Κλινική δ ιάγνωση και πορεία νόσου
37
Κλινική διάγνωση και πορεία νόσου Kαθ. Αθ.Σκουτέλης Ε΄Παθολογική Κλινική & Μονάδα Λοιμώξεων ΓΝΑ «Ευαγγελισμός» “ΛΟΙΜΩΞΗ ΑΠΟ ΤΟΝ ΙΟ ΓΡΙΠΗΣ A H1N1 ΝΕΩΤΕΡΑ ΔΕΔΟΜΕΝΑ” 22/09/2009, Δώμα, ΓΝΑ «Ευαγγελισμός»
-
Upload
jermaine-haney -
Category
Documents
-
view
52 -
download
4
description
“ΛΟΙΜΩΞΗ ΑΠΟ ΤΟΝ ΙΟ ΓΡΙΠΗΣ A H 1 N 1 ΝΕΩΤΕΡΑ ΔΕΔΟΜΕΝΑ” 22/09/2009, Δώμα, ΓΝΑ «Ευαγγελισμός». Κλινική δ ιάγνωση και πορεία νόσου. K αθ. Αθ.Σκουτέλης Ε΄Παθολογική Κλινική & Μονάδα Λοιμώξεων ΓΝΑ «Ευαγγελισμός». - PowerPoint PPT Presentation
Transcript of Κλινική δ ιάγνωση και πορεία νόσου
Κλινική διάγνωση και πορεία νόσου
Kαθ. Αθ.Σκουτέλης Ε΄Παθολογική Κλινική & Μονάδα Λοιμώξεων ΓΝΑ «Ευαγγελισμός»
“ΛΟΙΜΩΞΗ ΑΠΟ ΤΟΝ ΙΟ ΓΡΙΠΗΣ A H1N1 ΝΕΩΤΕΡΑ ΔΕΔΟΜΕΝΑ”22/09/2009, Δώμα, ΓΝΑ «Ευαγγελισμός»
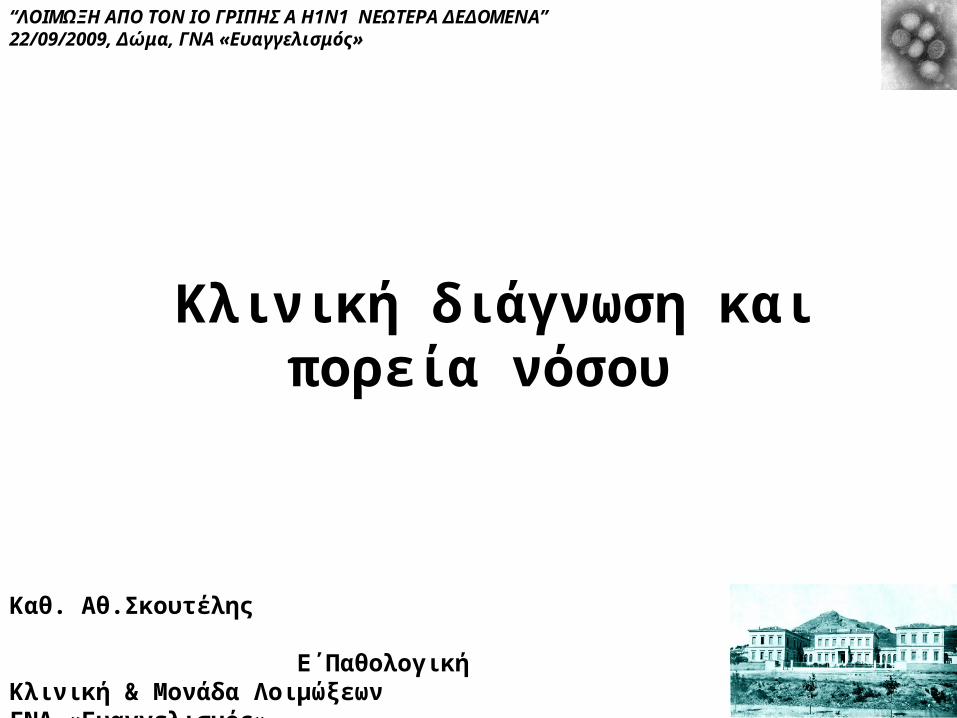
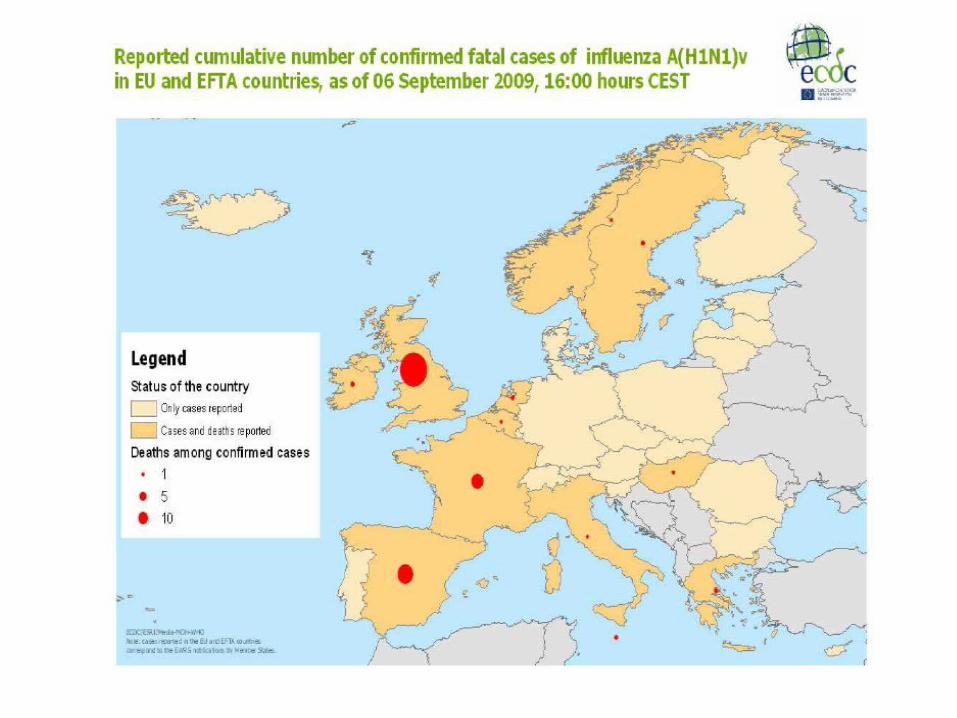
Influenza The Normal Burden of Disease
