σε ασφαλέστερη την αγγειογραφία με γαδολίνιο σε ασθενείς με επηρεασμένη νεφρική λειτουργία»ασθενείς με επηρεασμένη νεφρική λειτουργία»
• «Δεν υπάρχουν δεδομένα που να αποδεικνύουν την «Δεν υπάρχουν δεδομένα που να αποδεικνύουν την ασφάλεια του γαδολινίου σε δόσεις μεγαλύτερες του ασφάλεια του γαδολινίου σε δόσεις μεγαλύτερες του επιτρεπτού ορίου»επιτρεπτού ορίου»(1)(1)
• ««H H γενική τοξικότητα του γαδολινίου μπορεί να είναι γενική τοξικότητα του γαδολινίου μπορεί να είναι 6-26-255 φορές μεγαλύτερη από αυτή ισοδύναμων δόσεων φορές μεγαλύτερη από αυτή ισοδύναμων δόσεων ιωδιούχων σκιαγραφικών σε 70-kV DSA. Επομένως ιωδιούχων σκιαγραφικών σε 70-kV DSA. Επομένως ισοδύναμες δόσεις νέων ίωδιούχων σκιαγραφικών ισοδύναμες δόσεις νέων ίωδιούχων σκιαγραφικών έχουν ως αποτέλεσμα μικρότερη νεφροτοξικότητα από έχουν ως αποτέλεσμα μικρότερη νεφροτοξικότητα από τις έως σήμερα υπάρχουσες χηλικές ενώσεις τις έως σήμερα υπάρχουσες χηλικές ενώσεις γαδολινίου» γαδολινίου» ((22))
(1)(1) D.J Spinosa,D.J Spinosa, J A KaufmanJ A Kaufman et al et al Gadolinium Chelates in Angiography and Interventional Radiology: A Useful Gadolinium Chelates in Angiography and Interventional Radiology: A Useful Alternative to Iodinated Contrast Media for AngiographyAlternative to Iodinated Contrast Media for Angiography Radiology 2002; Radiology 2002; 223:319–325223:319–325
(2) (2) Nyman et al Nyman et al Are Gadolinium-basedAre Gadolinium-based Contrast Media Really SaferContrast Media Really Safer than Iodinated Media forthan Iodinated Media for Digital SubtractionDigital Subtraction Angiography in PatientsAngiography in Patients with Azotemia? Radiology with Azotemia? Radiology 2002; 223:311–3182002; 223:311–318

Σκιαγραφικά μέσα υπερηχογραφίαςΣκιαγραφικά μέσα υπερηχογραφίας

Σκιαγραφικά μέσα καιΣκιαγραφικά μέσα και ΥπερηχοτομογραφίαΥπερηχοτομογραφία
Φυσαλίδες αερίου έντονα ηχοανακλαστικές σε σχέση με Φυσαλίδες αερίου έντονα ηχοανακλαστικές σε σχέση με τους περιβάλλοντες ιστούς λόγω διαφορετικών φυσικών τους περιβάλλοντες ιστούς λόγω διαφορετικών φυσικών ιδιοτήτων και συμπεριφοράςιδιοτήτων και συμπεριφοράς

Κατηγορίες σκιαγραφικών μέσων Κατηγορίες σκιαγραφικών μέσων υπερηχογραφίαςυπερηχογραφίας
1.1. Μικροφυσαλίδες αερίου μη ενσωματωμένες σε κάψα Μικροφυσαλίδες αερίου μη ενσωματωμένες σε κάψα π.χ. ενεργοποιούμενες με κύματα υπερήχωνπ.χ. ενεργοποιούμενες με κύματα υπερήχων
2.2. Σταθεροποιημένες μικροφυσαλίδες αερίων (π.χ. με Σταθεροποιημένες μικροφυσαλίδες αερίων (π.χ. με σωματίδια σακχάρου)σωματίδια σακχάρου)
3.3. Μικροφυσαλίδες αερίου ενσωματωμένες σε κάψα Μικροφυσαλίδες αερίου ενσωματωμένες σε κάψα (π.χ. σε πρωτεΐνες, λιποσώματα ή πολυμερή)(π.χ. σε πρωτεΐνες, λιποσώματα ή πολυμερή)
4.4. Εναιώρημα μικροσωματιδίων ή γαλάκτωμα Εναιώρημα μικροσωματιδίων ή γαλάκτωμα ((perfluorooctyl bromide-PFOB)perfluorooctyl bromide-PFOB)
5.5. ΓαστρεντερικάΓαστρεντερικά

ΧαρακτηριστικάΧαρακτηριστικά
• Μικροφυσαλίδες (αέρας ή μη) σταθεροποιημένες με επικάλυψη Μικροφυσαλίδες (αέρας ή μη) σταθεροποιημένες με επικάλυψη βιοσυμβατού υλικού (πρωτεΐνες, λιπίδια, επιφανειοδραστικό βιοσυμβατού υλικού (πρωτεΐνες, λιπίδια, επιφανειοδραστικό παράγοντα, πολυμερή)παράγοντα, πολυμερή)
• Χρήση αερίων υψηλού μοριακού βάρουςΧρήση αερίων υψηλού μοριακού βάρους ( (αργή διάχυση αργή διάχυση διαμέσου των μεμβρανών – μακρά διάρκεια δράσης στην διαμέσου των μεμβρανών – μακρά διάρκεια δράσης στην κυκλοφορίακυκλοφορία))
• Διάμετρος <Διάμετρος <10 μm – 10 μm – αποφυγή εμβολισμού των τριχοειδώναποφυγή εμβολισμού των τριχοειδών• Αρκετά μικρά και σταθερά για να διασφαλιστεί η δίοδος από Αρκετά μικρά και σταθερά για να διασφαλιστεί η δίοδος από
την πνευμονική κυκλοφορία και τις καρδιακές κοιλότητες, στη την πνευμονική κυκλοφορία και τις καρδιακές κοιλότητες, στη συστηματική κυκλοφορία και η διατήρησή τους για ικανό συστηματική κυκλοφορία και η διατήρησή τους για ικανό χρονικό διάστημα για τη μελέτη των αγγείων και των βλαβώνχρονικό διάστημα για τη μελέτη των αγγείων και των βλαβών
• Το αέριο αποβάλλεται από τους πνεύμονες με την εκπνοή σε Το αέριο αποβάλλεται από τους πνεύμονες με την εκπνοή σε 10-1510-15min min μετά τη χορήγηση, ενώ οι σταθεροποιητικοί μετά τη χορήγηση, ενώ οι σταθεροποιητικοί παράγοντες φιλτράρονται από τους νεφρούς και παράγοντες φιλτράρονται από τους νεφρούς και απομακρύνονται από το ήπαρ απομακρύνονται από το ήπαρ


ΧαρακτηριστικάΧαρακτηριστικά
Το απεικονιστικό αποτέλεσμα εξαρτάται από τη Το απεικονιστικό αποτέλεσμα εξαρτάται από τη συμπιεστότητα των αερίωνσυμπιεστότητα των αερίων
Οι επικαλύψεις βελτιώνουν τη διατήρηση των Οι επικαλύψεις βελτιώνουν τη διατήρηση των φυσαλίδων του αερίου (σταθερότητα) και την φυσαλίδων του αερίου (σταθερότητα) και την ελαστικότητά τους (ακουστική ανάκλαση)ελαστικότητά τους (ακουστική ανάκλαση)
Η σταθερότητα της φυσαλίδας είναι ανάλογη Η σταθερότητα της φυσαλίδας είναι ανάλογη του πάχους της επικάλυψης τηςτου πάχους της επικάλυψης της
Η δράση της επικάλυψης είναι αντιστρόφως Η δράση της επικάλυψης είναι αντιστρόφως ανάλογη του μεγέθους της φυσαλίδαςανάλογη του μεγέθους της φυσαλίδας

Βασικές αρχές φυσικήςΒασικές αρχές φυσικής
• Η διέλευση των μικροφυσαλίδων διά μέσου ενός Η διέλευση των μικροφυσαλίδων διά μέσου ενός ακουστικού πεδίου προκαλεί συμπίεση και ακουστικού πεδίου προκαλεί συμπίεση και έκπτυξη αυτών (ταλάντευση)έκπτυξη αυτών (ταλάντευση)
• Στο διαγνωστικό εύρος συχνοτήτων (1-20Στο διαγνωστικό εύρος συχνοτήτων (1-20MHz) MHz) οι οι μικροφυσαλίδες συντονίζονται και μικροφυσαλίδες συντονίζονται και συμπεριφέρονται όπως τα μουσικά όργανασυμπεριφέρονται όπως τα μουσικά όργανα
• Εκπέμπουν αρμονικές ειδικές για τα είδη των Εκπέμπουν αρμονικές ειδικές για τα είδη των φυσαλίδωνφυσαλίδων

Βασικές αρχές φυσικήςΒασικές αρχές φυσικής
Η συμπεριφορά των φυσαλίδων εξαρτάται από την Η συμπεριφορά των φυσαλίδων εξαρτάται από την ακουστική πίεση που προκαλείται από τον ηχοβολέαακουστική πίεση που προκαλείται από τον ηχοβολέα
Το οπτικό αποτέλεσμα προέρχεται από την ανάκλαση Το οπτικό αποτέλεσμα προέρχεται από την ανάκλαση της ηχητικής δέσμης, την ασύμμετρη δόνηση και της ηχητικής δέσμης, την ασύμμετρη δόνηση και τελικά τη ρήξη των μικροφυσαλίδων τελικά τη ρήξη των μικροφυσαλίδων
Οι μεταβολές της συμπεριφοράς των μικροφυσαλίδων Οι μεταβολές της συμπεριφοράς των μικροφυσαλίδων πιθανόν να προκαλέσουν ανεπιθύμητες ενέργειεςπιθανόν να προκαλέσουν ανεπιθύμητες ενέργειες
Εξαρτώνται από το επίπεδο του μηχανικού δείκτη Εξαρτώνται από το επίπεδο του μηχανικού δείκτη ((MIMI), τις ιδιότητες του σκιαγραφικού μέσου και την ), τις ιδιότητες του σκιαγραφικού μέσου και την απεικονιστική ρύθμιση.απεικονιστική ρύθμιση.

Ανεπιθύμητες ενέργειες σκιαγραφικών Ανεπιθύμητες ενέργειες σκιαγραφικών μέσων υπερηχογραφίαςμέσων υπερηχογραφίας
Φαινόμενο σπηλαίωσηςΦαινόμενο σπηλαίωσης : : «ενδορρήξη» των «ενδορρήξη» των μικροφυσαλίδων – προκαλεί μεταβολές μικροφυσαλίδων – προκαλεί μεταβολές θερμοκρασίας και πίεσης στην περιοχήθερμοκρασίας και πίεσης στην περιοχή
1.1. Αιμόλυση Αιμόλυση
2.2. Συσσώρευση αιμοπεταλίωνΣυσσώρευση αιμοπεταλίων
3.3. Καταστροφή ενδοθηλίουΚαταστροφή ενδοθηλίου
4.4. Καρδιακές αρρυθμίεςΚαρδιακές αρρυθμίες
5.5. Διακοπή του αιματοεγκεφαλικού φραγμούΔιακοπή του αιματοεγκεφαλικού φραγμού

Αναφερόμενες ανεπιθύμητες ενέργειες Αναφερόμενες ανεπιθύμητες ενέργειες σκιαγραφικών μέσων υπερηχογραφίαςσκιαγραφικών μέσων υπερηχογραφίας
1.1. Συστηματικές Συστηματικές :: Κεφαλαλγία, υπερευαισθησία στο σημείο Κεφαλαλγία, υπερευαισθησία στο σημείο έγχυσης, κοιλιακό άλγος, αδυναμία, γενικευμένο ή έγχυσης, κοιλιακό άλγος, αδυναμία, γενικευμένο ή εντοπισμένο άλγος στο θώρακα ή την ράχη, κακουχίαεντοπισμένο άλγος στο θώρακα ή την ράχη, κακουχία
2.2. ΚαρδιαγγειακέςΚαρδιαγγειακές : : Κολπική μαρμαρυγή, ταχυκαρδία, Κολπική μαρμαρυγή, ταχυκαρδία, αίσθημα παλμών, υπέρτασηαίσθημα παλμών, υπέρταση
3.3. ΓαστρεντερικέςΓαστρεντερικές : : Ναυτία, διάρροια, δυσπεψία Ναυτία, διάρροια, δυσπεψία
4.4. ΝευρολογικέςΝευρολογικές : : Παραισθησίες, ζάλη, ξηροστομία, Παραισθησίες, ζάλη, ξηροστομία, διαταραχή γεύσης ή όσφρησης, αγγειοδιαστολή διαταραχή γεύσης ή όσφρησης, αγγειοδιαστολή
5.5. ΜυοσκελετικέςΜυοσκελετικές:: συσπάσεις μυών κάτω άκρων συσπάσεις μυών κάτω άκρων
6.6. ΑναπνευστικέςΑναπνευστικές : : Δύσπνοια Δύσπνοια
7.7. ΔερματικέςΔερματικές:: Εφίδρωση, εξάνθημα, κνησμός Εφίδρωση, εξάνθημα, κνησμός