• Seasonal Influenza– Globally: 250,000 to 500,000 deaths per year– In the US (per year)
• ~35,000 deaths• >200,000 Hospitalizations• $37.5 billion in economic cost (influenza & pneumonia)• >$10 billion in lost productivity
• Pandemic Influenza– An ever present threat
4
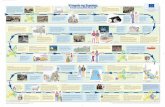
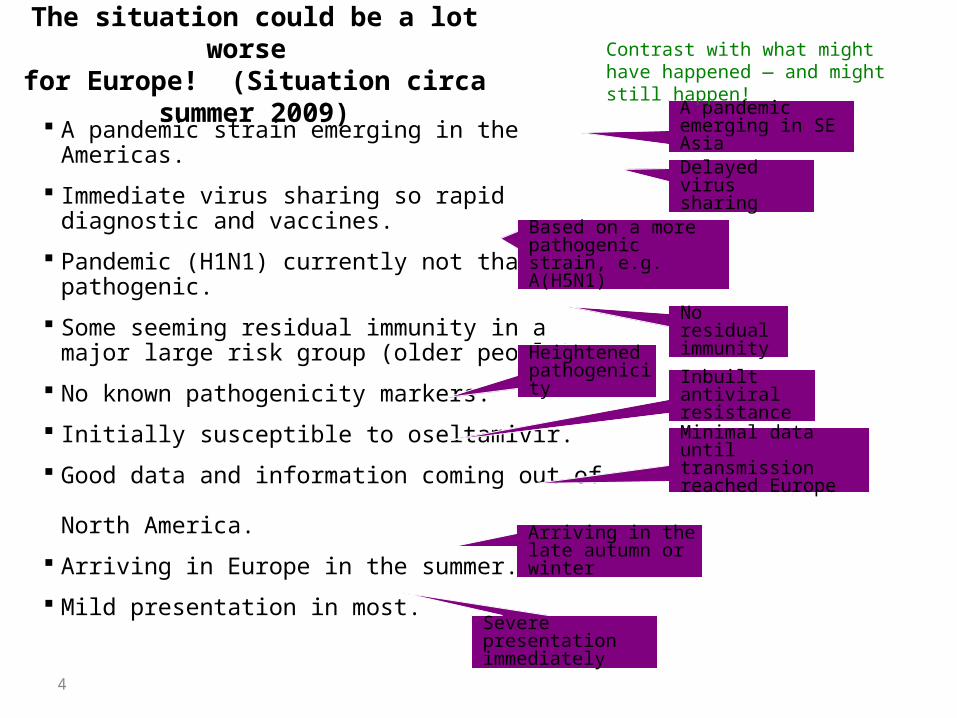
The situation could be a lot worse for Europe! (Situation circa summer 2009)
A pandemic strain emerging in the Americas.
Immediate virus sharing so rapid diagnostic and vaccines.
Pandemic (H1N1) currently not that pathogenic.
Some seeming residual immunity in a major large risk group (older people).
No known pathogenicity markers.
Initially susceptible to oseltamivir.
Good data and information coming out of North America.
Arriving in Europe in the summer.
Mild presentation in most.
A pandemic emerging in SE Asia
Delayed virus sharing