Σύσταση για τη χρήση Σκιαγραφικών Μέσων Σύσταση για τη χρήση Σκιαγραφικών Μέσων ΥπερήχωνΥπερήχων
Χρήση μόνο σε σοβαρή κλινική ένδειξη και μετά Χρήση μόνο σε σοβαρή κλινική ένδειξη και μετά από εκτίμηση της αναλογίας κινδύνου/ωφέλειαςαπό εκτίμηση της αναλογίας κινδύνου/ωφέλειας
Χρήση υψηλών τιμών Μηχανικού Δείκτη (Χρήση υψηλών τιμών Μηχανικού Δείκτη (MIMI) μόνο ) μόνο αν υπάρχει σοβαρή ένδειξηαν υπάρχει σοβαρή ένδειξη
European Commitee for Medical Ultrasound Safety (ECMUS) 2004

Οδηγίες για τη χρήση Σκιαγραφικών Μέσων Οδηγίες για τη χρήση Σκιαγραφικών Μέσων ΥπερήχωνΥπερήχων
Τα σκιαγραφικά μέσα υπερήχων γενικώς είναι ασφαλήΤα σκιαγραφικά μέσα υπερήχων γενικώς είναι ασφαλή Αντένδειξη:Αντένδειξη: Σοβαρή καρδιακή νόσος (π.χ. Σοβαρή καρδιακή νόσος (π.χ. New York New York κλάση κλάση
III/IV)III/IV) Σοβαρότητα ΠαρενεργειώνΣοβαρότητα Παρενεργειών: :
• Οι παρενέργειες στην πλειονότητά τους είναι ήπιες και Οι παρενέργειες στην πλειονότητά τους είναι ήπιες και υποχωρούν χωρίς ανάγκη θεραπείαςυποχωρούν χωρίς ανάγκη θεραπείας
• Αλλεργικού τύπου παρενέργειες εμφανίζονται σπανίωςΑλλεργικού τύπου παρενέργειες εμφανίζονται σπανίως
Για τη Μείωση του Κινδύνου: Για τη Μείωση του Κινδύνου: • Έλεγχος για τυχόν δυσανεξία σε κάποιο από τα Έλεγχος για τυχόν δυσανεξία σε κάποιο από τα
συστατικά τουσυστατικά του• Χρήση του Χρήση του χαμηλότερου επιπέδου ακουστικής ισχύοςχαμηλότερου επιπέδου ακουστικής ισχύος
και το και το συντομότερο χρόνο εξέτασηςσυντομότερο χρόνο εξέτασης που επιτρέπει μια που επιτρέπει μια διαγνωστική εξέτασηδιαγνωστική εξέταση
ESUR Guidelines on Contrast Media 2009


Αγγειογραφία με Αγγειογραφία με COCO22

Φυσικοχημικές ιδιότητες COΦυσικοχημικές ιδιότητες CO22
• Έγχυση Έγχυση COCO22 ενδαγγειακά ενδαγγειακά σύνδεση με Η σύνδεση με Η22Ο και παραγωγή Ο και παραγωγή
ανθρακικού οξέος. Στο κυκλοφορούν αίμα μετατρέπεται σε ανθρακικού οξέος. Στο κυκλοφορούν αίμα μετατρέπεται σε HCO3HCO3- - . Επανέρχεται σε μορφή . Επανέρχεται σε μορφή COCO22 πριν την απομάκρυνσή πριν την απομάκρυνσή
του από τα τριχοειδή στον πνεύμονα.του από τα τριχοειδή στον πνεύμονα.• Η καρβονική ανυδράση καταλύει τη μετατροπή του Η καρβονική ανυδράση καταλύει τη μετατροπή του COCO22 σε σε
δικαρβονικά και πρωτόνια.δικαρβονικά και πρωτόνια.• Το Το COCO22 αποβάλλεται από τους πνεύμονες με μία διέλευση αποβάλλεται από τους πνεύμονες με μία διέλευση
• Φυσαλίδες Φυσαλίδες COCO22 που χορηγήθηκε ενδοφλεβίως πιθανόν να που χορηγήθηκε ενδοφλεβίως πιθανόν να
περάσουν στη συστηματική κυκλοφορία δια του ωοειδούς περάσουν στη συστηματική κυκλοφορία δια του ωοειδούς τρήματος ή από ενδοκαρδιακά διαφραγματικά ελλείμματα.τρήματος ή από ενδοκαρδιακά διαφραγματικά ελλείμματα.

• Μη τοξικό αέριοΜη τοξικό αέριο
• ΑόρατοΑόρατο
• Υψηλή συμπιεσιμότηταΥψηλή συμπιεσιμότητα
• Πολύ χαμηλό ιξώδες (1/400 σε σχέση με τα ιωδιούχα)Πολύ χαμηλό ιξώδες (1/400 σε σχέση με τα ιωδιούχα)
• Επιπλέει στα υγράΕπιπλέει στα υγρά
• Δεν διαλύεται και δεν αραιώνεται από το αίμαΔεν διαλύεται και δεν αραιώνεται από το αίμα
• 20 φορές πιο διαλυτό από το Ο20 φορές πιο διαλυτό από το Ο22
• Απομακρύνεται από τα αγγεία με μία μόνο δίοδο από Απομακρύνεται από τα αγγεία με μία μόνο δίοδο από τους πνεύμονεςτους πνεύμονες
• Στερείται αλλεργικών και νεφροτοξικών αντιδράσεωνΣτερείται αλλεργικών και νεφροτοξικών αντιδράσεων
Φυσικοχημικές ιδιότητες COΦυσικοχημικές ιδιότητες CO22

COCO2 2 ως σκιαγραφικό μέσοως σκιαγραφικό μέσο
ΠλεονεκτήματαΠλεονεκτήματα Μη αλλεργιογόνοΜη αλλεργιογόνο Μη νεφρο- ή ηπατοτοξικόΜη νεφρο- ή ηπατοτοξικό Χαμηλό ιξώδες Χαμηλό ιξώδες εύκολη εύκολη
έγχυση δια μικροκαθετήρα έγχυση δια μικροκαθετήρα Δυνατή η έγχυση μεγάλων Δυνατή η έγχυση μεγάλων
ποσοτήτων με ποσοτήτων με μικροκαθετήρα και μικροκαθετήρα και σκιαγράφηση εγγύς κλάδων σκιαγράφηση εγγύς κλάδων με παλινδρόμησημε παλινδρόμηση
ΜειονεκτήματαΜειονεκτήματα Αόρατο Αόρατο πιθανή μη ανιχνεύσιμη πιθανή μη ανιχνεύσιμη
διαρροή στο χώροδιαρροή στο χώρο Απαιτεί ειδικό σύστημα έγχυσηςΑπαιτεί ειδικό σύστημα έγχυσης Συμπιέσιμο αέριοΣυμπιέσιμο αέριο Αντενδείκνυται για τη Αντενδείκνυται για τη
σκιαγράφηση των εγκεφαλικών, σκιαγράφηση των εγκεφαλικών, στεφανιαίων και αγγείων της στεφανιαίων και αγγείων της θωρακικής αορτής θωρακικής αορτής
Ελάττωση ή εξάλειψη της Ελάττωση ή εξάλειψη της εικόνας λόγω εντερικών αερίων εικόνας λόγω εντερικών αερίων ή κινητικών σφαλμάτωνή κινητικών σφαλμάτων
Η καλή ποιότητα διαγνωστικών Η καλή ποιότητα διαγνωστικών εικόνων απαιτεί πιο εργώδη εικόνων απαιτεί πιο εργώδη εξέτασηεξέταση

ΕνδείξειςΕνδείξεις
Αγγειογραφία σε ασθενείς με Αγγειογραφία σε ασθενείς με αλλεργία σε ιωδιούχα αλλεργία σε ιωδιούχα σκιαγραφικά μέσασκιαγραφικά μέσα ήή νεφρική ανεπάρκεια,νεφρική ανεπάρκεια, με εξαίρεση τις με εξαίρεση τις στεφανιαίες και εγκεφαλικές αρτηρίες.στεφανιαίες και εγκεφαλικές αρτηρίες.
Σε σύνθετες επεμβατικές πράξεις κατ’ αποκλειστικότητα ή σε Σε σύνθετες επεμβατικές πράξεις κατ’ αποκλειστικότητα ή σε συνδυασμό με ιωδιούχο σκιαγραφικό προς ελαχιστοποίηση συνδυασμό με ιωδιούχο σκιαγραφικό προς ελαχιστοποίηση του κινδύνου νεφρικών επιπλοκών ή υπερφόρτωσης όγκου σε του κινδύνου νεφρικών επιπλοκών ή υπερφόρτωσης όγκου σε ασθενείς με Σ.Κ.Αασθενείς με Σ.Κ.Α
Σκιαγράφηση φλεβικού δικτύου κεντρικότερα θρόμβωσηςΣκιαγράφηση φλεβικού δικτύου κεντρικότερα θρόμβωσης Εμβολισμό ηπατικών βλαβώνΕμβολισμό ηπατικών βλαβών Διενέργεια Διενέργεια TIPS (Transjugular Intrahepatic Portosystemic TIPS (Transjugular Intrahepatic Portosystemic
Shunt) Shunt) Ενδαγγειακή αντιμετώπιση ανευρυσμάτων σε ασθενείς Ενδαγγειακή αντιμετώπιση ανευρυσμάτων σε ασθενείς
υψηλού κινδύνου για ανάπτυξη νεφροπάθειας ή για τον υψηλού κινδύνου για ανάπτυξη νεφροπάθειας ή για τον εντοπισμό ενδοδιαφυγώνεντοπισμό ενδοδιαφυγών

Απόλυτες ΑντενδείξειςΑπόλυτες Αντενδείξεις
Αγγειογραφία Αγγειογραφία καρωτίδων και ενδοεγκεφαλικών αρτηριώνκαρωτίδων και ενδοεγκεφαλικών αρτηριών – – νευροτοξικότητανευροτοξικότητα
ΣτεφανιογραφίαΣτεφανιογραφία – ισχαιμία – ισχαιμία Αρτηριακή Αρτηριακή αγγειογραφία σε πρηνή θέσηαγγειογραφία σε πρηνή θέση – απόφραξη – απόφραξη
σπονδυλικών αρτηριών – ισχαιμία Ν.Μ.σπονδυλικών αρτηριών – ισχαιμία Ν.Μ. Αρτηριακή αγγειογραφία Αρτηριακή αγγειογραφία με άρση της κεφαλής του ασθενούςμε άρση της κεφαλής του ασθενούς – –
παλινδρόμηση στην ενδοεγκεφαλική κυκλοφορία παλινδρόμηση στην ενδοεγκεφαλική κυκλοφορία Αγγειογραφία του Αγγειογραφία του φλεβικού σκέλους σε αρτηριοφλεβώδη φλεβικού σκέλους σε αρτηριοφλεβώδη
fistulafistula

Σχετικές ΑντενδείξειςΣχετικές Αντενδείξεις
Αναισθησία με ΝΟΑναισθησία με ΝΟ όταν χορηγούνται μεγάλοι όγκοι όταν χορηγούνται μεγάλοι όγκοι COCO22 – –
αύξηση έως 6 φορές του όγκου του χορηγούμενου αύξηση έως 6 φορές του όγκου του χορηγούμενου COCO22 λόγω λόγω
διάχυσης του ΝΟδιάχυσης του ΝΟ Σε ασθενείς με Σε ασθενείς με αναπνευστική ανεπάρκεια ή πνευμονική αναπνευστική ανεπάρκεια ή πνευμονική
υπέρτασηυπέρταση - χρήση μικρότερων όγκων - χρήση μικρότερων όγκων COCO22 και αύξηση του και αύξηση του
χρόνου μεταξύ των εγχύσεων (2-3΄)χρόνου μεταξύ των εγχύσεων (2-3΄) Σε ασθενείς με Σε ασθενείς με εντερική ισχαιμία ή ΑΑΑεντερική ισχαιμία ή ΑΑΑ – χρήση μικρότερων – χρήση μικρότερων
όγκων όγκων COCO22 και αύξηση του χρόνου μεταξύ των εγχύσεων (2- και αύξηση του χρόνου μεταξύ των εγχύσεων (2-
3΄)3΄) Για τη διενέργεια φλεβογραφίας: βαρύ εμφύσημα, πνευμονική Για τη διενέργεια φλεβογραφίας: βαρύ εμφύσημα, πνευμονική
υπέρταση, γνωστά ενδοκαρδιακά ελλείμματα διαφράγματος ή υπέρταση, γνωστά ενδοκαρδιακά ελλείμματα διαφράγματος ή πνευμονικές αρτηριοφλεβώδεις δυσπλασίεςπνευμονικές αρτηριοφλεβώδεις δυσπλασίες