Based on a more pathogenic strain, e.g. A(H5N1)
No residual immunity
Heightened pathogenicity Inbuilt antiviral
resistance
Minimal data until transmission reached Europe
Arriving in the late autumn or winter
Severe presentation immediately
Contrast with what might have happened — and might still happen!
Η1Ν1-ΧΑΡΑΚΤΗΡΙΣΤΙΚΑ
• Μεγαλη μεταδοτικοτητα (>100Χ εποχικης)• Ηπια κλινικη εικονα• Μικρη θνητοτητα
ΓΙΑΤΙ ΑΝΗΣΥΧΟΥΜΕ;
H1N1
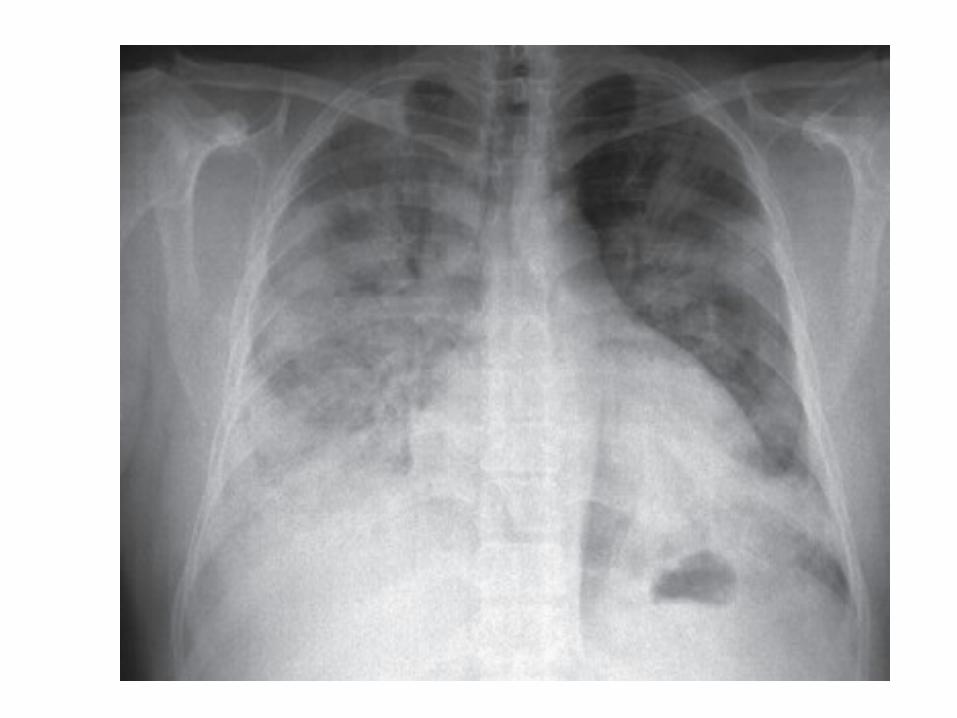
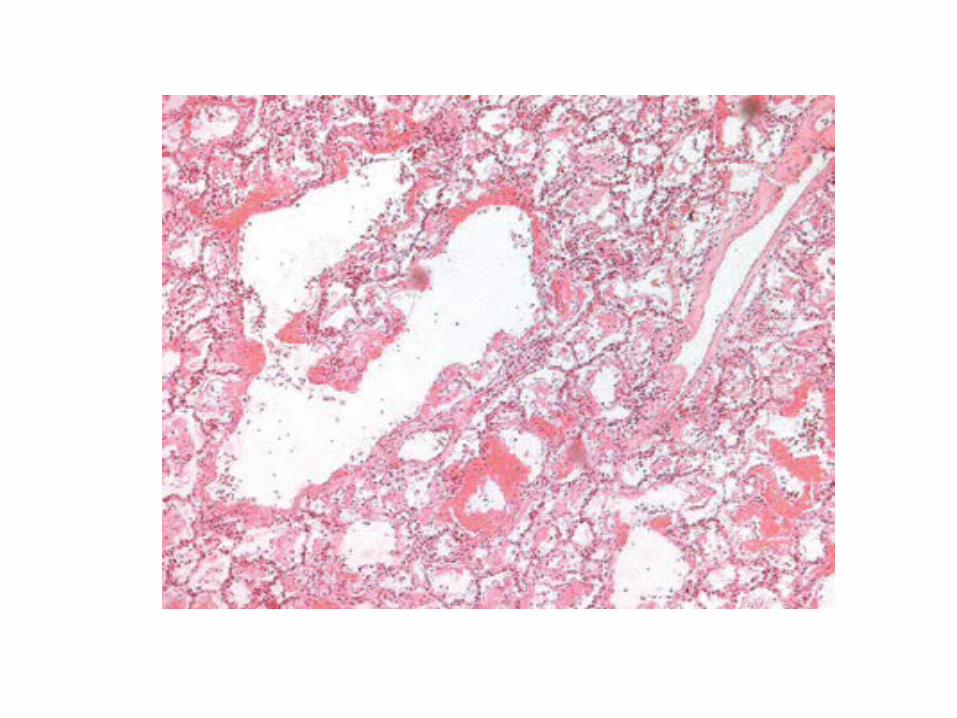
• Πανδημια• Προσβαλλει νεα/ανοσοεπαρκη ατομα• Μπορει να προκαλεσει αιφνιδια πνευμονια
ή/και ταχεια εξελιξη σε ARDS
Η1Ν1-ΧΑΡΑΚΤΗΡΙΣΤΙΚΑ
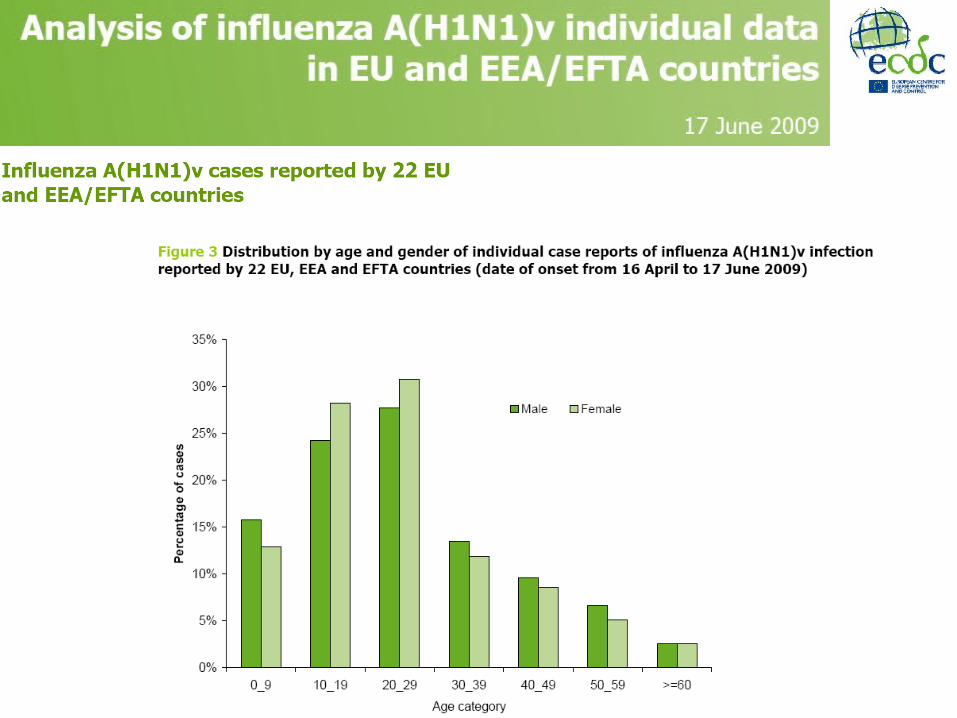
• Οι περισσοτερες περιπτωσεις:παιδια,νεοι ενηλικες• Φασμα κλινικων εκδηλωσεων:απο ηπια συμπτωματα
ανωτερου αναπνευστικου χωρις πυρετο, εως βαρεια θανατηφορο πνευμονια
• Συχνοτερα συμπτωματα: βηχας, πυρετος,κυναγχη,κακουχια,πονοκεφαλος