Πιθανές ΕπιπλοκέςΠιθανές Επιπλοκές
Χορήγηση Υπερβολικού όγκουΧορήγηση Υπερβολικού όγκου
• Πτώση της Α.Π., βραδυκαρδία, και ανύψωση ST στο Πτώση της Α.Π., βραδυκαρδία, και ανύψωση ST στο ΗΚΓΗΚΓ
• Ισχαιμία οργάνων από παγίδευση Ισχαιμία οργάνων από παγίδευση COCO22 σε σε τροφοδοτούσες αρτηρίεςτροφοδοτούσες αρτηρίες
ΠρόληψηΠρόληψη • Δεν Δεν συνδέουμε ποτέ άμεσασυνδέουμε ποτέ άμεσα τον ενδαγγειακό καθετήρα τον ενδαγγειακό καθετήρα
με τη συσκευή παροχής με τη συσκευή παροχής COCO22
• Χρήση της πεπερασμένης πλαστικής σακούλας Χρήση της πεπερασμένης πλαστικής σακούλας χορήγησης χορήγησης COCO22

Πιθανές ΕπιπλοκέςΠιθανές Επιπλοκές
Ατμοσφαιρική μόλυνσηΑτμοσφαιρική μόλυνση
• Εύκολη και γρήγορη η αντικατάσταση Εύκολη και γρήγορη η αντικατάσταση COCO22 από από
ατμοσφαιρικό αέρα εντός της σύριγγας χορήγησηςατμοσφαιρικό αέρα εντός της σύριγγας χορήγησης
• Πιθανή όταν η παρατηρείται ελάττωση της συστολικής Πιθανή όταν η παρατηρείται ελάττωση της συστολικής
πίεσης του ασθενούς κατά 10-20πίεσης του ασθενούς κατά 10-20mmHgmmHg
ΠρόληψηΠρόληψη • Χρήση Χρήση στεγανού συστήματος παροχής στεγανού συστήματος παροχής COCO22

Παρενέργειες και ΑντιμετώπισηΠαρενέργειες και Αντιμετώπιση
Εξαρτώνται από τη χορηγούμενη δόση ή από τη Εξαρτώνται από τη χορηγούμενη δόση ή από τη μόλυνση του αέραμόλυνση του αέρα
• ΑορτογραφίαΑορτογραφία- - ναυτία, άλγοςναυτία, άλγος : τοποθέτηση σε δεξιά ή : τοποθέτηση σε δεξιά ή αριστερή ημικαθιστή θέση, ελάττωση της χορηγούμενης αριστερή ημικαθιστή θέση, ελάττωση της χορηγούμενης δόσης δόσης COCO22
• Περιφερική αρτηριογραφίαΠεριφερική αρτηριογραφία - - άλγοςάλγος : ελάττωση της : ελάττωση της χορηγούμενης δόσης χορηγούμενης δόσης COCO22 εκλεκτική αρτηριογραφία εκλεκτική αρτηριογραφία
• Φλεβογραφία άνω άκρουΦλεβογραφία άνω άκρου – – άλγοςάλγος : καθαρισμός της : καθαρισμός της σύριγγας με 3σύριγγας με 3cc COcc CO22 και χορήγηση 20-40 και χορήγηση 20-40cc cc λιδοκαΐνης λιδοκαΐνης
άμεσα πριν την έγχυση άμεσα πριν την έγχυση COCO22

Παρενέργειες και ΑντιμετώπισηΠαρενέργειες και Αντιμετώπιση
• Αορτογραφία ΑΑΑΑορτογραφία ΑΑΑ – παγίδευση φυσαλίδων στο ανεύρυσμα – παγίδευση φυσαλίδων στο ανεύρυσμα απόφραξη κάτω μεσεντερίου αρταπόφραξη κάτω μεσεντερίου αρτ.: συνήθως παροδική .: συνήθως παροδική
• Εκ παραδρομής Εκ παραδρομής χορήγηση υπερβολικής ποσότητας χορήγηση υπερβολικής ποσότητας COCO22 ή ή
ατμοσφαιρική μόλυνσηατμοσφαιρική μόλυνση – – παγίδευση αέρα στην πνευμονική παγίδευση αέρα στην πνευμονική αρτηρίααρτηρία σοβαρή υπόταση : σοβαρή υπόταση :
• Ακτινοσκόπηση: φυσαλίδες αέρα στην Π.Α. που εμμένουν Ακτινοσκόπηση: φυσαλίδες αέρα στην Π.Α. που εμμένουν >30>30secsec
• Τοποθέτηση σε θέση Τοποθέτηση σε θέση Trendelenburg Trendelenburg και και αριστερή πλάγια αριστερή πλάγια κατακεκλιμένη θέσηκατακεκλιμένη θέση
• ΑναρρόφησηΑναρρόφηση του αέρα με καθετήρα του αέρα με καθετήρα
I.F. Hawkins,et al Carbon Dioxide in Angiography to Reduce the Risk of Contrast- Induced Nephropathy Radiol Clin N Am 47 (2009) 813–825

ΣυνοψίζονταςΣυνοψίζοντας
• Η Η CTA CTA ή ή DSADSA με χρήση ως με χρήση ως COCO22 σκιαγραφικού μέσου σκιαγραφικού μέσου
αποτελεί εναλλακτική λύση σε ασθενείς αποτελεί εναλλακτική λύση σε ασθενείς αλλεργικούς σε αλλεργικούς σε ιωδιούχα σκιαγραφικά μέσαιωδιούχα σκιαγραφικά μέσα ή πάσχοντες από ή πάσχοντες από νεφρική νεφρική ανεπάρκειαανεπάρκεια
• Απαραίτητη η χρήση Απαραίτητη η χρήση στεγανού συστήματος χορήγησηςστεγανού συστήματος χορήγησης για την αποφυγή επιπλοκώνγια την αποφυγή επιπλοκών
• Τεχνικά πιο απαιτητική και χρονοβόραΤεχνικά πιο απαιτητική και χρονοβόρα
Kyung J Cho, Irvin F Hawkins Carbon Dioxide Angiography e-medicine 21 Oct 2008

Ε υ χ α ρ ι σ τ ώΕ υ χ α ρ ι σ τ ώ


Εξαγγείωση ΣΜΕξαγγείωση ΣΜ
Τύπος βλαβώνΤύπος βλαβών
• Συνήθως μικρές βλάβες. Συνήθως μικρές βλάβες.
• Οι σοβαρές περιλαμβάνουν Οι σοβαρές περιλαμβάνουν δερματικά έλκηδερματικά έλκη, , νέκρωση νέκρωση μαλακών ιστώνμαλακών ιστών και και σύνδρομο διαμερισματοποίησηςσύνδρομο διαμερισματοποίησης
Παράγοντες κινδύνουΠαράγοντες κινδύνου
• ΤεχνικοίΤεχνικοί:: χρήση ισχυρού χρήση ισχυρού εγχυτήεγχυτή, έγχυση σε λιγότερο , έγχυση σε λιγότερο ενδεδειγμένα ενδεδειγμένα σωματικά μέρησωματικά μέρη (κάτω άκρα, μικρές περιφερικές (κάτω άκρα, μικρές περιφερικές φλέβες), μεγάλος φλέβες), μεγάλος όγκος ΣΜόγκος ΣΜ και και ΣΜ υψηλής ωσμωτικότηταςΣΜ υψηλής ωσμωτικότητας
• Σχετικοί με τον ασθενή:Σχετικοί με τον ασθενή: Αδυναμία επικοινωνίας, εύθραυστες Αδυναμία επικοινωνίας, εύθραυστες κατεστραμμένες φλέβες, αρτηριακή ανεπάρκεια, κατεστραμμένες φλέβες, αρτηριακή ανεπάρκεια, προβληματική φλεβική/λεμφική παροχέτευση και η προβληματική φλεβική/λεμφική παροχέτευση και η παχυσαρκίαπαχυσαρκία

Εξαγγείωση ΣΜΕξαγγείωση ΣΜ
Τρόποι μείωσης του κινδύνου Τρόποι μείωσης του κινδύνου
• Η ενδοφλέβια τεχνική θα πρέπει να γίνεται πάντοτε πολύ Η ενδοφλέβια τεχνική θα πρέπει να γίνεται πάντοτε πολύ προσεκτικά με τη χρήση πλαστικού φλεβοκαθετήρα κατάλληλου προσεκτικά με τη χρήση πλαστικού φλεβοκαθετήρα κατάλληλου μεγέθους τοποθετημένου στη σωστή φλέβα, ώστε να ρυθμίζεται η μεγέθους τοποθετημένου στη σωστή φλέβα, ώστε να ρυθμίζεται η ροή κατά τη διάρκεια της έγχυσηςροή κατά τη διάρκεια της έγχυσης
• Έλεγχος της έγχυσης με φυσιολογικό ορόΈλεγχος της έγχυσης με φυσιολογικό ορό
• Χρησιμοποίηση Χρησιμοποίηση μη ιονικού ιωδιούχου ΣΜμη ιονικού ιωδιούχου ΣΜ Θεραπευτική αγωγήΘεραπευτική αγωγή
• Στις περισσότερες περιπτώσεις η συντηρητική αγωγή είναι Στις περισσότερες περιπτώσεις η συντηρητική αγωγή είναι επαρκήςεπαρκής
Ανύψωση των ποδιώνΑνύψωση των ποδιών Εφαρμογή παγοκύστεων τοπικάΕφαρμογή παγοκύστεων τοπικά Προσεκτική παρακολούθησηΠροσεκτική παρακολούθηση
• Σε υποψία σοβαρής βλάβης, παραπομπή σε χειρουργόΣε υποψία σοβαρής βλάβης, παραπομπή σε χειρουργό

Επιδράσεις ιωδιούχων ΣΜ στους πνεύμονεςΕπιδράσεις ιωδιούχων ΣΜ στους πνεύμονες
Πνευμονικές παρενέργειεςΠνευμονικές παρενέργειες
• ΒρογχόσπασμοςΒρογχόσπασμος
• Αυξημένη πνευμονική αγγειακή αντίστασηΑυξημένη πνευμονική αγγειακή αντίσταση
• Πνευμονικό οίδημαΠνευμονικό οίδημα Ασθενείς υψηλού κινδύνουΑσθενείς υψηλού κινδύνου
• Ιστορικό άσθματοςΙστορικό άσθματος
• Ιστορικό πνευμονικής υπέρτασηςΙστορικό πνευμονικής υπέρτασης
• Αρχόμενη καρδιακή ανεπάρκειαΑρχόμενη καρδιακή ανεπάρκεια
Τρόποι μείωσης κινδύνουΤρόποι μείωσης κινδύνου
• Χρησιμοποίηση σκιαγραφικών μέσων Χρησιμοποίηση σκιαγραφικών μέσων χαμηλής ωσμωτικότητας χαμηλής ωσμωτικότητας ή ισοωσμωτικάή ισοωσμωτικά
• Αποφυγή μεγάλων δόσεων ΣΜΑποφυγή μεγάλων δόσεων ΣΜ

ΣΜ και όγκοι που παράγουν κατεχολαμίνη ΣΜ και όγκοι που παράγουν κατεχολαμίνη (Φαιοχρωμοκύττωμα – Παραγαγγλίωμα)(Φαιοχρωμοκύττωμα – Παραγαγγλίωμα)
Μετά τη χορήγηση υπερωσμωτικών ΣΜ προκαλείται αύξηση των Μετά τη χορήγηση υπερωσμωτικών ΣΜ προκαλείται αύξηση των κατεχολαμινών. Σε άμεση έγχυση στη νεφρική φλέβα ή αρτηρία κατεχολαμινών. Σε άμεση έγχυση στη νεφρική φλέβα ή αρτηρία μπορεί να προκληθεί υπερτασική κρίσημπορεί να προκληθεί υπερτασική κρίση
ΠροετοιμασίαΠροετοιμασία Εντοπισμός όγκου που παράγει κατεχολαμίνη και έχει ανιχνευθεί Εντοπισμός όγκου που παράγει κατεχολαμίνη και έχει ανιχνευθεί
βιοχημικάβιοχημικά1.1. Πριν την ΕΦ χορήγηση του σκιαγραφικού συνιστάται Πριν την ΕΦ χορήγηση του σκιαγραφικού συνιστάται α- και β-α- και β-
αδρενεργικός αποκλεισμόςαδρενεργικός αποκλεισμός με φάρμακα χορηγούμενα με φάρμακα χορηγούμενα per osper os. . Περαιτέρω α-αποκλεισμός με ΕΦ χορήγηση φαινοξυβενζαμίνης δεν Περαιτέρω α-αποκλεισμός με ΕΦ χορήγηση φαινοξυβενζαμίνης δεν είναι απαραίτητοςείναι απαραίτητος
2.2. Πριν την ενδαρτηριακή χορήγηση ιωδιούχου σκιαγραφικού μέσου Πριν την ενδαρτηριακή χορήγηση ιωδιούχου σκιαγραφικού μέσου προτείνεται προτείνεται α- και β-αδρενεργικός αποκλεισμόςα- και β-αδρενεργικός αποκλεισμός με φάρμακα με φάρμακα χορηγούμενα χορηγούμενα per osper os και και α-αποκλεισμός με ΕΦα-αποκλεισμός με ΕΦ χορήγηση χορήγηση φαινοξυβενζαμίνης υπό την επίβλεψη του παραπέμποντοςφαινοξυβενζαμίνης υπό την επίβλεψη του παραπέμποντος
Χαρακτηρισμός τυχαία ανακαλυφθείσας επινεφριδιακής μάζαςΧαρακτηρισμός τυχαία ανακαλυφθείσας επινεφριδιακής μάζας• Καμία ειδική προετοιμασίαΚαμία ειδική προετοιμασία
Χρησιμοποιούμενο ιωδιούχο ΣΜ: Χρησιμοποιούμενο ιωδιούχο ΣΜ: μη ιονικό μη ιονικό