• Προσβολη κατωτερου αναπνευστικου σε νοσηλευομενους ασθενεις
• Αλλες επιπλοκες:ραβδομυολυση με νεφρ.ανεπαρκεια, μυοκαρδιτις, επιδεινωση υποκειμενων νοσηματων
11
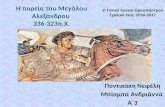
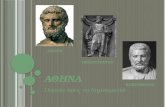
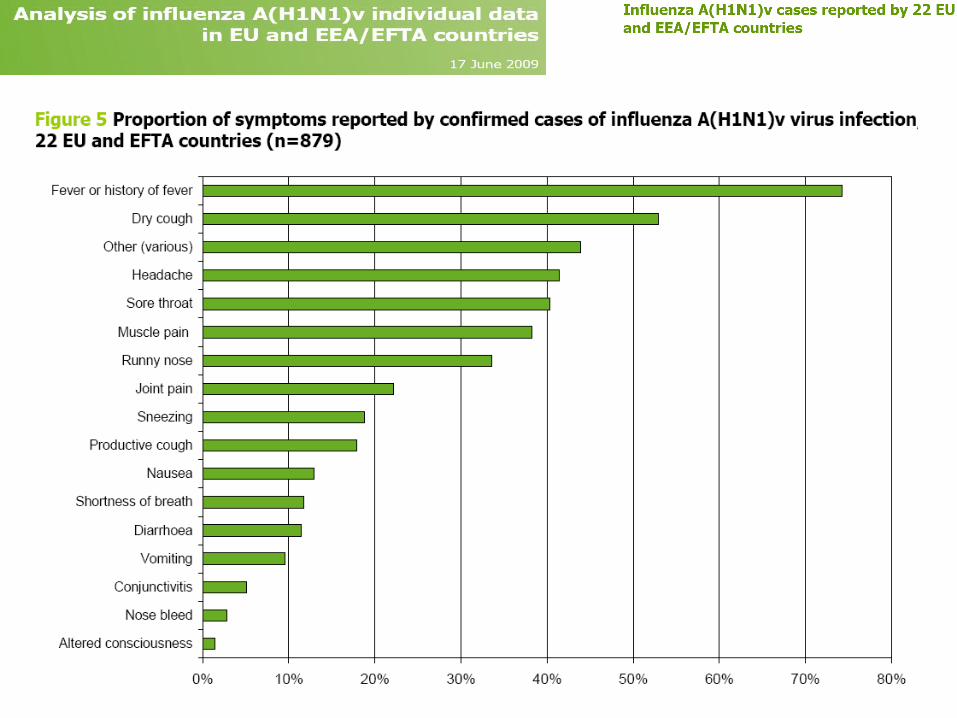
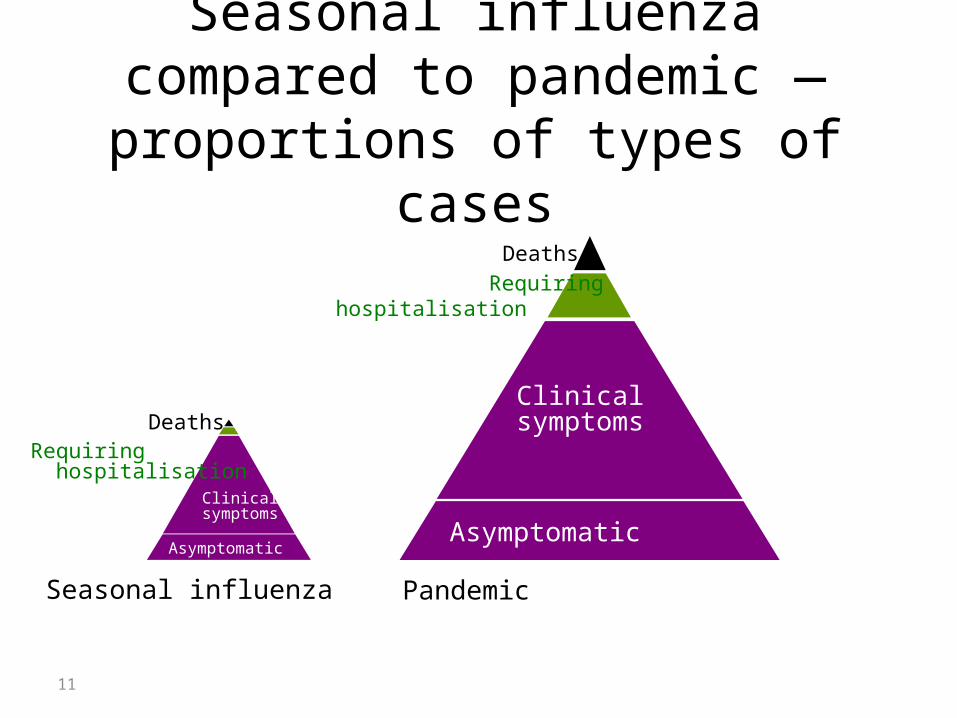
Seasonal influenza compared to pandemic — proportions of types of
cases
Asymptomatic
Clinicalsymptoms
Deaths
Requiring hospitalisation
Seasonal influenza Pandemic
Asymptomatic
ClinicalsymptomsDeaths
Requiring hospitalisation
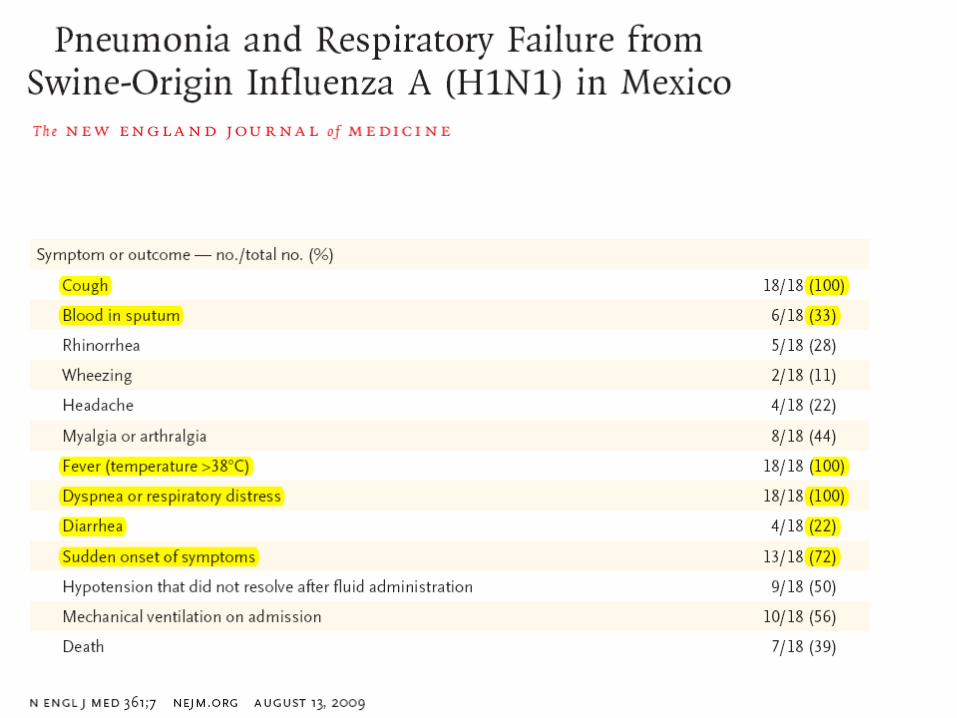
Laboratory findings
Both leukocytosis and leukopenia have been observed among hospitalized patients. In Mexico, many hospitalized patients have had leukopenia, elevated aminotransferases, elevated lactate dehydrogenase, and elevated creatinine phosphokinase. Some patients have also had renal insufficiency.