Εγκυμοσύνη και θηλασμόςΕγκυμοσύνη και θηλασμός
ΕγκυμοσύνηΕγκυμοσύνη• Σε εξαιρετικές περιπτώσεις, όταν η ακτινογραφική Σε εξαιρετικές περιπτώσεις, όταν η ακτινογραφική
εξέταση είναι απαραίτητη, μπορούν να δοθούν ιωδιούχα εξέταση είναι απαραίτητη, μπορούν να δοθούν ιωδιούχα σκιαγραφικά σε εγκυμονούσασκιαγραφικά σε εγκυμονούσα
• Μετά τη χορήγηση ιωδιούχου ΣΜ κατά την εγκυμοσύνη, Μετά τη χορήγηση ιωδιούχου ΣΜ κατά την εγκυμοσύνη, πρέπει να πρέπει να ελεγχθεί η λειτουργία του θυρεοειδούς του ελεγχθεί η λειτουργία του θυρεοειδούς του νεογνούνεογνού την 1 την 1ηη εβδ της ζωής του εβδ της ζωής του
ΘηλασμόςΘηλασμός• Μετά τη χορήγηση ιωδιούχου ΣΜ ο θηλασμός μπορεί να Μετά τη χορήγηση ιωδιούχου ΣΜ ο θηλασμός μπορεί να
συνεχιστεί κανονικάσυνεχιστεί κανονικά Εγκυμοσύνη ή θηλάζουσα με νεφρική ανεπάρκειαΕγκυμοσύνη ή θηλάζουσα με νεφρική ανεπάρκεια
• Ισχύουν οι γενικοί κανόνες για τους νεφροπαθείς, χωρίς Ισχύουν οι γενικοί κανόνες για τους νεφροπαθείς, χωρίς ιδιαίτερες προφυλάξεις για το έμβρυο ή το νεογνό ιδιαίτερες προφυλάξεις για το έμβρυο ή το νεογνό

Διαδραστικότητα με άλλα φάρμακαΔιαδραστικότητα με άλλα φάρμακα
ΜεταφορμίνηΜεταφορμίνη Νεφροτοξικά φάρμακαΝεφροτοξικά φάρμακα
• Κυκλοσπορίνη, Κυκλοσπορίνη, CisplatinCisplatin, Αμινογλυκοσίδες, ΜΣΑΦ, Αμινογλυκοσίδες, ΜΣΑΦ Β-αναστολείςΒ-αναστολείς
• Μπορεί να μειώσουν την ανταπόκριση στη θεραπευτική Μπορεί να μειώσουν την ανταπόκριση στη θεραπευτική αγωγή του βρογχόσπασμουαγωγή του βρογχόσπασμου
Ιντερλευκίνη-2Ιντερλευκίνη-2• Αυξάνει κίνδυνο όψιμων δερματικών αντιδράσεων Αυξάνει κίνδυνο όψιμων δερματικών αντιδράσεων
ΠαπαβερίνηΠαπαβερίνη• Η σύγχρονη ενδαρτηριακή χορήγηση με το ΣΜ προκαλεί Η σύγχρονη ενδαρτηριακή χορήγηση με το ΣΜ προκαλεί
κατακρήμνιση του ΣΜ ενδαγγειακά με συνέπεια κατακρήμνιση του ΣΜ ενδαγγειακά με συνέπεια θρόμβωσηθρόμβωση

• Αποτελούνται από πυρήνα Αποτελούνται από πυρήνα οξειδίου του σιδήρουοξειδίου του σιδήρου διαμ 3-5nm, που διαμ 3-5nm, που περιβάλλεται από χαμηλού μοριακού βάρους δεξτράνη και περιβάλλεται από χαμηλού μοριακού βάρους δεξτράνη και καρβοδεξτράνη αντίστοιχα προς αποφυγή ανεξέλεγκτης καθίζησης καρβοδεξτράνη αντίστοιχα προς αποφυγή ανεξέλεγκτης καθίζησης μαγνητικών κρυστάλλωνμαγνητικών κρυστάλλωνπ.χ. Ferumoxides (Feridex), Ferucarbotan (Resovist)π.χ. Ferumoxides (Feridex), Ferucarbotan (Resovist)
• Παράγοντες Τ2 χαλάρωσηςΠαράγοντες Τ2 χαλάρωσης: απώλεια σήματος σες Τ2 και Τ2* : απώλεια σήματος σες Τ2 και Τ2* ακολουθίεςακολουθίες
• Τα μικρά σωματίδια (USPIOs) κυκλοφορούν περισσότερο στο αίμα Τα μικρά σωματίδια (USPIOs) κυκλοφορούν περισσότερο στο αίμα και συσσωρεύονται σε μακροφάγα όπως στους λεμφαδένες, το και συσσωρεύονται σε μακροφάγα όπως στους λεμφαδένες, το σπλήνα και το ήπαρ, ενώ τα μεγάλα σωματίδια (SPIOs) είναι πιο σπλήνα και το ήπαρ, ενώ τα μεγάλα σωματίδια (SPIOs) είναι πιο ειδικά για το ήπαρ.ειδικά για το ήπαρ.
• Μετά την έγχυσή τους μεταβολίζονται σε διαλυτή μη-Μετά την έγχυσή τους μεταβολίζονται σε διαλυτή μη-υπερπαραμαγνητική μορφή σιδήρου. υπερπαραμαγνητική μορφή σιδήρου.
• Ενσωματώνεται στην αποθήκη σιδήρου του σώματος (π.χ. Ενσωματώνεται στην αποθήκη σιδήρου του σώματος (π.χ. φεριττίνη, αιμοσιδηρίνη και αιμοσφαιρίνη) εντός λίγων ημερών φεριττίνη, αιμοσιδηρίνη και αιμοσφαιρίνη) εντός λίγων ημερών
2. Υπερπαραμαγνητικά μέσα ΣΑ2. Υπερπαραμαγνητικά μέσα ΣΑ