World Health Organization. Human infection with new influenza A (H1N1) virus: clinical observations from Mexico and other affected countries, May 2009. Weekly epidemiological record 2009; 84:185.
ΔΙΑΓΝΩΣΗ• Η κλινικη διαγνωση εχει αυξημενη προγνωστικη
αξια, οσο αυξανεται η επιπτωση της νοσου• Εργαστηριακη διαγνωση χρειαζεται για: - διαχειριση κρούσματος - αντιιικη θεραπεια - αποφυγη ασκοπης χρησης αντιβιοτικων WHO, Aug. 9, 2009
Rapid antigen tests • Clinicians may consider using rapid influenza antigen tests as part of their evaluation of patients suspected of having
pandemic H1N1 influenza A, but results should be interpreted with caution [70]. Confirmation of pandemic H1N1 influenza A infection can only be made by real-time reverse-transcriptase (RT)-PCR or culture.
• sensitivity 51-63%• specificity 99 %
Recommended tests
• RT-PCR
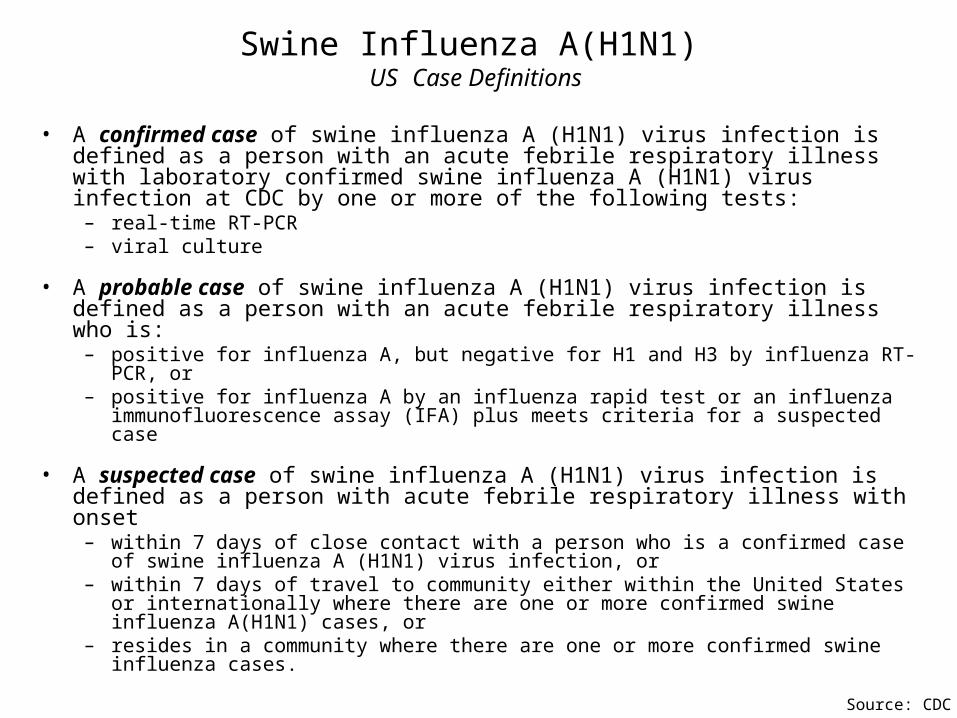
Swine Influenza A(H1N1) US Case Definitions
• A confirmed case of swine influenza A (H1N1) virus infection is defined as a person with an acute febrile respiratory illness with laboratory confirmed swine influenza A (H1N1) virus infection at CDC by one or more of the following tests:
– real-time RT-PCR – viral culture
• A probable case of swine influenza A (H1N1) virus infection is defined as a person with an acute febrile respiratory illness who is:
– positive for influenza A, but negative for H1 and H3 by influenza RT-PCR, or – positive for influenza A by an influenza rapid test or an influenza immunofluorescence assay
(IFA) plus meets criteria for a suspected case
• A suspected case of swine influenza A (H1N1) virus infection is defined as a person with acute febrile respiratory illness with onset
– within 7 days of close contact with a person who is a confirmed case of swine influenza A (H1N1) virus infection, or
– within 7 days of travel to community either within the United States or internationally where there are one or more confirmed swine influenza A(H1N1) cases, or
– resides in a community where there are one or more confirmed swine influenza cases.