Χηλικές ενώσεις γαδολινίου (Χηλικές ενώσεις γαδολινίου (Gd)Gd)
Φυσικοχημικές ιδιότητεςΦυσικοχημικές ιδιότητες
• Το Το GdGd3+ 3+ είναι σπάνιο στοιχείο με ισχυρές παραμαγνητικές ιδιότητες. είναι σπάνιο στοιχείο με ισχυρές παραμαγνητικές ιδιότητες. Ελεύθερο είναι εξαιρετικά τοξικό, γι’ αυτό ως σκιαγραφικά χρησιμοποιούνται Ελεύθερο είναι εξαιρετικά τοξικό, γι’ αυτό ως σκιαγραφικά χρησιμοποιούνται χηλικές του ενώσειςχηλικές του ενώσεις
• To GdTo Gd3+ 3+ διαθέτει 9 θέσεις σύνδεσηςδιαθέτει 9 θέσεις σύνδεσης
• Εξαιρετικά υδρόφιλα μόρια με φαρμακοκινητικά χαρακτηριστικά παρόμοια Εξαιρετικά υδρόφιλα μόρια με φαρμακοκινητικά χαρακτηριστικά παρόμοια με των ιωδιούχων ΣΜμε των ιωδιούχων ΣΜ
• Η σταθερότητα των μορίων τους εκφράζεται με τη Η σταθερότητα των μορίων τους εκφράζεται με τη σταθερά θερμοκινητικής σταθερά θερμοκινητικής σταθερότητας (σταθερότητας (KKthermtherm):): όσο υψηλότερη είναι τόσο σταθερότερο είναι το μόριο όσο υψηλότερη είναι τόσο σταθερότερο είναι το μόριο
και τόσο λιγότερο ελεύθερο και τόσο λιγότερο ελεύθερο GdGd3+ 3+ αποδίδεταιαποδίδεται
• Κινητική σταθερότηταΚινητική σταθερότητα : παράμετρος που καθορίζει την απομετάλλωση του : παράμετρος που καθορίζει την απομετάλλωση του μορίου από ανταγωνιστικά συγγενήμορίου από ανταγωνιστικά συγγενή όπως όπως χαλκός και ψευδάργυροςχαλκός και ψευδάργυρος που που παίρνουν τη θέση του στην ένωση με το παίρνουν τη θέση του στην ένωση με το ligandligand και βρίσκονται σε μικρές και βρίσκονται σε μικρές ποσότητες φυσιολογικά στο αίμα: ποσότητες φυσιολογικά στο αίμα: όσο υψηλότερη είναι τόσο πιο σταθερό όσο υψηλότερη είναι τόσο πιο σταθερό είναι το μόριο. Η κινητική σταθερότητα των γραμμικών μορίων είναι είναι το μόριο. Η κινητική σταθερότητα των γραμμικών μορίων είναι σημαντικά χαμηλότερη από των μακροκυκλικώνσημαντικά χαμηλότερη από των μακροκυκλικών

Χηλικές ενώσεις γαδολινίου (Χηλικές ενώσεις γαδολινίου (Gd)Gd)
• Οι χηλικές ενώσεις γαδολινίου απομακρύνονται από τον οργανισμό Οι χηλικές ενώσεις γαδολινίου απομακρύνονται από τον οργανισμό δια των δια των νεφρώννεφρών. Ο βιολογικός χρόνος ημίσειας ζωής . Ο βιολογικός χρόνος ημίσειας ζωής Τ1/2 είναι 1,5Τ1/2 είναι 1,5hh σε ασθενείς με φυσιολογική νεφρική λειτουργία. Σε ασθενείς με σε ασθενείς με φυσιολογική νεφρική λειτουργία. Σε ασθενείς με νεφρική ανεπάρκειανεφρική ανεπάρκεια παρατείνεται παρατείνεται >30>30hh
• Μετά την αποδέσμευσή του στον οργανισμό το Μετά την αποδέσμευσή του στον οργανισμό το GdGd3+ 3+ συνδέεται με συνδέεται με άλλα ανιόντα (φωσφορικά, κιτρικά, υδροξύλια ή καρβοξύλια) και άλλα ανιόντα (φωσφορικά, κιτρικά, υδροξύλια ή καρβοξύλια) και εναποτίθεται στους ιστούς ως αδιάλυτο σύμπλοκοεναποτίθεται στους ιστούς ως αδιάλυτο σύμπλοκο

Εγκυμοσύνη και θηλασμόςΕγκυμοσύνη και θηλασμός
ΕγκυμοσύνηΕγκυμοσύνη Όταν είναι απαραίτητη η εξέταση Μαγνητικού Συντονισμού, πρέπει Όταν είναι απαραίτητη η εξέταση Μαγνητικού Συντονισμού, πρέπει
να χορηγηθεί να χορηγηθεί η μικρότερη δυνατή ποσότητα η μικρότερη δυνατή ποσότητα του του πιο σταθερού πιο σταθερού σκευάσματος γαδολινίουσκευάσματος γαδολινίου (μακροκυκλικό παράγοντα) (μακροκυκλικό παράγοντα)
Μετά τη χορήγηση σκευασμάτων γαδολινίου κατά την εγκυμοσύνη Μετά τη χορήγηση σκευασμάτων γαδολινίου κατά την εγκυμοσύνη δεν είναι απαραίτητη η διενέργεια εξετάσεων στο νεογνόδεν είναι απαραίτητη η διενέργεια εξετάσεων στο νεογνό
ΘηλασμόςΘηλασμός Μετά τη χορήγηση ΣΜ γαδολινίου yψηλού κινδύνου, ο θηλασμός θα Μετά τη χορήγηση ΣΜ γαδολινίου yψηλού κινδύνου, ο θηλασμός θα
πρέπει να πρέπει να αποφευχθεί για 24 ώρεςαποφευχθεί για 24 ώρες
Εγκυμοσύνη ή θηλάζουσα με νεφρική ανεπάρκειαΕγκυμοσύνη ή θηλάζουσα με νεφρική ανεπάρκεια Θα πρέπει να αποφεύγεται η χορήγηση ΣΜ γαδολινίου Θα πρέπει να αποφεύγεται η χορήγηση ΣΜ γαδολινίου

ΣυνοψίζονταςΣυνοψίζοντας
Έλεγχος των ασθενών που ανήκουν σε Έλεγχος των ασθενών που ανήκουν σε ομάδες υψηλού ομάδες υψηλού κινδύνουκινδύνου
Χορήγηση Χορήγηση GdGd μόνο όταν κρίνεται μόνο όταν κρίνεται απολύτως απαραίτητοαπολύτως απαραίτητο Χρήση των Χρήση των πιο σταθερώνπιο σταθερών μορίων μορίων GdGd-ΣΜ -ΣΜ (μακροκυκλικά (μακροκυκλικά
χηλικά μόρια)χηλικά μόρια) Χορήγηση της Χορήγηση της χαμηλότερηςχαμηλότερης δυνατής δόσης δυνατής δόσης Αποφυγή πολλαπλών επαναλαμβανόμενων Αποφυγή πολλαπλών επαναλαμβανόμενων
χορηγήσεων σε μικρό χρονικό διάστημα (<1εβδ)χορηγήσεων σε μικρό χρονικό διάστημα (<1εβδ)