Source: CDC
Η1Ν1
Οι ομαδες υψηλου κινδυνου χρειαζονται ιδιαιτερη προσοχη/χειρισμο
18
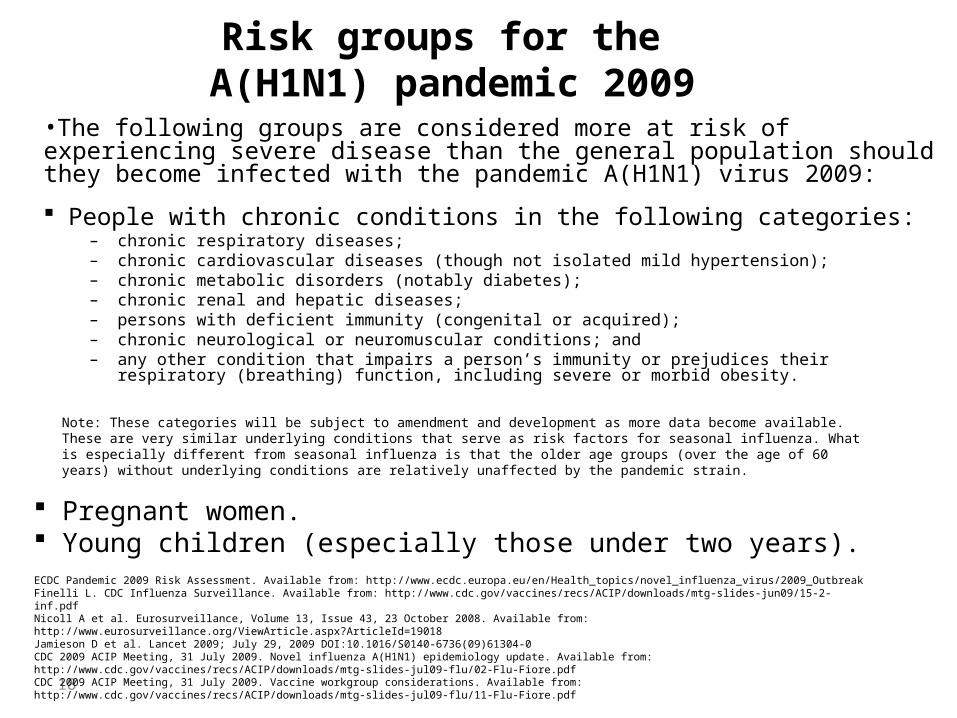
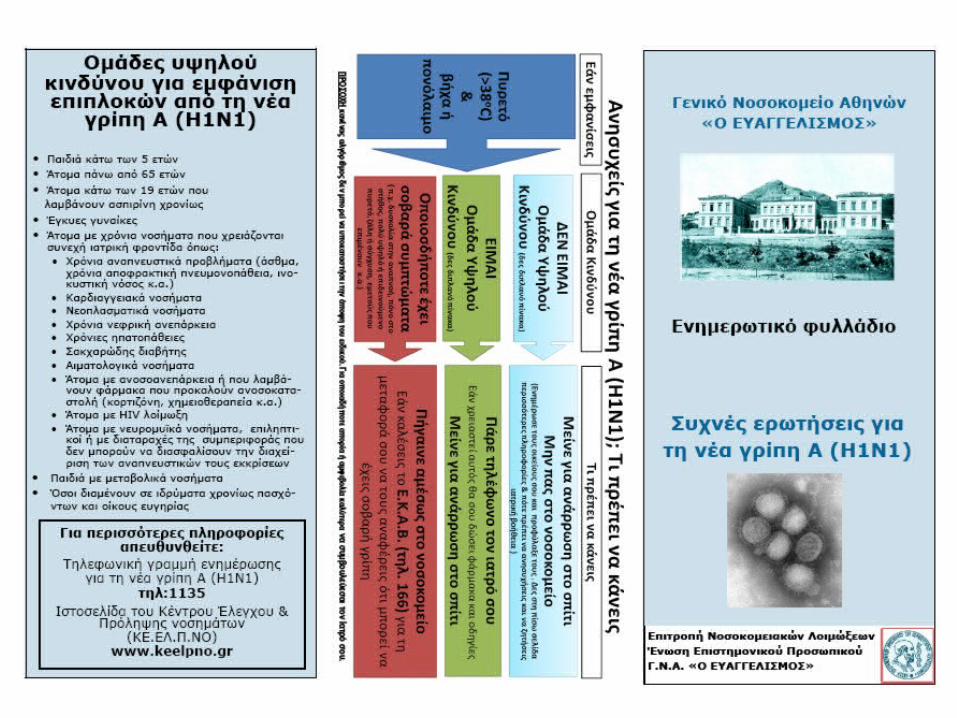
Risk groups for the A(H1N1) pandemic 2009
•The following groups are considered more at risk of experiencing severe disease than the general population should they become infected with the pandemic A(H1N1) virus 2009:
People with chronic conditions in the following categories: – chronic respiratory diseases; – chronic cardiovascular diseases (though not isolated mild hypertension); – chronic metabolic disorders (notably diabetes); – chronic renal and hepatic diseases; – persons with deficient immunity (congenital or acquired); – chronic neurological or neuromuscular conditions; and– any other condition that impairs a person’s immunity or prejudices their respiratory (breathing) function, including
severe or morbid obesity.
Note: These categories will be subject to amendment and development as more data become available. These are very similar underlying conditions that serve as risk factors for seasonal influenza. What is especially different from seasonal influenza is that the older age groups (over the age of 60 years) without underlying conditions are relatively unaffected by the pandemic strain.
Pregnant women. Young children (especially those under two years).ECDC Pandemic 2009 Risk Assessment. Available from: http://www.ecdc.europa.eu/en/Health_topics/novel_influenza_virus/2009_OutbreakFinelli L. CDC Influenza Surveillance. Available from: http://www.cdc.gov/vaccines/recs/ACIP/downloads/mtg-slides-jun09/15-2-inf.pdf Nicoll A et al. Eurosurveillance, Volume 13, Issue 43, 23 October 2008. Available from: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19018 Jamieson D et al. Lancet 2009; July 29, 2009 DOI:10.1016/S0140-6736(09)61304-0CDC 2009 ACIP Meeting, 31 July 2009. Novel influenza A(H1N1) epidemiology update. Available from: http://www.cdc.gov/vaccines/recs/ACIP/downloads/mtg-slides-jul09-flu/02-Flu-Fiore.pdfCDC 2009 ACIP Meeting, 31 July 2009. Vaccine workgroup considerations. Available from: http://www.cdc.gov/vaccines/recs/ACIP/downloads/mtg-slides-jul09-flu/11-Flu-Fiore.pdf
ΕΠΙΠΛΟΚΕΣ/ΝΟΣΗΛΕΙΑ
• Πνευμονια/ARDS σε υγιεις νεους• Επιδεινωση υποκειμενων νοσων• Αφυδατωση• ΚΝΣ, εγκεφαλιτις• Μικροβιακη επιλοιμωξη• Επιπλοκες: 15% των κλινικων περιστατικων• Νοσηλεια: 2-5% (?0.3%)• Θνητοτης (case fatality rate): 0.1-0.2 (0.35) %
Οξείες εγκεφαλίτιδες – εγκεφαλοπάθειες σε παιδιά 5% σχετίζονται με επιπλοκές γρίπη
•Σύσταση για test γρίπης σε περιπτώσεις αναπνευστικής νόσου και συμπτωμάτων από το ΚΝΣ
•Reye syndrome
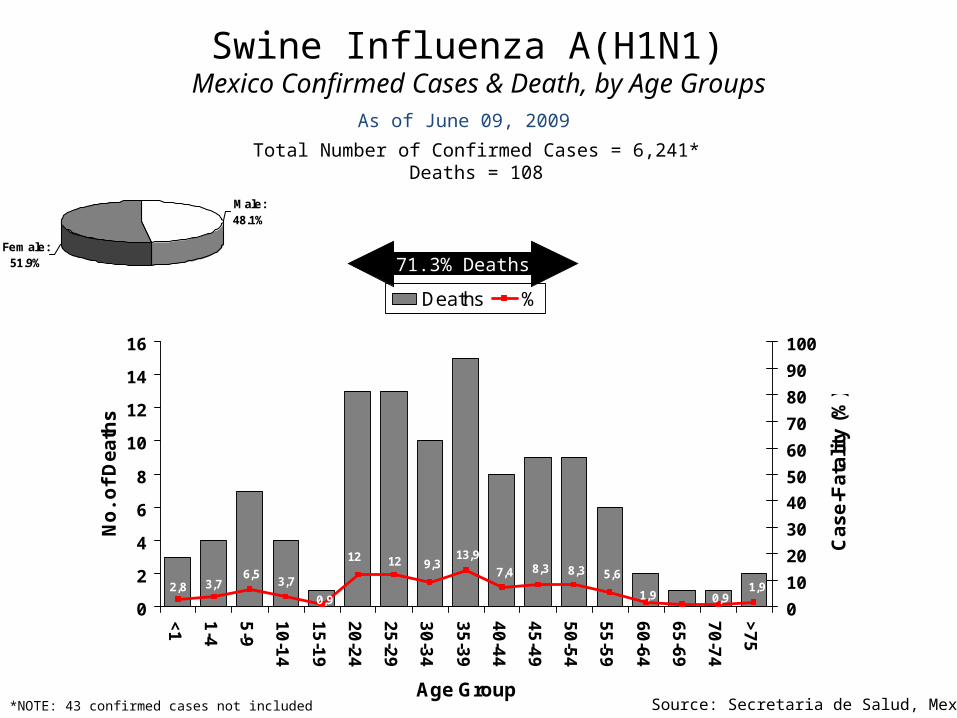
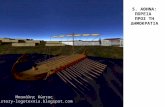
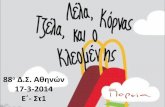
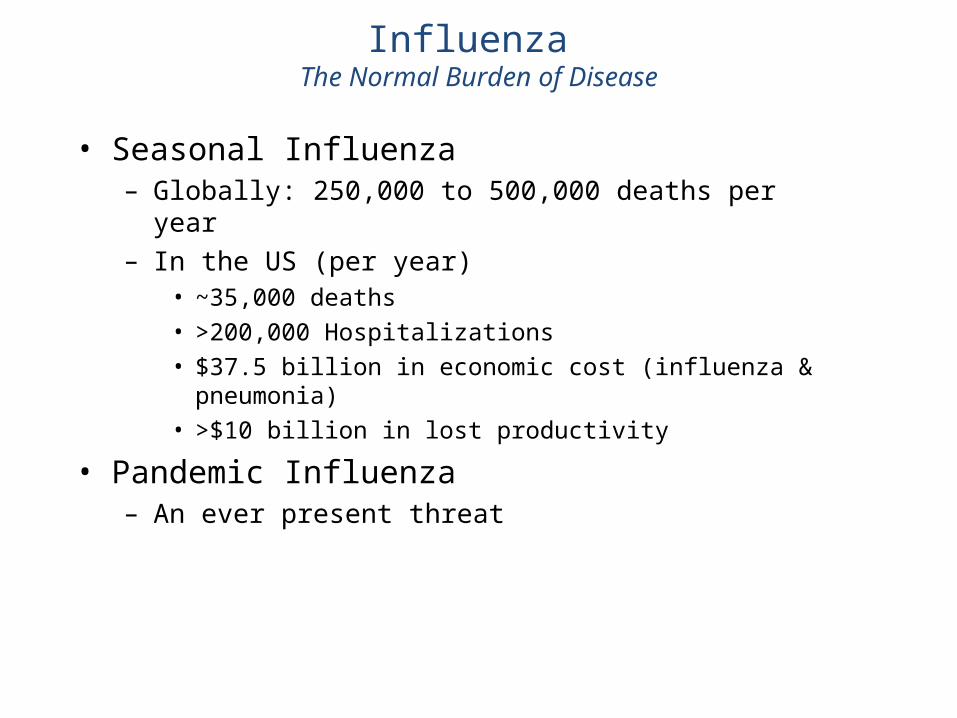
Swine Influenza A(H1N1) Mexico Confirmed Cases & Death, by Age Groups
1,90,91,9
5,68,38,37,4
13,99,31212
0,9
3,76,5
3,72,8
0
2
4
6
8
10
12
14
16
<1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
>7
5
Age Group
No
. o
f D
ea
ths
0
10
20
30
40
50
60
70
80
90
100
Ca
se
-Fa
tali
ty (
%)
Deaths %
Total Number of Confirmed Cases = 6,241*Deaths = 108
As of June 09, 2009
Source: Secretaria de Salud, Mexico
Male: 48.1%
Female: 51.9%
*NOTE: 43 confirmed cases not included
71.3% Deaths
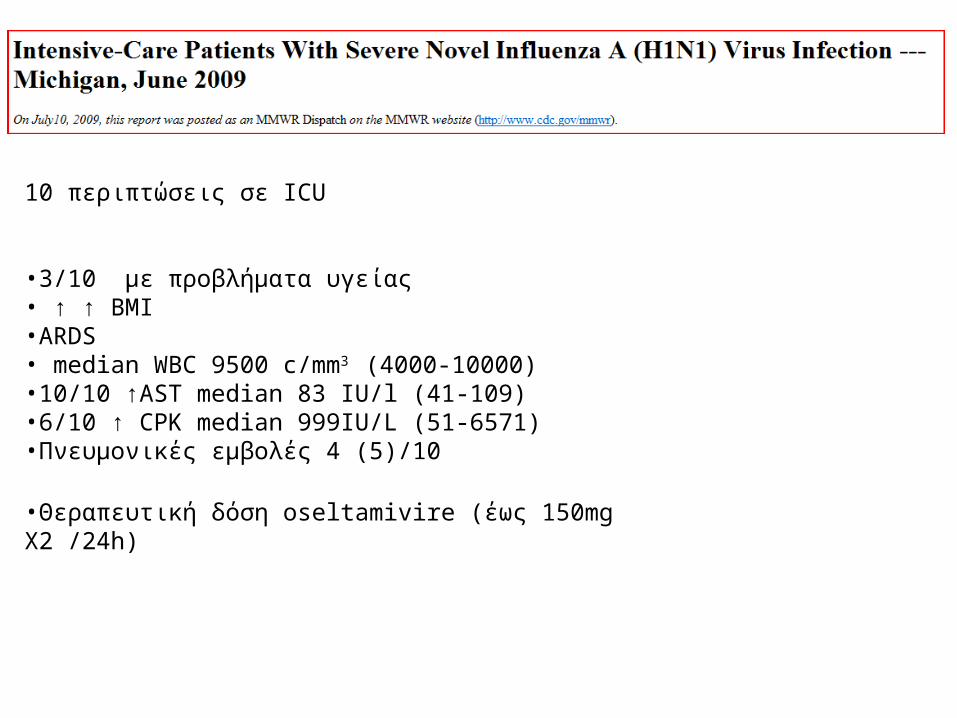
10 περιπτώσεις σε ICU
•3/10 με προβλήματα υγείας • ↑ ↑ BMI•ARDS • median WBC 9500 c/mm3 (4000-10000)•10/10 ↑AST median 83 IU/l (41-109)•6/10 ↑ CPK median 999IU/L (51-6571)•Πνευμονικές εμβολές 4 (5)/10
•Θεραπευτική δόση oseltamivire (έως 150mg X2 /24h)
...the 1918 H1N1 influenza virus pandemic…
Severe cases of H1N1 linked to low IgG2 levels
ICAAC Sep. 2009
ΝΟΣΟΚΟΜΕΙΑΚΗ ΠΕΡΙΘΑΛΨΗ
• ΑΥΞΗΜΕΝΗ ΘΝΗΤΟΤΗΤΑ• ΑΥΞΗΜΕΝΗ ΔΙΑΣΠΟΡΑ
Ορισμός ύποπτου κρούσματος για νέα γρίπη Α (Η1Ν1) σε ασθενείς που εισάγονται στο Νοσοκομείο για διερεύνηση ή
αντιμετώπιση.Οξύ εμπύρετο (>37,7 o C) χωρίς εστία λοίμωξης από την αντικειμενική εξέταση και τα πρώτα εργαστηριακά. Ασθενείς με συμπτωματολογία από το γαστρεντερικό και εμπύρετο θεωρούνται ύποπτα κρούσματα. Η κλινική κρίση του θεράποντος βαραίνει κατά περίπτωση.
Στους παραπάνω κρίνεται σκόπιμη η λήψη δείγματος για τον αποκλεισμό της νόσου και τη μείωση του κινδύνου της ενδονοσοκομειακής διασποράς
ΑΠΟΦΥΓΗ ΕΝΔΟΝΟΣΟΚΟΜΕΙΑΚΗΣ ΔΙΑΣΠΟΡΑΣ ΠΟΥ ΜΠΟΡΕΙ ΝΑ ΕΧΕΙ ΤΡΑΓΙΚΕΣ ΣΥΝΕΠΕΙΕΣ
BAΡΕΙΑ ΠΕΡΙΣΤΑΤΙΚΑ ΚΑΤΑ ΚΑΝΟΝΑ
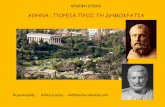
ΓΙΑΤΙ ΟΙ ΝΟΣΗΛΕΥΟΜΕΝΟΙ ΑΠΟΤΕΛΟΥΝ ΠΡΟΚΛΗΣΗ ΣΤΗΝ ΑΣΚΗΣΗ ΜΕΤΡΩΝ
ΠΡΟΣΤΑΣΙΑΣ;
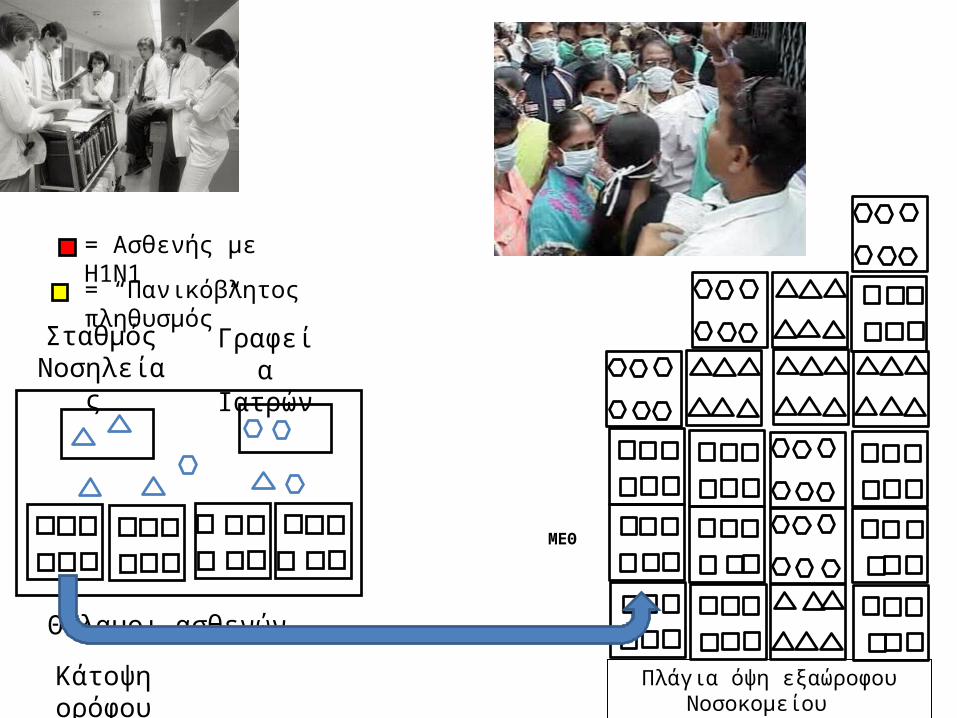
Κάτοψη ορόφου
Θάλαμοι ασθενών
ΣταθμόςΝοσηλείας
Γραφεία Ιατρών
Πλάγια όψη εξαώροφου Νοσοκομείου
ΜΕΘ
= Ασθενής με Η1Ν1
= “Πανικόβλητος πληθυσμός”

O H1N1 AΛΛΑΖΕΙ, ΕΜΕΙΣΠΡΟΣΑΡΜΟΖΟΜΑΣΤΕ!
Ε Υ Χ Α Ρ Ι Σ Τ Ω !